Embed Size (px)
Citation preview

Cardiovascular Outcome Trials in Diabetes Cardiovascular Outcome Trials in Diabetes and Diabetes Preventionand Diabetes Prevention
Measuring the Balance of Benefit and Risk Measuring the Balance of Benefit and Risk of Unsweetening the Bloodof Unsweetening the Blood
Robert M. Califf, MDRobert M. Califf, MDVice Chancellor for Clinical Research Vice Chancellor for Clinical Research
Duke UniversityDuke University

CV Outcome Trials in DiabetesCV Outcome Trials in Diabetes
Conceptual framework Conceptual framework
Key tradeoffsKey tradeoffs
Barriers to implementationBarriers to implementation
Consequences of status quoConsequences of status quo

Therapeutic Principles for Cardiovascular TherapeuticsTherapeutic Principles for Cardiovascular Therapeutics
Treatment effects usually modestTreatment effects usually modest
Qualitative interactions are uncommonQualitative interactions are uncommon
Quantitative interactions commonQuantitative interactions common
Unintended targets commonUnintended targets common
Long-term vs. short-term effects may differLong-term vs. short-term effects may differ
Combinations are unpredictableCombinations are unpredictable
Class effect may not be validClass effect may not be valid
Most treatments produce a mixture of benefits and risksMost treatments produce a mixture of benefits and risksCaliff and DeMets Circ 2002

Therapeutic Principles for Cardiovascular TherapueticsTherapeutic Principles for Cardiovascular Therapuetics
Most beneficial therapies do not save money, but Most beneficial therapies do not save money, but create incremental benefit for incremental costcreate incremental benefit for incremental cost
Applying the results of clinical trials is beneficialApplying the results of clinical trials is beneficial
Many areas of medicine are underserved and Many areas of medicine are underserved and therefore lack evidence to guide practicetherefore lack evidence to guide practice
Our current method of doing trials is Our current method of doing trials is unnecessarily expensiveunnecessarily expensive
Participation is criticalParticipation is criticalCaliff and DeMets Circ 2002

Therapeutics—Inescapable FactsTherapeutics—Inescapable Facts
What we know:What we know:
Systemic therapies affect multiple biological systemsSystemic therapies affect multiple biological systems
On target and off target (most of which we do not On target and off target (most of which we do not understand while the drug is being developed)understand while the drug is being developed)
How we behave:How we behave:
As if we can tell that a treatment is providing a As if we can tell that a treatment is providing a benefit by looking at one or 2 parameters (BP, Hgb benefit by looking at one or 2 parameters (BP, Hgb A1C)A1C)

Unintended TargetsUnintended Targets
TorcetrapibTorcetrapib ? Aldosterone/adrenal? Aldosterone/adrenal
TZDsTZDs BonesBones
ErythropoietinErythropoietin CV eventsCV events
Drug eluting stentsDrug eluting stents Stent thrombosisStent thrombosis

Therapeutics—Inescapable FactsTherapeutics—Inescapable Facts
What we know:What we know:
Effects of most therapies on humanly meaningful Effects of most therapies on humanly meaningful outcomes are modest so that randomization is outcomes are modest so that randomization is essential with large sample sizesessential with large sample sizes
How we behave:How we behave:
Doctors can tell whether chronic therapies are Doctors can tell whether chronic therapies are having a net beneficial effect by their memories of having a net beneficial effect by their memories of their own patients or observing individual patientstheir own patients or observing individual patients
Post randomization databases can tell us about post Post randomization databases can tell us about post marketing treatment effectsmarketing treatment effects

Aspirin: A “Wonder” Drug

Aspirin: A “Wonder” Drug

PtsRandomized Chance of Comments
Deaths (Risk = 10%) Type II Error* on Sample Size
0-50 < 500 > 0.9 Utterly inadequate
50-150 1000 0.7-0.9 Probably inadequate
150-350 3000 0.3-0.7 Possibly inadequate
350-650 6000 0.1-0.3 Probably adequate
> 650 10000 < 0.1 Adequate
PtsRandomized Chance of Comments
Deaths (Risk = 10%) Type II Error* on Sample Size
0-50 < 500 > 0.9 Utterly inadequate
50-150 1000 0.7-0.9 Probably inadequate
150-350 3000 0.3-0.7 Possibly inadequate
350-650 6000 0.1-0.3 Probably adequate
> 650 10000 < 0.1 Adequate
Sample SizeSample SizeSample SizeSample Size
Yusuf Progr CV Dis 1985Yusuf Progr CV Dis 1985
*Probability of failing to achieve p < .01 if risk reduction = 25%
9503CG019503CG01

