Embed Size (px)
Citation preview

Cardiometabolic Health Disparities in Native Hawaiians and OtherPacific Islanders
Marjorie K. Mau, Ka‘imi Sinclair, Erin P. Saito, Kau‘i N. Baumhofer, and Joseph Keawe‘aimokuKaholokulaCenter for Native and Pacific Health Disparities Research, Department of Native Hawaiian Health,John A. Burns School of Medicine, University of Hawai‘i at Manoa, Honolulu, Hawai‘i
AbstractElimination of health disparities in the United States is a national health priority. Cardiovasculardisease, diabetes, and obesity are key features of what is now referred to as the “cardiometabolicsyndrome,” which disproportionately affects racial/ethnic minority populations, including NativeHawaiians and other Pacific Islanders (NHOPI). Few studies have adequately characterized thecardiometabolic syndrome in high-risk populations such as NHOPI. The authors systematicallyassessed the existing literature on cardiometabolic disorders among NHOPI to understand the bestapproaches to eliminating cardiometabolic health disparities in this population. Articles wereidentified from database searches performed in PubMed and MEDLINE from January 1998 toDecember 2008; 43 studies were included in the review. There is growing confirmatory evidencethat NHOPI are one of the highest-risk populations for cardiometabolic diseases in the United States.Most studies found increased prevalences of diabetes, obesity, and cardiovascular risk factors amongNHOPI. The few experimental intervention studies found positive results. Methodological issuesincluded small sample sizes, sample bias, inappropriate racial/ethnic aggregation of NHOPI withAsians, and a limited number of intervention studies. Significant gaps remain in the understandingof cardiometabolic health disparities among NHOPI in the United States. More experimentalintervention studies are needed to examine promising approaches to reversing the rising tide ofcardiometabolic health disparities in NHOPI.
Keywordscardiovascular diseases; diabetes mellitus; healthcare disparities; health status disparities; metabolicsyndrome X; minority groups; minority health; obesity
INTRODUCTIONThe prevalence of cardiometabolic disorders, including cardiovascular disease, diabetes, andobesity, has reached epidemic proportions worldwide. Prevalences of diabetes andcardiovascular disease among ethnic minorities in the United States exceed those seen in thegeneral population (1–7). Because of the excess health burden of cardiovascular disease anddiabetes in ethnic minorities, cardiometabolic risk, as the precursor of these diseases, providesa specific target for conducting investigations that aim to reverse and/or eliminate these
© The Author 2009. Published by the Johns Hopkins Bloomberg School of Public Health.Correspondence to Dr. Marjorie K. Mau, Department of Native Hawaiian Health, John A. Burns School of Medicine, University ofHawai‘i at Manoa, 677 Ala Moana Blvd., Suite 1016B, Honolulu, HI 96813 ([email protected]).Conflict of interest: none declared.
NIH Public AccessAuthor ManuscriptEpidemiol Rev. Author manuscript; available in PMC 2010 June 28.
Published in final edited form as:Epidemiol Rev. 2009 ; 31: 113–129. doi:10.1093/ajerev/mxp004.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

disparities. Moreover, obesity, as one of the central pathophysiologic mechanisms underlyingthe syndrome of cardiometabolic risk, might constitute an earlier “upstream” target fortreatment and prevention that could be effective in reducing excess morbidity.
In this review, we focused on cardiometabolic health disparities among Native Hawaiians andother Pacific Islanders (NHOPI). As a federal designation, “Native Hawaiian or Other PacificIslander” refers to persons with origins in any of the original peoples of the islands of Polynesia,Micronesia, and Melanesia (8). The first Polynesian settlers of the Hawaiian Islands are thoughtto have migrated from the Marquesas Islands as early as 100 B.C.E., some 2,000 years ago(9). Hawaiians lived in isolation until 1778, when European explorers brought with them deadlyforeign infectious diseases that decimated the Native population. Colonization and the eventualoverthrow of the Hawaiian monarchy resulted in a loss of land and political power, as well astraditional practices and customs, including the near extinction of the Hawaiian language (9).
Events such as the cultural revival referred to as the “Hawaiian Renaissance,” the return of theisland of Kahoolawe to the Hawaiian people, the formation of political bodies such as the Officeof Hawaiian Affairs, the public recognition of the illegal overthrow of the Hawaiian monarchy,and the ongoing voyages of the Hokule‘a using historical navigation techniques of NativeHawaiians serve to highlight the resiliency and strength of this population. However, despitethese positive social and political developments, NHOPI are overrepresented in lowersocioeconomic groups, report greater difficulties in obtaining health care, and may be affectedby internalized racism as a consequence of their historical experience of disenfranchisementand loss of power within their traditional homeland (10–12). In addition, NHOPI continue tobear a disproportionate burden of disease, including cardiovascular disease and diabetes.
Today, the state of Hawai‘i has the largest population of Native Hawaiians in the United States,followed by California. Among ethnic subgroups in Hawai‘i, Native Hawaiians have thehighest prevalence of diagnosed diabetes (11.5%), with reported prevalences ranging from19% to 22% for type 2 diabetes and from 16% to 35% for impaired glucose tolerance (5,13,14). Cardiovascular disease mortality among Native Hawaiians in 2004 was more than twicethat in Japanese, who had the lowest rates (372 per 100,000 population vs. 167 per 100,000population), and diabetes-related mortality was 3 times higher in Native Hawaiians than inCaucasians (39 per 100,000 population vs. 13 per 100,000 population) (6). The NativeHawaiian Health Research (NHHR) Project examined the relation between a clustering ofcardiovascular risk factors and biochemical markers of insulin resistance (fasting insulin andC-peptide levels) (7). The investigators found that fasting insulin concentrations werecorrelated with body mass index, waist-to-hip ratio, blood pressure, and levels of triglyceride,high density lipoprotein cholesterol, and glucose. A significant correlation was also foundbetween increasing insulin resistance and increased clustering of cardiovascular disease riskfactors. The NHHR study, in addition to a limited number of other studies on NHOPI, suggeststhat significant disparities occur between and among these populations. The purpose of thisreview was to systematically assess the state of the science related to cardiovascular disease,diabetes, and adiposity among NHOPI.
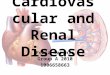
METHODSDatabase searches were performed in PubMed and MED-LINE for the time period of January1998 to December 2008, with keyword combinations of the following racial/ethnic groups inan “OR” search term: Native Hawaiian, Hawaiian, Pacific Islander, Samoan, Tongan,Micronesian, New Zealand, Maori, Melanesia, Chamorro, Guamanian, Fijian, andPolynesian (Figure 1). The racial/ethnic groups were then included in combination with thefollowing terms defined as an “OR” function: minority, minorities, groups, ethnicity, andethnicities. The above racial/ethnic AND minorities search term was identified as a “Set A”
Mau et al. Page 2
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

keyword search. Results from the Set A keyword search were then combined with Set Bkeywords as an “OR” search term which included the following: inequity, inequality, healthdisparities, health differences, cardiovascular, hypertension, heart, heart failure, heartdisease, heart disease risk factors, cardiac, cardiomyopathy, diabetes, syndrome X, metabolicsyndrome, insulin resistance, glucose intolerance, prediabetes, cardiometabolic, obesity,adiposity, overweight, physical inactivity, physical activity, nutrition, diet, and smoking incombination with United States.
Additional studies (n = 21) were also extracted from the reference lists of the articles identifiedin the initial search using Set A AND Set B keywords; these studies were reviewed forinclusion/exclusion. The searches were restricted to English-language articles on humans aged≥19 years that had been published in peer-reviewed scientific journals. Articles were excludedfrom the review if they were letters, editorials, or literature reviews without new data; if theyhad been published in a foreign language; or if they were nonempirical.
Using this search strategy, we identified 311 citations, of which 98 were deemed relevantthrough review of the article title (performed by a single reviewer). All 98 articles underwentabstract review by 2 independent reviewers, using a standard checklist adapted from otherreviews of the health-disparities literature (15). Of the 98 abstracts reviewed, 71 articles wereselected for a full text review, which was performed by 2 independent reviewers to ensurecompliance with all inclusion criteria, as well as ranking on the following study design criteria:1) use of appropriate indicators for patient characteristics (e.g., race, ethnicity, or ancestry, sex,age, education, income); 2) inclusion of objective measures of the outcomes of interest (i.e.,measured height, weight, and systolic and diastolic blood pressure; self-report of or medicalchart review to determine obesity, cardiovascular disease, and/or diabetes status, etc.); 3)inclusion of well-defined measures of disease status; and 4) appropriate adjustment for patientcomorbid conditions (i.e., age, sex, body mass index for diabetes outcomes, blood pressure forcardiovascular outcomes, etc.).
After full text review, a joint review meeting was convened to determine the final selection ofarticles to be included in this study. A total of 28 articles were excluded for 1 or more of thefollowing reasons: 1) NHOPI were aggregated with other racial/ethnic groups (i.e., “Asiansand Pacific Islanders” was a single category) (18% of articles); 2) the article was a review oreditorial (36%); 3) the study included NHOPI but there was no specified outcome related tocardiometabolic diseases (21%); 4) the NHOPI study population lived outside of the UnitedStates (14%); 5) the study population was under age 19 years (i.e., children or youths) (7%);and 6) there was another miscellaneous reason for study exclusion (the article had beenpublished in a non-peer-reviewed journal, no NHOPI population was included, etc.) (4%).Thus, the final number of articles included in this literature review of cardiometabolic healthand health-care disparities among NHOPI was 43.
RESULTSCardiovascular disease
Study characteristics—A total of 12 papers pertaining to cardiovascular disease or its riskfactors were reviewed (Table 1). The majority of studies (n = 10) were cross-sectional. In 4 ofthe 10 cross-sectional studies, investigators had prospectively collected new data, and in 2 theyhad used retrospective data collected from administrative databases. A single prospective studyincluded a cohort that had been followed for over 4 years. One study included qualitative datacollected through focus groups of NHOPI. The only study in which researchers had proposedtesting an intervention had had a quasi-experimental, pre-post study design without controlsfor testing of a Native Hawaiian cultural intervention designed to improve hypertension
Mau et al. Page 3
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

profiles. Fifty percent of the papers included a study sample of at least 300 participants ofNHOPI ancestry.
Study findings—NHOPI women were found to have a high frequency of hypertension andhigh cholesterol in comparison with whites and other ethnic groups (16,17). Studies thatexamined hypertension along with other covariates in NHOPI found that hypertension wassignificantly related to degree of Hawaiian ancestry and especially diastolic blood pressureafter controlling for other covariates (18). The sole genetic study found that increased correctedQ–T interval (Q-Tc), which has been associated with heart disease and sudden death, wasassociated with the angiotensin-converting enzyme insertion/insertion (ACE II) genotype,which is found with greater frequency among Native Hawaiians than in other ethnic groups(19). Verderber et al. (20) compared post-coronary artery bypass graft (CABG) complicationsacross ethnic groups and found that NHOPI had similar early post-CABG complications (first20 hours after CABG) but experienced significantly more ventricular arrhythmias requiringmedical treatment on postoperative day 2 than Japanese. In another study, NHOPI men withacute coronary syndrome were significantly more likely to receive CABG (odds ratio = 1.8,95% confidence interval: 1.2, 2.7) and less likely to receive percutaneous coronary interventionfollowing their first hospitalization than were whites (21). No ethnic differences inendovascular treatment for acute coronary syndrome were found in women (21).
In the only longitudinal prospective cohort study, investigators were interested in examiningmeasures of socioeconomic status and cardiovascular disease risk factors in American Samoansversus Western Samoans. Ezeamama et al. (22) found that high socioeconomic status wasassociated with increased odds of cardiovascular disease risk factors in Western Samoa butdecreased odds in more developed American Samoa. The authors attributed this differentialeffect of socioeconomic status on cardiovascular disease risk factors to the heterogeneity acrossthe Samoan Islands in specific exposures to economic development and the natural history ofindividual cardiovascular disease risk profiles.
Study limitations—The cardiovascular disease literature reviewed had a number oflimitations. First, nearly all of the studies were observational studies with cross-sectional data,which does not permit a clear understanding of cause and effect for significant associationsbetween outcomes and exposures. Half of the studies reviewed had relatively small samplesizes or had serious sample biases that confounded the study’s findings. Finally, several of thestudies of sufficient quality were drawn from 2 research groups that have established cohortsin rural communities in Hawai‘i (Grandinetti et al. (19,23)) and in Western and AmericanSamoa (Ezeamama et al. (22)); those findings may not be generalizable to other NHOPIpopulations in the United States.
