Embed Size (px)
Citation preview

Cardiovascular Diseases in Greece*
CHRIST ARAVANIS, M.D. and GEORGE MICHAELIDES, M.D.
Athens, Greece
D URING the past few years, pilot studies have been initiated in various countries all over
the world in order to discover if there is any con- nection between the way of life and heart diseases. We already have evidence that the incidence of coronary, arteriosclerotic and rheumatic heart diseases varies in different countries. The part played by climate, diet, work and the stress of modern life has to be further elucidated through intensive and well- organized, comparative investigations.
The present study includes an analysis of the files of 17,084 patients of a general hospital in Athens within the past 12 years. The results concerning coronary, hypertensive, rheumatic and rarer heart diseases are presented.
MATERIAL
This study was done in the Department of Cardi- ology of the University of Athens Medical School at the Hippokrates Hospital, a 700 bed charity hospital, which has one of the largest outpatient clinics for cardiac patients, and a cardiac ward. This hospital accepts patients of the low and middle classes from all over the country, the majority being poor farmers, peasants and manual workers.
The material presented here consisted of patients of the outpatient clinic and of ward patients.
The outpatient clinic material covers the period 1948 to 1960. (Records prior to 1948 were not con- sidered reliable for evaluation.) The inpatient ma- terial covers the period from 1954, when the cardiac ward was established, through 1960. Patients from the city of Athens were evaluated separately from those of the rest of the country, which was divided into seven areas having similar climatic and socio- economic conditions.
Of the 17,084 patients examined in the Depart- ment of Cardiology during these periods, 2,317 had coronary heart disease; 2,741 had hypertensive heart disease ; 2,420 had rheumatic heart disease; 516 had rare heart diseases, and 9,090 suffered from neurocirculatory asthenia or had a normal heart (Table I). During the period 1948 to 1960, 14,716 patients were examined in the cardiac clinic, 9,516 (65.70/,) from the country and 5,140 (34.3%) from
the city of Athens. During the period 1954 to 1960, 2,368 patients were treated in the cardiac wards, 588 (20.37,) from Athens and 1,780 (79.70/(,) from the country.
CORONARY HEART DISEASE
Morbidity and mortality from coronary heart disease is known to vary in different countries.1-4 In the United States and other Western countries, coronary heart disease is the leading cause of death and has increased in the last years,5 as confirmed by epidemiologic studies.6-8 In Greece, similar studies were started in 1957 under the direction of Ancel Keys of the University of Minnesota, as part of an international study of coronary heart disease. The data collected so fal support the o/&ion that coronary heart disease is rare in the rural areas of this country. Other comparable statistics are not available in Greece, but the general opinion is that, although coronary heart disease has in- creased in the last years, it still is rare, particu- larly in the rural areas. This seems due to differences in diet, daily life and habits.
The present study was undertaken with the hope that interesting data could be drawn from the clinical material of a general hospital.
The diagnosis of coronary heart disease was established according to the classification of the New York Heart Association.g The diagnosis was based on data from the history, physical examination, electrocardiogram, x-ray examina- tion and other laboratory tests.
Incidence of Coronary Heart Disease: Among the clinic patients, 1,537 (10.57,) were found to suffer from coronary heart disease (Table II). Among the hospitalized patients, 780 (32.7y0) were found to have coronary heart disease. The sex and geographic distribution are shown in Table II. In the same periods 92,000 pa- tients were examined in the outpatient clinic and 20,000 entered the medical wards, while 404,976 patients were examined in all clinics of the hospital, and 45,000 entered the various wards.
* Prom the Department of Cardiology of the University of Athens Medical School at the Hippokratrs Hospital.
SEPTEMBER 1962 349

350 _kavanis and Michaelides
‘rABLK I Distribution of ‘Total Number of Inpatients and Outpatients According to Heart Disease
Clinic
Hospital
Total No. Examined
Patients
14,716
2,368
Coronary Heart
Disease
1,537 (lO.Sc:I,)
780 (32.3’/; )
Hypertensive Heart
Disease
2,511 (16.7(/;)
230 (9.9Yi )
Khuematic Heart
Disease
1,536 (10.55;))
884 (37.9’;il,)
Rare Heart Diseases
162 (1.1 %I)
354 (14.9%)
Neuro- circulatory Asthenia or
Normal
8,970 (61.2%)
120 (5.4Yi,)
TABLE II
Distribution of Coronary Heart Disease Patients i\ccording to Sex and Origin
Total No. No. of Coronary Examined Heart Disease
Patients Patients Men Women Athens Country
Clinic
Hospital
14,716 1,537 957 580 521 1,016 (10.59;) (62.3:‘;9) (37.77;) (33.8%) (66.2%)
2,368 780 491 289 268 512 (32.7’:,;,) (62.9:&) (37.1 y;) (34.3%) (65.7:;)
TABLE III
Distribution of Clinical Material of the Entk- Hospital from 1948-l 960
Total No. Coronary Patients Medical Cardiac Heart
from Cases Cases Discase 1948-1960 (No.) (No.) (No.)
Clinic 404,976 92.000 14,716 1,537
Hospital 45,320 20 ~ 000 2,368 780
The ratio of coronary heart disease patients to the total number of cardiac patients was 13.4 per cent; to the total number of medical cases was 2.1 per cent: and to the total number of patients admitted to the hospital was 0.55 per cent (Table III). Of the total number of patients with coronary heart disease 1,448 (67.2%) were men and 869 (32.8yfi) women.
The number of patients examined in the d@erent years is shown in Table IV. The increased but fluctuating number of patients from year to year probably does not reflect a real increase in the incidence of coronary heart disease but rather the trend toward increase in the number of patients coming for examination. The same was also true for the hospitalized patients.
The peak a,ge incidence of coronary heart disease
was between 51 and 60 years of life (Table v). About two thirds of all cases were between 51 and 70 years, and only 2.3 per cent were below the age of 40 in the outpatient clinic and 0.8 per cent among the hospital patients. No case was found below the age of 31.
i\mong the clinic patients, 200 (2.3%) were found to have a myocardial infarction and 373 (4.1%) were suffering from angina pectoris. Among the hospitalized, 235 (9.9y0) had an infarction and 122 (5.1%) presented angina. The ratio of myocardial infarction to all cardiac cases was 2.5 per cent; to the total number of medical cases, 0.39 per cent; and to the total number of cases examined and admitted to the hospital, 0.10 per cent. The ratio of angina pectoris to all cardiac cases was 4.5 per cent; to the total number of medical cases, 0.44 per cent; and to the total number of hospital pa- tients, 0.11 per cent. The electrocardiographic findings of the coronary heart disease patients are shown in Table VI.