Therapeutics—Inescapable FactsTherapeutics—Inescapable Facts
What we knowWhat we know
The effects of therapies are context dependentThe effects of therapies are context dependent
Interactions with other treatments are common and Interactions with other treatments are common and unpredictableunpredictable
Length of treatment is importantLength of treatment is important
Clinical environment mattersClinical environment matters
How we behaveHow we behave
Drugs can be “tested” for measurement of human Drugs can be “tested” for measurement of human benefit as in a laboratory over a short period of time benefit as in a laboratory over a short period of time in any part of the worldin any part of the world

Therapeutics—Inescapable FactsTherapeutics—Inescapable Facts
What we know:What we know:
Therapies cause a mixture of benefit and harm often Therapies cause a mixture of benefit and harm often involving different organs/systems over different involving different organs/systems over different periods of timeperiods of time
How we behaveHow we behave
Short term studies done preapproval can actually Short term studies done preapproval can actually provide assurance that a drug is “safe and effective”provide assurance that a drug is “safe and effective”

Good EffectsGood EffectsGood EffectsGood Effects Bad EffectsBad EffectsBad EffectsBad Effects
Adapted from FurbergAdapted from Furberg
Therapies Always Cause a Combination Therapies Always Cause a Combination of:of:

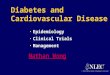
Zoledronic Acid 5 mg Reduced Risk of All-Cause Mortality by 28% Over Time—but no difference seen in first 16 months!
Zoledronic Acid 5 mg Reduced Risk of All-Cause Mortality by 28% Over Time—but no difference seen in first 16 months!
Month
0
2
4
6
8
10
12
14
16
18 Hazard Ratio, 0.72 (95% CI, 0.56–0.93)P = .0117
Cu
mu
lati
ve I
ncid
en
ce (
%)
0 4 8 12 16 20 24 28 32 36
No. at RiskZOL 5 mg 1054 1029 987 943 806 674 507 348 237 144
Placebo 1057 1028 993 945 804 681 511 364 236 149
ZOL 5 mg (n = 1065)Placebo (n = 1062)
28%
Absolute Risk Reduction, 3.7%

The Failure of Hormone Replacement Therapy: The Failure of Hormone Replacement Therapy: Worse than neutral initially!Worse than neutral initially!
1515
1010
55
00
Estrogen + ProgestinEstrogen + ProgestinPlaceboPlacebo
Inci
denc
e (%
)In
cide
nce
(%)
Follow-Up, y (No. at Risk)Follow-Up, y (No. at Risk)
Log Rank p=0.91Log Rank p=0.91
00(2763)(2763)
11(2631)(2631)
22(2506)(2506)
33(2392)(2392)
44(1435)(1435)
55(113)(113)
HERSHERSHERSHERS WHIWHIWHIWHI

AdvertisingAdvertising
““The science of arresting the human intelligence The science of arresting the human intelligence long enough to get money from it” long enough to get money from it” — — Stephen Stephen LeacockLeacock
Hippocampus—”prescription-writing center of Hippocampus—”prescription-writing center of the brain”…”processes information by the brain”…”processes information by connecting new concepts with the parts of the connecting new concepts with the parts of the brain where gut instincts are formed, areas that brain where gut instincts are formed, areas that influence emotional behavior and form influence emotional behavior and form memories”memories”
—Advertisements that go directly to the hippocampus. Lancet 1996

Therapeutics—Inescapable FactsTherapeutics—Inescapable Facts
What we know:What we know:
Our current methods of implementing clinical trials Our current methods of implementing clinical trials are harmfully and unnecessarily bureaucratic and are harmfully and unnecessarily bureaucratic and expensiveexpensive
How we behave:How we behave:
Since we can’t change the cost of trials we have to Since we can’t change the cost of trials we have to find shortcuts even if it jeopardizes the public healthfind shortcuts even if it jeopardizes the public health