Type 2 diabetes mellitusStudy characteristics—A total of 16 diabetes-related studies were reviewed. Most werecross-sectional investigations (10 studies), although 1 study was descriptive and 2 wereretrospective (Table 2). Nine of the cross-sectional studies examined the population-based dataof the NHHR Project, including a quasi-experimental study that was a nonrandomizedconcurrent intervention which included Native Hawaiians with diabetes or at risk for diabetes.Another quasi-experimental study compared “before” and “after” hemoglobin A1c levels in asmall sample of Native Hawaiian, Samoan, and Tongan participants undergoing an interventiondelivered by community health workers. Sample sizes ranged from 78 participants to morethan 3,000. The 2 retrospective studies examined the incidence of macrosomia and gestationalhypertension among NHOPI women.
Mau et al. Page 4
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Study findings—Among studies using the NHHR data, Grandinetti et al. (5) foundprevalences of type 2 diabetes and impaired glucose tolerance to be higher among NHOPI thanamong Caucasian participants. The overall prevalence of diabetes was 4 times higher in theNHHR participants than in the Second National Health and Nutrition Examination Surveypopulation, and the prevalence of diabetes was also significantly higher among full Hawaiiansthan among part-Hawaiians. In comparison with global estimates of standardized prevalencerates (24), 1 study revealed that the prevalences of diabetes and impaired glucose toleranceamong Hawaiians in the NHHR study were among the highest reported, except for Pima andNauruan populations (5). Grandinetti et al. (5) also found that the age-adjusted prevalence ofimpaired glucose tolerance was higher in Hawaiian women than in men and was significantlyassociated with measures of adiposity (i.e., body mass index, waist circumference, and waist-to-hip ratio). Similarly, Kaholokula et al. (18) reported that increased Hawaiian blood quantumwas significantly associated with higher fasting glucose concentration, body mass index, andwaist-to-hip ratio.
Three studies examined the relation between ethnicity, depressive symptoms, and diabetesamong NHHR participants. Among Native Hawaiians with diabetes, depressive symptomswere associated with poorer physical functioning, poorer perception of general health, moresevere and limiting bodily pains, less energy, and more emotional problems (25). NHHRparticipants with elevated hemoglobin A1c levels reported more depressive symptoms and alower quality of life than participants with normal hemoglobin A1c levels (26,27). Anothercross-sectional study of NHHR participants examined dietary patterns, ethnicity, and theprevalence of diabetes and found that consumption of local ethnic foods was positivelycorrelated with body mass index, smoking, waist-to-hip ratio, fasting glucose, and 2-hourglucose (28). Native Hawaiians were found to have significantly higher consumption of thesefoods and the highest total energy intake in comparison with all other ethnic groups. Theseresults suggest that total energy intake may be a more significant risk factor for diabetes thana specific dietary pattern among Native Hawaiians (28). In the nonrandomized concurrentintervention study that enrolled Native Hawaiians with diabetes or at risk for diabetes,participants in a family support intervention were more likely than a standard interventiongroup to advance from the pre-action stage of change to the action/maintenance stage withregard to fat intake and physical activity (29).
Three additional studies examined diabetes-related conditions. Mau et al. (30) found that theprevalence of chronic kidney disease was higher among Native Hawaiians than among Asianand Pacific Islander participants in the National Kidney Foundation’s Kidney Early EvaluationProgram community screening. In a retrospective study of perinatal outcomes in NHOPIwomen by Silva et al. (31), a higher percentage of NHOPI women required insulin duringpregnancy and before 20 weeks’ gestation, suggesting that there may be a larger subset ofNHOPI women with preexisting undiagnosed diabetes.
Study limitations—A major limitation of the diabetes-related research with NHOPIpopulations is the lack of studies that have tested the efficacy of interventions. A large numberof studies were observational, cross-sectional studies that precluded causal inferences. Severalof the studies also had small sample sizes, resulting in limited generalizability.
ObesityStudy characteristics—There were 15 obesity-related studies reviewed (Table 3). Fourstudies examined data from the Multiethnic Cohort Study, a population-based cohort studydesigned to examine risk factors for cancer (i.e., obesity) that included Asian, black, Hawaiian,Latino, and white adults from Hawai‘i and California. One additional study was a population-based prospective cohort study of ethnic groups residing in Hawai‘i. Another study pooled data
Mau et al. Page 5
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

from 18 population-based epidemiologic studies conducted in Hawai‘i over a period of 25years to examine trends in body mass index among different ethnic groups in Hawai‘i and toexplore associations between food intake and excess weight. Seven studies were cross-sectional. Two studies, 1 cross-sectional and 1 longitudinal, examined genetic associationswith body mass index among Samoans residing in American Samoa. One study was qualitative;the researchers conducted focus groups with 32 Native Hawaiian community college studentsto explore facilitators and barriers to living a healthy lifestyle.
Study findings—Prevalences of overweight and obesity were consistently higher amongNative Hawaiians than in other ethnic groups (whites, blacks, Latinos, Asians, and Filipinos)across studies. Grandinetti et al. (32) reported a combined prevalence of 82% for overweightand obesity in NHHR study participants, as compared with a national prevalence of 53%; 49%were obese as compared with 21% nationally. Body mass index was also higher in personswith an ethnic admixture that included Native Hawaiian ancestry, as compared with most otherethnic combinations (32,33). In pooled data from 18 population-based studies carried out over25 years, Native Hawaiians had the highest prevalence of excess weight at all times (34).
Energy intake was consistently higher among NHOPI than in other ethnic groups in Hawai‘i.Both the NHHR and Multiethnic Cohort studies found that total dietary energy intake wassignificantly associated with Native Hawaiian ancestry and increased body mass index (32,34). In 2 large population-based prospective studies, Native Hawaiians had the highest chronicdisease risk scores in comparison with other ethnic groups, primarily because of highprevalences of overweight and obesity, higher rates of smoking, and chronic alcohol use (35).In the NHHR study, increased body weight was strongly associated with glucose intolerance(5). Despite the high prevalence of overweight and obesity, NHOPI reported a higherprevalence of physical activity in the 2001 Hawai‘i Behavioral Risk Factor SurveillanceSystem survey than did other ethnic groups (36).
Study limitations—The obesity-related studies reviewed had several limitations. First, thecross-sectional design of many of the studies did not allow for determination of causal relations.Second, many of the studies were questionnaire-based and may have been vulnerable to recallbias or a propensity towards giving socially desirable answers. Finally, investigators in severalstudies were unable to measure confounding variables, which limited the potential forunderstanding the true association between exposure and disease.
DISCUSSIONStudies of cardiometabolic disparities among NHOPI are sparse. The 43 studies in this reviewwere published in the last 10 years and provide growing evidence that NHOPI are one of thehighest-risk US populations affected by cardio-metabolic diseases. Some progress has beenmade in addressing these disparities, as evidenced by the handful of studies that have shiftedfrom observational research towards program development and then to experimental andclinical trial-type studies that include NHOPI. However, there were a number ofmethodological issues apparent during the course of this literature review. For example, therewere several studies that were limited by sample bias (convenience samples, etc.) and relativelysmall sample sizes (i.e., <50 subjects). NHOPI comprise less than 1% of the US population,and thus recruitment of NHOPI into research studies remains a challenge. Despite thesechallenges, a number of research teams have been successful in enrolling sufficient-sizedsamples or have taken advantage of existing data or administrative databases to betterunderstand cardiometabolic diseases in this population. Moreover, recent developments in theuse of community engagement approaches have served to increase the participation of thispopulation in research activities and ensure that studies are relevant and translatable to NHOPIcommunities.
Mau et al. Page 6
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Aggregation of NHOPI with Asian Americans in several publications limited the number ofavailable studies for this review. There was also a paucity of experimental studies that wereadequately designed to reduce treatment bias (i.e., randomization) and longitudinal prospectivecohort studies that would allow elucidation of cause-and-effect relations in cardiometabolicdiseases. However, a few focus groups and quasi-experimental studies provided preliminarydata that offer potential for designing intervention studies in the future.
Several studies (29,37–40) provided initial insights on promising approaches in NHOPIpopulations, such as social and/or family support and the inclusion of cultural and/or traditionalhealing methods as alternatives or supplements to conventional medical regimens. Otherstudies provided empirical evidence with which to develop scientifically informed andculturally specific diet-based interventions for prevention and treatment of cardiometabolicdisparities. Health care differences in cardiovascular disease treatment suggest that more studyis needed in order to determine the best medical treatments for high-risk ethnic groups such asNHOPI (20,21). Further investigation is needed to examine both provider factors and patientfactors that may underlie the treatment differentials between patients who may receive differenttreatments and hence have different outcomes.
There remain significant gaps in our understanding as to why cardiometabolic diseases occurmore frequently in the NHOPI population in the United States (Figure 2). Any number offactors, alone or in combination, may contribute to the creation of disparities in health withinthis population. Compared with most other US ethnic groups, NHOPI are overrepresented inthe lower socioeconomic strata, under-represented in higher education, and more likely to bemarginalized from the larger society (41). Behavioral risk factors for diabetes andcardiovascular disease, such as tobacco use and psychological distress, are highly prevalent inNHOPI (42). In the case of Native Hawaiians, many health professionals have suggested thatthe health disparities experienced by Native Hawaiians are associated with their lower socialstatus and adverse historical relations with Western governments (43,44). Thus, it would seemappropriate in future studies to explore psychosocial stressors that may contribute to healthdisparities in NHOPI.
Future research aimed at eliminating cardiometabolic disparities in health and health careamong NHOPI needs to move beyond observational studies into intervention studies that willengage NHOPI communities in the process while maintaining scientific rigor. Researchersshould consider the whole spectrum of types of scientific studies—ranging from genetic, benchstudies to clinical studies to effectiveness studies that test interventions in real-world settings.NHOPI can participate in this research not only as study subjects but also as investigators. Inthis way, they can both obtain health equity and, more importantly, help to promote health andwellness for all.
Abbreviations
CABG coronary artery bypass graft
NHHR Native Hawaiian Health Research
NHOPI Native Hawaiians and other Pacific Islanders
AcknowledgmentsThis work was supported by the Center for Native and Pacific Health Disparities Research, Department of NativeHawaiian Health, John A. Burns School of Medicine, University of Hawai‘i at Manoa; The Myron Pinky ThompsonEndowed Chair (grant S21 MD 000228); the National Center on Minority Health and Health Disparities (grants P20MD000173 and R24 MD 001660); and the National Heart, Lung, and Blood Institute (grant U01HL 079163).
Mau et al. Page 7
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

REFERENCES1. Acton KJ, Burrows NR, Moore K, et al. Trends in diabetes prevalence among American Indian and
Alaska Native children, adolescents, and young adults. Am J Public Health 2002;92(9):1485–1490.[PubMed: 12197981]
2. Allison MA, Budoff MJ, Wong ND, et al. Prevalence of and risk factors for subclinical cardiovasculardisease in selected US Hispanic ethnic groups: the Multi-Ethnic Study of Atherosclerosis. Am JEpidemiol 2008;167(8):962–969. [PubMed: 18283034]
3. Burrows NR, Geiss LS, Engelgau MM, et al. Prevalence of diabetes among Native Americans andAlaska Natives, 1990–1997: an increasing burden. Diabetes Care 2000;23(12):1786–1790. [PubMed:11128353]
4. Egede LE, Dagogo-Jack S. Epidemiology of type 2 diabetes: focus on ethnic minorities. Med ClinNorth Am 2005;89(5):949–975. viii. [PubMed: 16129107]
5. Grandinetti A, Chang HK, Mau MK, et al. Prevalence of glucose intolerance among Native Hawaiiansin two rural communities. Native Hawaiian Health Research (NHHR) Project. Diabetes Care 1998;21(4):549–554. [PubMed: 9571341]
6. Johnson DB, Oyama N, LeMarchand L, et al. Native Hawaiians mortality, morbidity, and lifestyle:comparing data from 1982, 1990, and 2000. Pac Health Dialog 2004;11(2):120–130. [PubMed:16281689]
7. Mau MK, Grandinetti A, Arakaki RF, et al. The insulin resistance syndrome in native Hawaiians.Native Hawaiian Health Research (NHHR) Project. Diabetes Care 1997;20(9):1376–1380. [PubMed:9283783]
8. Revisions to the Standards for the Classification of Federal Data on Race and Ethnicity. Washington,DC: OMB Publications Office; 1997 [Accessed April 6, 2009]. Executive Office of the President,Office of Management and Budget, Office of Information and Regulatory Affairs.http://www.whitehouse.gov/omb/fedreg_1997standards/
9. Bushnell, OA. The Gifts of Civilization: Germs and Genocide in Hawaii. Honolulu, HI: University ofHawaii Press; 1993.
10. Fong M, Braun KL, Tsark JU. Improving Native Hawaiian health through community-basedparticipatory research. Cal J Health Promot 2003;1:136–148. special issue: Hawaii.