The ooer-all mortality for the patients treated in the hospital was 7.8 per cent.
Geographic Di#erences: For a more detailed epidemiologic study, Greece was divided in seven large areas with similar climatic and socioeconomic conditions. The city of Athens and its suburbs with a population of 1,300,OOO
THE AMERICAN JOURNAL OF CARDIOLOGY

Cardiovascular Diseases in Greece 351
TABLE IV
Distribution of Patients According to Year
1948 1949 1950 1952 1953 1954 1955 1956 1957 1958 1959 1960
Clinic 18 85 57 115 160 180 140 200 210 140 192 42
Hospital . 74 108 77 73 192 189 67
TABLE v
Age Distribution of 2,317 Cases of Coronary Heart Disease
Age 31-40 41-50 51-60 61-70 71-80 81-90 91-100
Clinic (2.?%) 238 528 493 216 (15.5%) (34.3%) (32.0%) (14.0%) (l.?%) (O.&)
Hospital 6 (0.77%) (lO?%)
211 319 147 (27.0%) (40.9%) (18.5%) (Z% ...
TABLE VI
Electrocardiographic Data of Coronary Heart Disease Patients
Infarction Angina Pectoris
Ischemia, or Left
Ventricular Left Bundle Right Bundle A-V Atria1 Hypertrophy Branch Block Branch Block Block Fibrillation
Clinic 200 373 638 (13.1%) (24.3%) (41.3%) (3.?%) (4.?%) (0.7%)
177 (11.5’;;,)
Hospital 235 122 320 (30.1%) (15.6%) (41.3%) (0.65%) (l.l4l%)
was considered separately in order to find possi- ence. In the last group the mean serum choles- ble differences between city and country areas. terol value was 209 mg.
The incidence of coronary heart disease in some of these areas was found considerably lower than in others. This may not reflect the actual situation and may be due to the fact that patients from the three more remote areas of the country are less likely to travel to Athens for an examination, unless they are complex cases. The ratio of coronary heart disease in the city of Athens to its population was 0.06 per cent; it was 0.02 per cent in the rest of the country. However, if we exclude the three northern re- mote areas, the other areas have a ratio of 0.03 per cent.
HYPERTENSIVE HEART DISEASE
Total serum cholesterol was measured in 48 per cent of patients with coronary heart disease attending the outpatient clinic, and the mean value was 246 mg. In the ward patients with coronary heart disease, the mean value was 253 mg. A comparison with a control group of patients suffering from other heart diseases or medical illnesses showed a considerable differ-
The pathogenesis of hypertension is still un- certain, and further experimental, clinical and epidemiologic work remains to be done be- fore final conclusions are reached. Useful in- formation has been obtained in recent years from studies in different ethnic groups concern- ing factors affecting blood pressure. From these studies it appears that in some racial groups, like Chinese, African Negroes, Mexican Indians and Filipinos, hypertension is uncom- mon . It also appears that hypertension is more common in the males until the fifth decade of life, and becomes thereafter more prevalent in females. Although heredity plays an im- portant role, how socioeconomic factors such as diet, work and tempo of life influence blood pressure remains to be clarified, largely through epidemiologic studies.8J0-17
In evaluating blood pressure, technical prob-
SEPTEMBER 1962

352 Aravanis and Michaelides
7i-ABLE “II
Distribution of Patients with Hypertensive Heart Disease According to Sex and Origin
Total No. Examined Total No.
Patients Nypertensives Men Women Athens Country ______
Clinic 14,716 2.511 930 1,581 983 1,528 (16.7’;; 1 (37.O’,i ) (63.07;) (39.1 ‘;,, (60.9’); )
Hospital 2.368 230 67 163 161 (9.7’;;,) (29.1:;,) (70.9’&) ( 30!&;, ) (70.04; 1
TABLF. “11,
Age Distribution of 2,741 Hypertensiw Patients
Age 1 l-20 21-30 31-40 41-50 51-60 61-70 7 l-80 81-90 91-100
Clinic 4 (& 130 503 897 667 246 16 2 (0.14’:;,) is.1 c/; ) (2o.o’i;f) (35.6’,;) (27.1%,, (9.8%) (O.G’,‘,,,) (.06’,;,)
Hospital (I.&) (4.;; )
OY& ( 1 )
(42?;<,) 60 (26.17;) (13:;:; ) &)
TABLE IX
Distribution of Hypertensive Patients by Age and the Ratio to Other Forms of Organic Heart Disease
Age 11-20 21-30 31-40 41-50 51-60 61-70 71-80 81-90 91-100 _ -____
Hypertensives 4 48 140 527 995 727 278 18 2
Total No. of Cardiacs 723 1.570 1,411 1.544 1,101 631 228
(0.55;,1 (3.0:;) (9.97;;) (34.O!‘i) (81.0’:;.) (llS’,&) (122’;;) (782;;)
lems must be taken into consideration because various circumstances may change blood pres- sure during the examination.‘*-20 Since a dividing line cannot be drawn between hyper- and normotensive patients in the present study, every patient presenting a stable blood pressure above 145/90 mm. Hg was considered hyper- tensive. The level of diastolic blood pressure was considered more important since it is known that there is a tendency for increase of the systolic pressure with age. In a number of patients, examination of the fundus was done, particularly in those with high diastolic blood pressure. Papilledema, exudates and hemor- rhages were considered characteristic signs of malignant hypertension.
were men and 163 (70.0”j0) were women. The male-to-female ratio was about 1 : 2, and this proportion in favor of women increased after the age of 50, while below such age the ratio was about 1 : 1.
From the total number of clinic patients, 983 (39.1%) were from the city of Athens, and 1,528 (60.9%) from the rural areas. The percentage of hypertensive patients in the total population was 0.09 per cent in Athens, and 0.02 per cent in the rural areas. However, if the three most remote areas are excluded, the percentage for the rural areas increases to 0.03 per cent. The area with the highest percentage of hypertensives was that comprising the islands, with an average of 0.04 per cent.