Therapeutics—Inescapable FactsTherapeutics—Inescapable Facts
What we know: What we know:
We all have biases and conflicts of interest that prevent We all have biases and conflicts of interest that prevent one sure answer to most clinical trial questionsone sure answer to most clinical trial questions
How we behave:How we behave:
Companies can conduct their own trials, “hiring” Companies can conduct their own trials, “hiring” investigators without independent study investigators without independent study management and analysis of the results and management and analysis of the results and produce unbiased results or …produce unbiased results or …
If its NIH there is no biasIf its NIH there is no bias

Relation Between Statistical Significance Relation Between Statistical Significance and Publication Status in 285 Studiesand Publication Status in 285 Studies
Easterbrook, Lancet, 1991Easterbrook, Lancet, 1991

Reasons for Not Publishing 78 of 285 Reasons for Not Publishing 78 of 285 StudiesStudies Easterbrook, Lancet, 1991Easterbrook, Lancet, 1991

Copyright restrictions may apply.
Ridker, P. M et al. JAMA 2006;295:2270-2274.
Proportion of Trials Significantly Favoring Newer Treatments Over Standard of Care

Turmoil in Clinical Research:Turmoil in Clinical Research:Research Agreements between AMCs and Research Agreements between AMCs and IndustryIndustry
Do research agreements between medical Do research agreements between medical schools and industry sponsors adhere to the schools and industry sponsors adhere to the
standards embodied in the new ICMJE standards embodied in the new ICMJE guidelines?guidelines?
““We encourage investigators to use theWe encourage investigators to use therevised ICMJE requirements…to guide therevised ICMJE requirements…to guide the
negotiation of research contracts.”negotiation of research contracts.”
JAMA. 2001;286:1232-1234.JAMA. 2001;286:1232-1234.——Schulman KA, et al. NEJM 2002;347:1335Schulman KA, et al. NEJM 2002;347:1335

Conflict of Interest in Clinical Research:Conflict of Interest in Clinical Research:Research Agreements between AMCs and Research Agreements between AMCs and IndustryIndustry
Conflict of Interest in Clinical Research:Conflict of Interest in Clinical Research:Research Agreements between AMCs and Research Agreements between AMCs and IndustryIndustry
——Schulman KA, et al. NEJM 2002;347:1335Schulman KA, et al. NEJM 2002;347:1335

Impugning the Integrity of Medical ScienceImpugning the Integrity of Medical ScienceThe Adverse Effects of Industry InfluenceThe Adverse Effects of Industry InfluenceCatherine D. DeAngelis, MD, MPHCatherine D. DeAngelis, MD, MPHPhil B. Fontanarosa, MD, MBAPhil B. Fontanarosa, MD, MBA
JAMA, April 16, 2008—Vol 299, No. 15JAMA, April 16, 2008—Vol 299, No. 15

Consistency of Conflict of Interest Reporting
• Searched PubMed for English-language articles published in 2006 that provided evidence or guidance regarding the use of coronary artery stents
• Resulting database of 746 articles, 2985 authors, and 135 journals
• Recorded article characteristics, including information about authors’ financial disclosures
• Main outcome measures were the prevalence, nature, and consistency of financial disclosures
» Weinfurt KP; PLOS 1, May 7th, 2008

COI Disclosure in Stent TrialsWeinfurt KP; PLOS 1, May 7th, 2008

Comparisons Between Disclosures in Articles by the Same Author (N = 5573)
0
10
20
30
40
50
60
70
80
90
100
Absent-absent Present-present None declared-nonedeclared
Absent-none declared Present-absent Present-none-declared
Result of Comparison Between Articles
Per
cent
age
Agreement Disagreement

Interpretation
• In rare instances when financial interests were disclosed, they were not disclosed consistently, suggesting problems with transparency in the literature
• An inconsistent system of disclosure may be more harmful than no disclosure at all, because it creates the impression rather than the reality of transparency
• The relative contributions of journals and authors to this problem are unclear

Trial Organizational StructureTrial Organizational Structure
SponsorSponsorSponsorSponsorSteering CommitteeSteering CommitteeChairmen + NCs + RDs + Chairmen + NCs + RDs + experts in clinical studiesexperts in clinical studies
Steering CommitteeSteering CommitteeChairmen + NCs + RDs + Chairmen + NCs + RDs + experts in clinical studiesexperts in clinical studies
Executive Executive CenterCenter
Study ChairStudy Chair
Executive Executive CenterCenter
Study ChairStudy Chair
Coordinating Coordinating CenterCenter
Study Co-ChairStudy Co-Chair
Coordinating Coordinating CenterCenter
Study Co-ChairStudy Co-Chair
International International Data CentersData Centers
International Co-International Co-ChairChair
International International Data CentersData Centers
International Co-International Co-ChairChair
Events Review Events Review CommitteeCommittee
Events Review Events Review CommitteeCommittee
DSMBDSMBDSMBDSMB