11. Kana’iaupuni, SM.; Malone, NJ.; Ishibashi, K. Income and Poverty Among Native Hawaiians:Summary of Ka Huaka’i Findings. (PASE report). Honolulu, HI: Policy Analysis and SystemEvaluation; 2005 [Accessed April 6, 2009].(http://www.ksbe.edu/spi/PDFS/Reports/Demography_Well-being/05_06_5.pdf
12. Salvail, FR.; Nguyen, D.; Liang, SL. 2008 State of Hawaii—By Demographic Characteristics.Behavioral Risk Factor Surveillance System. Honolulu, HI: Hawaii State Department of Health; 2008[Accessed April 6, 2009]. http://hawaii.gov/health/statistics/brfss/brfss/brfss2008/demo08.html
13. Grandinetti A, Kaholokula JK, Theriault AG, et al. Prevalence of diabetes and glucose intolerance inan ethnically diverse rural community of Hawaii. Ethn Dis 2007;17(2):250–255. [PubMed:17682354]
14. Salvail, FR.; Nguyen, D. 2006 State of Hawaii—By Demographic Characteristics. Behavioral RiskFactor Surveillance System. Honolulu, HI: Hawaii State Department of Health; 2006 [Accessed April6, 2009]. Have you ever been told by doctor that you have diabetes? State of Hawaii BRFSS 2006[table]. http://hawaii.gov/health/statistics/brfss/brfss/brfss2006/demo06.html
15. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Washington, DC:National Academies Press; 2003. Institute of Medicine, Committee on Understanding andEliminating Racial and Ethnic Disparities in Health Care, Board on Health Sciences Policy.
16. Novotny R, Davis J, Ross P, et al. Adiposity and blood pressure in a multiethnic population of womenin Hawaii. Ethn Health 1998;3(3):167–173. [PubMed: 9798115]
17. Sundaram AA, Ayala C, Greenlund KJ, et al. Differences in the prevalence of self-reported risk factorsfor coronary heart disease among American women by race/ethnicity and age: Behavioral Risk FactorSurveillance System. Am J Prev Med 2005;29(5 suppl 1):25–30. 2001. [PubMed: 16389122]
18. Grandinetti A, Chen R, Kaholokula JK, et al. Relationship of blood pressure with degree of Hawaiianancestry. Ethn Dis 2002;12(2):221–228. [PubMed: 12019931]
Mau et al. Page 8
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

19. Grandinetti A, Seifried SE, Chow DC, et al. Association between angiotensin-converting enzymegene polymorphisms and QT duration in a multiethnic population in Hawaii. Auton Neurosci2006;130(1–2):51–56. [PubMed: 16769256]
20. Verderber A, Castelfranco AM, Nishioka D, et al. Cardiovascular risk factors and cardiac surgeryoutcomes in a multiethnic sample of men and women. Am J Crit Care 1999;8(3):140–148. [PubMed:10228654]
21. Taira DA, Seto TB, Marciel C. Ethnic disparities in care following acute coronary syndromes amongAsian Americans and Pacific Islanders during the initial hospitalization. Cell Mol Biol (Noisy-le-Grand) 2001;47(7):1209–1215. [PubMed: 11838969]
22. Ezeamama AE, Viali S, Tuitele J, et al. The influence of socioeconomic factors on cardiovasculardisease risk factors in the context of economic development in the Samoan archipelago. Soc Sci Med2006;63(10):2533–2545. [PubMed: 16876925]
23. Grandinetti A, Keawe’aimoku Kaholokula J, Chang HK, et al. Relationship between plasma glucoseconcentrations and Native Hawaiian ancestry: the Native Hawaiian Health Research Project. Int JObes Relat Metab Disord 2002;26(6):778–782. [PubMed: 12037647]
24. King H, Rewers M. Global estimates for prevalence of diabetes mellitus and impaired glucosetolerance in adults. WHO Ad Hoc Diabetes Reporting Group. Diabetes Care 1993;16(1):157–177.[PubMed: 8123057]
25. Kaholokula JK, Haynes SN, Grandinetti A, et al. Ethnic differences in the relationship betweendepressive symptoms and health-related quality of life in people with type 2 diabetes. Ethn Health2006;11(1):59–80. [PubMed: 16338755]
26. Grandinetti A, Kaholokula JK, Crabbe KM, et al. Relationship between depressive symptoms anddiabetes among native Hawaiians. Psychoneuroendocrinology 2000;25(3):239–246. [PubMed:10737695]
27. Kaholokula JK, Haynes SN, Grandinetti A, et al. Biological, psychosocial, and sociodemographicvariables associated with depressive symptoms in persons with type 2 diabetes. J Behav Med 2003;26(5):435–458. [PubMed: 14593852]
28. Kim H, Park S, Grandinetti A, et al. Major dietary patterns, ethnicity, and prevalence of type 2 diabetesin rural Hawaii. Nutrition 2008;24(11–12):1065–1072. [PubMed: 18586461]
29. Mau MK, Glanz K, Severino R, et al. Mediators of lifestyle behavior change in Native Hawaiians:initial findings from the Native Hawaiian Diabetes Intervention Program. Diabetes Care 2001;24(10):1770–1775. [PubMed: 11574440]
30. Mau MK, West MR, Shara NM, et al. Epidemiologic and clinical factors associated with chronickidney disease among Asian Americans and Native Hawaiians. Ethn Health 2007;12(2):111–127.[PubMed: 17364897]
31. Silva JK, Kaholokula JK, Ratner R, et al. Ethnic differences in perinatal outcome of gestationaldiabetes mellitus. Diabetes Care 2006;29(9):2058–2063. [PubMed: 16936153]
32. Grandinetti A, Chang HK, Chen R, et al. Prevalence of overweight and central adiposity is associatedwith percentage of indigenous ancestry among native Hawaiians. Int J Obes Relat Metab Disord1999;23(7):733–737. [PubMed: 10454107]
33. Albright CL, Steffen A, Wilkens LR, et al. Body mass index in monoracial and multiracial adults:results from the Multiethnic Cohort Study. Ethn Dis 2007;17(2):268–273. [PubMed: 17682357]
34. Maskarinec G, Takata Y, Pagano I, et al. Trends and dietary determinants of overweight and obesityin a multiethnic population. Obesity (Silver Spring) 2006;14(4):717–726. [PubMed: 16741275]
35. Maskarinec G, Carlin L, Pagano I, et al. Lifestyle risk factors for chronic disease in a multiethnicpopulation: an analysis of two prospective studies over a 20-year period. Ethn Dis 2007;17(4):597–603. [PubMed: 18072366]
36. Mampilly CM, Yore MM, Maddock JE, et al. Prevalence of physical activity levels by ethnicityamong adults in Hawaii, BRFSS 2001. Hawaii Med J 2005;64(10):270–273. [PubMed: 16294701]
37. Boyd JK, Braun KL. Supports for and barriers to healthy living for Native Hawaiian young adultsenrolled in community colleges [electronic article]. Prev Chronic Dis 2007;4(4):A88. [PubMed:17875263]
Mau et al. Page 9
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

38. Elstad E, Tusiofo C, Rosen RK, et al. Living with ma’i suka: individual, familial, cultural, andenvironmental stress among patients with type 2 diabetes mellitus and their caregivers in AmericanSamoa [electronic article]. Prev Chronic Dis 2008;5(3):A79. [PubMed: 18558029]
39. Kaholokula JK, Saito E, Mau MK, et al. Pacific Islanders’ perspectives on heart failure management.Patient Educ Couns 2008;70(2):281–291. [PubMed: 18068939]
40. Kretzer K, Davis J, Easa D, et al. Self identity through ho’oponopono as adjunctive therapy forhypertension management. Ethn Dis 2007;17(4):624–628. [PubMed: 18072370]
41. Marsella, AJ.; Oliveira, J.; Plummer, CM., et al. Native Hawaiian (kanaka maoli) culture, mind, andwell-being. In: McCubbin, HI.; Thompson, EA.; Fromer, JE., editors. Resiliency in Ethnic MinorityFamilies: Native Immigrant American Families. Madison, WI: University of Wisconsin, Center forExcellence in Family Studies; 1995. p. 93-113.
42. Wong MM, Klingle RS, Price RK. Alcohol, tobacco, and other drug use among Asian American andPacific Islander adolescents in California and Hawaii. Addict Behav 2004;29(1):127–141. [PubMed:14667425]
43. Crabbe KM. Conceptions of depression: a Hawaiian perspective. Pac Health Dialog 1999;6(1):122–126.
44. Rezentes, WCIII. Ka Lama Kukui—Hawaiian Psychology: An Introduction. Honolulu, HI: ‘A’ali’iBooks; 1996.
45. Yeo KK, Beauvallet S, Mau MK, et al. Procedural success and complications following percutaneouscoronary interventions among Asians and Pacific Islanders. Clin Cardiol 2005;28(9):429–432.[PubMed: 16250266]
46. Chiem B, Nguyen V, Wu PL, et al. Cardiovascular risk factors among Chamorros [electronic article].BMC Public Health 2006;6:298. [PubMed: 17156462]
47. Taira DA, Gelber RP, Davis J, et al. Antihypertensive adherence and drug class among Asian PacificAmericans. Ethn Health 2007;12(3):265–281. [PubMed: 17454100]
48. Grandinetti A, Chang HK, Theriault A, et al. Metabolic syndrome in a multiethnic population in ruralHawaii. Ethn Dis 2005;15(2):233–237. [PubMed: 15825969]
49. Wu PL, Sadler GR, Nguyen V, et al. Diabetes management in San Diego’s Chamorro community.Diabetes Educ 2005;31(3):379–390. [PubMed: 15919638]
50. Beckham S, Bradley S, Washburn A, et al. Diabetes management: utilizing community health workersin a Hawaiian/Samoan population. J Health Care Poor Underserved 2008;19(2):416–427. [PubMed:18469413]
51. Kaholokula JK, Nacapoy AH, Grandinetti A, et al. Association between acculturation modes and type2 diabetes among Native Hawaiians. Diabetes Care 2008;31(4):698–700. [PubMed: 18202248]
52. Maskarinec G, Meng L, Kolonel L. Alcohol intake, body weight, and mortality in a multiethnicprospective cohort. Epidemiology 1998;9(6):654–661. [PubMed: 9799177]
53. Galanis DJ, McGarvey ST, Quested C, et al. Dietary intake of modernizing Samoans: implicationsfor risk of cardiovascular disease. J Am Diet Assoc 1999;99(2):184–190. [PubMed: 9972185]
54. McGarvey ST, Forrest W, Weeks DE, et al. Human leptin locus (LEP) alleles and BMI in Samoans.Int J Obes Relat Metab Disord 2002;26(6):783–788. [PubMed: 12037648]
55. Henderson KD, Goran MI, Kolonel LN, et al. Ethnic disparity in the relationship between obesityand plasma insulin-like growth factors: the Multiethnic Cohort. Cancer Epidemiol Biomarkers Prev2006;15(11):2298–2302. [PubMed: 17119061]
56. Howarth NC, Murphy SP, Wilkens LR, et al. Dietary energy density is associated with overweightstatus among 5 ethnic groups in the Multiethnic Cohort Study. J Nutr 2006;136(8):2243–2248.[PubMed: 16857848]
57. Dai F, Keighley ED, Sun G, et al. Genome-wide scan for adiposity-related phenotypes in adults fromAmerican Samoa. Int J Obes (Lond) 2007;31(12):1832–1842. [PubMed: 17621312]
58. Novotny R, Nabokov V, Derauf C, et al. BMI and waist circumference as indicators of health amongSamoan women. Obesity (Silver Spring) 2007;15(8):1913–1917. [PubMed: 17712106]
59. Maskarinec G, Aylward AG, Erber E, et al. Soy intake is related to a lower body mass index in adultwomen. Eur J Nutr 2008;47(3):138–144. [PubMed: 18427855]
Mau et al. Page 10
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1.Procedures used to review the literature on cardiometabolic health disparities among NativeHawaiians and other Pacific Islanders, January 1998–December 2008. Set A: inclusion ofNative Hawaiian, Hawaiian, Pacific Islander, Samoan, Tongan, Micronesian, New Zealand,Maori, Melanesia, Chamorro, Guamanian, Fijian, and Polynesian in an “OR” search termalong with the following racial/ethnic terms: minority, minorities, groups, ethnicity, andethnicities, defined as an “OR” search term. Set B: inequity, inequality, health disparities,health differences, cardiovascular, hypertension, heart, heart failure, heart disease, heartdisease risk factors, cardiac, cardiomyopathy, diabetes, syndrome X, metabolic syndrome,insulin resistance, glucose intolerance, prediabetes, cardiometabolic, obesity, adiposity,overweight, physical inactivity, physical activity, nutrition, diet, and smoking in combinationwith United States.