Incidence: During the period 1948 to 1960, The dzstribution qf hypertensiue patients according
2,511 hypertensive patients were examined in to d$erent ages is shown in Table VIII. From the cardiac clinic, and 230 were admitted to the total number, 35.6 per cent were between the cardiac wards (Table VII). Of clinic pa- 51 and 60 years, 20 per cent between 41 and 50 tients, 930 (3770) were men and 1,581 (6370) years and 27.1 per cent between 61 and 70 were women; of the ward patients 67 (29.1’%) years. Below the age of 40 and above the age
THE AMERICAN JOURNAL OF CARDIOLOGY

Cardiovascular Diseases in Greece 353
TABLE x
Distribution of Inpatients and Outpatients with Hypertension from 1948 to 1960
Year 1948 1949 1950 1951 1952 1953 1954 1955 1956 1957 1958 1959 1960
Clinic 28 286 229 40 222 219 313 261 280 339 133 97 64
Hospital 19 25 19 37 66 44 20
TABLE XI
Electrocardiographic Data of Hypertensive Patients
Right Left L& Left Ventricular Bundle Bundle
Angina Myocardial Ventricular Hypertrophy Branch Branch A-V Auricular Pectoris Infarction Hypertrophy & Ischemia Block Block Block Fibrillation
Clinic 172 (2.& 497 401 (6.89;)) (19.Ooi;) (15.9%) (I.&) (l.& (0.132~~)
120 (4.8%)
Hospital (6.;;; ) (2.25%)
156 (72.2’j/,) (3.&G) (O&)
TABLE XII TABLE XIII
Comparative Incidence of Myocardial Infarction and Distribution of Benign and Malignant Cases of Hypcr- Angina PFctoris in Hypertensive Patients and Those tension and Their Percentage of Mortality
with Coronary Heart Disease
Hypertensive Coronary Heart Disease Heart Disease
Myocardial Angina Myocardial Angina Infarction Pectoris Infarction Pectoris
(%)
Clinic 2.2
Hospital 2.8
(%) (%) (%)
6.9 13.1 24.3
6.9 30.1 15.6
Benign Malignant Total No. Hyper- Hyper- Hyper- tension tension Died tensives
____ Clinic 2,475 36 ? 2,511
(98.2’&) (1.8’;;) ( 100 :‘b )
Hospital 224 6 9 230 (97.4’/,;) (2.67;) (3.97;) (loot;;.)
of 70, the incidence of hypertension drops significantly. Only 4 cases with high blood pressure were found between 11 and 20, and 2 between 91 and 100 years. The percentage of hypertensive patients by age in relation to the total number of all cardiac patients is shown in Table IX.
per cent of all cases with hypertension after excluding the cases with evidence of associated coronary heart disease. The mean value was 223 mg. This is in agreement with other authors who found increased amounts vf serum cholesterol in the blood of hypertensive patients.
Forty-two cases (2.2%) had malignant hyper- tension (Table XIII).
There is a fluctuation in the number of ex- amined patients from year to year due to un- determined reasons, as shown in Table x. The incidence of associated myocardial infarction and angina pectoris, as well as other electro- cardiographic abnormalities, is shown in Table XI. Of all hypertensive patients, 2.6 per cent had an infarction, and 6.9 per cent presented angina pectoris. A comparison of the incidence of myocardial infarction and angina pectoris in the coronary and hypertensive patients is shown in Table XII.
The over-all mortality of hypertensive patients treated in the hospital was 3.9 per cent. This was mainly due to cerebrovascular accidents and seldom to heart failure.
RHEUMATIC HEART DISEASES
Ttle total serum cholesterol was measured in 30
Rheumatic heart disease is the second great cause of cardiac disability today. The patho- genesis of rheumatic fever which is responsible for the rheumatic heart disease is obscure, al- though considerable knowledge has been gained in the last few years. Its relationship to strep- tococcal infection is well known. It is found
SEPTEMBER 1962
354 Aravanis and Michaelides
‘,-ABLE XI”
Distribution of Cases of Rhrumatic Hrart Disrasr According to Sex and Origin
Total No. Rhrumatic Ht.art Examined Disease
Patients (No.) Mrn \Vomcn Athrns Country Deaths -~~
Clinic 14.716 1.536 560 976 397 1,139 ? (10.5”;) (36.4’,{) (63.9’; ) (25.2’ ; ) (74.8’:;)
Hospital 2,368 884 327 557 143 741 80 (3G.9’,; ) (30.9’ ( j (63.1’ ) , (16.2”;) (83.8’ ; ) (9.1’$,)
‘1‘AHI.E XV
Distribution of Inpatients and Outpatirnts with Rheumatic Heart Disease in a 12 Year Period
Year 1948 1949 1950 1951 1952 1953 19.54 1955 1956 1957 1958 1959 1960
Clinic 18 150 80 46 104 11X 174 140 163 193 117 151 82
Hospital 40 57 90 129 230 242 96 _
TABLE xv,
Distribution of Cases of Rheumatic Heart Disease According to Valvular Damage
hlitral Stenosis
Mitral Insuffi- ciency
Doublr Mitral Lesion
Aortic Stenosis
Aortic Insufi- ciency
4clivc Doublr Rheu- Aortic Combined matic Lesion Lesions Fever Total
Clinic 507 150 290 (17 ‘((
I 92 242 (5.&) (3.7;;)
1,536 (33.0’ ; 1 (C).7’;;, 1 (18.8’;) ) 111.8’; J (15.6’;c )
Hospital 361 30 155 23 84 172 884 (40.8’,‘;) (3.5’,/;. ) c17.5:,; 1 (2.6’ ; j (9.5%;) (19.4”; )
in all age groups, the majority of cases occurring in childhood.
In a discussion of the epidemiology of rheu- maticfever, many factors, such as climate, envi- ronment and socioeconomic conditions, must be taken into consideration. It has been stated that people in the low income groups living in cold, humid and crowded environment present a higher frequency of rheumatic fever and rheumatic heart disease.‘~“~r”~“‘-‘”
Exact epidemiologic data of the incidence of rheumatic heart disease are not commonly found since it is not a reportable disease, and misdiagno- sis is possible. Such epidemiologic studies are very important in order to find the frequency of rheumatic heart disease in different countries having different climate and different sccio- economic conditions. Greece offers advan- tages from many points of view, because its climate is warm most of the time, humid in some areas and dry in others. The socio- economic lelrel is very low in the rural areas,
higher in the city of Athens, but generally pour. The diagnosis of rheumatic heart disease was
made according to the criteria of the New York Heart Association. A history, physical exami- nation, electrocardiogram, x-ray films, and other laboratory tests were obtained in all patients. A number of patients were catheterized.