Key Issues—Big Ticket ItemsKey Issues—Big Ticket Items
Tradeoff of Generalizability and ValidityTradeoff of Generalizability and Validity
Biological issuesBiological issues
Culture and practiceCulture and practice
Target vs DrugTarget vs Drug
Superiority/NoninferioritySuperiority/Noninferiority
Clinically important differencesClinically important differences
Trial conductTrial conduct
Sensible or nonsensical?Sensible or nonsensical?
Regulatory dysharmonyRegulatory dysharmony

Important DetailsImportant Details Enrollment criteriaEnrollment criteria
Concomitant therapyConcomitant therapyComparatorComparator
Other therapyOther therapy
Diabetes Diabetes
CV diseaseCV disease
““Diabetology” issuesDiabetology” issues““glycemic equipoise”glycemic equipoise”
DurabilityDurability
EndpointsEndpointsDefinitionsDefinitions
AdjudicationAdjudication

GeneralizabilitGeneralizabilityy
ValidityValidity
GoalGoal
XX

The pragmatic trial is really a way The pragmatic trial is really a way of finding the best compromise of finding the best compromise between validity and between validity and generalizabilitygeneralizability

Diabetes CV Outcome TrialsDiabetes CV Outcome Trials
Focused on Focused on GeneralizabilityGeneralizability
Broad entry criteriaBroad entry criteria
Broad allowance for Broad allowance for concomitant therapyconcomitant therapy
Embrace “standards of Embrace “standards of care” but avoid detailed care” but avoid detailed proscriptive protocolsproscriptive protocols
Focused on ValidityFocused on Validity
Specific entry criteria Specific entry criteria carefully measured well carefully measured well beyond what is done in beyond what is done in practicepractice
Additional therapies Additional therapies determined by protocoldetermined by protocol
Detailed protocol for Detailed protocol for clinical careclinical care

Common GroundCommon Ground
Proper consent and randomizationProper consent and randomization
Measurement of adherence/persistence to Measurement of adherence/persistence to randomized txrandomized tx
Measurement of endpoints in unbiased mannerMeasurement of endpoints in unbiased manner
What amazes me is how often industry SOP’s What amazes me is how often industry SOP’s and FDA inspectors fail to distinguish what is and FDA inspectors fail to distinguish what is important from what is fundamentally irrelevant important from what is fundamentally irrelevant to answering the question posed by the trial!to answering the question posed by the trial!

Target vs DrugTarget vs Drug
Assessing DrugAssessing Drug
Hold background Hold background constantconstant
Isolate on effects of Isolate on effects of drugdrug
CANNOT RELIABLY CANNOT RELIABLY USE SLOPE OF USE SLOPE OF TARGET/OUTCOME TARGET/OUTCOME TO ASSESS VALUE OF TO ASSESS VALUE OF TARGETTARGET
Assessing TargetAssessing Target
Achieving target is the Achieving target is the goal regardless of tx goal regardless of tx used to get thereused to get there
Understood that Understood that background tx will varybackground tx will vary
Cannot tease out Cannot tease out individual effects of individual effects of drugsdrugs

Inescapable FactInescapable Fact
We need both types of trials:We need both types of trials:
Drug trials to assess the specific balance of benefit Drug trials to assess the specific balance of benefit of risk of individual drugsof risk of individual drugs
Therapeutic target trials to understand whether in Therapeutic target trials to understand whether in general it is beneficial to drive a biomarker to a general it is beneficial to drive a biomarker to a targettarget
In the end we will always be left with some In the end we will always be left with some uncertainty about this mixuncertainty about this mix

Fundamental Trial Fundamental Trial Construct—Superiority/NoninferiorityConstruct—Superiority/Noninferiority
SuperioritySuperiority
Easy to understandEasy to understand
““Hard to imagine” that a Hard to imagine” that a tx that lowers sugar tx that lowers sugar shouldn’t reduce shouldn’t reduce macrovascular dzmacrovascular dz
Tough hurdle in Tough hurdle in comparative trialscomparative trials
NoninferiorityNoninferiority
No one can explain to No one can explain to practitionerspractitioners
Neutrality on Neutrality on macrovascular disease macrovascular disease should be sufficient if should be sufficient if glycemic effect is glycemic effect is known to be beneficialknown to be beneficial

