Upload
others
View
1
Download
0
Embed Size (px)
Citation preview
Changes in Growth Factor Responsiveness during In Vitro Maturation of Human Pluripotent Stem Cell-Derived
Cardiomyocytes
by
Petra Barbara Lücker
A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy
Department of Chemical Engineering and Applied Chemistry University of Toronto
© Copyright by Petra B. Lücker 2018
ii
Changes in Growth Factor Responsiveness during In Vitro
Maturation of Human Pluripotent Stem Cell-Derived
Cardiomyocytes
Petra Barbara Lücker
Doctor of Philosophy
Department of Chemical Engineering and Applied Chemistry
University of Toronto
2018
Abstract
Human pluripotent stem cell (hPSC)-derived cardiomyocytes (CMs) offer a promising source of
non-proliferative CMs that can be used to identify conditions that stimulate heart regeneration.
Realizing this potential requires efficient methods to generate matured hPSC-CMs that do not
readily respond to exogenous cell cycle stimulation. Therefore, the goal of this project was to
mature hPSC-CMs and test their cell cycle response in growth factor screens. Alignment on
nano-grooved substrates was the first method investigated to mature hPSC-CMs. While aligned
tissues formed and established functional syncytia, strong contractions resulted in tissue
detachment from the substrate. Next, 3D aggregate suspension was explored as an approach to
mature hPSC-CMs. Following 4 weeks in suspension, hPSC-CMs displayed a more mature
morphology, gene expression profile, and electrophysiology. Importantly, matured hPSC-CMs
were unresponsive to growth factor stimulation for cell cycle induction. Following stimulation of
aggregates with bFGF and HRG for 24h, immature hPSC-CMs initiated DNA synthesis, while
matured hPSC-CMs did not. Interestingly, both immature and matured hPSC-CMs exhibited
ERK activation in response to stimulation. A significant increase in expression of cyclin
dependent kinase (CDK) inhibitors, with a corresponding significant decrease in expression of
iii
most cyclins and CDKs, is a likely explanation for this result. To test the effect of 40 additional
growth factors on cell cycle response, a screening platform was developed. The screen revealed
overlapping and distinct hits in immature and matured hPSC-CMs. Transferring screening results
to 3D, however, resulted in no effect in matured CMs, which was found to likely be the result of
dedifferentiation in 2D, highlighting the need to perform cell cycle stimulation assays in a 3D
environment that supports a mature CM state. Overall, these results provide insights into the
development of adequate model CMs and experimental assays for discovering treatments that
induce CM cell cycle re-entry for regenerative purposes.
iv
Acknowledgments
I would like to thank my supervisor Peter Zandstra for accepting me into his lab and giving me
time and space to grow up into an independent researcher, as well as for providing the best
playground a budding scientist could ask for.
I would also like to thank Alison McGuigan for letting me work in her lab and fostering my
creativity for developing cell culture tools.
I am also grateful for my committee members Mansoor Husain and Molly Shoichet for keeping
me on my toes and always having encouraging words after every committee meeting that kept
me motivated.
I would further like to acknowledge all my collaborators for their hard work: Sahar Javaherian,
John Soleas and Duncan Halverson on the nanogroove project, Serena Tedesco for the CM
maturation studies, and Micheal Gollob and Qiuju Li for electrophysiology experiments. Thanks
to Geoff Clarke for stats support ($1000/hr) and mentorship, Céline Bauwens for writing support
and Jelena Tomic for experimental advice and discussion of my FACS data, professional advice,
and friendly chats.
I would also like to acknowledge Monica Flack, Pauline Martini, Joan Chen, and Elizabeth
Flannery for helping me navigate the administrative jungle, and especially Monica for always
having an open ear and helpful advice.
Regarding the day to day operations, there are many smart and amazing people who have made
this experience special.
Thanks to all the current and former members of the Zandstra lab for making the lab a place that
does not feel like work and where I'm never alone for too long, no matter what day of the week
or time of the day (or night).
Specifically, I'd like to thank all my fellow Zandstras who made the lab a home away from home
for me when I first came to Canada - Faisal, Kento, Naz, Nims, Chuck, Hannah, Liz, Shreya,
v
Nafees - thanks for the late-night lab dinners, movie nights, pub nights, wizard nights, camping
trips, Tetris contests, afternoon frisbee/soccer breaks, and countless tea times. And for dealing
with my European fashion advice - "Are you going running? ...Then why are you wearing
running shoes??"
Special thanks go to Faisal for proofreading and editing (read: writing from scratch) my entire
email correspondence with Peter for the first 6+ months; to Chuck for first class IT support
throughout my entire PhD, being the most helpful person I know, occasionally dealing with my
no-sleep alter ego, and challenging me to the bubble game competition; and to my night shift
buddy Nims for letting me steal his summer student desk, fighting fierce fights for the right side
of the hood, braving early morning fire alarms with me, starting spontaneous lab movie nights,
and alumin(i)um foil balls.
Thanks to my wonderful summer student (read: visiting PhD student) Serena for helping me with
my project (read: mold cultures) and fun times exploring Toronto together - I was so lucky to
have met you, have you visit a second time during a stressful job interview period, and have you
be there for me to distract me and to celebrate afterwards - CN Towerrrr!!
Thanks to Stan for great chats, helpful advice, and for taking pleasure in getting me to try
random new foods. Thanks to Yonatan for practical professional advice and being a helpful and
chatty tissue culture hood neighbor. Thanks to Himanshu Kaul for critical discussion of my
research, very helpful professional advice, spontaneous chat marathons, and mental support
during thesis writing. Thanks to Carl for making the last stretch so much more comfortable with
a bean bag chair.
Thanks to Ting, our lab mommy, for always keeping everything in order, offering emotional
support and practical advice, putting up with my endless stacks of plates, and for placing all
those last-minute orders.
Finally, thanks to Mama & Papa for all the 500±0 grams survival packages, being my safe place
during stressful times, and for always being my proudest cheerleaders.
vi
Table of Contents
Acknowledgments .......................................................................................................................... iv
Table of Contents ........................................................................................................................... vi
List of Figures ................................................................................................................................ xi
List of Abbreviations ................................................................................................................... xiii
List of Appendices ....................................................................................................................... xvi
Chapter 1 ......................................................................................................................................... 1
1 Introduction ................................................................................................................................ 2
1.1 Heart Failure ....................................................................................................................... 2
1.1.1 Research for therapies ............................................................................................. 2
1.2 HPSC-derived CMs for regenerative medicine research .................................................... 4
1.2.1 HPSC differentiation to CMs .................................................................................. 4
1.2.2 hPSC-derived CMs as in vitro model system for adult human heart ...................... 5
1.3 CM Maturation .................................................................................................................... 6
1.3.1 CM maturation during development in vivo ........................................................... 6
1.3.2 CM maturation in vitro ........................................................................................... 8
1.4 CM Cell Cycle .................................................................................................................. 16
1.4.1 Cell cycle mechanism and regulatory signaling molecules .................................. 16
1.4.2 CM cell cycle activity during human development and disease ........................... 20
1.4.3 Cell cycle in hPSC-derived CMs .......................................................................... 24
1.4.4 Targeting the CM cell cycle for therapeutic purposes .......................................... 25
1.5 Thesis hypothesis and summary ....................................................................................... 31
1.5.1 Hypothesis ............................................................................................................. 31
1.5.2 Thesis summary .................................................................................................... 31
Chapter 2 ....................................................................................................................................... 33
vii
2 A microgroove patterned multiwell cell culture plate for high-throughput studies of cell
alignment .................................................................................................................................. 34
2.1 Abstract ............................................................................................................................. 35
2.2 Introduction ....................................................................................................................... 35
2.3 Methods ............................................................................................................................. 38
2.3.1 Microgroove Plate Formation ............................................................................... 38
2.3.2 Generation of Patterned Microgrooved Substrates ............................................... 39
2.3.3 Characterization of Microgrooved Surface ........................................................... 40
2.3.4 Cell Culture and Seeding of Microgrooved Plates ............................................... 40
2.3.5 Immunocytochemistry and Proliferation Analysis ............................................... 41
2.3.6 Cell Alignment Analysis ....................................................................................... 42
2.3.7 Statistics ................................................................................................................ 42
2.4 Results and Discussion ..................................................................................................... 42
2.4.1 Fabrication and Characterization of Microgrooved 96- Well Plates .................... 42
2.4.2 Cellular Response to Microgrooved Topography ................................................. 45
2.4.3 Patterned Topographic Surfaces ........................................................................... 46
2.5 Conclusions ....................................................................................................................... 52
Chapter 3 ....................................................................................................................................... 54
3 Changes in growth factor responsiveness during in vitro maturation of pluripotent stem cell-derived cardiomyocytes .................................................................................................... 55
3.1 Abstract ............................................................................................................................. 56
3.2 Introduction ....................................................................................................................... 56
3.3 Materials and Methods ...................................................................................................... 58
3.3.1 hPSC culture ......................................................................................................... 58
3.3.2 Cardiomyocyte differentiation .............................................................................. 59
3.3.3 Cardiomyocyte maturation .................................................................................... 59
3.3.4 Aggregate size measurements ............................................................................... 60
viii
