Embed Size (px)
Citation preview
1/3/2017
1
Cardiac ArrestJanuary 2017
Corey M. Slovis, M.D.Vanderbilt University Medical Center
Metro Nashville Fire DepartmentNashville International Airport
Nashville, TN
CPR2017
• 31,292 ALS vs 1,643 BLS cases
• Medicare billing data records (20% of total)
• Harvard study 2009 – 2011, no rural services
• Propensity matching utilized
JAMA 2015;175:196-204
Is ALS significantly better than BLS for out of hospital cardiac arrest?
ALS younger, more male, less likely to have chronic medical condition and picked up at a residence
BLS more likely to be picked up at a skilled nursing facility
Used data based on protocol that BLS was dispatched if ALS not available
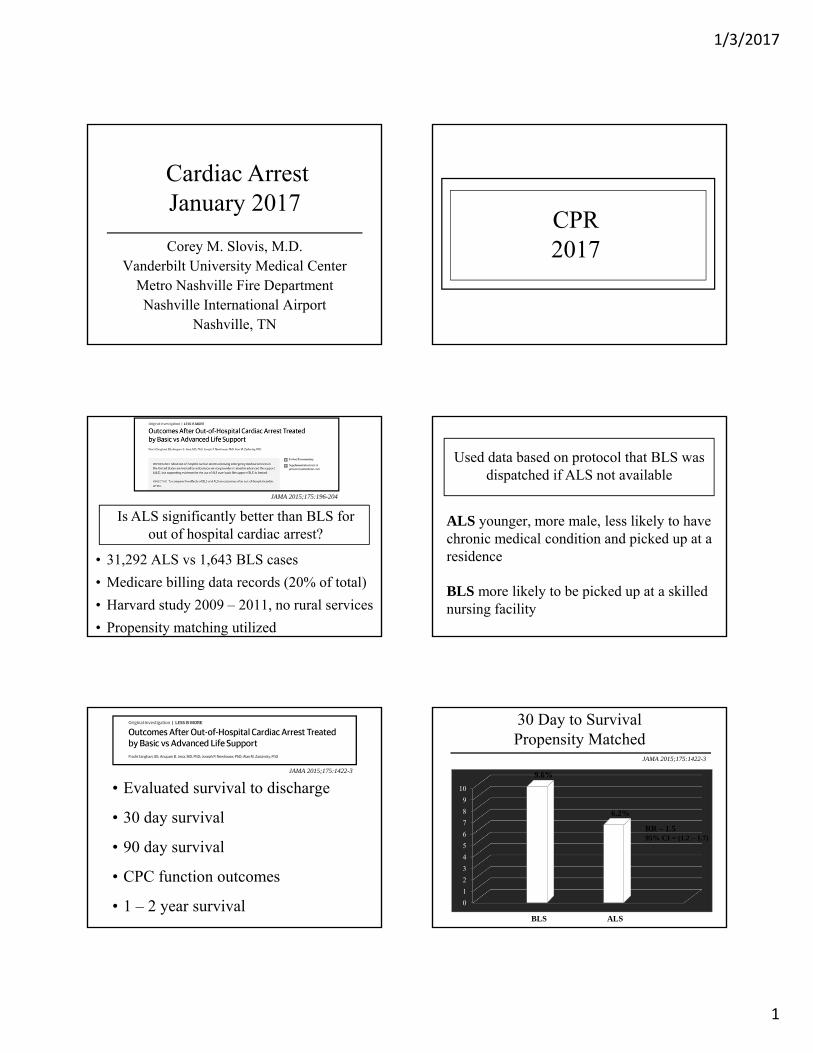
• Evaluated survival to discharge
• 30 day survival
• 90 day survival
• CPC function outcomes
• 1 – 2 year survival
JAMA 2015;175:1422-3
0
1
2
3
4
5
6
7
8
9
10
9.6%
6.2%
30 Day to SurvivalPropensity Matched
BLS ALS
RR – 1.595% CI = (1.2 – 1.7)
JAMA 2015;175:1422-3