Superiority/NoninferioritySuperiority/Noninferiority
Really a false argument—the real question is:Really a false argument—the real question is:
What is the estimated effect of the tx on the net What is the estimated effect of the tx on the net balance of risk and benefit?balance of risk and benefit?
A trial can test for both noninferiority and superiority A trial can test for both noninferiority and superiority without penalty if the trial is set up properlywithout penalty if the trial is set up properly
The real question is: The real question is:
What is the minimally important clinical difference What is the minimally important clinical difference that should be excluded in noninferiority trials and that should be excluded in noninferiority trials and exceeded in superiority trials? exceeded in superiority trials?

Minimally Important DifferenceMinimally Important Difference
Typically 10-15% relative difference or 1% Typically 10-15% relative difference or 1% absolute difference per year in ASCVD absolute difference per year in ASCVD outcomesoutcomes
Key factorsKey factors
Underlying risk (> absolute risk makes smaller Underlying risk (> absolute risk makes smaller relative difference worthwhile)relative difference worthwhile)
Cost and logistic feasibility of interventionCost and logistic feasibility of intervention
Size of population affectedSize of population affected
A treatment taken by 5 million people with 1% A treatment taken by 5 million people with 1% excess mortality per year would kill 50,000 people excess mortality per year would kill 50,000 people per yearper year

What is a Meaningful Difference in CV EndpointsWhat is a Meaningful Difference in CV Endpoints
““A difference to be a A difference to be a difference must make a difference must make a difference”difference”
? Gertrude Stein? Gertrude Stein

Sensible or Nonsensical Clinical TrialsSensible or Nonsensical Clinical Trials
Goals of medical intervention:Goals of medical intervention:
Live longer, feel better, avoid unpleasant events and Live longer, feel better, avoid unpleasant events and spend less moneyspend less money
Balance of risk and benefitBalance of risk and benefit
Surrogates can work for “on target” and “off target” Surrogates can work for “on target” and “off target” effects separately effects separately
Off target effects are ubiquitousOff target effects are ubiquitous


Clinical Trial Cost EstimatesClinical Trial Cost Estimates
$0
$50
$100
$150
$200
$250
$300
$350
$400
$450
T o tal
Co o rd in atin g Cen ter
S ite Paym en ts
Oth er
Full Cost Industry
Streamlined Industry
More Streamlined
$ In US 2007 Millions

Defining Quality in Clinical Trials
Janet Woodcock M.D.Deputy Commissioner/Chief
Medical Officer, FDAMay 10, 2007

Defining Quality
Contemporary definition: meets customer needs
Restatement: “Fitness for use” Use: customers rely on the data to make
decisionsFDA: Regulatory decisionsSponsors: Claims about productPhysicians and patients: treatment
choices IOM Workshop definition of data quality: data
good enough that decision would not change if completely accurate data used

Regulatory DysharmonyRegulatory Dysharmony
Which makes more sense?Which makes more sense?
Conducting a separate trial in every countryConducting a separate trial in every country
Conducting global trials Conducting global trials
How can we do what makes sense if regulatory How can we do what makes sense if regulatory requirements are different in every country?requirements are different in every country?
There is a perception that this problem has There is a perception that this problem has worsened in the past few yearsworsened in the past few years

Study Undertaken by FDA Study Undertaken by FDA statisticians to evaluate statisticians to evaluate possibility of systematic possibility of systematic
regional differencesregional differences Major cardiovascular outcome Major cardiovascular outcome
studies evaluated over the last 10 studies evaluated over the last 10 yearsyears
Overall study result statistically Overall study result statistically positive, ie. demonstrated overall positive, ie. demonstrated overall effecteffect
Region never pre-specified as a Region never pre-specified as a factor to be evaluated statisticallyfactor to be evaluated statistically
16 independent studies16 independent studies

difference of log-hazard ratios
Study % US
-1.5 -1.0 -0.5 0.0 0.5 1.0 1.5
311
452
273
94
45
196
437
388
49
7410
7411
912
313
2914
1715
9016
Estimates and confidence intervals for difference between US and Non-US treatment effects for each
study
J. Lawrence
In 13 of 16 , US log hazard above 0