3.3.5 Cell cycle responsiveness experiment .................................................................. 60
3.3.6 Flow cytometry ..................................................................................................... 60
3.3.7 Immunocytochemistry .......................................................................................... 61
3.3.8 Transmission electron microscopy ....................................................................... 61
3.3.9 qRT-PCR ............................................................................................................... 62
3.3.10 Electrophysiology ................................................................................................. 62
3.3.11 Statistical analysis ................................................................................................. 63
3.4 Results ............................................................................................................................... 63
3.4.1 Re-aggregation of hPSC-derived CMs in suspension culture results in small
homogeneous aggregates ...................................................................................... 63
3.4.2 Re-aggregated hPSC-CMs display matured contractile cytoskeleton
morphology after 4 weeks ..................................................................................... 65
3.4.3 Re-aggregated hPSC-CMs display matured ion channel and contractile cytoskeleton gene expression ................................................................................ 66
3.4.4 Re-aggregated hPSC-CMs display changes in action potential morphology
and duration correlating with matured calcium current density ........................... 68
3.4.5 Re-aggregated hPSC-CMs do not respond to cell cycle stimulating factors ........ 70
3.5 Discussion ......................................................................................................................... 73
3.6 Conclusion ........................................................................................................................ 76
3.7 Acknowledgements ........................................................................................................... 76
Chapter 4 ....................................................................................................................................... 77
4 hPSC-derived CMs show maturation state-dependent differences in growth factor-induced
cell cycle activation in 2D and 3D assays ................................................................................ 78
4.1 Abstract ............................................................................................................................. 79
4.2 Introduction ....................................................................................................................... 79
4.3 Methods ............................................................................................................................. 82
4.3.1 hESC-CM differentiation ...................................................................................... 82
4.3.2 CM maturation ...................................................................................................... 82
ix
4.3.3 Micro-patterning ................................................................................................... 83
4.3.4 Immunocytochemistry .......................................................................................... 83
4.3.5 Growth factor screening assay .............................................................................. 83
4.3.6 Flow cytometry ..................................................................................................... 84
4.3.7 Statistics ................................................................................................................ 85
4.4 Results ............................................................................................................................... 85
4.4.1 Optimizing screening assay .................................................................................. 85
4.4.2 Patterned hPSC-CMs exhibit maturation state-dependent differences in baseline cell cycle activity as well as responsiveness to stimulation .................... 90
4.4.3 Screening of growth factor responsiveness in immature and matured CMs reveals different hit factors ................................................................................... 91
4.4.4 3D stimulation assay reveals different responsiveness of matured CMs compared to 2D stimulation .................................................................................. 92
4.5 Discussion ......................................................................................................................... 95
4.6 Conclusions ....................................................................................................................... 97
Chapter 5 ....................................................................................................................................... 98
5 Discussion ................................................................................................................................ 99
5.1 CM maturation methods evaluated with respect to application in cardiac regenerative
medicine research ............................................................................................................ 100
5.2 A roadmap for developing a therapeutic strategy ........................................................... 102
5.3 Limitations and Future Work .......................................................................................... 105
5.3.1 Limitations .......................................................................................................... 105
5.3.2 Future Work ........................................................................................................ 109
5.4 Summary and Conclusion ............................................................................................... 111
References ................................................................................................................................... 112
Appendix I .................................................................................................................................. 145
Appendix II ................................................................................................................................. 148
Appendix III ................................................................................................................................ 155
x
Appendix IV ................................................................................................................................ 157
Copyright Acknowledgements .................................................................................................... 159
xi
List of Figures
Figure 1-1: Schematic of CM cell cycle and its possible outcomes. ............................................ 19
Figure 2-1: Design and characterization of microgrooved cell culture plates. ............................. 44
Figure 2-2: Morphological alignment and quantification of confluent cells. ............................... 46
Figure 2-3: Micropatterning strategy to generate patterned topographic surfaces. ...................... 50
Figure 2-4: The effect of grooved topography on cell proliferation. ............................................ 50
Figure 2-5: Quantification of cell alignment in grooved/flat hybrid wells. .................................. 51
Figure 2-6: Average angular deviation of cells on grooves and flat spots. ................................... 52
Figure 3-1: Suspension culture of single hPSC-derived CMs leads to the formation of small,
homogenous aggregates. ............................................................................................................... 64
Figure 3-2: Structural maturation following suspension culture maturation is observed in
subsequent 2D culture and sectioned aggregates. ......................................................................... 65
Figure 3-3: Gene expression levels reveal maturation of cytoskeletal proteins and ion channels
involved in calcium handling after 4 weeks of suspension culture. ............................................. 68
Figure 3-4: Comparison of action potential and current density measurements between immature
and matured CMs reveals changes in action potential morphology and calcium current density in
matured CMs. ................................................................................................................................ 69
Figure 3-5: Downregulation of cell cycle activity and growth factor responsiveness is observed
after 4 weeks of suspension maturation. ....................................................................................... 73
Figure 4-1: CM screening assay setup. ......................................................................................... 88
Figure 4-2: CM cell cycle screening assay optimization. ............................................................. 90
Figure 4-3: Screening immature and matured CMs for cell cycle activity reveals different results
for the different maturation states. ................................................................................................ 92
xii
Figure 4-4: Transferring 2D screening results to 3D setting reveals differences in cell cycle
response in the different environments and suggests dedifferentiation of matured CMs in 2D. .. 95
Figure 5-1: Schematic of cell cycle activation roadmap. ............................................................ 105
xiii
List of Abbreviations
2D two-dimensional
3D three-dimensional
αMHC alpha myosin heavy chain
βMHC beta myosin heavy chain
AFM atomic force microscopy
AKT Protein kinase B
AP action potential
APD90 action potential duration at 90% repolarization
AR aspect ratio
ARPE19 Human retinal epithelial cells
bFGF basic fibroblast growth factor, fibroblast growth factor 2
BIO 6-bromoindirubin-3′-oxime
BJ human foreskin fibroblast cells
BMP4 bone morphogenic protein 4
BrdU 5-bromo-2'-deoxyuridine
BTC betacellulin
CAK CDK activating kinase
CAMK Ca2+/calmodulin-dependent protein kinase
CD90 cluster of differentiation 90
Cdc2 Cyclin-dependent kinase 1, cell division cycle protein 2 homolog
CDK cyclin dependent kinase
Cip CDK-interacting protein 1
CM cardiomyocyte
Cyc Cyclin
DAPI 40,6-diamidino-2-phenylindole
DiD VybrantTM DiD cell-labeling solution
DKK1 Dickkopf WNT Signaling Pathway Inhibitor 1
DMEM/F12 Dulbecco's Modified Eagle Medium: Nutrient Mixture F-12
DNA deoxyribonucleic acid
EB embryoid body
ECM extracellular matrix
EdU 5-Ethynyl-2´-deoxyuridine
ErbB4 Receptor tyrosine-protein kinase erbB-4
ERK extracellular signal–regulated kinase
FACS fluorescence activated cell sorting
FBS fetal bovine serum
FGF-1 fibroblast growth factor 1
FH fetal heart
Fluo-PDMS fluorescent PDMS
FnGel fibronectin gelatin
GFP green fluorescent protein
GLUT1 Glucose transporter 1
GLUT4 Glucose transporter type 4
GSK3b Glycogen synthase kinase 3 beta
hESC human embryonic stem cell
xiv
HGF hepatocyte growth factor
hiPSC human induced pluripotent stem cell
hPSC human pluripotent stem cell
HRG heregulin (alternative name: neuregulin)
HRGex heregulin, extracellular domain
HUVEC primary human umbilical vein endothelial cells
ICa voltage-gated calcium channel alpha 1C subunit, Cav1.2, CACNA1C
IF immunofluorescence
IGF1 insulin-like growth factor 1
IGF2 insulin-like growth factor-2
IgG immunoglobulin G
IKr potassium voltage-gated channel subfamily H member 2, hERG, KCNH2
IK1 inward-rectifier potassium ion channel, Kir2.1, KCNJ2
INa sodium voltage-gated channel alpha subunit 5, Nav1.5, SCN5A
Ink4a cyclin-dependent kinase inhibitor 2A, p16
IWP-2 inhibitor of WNT production 2
Kip Cyclin-dependent kinase inhibitor 1B
Kir2.1 potassium voltage-gated channel subfamily J member 2
KOSR knockout serum replacement
LA left atrium
lCPT1 Carnitine palmitoyltransferase I, liver isoform
lGS glycogen synthase, liver isoform
LV left ventricle
LY294002 PI3K inhibitor
MAP kinase mitogen-activated protein kinase
MAPK mitogen-activated protein kinase
mCPT1 Carnitine palmitoyltransferase I, muscle isoform
MEF mouse embryonic fibroblast
MEK Mitogen-activated protein kinase kinase, MAPK/ERK Kinase
MEKi MEK inhibitor
mGS glycogen synthase, muscle isoform
MI myocardial infarction
miRNA microRNA
MKL-1 mitotic kinesin-like protein-1
MLC2a myosin light chain 2, atrial isoform
MLC2v myosin light chain 2, ventricular isoform
mRNA messenger RNA
MTG monothioglycerol
MYH6 myosin heavy chain alpha
MYH7 myosin heavy chain beta
NEAA nonessential amino acids
NRG neuregulin (alternative name: heregulin)
P/S penicillin/streptomycin
p130 Retinoblastoma-Related Protein 2
p38 p38 MAP kinase
pAKT phosphorylated AKT
PBS phosphate buffered saline
PBST PBS with Tween-20 or Triton X-100.