1/3/2017
2
0
10
20
30
40
50
21.8%
44.8%
Poor Neurologic Outcome – Discharged PtsPropensity Matched
BLS ALS
(95% CI = 18.6 – 27.4)
JAMA 2015;175:1422-3
BLS vs ALS Take Homes
• AEDs and O2 by BVM are key
• How important is ALS?
• Not a randomized study
• Many potential confounders
• 30,381 witnessed Swedish cardiac arrests• CPR vs no CPR pre EMS• Evaluated 30 day survival• Multiple other variables evaluated
How important is CPR pre EMS arrivalNEJM 2015; 372: 2307-15
0123456789
101112131415
No CPR CPR pre EMS
11 Min
13 Min
Collapse to defibrillation Median Time
NEJM 2015; 372: 2307-15
P < 0.001
0%
1%
2%
3%
4%
5%
6%
7%
8%
9%
10%
11%
12%
No CPR CPR pre EMS
4.0%
10.5%
Hu
nd
red
s
30 Day Survival NEJM 2015; 372: 2307-15
P < 0.001
0%
5%
10%
15%
20%
25%
30%
0-3 4-8 9-14 > 14
26.4%
15.6%
7.9%
2.7%
Hu
nd
red
s
Start Time (Min)
P < 0.001
CPR start time and 30 day survivalVF/VT
NEJM 2015; 372: 2307-15

1/3/2017
3
Bystander CPR & AED use resulted in a 40.7% survival rate
JAMA 2015;314:247-54
• North Carolina CARES registry 2010-2013
• 4,961 patients
• Increased AED use by police, rescue squads, etc.
• Urban, suburban, rural
Does a statewide CPR education and AED first responder program make a difference?
JAMA 2015;314:255-64
0%
5%
10%
15%
20%
25%
2010 2013
14.1%
23.1%
Hu
nd
red
s
Bystander CPR & First Responder AED Use
JAMA 2015;314:255-64
P = 0.02
• 5,989 volunteers CPR trained• Used phones with GPS• 667 cardiac arrests• 911 system sends mobile alerts
Does a phone alert to those close to a cardiac arrest improve bystander CPR
NEJM 2015; 372: 2316-25
This was a blinded study where phone activation to those within 0.3 miles (500 meters) was turned on or off in
1:1 randomized manner
0%
10%
20%
30%
40%
50%
60%
70%
GPS Sent No GPS
62%
48%
Hu
nd
red
s
Bystander CPR NEJM 2015; 372: 2316-25
P < 0.001

1/3/2017
4
CPR 2015-2016Take Homes
• Bystander CPR can double survival
• More than 80% of 30-day survivors will be neurologically intact
• 911 center cell phone activation of CPR providers increases the likelihood of bystander CPR pre EMS arrival
• The more bystander CPR the better
• Can double survival rate
• Low cost, high yield
• AEDs in public locations < $1,000
• Less A and more B in CLS
Importance of BCLSTake Homes
• 100-120 compressions/minute
• Depress to 2 inches
• Allow full recoil
• Don’t hyperventilate: 8-10 times/minute
• Minimize interruptions / pre shock pauses
Expert BCLS
ACLS2017
• 147 references
• 15 writing groups
• All based on 2015 ILCOR topics
Circulation 2015:132 (suppl 2);5444-64
The AHA 2016 Guidelines for ACLS
But not after ROSC93-95% if well performed
89-92% if COPD
Circulation 2015:132 (suppl 2);5444-64
Use 100% O2 during CPR
Oxygen Use

1/3/2017
5
• No high quality evidence to favor any
• ETI may decrease compression fraction
Circulation 2015:132 (suppl 2);5444-64
BVM vs SGA vs ETT
“For healthcare providers trained in their use either an SGA or ETT may be used as the
initial airway during CPR”
Circulation 2015:132 (suppl 2);5444-64
Continuous waveform capnography is recommended for placement and monitoring
If not available then colorimetric, EDD or ultrasound may be used
Assessment of ETT Placement
Circulation 2015:132 (suppl 2);5444-64
10 breaths per minute (Q 6 seconds)after advanced airway in place
Ventilation Rate• Amiodarone may be considered
• Lidocaine may be considered as alternative
• Magnesium not recommended
Circulation 2015:132 (suppl 2);5444-64
“No antiarrhythmic as yet been shown to increase survival or neurologic outcome after
cardiac arrest due to VF/pVT”
Antiarrhythmic for VF/pVT
• 3,026 pts., 10 ROC sites
• Randomized, double blind, placebo controlled
• VF/pVT, s/p 1 or more shocks, s/p epi
• Only adult medical VF/pVT OOH
New Engl J Med 2016; 374:1711-22
What is the best antiarrhythmic for shock resistant VF/pVT:
Amiodarone vs Lidocaine vs Placebo?
• Average age 63 ± 14 y; 80% M
• 60% had bystander CPR
• BLS in 5.8 min
• ALS in 8 min
• EMS call to drug: 19 min(prior trials 21-25 min)
New Engl J Med 2016; 374:1711-22