Mau et al. Page 11
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 2.Conceptual model of health and health-care disparities.
Mau et al. Page 12
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mau et al. Page 13
Tabl
e 1
Lite
ratu
re o
n C
ardi
ovas
cula
r Hea
lth D
ispa
ritie
s Am
ong
Nat
ive
Haw
aiia
ns a
nd O
ther
Pac
ific
Isla
nder
s, Ja
nuar
y 19
98–D
ecem
ber 2
008
Stud
y A
utho
rsan
dY
ear
(Ref
. No.
)Sa
mpl
e an
dN
o. o
f Sub
ject
s
% o
fT
otal
Sam
ple
Who
Wer
eN
HO
PI
Age
,ye
ars
Stud
y D
esig
nM
ain
Goa
l and
Out
com
es/F
indi
ngs
Lim
itatio
ns
Nov
otny
et a
l., 1
998
(16)
66 N
ativ
e H
awai
ian
wom
en o
ut o
f a to
tal m
ultie
thni
c s
ampl
e of
421
1625
–35
Obs
erva
tiona
l, cr
oss-
sect
iona
l, c
linic
al re
sear
ch sa
mpl
eEx
amin
e an
thro
pom
etric
var
iatio
ns b
etw
een
mul
tieth
nic
wom
en a
nd th
eir
rel
atio
n to
blo
od p
ress
ure
and
cho
lest
erol
.
Sam
ple b
ias;
rela
tivel
y sm
all s
tudy
.
Nat
ive
Haw
aiia
n w
omen
had
the
high
est
mea
sure
s of a
dipo
sity
. Cho
lest
erol
was
not
ass
ocia
ted
with
adi
posi
ty. B
lood
pre
ssur
e w
as a
ssoc
iate
d w
ith a
dipo
sity
but
did
not
var
y by
eth
nici
ty.
Ver
derb
er e
t al.,
199
9 (2
0)23
Pac
ific
Isla
nder
s out
of
a to
tal m
ultie
thni
c sa
mpl
e o
f 60
3840
–85
Obs
erva
tiona
l, cr
oss-
sect
iona
l, h
ospi
tal s
urge
ry sa
mpl
eD
escr
ibe
risk
fact
ors f
or c
ardi
ac d
isea
se a
nd p
ost-C
AB
G o
utco
mes
and
com
plic
atio
ns in
mul
tieth
nic
patie
nts.
Sam
ple
bias
(sin
gle
hosp
ital,
rela
tivel
y s
mal
l sam
ple)
. No
adju
stm
ent f
or p
hysi
cian
as c
ovar
iate
.N
o et
hnic
diff
eren
ces i
n po
stop
erat
ive
com
plic
atio
ns in
firs
t 20
hour
s. A
t 48
hou
rs p
ost-C
AB
G, P
acifi
c Is
land
ers
req
uire
d si
gnifi
cant
ly m
ore
care
than
Jap
anes
e (P
< 0
.01)
.
Taira
et a
l., 2
001
(21)
361
Nat
ive
Haw
aiia
ns o
ut o
f a
tota
l mul
tieth
nic
sam
ple
of 2
,962
11≥1
8O
bser
vatio
nal,
cros
s-se
ctio
nal,
adm
inis
trativ
e da
taba
se s
ampl
e
Exam
ine
diff
eren
ces i
n re
vasc
ular
izat
ion
and
mor
talit
y ra
tes f
ollo
win
g ac
ute
cor
onar
y sy
ndro
me
in a
mul
tieth
nic
pat
ient
pop
ulat
ion.
Cro
ss-s
ectio
nal;
clai
ms d
ata
fro
m si
ngle
hea
lth in
sure
r.
Ethn
ic d
iffer
ence
s in
type
s of p
roce
dure
s r
ecei
ved
wer
e si
gnifi
cant
onl
y fo
r men
. N
ativ
e H
awai
ian
men
wer
e le
ss li
kely
to r
ecei
ve p
ercu
tane
ous c
oron
ary
int
erve
ntio
n (a
djus
ted
OR
= 0
.51,
95%
CI:
0.34
, 0.7
5) a
nd m
ore
likel
y to
rece
ive
CA
BG
(adj
uste
d O
R =
1.8
, 95%
CI:
1.2,
2.7
) tha
n w
hite
s. N
o si
gnifi
cant
eth
nic
diff
eren
ces i
n w
omen
.
Gra
ndin
etti
et a
l., 2
002
(18)
572
Nat
ive
Haw
aiia
ns;
non
preg
nant
100
≥30
Obs
erva
tiona
l, re
trosp
ectiv
e c
ohor
t, po
pula
tion-
base
d s
ampl
e
Exam
ine
degr
ee o
f Haw
aiia
n an
cest
ry a
nd b
lood
pre
ssur
e an
d re
latio
n to
oth
er c
ovar
iate
s.
Perc
enta
ge o
f Haw
aiia
n an
cest
ry w
as se
lf-re
porte
d; c
ross
-sec
tiona
l d
esig
n; sa
mpl
e po
pula
tion
only
from
rur
al lo
catio
n. A
sses
smen
t of
ade
quat
e bl
ood
pres
sure
con
trol
with
med
icat
ions
not
des
crib
ed.
Adj
uste
d pr
eval
ence
of h
yper
tens
ion
inc
reas
ed w
ith d
egre
e of
Haw
aiia
n a
nces
try, e
xcep
t for
100
% H
awai
ian
anc
estry
. Haw
aiia
n an
cest
ry w
as s
igni
fican
tly a
ssoc
iate
d w
ith sy
stol
ic a
nd d
iast
olic
blo
od p
ress
ure
(P <
0.0
001)
. A
fter a
djus
tmen
t for
all
sign
ifica
nt
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mau et al. Page 14
Stud
y A
utho
rsan
dY
ear
(Ref
. No.
)Sa
mpl
e an
dN
o. o
f Sub
ject
s
% o
fT
otal
Sam
ple
Who
Wer
eN
HO
PI
Age
,ye
ars
Stud
y D
esig
nM
ain
Goa
l and
Out
com
es/F
indi
ngs
Lim
itatio
ns
cov
aria
tes,
only
dia
stol
ic b
lood
pre
ssur
e w
as a
ssoc
iate
d w
ith H
awai
ian
ance
stry
(P
= 0.
008)
.
Sund
aram
et a
l., 2
005
(17)
510
NH
OPI
wom
en o
ut o
f a
tota
l mul
tieth
nic
sam
ple
of 1
20,0
35
<1≥1
8O
bser
vatio
nal,
cros
s-se
ctio
nal
tel
epho
ne su
rvey
, 200
1 B
RFS
S
Det
erm
ine
prev
alen
ce o
f car
diov
ascu
lar
dis
ease
risk
fact
ors a
mon
g m
ultie
thni
c w
omen
in 2
001
BR
FSS.
All
data
wer
e se
lf-re
porte
d. C
ross
- s
ectio
nal;
rela
tivel
y sm
all s
ampl
e c
ompa
red
with
oth
er e
thni
cgr
oups
.N
HO
PI w
omen
had
seco
nd h
ighe
st p
reva
lenc
e of
hyp
erte
nsio
n at
33.
7% (
age-
adju
sted
) and
hig
hest
pre
vale
nce
of h
igh
chol
este
rol (
23.9
%).
Yeo
et a
l., 2
005
(45)
377
Paci
fic Is
land
ers o
ut o
f a
tota
l mul
tieth
nic
sam
ple
of 2
,598
14≥1
8O
bser
vatio
nal,
case
-con
trol,
hos
pita
l adm
inis
trativ
e d
atab
ase
sam
ple
Exam
ine
ethn
ic d
iffer
ence
s in
per
cuta
neou
s cor
onar
y in
terv
entio
n s
ucce
ss a
nd/o
r com
plic
atio
ns in
hos
pita
lized
pat
ient
s.
Sam
ple
bias
(rec
ruite
d fr
om a
sing
le h
ospi
tal).
Cro
ss-s
ectio
nal d
ata;
no
lon
g-te
rm o
utco
mes
ava
ilabl
e.
Des
pite
hig
her r
ates
of d
iabe
tes,
hyp
erte
nsio
n, o
besi
ty, a
nd re
nal f
ailu
re in
NH
OPI
, the
re w
as n
o di
ffer
ence
in p
ercu
tane
ous c
oron
ary
inte
rven
tion
com
plic
atio
ns c
ompa
red
with
whi
tes o
r J
apan
ese.
Chi
em e
t al.,
200
6 (4
6)22
8 C
ham
orro
s10
0≥1
8O
bser
vatio
nal,
cros
s- s
ectio
nal t
elep
hone
surv
ey,
com
mun
ity a
dmin
istra
tive
dat
abas
e sa
mpl
e
Des
crib
e ca
rdio
vasc
ular
dis
ease
risk
fac
tors
in C
ham
orro
com
mun
ity to
aid
in d
evel
opin
g pr
ogra
ms.
Sam
ple
bias
(rec
ruite
d fr
omco
mm
unity
dat
abas
e). N
o ad
just
men
t for
cov
aria
tes.
Cro
ss-s
ectio
nal d
ata.
Sel
f-re
porte
d he
alth
risk
fact
ors.
Cru
de fr
eque
ncie
s of h
yper
tens
ion,
dia
bete
s, hy
perli
pide
mia
, and
phy
sica
l i
nact
ivity
wer
e hi
gher
in C
ham
orro
s tha
n i
n U
S w
hite
s. C
ham
orro
wom
en w
ere
mor
e lik
ely
to h
ave
hype
rtens
ion
and
dia
bete
s. M
en w
ere
mor
e lik
ely
to h
ave
ele
vate
d bo
dy m
ass i
ndex
and
cho
lest
erol
.
Ezea
mam
a et
al.,
200
6 (2
2)1,
289
Sam
oans
(Am
eric
an a
nd W
este
rn S
amoa
n)10
025
–58
Obs
erva
tiona
l, pr
ospe
ctiv
e c
ohor
t, po
pula
tion-
base
d s
ampl
e
Inve
stig
ate
cros
s-se
ctio
nal a
nd p
rosp
ectiv
e as
soci
atio
ns b
etw
een
SES
and
car
diov
ascu
lar d
isea
se ri
sk fa
ctor
s a
nd p
redi
ct th
e pr
obab
ility
of r
isk
fact
ors
by
SES
leve
l bet
wee
n A
mer
ican
Sam
oa a
nd S
amoa
.
Rel
ativ
ely
larg
e sa
mpl
e of
Sam
oan
par
ticip
ants
; sub
ject
s wer
eyo
unge
r a
nd th
us th
ere w
ere f
ewer
case
s of
car
diov
ascu
lar d
isea
se ri
sk fa
ctor
s. M
en lo
st to
follo
w-u
p in
bot
h l
ocat
ions
wer
e m
ore
likel
y to
be
em
ploy
ed in
the
wag
e-la
bor
mar
ket
and
may
hav
e in
trodu
ced
attri
tion
bia
s.
Hig
h SE
S w
as a
ssoc
iate
d w
ith in
crea
sed
odd
s of r
isk
fact
ors i
n le
ss d
evel
oped
Wes
tern
Sam
oa a
nd d
ecre
ased
odd
s of
ris
k fa
ctor
s in
mor
e de
velo
ped
Am
eric
an S
amoa
. Inv
erse
ass
ocia
tion
betw
een
SES
and
risk
fact
ors i
n W
este
rn S
amoa
vs.
Am
eric
an S
amoa
is a
ttrib
utab
le to
het
erog
enei
ty a
cros
s the
Sam
oan
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mau et al. Page 15
Stud
y A
utho
rsan
dY
ear
(Ref
. No.