xv
PD0325901 MEK inhibitor
PDGF-AA platelet-derived growth factor-AA
PDGF-BB platelet-derived growth factor-BB
PDMS polydimethylsiloxane
PEG polyethylene glycol
pERK phosphorylated ERK
PFA paraformaldehyde
pH3 phosphorylated histone 3
PI3K Phosphatidylinositol-4,5-bisphosphate 3-kinase
PI3Ki PI3K inhibitor
ROS reactive oxygen species
proANP pro-atrial natriuretic peptide
PSC pluripotent stem cell
PVC polyvinyl chloride
qRT-PCR quantitative real time – polymerase chain reaction
RA retinoic acid
RA right atrium
Rb retinoblastoma
RMP resting membrane potential
RNA ribonucleic acid
Rock inhibitor p160-Rho associated coiled-coil kinase inhibitor Y-27632
RV right ventricle
RyR ryanodine receptor
SB203580 p38 inhibitor
SD standard deviation
SEM scanning electron microscopy
SEM standard error of the mean
SERCA sarcoplasmic/endoplasmic calcium ATPase
SF serum free medium
siRNA short interfering RNA
SIRPA signal-regulatory protein alpha
SP StemPro-24 medium
TBP TATA-box binding protein
TBT Tert-Butanol
TCPS tissue culture polystyrene
TEM transmission electron microscopy
TF Thick filaments
TMRM tetramethylrhodamine methyl ester perchlorate
TNNI1 Troponin I 1, slow skeletal type
TNNI3 Troponin I 3, cardiac type
TnT Troponin T (protein)
TNT Troponin T (gene)
T3 Tri-iodo-L-thyronine
TWEAK TNF-like weak inducer of apoptosis
VEGF vascular endothelial growth factor
Wnt-3a Wnt family member 3A
ZB Z-bodies
xvi
List of Appendices
Appendix I
Supplementary figures for chapter 2.
Appendix II
Supplementary figures for chapter 3.
Appendix III
Supplementary figures for chapter 4.
Appendix IV
Supplementary figures for chapter 5.
1
Chapter 1
2
1 Introduction
1.1 Heart Failure
Cardiovascular disease is the most common cause of death worldwide being responsible for
~30% of all deaths in 2013 and according to projections, over 40% of US citizens will suffer
from a form of heart disease by 2030 (Benjamin et al., 2017; S. Mendis, Davis, & Norrving,
2015). Structural and functional abnormalities in the heart can lead to congestive heart failure
which is characterized by reduced cardiac output. Over 6 million Americans over the age of 20
die from heart failure every year with myocardial infarction (MI) being the most prevalent
underlying cause. A large MI can eradicate up to 1 billion cardiomyocytes (CMs) which
corresponds to 25% of the heart (reviewed in (Laflamme & Murry, 2011)) and the heart cannot
regenerate enough CMs to compensate for this loss. Therefore, regenerative medicine strategies,
including induction of proliferation of remaining CMs, are highly desirable.
1.1.1 Research for therapies
The goal of all therapies for myocardial injury is to re-establish the functional capacity that was
present in the healthy heart, mostly by re-establishing original CM numbers. This can be done
either via reconstitution or regeneration (Foglia & Poss, 2016). The concept of reconstitution
involves administering exogenous cells or tissue patches to restore the original function, while
the concept of regeneration focuses on using the remaining cells in the heart to generate new
cardiomyocytes, e.g. via stimulation with cell cycle induction factors.
Regarding reconstitution therapy, several studies have been conducted in rodent hearts with
varying outcomes. Different methods of administering cells are injection of cell suspensions, as
well as tissue engineering approaches including transplantation of scaffolds or cell sheets, and
injection of cells in gels (reviewed in (Feric & Radisic, 2016)). Aside from the different ways of
administration of cells, another question that exists is regarding the cell source. The latest
approach is to use human pluripotent stem cell (hPSC)- or human induced pluripotent stem cell
(hiPSC)-derived CMs since these will be the cells that most likely would ultimately be used in
clinical trials (reviewed in (Gerbin & Murry, 2015)). Riegler et al. have transplanted collagen-
3
based constructs containing hPSC-derived CMs (hPSC-CMs) into rat heart after induced MI, and
observed engraftment and long term survival (over 200 days) of the graft (over 25% of
transplanted CMs) including progressive maturation of grafted CMs, but no functional
improvement in a chronic MI model, possibly due to a lack of electrical integration of the
transplanted constructs into the host hearts caused by differences in ion channel expression
between species (Riegler et al., 2015).
Regenerative therapy could be achieved via stimulation of existing cells by stimuli from different
sources. Stimulation could occur via administration of cells that secrete stimulating factors and
provide an environment permissive for regeneration, or via administration of stimulating factors
directly. The most well studied cell source for stimulation of regeneration are mesenchymal stem
cells (MSCs), administered either via injection or via transplantation of a cell-laden patch. When
injected after MI, hypoxia preconditioned MSCs did not result in formation of new muscle but
did have significant beneficial effects on heart function and infarct size (Hu et al., 2016).
Another cell source tested are hiPSC-CMs which were shown to not engraft very well but still
result in significant functional improvement due to secretion of pro-angiogenic and pro-survival
factors (Ong et al., 2015).
The other way of achieving stimulation of endogenous repair is via administration of active
factors to manipulate remaining cells. Possible factors that have been examined for induction of
CM proliferation include growth factors, micro-RNAs, short interfering RNAs (siRNAs),
engineered viruses (for genetic manipulation), and small molecules. These studies will be
described in more detail when discussing approaches to target the CM cell cycle. Potential issues
with these approaches to be aware of include dedifferentiation of remaining CMs as part of the
proliferation process and any temporary reduction in cardiac function that may occur if too many
cells divide at the same time, as well as electrical integration and maturation of the newly formed
CMs. Another approach that has been investigated for achieving repair without cell or tissue
transplantation is the conversion of fibroblasts from the fibrotic scar to CMs. Since it has been
shown that direct conversion is possible without the use of genetic manipulation, this approach
has become a feasible option (Y. Fu et al., 2015). Low conversion efficiencies (
4
When comparing the reconstitution versus the regeneration approach with respect to feasibility
and ease of use, there are clearly challenges with cell-based reconstitution therapies including
immunocompatibility as well as cell and tissue manufacturing, which make non-cell-based
regenerative therapies a more attractive option. Research for potential regeneration inducing
factors requires an appropriate in vitro model. hPSC-CMs provide a promising cell source since
the development of efficient hPSC differentiation protocols makes them readily available.
1.2 HPSC-derived CMs for regenerative medicine research
1.2.1 HPSC differentiation to CMs
HPSCs were first discovered in 1998 (Thomson et al., 1998) and have since then been used to
generate a variety of cell types (Tabar & Studer, 2014), amongst them cardiomyocytes which
were first generated in 2001 (Kehat et al., 2001). HPSC- CMs represent a great renewable source
of CMs for in vitro experiments and possibly cell therapy. Several differentiation protocols have
been developed over the years (reviewed in (Lewandowski, Kolanowski, & Kurpisz, 2017)).
First attempts were using serum (Kehat et al., 2001; C. Xu, Police, Rao, & Carpenter, 2002; J.