A figure
From the label

The Consequences of Regulatory DysharmonyThe Consequences of Regulatory Dysharmony
Given differences of opinions by regulators in Given differences of opinions by regulators in different countries the sponsor must either different countries the sponsor must either reduce countries or revert to the most reduce countries or revert to the most expensive common denominatorexpensive common denominator
This leads to a vicious cycleThis leads to a vicious cycle
If the trials are too expensive we can’t do them, If the trials are too expensive we can’t do them, therefore we’ll just have to accept or ignore therefore we’ll just have to accept or ignore uncertainty in order to enable development of uncertainty in order to enable development of new drugsnew drugs
We need a virtuous cycle of developing We need a virtuous cycle of developing common methods to reduce uncertaintycommon methods to reduce uncertainty

Enrollment CriteriaEnrollment Criteria
History of ASCVD present or absentHistory of ASCVD present or absent
ComorbiditiesComorbidities
Severity of diabetesSeverity of diabetes
On label/off labelOn label/off label

Enrollment CriteriaEnrollment Criteria
Early in disease phase Early in disease phase
More chance to “modify More chance to “modify disease”disease”
Low event rates in this Low event rates in this population (DREAM < population (DREAM < 1% /yr; NAVIGATOR 1% /yr; NAVIGATOR below expectations)below expectations)
Later in disease phaseLater in disease phase
Many more events Many more events allows shorter or allows shorter or smaller trialssmaller trials
Risk that “the horse is Risk that “the horse is out of the barn so there out of the barn so there will be no effect”will be no effect”

Concommitant TherapyConcommitant Therapy --Diabetes--Diabetes
Placebo or direct comparative trialsPlacebo or direct comparative trials
Currently no proven winnerCurrently no proven winner
Active add on vs placebo add on will be a Active add on vs placebo add on will be a viable approach for some time to comeviable approach for some time to come
As winners emerge, active control and As winners emerge, active control and combination trials will be necessarycombination trials will be necessary

Concomitant Therapy—CV RiskConcomitant Therapy—CV Risk
Risk factor controlRisk factor control
BP, lipids, smoking, exerciseBP, lipids, smoking, exercise
Secondary preventionSecondary prevention
Anitplatelet, antithrombotic, revascularizationAnitplatelet, antithrombotic, revascularization
OptionsOptions
Mandate—expensive Mandate—expensive
Recommend local guideline based careRecommend local guideline based care

On Label/Off label conundrumOn Label/Off label conundrum
Diabetes drugs are typically developed in Diabetes drugs are typically developed in narrow populations and then used broadlynarrow populations and then used broadly
If pragmatic outcome trials are limited to “on If pragmatic outcome trials are limited to “on label” use, they will not reflect actual use of the label” use, they will not reflect actual use of the drugdrug
Nor will they capture the nexus of most benefit and Nor will they capture the nexus of most benefit and harm in CV disease (the high risk population)harm in CV disease (the high risk population)
Key issues: renal dysfunction, multiple Key issues: renal dysfunction, multiple comorbidities, esp. in the elderlycomorbidities, esp. in the elderly

Glycemic EquipoiseGlycemic Equipoise
Adding a new therapy will create a difference in Adding a new therapy will create a difference in glycemia on Day 1 of the trialglycemia on Day 1 of the trial
If the goal is to examine the “non-glycemic” If the goal is to examine the “non-glycemic” benefit or harm of the treatment, the goal benefit or harm of the treatment, the goal should be to close this gap as quickly as should be to close this gap as quickly as possiblepossible
““Intensifying” the comparator brings into play Intensifying” the comparator brings into play the beneficial or detrimental effects of multiple the beneficial or detrimental effects of multiple drugsdrugs

DurabilityDurability
Many doctors want to know whether the Many doctors want to know whether the glycemic effect of the drug is a fundamental glycemic effect of the drug is a fundamental biological modification or just a suppression of biological modification or just a suppression of glucose that lasts while the drug is on boardglucose that lasts while the drug is on board
Evaluating this requires stopping the active Evaluating this requires stopping the active treatment and measuring glycemic statustreatment and measuring glycemic status

OutcomesOutcomes
““Hard” CV eventsHard” CV events
““Soft CV events”Soft CV events”
Adverse eventsAdverse events
Quality of lifeQuality of life
EconomicsEconomics

