Embed Size (px)
Citation preview

Care Transitions : Are You in the Game?
Naomi Hauser RN, MPA
Director Care Transitions
Quality Insights of Pennsylvania
May 16, 2012

Welcome
What we’ll cover today: – Introduction of Care Transitions Program– The Role of HCA in the Community– Discuss Evidence Based Interventions to reduced
avoidable readmissions– Share Lessons Learned form 3 Year Pilot– Open Discussion
Why Are We Here?
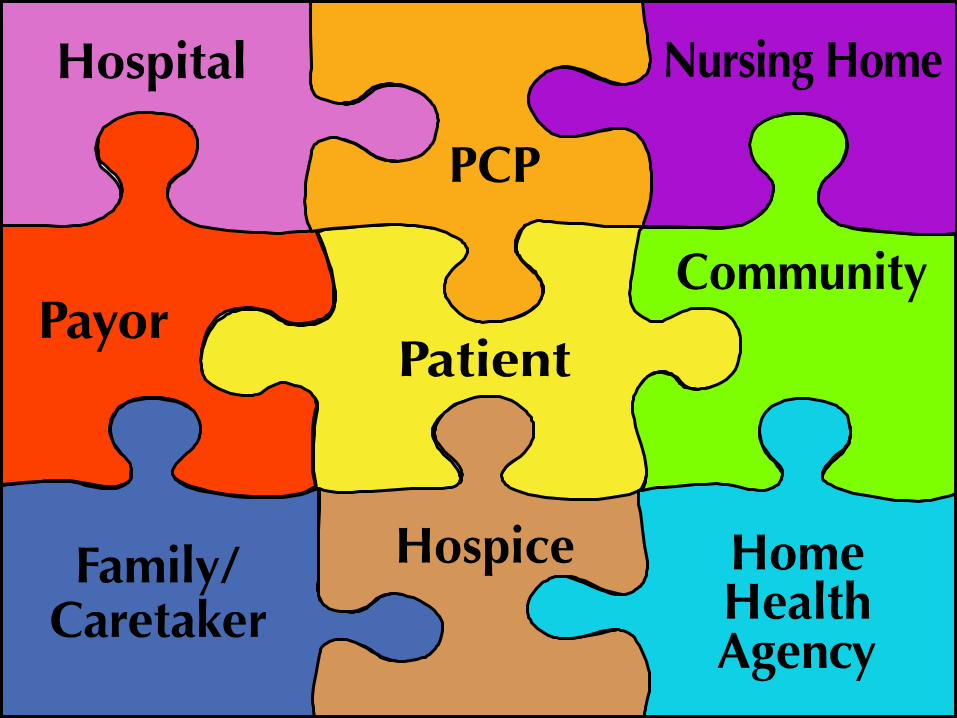
To learn about and promote safe/effective transitions of care as patients navigate from one provider setting to another – or one caregiver to another
Develop partnerships

Integrated Care For Populations and
Communities
GOALTo promote safe/effective transitions of
care as patients navigate from one provider setting to another – or one caregiver to another

30 Day Readmissions: The Problem Nationally – 17.6% of Medicare beneficiaries
discharged from the hospital are readmitted within 30 days.
More than 85% of these re-hospitalizations are unplanned.
20-40% of re-hospitalizations are possibly preventable.
64% of Medicare beneficiaries who are readmitted within 30 days do not receive any post-discharge care before readmission.

Mrs. B’s Story

339 Days in the Life of Mrs. B Day 1 – New internal medicine physician, poorly controlled diabetes with neuropathy, HTN,
osteoporosis. To see physician q. 2 wks Day 15 – Sees physician, fully functional, assists with care of grandchild and husband Day 60 – Mrs. B falls on the ice, to ER, no fractures but abrasions. Referred to home health Day 68 – Not feeling well Day 69 – Hospitalized with Staph Septicemia, dehydration, ARF, CHF, A-Fib, PN and
uncontrolled diabetes Day 82 – Transferred to SNF for short-term rehab and wound care Day 182 – Discharged to home, depressed, abrasions healed, diabetes under good control Day 183 – Nauseated, can’t find her teeth, dgt intends to call home health Day 184 – Readmitted to the hospital for dehydration, CHF, A-Fib and diabetes Day 191-337 – Admitted to in-pt rehab then to nursing home Day 338 – Readmitted to hospital w/ ARF, CHF, ARF Day 339 – Mrs. B dies

Timeline for payment penalty for hospitals
Beginning October 2012 Medicare will apply penalties and will withhold payment for avoidable 30 day acute care readmissions with a progressively increasing scale for certain DRGs.