Zhang et al., 2009) or END2 mouse endoderm-like cell co-culture (Mummery, Ward, & Passier,
2007), while the current state of the art protocols use a serum-free approach with small
molecules and recombinant proteins mimicking the signaling events during human cardiogenesis
in a controlled manner (Kattman et al., 2011; Xiaojun Lian et al., 2013). Differentiation can
occur in both 2D (Burridge et al., 2014; Burridge, Holmström, & Wu, 2015; Xiaojun Lian et al.,
2013, 2015; Mummery et al., 2007) and 3D (Kattman et al., 2011). Widely used 2D protocols
(Burridge et al., 2014; Xiaojun Lian et al., 2013) result in purities of up to 95 percent CMs.
These approaches use cost effective media, but require a lot of space due to the 2D culture. 3D
protocols are more amenable to large scale production. 3D differentiation in aggregates can be
done either in 6-well plates (Kattman et al., 2011) or in bioreactors (V. C. Chen et al., 2015;
Fonoudi et al., 2015; Kempf, Kropp, Olmer, Martin, & Zweigerdt, 2015). For the differentiation
of hPSCs to CMs, certain steps from the embryonic development in vivo need to be recapitulated
in vitro. This is best achieved using a specific 16-day regime of cytokine and small molecule
treatments in serum-free media (Kattman et al., 2011; L. Yang et al., 2008). At the end of the
differentiation process, after less than 3 weeks in culture, the cells express cardiac markers such
5
as Troponin T (TnT), αMHC, βMHC, MLC2v and MLC2a (Dubois et al., 2011). Regarding the
specific cardiomyocyte subtype, it has been shown that differentiation results in a mixture of
atrial, ventricular, and nodal cells (Lieu et al., 2013). Researchers have started trying to produce
specific CM subtypes, but more studies are required. An early study identified that neuregulin
signaling leads to the formation of working CMs (atrial and ventricular) and the researchers were
able to use either addition of neuregulin or anti-neuregulin antibodies to modulate the percentage
of the pacemaker cells (Wei-zhong Zhu et al., 2010). Adding neuregulin from day 5 until day 25
of differentiation resulted in a decrease of the pacemaker population from around 20% in the
control condition to 5% in the neuregulin treated condition, and adding neuregulin neutralizing
antibodies resulted in an increase of nodal cells to about 60% of the total population. This study
shows that modulation of the differentiation media formulation alone can change the output
distribution of cardiomyocyte subtypes. One of the more desirable types would be the left
ventricular working CMs since these are the ones mostly affected by injury such as myocardial
infarction (reviewed in (Laflamme & Murry, 2011)). So far, however, researchers have not
managed to specifically create only this subtype.
1.2.2 hPSC-derived CMs as in vitro model system for adult human heart
To develop new treatments for cardiac injury such as MI, regenerative medicine options need to
be studied and tested in vitro. Primary human cardiomyocytes are not readily available and
cannot be cultured in vitro for more than a month (Brandenburger et al., 2012). Cardiac myocyte
cell lines exist but are not ideal. A cardiomyocyte cell line, HL-1, that can be propagated in vitro
exists only for mouse cells and those cardiomyocytes are of the atrial subtype, i.e. not relevant
for research targeting ventricular CMs, and proliferate in culture which makes them different
from adult CMs (Claycomb et al., 1998). Animal models, mostly rodents, have proven useful,
but there are substantial differences between rodent and human hearts that may lead to non-
transferable results (Matsa, Burridge, & Wu, 2014). Thus, a suitable in vitro model system for
human adult CMs is urgently needed.
hPSC-CMs have become a well-established cell source for in vitro experiments in the field of
regenerative medicine and pharmaceutical drug development and toxicity testing since their
phenotype closely resembles that of CMs in vivo expressing relevant sarcomeric proteins and ion
6
channels (Asp et al., 2010). Unlike isolation of primary cells from mouse, rat, or human cardiac
tissue, the hPSC differentiation system provides large numbers of CMs that are required for e.g.
tissue engineering or screening purposes. Sharma et al., for instance, were able to successfully
use hiPSC-CMs for toxicity screening of anticancer drugs (Sharma et al., 2017). The use of
hPSC-CMs as a model system for adult cardiac tissue, however, still faces a major challenge
since regarding their maturation state, these cells resemble fetal cardiac cells more than adult
ones (Cao et al., 2008; Robertson, Tran, & George, 2013; Synnergren, Améen, Jansson, &
Sartipy, 2011; X. Q. Xu, Soo, Sun, & Zweigerdt, 2009). The short time frame of about two
weeks of differentiation combined with the lack of other maturation cues is not enough to result
in mature characteristics that are comparable to adult CMs. More time and further treatment is
necessary to mature the cells beyond the fetal stage such that they better resemble mature, or at
least neonatal cardiac tissue. Moreover, a system that provides CMs from the same source in
both an immature and a mature state would allow for developmental studies as well as changes in
responsiveness during development to identify underlying reasons for the specific characteristics
of mature CMs such as differences in electrophysiology, morphology, cell cycle activity, and
response to drugs.
1.3 CM Maturation
1.3.1 CM maturation during development in vivo
Immature fetal CMs are relatively small, amorphous, without a well-developed contractile
cytoskeleton, which combined with slow fetal isoforms of ion channels, results in a weak
contractile force. They also exhibit automaticity and are not yet specified into the different
subtypes (atrial, ventricular, nodal) (reviewed in (Bedada, Wheelwright, & Metzger, 2016)). As
the fetus grows, the demands to the heart increase, requiring changes in cardiomyocyte
phenotype to keep up. The cells dramatically increase in size and shape, their energy metabolism
switches from mainly glycolysis to mainly fatty acid metabolism, and isoform changes occur in
proteins of the contractile apparatus (reviewed in (Bloomekatz, Galvez-Santisteban, & Chi,
2016)). CM maturation mainly occurs in the weeks following birth (reviewed in (Jacot, Martin,
& Hunt, 2010)). This process includes formation of defined sarcomeres, cell elongation towards
a more rod-shaped morphology, hypertrophy, changes in mechanisms of calcium handling, and
7
loss of automaticity in non-pacemaker type CMs. Gene expression studies in mouse and human
cells have identified molecular differences between primary immature fetal or neonatal and
mature CMs (Harrell, Harbi, Hoffman, Zavadil, & Coetzee, 2007; Razeghi et al., 2001;
Shinozawa et al., 2009). These include expression changes in contractile proteins (e.g. increased
ratio of αMHC/βMHC (Everett, 1986) and isoform switch from TNNI1 to TNNI3 (Bedada et al.,
2014)), ion-channels (Lompré, Lambert, Lakatta, & Schwartz, 1991; Nakamura, Lee, Artman,
Rudy, & Coetzee, 1999; Qu & Boutjdir, 2001) and metabolic proteins (GLUT1 to GLUT4, lGS
to mGS, lCPT1 to mCPT1 (Razeghi et al., 2001)). Development of a strong, well-organized
contractile cytoskeleton, which involves sarcomeric protein up-regulation and organization is a
key marker for cardiomyocyte maturation. Another change is the increasing amount of
mitochondria, which can be measured via FACS (Hattori et al., 2010), and the concomitant
switch in energy metabolism from primarily glucose-based to primarily fatty acid-based
(Lopaschuk & Jaswal, 2010; Tohyama et al., 2013). Morphologically, mature cells are rod-
shaped (Bird et al., 2003) and have an increased aspect ratio of about 7:1 (132.3µm : 18.9 µm)
similar to healthy adult human CM which have aspect ratio of ~7.5:1. With this aspect ratio,
myofibrils are aligned along a single axis (Bray, Sheehy, & Parker, 2015). Regarding changes in
ion channels during maturation, calcium transients in neonatal CMs occur via extracellular
calcium current through membrane channels, while calcium transients in adult CMs occur via
calcium release from internal sarcomeric stores; this coincides with an increase in expression of
sarcoplasmic/endoplasmic calcium ATPase (SERCA2a) and Ryanodine receptor 2 (RyR)
(reviewed in (Jacot et al., 2010)). With respect to contractile function of working CMs, during
early mammalian cardiogenesis, all CMs are characterized by automaticity and a slow
conduction velocity (Mangoni & Nargeot, 2008). In the mature heart, however, ventricular
working CMs have lost their automaticity and now require stimulation from pacemaker cells to
contract (Otsuji et al., 2010). Moreover, mature CMs are characterized by a fast conduction
velocity (Mangoni & Nargeot, 2008). Another major change that occurs after birth is the change
in cell cycle activity with CMs terminally exiting the cell cycle (reviewed in (Laflamme &
Murry, 2011). In humans, this process seems to start before birth, since neonates were shown to
already have binucleated CMs, which are the result of an incomplete cell cycle. Eventually,
about 25% of CMs are binucleated in humans (Bergmann et al., 2015). Aside from binucleation,
the slow withdrawal from heart growth via cell division in humans also leads to CMs with
progressively higher DNA content, which continues until the heart has reached its final adult
8
weight (reviewed in (Laflamme & Murry, 2011)). Since CMs will increase in size by 30- to 40-
fold during heart growth after birth, they require a higher DNA content to sustain this increased
cell size. Therefore, most human CMs have a DNA content of 4n or higher.