Hard EventsHard Events Death, myocardial infarction, strokeDeath, myocardial infarction, stroke
Discrete, measurable events with unarguable impact on Discrete, measurable events with unarguable impact on duration and quality of lifeduration and quality of life
DeathDeath
All cause vs CV All cause vs CV
Myocardial infarctionMyocardial infarction
As ability to measure improves many more MI cases As ability to measure improves many more MI cases relative to unstable anginarelative to unstable angina
Symptomatic vs silentSymptomatic vs silent
StrokeStroke
All cause vs ischemicAll cause vs ischemic
Imaging vs clinically evidentImaging vs clinically evident

““Soft Events”Soft Events” ACS without myocardial necrosis (unstable ACS without myocardial necrosis (unstable
angina)angina)
Diagnosis complex and difficult to verifyDiagnosis complex and difficult to verify
Majority of chest pain ED visits not UAPMajority of chest pain ED visits not UAP
RevascularizationRevascularization
Very dependent upon cultural context Very dependent upon cultural context
In a blinded trial, unbiasedIn a blinded trial, unbiased
Heart failure admissionHeart failure admission
Half way between hard and softHalf way between hard and soft

Adverse EventsAdverse Events Important events of interestImportant events of interest
Open ended adverse events will miss a large Open ended adverse events will miss a large proportion of eventsproportion of events
““Tickbox” clearly the way to goTickbox” clearly the way to go
SAE’sSAE’s
Must collect because of ubiquitous off target effects Must collect because of ubiquitous off target effects (fractures with TZDs)(fractures with TZDs)
Non-serious AEsNon-serious AEs
Focused collection via tickboxFocused collection via tickbox
Please forget open ended non-serious AE collection Please forget open ended non-serious AE collection at this point!!!at this point!!!

Cost Effectiveness:Cost Effectiveness:Conceptual GoalConceptual Goal
Year of LifeYear of Life $50-$50-100,000100,000

The Cycle of Quality: Generating Evidence to The Cycle of Quality: Generating Evidence to Inform PolicyInform Policy
Califf RM et al, Califf RM et al, Health Affairs, 2007Health Affairs, 2007
Measurement Measurement andand
EducationEducation
Measurement Measurement andand
EducationEducation
Early Translational
Steps
Early Translational
Steps
ClinicalTrials
ClinicalTrials
ClinicalPractice
Guidelines
ClinicalPractice
Guidelines
PerformanceMeasures
PerformanceMeasures
OutcomesOutcomes
Discovery ScienceDiscovery Science
DataDataStandardsStandards
DataDataStandardsStandards
NetworkNetworkInformationInformation
NetworkNetworkInformationInformation
EmpiricalEmpiricalEthicsEthics
EmpiricalEmpiricalEthicsEthics
PrioritiesPrioritiesand Processesand Processes
PrioritiesPrioritiesand Processesand Processes
InclusivenessInclusivenessInclusivenessInclusiveness
Use forUse forFeedbackFeedback
on Prioritieson Priorities
Use forUse forFeedbackFeedback
on Prioritieson Priorities
Conflict-of-interestConflict-of-interestManagementManagement
Conflict-of-interestConflict-of-interestManagementManagement
Evaluation of SpeedEvaluation of Speedand Fluencyand Fluency
Evaluation of SpeedEvaluation of Speedand Fluencyand Fluency
Pay forPay forPerformancePerformance
Pay forPay forPerformancePerformance
TransparencyTransparencyto Consumersto ConsumersTransparencyTransparencyto Consumersto Consumers
FDAFDACritical PathCritical Path
FDAFDACritical PathCritical Path
NIH RoadmapNIH RoadmapNIH RoadmapNIH Roadmap12 3
4
5
6
7
8
910
11
12