July2008-August 2011
Pilot Project

14 QIOs with 14 Target Communities
AL: Tuscaloosa CO: Northwest Denver FL: Miami GA: Metro Atlanta East IN: Evansville LA: Baton Rouge MI: Greater Lansing area NE: Omaha NJ: Southwestern NJ NY: Upper capital PA: Western PA RI: Providence TX: Harlingen HRR WA: Whatcom county

Targeted Community Higher than state average re-admission rate Located in southwestern PA, in a community surrounding the southern
Pittsburgh metropolitan area Community spans most of Westmoreland County and small portions of
Allegheny, Washington, and Fayette counties

9th SOW Overview
CMS– 14 states
– Community cross-setting
– Transparent
– Remove silos
SWPA– 5 hospitals
– 8 home health agencies
– 15 nursing homes
– 2 AAAs
– 32 interventions
– 14% relative improvement

Structure of the Project
Cross-setting Community-based Collaborative

The Shift to…
Chronic illness management Self-care management
– Empowerment– Responsibility– Accountability– Patient activation

Cross-Setting Goal
Develop a practical, cross-setting approach Unite providers from all settings Share vision of improved health care quality Equal voices Identify provider strength

The Role of Agencies
•Home Health
•Hosicpe

Hospital Elements
Leadership buy-in Operational level leadership Education Silos Bureaucracy/slow to change Competitive Non-transparent

Hospital Interventions
Self reported readmission rate Discharge process Discharge instructions End of life options 48-hour follow-up call Schedule follow-up PCP visit CTI-AAA

SNF Elements
Education Eager to learn Eager to share Share competence levels Family Physicians Turnover

SNF Interventions
SBAR Communication transfer form Chart reviews End of life options/education POLST/AD Coach CTI

Home Health Elements
Focus on ACH vs. readmissions Medication management Low referral rates Educate on referral criteria Coaching Hands on in home care

Drivers of Hospital Readmission
Same for home care as other health care providers:– Patient activation– Standard, known processes– Transfer of information

Home Health Compare
Top 20% for this measure has maintained an unplanned hospitalization rate of 21% since last quarter
While stakeholders are focusing on reducing unnecessary hospitalizations, the data tells us that we still have work to do and…– What about those 30-day readmissions?
– Low-hanging fruit for home care to determine root cause and intervene in real-time—win-win for everyone

Home Health Compare
The latest Home Health Compare (HHC) scores were published on October 13th and reflect a data collection period of July 2010 - June 2011. Overall, the results have improved.
Hospitalization result has had a setback– Hospitalization worsened from 26% last quarter to
27%
www.Fazzi.com

Intervention HHA
Communication transfer sheet Front load visits Telehealth Phone monitoring Life line Chronic care education Coaching/partnering Depression screening Chart reviews

Best Practices
Home Health Quality Improvement National Campaign Best Practice Intervention Packages (BPIPs)
Focus on reducing ACH, improving management of oral medications and cross-setting collaboration– Simplified approach to use packages
– Standardized steps to follow for each publication
– Flexible for HHA implementation
BPIPs free to download at: http://www.homehealthquality.org/hh/default.aspx

BPIPs Include Hospitalization Risk Assessment Emergency Care Planning Medication Management Fall Prevention Care Transitions Coaching Patient Self-Management Disease Management Telehealth Introduction to new ideas/topics: Patient Centered Medical Home;
Accountable Care Organizations and others

Learn more…Coach/HH nurse
Coaching and home health service Increase Medicare HH referrals Oasis takes time Coach non-clinical Different role Medication review… patient driven Complementary/respectful

Lessons Learned
Community focus Root cause analysis Communication Transparency Leadership buy-in
Collaboration Patient-centered Ongoing monitoring Community outreach Sustainability