1.3.2 CM maturation in vitro
Differences between immature and adult CMs are reviewed in Yang et al. (X. Yang, Pabon, &
Murry, 2014). Several cell culture models have been developed for CM maturation that induce
measurable differences between immature input and matured output CMs. Strategies for
maturation include cell alignment, culture in scaffolds, overexpression of ion channels or
miRNAs, addition of soluble factor, as well as prolonged culture time, all of which may include
electrical and/or mechanical stimulation. The ideal strategy may depend on the final applications
which could require different levels of maturation, complexity of tissue, and scalability.
The success of a maturation protocol can be measured in several different ways. Ideally, a
combination of analysis methods would prove changes in different cellular characteristics. To
date, maturation can be measured with respect to morphology, gene expression,
electrophysiology and contractile force. Morphological analysis can include measurements of the
overall cell size and shape and the distribution and arrangement of the contractile cytoskeleton
and organelles such as mitochondria. The former can be done via immunofluorescence (IF)
microscopy and the latter can best be assessed via transmission electron microscopy (TEM).
Generally, maturation is indicated by a larger cell size and an increased aspect ratio (leading to
the so-called rod-shaped morphology), as well as organized sarcomeres. Another aspect of
maturation is an increase in the number of mitochondria distributed along the sarcomeres
(visualized via TEM). This characteristic has also been exploited in 50-90 day old hPSC-derived
CMs to sort for CMs in a mixed population via FACS using the mitochondrial dye
tetramethylrhodamine methyl ester perchlorate (TMRM) (Hattori et al., 2010). Gene expression
analysis would ideally include a combination of measurements of proteins of the contractile
cytoskeleton, ion channels, metabolic enzymes, as well as cell cycle related proteins (Razeghi et
al., 2001). Electrophysiological analysis could measure action potentials as well as ion channel
current densities via whole cell patch clamp (Lieu et al., 2013) or calcium imaging (Nunes et al.,
2013) and could assess the response to cardioactive compounds such as caffeine, or epinephrine
9
(Nunes et al., 2013). Contractile force can be measured by putting cells on an array of micro-
posts and measuring cell movement via video microscopy (Rodriguez et al., 2014) or by putting
cells in a tissue anchored on a post on either side and then measuring post deflection via video
microscopy (Boudou et al., 2012).
1.3.2.1 Alignment
Geometric cues are important for normal CM physiology, as CMs organize their contractile
cytoskeleton in response to cues from the underlying extracellular matrix (ECM). CM shape, in
turn, regulates their contractility (Bray et al., 2015). CMs are attached to the ECM via
transmembrane receptors, such as integrins, which also transmit external geometric cues into the
intracellular space. Thus, the ECM plays an essential role in regulating the morphological
response of CMs to external perturbation (Bray et al., 2015). Changes in the ECM in vivo have
been associated with heart disease and the resulting changes in the morphology of CMs are
responsible for downstream alterations in myocardial contractility. The most important
morphological feature seems to be the aspect ratio (AR): Adult CMs isolated from healthy
human hearts have an AR of ~7.5 (Gerdes et al., 1992), whereas e.g. in the case of hypertrophy
ARs are decreased and in the case of dilated cardiomyopathy ARs are increased (reviewed in
(Gerdes, 2002)). Bray et al. investigated the influence of CM shape on the contractile
cytoskeleton (Bray et al., 2015). They found that with increasing CM aspect ratio, the number of
aligned myofibrils increases until in CMs with an aspect ratio of 7:1 the myofibrils are aligned
along one single axis, similar to what can be found in vivo.
Various groups have cultured CMs on patterned ECM lines of various dimensions to obtain
anisotropic cell organization (Nenad Bursac, Parker, Iravanian, & Tung, 2002; Camelliti,
Mcculloch, & Kohl, 2005; Gopalan et al., 2003; Lieberman, Roggeveen, Purdy, & Johnson,
1972; Motlagh, Hartman, Desai, & Russell, 2003; Motlagh, Senyo, Desai, & Russell, 2003;
Purdy, Liebeman, Roggeveen, & Kirk, 1972; Rohr, Schölly, & Kléber, 1991; Thomas et al.,
2000). Micro-scale cues of patterned lines of fibronectin, 20µm wide and 20µm spaced apart
(Domian et al., 2009), as well as alternating lines (12-25µm wide) of low and high
concentrations of fibronectin (Nenad Bursac et al., 2002; Feinberg et al., 2007) were shown to
align primary mouse CM progenitors and mouse embryonic stem cell-derived CMs (mESC-
10
CMs), as well as neonatal rat CMs, respectively. Another study demonstrated that parallel ECM
lines, 11-20µm wide and 2-8.5µm spaced apart, that were angled to match local fiber directions
measured via diffusion tensor magnetic resonance imaging (DTMRI), can mimic in vivo tissue
alignment when seeded with neonatal rat CMs (Badie, Satterwhite, & Bursac, 2009). A study by
Parrag et al. showed that culture of mESC-CMs on aligned electrospun polyurethane scaffolds
with fibre diameters of 0.6-7µm leads to in improved sarcomere organization (Parrag, Zandstra,
& Woodhouse, 2012). Moreover, on a grooved/aligned polydimethylsiloxane (PDMS) surface
with 10µm wide ridges and grooves neonatal rat CMs were shown to have a higher contractility
and to express more cardiac actin (J. Kim et al., 2008). Another technique that resulted in CM
alignment is micro-abrasion, used e.g. by Bursac et al., where polyvinyl chloride (PVC)
coverslips are micro-abraded using lapping papers (Nenad Bursac et al., 2002).
Furthermore, aside from micro-scale cues, nano-scale features can guide CM morphology as
well. A study by Kim et al. showed that culturing rat CMs on nano-scale patterned lines of
polyethylene glycol (PEG) hydrogels results in aligned tissue with improved cardiac function in
vitro. Ridge and groove sizes ranging between 250-800nm produced aligned tissue when seeded
with neonatal rat CMs (D. Kim et al., 2010). This study also determined that it takes about 5 days
for the cells to reach the maximum alignment and length. Another way of producing nano-scale
PDMS patterns is to use molds created by thermally inducing metal-coated polystyrene to shrink;
the resulting wrinkles on the surface of molded PDMS can be used to align neonatal mouse CMs
and mESC-CMs (Luna et al., 2011). Polyurethane is another substrate that can be engineered to
produce an aligned surface. Alignment of mESC-CMs in vitro using anisotropic electrospun
polyurethane has been shown to increase their maturation state as evidenced by a decrease in
ANP production (Rockwood, Akins, Parrag, Woodhouse, & Rabolt, 2008). Aside from rodent
CMs, hPSC-CMs have also been cultured on aligned substrates. Wang et al. showed better
conduction velocities and a lower incidence of arrhythmias in anisotropic hPSC-CMs cultured on
grooved substrates compared to isotropic controls (Jiaxian Wang et al., 2013).
It is noteworthy that a recent study by Han et al. did not find any beneficial effect of alignment
alone on functional maturation after culture for two weeks on fibrous scaffolds (Han, Wu, Xia,
Wagner, & Xu, 2016). The cells did show significant alignment and increase in relevant
cytoskeletal and ion channel genes, but still exhibited slower calcium transients than cells grown
on regular tissue culture polystyrene (TCPS), which made them functionally immature. The fact
11
that cells on both isotropic and anisotropic scaffolds showed more immature calcium handling
properties than cells on TCPS though suggests that the reason for the more immature functional
state may be in the scaffold material or configuration and unrelated to alignment.
In summary, CMs cultured on patterned or grooved surfaces have a more longitudinally stretched
out morphology and form anisotropic tissues. Thus, they resemble the natural shape and
organization of CMs in vivo more closely than CMs cultured on flat surfaces which are usually
pleomorphic and form isotropic tissues. Therefore, in vitro models of mature cardiac tissue
should make use of patterned surfaces to optimally mimic in vivo conditions. Unfortunately,
most of the abovementioned methods are either rather inaccurate with respect to reproducibility
of the surface geometry or very elaborate and per experiment only a few culture wells, each
around a few square centimetres in size, were used. This also required a relatively high number
of cells just to test one condition. Thus, the development of a high-throughput platform for
cardiomyocyte alignment for maturation assays would be advantageous.