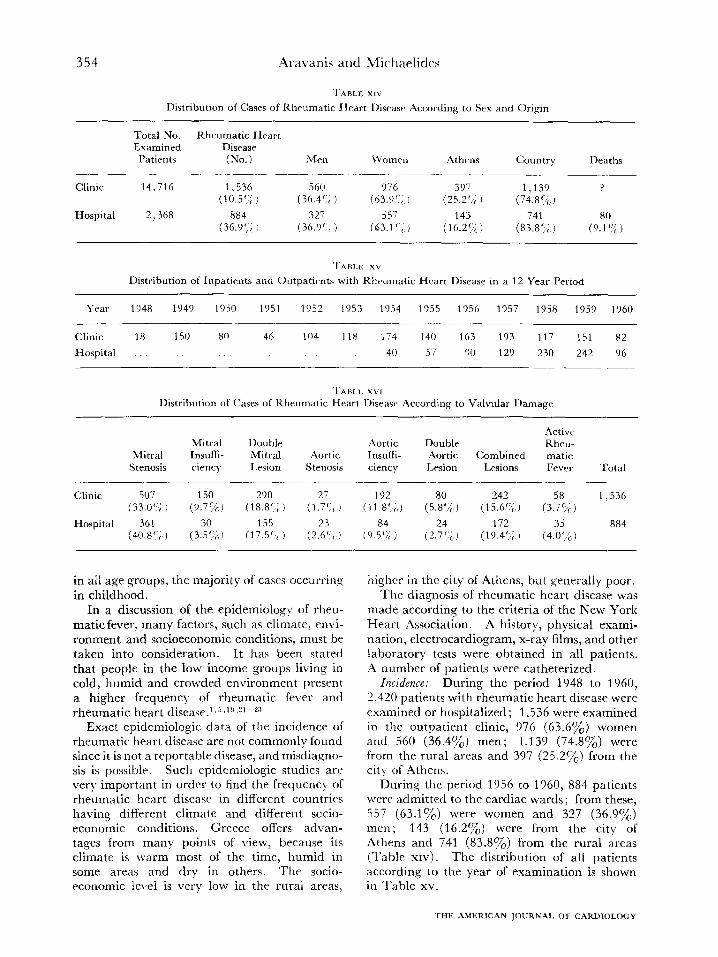
Incidence: During the period 1948 to 1960, 2,420 patients with rheumatic heart disease were examined or hospitalized ; 1,536 were examined in the outpatient clinic, 976 (63.6%) women and 560 (36.4y0) men; 1,139 (74.8%) were from the rural areas and 397 (25.27,) from the tit\- of Athens.
During the period 1956 to 1960, 884 patients were admitted to the cardiac wards; from these, 557 (63.1%) were women and 327 (36.9%) men ; 143 (16.27,) were from the city of Athens and 741 (83.870) from the rural areas (Table XIV). The distribution of all patients according to the year of examination is shown in Table xv.
THE AMERICAN IOIJRNAI. OF CARDIOLOGY

Cardiovascular Diseases in Greece 355
TABLE XVII
Distribution of Cases of Rheumatic Heart Disease According to Age
.4ge O-10 11-20 21-30 31-40 41-50 51-60 61-70 71-80 Total
Number of patients
(1.460%) (184572%) (3Z%) (2Z%) 443 184
(1.k (0.26%) 2,420
(18.3%) (7.6%)
TABLE XVIII
Distribution of Patients with Mitral Stenosis and Hypertension According to Age and Average Blood Pressure
Age 25-29 30-34 35-59 40-44 45-59 50-54 55-59 60-64 65-69
Number of patients 3 1 1 2 8 6 4 3 2 Average blood pres-
sure (mm. Hg) 170 160 177 178 179 185 180 190 192 -
90 -G 104 -GJ G -G - -
98 90 92
For epidemiologic reasons, Greece was divided into seven areas plus the city of Athens with its suburbs. From the ratio of examined patients to that of the population of the different areas, it seems that some areas have a higher frequency of rheumatic heart disease than others. The islands, numbering about one hundred, present the higher frequency as compared to the mountainous areas of the mainland, which present lower incidence.
The rheumatic lesions of the dzyerent values is shown in Table XVI. Isolated mitral stenosis was found in 868 (36.9%) patients. This was the most common valvular lesion, particularly in women, with a ratio of females to males of 2: 1. Mitral stenosis and insufficiency was second, and was found in 445 (18.1%) patients. The third common lesion was represented by the combined lesions of the mitral and aortic valves with 414 (17.5%) patients. Aortic insufficiency was found in 276 (10.6°~o) cases, and isolated aortic stenosis, the most rare valvular lesion, was found only in 50 (2.1%) patients. Tricuspid valvular lesions were found always associated with mitral lesions in 27 (1.17e). The aortic lesions were encountered more often in men than in women with a ratio of 2:l.
Actiue rheumatic fever with cardiac involvement in the first attack or as an active carditis in a previously damaged heart was found in 3.8 per cent of the total number; 81 per cent of these patients were below the age of 20.
Age: The incidence of rheumatic heart disease in the different ages is shown in Table
SEPTEMBER 1962
XVII. The highest was in patients between 21 and 30 years of age, with a total number of 728 (30.2%) patients. Ages 11 to 20 and 31 to 50 presented about the same incidence, with a total number of 1,417 (59yo) patients. A sharp reduction was noted in patients after 50 years of age or more, and only 6 (0.2yo) cases were found in patients over 70. In patients below the age of 10, only 40 (1 .670) cases with already damaged valves were found.
Mitral stenosis was associated with hyperten- sion in 30 cases (1.270) (Table XVIII).
The ratio of rheumatic heart disease to all other heart diseases was 21.9 per cent; to all patients in the Department of Medicine, 2.2 per cent; and to the total number of hospital admissions, 0.9 per cent.
The functional class$ication of the patients with rheumatic heart disease, according to the New York Heart Association classification, was as follows: class I, 24 per cent; class II, 45.6 per cent ; class III, 21.2 per cent; and class IV,
9.2 per cent. Mortality in the hospital-treated patients was
9.1 per cent. The causes of death in decreasing order of frequency were acute rheumatic carditis, heart failure, bacterial endocarditis and embolism.