The Key in ACS is doing the right trialsThe Key in ACS is doing the right trials Reduction in deaths:Reduction in deaths:
TherapyTherapy # pts# pts RelativeRelative AbsoluteAbsolute C/EC/E
MI:MI: AspirinAspirin 18,77318,773 23%23% 2.4%2.4% ++++++++++
FibrinolyticsFibrinolytics 58,00058,000 18%18% 1.8%1.8% ++++++++
Beta blockerBeta blocker 28,97028,970 13%13% 1.3%1.3% ++++++++
ACE inhibitorACE inhibitor 101,000101,000 6.5%6.5% .6%.6% ++
2nd prev: Aspirin 54,360 15% 1.2% +++++
Beta blocker 20,312 21% 2.1% ++++
StatinsStatins 17,61717,617 23%23% 2.7%2.7% ++++++++
ACE inhibitor 9,297 17% 1.9% ++++
CHF: ACE inhibitor 7,105 23% 6.1% +++++
Beta blocker 12,385 26% 4% +++++
SpironolactoneSpironolactone 1,6631,663 30%30% 11%11% ++++++++++

Given the Right Trials, Adherence Matters!Given the Right Trials, Adherence Matters!Improve Adherence to ACC/AHA Guidelines for Improve Adherence to ACC/AHA Guidelines for Patients with Unstable Angina/Non-STEMIPatients with Unstable Angina/Non-STEMI
Acute TherapiesAcute Therapies
AspirinAspirin
ClopidogrelClopidogrel
Beta BlockerBeta Blocker
Heparin (UFH or LMWH)Heparin (UFH or LMWH)
Early CathEarly Cath
GP IIb-IIIa InhibitorGP IIb-IIIa Inhibitor
All receiving cath/PCIAll receiving cath/PCI
Discharge TherapiesDischarge Therapies
AspirinAspirin
ClopidogrelClopidogrel
Beta BlockerBeta Blocker
ACE Inhibitor ACE Inhibitor
Statin/Lipid LoweringStatin/Lipid Lowering
Smoking CessationSmoking Cessation
Cardiac RehabilitationCardiac Rehabilitation
Circulation, JACC 2002 — ACC/AHA Guidelines updateCirculation, JACC 2002 — ACC/AHA Guidelines update
Evaluating the Process of CareEvaluating the Process of Care
An adherence score is applied to each patient. An adherence score is applied to each patient. incorporating the components of process of care.incorporating the components of process of care.
The score from each patient then combined for all The score from each patient then combined for all patients at each hospital. patients at each hospital. Typical scores ranged from 50 to 95%.Typical scores ranged from 50 to 95%.
All 400 hospital adherence scores then ranked in All 400 hospital adherence scores then ranked in quartiles — best to worst.quartiles — best to worst.
Evaluating the Process of CareEvaluating the Process of Care
An adherence score is applied to each patient. An adherence score is applied to each patient. incorporating the components of process of care.incorporating the components of process of care.
The score from each patient then combined for all The score from each patient then combined for all patients at each hospital. patients at each hospital. Typical scores ranged from 50 to 95%.Typical scores ranged from 50 to 95%.
All 400 hospital adherence scores then ranked in All 400 hospital adherence scores then ranked in quartiles — best to worst.quartiles — best to worst.

Overall Adherence Score Trends Over TimeOverall Adherence Score Trends Over Time
68.1%69.6%
71.0%72.3%
73.0% 73.6%75.2%
77.9% 78.0%79.3%
60%
70%
80%
Q1'02
Q4'02
Q3'03
Q2'04

Peterson et al, ACC 2004Peterson et al, ACC 2004
Applying High Quality Evidence Improves Applying High Quality Evidence Improves OutcomesOutcomes
0
2
4
6
8
<=25% 25–50% 50–75% >=75%
Hospital Composite Quality Quartiles
% In
-ho
spit
al M
ort
alit
y Adjusted Unadjusted
Every 10% in guidelines adherence 11% in mortality

The Cycle of QualityThe Cycle of Quality
We should be able to do this in diabetesWe should be able to do this in diabetes
The key is high quality pragmatic trials that The key is high quality pragmatic trials that measure the balance of benefit and risk!measure the balance of benefit and risk!

Alternatives to EBMAlternatives to EBM
Eminence-based medicineEminence-based medicine
Confidence-based medicineConfidence-based medicine
Eloquence-based medicineEloquence-based medicine
Vehemence-based medicineVehemence-based medicine
Providence-based medicineProvidence-based medicine
Diffidence-based medicineDiffidence-based medicine
Nervousness-based medicineNervousness-based medicine
Isaacs D, Fitzgerald D. Br Med J 1999;319:1618.


All others must have All others must have data!data!
“and when you get “and when you get the data you find its the data you find its not as simple as what not as simple as what you believed when you believed when you had no data”you had no data”H Gerstein 2008H Gerstein 2008