Aside from geometric cues, other features of 2D culture substrates are important as well. In a
study by Bird et al., the phenotype of primary human adult CMs was investigated. They found
that these cells dedifferentiate on a plastic or glass surface (Bird et al., 2003), but when cultured
without serum at least the rod-shaped morphology was maintained. This shows that a different
culture surface than the commonly used TCPS might be necessary to achieve significant
maturation of hPSC-CMs. Using collagen-coated polyacrylamide gels with varying stiffness,
Jacot et al. showed that CMs on soft substrates with a stiffness of 10kPa had aligned sarcomeres
(Jacot, McCulloch, & Omens, 2008). The stiffness of glass, polystyrene, and PDMS are 50-90
GPa, 3-3.5 GPa, and 2.5 MPa (base:cure ratio 10:1, (Gray, Tien, & Chen, 2003))-12kPa
(base:cure ratio 50:1, (Gray et al., 2003)), respectively. Thus, out of these three substrates,
PDMS would be the best choice for maturation studies.
1.3.2.2 Tissue engineered constructs
Many studies have produced three-dimensional cardiac tissue constructs using hPSC- or hiPSC-
CMs (derived via 2D- or 3D-based differentiation protocols), either purely for in vitro studies, or
for transplantation purposes, the latter usually being larger in size. In this section, these studies
12
are examined based on the maturation state of PSC-CMs achieved in vitro. Most tissue
constructs in the literature consist of CMs and additional supporting cell types. Co-culture of
CMs with other cardiovascular cell types has been shown to be beneficial for CM morphology
and maturation, as well as tissue function (Masumoto et al., 2016; Thavandiran et al., 2013;
Tiburcy et al., 2017). Another common feature between most tissue engineered constructs is the
presence of mechanical load by positioning the tissue between two or more posts, since
mechanical load has been shown to be beneficial for maturation of CMs (Ruan et al., 2015;
Tiburcy et al., 2011). Aside from this static stimulant, some studies apply additional stimulation
such as cyclic stretch (Ruan et al., 2015) or electrical pacing (Nunes et al., 2013; Ruan et al.,
2016) to further drive the maturation state of the tissues.
A study by Tiburcy et al. showed that collagen gel-based engineered heart tissue with neonatal
rat CMs can support maturation as determined e.g. by anisotropic sarcomere organization and a
switch from fetal to adult gene expression patterns (Tiburcy et al., 2011). This study also
investigated cell cycle characteristics including cell cycle activity analyzed via DAPI staining
measured by flow cytometry which showed around 10% of CMs in S-phase on day 0 of construct
formation, which then decreased to 5% throughout the 12-day culture period. Interestingly, at the
end of the culture period, the authors found that around 40% of the CMs were binucleated, which
is a sign of CM maturation in rodents. Another rodent CM study worth mentioning achieved t-
tubulation, a sign of advanced maturation, in a tissue engineered construct of neonatal rat CMs
(Bian, Badie, Himel, & Bursac, 2014). This study also mimicked the fibre orientation in the
native human ventricle as measured via diffusion tensor magnetic resonance imaging. Three
weeks of culture resulted in matured cell morphology, conduction velocity, and calcium
handling, and importantly, the formation of t-tubules (analyzed via immunofluorescence staining
for caveolin-3) which had not been shown previously in vitro.
In the relatively new field of hPSC- and hiPSC-CM constructs, several studies have made
advances in determining the optimal formulation for induction of CM maturation. A study
comparing culture in 3D constructs of fibrinogen and Matrigel to age-matched 2D controls
observed a higher maturation state in the 3D condition after 2 weeks regarding conduction
velocity, sarcomere length, and gene expression profile of cytoskeletal proteins and ion channels
(D. Zhang et al., 2013). A more advanced study by Nunes et al. created a collagen construct by
assembling hPSC-CMs around a suture stretched between two PDMS posts (Nunes et al., 2013).
13
The researchers determined that electrical stimulation at physiological intervals for 1 week
(starting after an initial week of preculture) increases the maturation state of CMs regarding
morphology, calcium handling, and drug responses. Even though culture and treatment of
constructs for about 2 weeks seems to be most common in the field, a study by Mihic et al. found
that hPSC-CMs cultured on Gelfoam under cyclic stretch for only 3 days already showed
significant improvements in gene expression levels of cytoskeletal and ion channel proteins and
improved calcium handling properties of the constructs (Mihic et al., 2014).
Two studies by Ruan et al. used hPSC and hiPSC-CMs in collagen constructs under mechanical
load with the addition of cyclic stress (Ruan et al., 2015) or electrical stimulation (Ruan et al.,
2016) to investigate tissue maturation. The first study showed that application of cyclic stress
increased the maturation state of the tissues over static or no stress. When in the second study
electrical pacing was added to the static mechanical load, aside from the typical structural and
functional maturation (alignment, cell size, force of contraction) achieved in tissues under
mechanical load, the authors observed a further significant increase in force generation (Ruan et
al., 2016). Thus, both cyclic stress and electrical stimulation were shown to enhance the
maturation state of engineered hPSC-CM tissue constructs.
Regarding cell composition, a recent study cultured a mixture of hiPSC-CMs, endothelial cells
and vascular mural cells in mesh-like constructs of collagen I and Matrigel (Nakane et al., 2017).
Prolonged in vitro culture for 4 weeks resulted in functional maturation compared to just 2 weeks
of culture, concomitant with increased gene expression levels of ion channels. Unfortunately,
single cell-level analysis was lacking in this study (e.g. comparison of morphological aspects
such as cell size and sarcomere length, as well as binucleation and cell cycle activity). A very
recent comprehensive study by Tiburcy et al. determined optimal tissue conditions regarding
extracellular matrix, media, and cell composition (Tiburcy et al., 2017). In the optimal condition
the authors were able to achieve a high degree of maturation after 6 weeks including morphology
(rod-shape and M-bands), gene expression, and function (force of contraction, positive force
frequency response, and inotropic response). This study also showed that a high degree of hPSC-
CM maturation is possible in vitro in serum-free conditions, which is highly relevant for in vitro
studies aiming to determine the effect of e.g. growth factor stimulation.
14
Overall, these tissue engineering studies show that in hPSC-CMs, 3D culture under mechanical
load alone promotes maturation, which is increased by addition of various stimuli including
cyclic stretch and electrical pacing, and that co-culture with other cardiovascular cell types such
as fibroblasts and endothelial cell types enhances structural (and thereby also functional)
maturation of the engineered heart tissues.
1.3.2.3 Prolonged culture time
Time in culture has been shown to play a significant role in the maturation of hPSC-CMs in most
maturation protocols. In one of the earlier published differentiation protocols, Snir et al. analyzed
the differences between early and late stage embryoid bodies (EBs) differentiated using serum
(Snir et al., 2003). Early stage EBs were defined as 10-21 days old, intermediate as 21-35 days
old, and late stage from 35 days onwards. TEM showed randomly distributed myofibrils in early
stage EBs, Z-bodies in mid-stage EBs, and fusion of Z-bodies to create Z-bands in late stage
EBs, as well as organized sarcomeres in 60 days old EBs. They also found that CMs from older
EBs (day 36-60) exhibited increased cell length and almost completely exited the cell cycle as
evidenced by only 1% Ki67 and [3H]thymidine positive cells. A more recent EB-based
maturation study by Kamakura et al. observed hiPSC-derived CMs in embryoid bodies in long
term culture for a year (Kamakura et al., 2013). While there was barely any ultrastructural
organization in 2 weeks old EBs, good organization was observed after 6 months and the highest
level of organization was finally observed after 1 year of culture. Another 3D maturation
approach also analyzed hPSC-CMs after a year of suspension culture (Otsuji et al., 2010). Otsuji
et al. used a culture regime composed of adhesion culture, picking CM clusters, re-plating cells
in suspension, re-plating in adhesion culture, picking CM clusters, etc. which resulted in more
mature ion channels. Beating of aggregates was maintained for at least 3 months in suspension;
non-pacemaker cells, however, lose automaticity over time in culture as part of their maturation.
It was also found that adhesive culture arrests maturation, while suspension culture for 14 days
increases expression levels of αMHC, i.e. promotes maturation. Interestingly, primary human
adult ventricular CMs were shown to be able to survive in suspension culture for several days
(Bird et al., 2003).