)Sa
mpl
e an
dN
o. o
f Sub
ject
s
% o
fT
otal
Sam
ple
Who
Wer
eN
HO
PI
Age
,ye
ars
Stud
y D
esig
nM
ain
Goa
l and
Out
com
es/F
indi
ngs
Lim
itatio
ns
Isl
ands
in sp
ecifi
c ex
posu
res t
o e
cono
mic
dev
elop
men
t and
nat
ural
his
tory
of i
ndiv
idua
l ris
k fa
ctor
s.
Gra
ndin
etti
et a
l., 2
006
(19)
185
Nat
ive
Haw
aiia
ns o
ut o
f a
tota
l mul
tieth
nic
sam
ple
of 5
88; n
onpr
egna
nt
31≥3
0O
bser
vatio
nal,
retro
spec
tive
coh
ort;
rand
omly
sele
cted
nes
ted
stud
y of
pop
ulat
ion-
bas
ed sa
mpl
e
Exam
ine
angi
oten
sin-
conv
ertin
g e
nzym
e ge
ne p
olym
orph
ism
s and
inc
reas
ed Q
-Tc
(ass
ocia
ted
with
hea
rt d
isea
se) b
etw
een
ethn
ic g
roup
s.
Cro
ss-s
ectio
nal p
reva
lenc
e C
ases
may
lead
to b
ias.
Incr
ease
d Q
-Tc
was
hig
hest
am
ong
per
sons
with
the
ACE
II g
enot
ype.
AC
E II
gen
otyp
e w
as h
ighe
r in
Nat
ive
Haw
aiia
ns (
50.3
%) t
han
in w
hite
s (21
%).
Afte
r a
djus
tmen
t, pr
eval
ence
of i
ncre
ased
Q-
Tc
was
sign
ifica
ntly
ass
ocia
ted
with
AC
E I
I gen
otyp
e in
depe
nden
tly o
f eth
nici
ty (
P <
0.01
).
Kre
tzer
et a
l., 2
007
(40)
15 N
ativ
e H
awai
ians
out
of
a to
tal m
ultie
thni
c sa
mpl
e o
f 23
65≥3
0Q
uasi
-exp
erim
enta
l (no
con
trol g
roup
), pr
e-po
st i
nter
vent
ion,
com
mun
ity s
ampl
e
Eval
uate
whe
ther
a c
lass
on
self-
iden
tity
via
ho‘
opon
opon
o w
ould
impr
ove
high
blo
od p
ress
ure.
No
cont
rol g
roup
, sm
all s
ampl
esi
ze,
and
pot
entia
lly b
iase
d sa
mpl
e. N
o a
djus
tmen
t for
med
icat
ion
chan
ges.
Ho‘
opon
opon
o in
terv
entio
n (4
-hou
r g
roup
cla
ss) r
educ
ed m
ean
syst
olic
and
dia
stol
ic b
lood
pre
ssur
e, w
hich
was
sus
tain
ed fo
r 2 m
onth
s afte
r int
erve
ntio
n. R
esul
ts fo
r the
15
Nat
ive
Haw
aiia
ns w
ere
agg
rega
ted
with
thos
e fo
r the
rem
aini
ng 8
oth
er n
on-H
awai
ian
parti
cipa
nts.
Taira
et a
l., 2
007
(47
)3,
746
Nat
ive
Haw
aiia
ns o
ut o
f a to
tal m
ultie
thni
c s
ampl
e of
28,
395
13≥1
8O
bser
vatio
nal,
cros
s- s
ectio
nal;
heal
th in
sura
nce
adm
inis
trativ
e da
taba
se s
ampl
e
Exam
ine
fact
ors a
ssoc
iate
d w
ith a
ntih
yper
tens
ive
med
icat
ion
adhe
renc
e w
ithin
a m
ultie
thni
c pa
tient
pop
ulat
ion
usi
ng a
dmin
istra
tive
clai
ms d
ata.
Cro
ss-s
ectio
nal c
laim
s dat
a fr
om a
sing
le h
ealth
insu
ranc
e pl
an.
Pat
ient
adh
eren
ce w
as m
easu
red
by fill
ing
of p
resc
riptio
ns, n
ot a
tpa
tient
lev
el. L
ack
of in
form
atio
n on
impa
ct o
f com
orbi
d co
nditi
ons o
n m
edic
atio
n ad
here
nce.
Ove
rall
adhe
renc
e in
all
ethn
ic g
roup
s w
as le
ss th
an 6
5%. A
fter a
djus
tmen
t, N
ativ
e H
awai
ians
wer
e le
ss li
kely
to a
dher
e th
an w
hite
s (O
R =
0.8
4, 9
5% C
I: 0
.78,
0.9
1), a
nd th
is w
as c
onsi
sten
t a
cros
s the
rape
utic
cla
sses
. Oth
er p
atie
nt f
acto
rs a
ssoc
iate
d w
ith lo
wer
adh
eren
ce:
you
nger
age
, hig
her m
orbi
dity
, and
his
tory
of h
eart
dise
ase.
See
ing
a p
hysi
cian
of t
he sa
me
ethn
icity
did
not
im
prov
e ad
here
nce.
Kah
olok
ula
et a
l., 2
008
(39)
36 N
HO
PI a
nd fa
mily
car
egiv
ers
100
≥18
Focu
s gro
up, c
omm
unity
sam
ple
Iden
tify
heal
th b
elie
fs, a
ttitu
des,
pra
ctic
es, a
nd so
cial
and
fam
ily re
latio
ns i
mpo
rtant
in h
eart
failu
re tr
eatm
ent
am
ong
NH
OPI
.
Smal
l sam
ple
size
, and
onl
y 30
% w
ere
hear
t fai
lure
pat
ient
s. Q
ualit
ativ
e st
udy
desi
gn w
ith p
oten
tially
subj
ectiv
e re
spon
ses.
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mau et al. Page 16
Stud
y A
utho
rsan
dY
ear
(Ref
. No.
)Sa
mpl
e an
dN
o. o
f Sub
ject
s
% o
fT
otal
Sam
ple
Who
Wer
eN
HO
PI
Age
,ye
ars
Stud
y D
esig
nM
ain
Goa
l and
Out
com
es/F
indi
ngs
Lim
itatio
ns
Nat
ive
Haw
aiia
ns w
ith h
eart
failu
re r
epor
ted
copi
ng e
xper
ienc
es o
f den
ial o
f i
llnes
s, ho
pele
ssne
ss, a
nd d
espa
ir an
d r
elie
d on
spiri
tual
/relig
ious
bel
iefs
for
sup
port.
Sam
oans
pre
ferr
ed b
eing
tre
ated
by
phys
icia
ns, w
hile
Nat
ive
Haw
aiia
ns p
refe
rred
trad
ition
al h
eale
rs.
Bar
riers
to h
eart
failu
re c
are
incl
ude
poor
kno
wle
dge,
lack
of t
rust
of t
he p
hysi
cian
, a
poo
r pat
ient
-phy
sici
an re
latio
nshi
p, f
inan
ces,
diet
ary
chan
ges,
and
incr
ease
d d
eman
ds o
n tim
e.
Abb
revi
atio
ns: A
CE
II, a
ngio
tens
in-c
onve
rting
enz
yme
inse
rtion
/inse
rtion
; BR
FSS,
Beh
avio
ral R
isk
Fact
or S
urve
illan
ce S
yste
m; C
AB
G, c
oron
ary
arte
ry b
ypas
s gra
ft; C
I, co
nfid
ence
inte
rval
; NH
OPI
, Nat
ive
Haw
aiia
ns a
nd o
ther
Pac
ific
Isla
nder
s; O
R, o
dds r
atio
; Q-T
c, c
orre
cted
Q–T
inte
rval
; SES
, soc
ioec
onom
ic st
atus
.
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mau et al. Page 17
Tabl
e 2
Lite
ratu
re o
n D
iabe
tes H
ealth
Dis
parit
ies A
mon
g N
ativ
e H
awai
ians
and
Oth
er P
acifi
c Is
land
ers,
Janu
ary
1998
–Dec
embe
r 200
8
Stud
y A
utho
rs a
ndY
ear
(Ref
. No.
)Sa
mpl
e an
dN
o. o
f Sub
ject
s%
of T
otal
Sam
ple
Who
Wer
e N
HO
PIA
ge,
year
sSt
udy
Des
ign
Mai
n G
oal a
ndO
utco
mes
/Fin
ding
sL
imita
tions
Gra
ndin
etti
et a
l., 1
998
(5)
574
Nat
ive
Haw
aiia
ns fr
om 2
rur
al c
omm
uniti
es in
Haw
ai‘i;
non
preg
nant
100
≥30
Obs
erva
tiona
l, re
trosp
ectiv
e c
ohor
t, po
pula
tion-
base
d s
ampl
e
To e
stim
ate
prev
alen
ces o
f typ
e 2
dia
bete
s and
impa
ired
gluc
ose
tol
eran
ce.
Cro
ss-s
ectio
nal;
self-
repo
rted
anc
estry
, con
tribu
ting
to p
ossi
ble
mis
clas
sific
atio
n.
Prev
alen
ce o
f im
paire
d gl
ucos
e t
oler
ance
was
16%
; dia
bete
s, 20
%.
Pre
vale
nce
of im
paire
d gl
ucos
e t
oler
ance
was
sign
ifica
ntly
hig
her i
n w
omen
and
sign
ifica
ntly
ass
ocia
ted
with
bod
y m
ass i
ndex
, wai
st c
ircum
fere
nce,
and
wai
st-to
-hip
ratio
. A
ge-a
djus
ted
prev
alen
ce o
f dia
bete
s w
as 4
tim
es h
ighe
r tha
n in
the
Sec
ond
Nat
iona
l Hea
lth a
nd N
utrit
ion
Exam
inat
ion
Surv
ey p
opul
atio
n.
Gra
ndin
etti
et a
l., 2
000
(26)
581
Nat
ive
Haw
aiia
ns fr
om 2
rur
al c
omm
uniti
es in
Haw
ai‘i;
non
preg
nant
100
≥30
Obs
erva
tiona
l, re
trosp
ectiv
e c
ohor
t, po
pula
tion-
base
d a
mpl
e
To e
xam
ine
the
asso
ciat
ion
betw
een
dia
bete
s and
CES
-D d
epre
ssiv
e s
ympt
oms.
Cro
ss-s
ectio
nal d
esig
n; th
us, t
he t
empo
ral r
elat
ion
betw
een
gly
cem
ic c
ontro
l and
CES
-D d
epre
ssiv
e sy
mpt
oms c
ould
not
be
dete
rmin
ed.
Am
ong
parti
cipa
nts r
epor
ting
a pr
ior
his
tory
of d
iabe
tes,
both
mea
n C
ES-D
sco
re a
nd d
epre
ssiv
e sy
mpt
om p
reva
lenc
e w
ere
sign
ifica
ntly
hig
her
tha
n in
par
ticip
ants
with
no
prio
r h
isto
ry o
f chr
onic
illn
ess,
afte
r a
djus
tmen
t for
age
and
soci
al su
ppor
t. H
igh
hem
oglo
bin
A1c
leve
l (≥7
%) w
as a
lso
asso
ciat
ed w
ith h
ighe
r p
reva
lenc
e of
CES
-D-a
sses
sed
dep
ress
ive
sym
ptom
s. R
esul
ts s
ugge
st th
at h
yper
glyc
emia
may
exp
lain
the
high
pre
vale
nce
of d
epre
ssiv
e sy
mpt
oms a
mon
g p
artic
ipan
ts w
ith k
now
n an
d ne
wly
ide
ntifi
ed d
iabe
tes.
Mau
et a
l., 2
001
(29)
147
Nat
ive
Haw
aiia
ns w
ith d
iabe
tes o
r met
abol
ic s
yndr
ome
and
thei
r ‘oh
ana
(fa
mily
) sup
port
pers
on
100
≥30
Qua
si-e
xper
imen
tal,
non
rand
omiz
ed, c
ontro
lled
tria
l; su
bjec
ts re
crui
ted
from
pop
ulat
ion-
base
d sa
mpl
e
To e
xam
ine
asso
ciat
ion
of st
age
of c
hang
e w
ith d
iet a
nd e
xerc
ise
in r
espo
nse
to li
fest
yle
inte
rven
tion.
Non
rand
omiz
ed in
terv
entio
n; l
ack
of tr
ue c
ontro
l gro
up.
Stag
e of
cha
nge
was
sign
ifica
ntly
ass
ocia
ted
with
pos
itive
die
tary
and
exe
rcis
e be
havi
ors.