UNCOMMON HEART DISEASES
This group includes 516 patients (37c) who presented rare types of heart disease. The fol- lowing were encountered, and their incidence is listed (Table xx) :

356 Aravanis and Michaelides
1. Congenital Heart Disease: Among the 149 patients diagnosed as having congenital heart disease, representing I .05 per cent of the total number of cardiac patients, 125 were males and 24 females. The majority were between 10 and 30 years, but a small number of patients were between 30 and 50, and only 13 were above 50 years of age. A detailed analysis of the type of malformations is impossible since a number of these patients were incompletely studied prior to 1954. In a decreasing order of frequency, the following types of congenital malformations were found : atria1 septal defect, ventricular septal defect, tetralogy of Fallot, patent ductus arteriosus, pulmonary stenosis, trilogy of Fallot, coarctation of the aorta, tricuspid atresia and Ebstein malformation, and pentalogy of Fallot.
2. Cvr Pulmonale: There were 34 patients (0.26ry0) with car pulmonale, 16 women and 18 men. None was below 31 years, and the majority were between SO and 70. Most of these patients were in an advanced stage of failure. No relationship was found between disease and occupation, although the majorit) were farmers. Most patients were hcav!- smokers.
3. Luetic Heart Disease: There were 38 patients (0.27(g) with aortic insufhciency of luetic origin: 25 per cent also had angina pec- toris; 50 per cent were women. The majorit!- were between the ages of 40 and 60, only 6 patients being below 40 and 8 above 60. All these patients had positive FVassermann and Kahn tests.
4. Pericarditis: There were 46 patients (0.28(!&) diagnosed as having pericarditis of various etiologies. The majority were between 30 and 50, and only two were above 70 vcars of age. In order of frequency, the following types were observed : tuberculous, idiopathic, due to collagen disease, and cancerous.
5. Suhacilte Bactrrial Endocardit2.s: Only ten cases (O.O7(:J):,) were found. All patients had rheumatic heart disease. Three of them devel- oped endocarditis followine mitral commissur- otomy.
6. Thyroid Heart Diseasrp: Of the 90 patients (0.52%) with thyroid heart disease, 76 were women and 14 were men. The ma.jority were between the ages of 30 and 50. Eight patients presented myxedema while the others had thyrotoxicosis; 35 per cent had atria1 fibrilla- tion.
7. Echinococcus cysts: Two patients (O.Oloj,) were found to have an echinococcus cyst: one
was attached to the pericardium and one in- vaded the myocardium of the left ventricle.
8. Other tybes of rare cardiovascular disorders: a. Intermittent claudication was found in 54
patients (0.34’%), only four in women; the rest were men of middle or advanced age and were diagnosed as having arteriosclerosis obliterans.
b. Paroxysmal atria1 tachycardza was observed in 16 patients (O.lOc~O), mostly young people without any underlying cardiac disease.
c. Wolf-Parkinson- White syndrome was found in 11 patients (0.08%), most of them young people without obvious heart disease.
DISCUSSION
CORONARY HEART DISEASE
Studies of coronary heart disease have not been made in Greece, except for recent observa- tions of Keys and Aravanis in the islands of Crete and Corfu which will be published soon. From these epidemiologic studies and the data of the present work, it seems that coronary heart disease has a much lower incidence in Greece than in Western countries. Although there is the impression among specialists that an increase of coronary heart disease has taken place in Greece during the last years, still the percentage is lower than in other countries. It is difficult to find the exact reasons for this low incidence, but the following facts should be taken into consideration.
Dirt: People of the low and middle socio- economic classes in Greece, the majority of the population, eat food poor in animal fats and proteins, as their income is low and does not per- mit any other diet. However, these people get the basic caloric needs, and no malnutrition or deficiency is observed. The staple food is bread made from wheat, pulses and vegetables in considerable quantities prepared with olive oil. People in the villages eat meat once or twice a week, and many families, only once or twice a month. The use of dairy products is limited because the poor farmer or shepherd prefers to sell what he produces in order to satisfy his basic needs. LVine is in daily use: in some areas, other locally- made alcoholic drinks are also consumed. The main nutri- tional sources are carbohydrates from cooked or raw vegetables and pulses, plus unsaturated fats (usually olive oil), which in some areas add up to 40 per cent of the total calories. The sources for proteins are mainly from pulses and vegetables which, as it is known, contain pro-
THE AzMERICAN JOURNAL OF CARDIOLOGY

Cardiovascular Diseases in Greece 357
teins of lower biologic value. People on the in a continuous struggle for “something more islands and near the coast consume more fish and better” without being able to achieve what than meat. they desire.
The effect of unsaturated fats on serum cho- lesterol is known from clinical and experimental studies,‘l but the influence of considerable amounts of carbohydrates in cooked or raw preparations on serum cholesterol has to be investigated further. FurmanZ5 has noted a decrease in serum cholesterol when proteins were replaced by an isocaloric carbohydrate diet. The studies of Olson and Sebre1126~27 support the view that a low protein diet has a diminishing effect on serum cholesterol. If this takes place in the rural population of this country, it should be better investigated.
Body Weqlrt and Activity: Another important fact is that overweight is uncommon in either sex among the rural people. Their body weight is low and decreases as they become older. They are physically active and obesity is excep- tional. The majority are poor peasants or shepherds who work hard all day in the fields because agriculture is still underdeveloped and is conducted by primitive means. Families are usually large; women do not make any signifi- cant economic contribution, and support falls on the male adult members of the family. For these reasons the income per capita is very low.
If we take into consideration also the fact that the population of the country has not changed significantly through the years, and that the population of Athens has tremendously increased in the last two generations, mainly from people migrating from the country to Athens, we can see that people having the same origin and inheritance as those of the country, when living in Athens, experience coronary heart disease more often than in the rural areas. It seems that we are dealing with a kind of mal- adaptation between these people and their en- vironment, probably growing out of a raised standard of living which has changed nutritional hahits.
The last fact is the tempo of life, which is still slow in the rural areas. The poor Greek is still living far from the achievements of modern civilization and the daily strain of competition.
Although these considerations do not explain the relationship between coronary heart disease, food, work and life, they confirm similar find- ings in other countries and prove that some im- portant relationship must exist among the ahove factors.