15
Aside from culture in aggregates, 2D approaches have also been tested for CM maturation. A
study by Ivashchenko et al. used commercially available hiPSC-derived CMs from Cellular
Dynamics International (CDI) to determine the effect of prolonged culture time in 2D
(Ivashchenko et al., 2013). Cells were cultured in confluent sheets on gelatin-coated TCPS in the
presence of 10% FBS for up to 80 days. The authors found signs of progressive maturation
including more mature gene expression patterns (including a higher MYH6:MYH7 ratio and
increased Kir2.1 expression) as well as action potentials that could be differentiated into
ventricular, atrial, and nodal types. Another study that used prolonged 2D culture to mature
hPSC- and hiPSC-CMs cultured the cells at a sparse density instead of in confluent sheets
(Lundy, Zhu, Regnier, & Laflamme, 2013). Lundy et al. analyzed the cells after 80-120 days of
culture and found striking changes in morphology including overall cell size and shape as well as
ultrastructural organization accompanied by matured gene expression profiles. In addition, the
matured CMs also showed improved calcium handling properties and matured action potential
characteristics. In contrast to the other hPSC-CM studies, Lundy et al. also assessed
multinucleation and observed a 10-fold increase in multinucleated CMs, which is a sign of cell
cycle maturation. Unfortunately, no other cell cycle characteristics were analyzed. A more recent
study used a similar long-term single cell 2D culture approach for hiPSC-CM maturation, with
the addition of using a nanopatterned culture surface that led to alignment of CMs along the
patterns (Pioner et al., 2016). Notably, in addition to the usual signs of maturation, this study also
achieved the formation of t-tubules, a sign of advanced maturation, after 80-100 days in culture.
Regarding the overall maturation state of PSC-CMs in culture, a relevant study by Uosaki et al.
investigated the transcriptional landscape of primary mouse CMs during maturation and
compared the results to the gene expression profile of mouse PSC-CMs (Uosaki et al., 2015).
They determined that mPSC-CMs even after prolonged 2D culture for about a month are at the
fetal level and also revealed that specifically low fatty acid metabolism (gene expression was
supposed to increase) as well as high beta-catenin (gene expression was supposed to decrease)
blocks the CMs from maturing further. These findings provide a reference point for further
improvement of in vitro hPSC-CM maturation protocols.
16
1.4 CM Cell Cycle
The CM cell cycle is a unique system, highly specialized towards the cardiomyocyte cell type,
and different from the cell cycle in other somatic cells, which is why special attention is required
for researching, describing and understanding the differences. CMs actively divide during the
fetal developmental stage, but then mostly withdraw from the cell cycle shortly after birth by
first ceasing cellular divisions and subsequently also nuclear divisions. In recent years, some
light has been shed on the cause of cell cycle withdrawal in rodent CMs, identifying the switch
from a developmental hypoxic to a normoxic environment after birth as a contributor (Puente et
al., 2014), but the mechanism is still incompletely understood. It is also not well understood what
keeps adult CMs locked in a post-mitotic state. Fully understanding this mechanism could enable
the development of regenerative treatments for cardiac injury.
1.4.1 Cell cycle mechanism and regulatory signaling molecules
The mammalian cell cycle is a specific sequence of events that lead to DNA replication and
eventual equal distribution of this DNA to two daughter cells and full separation of the latter.
This result is then referred to as proliferation. The cell cycle needs to be tightly regulated to
prevent propagation of damaged DNA and to prevent unregulated proliferation, i.e. malignant
growth (reviewed in (Sheridan, Vaidya, & Mehendale, 2005)). Overall, cell cycle activity
depends on a balance of mitogenic and antimitogenic stimuli; mitogenic stimuli include
cytokines and growth factors while antimitogenic stimuli include e.g. oxidative stress and the
resulting DNA damage and presence of the p53 tumour suppressor (reviewed in (Blagosklonny,
2003)). To decide whether or not to enter the cell cycle, a cell needs to integrate extracellular and
intracellular signals including the requirement of a new cell for organ growth or homeostasis, the
presence of an adequate microenvironment for a division (including availability of nutrients), the
presence of necessary factors for proliferation (mainly ribosomes to ensure rapid transcription
during cycling), and an undamaged state of the genome to ensure healthy progeny (reviewed in
(Malumbres & Barbacid, 2001)).
Cells that are not actively cycling are considered to be in the G0 phase; these cells can be
quiescent, senescent, or terminally differentiated with only cells in the first state being able to re-
17
enter the cell cycle. For a quiescent cell to leave the G0 state, it needs to receive an exogenous
stimulus, for example in the form of a growth factor. Once a cell enters the cell cycle, it goes
through four consecutive phases, namely the initial growth phase (G1), the DNA synthesis phase
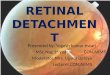
(S), the continued growth phase (G2), and the mitotic phase (M) (Figure 1-1A).
Progression through these different phases is driven via the activity of complexes comprised of a
cyclin dependent kinase (CDK) and a specific cyclin (cyc). During G0, the Retinoblastoma
protein (Rb) is bound to the transcription factor E2F, inhibiting its activity. Upon exogenous cell
cycle stimulation, an active cyclin/CDK complex phosphorylates Rb rendering it inactive, which
releases E2F. The E2F transcription factor then activates transcription of further cell cycle
progression proteins such as cyclins. Different phases of the cell cycle are marked by activity of
different cyclin/CDK complexes. Cyclin D/CDK4,6 are initiating G1-phase entry, while Cyclin
E/CDK2 is responsible for G1-phase progression. Cyclin E,A/CDK2 regulate entry and
progression through S-phase. The M-phase is regulated via Cyclin A,B/CDK1, with Cyclin
B/CDK1 specifically controlling the G2/M-phase transition. There are three Rb homologs, Rb,
p107, and p130, which all cause arrest in G1 by inhibiting transcription of genes for cell cycle
progression. Rb is regulated via its phosphorylation status at its 16 phosphorylation sites. In a
hypophosphorylated state, Rb binds E2F which inhibits transcription of E2F target genes. In a
hyperphosphorylated state, caused by CDKs in complex with cyclins, E2F is released and its
target genes can drive G1 and S progression. The CDKs, the active kinases of these complexes,
are regulated via three different mechanisms, including binding of cyclins, phosphorylation via
CDK activating kinases (CAKs), and binding of CDK inhibitors. CDKs are constitutively present
throughout the cell cycle, while the levels of cyclins fluctuate, regulated via on demand
synthesis, a short half-life (
18
The INK4 proteins are specific to the CycD/CDK4,6 complex and prevent complex formation by
binding to the CDK thereby preventing CycD from binding and activating the kinase. Members
of this family are p16 INK4a, p15 INK4b, p18 INK4c, and p19 INK4d. The second family of
CDK inhibitors are the CIP/KIP family, comprising of p21, p27, and p57, which are not specific
to any one cyclin/CDK complex.
Throughout the cell cycle there are two important checkpoints that ensure that only a healthy cell
that is fully prepared for the next stage progresses in the cell cycle. The first checkpoint is at the
G1/S transition when the cell needs to decide if the environment is still amenable for division.
This is also called the restriction point, and it determines if a cell fully commits to the cell cycle
without the need for further mitogenic stimuli or moves to a quiescent state (G0). Transition
through this point is controlled via the CycD/CDK4,6 complex. The second checkpoint is at the
G2/M transition when the cell needs to decide whether it is healthy enough (no extensive DNA
damage) to warrant and allow for proliferation.
In some cell types such as muscle cells, cell growth can be uncoupled from cell division
(reviewed in (Malumbres & Barbacid, 2001)). Moreover, unlike most other cell types,
cardiomyocytes passing through the restriction point do not have to finish the cell cycle with the
event of cell division at the end of M-phase. CMs can exit the cell cycle at different stages
(Figure 1-1B). Exiting after S-phase will result in polyploid CMs; this process is also called
endoreplication or endoreduplication. Exiting the cell cycle after nuclear division will result in
multinucleated CMs. Both options are common in healthy adult human hearts (reviewed in
(Laflamme & Murry, 2011)).
19
Figure 1-1: Schematic of CM cell cycle and its possible outcomes. (A) Blue circles containing two protein names indicate a complex; red rectangles indicate cell cycle blockers; green circles indicate
outcomes. (B) Cell cycle outcomes of a cycling CM.
20
1.4.2 CM cell cycle activity during human development and disease
During fetal heart development, CMs rapidly cycle, contributing to heart growth via cell division
(hyperplasia). This phase stops rapidly after birth when CMs exit the cell cycle and mostly
remain terminally differentiated. The majority of further growth then occurs through
hypertrophy, the increase in cell size of individual CMs while cell numbers remain mostly the
same (reviewed in (Laflamme & Murry, 2011)).