1/3/2017
6
0
5
10
15
20
25
30 24.4 23.7
Survival to DischargeNeurologic Outcome
Survival
2118.8
New Engl J Med 2016; 374:1711-22
%
A PL A
17.516.6
Mod Rankin ≤ 3
L P
Percentage Differences• Amiodarone vs Placebo
• Amiodarone vs Lidocaine
• Lidocaine vs Placebo
• Amiodarone vs Placebo
Modified Rankin ≤ 3
• Amiodarone vs Lidocaine
Modified Rankin ≤ 3
3.2% (p=0.08)
0.7% (p=0.70)
2.6% (p=0.16)
2.2% (p=0.19)
1.3% (p=0.44)
New Engl J Med 2016; 374:1711-22
• 5% absolute improvement of Amiodarone over placebo (p ≤ 0.04) if arrest witnessed (1934 pts)
• 21.9% absolute increase Amiodarone vs placebo if EMS witnessed and gave drugs near immediately (p < 0.01 for 154 pts)
NEJM 2016:375;801-3
Authors Note in Letter to Editor
• 7 studies: 3 RCTs, 4 non-RCTs
• 3,877 pts in RCTs and 700 in non-RCTs
• Includes 2016 NEJM trial
• Admission and Discharged Alive evaluated
Resuscitation 2016;107:31-7
What do all studies combined tell us about Amiodarone vs Lidocaine in VF/pVT?
ResultsAmiodarone vs Placebo:
- trend for hospital discharge with Amio(p=0.08)
- No difference in favorable neuro outcomes
Lidocaine vs Placebo:- No significant difference at discharge
Amiodarone vs Lidocaine:- No difference in hospital discharge (p=0.81)
Resuscitation 2016;107:31-7
Amiodarone vs Lidocaine vs PlaceboTake Homes
• There is no strong evidence on antiarrhythmic efficacy in VF/pVT
• If 3% superiority of Amiodarone over placebo was true difference (requires larger study) then 1,800 lives would be saved in North America yearly
• The data is not conclusive
• The drugs are given 10-20+ minutes into arrest

1/3/2017
7
At the present time, there is no clear benefit of Amiodarone vs Lidocaine
Late in VF it’s not clear either drug is beneficial
• Randomized European trial of 62 patients
• 10 mg/kg of procainamide over 20 minutes (33 pts.)
• 5 mg/kg of amiodarone over 20 minutes (29 pts.)
• All had BP > 90 mm Hg and no SOB
• Evaluated both efficacy and major adverse events
Eur Heart J 2016; June 28 Epub ahead of print
Is amiodarone really the best antiarrhythmic for VTach / Wide complex QRS tachycardias?
0%
10%
20%
30%
40%
50%
60%
70%
Hu
nd
red
s
Wide QRS Tachycardia Termination vs Side Effects
Eur Heart J 2016; June 28 Epub ahead of print
Termination Major Adverse Effects
67%
Pro Amio Pro Amio
P=0.026 P=0.006
9%
41%38%
Hypotension
• Hypotension common with both drugs
• 41% of amiodarone required immediate cardioversion
• Less than 1/10 (9%) in procainamide group required emergency cardioversion
• Total adverse events double with amiodarone (48% vs 24%)
Eur Heart J 2016; June 28 Epub ahead of print
Amiodarone vs Procainamide for VTachTake Homes
• Procainamide clearly superior in this study and much less toxic
• Amiodarone dose of 5 mg/kg is about 300 mg which is double the 150 mg/10 minutes
• But even with high dose amiodarone, procainamide much more efficacious
• My bias is to not use amio in stable wide complex patients and I use procainamide as my antiarrhythmic of choice
Stable Wide Complex Tachycardia5 Steps
• Be sure it is regular
• Modified Vagal Maneuver
• Adenosine: 12 mg IVP
• Procainamide: 100 mg/min x 2 then 50 mg/min x 5
• Shock