Differences in Urban and Rural Classes: Con- trary to the people living in the country, people living in Athens belong to a different socio- economic class. They have a higher income per capita, which permits them to eat better in quality and quantity, and they work fewer hours because they are protected by law. For these reasons, these people, in comparison to the rural, are often overweight, and obesity is not uncommon. Food is high in quantity and hetter in quality. The use of animal proteins and fats, mostly saturated, is much higher. The mean cholesterol value in a number of these people was 16 per cent higher than in the rural people. Moreover, these people suffer frcm the burden of modern civilization and are
Incidence and Mortality: The present study has shown that the frequency of coronary heart disease is low in this country in comparison with other countries. A significant difference of 2: 1 was found between rural and urban areas, probably due to the above mentioned factors. ,411 the rural areas had about the same incidence of coronary heart disease, 0.3 per cent, in comparison to the city of Athens which had 0.6 per cent. The ratio of men to women suffering from coronary heart disease was 6: 1 below the age of 50, and 3: 1 above this age. The low frequency of coronary heart disease in the female is a known fact, but no satisfactory explanation has yet been given. The percent- age of coronary heart disease to all other organic heart diseases (after excluding cases of neurocir- culatory asthenia or other ncnorganic condi- tions) was 25 per cent. This incidence is lower than in similar statistics in Western countries. The frequency of myocardial infarction plus angina pectoris, based on clinical and laboratory data, was 37.4 per cent in the outpatient clinic and 45.7 per cent in the wards. This increase is due to the fact that patients with a myocardial infarction are usually admitted to the hospital.
The incidence of right and left bundle branch block was about equal, i.e., 3.4 per cent; the frequency of complete A-V block, 1 .l per cent.
HYPERTENSIVE HEART DISEASE
Concerning hypertensive heart disease, 2,741 patients were found with high blood pressure. This corresponds to an incidence of 16 per cent of all cardiac patients, 2.4 per cent of all medical cases and 0.6 per cent of all hospital admissions. The percentage of hypertension by age to all
SEPTEMBER t 962

358 Aravanis and Michaelides
‘I-ABLE SIX
Average Blood Pressurr Distribution According to Age of 2,741 Hypertensive Patients
AT (yr. 1 1 l-20 21-30 31.-40 41_~50 51-60 61-70 71-80 81-90 91-100
B.P. (mm. Hg) 150 153 160 1 70 172 178 185 192 190
- To - -
loo -z -
105 100 115 126 118 95
other organic heart diseases is greatest in the hypertension in these areas remains to be deter- sixth and seventh decades of life (Table IX). mined.
It was noticed that, as the age advances, systolic and diastolic blood pressures increase, although this increase has no consistent rela- tionship to age (Table XIX). Diastolic blood pressure increases at a slower rate than systolic, and drops after the age of 70, probabl>- because of loss of elasticity of the large arteries. The highest incidence of hypertension was between 50 and 60 years, covering 35.6 per cent of all cases. Below the age of 40 and abo\re 70, the number with hypertension drops significantly. Generally the number of women suffering from high blood pressure was about twice that of men. Below this age, the number with hyper- tension was the same in both sexes. Many women presented hypertension during or after the menopause. The family histor!., although an important consideration, was unreliable in the majority of our cases.
The incidence o,f coronary heart disease in the hyper- trnsive group was found much lower than in the arteriosclerotic group; 2.5 per cent for myo- cardial infarction and 6.9 per cent for angina pcctoris in the hypertensive group, in contrast to 21.6 per cent for infarction and 20 per cent for angina in the arteriosclerotic group. Since it is difficult in many cases to assert which started first, atherosclerosis or hypertension, the ques- tion arises as to the interrelation between these two conditions. These two disorders may have an independent course and can be found in cithcr pure or combined form. There are many interrelated factors responsible for their simul- taneous or successive appearance.
Geographic lh~eermc~s: A significant cliff’erencc in the incidence of hypertension was observed between the city of Athens (O.CNc,th) and the rural areas (0.02~~). Excluding thr three more remote areas, patients of which arc less likely to come to &4thens for an examination. the incidence for the rural areas incrcascs to 0.03 per cent. It is interesting to note that the population of hthens has increased manyfold in the last two o;enerations through migration of people who, by origin and inheritance, are simi- lar to those of the rural areas. This seems to indicate that the higher incidence of hypcrtcn- sion is connected with the different \vay of life. Comparing all areas, the islands were found to have a slightly higher incidence of hypcrtcn- sion, 0.04 per cent.
The majority of our patients who were hypertensive and had definite signs of coronary heart disease stated that hypertension had lasted for man)- years before the onset of complaints caused by coronary heart disease. Only a minority stated the opposite.
The total serum cholesterol of hypertensive patients without evidence of coronary heart discasc averaged 223 mg.: it was 251 mg. in the group with coexisting coronary heart disease. These data support findings of others to the effect that hypertensi\re patients have a higher \,aluc of cholesterol.
Factors that should bc taken into considera- tion are the diet, which is low in animal protein and fat, the light weight and lack of obesity, the physical activity, and the slow tempo of life of the country people. Another factor to be considered is the high consumption of salt in the islands. Whether there is a causal relationship between this fact and the higher incidcncc of
Cardiac ,2ilanifestations: The electrocardio- graphic changes due to high blood pressure were those of left ventricular hypertrophy, alone or with ischemia; 34.9 per cent of the clinic pa- tients and 94.8 per cent of the hospital patients presented these signs. However, the incidence of other important electrocardiographic findings was higher in the hospital group. This is ex- plained by the fact that patients who entered the hospital were in a more advanced stage of their illness. The same holds true for heart failure; 72 per cent of the hospital patients were in heart failure, in comparison to 17.6 per cent of the clinic patients. It is interesting to note that more than one half of the hypertensive patients over 70 years of age did not present
THE AMERICAN JOURNAL OF CARDIOLOGY

Cardiovascular Diseases in Greece 359
evidence of heart failure. This seems to indicate that high blood pressure after a certain age is compatible with longevity or that a higher value of blood pressure after a certain age represents a variant of what is called “normal blood pressure.”
The incidence of malignant hypertension in females was double that of males.
No exact data of the results of treatment fol- lowed by these patients are given in this study. The over-all mortality in the hospitalized group was 3.9 per cent. The mortality in the clinic was impossible to determine.
RHEUMATIC HEART DISEASE
Statistics of the frequency of rheumatic heart disease are unavailable in Greece, and this is one reason for our pilot study. Greece belongs to the temperate zone, and its climate is warm most of the year, except in the northern parts where winter is colder. The country is sur- rounded by sea, in which can be found about a hundred islands. The climate presents minor local variations, but the islands and the coast have a humid climate, unlike the mountainous areas, which have a dry and rather cold climate. The weather is sunny most of the year.
Socioeconomic conditions are about the same in all rural areas. How these factors can in- fluence the incidence of rheumatic fever is not clear, but their relationship to the epidemiology of streptococcal infections is probable.