In recent years, evidence has been found that there is turnover of CMs during adult life in
humans. Very low amounts of cell cycle activity have been detected after birth and mostly been
shown to occur in children and adolescents until the heart has reached its mature size around age
20 after which no more cellular division occurs. Using two different techniques, two independent
studies (Bergmann et al., 2009; Mollova et al., 2013) reported CM turnover around age 20
between 1 and 2%. Bergmann et al. used 14C-based birth-dating (sorted for CM nuclei and
corrected for polyploidy) (Bergmann et al., 2009). Using a mathematical model in combination
with their data, they determined that CMs renew at an age-specific rate of 1% per year at 25
years and 0.45% per year at 75 years. Mollova et al. used mostly immunofluorescence staining
and microscopy for analysis (Mollova et al., 2013). Staining for phosphorylated histone 3 (pH3)
was used as a marker for nuclear division and staining for mitotic kinesin-like protein-1 (MKL-
1) was used as a marker for cellular division. The researchers found that humans had mitotic
cardiomyocytes that stained positive for pH3 throughout their lifespan, ranging from 0.01% in 1-
year old infants, to 0.009% between age 10 and 20. Cellular division via MKL-1 staining was
also detected at very low levels, ranging from 0.016% in hearts from age 0-1 years to 0.005% in
hearts between 10 and 20 years of age. Above 20 years of age, no pH3 positive or MKL-1
positive CMs were detected. Overall, this study determined that heart growth from year 1 to year
20 takes place via a 3.4-fold increase in CM numbers and an 8.6-fold increase in CM volume. A
follow-up study by Bergmann et al. using 14C-based analysis again further showed that even
though there is a low amount of constant CM turnover (
21
determined to be slightly below 70% (Mollova et al., 2013) or around 75% (Bergmann et al.,
2015; Olivetti et al., 1996) throughout life. Most other cells were found to be binucleated.
Trinucleation was found in 0.4% (Olivetti et al., 1996) or 1% (Bergmann et al., 2015) of CMs. In
addition, one of the studies also investigated the incidence of CMs with more than three nuclei
and found that 0.1% were tetranucleated (Olivetti et al., 1996). Multinucleation occurs mostly
after birth, but nevertheless, binucleated CMs were detected in human neonates, which suggests
that in some cells terminal differentiation starts before birth (reviewed in (Paradis, Gay, &
Zhang, 2014)).
While nucleation levels remain more or less the same throughout life, ploidy (the amount of
DNA copies per nucleus (2N indicating one set)), was found to change over time. Bergmann et
al. determined CM ploidy via DNA content of CM nuclei measured by FACS (Bergmann et al.,
2009), while Mollova et al. determined it via fluorescence in situ hybridization staining for a
specific chromosome and counting the number of chromosomes per nucleus (Mollova et al.,
2013); both studies obtained similar results. At birth, most CMs are diploid, but during the
hypertrophic growth phase of the heart, CM nuclei increase their DNA levels and become
tetraploid during childhood and up to 10 years of age. It was determined that there was no
increase in ploidy after the age of 10 (Bergmann et al., 2009; Mollova et al., 2013). The amount
of CMs with greater than 2N increased from around 15% to about 60% in the first 20 years and
then this percentage remained unchanged.
Even though humans cannot regenerate lost CMs sufficiently after cardiac injury to result in
functional improvement, there is evidence for increased cell cycle activity in the infarct border
zone after MI. A study by Beltrami et al. measured positive Ki67 staining in 4% of CMs in the
infarct border zone compared to 1% in the rest of the heart (Beltrami et al., 2001). This study
also used DNA staining patterns visualized via confocal imaging of propidium iodide staining (in
combination with sarcomeric α-actin) as markers for mitosis, nuclear division, and cellular
division to confirm their results. A study by Li et al. showed similar results in rats where the
percentage of cells stained positive for Ki67, phosphorylated histone 3, and aurora B kinase were
all increased in the infarct border zone compared to the rest of the heart (Y. Y. Li et al., 2013).
This study also found that the percentage of cell positive for cyclin A2 was about double in the
border zone compared to the rest of the heart (6% versus 11%). Cyclin A has been used as a
marker for S-phase and showed similar results to BrdU (Oliver & MacDonald, 2000). The
22
increase in CM cell cycle activity measured in the studies mentioned above is not nearly enough
to replace the lost cells after injury. Taken together, however, all these studies suggest that
therapies enhancing the low natural turnover and response to injury may be a valuable strategy
for treatment of cardiac injury.
1.4.2.1 Mechanism of cell cycle exit
During fetal development, CMs express high levels of positive cell cycle regulators including
cyclins and CDKs that drive cell cycle progression. Cell cycle exit after birth is accompanied by
increased levels of CDK inhibitors, decreased levels of cell cycle proteins such as cyclins and
CDKs, as well as epigenetic changes (reviewed in (Yester & Kühn, 2017)). The first stage of cell
cycle exit is the decoupling of DNA duplication from any further cell cycle events leading to
nuclei with increased DNA content, and the decoupling of nuclear division from cellular division
leading to multi-nucleated cells. The second stage subsequently involves complete cessation of
any cell cycle activity.
A lot of research has been done to identify the regulators and drivers of CM cell cycle exit
(reviewed in (Paradis et al., 2014)). Various regulatory mechanisms have been revealed that are
involved in the process and when manipulated can change the post-mitotic fate. These
mechanisms are all very diverse regarding the signaling pathways and sources of stimuli
involved. No one comprehensive theory has been published that encompasses all these
mechanisms and links them to an underlying driver. Moreover, there are considerable differences
between human and rodent CMs. In human CMs, the cell cycle exit is taking place slowly via the
course of childhood and adolescence, resulting in mostly mono-nucleated CMs with increased
DNA content (reviewed in (Laflamme & Murry, 2011)). In rodent CMs on the other hand, the
cell cycle exit occurs quite abruptly with cell division ceasing at birth and rapid cycling for about
7 days after birth leading to mostly bi-nucleated CMs (with normal 2n DNA content per
nucleus). Unfortunately, most research has been done in rodent CMs and the applicability to
human cells remains to be investigated.
A mouse study identified an environmental factor contributing to CM cell cycle withdrawal after
birth, namely the change in environmental oxygen concentration that the heart is experiencing
23
after birth. The oxygen-rich environment after birth increases levels of reactive oxygen species
(ROS) leading to DNA damage which then causes cell cycle exit (Puente et al., 2014). Treatment
of mice with n-acetyl cysteine, a ROS scavenger, on the other hand, decreases ROS levels,
thereby decreasing the DNA damage response, which then prolongs the proliferative phase after
birth.
Regarding regulators of cell cycle withdrawal, epigenetic mechanisms have been investigated as
a cause of gene expression changes leading to decreased cell cycle activity. It has been shown
that the pocket proteins Rb and p130 are required for this process (MacLellan et al., 2005) and
that the post-mitotic state is maintained via accumulation of heterochromatin (Sdek et al., 2011).
Specifically, Rb and p130 were shown to recruit HP1-γ, which is an essential component of
heterochromatin, to the promoters of E2F transcription factor-dependent genes necessary for
G2/M transition and cytokinesis, thereby silencing these genes. Kou et al. observed an increase
in global methylation in the rat heart after birth as well as increased expression of enzymes
involved in de novo DNA methylation such as methyltransferases (Kou et al., 2010). Overall,
DNA methylation in mouse CMs has also been shown to be dynamic with changes occurring
during maturation and disease playing an important regulatory role in gene expression changes
(Gilsbach et al., 2014). Another regulating mechanism for cell cycle exit in mice has been
identified to be miRNAs. Porello et al. observed that miR-195 was highly upregulated 10 days
after birth compared to the levels at birth (Porrello et al., 2011). Manipulation of miR-195 levels
resulted in altered cell cycle activity. Specifically, upregulation of miR-195 during embryonic
development resulted in reduced CM proliferation, while its knockdown at the neonatal stage
caused extended CM proliferation.
Aside from involving specific regulators, it has also been proposed that the lack of cellular
division could be due to a dysfunction in the mechanical aspects of this process, specifically, the
assembly of the contractile ring or the cleavage furrow (reviewed in (Paradis et al., 2014)). A
complex scenario with multiple regulators that may include mechanical dysfunction seems
likely.
24
1.4.3 Cell cycle in hPSC-derived CMs
CM cell cycle activity in vitro can be detected via several different methods, all of which require
co-labeling with a CM marker to exclude non-CMs from the analysis. Widely used methods are
staining for Ki67, BrdU/EdU incorporation, pH3, and aurora B kinase, as well as cell counting.
Ki67, whose function is not known, shows nuclear staining in cycling cells in all phases and is
only absent in G0 (MacCallum & Hall, 2000; Scholzen & Gerdes, 2000). Incubation with and
subsequent staining for BrdU or EdU reveals DNA synthesis as cells incorporate these
compounds into the DNA during S-phase (Mead & Lefebvre, 2014). Staining for phosphorylated
histone 3 identifies cells in mitosis from prophase to telophase that are undergoing nuclear
division (Juan et al., 1998). Finally, dividing cells during cytokinesis can be visualized via
staining for aurora B kinase which is part of the midbody during cytokinesis (Afonso,
Figueiredo, & Maiato, 2017; J. Fu, Bian, Jiang, & Zhang, 2007) or MKL-1 (Mollova et al.,
2013).
Several studies have investigated the cell cycle activity of hPSC-CMs during in vitro culture as
part of an overall charac