Lessons Learned Re-Engineers the discharge
process (Project Red, Project Boost, Medication reconciliation)
Change the paradigm of patient education (Teach Back)
Improve information transfer (Cross setting transfer form)
Increase community outreach (Collaboration with community resources, Handover)
Increase post discharge process and support (PHR, Medication management, PCP f/u appointment and coaching)

August 2011-July 2014
10th SOW
AIMS and Goals
Strategic Aims
“What will be done”
Integrate Care for Populations• Care Transitions that reduce re-admissions by 20%
within 3 years.
CMS 10th SOW for QIOs
Form a community coalition to ensure community-wide adoption of improved practices in care transitions
Assist communities in applying for the CMS 3026 CCTP funding opportunity
Form a Learning and Action Network (LAN) and provide evidence-based interventions associated with known drivers of hospital readmissions (Jan. 26, 2012)
Host quarterly LAN sessions; one in-person each year
CMS 10th SOW for QIOs
Provide the community with a template for coalition charters to help the partners formalize structure and procedures
Assist the community with root cause analysis to identify community-specific causes for poor transitions and develop data reports to monitor progress
Assist in the selection of the most appropriate evidence-based interventions
The Importance of Communities to Improve Health Care
Integrating Care for Populations and Communities

CMS Defines a Community
Defined by contiguous zip codes– Medicare beneficiaries that live in those zip codes – Committed providers and stakeholders

Community Essentials
Developed around collaborative care delivery– Shared vision– Shared mission– Shared resources– Shared decision making– Environment of trust

A Community
Social network analysis for Medicare beneficiaries in 2009– Allows visualization of relationships between
providers through network diagrams– Shows flow of transitions among providers– Senders, receivers, provider type and strength of
relationship




4 Recruited Communities
Western Pennsylvania Lehigh Valley York Chester County

Building Community Leaders reach to other leaders Expand the circle of support Grow more resources Develop/sustain commitment Recruit people
The more volunteers or members who find purpose in the community -the more they will commit resources that you may never have known existed.

Community Development
CMS suggested communities Hospitals in contiguous Zip Codes Overlap of beneficiaries/penetration Desire to reduce re-admission rates Agree to collaboration/relationship Transparency Downstream Providers

Provider Responsibilities Leadership commitment Active involvement of provider teams including
leadership in meetings, conference calls, webinars and coalition activities
Implement improvement strategies using rapid cycle testing
Create new strategies that maximize improvement for all participants
Track, monitor and share real time data

Stakeholder Support
Are the cornerstone for the community Learn from the community Inform members of CT strategies Support/provide community education sessions Participate in quarterly calls Provide publications via newsletter Post information/links of CT on Web sites

Expand the Circle of Support… Motivating Call to Action

Community
Intervention Selection

Standard/Known Process
– BOOST (Better Outcomes for Older adults through Safe Transitions)
– TCM (Transitional Care Model)
– F/U appointment made at discharge
– Pharmacy
– Telephone F/U
– Document standardization

Based on discharges from 2007. Clinical Classification Software (CCS) 2008 downloadable from http://www.ahrq.gov/data/hcup/ .
Drivers of Readmissions

Lessons Learned
Key drivers of 30 day readmissionLow patient activationLack of standard processesInadequate transfer of information across care settings
Key strategies for 30 day readmission reduction Community organizationPatient activationMulti-provider process improvement

Of discharges of CT residents from the five targeted hospitals that result in a 30-day readmission to any acute care hospital during the last six months of life– 35% are discharges to a SNF
– 33% are discharges to home under the care of a HHA
– 23% are discharges to home or self-care
– 28% of all readmissions occur during the last six months of life
End of Life
Root Cause Analysis
Simply stated RCA is a process designed to help identify not only– What and how BUT– Why
Leads to interventions selection and ongoing identification of gaps in care delivery across settings.