From a total number of 17,084 patients who were examined and hospitalized in a 12 year period, 2,420 presented rheumatic heart disease, corresponding to an incidence of 14.1 per cent of all cardiac cases. The incidence in females was double that in males at all ages. This holds especially true for lesions of the mitral valve, a fact which is in disagreement with other studies.28 On the other hand, aortic valve lesions were more frequent in males.
Incidence of Rheumatic Fezfer: It is difficult to state what is the incidence of rheumatic fever in this country. About three quarters of the pa- tients came from the rural areas and one fourth from the city of Athens. Most of the rural areas are mountainous; people live in small villages at relatively high altitude and are farmers, shepherds or manual workers. The climate is colder and dry throughout the year, more so during winter, with occasional snow. These areas presented a lower incidence of rheumatic heart disease than those surrounded by the sea, particularly the islands, which have a warmer
SEPTEMBER 1962
climate, higher humidity and a longer rainy season. It was noticed also that coastal areas had a higher incidence of rheumatic heart dis- ease than inland areas. Living conditions are about the same in all areas as far as housing, diet and average income are concerned. In- adequate clothing, inadequate food, unheated but not crowded homes are typical.
In the city of Athens living conditions are different: Poor people live in small, crowded homes where streptococcal transmission is easier, but food is better and the climate is warmer and dry. The incidence of rheumatic heart disease in Athens was 0.04 per cent of the popula- tion, in contrast to 0.027 per cent in the rural areas, except for the islands where it increased to 0.056 per cent.
Acute rheumatic fever was found in 3.8 per cent (usually at the second or third attack) of patients who had already suffered from valvular damage in previous episodes and did not receive prophylaxis. It seems that rheumatic fever is often misdiagnosed in the rural areas. This is why these patients often reached the hospital with pancarditis and heart failure. Many died without responding to treatment. Even high doses of steroids gave no help in these cases; 81 per cent were below the age of 20, and, with increase in age, fewer cases were ob- served.
Valuular Lesions: Of all valves, the mitral was found to be the most commonly involved. Mitral stenosis was found in 36.9 per cent of all patients. Mitral stenosis and insufficiency and combined lesions of the mitral and aortic valves followed in frequency. Isolated lesions of the aortic valve were third, and the most infre- quent were those of the tricuspid valve, which were always associated with mitral valve dam- age. Mitral lesions, particularly mitral steno- sis, caused symptoms earlier than aortic lesions.
Only in 484 cases (2Oyo) was a history of rheumatic fever elicited, and in 5 cases a history of chorea. About two thirds stated that this took place in childhood. Almost all patients presented a history of repeated attacks of ton- silitis. The reported incidence of rheumatic fever is probably not correct because minor signs of rheumatic fever are usually overlooked in the rural areas. It is the opinion of the authors that a program for diagnosis, treatment and prevention of rheumatic fever is needed in Greece.
Mitral stenosis was associated with systemic hypertension in 3.4 per cent of the cases. It

360 Aravanis and Michaelides
Distribution of Uncommon Cardiovascular I)iwaws and Prrcmtase of the Total Numhcr of Cardiac Patirnts
I. (:ongenital heart disrasc 179 (I.osl;)
2. Car pulmonalc 44 (C).26’, ) 3. Lwtic heart diseasr 47 (C).27”;,)
4. Pcricarditis 50 (0.28’ ; ) 5. I:ndocarditis 11 (0.28’, I
6. Thyroid hrart disrasc 9s (O.SZ’ ;
7. Echinocxcus cysts 2 (CJ.01 ’ ,
8. Intrrmittcnt claudication 58 10.34 ’ ( )
9. Paroxysmal auricular tachycardia 1X (o.lo’;,J
10. Wolf-Parkinson-White syndrome 12. (0.08”; I
-
has been stated that coexisting hypertension in
Discanc
patients with mitral stenosis‘;hai’ a favorable effect, due to dilatation of the left vcntriclc and of the A-\’ ring. No conclusions could be drawn from our cases.
The highest frequency of rlleumatic heart disease was in the 21 to 30 year agr group, i.e., 30.2 per cent of the total number. Between the ages 11 to 20 and 31 to 50 the rate was also high, but after SO, it dropped significantly; only 53 cases were found above 61. The oldest patient \vith mitral stenosis was still alive at the age of 74. It was observed that patients with mitral stenosis or insufliciency li\.ed longer than patients \vith aortic valve lesions, ItcXausc the former, c\cYi though they were for man) years in and out of heart failure, responded better to trratment. On the contrary. patients with aortic lesions often had an uneventful lift until the fourth decade but, when heart failure started, the evolution was rapid, and respons< to treatment was poor. Under the age of 10, 1%~’ found only 41) cases (1 .6C,?&) with vstal>lishrd valvular lesions. The youngest was a 3 yeas old girl with mitral stcnosiq. It is intcr0ting to note that her mother had suffered from rlleu- matic fever during pregnancy.
The ma,jorit). of the cases belonged to classes 11 and III. This is due to the fact that many patients from the rural areas had been diaynosrd only after their functional capacity was signifi- cantly diminished and they had been workinq hard until latex in the course of the disaasc.
The electrocardiographic findings usually reflected thr hcmodynamic burdrn of the \,al\ru- lar damaqc. ;2trial fibrillation was found in 363 cases (1 i(,Z&) : 82 per cent were patients with mitral lesions.
The mortality rate \vas 9.1 per cent in the hospital-treated patients, and was due, in order c:f frequency, to rheumatic carditis, heart failure, t)actrrial endocarditis and embolism.Yg-“’
SL-hIMARY
‘Ik clinical material of the last 12 years ob- served in the department of cardiology of a 700 bed charity hospital in the city of Athens was studied in order to find the prevalence of coro- nary, hypertensive, rheumatic and rare heart diseases.
It was found that the incidence of coronary hr’art cl&ease and its sequelae in the low and middle socioeconomic classes is law both in the rural areas and the city of Athens, though with dXerenccs, probably due to different diet and \vay of life. Serum cholesterol was found to he lower in the rural areas, though higher among people suffering from coronary heart disease. A 16 per cent incrrase of cholesterol was found in the city of Athens in comparison with the rural areas. Although the population of Athens is basically the same as that of the country, it leas an incidence of coronary heart disease cioul)le that of the country population, probably CILK to environmental factors which have also cllanged nutritional habits.