Parti
cipa
nts
in
the
fam
ily su
ppor
t int
erve
ntio
n g
roup
wer
e m
ore
likel
y to
adv
ance
fro
m p
re-a
ctio
n to
act
ion/
mai
nten
ance
reg
ardi
ng fa
t int
ake
and
phys
ical
act
ivity
than
the
stan
dard
inte
rven
tion
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mau et al. Page 18
Stud
y A
utho
rs a
ndY
ear
(Ref
. No.
)Sa
mpl
e an
dN
o. o
f Sub
ject
s%
of T
otal
Sam
ple
Who
Wer
e N
HO
PIA
ge,
year
sSt
udy
Des
ign
Mai
n G
oal a
ndO
utco
mes
/Fin
ding
sL
imita
tions
gro
up.
Gra
ndin
etti
et a
l., 2
002
(18)
578
Nat
ive
Haw
aiia
ns fr
om 2
rur
al c
omm
uniti
es in
Haw
ai‘i;
non
preg
nant
100
≥30
Obs
erva
tiona
l, re
trosp
ectiv
e c
ohor
t, po
pula
tion-
base
d s
ampl
e
To in
vest
igat
e th
e re
latio
n be
twee
n g
luco
se a
nd p
erce
ntag
e of
Haw
aiia
n b
lood
qua
ntum
.
Cro
ss-s
ectio
nal s
urve
y; se
lf- r
epor
ted
ance
stry
, con
tribu
ting
to p
ossi
ble
mis
clas
sific
atio
n; se
lf- r
epor
ted
lifes
tyle
beh
avio
urs
Incr
ease
d H
awai
ian
bloo
d qu
antu
m w
as s
igni
fican
tly a
ssoc
iate
d w
ith in
crea
sed
fas
ting
gluc
ose
leve
l, bo
dy m
ass
ind
ex, w
aist
-to-h
ip ra
tio, a
nd a
ge. F
ull
Haw
aiia
ns h
ad h
ighe
r glu
cose
con
cent
ratio
ns th
an p
art-H
awai
ians
afte
r adj
ustm
ent f
or a
ge, s
ex, b
ody
mas
s ind
ex, a
nd w
aist
-to-h
ip ra
tio.
Kah
olok
ula
et a
l., 2
003
(27)
59 N
ativ
e H
awai
ians
out
of
a to
tal m
ultie
thni
c sa
mpl
e of
141
; non
preg
nant
41≥3
0O
bser
vatio
nal,
nest
ed c
ase
stu
dy fr
om a
pop
ulat
ion-
bas
ed sa
mpl
e
To e
xam
ine
corr
elat
ions
bet
wee
n g
lyce
mic
stat
us a
nd h
ealth
-rel
ated
qua
lity
of li
fe a
nd d
epre
ssiv
e s
ympt
oms.
Lim
ited
gene
raliz
abili
ty; l
ittle
var
iabi
lity
in b
ody
mas
s ind
ex a
nd w
aist
-to-h
ip ra
tio.
No
corr
elat
ion
betw
een
depr
essi
ve s
ympt
oms a
nd g
lyce
mic
stat
us w
as o
bser
ved.
Hea
lth-r
elat
ed q
ualit
y of
life
had
the
grea
test
mag
nitu
de o
f eff
ect
on
depr
essi
ve sy
mpt
oms i
n pe
ople
with
dia
bete
s com
pare
d w
ith g
lyce
mic
sta
tus a
nd k
now
ledg
e of
dia
bete
s d
iagn
osis
. Rel
atio
n be
twee
n d
epre
ssiv
e sy
mpt
oms a
nd h
ealth
- r
elat
ed q
ualit
y of
life
was
influ
ence
d by
gly
cem
ic st
atus
, sex
, edu
catio
n, m
arita
l sta
tus,
and
soci
al su
ppor
t.
Gra
ndin
etti
et a
l., 2
005
(48)
510
Nat
ive
Haw
aiia
ns o
ut o
f a
tota
l mul
tieth
nic
sam
ple
of 1
,447
; non
preg
nant
35≥3
0O
bser
vatio
nal,
retro
spec
tive
coh
ort,
popu
latio
n-ba
sed
sam
ple
To e
stim
ate
the
prev
alen
ce o
f met
abol
ic s
yndr
ome.
Cro
ss-s
ectio
nal
Prev
alen
ce o
f met
abol
ic sy
ndro
me
was
sig
nific
antly
hig
her a
mon
g N
ativ
e H
awai
ians
and
all
othe
r min
ority
eth
nic
gro
ups t
han
amon
g C
auca
sian
s. P
reva
lenc
es w
ere
sim
ilar i
n al
l non
- C
auca
sian
gro
ups.
Prev
alen
ce o
f a
bdom
inal
obe
sity
and
low
hig
h d
ensi
ty li
popr
otei
n ch
oles
tero
l was
hig
hest
in N
ativ
e H
awai
ians
.
Wu
et a
l., 2
005
(49)
228
Cha
mor
ros i
n Sa
n D
iego
, Cal
iforn
ia10
0≥1
8O
bser
vatio
nal,
cros
s- s
ectio
nal t
elep
hone
surv
ey,
adm
inis
trativ
e da
taba
se
To a
sses
s dia
bete
s ris
k s
tatu
s, in
cide
nce,
and
mor
bidi
ty.
Dat
a w
ere
popu
latio
n- a
nd g
eogr
aphy
-spe
cific
and
may
not
be
gene
raliz
able
. Sel
f-re
porte
d d
ata.
Dia
bete
s pre
vale
nce
was
16.
2%; 6
0% o
f r
espo
nden
ts w
ith d
iabe
tes w
ere
obe
se a
s com
pare
d w
ith 2
1% o
f tho
se w
ithou
t dia
bete
s. R
espo
nden
ts w
ithou
t dia
bete
s rep
orte
d m
ore
days
of m
oder
ate
phys
ical
act
ivity
than
tho
se w
ith d
iabe
tes.
Mor
e th
an h
alf o
f
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mau et al. Page 19
Stud
y A
utho
rs a
ndY
ear
(Ref
. No.
)Sa
mpl
e an
dN
o. o
f Sub
ject
s%
of T
otal
Sam
ple
Who
Wer
e N
HO
PIA
ge,
year
sSt
udy
Des
ign
Mai
n G
oal a
ndO
utco
mes
/Fin
ding
sL
imita
tions
all
men
and
wom
en re
porte
d c
onsu
min
g le
ss th
an th
e r
ecom
men
ded
5 or
mor
e fr
uits
and
veg
etab
les p
er d
ay. P
reva
lenc
e of
hig
h bl
ood
pres
sure
was
42.
5%,
hig
her t
han
the
natio
nwid
e 20
03 B
ehav
iora
l Ris
k Fa
ctor
Sur
veill
ance
Sys
tem
pre
vale
nce
of 2
4.8%
.
Kah
olok
ula
et a
l., 2
006
(25)
80 N
ativ
e H
awai
ians
out
of
a m
ultie
thni
c to
tal s
ampl
e of
190
; non
preg
nant
, with
dia
bete
s
50≥3
0O
bser
vatio
nal,
nest
ed c
ase
stu
dy fr
om p
opul
atio
n- b
ased
sam
ple
To e
xam
ine
rela
tion
betw
een
dep
ress
ive
sym
ptom
s and
asp
ects
of h
ealth
-rel
ated
qua
lity
of li
fe i
n ty
pe 2
dia
bete
s.
Cro
ss-s
ectio
nal s
urve
y, s
mal
l sam
ple
size
s.
Ethn
icity
mod
erat
ed th
e r
elat
ion
betw
een
depr
essi
ve s
ympt
oms a
nd q
ualit
y-of
-life
asp
ects
of p
hysi
cal a
nd ro
le-e
mot
iona
l f
unct
ioni
ng, b
odily
pai
n, v
italit
y, a
nd g
ener
al h
ealth
.
Silv
a et
al.,
200
6 (3
1)61
4 N
HO
PI w
omen
out
of
a m
ultie
thni
c to
tal s
ampl
e of
2,1
55 w
omen
28≥1
8O
bser
vatio
nal,
retro
spec
tive
coh
ort,
med
ical
-rig
ht-
bas
ed sa
mpl
e
To e
xam
ine
ethn
ic d
iffer
ence
s in
per
inat
al o
utco
mes
am
ong
wom
en w
ith g
esta
tiona
l dia
bete
s.
Ret
rosp
ectiv
e st
udy;
eth
nici
ty w
as s
elf-
repo
rted.
Bei
ng N
HO
PI w
as a
sign
ifica
nt p
redi
ctor
of f
etal
mac
roso
mia
. Hig
her
per
cent
age
of N
HO
PI w
omen
requ
ired
ins
ulin
dur
ing
preg
nanc
y an
d be
fore
20
wee
ks’ g
esta
tion,
sugg
estin
g th
at t
here
may
be
a la
rger
subs
et o
f NH
OPI
wom
en w
ith p
reex
istin
g un
diag
nose
d d
iabe
tes.
Gra
ndin
etti
et a
l., 2
007
(13)
510
Nat
ive
Haw
aiia
ns o
ut o
f a
tota
l mul
tieth
nic
sam
ple
of 1
,452
; non
preg
nant
35≥3
0O
bser
vatio
nal,
retro
spec
tive
coh
ort,
popu
latio
n-ba
sed
sam
ple
To a
sses
s pre
vale
nces
of d
iabe
tes a
nd g
luco
se in
tole
ranc
e.C
ross
-sec
tiona
l; se
lf-re
porte
d l
ifest
yle
beha
vior
s.
Thre
efol
d hi
gher
pre
vale
nce
of d
iabe
tes
am
ong
Asi
an a
nd N
ativ
e H
awai
ian
gro
ups t
han
amon
g C
auca
sian
s; d
iabe
tes p
reva
lenc
es w
ere
sim
ilar
acr
oss n
on-C
auca
sian
eth
nic
grou
ps d
espi
te d
iffer
ence
s in
body
mas
s i
ndex
.
Mau
et a
l., 2
007
(32
)19
6 N
ativ
e H
awai
ians
out
of a
tota
l mul
tieth
nic
sam
ple
of 7
93
25≥1
8O
bser
vatio
nal,
cros
s- s
ectio
nal,
com
mun
ity c
lust
ered
sam
ple
To e
xam
ine
asso
ciat
ions
bet
wee
n f
acto
rs a
ssoc
iate
d w
ith c
hron
ic k
idne
y d
isea
se.
Cro
ss-s
ectio
nal;
com
mun
ity sa
mpl
e m
ay h
ave
been
bia
sed.
Chr
onic
kid
ney
dise
ase
was
hig
hest
am
ong
Nat
ive
Haw
aiia
ns. D
iabe
tes,
hyp
erte
nsio
n, a
nd lo
wer
edu
catio
n w
ere
sign
ifica
ntly
ass
ocia
ted
with
inc
reas
ed c
hron
ic k
idne
y di
seas
e in
Nat
ive
Haw
aiia
ns.
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mau et al. Page 20
Stud
y A
utho
rs a
ndY
ear
(Ref
. No.
)Sa
mpl
e an
dN
o. o
f Sub
ject
s%
of T
otal
Sam
ple
Who
Wer
e N
HO
PIA
ge,
year
sSt
udy
Des
ign
Mai
n G
oal a
ndO
utco
mes
/Fin
ding
sL
imita
tions
Bec
kham
et a
l., 2
008
(50)
78 N
ativ
e H
awai
ians
, S
amoa
ns, a
nd T
onga
ns o
ut o
f a to
tal s
ampl
e of
116
dia
bete
s clin
ic p
atie
nts
67≥1
8Q
uasi
-exp
erim
enta
l, re
fusa
l c
ontro
l gro
up, p
re-p
ost
int
erve
ntio
n w
ith la
ck o
f c
ontro
l for
num
ber o
f vis
its,
clin
ic sa
mpl
e
To e
xam
ine
the
effe
ctiv
enes
s of a
cul
tura
lly ta
ilore
d di
abet
es m
anag
emen
t pro
gram
del
iver
ed b
y c
omm
unity
hea
lth w
orke
rs, u
sing
int
erve
ntio
n re
fuse
rs a
s the
com
paris
on g
roup
.
Smal
l sam
ple
size
, pre
-pos
t stu
dy d
esig
n, b
iase
d sa
mpl
e w
ithou
t tru
e c
ontro
l gro
up. 4
2% o
f the
con
trol
gro
up v
s. 10
% o
f the
inte
rven
tion
gro
up w
as lo
st to
follo
w-u
p. I
nter
vent
ion
grou
p re
ceiv
ed m
ore
vis
its th
an c
ontro
ls.