Intervention Selection
Derived from root cause findings Monitor & Measure
– Process Measures• System Components
– Outcome Measures• Effect of change on patient

Intervention Selection by Driver
Patient ActivationStandard/Known ProcessTransfer of Information

PROJECT RED(ReEngineered Discharge) Evidenced based toolkit. Developed by Boston University Medical Center Addresses key factors identified in RCA
– Delayed Transfer of Discharge Summary– Unknown Test Results– Patients Failure to Follow-up– Medication Interactions and Adverse Events

Transfer of Information
–Communication Re-design
–HIT
–SBAR
–Beneficiary and community outreach

Patient Activation
– INTERACT
– RED (Re-engineered Discharge)
– Medication Reconciliation
– Coaching
– Teach-Back

Coming together is a beginning.Keeping together is progress.Working together is success.
~Henry Ford

Community Care Transitions Program

The Community–based Care Transitions Program (CCTP)
The CCTP, mandated by section 3026 of the Affordable Care Act, provides funding to test models for improving care transitions for high risk Medicare beneficiaries.
•Increasing rates of avoidable hospital readmissions will result in negative health outcomes for Medicare beneficiaries impacting their levels of safety and quality of care.
•The CCTP seeks to correct these deficiencies by encouraging communities to come together and work together to improve quality, reduce cost, and improve patient experience.

CCTP: Program Goals Improve transitions of beneficiaries from the
inpatient hospital setting to other care settings •Improve quality of care •Reduce readmissions for high risk
beneficiaries •Document measureable savings to the
Medicare program

Eligible Applicants Are statutorily defined as: Acute Care Hospitals
with high readmission rates in partnership with a community based organization
Community-based organizations (CBOs) that provide care transition services
•There must be a partnership between the acute care hospitals and the CBO

CCTP: Definition of CBO
Community-based organizations that provide care transition services across the continuum of care through arrangements with subsection (d) hospitals−Whose governing bodies include sufficient representation of multiple health care stakeholders, including consumers
CCTP: Key Points CBOs will use care transition services to effectively
manage transitions and report process and outcome measures on their results.
•Applicants will not be compensated for services already required through the discharge planning process under the Social Security Act and stipulated in the CMS Conditions of Participation.
•Applicants will be required to participate in ongoing learning collaboratives

CCTP: Application Guidance Applicants are required to complete a root
cause analysis The proposals must specify how the root causes
will be addressed The proposal will describe how they will work
with accountable care organizations and medical homes if applicable
The proposal will describe how they will align their care transition programs

CCTP: Conclusion The program solicitation was announced in the
Federal Register and is now available at: http://www.cms.gov/DemoProjectsEvalRpts/MD/itemdetail.asp?itemID=CMS1239313
The program will run for 5 years with the possibility of expansion beyond 2015
If community progress is not occurring within 2 years of receiving funding, funding will be stopped
Please direct CCTP questions to: http://www.cms.gov/DemoProjectsEvalRpts/MD/itemdetail.asp?itemID=CMS1239313
CCTP Website Visit the program website for daily updates on
program status at http://www.cms.gov/DemoProjectsEvalRpts/MD/itemdetail.asp?itemID=CMS1239313
Do not forget to note Frequently-Asked Questions
On the Site

What Actions Can You Take? Look at your process What do you already have in place? What strength do you bring to the community? Be a good team player How can you collaborate to
– Improve care delivery across the continuum
– Reduce errors and avoidable re-admissions
– Share resources and reduce cost
– Improve communication and information transfer
– Improve Care Transitions

10th Scope of Work: The Opportunity for You…. Communities are developing
– Position yourselves
– Promote cross setting best practices you have implemented
– Integrate with upstream and downstream providers
– Be part of the discussion and strategic planning
– Let everyone know the role of home care and the services are critical to decreasing the rate of 30-day readmissions
– Be part of the solution!

QIO Technical Assistance
Learning and Action Networks (LAN) on a state-wide level
Webinars provided and recorded Connect to downstream providers Provide current Medicare data to providers
Resource Sharing
Upcoming conferences or meetings E-newsletters
– Share with us/success stories– Or how can we share an article with you?
Contact Krista Davis at [email protected] or
[email protected] www.qipa.org

You must be the change you wish to see in the world
MahatmasGandhi

This material was prepared by Quality Insights of Delaware, the Medicare Quality Improvement Organization for Delaware, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. Publication number 10SOW-DE-ICP-KD-010612A. App. 1/12.





