1/3/2017
8
• Use not addressed during VF/pVT
• “Inadequate evidence” to support post CPR use
• May be considered
• Not enough evidence to be for or against lidocaine or beta blockers s/p VF/pVT
Circulation 2015:132 (suppl 2);5444-64
Beta Blockers
• Retrospective ED study
• All EMS to ED arrivals
• All s/p 3 shocks, 3 doses Epi, 300mg Amio
• Compares Esmolol vs no Esmolol
Resuscitation 2014;85:1337-1341
Is Esmolol effective in refractory VF/VT?
0
10
20
30
40
50
60
70
80
33%
66%
Esmolol for Refractory VF/VTSustained ROSC and Good Neuro D/C
Sustained ROSC Good Neuro D/C
10.5%
50%
No NoEsmolol Esmolol
Resuscitation 2014;85:1337-1341
• Very small study
• But impressive results
• Certainly not harmful
• Has been suggested for 50 years
• I think worth a try
BB For Refractory VF/VT
• Vasopressin + Epi no longer recommended
• Vasopressin no longer recommended
Circulation 2015:132 (suppl 2);5444-64
Vasopressin has been removed from ACLS algorithm
VasopressinCirculation 2015:132 (suppl 2);5444-64
Standard dose epinephrine (1 mg Q 3-5 minutes) may be reasonable for patients
with cardiac arrest (class 11b)
Epinephrine Use
• Early administration may improve ROSC and neurologic outcomes – later administration may decrease both

1/3/2017
9
• 2,974 VF/pVT arrests, 1,510 with epi < 2 min
• Inpatient data from 300 GWTG-R hospitals
• Propensity matched cardiac arrest pts
• Compared epi before vs after 2nd shock
BMJ 2016;353:1577-87
Does giving epinephrine before 2nd shock help or hinder resuscitation?
• 51% of patients received epi before 2nd shock
• 87% of both groups received 2nd defib
• Groups equal for total defibrillations (3)
• Early epi group received 3 mgs or epi on average vs 1 mg in later dosing
• Similar TOR times (22 vs 21 mins)
BMJ 2016;353:1577-87
0
10
20
30
40
50
60
70
8067%
79%
Epi Before vs After 2nd Shock
ROSC
31%
48%
BMJ 2016;353:1577-87
%
< 2 < 2> 2 min > 2 min
25%
41%
Good Neuro
< 2 > 2 min
Survival
All p < 0.001
Early Epinephrine AdministrationTake Homes
• Wait for second shock before administering epinephrine
• The role of epi is still not clearly defined…but wait to administer it
• Epinephrine is the most potent cardiac stimulant – wait to give it during VF
JAMA 2015;314:802-10
• 1,558 pediatric patients
• Average age = 9 mos
• 31.3% overall survival rate
• 17.1% favorable neurologic status
• Matched rhythm and numerous variables
Does time to epinephrine affect outcomes innon-VF-VT pediatric arrests?
JAMA 2015;314:802-10
• Longer time to epi = worse survival
• Longer time to epi = ROSC
• time to epi = neurologic outcomes
Results

1/3/2017
10
• The role of epinephrine remains unclear but this study shows earlier use improves survival
• Each minute delay decreases survival
• One of the few positive studies on the efficacy of epinephrine
• Not an epi vs no-epi study
Epinephrine in CPRTake Homes
Circulation 2015:132 (suppl 2);5444-64
Steroids• There is no recommendation for or against
steroids for in-hospital cardiac arrest
• Use of steroids in out-of-hospital arrests are “of uncertain benefit”
TherapeuticHypothermia
ACC/AHA GuidelinesPCI and Hypothermia
• Therapeutic hypothermia should be started ASAP for all comatose STEMI patients and out of hospital arrests due to VF or VT (1B)
• Immediate PCI is indicated in all STEMI arrest patients including those who are receiving therapeutic hypothermia (1B)
• What temperature for Therapeutic Hypothermia?
• 939 patients in randomized trial
• 36 ICUs in Europe and Australia
• Evaluated: mortality & neuro outcome at 180d
• 80% VF/VT; 20% AS and PEA (12%/7%)
New Engl J Med 2013, 369:2197-2206
• Compares 32 -33 to 35 -36 TH
• No unwitnessed Asystole patients
• 24% intravascular; 76% surface cooled
• 28 hours of cooling
• Rewarmed at 0.5 /hour
New Engl J Med 2013, 369:2197-2206

1/3/2017
11
• Groups the same for:
‾ First measured temps (35.2 – 35.3)
‾ Serum pH (7.2)
‾ Serum lactate (6.7)
‾ Circulatory shock (70% vs 67%)
‾ ST segment (40% vs 42%)
New Engl J Med 2013, 369:2197-2206
0
10
20
30
40
50
60
%52
54
Hypothermia vs Normal TempSurvival and Neuro Outcomes
Survival Poor Neuro
36Survival Poor Neuro
33
53 52
P = NS
New Engl J Med 2013, 369:2197-2206
• The future of deep TH is unclear
• Preventing Hyperthermia appears crucial
• Future studies will determine optimal TH temp
• Well done study, but likely not the final study
Therapeutic HypothermiaTake Homes
• 35 – 36 looks like the new 32 – 34
• Does Prehospital TH have benefits?
• 1.359 patients; Randomized trial
• King County Washington Medic 1
• 583 with VF; 776 without VF
• Almost all patients cooled on hospital arrival
JAMA 2014;311:45-52
• EMS cooling: up to 2L of 4 C LR
• Mean core temp by 1.20 C to ED
• EMS patients took 1 hr less to get to 34
• Study evaluated mortality and neuro status
• EMS pts: 7-10mg pavulon + 1-2mg valium
JAMA 2014;311:45-52
0
10
20
30
40
50
60
70
64.3%
16.3%
Survival to Discharge
VF Non-VF
No EMS THVF
EMS TH
62.7%
19.2%
Non-VF
P = NS
JAMA 2014;311:45-52