72 o
f 80
parti
cipa
nts i
n th
e co
mm
unity
- h
ealth
-wor
ker-
deliv
ered
inte
rven
tion
had
a p
ostin
terv
entio
n de
crea
se in
hem
oglo
bin
A1c
leve
l of 2
.2%
(SD
, 1
.8),
as c
ompa
red
with
21
of 3
6 p
artic
ipan
ts w
ho d
eclin
ed c
omm
unity
hea
lth w
orke
r int
erve
ntio
n, w
ho h
ad a
0.2
% (S
D, 1
.5) d
ecre
ase
in h
emog
lobi
n A
1c.
Elst
ad e
t al.,
200
8 (3
8)64
Sam
oans
(35
with
dia
bete
s and
29
care
give
rs)
100
≥18
Focu
s gro
ups,
com
mun
ity s
ampl
eTo
stud
y pe
rcep
tions
of d
iabe
tes t
o d
esig
n a
cultu
rally
app
ropr
iate
pro
gram
.
Smal
l sam
ple
size
; foc
us g
roup
s w
ere
mix
ed w
ith p
erso
ns w
ith d
iabe
tes a
nd c
areg
iver
s, w
hich
may
hav
e bi
ased
resp
onse
s.A
mer
ican
Sam
oans
with
type
2 d
iabe
tes
exp
erie
nced
mul
tiple
type
s of s
tress
. E
nviro
nmen
tal a
nd fa
mili
al st
ress
wor
sene
d th
eir g
luco
se le
vels
. D
espi
te th
e ef
fect
s of f
amily
stre
ss o
n d
iabe
tes,
fam
ily m
embe
rs w
ere
ofte
n t
he p
rimar
y ca
regi
vers
.
Kah
olok
ula
et a
l., 2
008
(51)
495
Nat
ive
Haw
aiia
ns fr
om 2
rura
l com
mun
ities
in H
awai
‘i; n
onpr
egna
nt
100
≥30
Obs
erva
tiona
l, re
trosp
ectiv
e c
ohor
t, po
pula
tion-
base
d s
ampl
e
To e
xam
ine
asso
ciat
ions
bet
wee
n m
odes
of a
ccul
tura
tion
and
diab
etes
pre
vale
nce.
Cro
ss-s
ectio
nal s
urve
y. M
odes
of
acc
ultu
ratio
n in
clud
ed o
nly
Nat
ive
Haw
aiia
n vs
. Am
eric
an; o
ther
eth
nic
cultu
res w
ere
not i
nclu
ded.
Nat
ive
Haw
aiia
ns w
ith a
trad
ition
al m
ode
of a
ccul
tura
tion
wer
e m
ore
likel
y to
hav
e di
abet
es (2
7.9%
) tha
n pe
rson
s w
ith in
tegr
ated
(15.
4%),
assi
mila
ted
(12
.5%
), or
mar
gina
lized
(10.
5%)
mod
es.
Kim
et a
l., 2
008
(28)
434
Nat
ive
Haw
aiia
ns o
ut o
f a
mul
tieth
nic
tota
l sam
ple
of 1
,257
; non
preg
nant
35≥3
0O
bser
vatio
nal,
retro
spec
tive
coh
ort,
popu
latio
n-ba
sed
sam
ple
To e
xam
ine
asso
ciat
ions
of
dia
bete
s with
die
tary
pat
tern
and
eth
nici
ty.
Cro
ss-s
ectio
nal;
poss
ible
reca
ll bi
as o
n fo
od fr
eque
ncy
ques
tionn
aire
; m
easu
rem
ent e
rror
in e
stim
atio
n of
foo
d po
rtion
s.C
onsu
mpt
ion
of lo
cal e
thni
c fo
ods w
as c
orre
late
d w
ith b
ody
mas
s ind
ex,
sm
okin
g, w
aist
-to-h
ip ra
tio, a
nd g
luco
se. C
onsu
mpt
ion
of th
ese
food
s w
as h
ighe
r for
Nat
ive
Haw
aiia
ns th
an f
or o
ther
eth
nic
grou
ps. N
ativ
e H
awai
ians
had
the
high
est t
otal
ene
rgy
inta
ke.
Abb
revi
atio
ns: C
ES-D
, Rig
ht fo
r Epi
dem
iolo
gic
Stud
ies D
epre
ssio
n Sc
ale;
NH
OPI
, Nat
ive
Haw
aiia
ns a
nd o
ther
Pac
ific
Isla
nder
s; S
D, s
tand
ard
devi
atio
n.
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mau et al. Page 21
Tabl
e 3
Lite
ratu
re o
n O
besi
ty H
ealth
Dis
parit
ies A
mon
g N
ativ
e H
awai
ians
and
Oth
er P
acifi
c Is
land
ers,
Janu
ary
1998
–Dec
embe
r 200
8
Stud
y A
utho
r(s)
and
Yea
r (R
ef. N
o.)
Sam
ple
and
No.
of S
ubje
cts
% o
fT
otal
Sam
ple
Who
Wer
eN
HO
PI
Age
,ye
ars
Stud
y D
esig
nM
ain
Goa
l and
Out
com
es/F
indi
ngs
Lim
itatio
ns
Mas
karin
ec e
t al.,
199
8 (5
2)4,
321
Nat
ive
Haw
aiia
ns o
ut o
f a
tota
l mul
tieth
nic
sam
ple
of 2
7,67
8
16>3
0O
bser
vatio
nal,
pros
pect
ive
coh
ort,
popu
latio
n-ba
sed
sam
ple
of 2
% o
f the
Haw
ai‘i
Sta
te p
opul
atio
n
To in
vest
igat
e ef
fect
s of a
lcoh
ol in
take
and
bod
y w
eigh
t on
mor
talit
y fr
om a
ll ca
uses
, c
ance
r, ce
rebr
ovas
cula
r dis
ease
, and
cor
onar
y he
art d
isea
se.
No
info
rmat
ion
on p
reex
istin
g c
ardi
ovas
cula
r dis
ease
, ser
um c
hole
ster
ol le
vel,
hype
rtens
ion,
dia
bete
s, or
fam
ily h
isto
ry.
Nat
ive
Haw
aiia
ns h
ad th
e hi
ghes
t mor
talit
y r
ate
and
a hi
gher
pre
vale
nce
of o
besi
ty.
BM
Ia >
29.3
was
ass
ocia
ted
with
50%
hig
her r
isk
of d
eath
. Cor
onar
y he
art
dis
ease
mor
talit
y w
as h
ighe
r in
Nat
ive
Haw
aiia
ns w
ith B
MIs
>29
.3.
Gal
anis
et a
l., 1
999
(53)
946
Sam
oans
in W
este
rn S
amoa
and
Am
eric
an S
amoa
100
25–5
5O
bser
vatio
nal,
cros
s- s
ectio
nal,
retro
spec
tive
coh
ort,
com
mun
ity a
nd w
orkp
lace
sam
ple
To d
escr
ibe
diet
ary
inta
ke a
s mea
sure
d b
y 24
-hou
r rec
all o
f Am
eric
an S
amoa
ns a
nd W
este
rn S
amoa
ns.
No
bioc
hem
ical
mea
sure
men
t of
car
diov
ascu
lar d
isea
se ri
sk o
r c
orre
latio
ns w
ith a
nthr
opom
etric
mea
sure
men
ts; p
oten
tial s
ampl
e b
ias;
reca
ll bi
as o
n di
etar
y a
sses
smen
t.A
mer
ican
Sam
oans
con
sum
ed a
gre
ater
pro
porti
on o
f car
bohy
drat
es a
nd p
rote
in b
ut le
ss fa
t or s
atur
ated
fat t
han
Wes
tern
Sam
oans
. The
mea
n B
MI o
f A
mer
ican
Sam
oans
was
35.
2 as
com
pare
d w
ith 3
0.3
for W
este
rn S
amoa
ns.
Gra
ndin
etti
et a
l., 1
999
(32)
567
Nat
ive
Haw
aiia
ns in
2 r
ural
com
mun
ities
in H
awai
‘i; n
onpr
egna
nt
100
≥30
Obs
erva
tiona
l, re
trosp
ectiv
e c
ohor
t, po
pula
tion-
base
d s
ampl
e
To a
sses
s the
rela
tion
of d
egre
e of
Nat
ive
Haw
aiia
n an
cest
ry w
ith B
MI a
nd w
aist
- t
o-hi
p ra
tio.
Cro
ss-s
ectio
nal;
self-
repo
rted
anc
estry
and
die
tary
reca
ll.
Com
bine
d pr
eval
ence
of o
verw
eigh
t and
/ o
r obe
sity
was
81.
5% in
Nat
ive
Haw
aiia
ns a
s com
pare
d w
ith th
e U
S p
reva
lenc
e of
52.
6%. 4
9% o
f Nat
ive
Haw
aiia
ns w
ere
obes
e as
com
pare
d w
ith th
e U
S pr
eval
ence
of 2
1%
Incr
ease
d w
aist
circ
umfe
renc
e w
as f
ound
in 5
1% o
f Nat
ive
Haw
aiia
ns. M
ore
wom
en (5
9%) t
han
men
(39%
) had
inc
reas
ed w
aist
circ
umfe
renc
e. A
ge,
per
cent
age
of N
ativ
e H
awai
ian
ance
stry
, a
nd to
tal d
ieta
ry e
nerg
y in
take
wer
e s
igni
fican
tly a
ssoc
iate
d w
ith in
crea
sed
BM
I and
wai
st-to
-hip
ratio
. Adi
posi
ty i
ncre
ased
with
per
cent
age
of N
ativ
e H
awai
ian
ance
stry
.
McG
arve
y et
al.,
200
2 (5
4)18
1 Sa
moa
ns a
nd A
mer
ican
Sam
oans
100
25–5
5O
bser
vatio
nal,
nest
ed st
udy
in
a pr
ospe
ctiv
e co
hort;
To te
st th
e as
soci
atio
n of
6 g
enet
ic m
icro
sate
llite
mar
kers
rela
ted
to th
eFu
nctio
nal s
igni
fican
ce o
f pre
sent
fin
ding
rem
ains
unc
lear
.
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mau et al. Page 22
Stud
y A
utho
r(s)
and
Yea
r (R
ef. N
o.)
Sam
ple
and
No.
of S
ubje
cts
% o
fT
otal
Sam
ple
Who
Wer
eN
HO
PI
Age
,ye
ars
Stud
y D
esig
nM
ain
Goa
l and
Out
com
es/F
indi
ngs
Lim
itatio
ns
pop
ulat
ion-
base
d sa
mpl
e h
uman
lept
in (L
EP) l
ocus
and
the
pro-
opi
omel
anoc
ortin
gen
e re
gion
in a
dult
Sam
oans
and
Am
eric
an S
amoa
ns.
Sign
ifica
ntly
gre
ater
freq
uenc
y of
alle
le 2
26 a
t the
LEP
locu
s in
the
nono
bese
Sam
oans
than
in th
e ob
ese
subj
ects
.
Mam
pilly
et a
l., 2
005
(36)
585
Nat
ive
Haw
aiia
ns o
ut o
f a
tota
l mul
tieth
nic
sam
ple
of 3
,732
16≥1
8O
bser
vatio
nal,
cros
s- s
ectio
nal t
elep
hone
surv
ey;
Beh
avio
ral R
isk
Fact
or S
urve
illan
ce S
yste
m p
opul
atio
n sa
mpl
e
To a
sses
s the
phy
sica
l act
ivity
leve
ls o
f m
ultie
thni
c gr
oups
in H
awai
‘i.Te
leph
one
surv
ey; s
elf-
repo
rt of
phy
sica
l act
ivity
. Sel
f-re
porte
d w
eigh
t and
hei
ght.
Nat
ive
Haw
aiia
ns w
ere
mor
e a
ctiv
e (3
9% m
oder
ate,
24%
vig
orou
s) t
han
othe
r Asi
ans a
nd P
acifi
c Is
land
ers
but
less
act
ive
than
whi
tes.
48%
of
Nat
ive
Haw
aiia
ns re
porte
d be
ing
ove
rwei
ght a
s com
pare
d w
ith 5
8% o
f w
hite
s, 42
% o
f Fili
pino
s, an
d 41
% o
f J
apan
ese.