The incidence of hypertensive heart disease in the city of Athens was three times higher than in rural areas. Women presented hypertension three times more often than men after the age of 50 but had the same incidence below this a,ge. An increase of systolic blood pressure was ob- srrvcd with aqe, hut was not proportional to it. Diastolic blood pressure also increases but at a lower rate, and after the age of 70, it drops, so that a wider pulse pressure can be observed. .An average mortality of 3.9 per cent \vas found in the hospital patients, mainly due to cerrbro- \,ascular complications or heart failure.
The incidence of rheumatic heart disease was 14.1 per cent of all cardiac cases with a ratio of females to males of 2 to I. The frequency of rheumatic heart disease was found lower in the. city of Athens. This was probably due to diff‘crrnccs in socioeconomic and phvsical en- vironments. Estahlished valvular lesions were found in the majority of patients at the age of 20. The mortality of hospital patients was 9.1 per cent, the result of misdia,gnosed or inadequately treated cases of acti1.e rheumatic fever, heart failure, bacterial endocarditis and embolism. Rheumatic heart disease is not rare in Greece, t)ut there arc differences between the various

Cardiovascular Diseases in Greece 361
areas, probably due to living conditions, cli- mate and poorer diagnosis and treatment in the rural areas. A program of prevention and treatment of rheumatic fever is needed in this country.
KEYS, A. Epidemiological aspects of coronary heart disease. J. C/won. Dis., 6: 552, 1957.
KEYS, A. Opinions, decisions, and facts. Czrcula- tion, 22: 501, 1960.
KEYS, A. The risk of coronary heart disease. Cir- culation, 23: 805, 1961.
5.
6.
7.
KEYS, A. and FIDANZA, F. Serum cholesterol and
KEYS, A. Diet and the epidemiology of coronary heart disease. J.A.M.A.. 164: 1912, 1957.
relative body weight of coronary patients in dif- ferent populations. Circulation, 22 : 1091, 1960.
WHITE, P. D. Heart Disease, ed. 4, p. 520. New York, 1951. The Macmillan Co.
KEYS, A., KARVONEN, M. J. and FIDANZA, F. Serum cholesterol studies in Finland. Lancet, 26: 175, 1958.
8. KEYS, ‘4. and WHITE, P. D. World Trends in Cardiology. Vol. 1. Cardiovascular Epidemi- oloev. D. 3. New York. 1956. P. B. Hoeber. Inc.
YII I
9. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Blood Vessels. New York Heart Association Inc., 1953.
10.
Il.
12.
13.
14.
15.
16.
DONNISSON, C. I’. Blood pressure in the African native. Its bearing upon the etiology of hyper- piesia and arteriosclerosis. Lancct, 1 : 6, 1929.
WILLIAMS, A. W. Blood pressure of Africans. East rlfrican M. J., 18: 109, 1941.
WILI.IAMS, A. W. Heart disease in native population of Uganda; hypertensive heart disease. East .4frican M. J., 21: 328, 1944.
ORDMAN, B. Review of incidence of hypertension in non-European races; survey of blood pressure in South African Bantu. Clin. PTOC., 7: 183, 1948.
TUNG, C. L. Blood pressure in northern Chinese males. Chinese J. Physiol., 4: 117, 1930.
NYE, L. J. a. Blood pressure in the Australian ab- original with a consideration of possible aetio- logical factors in hyperpiesia and its relation to civilization. Australian M. J., 2: 1000, 1937.
MIAI.L, W. E. and OLDHAM, P. D. Factors in- fluencing arterial blood pressure in the general population. Clin. SC., 17: 409, 1958.
REFERENCES
17. MIASNNIKOV, A. L. Diagnostic and pathogenic borderlines between hypertensive disease and atherosclerosis. Am. J. Cardiol., 5: 692, 1960.
18. HAMILTON, M., PICKERING, G. W., ROBERTS, J. A. F. and SOWRY, G. S. C. The aetiology of essen- tial hypertension; the arterial pressure in the general population. Clin. SC., 13: 11, 1954.
19. LUISADA, A. A. Heart, ed. 2, p. 63. Baltimore, 1954. Williams and Wilkins.
20. FRIEDBERG, C. K. Diseases of the Heart, ed. 2, p. 921. Philadelphia, 1956. W. B. Saunders.
21. LIEBER, S. L. and HOLOUBEK, J. E. Acute rheu- matic fever in a large southern hospital over the five year period 1950-1954. Ann. Int. Med., 45: 7, 1956.
22. SALAZAR-MALLEN, M. and RULFO, .J. On some fea- tures of rheumatic fever and rheumatic heart disease as seen in the National Cardiological Institute of Mexico. Ann. Int. Med., 42: 607, 1955.
23. COHN, E. A. and LINGG, C. The natural history of rheumatic cardiac disease. Mod. Convpts Cardio- uas. Zk., 11 : 7, 1942.
24. KEYS, A., ANDERSON, J. T. and GRANDE, F. Ef- fect on serum cholesterol in man of monoene fatty acid (oleic acid) in the diet. Proc. Sot. Ex@r. Biol. @ Med., 98: 387, 1958.
25. FURMAN, R. H., HOWARD, R. P. and NORGIA, L. N. Hormones and Atherosclerosis. Edited by G. Pincus. New York, 1959. Academic Press.
26. OLSON, R. E., VESTER, J. W., GURSEY, D., DAVIS, N. and LONGMAN, D. The effect of low protein diets upon serum cholesterol in man. Am. J. Clin. Nutrition, 6: 310, 1958.
27. SEBRELL, W. H. et al. Appraisal of nutrition in Haiti. Am. <J. Clin. Nutrition, 7: 538, 1959.
28. SAI.AZAR-MALLEN, hl., EVANS, M. and BALCAZAR, J. Further studies on rheumatic fever epidemi- ology. Am. J. Cardiol., 1: 431, 1958.
29. BLAND, E. F. and JONES, T. D. The natural history of rheumatic fever: a 20 year perspective. Ann. Znt. Med., 37: 1006, 1952.
30. WILSON, M. G. and LURSCHEZ, R. Longevity of rheumatic fever, based on experience in 1042 children observed over period of 30 years. J.A.M.A., 138: 794, 1948.
31. SOLOFF, L. A. and ZATUCHNI, J. Causes of death in rheumatic heart disease. Relationship to the incidence of mitral stenosis occurring alone or with other valvular lesions. Am. J. Mrd., 18: 419, 1955.
SEPTEMBER i 962