1/3/2017
12
• No improvement in neuro status in any group
• EMS TH group had more re-arrests
• EMS TH group had more pulmonary edema
• No difference in pressor use (9%)
Additional Results
(26% vs 21%; p = 0.008)
(41% vs 30%; p < 0.001)
JAMA 2014;311:45-52
• TH by EMS offers no benefits
• Lots of EMS training, resources and expense,
• In my opinion: this is a large and definitive
Prehospital TH InductionTake Homes
yet no benefits shown
study
Does ECMO have a role in CPR?
Resuscitation 2015;86:88-94
• Refractory VF x 30 minutes
• No known underlying severe disease
• CPR within 10 minutes of arrest
• Mechanical CPR available
• ECMO Team with 2 MDs present
Does ECMO improve post-arrest resuscitation outcomes – The CHEER trial
Resuscitation 2015;86:88-94
• ECMO
• Mechanical CPR
• Therapeutic Hypothermia
• Immediate post ECMO PCI
• 24 hours of TH
“E-CPR”• 26 patients (11 OHCA, 15 IHCA)
• ECMO within 56 minutes; 2 days on
• 96% ROSC
E-CPR Results
54% (14/26) survived to discharge with CPC score of 1 – full neurologic recovery
Resuscitation 2015;86:88-94

1/3/2017
13
• Requires large team and planning
• Careful patient selection
• 76% complication rate
• May require transfer to OR
• Things continue to get more complex
ECMO CPRTake Homes
Lancet 2015;385:947-55
Can mechanical CPR improve resuscitation outcomes – PARAMEDIC trial
• 4471 patients randomized
• Used LUCAS-2 mechanical device
• 4 UK Ambulance Services
• 21% VF, 25% PEA, 49% AS
0
5
10
15
20
25
30 23% 23%
Arrest and 3 Months Survival
LUCAS CONTROL
EventLUCAS CONTROL
4 Months
6% 6%
Lancet 2015;385:947-55
PARAMEDIC trial found no evidence of any advantages with mechanical
CPR: Both acute and long term survival, along with neurologic
function were all similar manual vs mechanical.
• No proven benefit yet
• Excellent for stairs or long transports
• Essential for Cath Lab
• Expensive
Mechanical CPRTake Homes
Can we have a TOR criteria that gives us 100% specificity and a PPV of 100% for non-survival?
• Prospective French trial, the PRESENCE Study
•1,771 pts from Paris’ Sudden Death Expertise Center
• Tested and applied 3 criteria
• Used prospective data from Paris & King County
• Prospectively tested in 5,192 patients
Annals Int Med 2016;165:770-8

1/3/2017
14
• Not witnessed by FF/EMS First Responders
• Non-shockable rhythm
• No ROSC after 2 doses of epinephrine
Paris TOR Criteria 2,799 Patients Meeting All 3 CriteriaNot witnessed, no shock, 2 doses epi
Study
Paris 1 year cohort
Paris validation cohort
PRESENCE Trial
King County, USA
N Survived
772 0
1569 1*
285 0
173 0
*Persistent vegetative state
Take Homes• Use 3 criteria for TOR
- Non-shockable, not witnessed by first responders
- Non-responsive to two doses epi
• Terminating sooner can decrease transport with 100% reliability
• Has potential to increase organ donations
• 30 minutes on scene for non-shockable rhythm is not needed
BCLS 2016Take Homes
• Bystander CPR can double survival
• More than 80% of 30-day survivors will be neurologically intact
• 911 center cell phone activation of CPR providers increases the likelihood of bystander CPR pre EMS arrival
• 30:2 may be superior to continuous
• 100-120 compressions/minute
• Depress to 2 inches
• Allow full recoil
• Don’t hyperventilate: 8-10 times/minute
• Minimize interruptions / pre-shock pauses
Expert BCLS





