Hen
ders
on e
t al.,
200
6 (5
5)15
9 N
ativ
e H
awai
ians
out
of
a ra
ndom
subs
ampl
e of
811
per
sons
from
Haw
ai‘i
and
Cal
iforn
ia
2045
–74
Obs
erva
tiona
l, ne
sted
stud
y i
n a
pros
pect
ive
coho
rt; r
ando
mly
sele
cted
sam
ple
To e
xam
ine
the
rela
tion
betw
een
circ
ulat
ing
leve
ls o
f 2 p
rimar
y pr
otei
ns (
IGF-
1 an
d IG
FBP-
3) in
the
insu
lin-li
ke g
row
th fa
ctor
pat
hway
and
obe
sity
in 5
rac
ial/e
thni
c gr
oups
usi
ng B
MI a
s an
ind
icat
or o
f adi
posi
ty.
Unm
easu
red
conf
ound
ing
fact
ors;
rac
ial/e
thni
c di
ffer
ence
s in
BM
I c
utpo
ints
may
hav
e co
nfou
nded
stu
dy. P
lasm
a IG
F-I a
nd IG
FBP-
3 w
ere
mea
sure
d at
a si
ngle
tim
e p
oint
.
No
sign
ifica
nt in
tera
ctio
n w
as f
ound
bet
wee
n IG
F-1
and
BM
I in
Nat
ive
Haw
aiia
ns a
s com
pare
d w
ith Ja
pane
se a
nd L
atin
os, i
n w
hom
dec
reas
ed IG
F-1
was
ass
ocia
ted
with
incr
easi
ng B
MI.
How
arth
et a
l., 2
006
(56)
433
Nat
ive
Haw
aiia
ns o
ut o
f a
tota
l mul
tieth
nic
sam
ple
of 2
,326
per
sons
from
Haw
ai‘i
and
Cal
iforn
ia
1945
–74
Obs
erva
tiona
l, pr
ospe
ctiv
e c
ohor
t; po
pula
tion-
base
d s
ampl
e
To d
eter
min
e w
heth
er d
ieta
ry e
nerg
y de
nsity
was
rela
ted
to c
urre
nt B
MI a
nd ri
sk o
f ove
rwei
ght/o
besi
ty in
a m
ultie
thni
c po
pula
tion.
Food
freq
uenc
y as
sess
men
t of d
ieta
ry e
nerg
y de
nsity
bas
ed o
n re
call.
Die
tary
reca
ll m
ay v
ary
by b
ody
wei
ght.
Nat
ive
Haw
aiia
n m
en h
ad th
e hi
ghes
t BM
I; w
eigh
t and
die
tary
ene
rgy
dens
ity w
ere
sig
nific
antly
rela
ted
to B
MI.
Nat
ive
Haw
aiia
n w
omen
wer
e se
cond
-hea
vies
t a
fter A
fric
an A
mer
ican
s. H
ighe
r ene
rgy
den
sity
was
sign
ifica
ntly
ass
ocia
ted
with
gre
ater
like
lihoo
d of
bei
ng o
verw
eigh
t in
all
ethn
ic a
nd se
x gr
oups
. Nat
ive
Haw
aiia
ns w
ere
unus
ual i
n th
at lo
w e
nerg
y de
nsity
was
ass
ocia
ted
with
hig
h B
MI.
Mas
karin
ec e
t al.,
200
6 (3
4)9,
994
Nat
ive
Haw
aiia
ns o
ut o
f a
tota
l mul
tieth
nic
sam
ple
of 7
6,16
3
13≥1
8O
bser
vatio
nal,
pros
pect
ive
coh
ort;
pool
ed d
ata
from
18
pop
ulat
ion-
base
d st
udie
s
To d
escr
ibe
trend
s in
BM
I and
the
rela
tions
of n
utrie
nt a
nd fo
od in
take
with
exc
ess
Lim
ited
in co
mpa
rabi
lity
of n
utrit
iona
l m
easu
res a
cros
s stu
dies
ove
r tim
e, m
ainl
y be
caus
e di
etar
y as
sess
men
t
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mau et al. Page 23
Stud
y A
utho
r(s)
and
Yea
r (R
ef. N
o.)
Sam
ple
and
No.
of S
ubje
cts
% o
fT
otal
Sam
ple
Who
Wer
eN
HO
PI
Age
,ye
ars
Stud
y D
esig
nM
ain
Goa
l and
Out
com
es/F
indi
ngs
Lim
itatio
ns
car
ried
out o
ver 2
5 ye
ars i
n H
awai
‘i w
eigh
t. m
etho
ds h
ave
impr
oved
ove
r the
yea
rs; r
ecal
l bia
s.N
ativ
e H
awai
ians
had
the
high
est
pre
vale
nce
of e
xces
s wei
ght a
t all
times
. C
arbo
hydr
ates
wer
e po
sitiv
ely
ass
ocia
ted
with
exc
ess w
eigh
t am
ong
Nat
ive
Haw
aiia
ns. N
utrit
iona
l d
eter
min
ants
of e
xces
s wei
ght w
ere
sim
ilar a
mon
g w
hite
s, Ja
pane
se, a
nd N
ativ
e H
awai
ians
, des
pite
mar
ked
diff
eren
ces i
n B
MI.
Alb
right
et a
l., 2
007
(33)
12,3
06 N
ativ
e H
awai
ians
out
of a
mul
tieth
nic
tota
l sam
ple
of 2
00,0
03
645
–74
Obs
erva
tiona
l, pr
ospe
ctiv
e c
ohor
t; po
pula
tion-
base
d s
ampl
e
To e
xam
ine
BM
I in
pers
ons w
ith e
thni
c a
dmix
ture
as c
ompa
red
with
per
sons
who
wer
e m
onor
acia
l but
shar
ed a
com
mon
eth
nici
ty/ra
ce.
Self-
repo
rted
heig
ht, w
eigh
t, an
d e
thni
city
; una
ble
to q
uant
ify th
e g
enet
ic c
ontri
butio
n of
eac
h et
hnic
ity r
epor
ted.
Nat
ive
Haw
aiia
ns h
ad th
e hi
ghes
t BM
I c
ompa
red
with
oth
er e
thni
c gr
oups
. E
thni
c ad
mix
ture
s tha
t inc
lude
d N
ativ
e H
awai
ian
herit
age
had
high
er B
MIs
than
mos
t oth
er e
thni
c co
mbi
natio
ns.
Boy
d, 2
007
(37)
32 N
ativ
e H
awai
ian
com
mun
ity c
olle
ge st
uden
ts10
018
–25
Focu
s gro
up, u
nive
rsity
con
veni
ence
sam
ple
To a
sses
s per
cept
ions
of h
ealth
y lif
esty
les
and
supp
orts
for a
nd b
arrie
rs to
hea
lthy
liv
ing.
Smal
l sam
ple
size
; bia
sed
sam
ple.
Dem
andi
ng li
fest
yle
and
lazi
ness
wer
e c
ited
as b
arrie
rs to
bei
ng p
hysi
cally
act
ive.
Pre
fere
nces
for g
roup
-orie
nted
and
col
lege
-cou
rse-
base
d op
portu
nitie
s t
o le
arn
abou
t hea
lthy
livin
g an
d ho
w to
bec
ome
mor
e ph
ysic
ally
act
ive.
Dai
et a
l., 2
007
(57)
583
Am
eric
an S
amoa
ns10
0≥1
8O
bser
vatio
nal,
nest
ed st
udy
in
a pr
ospe
ctiv
e co
hort;
ran
dom
sele
ctio
n sa
mpl
e
To d
etec
t tra
it lo
ci in
fluen
cing
adi
posi
ty-
rel
ated
phe
noty
pes u
sing
a w
hole
gen
ome
linka
ge sc
an a
ppro
ach
in f
amili
es fr
om A
mer
ican
Sam
oa.
No
adju
stm
ent f
or o
ther
impo
rtant
gen
etic
and
env
ironm
enta
l fac
tors
tha
t con
tribu
te to
adi
posi
ty, s
uch
as d
iet a
nd p
hysi
cal a
ctiv
ity.
Stro
ng e
vide
nce
for a
maj
or lo
cus o
n c
hrom
osom
e 6q
23.2
influ
enci
ng se
rum
lep
tin le
vels
. Ano
ther
gen
etic
regi
on,
16q
21, a
ppea
rs to
be
a su
scep
tibili
ty l
ocus
that
aff
ects
phe
noty
pes f
or B
MI,
per
cent
age
of b
ody
fat,
lept
in le
vels
, and
wai
st c
ircum
fere
nce.
Mas
karin
ec e
t al.,
200
7 (3
5)16
,079
Nat
ive
Haw
aiia
ns o
ut o
f a m
ultie
thni
c to
tal s
ampl
e o
f 117
,065
14≥4
0O
bser
vatio
nal,
pros
pect
ive
coh
ort;
popu
latio
n-ba
sed
sam
ple
To in
vest
igat
e ch
ange
s in
risk
fact
ors i
n H
awai
‘i ov
er 2
0 ye
ars a
nd c
ompa
re h
ealth
beh
avio
rs a
mon
g et
hnic
gro
ups.
Diff
eren
ces i
n da
ta c
olle
ctio
n ac
ross
2 st
udie
s; im
prov
emen
ts in
nut
ritio
nal a
sses
smen
t ove
r tim
e; v
alid
ity o
f eth
nici
ty a
ssig
nmen
t (se
lf- r
epor
ted)
; litt
le in
form
atio
n on
soc
ioec
onom
ic st
atus
.N
ativ
e H
awai
ians
had
the
high
est c
hron
ic d
isea
se ri
sk sc
ores
in c
ompa
rison
with
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mau et al. Page 24
Stud
y A
utho
r(s)
and
Yea
r (R
ef. N
o.)
Sam
ple
and
No.
of S
ubje
cts
% o
fT
otal
Sam
ple
Who
Wer
eN
HO
PI
Age
,ye
ars
Stud
y D
esig
nM
ain
Goa
l and
Out
com
es/F
indi
ngs
Lim
itatio
ns
oth
er g
roup
s. B
MI w
as h
ighe
st fo
r Nat
ive
Haw
aiia
ns.
Nov
otny
et a
l., 2
007
(58)
55 S
amoa
n w
omen
100
18–2
8O
bser
vatio
nal,
cros
s- s
ectio
nal,
conv
enie
nce
sam
ple
To e
xam
ine
anth
ropo
met
ric c
utof
f poi
nts
as i
ndic
ator
s of c
hron
ic d
isea
se ri
sk.
Cro
ss-s
ectio
nal,
smal
l sam
ple
of S
amoa
n w
omen
; bia
sed
sam
ple.
80%
of s
ampl
e w
as o
verw
eigh
t or o
bese
. B
MI a
nd d
ual-e
nerg
y X
-ray
abs
orpt
iom
etry
lean
mas
s wer
e s
igni
fican
tly a
nd p
ositi
vely
ass
ocia
ted
with
glu
cose
leve
ls.
Mas
karin
ec e
t al.,
200
8 (5
9)25
4 N
ativ
e H
awai
ian
wom
en o
ut o
f a m
ultie
thni
c to
tal
sam
ple
of 1
,418
18≥2
1O
bser
vatio
nal,
cros
s- s
ectio
nal,
brea
st-c
ance
r- r
elat
ed p
artic
ipan
t sam
ple
To e
xam
ine
rela
tion
of so
y in
take
with
bod
y w
eigh
t ove
r the
life
span
of w
omen
.Se
lf-re
porte
d he
ight
, wei
ght,
and
diet
dat
a; li
fetim
e re
call
of so
y in
take
was
diff
icul
t.M
eat a
nd v
eget
able
inta
ke a
nd to
tal e
nerg
y in
take
(kca
l/day
) wer
e h
ighe
r for
Nat
ive
Haw
aiia
ns. E
atin
g m
ore
soy
food
s in
adul
thoo
d di
d no
t pre
dict
low
er B
MI o
r low
er a
nnua
l wei
ght g
ain
for
Nat
ive
Haw
aiia
ns.
Abb
revi
atio
ns: B
MI,
body
mas
s ind
ex; I
GF-
1, in
sulin
-like
gro
wth
fact
or 1
; IG
FBP-
3, in
sulin
-like
gro
wth
fact
or b
indi
ng p
rote
in 3
; NH
OPI
, Nat
ive
Haw
aiia
ns a
nd o
ther
Pac
ific
Isla
nder
s.
a Wei
ght (
kg)/h
eigh
t (m
)2.
Epidemiol Rev. Author manuscript; available in PMC 2010 June 28.



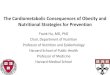















![Cardiovascular disease [autosaved]](https://img.dokumen.tips/doc/110x75/554b2ab7b4c905d3088b4ab0/cardiovascular-disease-autosaved.jpg)