Embed Size (px)
Citation preview
Journal of Plastic, Reconstructive & Aesthetic Surgery (2010) 63, 1388e1390
CASE REPORT
Capsular flap for coverage of an exposed implantafter skin-sparing mastectomy and immediatebreast reconstruction
Michael Brandstetter a, Thomas Schoeller b, Petra Pulzl b,Heinrich Schubert b,*, Gottfried Wechselberger b
a Paracelsus Medical University, Strubergasse 21, 5020 Salzburg, Austriab Department of Plastic and Reconstructive Surgery, Medical University Innsbruck, Anichstraße 35, 6020 Innsbruck, Austria
Received 2 July 2009; accepted 13 November 2009
KEYWORDSCapsular flap;Implant;Coverage;Wound healing
* Corresponding author. Tel.: þ43 5E-mail address: heinrich.schubert@
1748-6815/$-seefrontmatterª2009Bridoi:10.1016/j.bjps.2009.11.054
Summary Native skin-flap necrosis following skin-sparing mastectomy (SSM) is treated byraising a capsular flap, formed as a consecutive physiological reaction around breast implant.Using this highly vascularised thin tissue layer as an implant coverage withdraws pressure fromthe defect and allocates a good background for wound healing.ª 2009 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published byElsevier Ltd. All rights reserved.
Skin-sparing mastectomy (SSM) followed by immediateimplant reconstruction has been advocated as an effectivetreatment option in breast reconstruction. It minimisesdeformity and improves aesthetics through preservation ofthe natural skin envelope of the breast. However, native skinflap necrosis can occur and lead to implant exposure andinfection, thus significantly jeopardising the result. Skinnecrosis is easier to treat if the implant is covered under-neath the pectoralis muscle or other well-vascularisedtissue, such as a capsule surrounding the breast implants.The latter was already successfully used as a capsular flap forcorrection of contour deformities of the breast1 and to
12 504 80893.i-med.ac.at (H. Schubert).
tishAssociationofPlastic,Reconstruc
correct breast implant malposition.2 Basic requirement forall these techniques is that, at the time of the necessarysurgical intervention, sufficient capsular growth shouldalready have occurred. We herein present the use of a pedi-cled capsular flap for salvage of an exposed breast implant, 7months after SSM and immediate breast reconstruction.
Technique
Using the initial approach of SSM, the wound is re-openedand the necrotic parts are excised.
After removal of the breast implant, capsulotomy is per-formed, carefully sparing out the base of the planned flap. Inour patients a lateral, posteriorly based pedicled flap wasrisen. Sufficient circulation and viability are attested byvisible arterial bleeding seen at the flap edges (Figure 2).
tiveandAestheticSurgeons.PublishedbyElsevierLtd.All rightsreserved.

Figure 1 Partial skin flap necrosis, exposing the implant.
Figure 3 Covering the new implant with the excised flap.
Capsular flap for coverage of an exposed implant 1389
The decision, from which side the flap is pedicled,depends on the extent and location of the defect and islimited by the size of the capsular pocket.
The flap should be long enough to range from its base onthe chest wall to the excised defect, enclosing the implantanteriorly and with an adequate overall width to guaranteesecure closure. Subsequently, a new implant is inserted andcovered with the excised flap of the capsular tissue(Figure 5).
To secure the desired level of the implant, the flap istightened to the opposite side of the pocket, usingabsorbable sutures (4/0 Vicryl�). Thereby the tension istaken off the vulnerable area of the skin and a well-vascularised base for wound healing is provided. Forpostoperative care, a supportive dressing is advised for10e14 days.
Figure 2 Raising a lateral, posteriorly based pedicledcapsular flap.
Results
Capsular flaps were used on three middle-aged patientsover the past 3 years. All patients showed satisfactoryresults with no history of wound-healing disturbance orpalpable indurations.
Case report
A 38-year-old woman presented with ductal carcinoma insitu (DCIS) of the left breast after she had undergonea lumpectomy from the upper part of the right breast 4years previously. The patient was tested positive for BRCA-1 mutation. So finally a bilateral SSM followed by immediate
Figure 4 Postoperative view (5 months later).
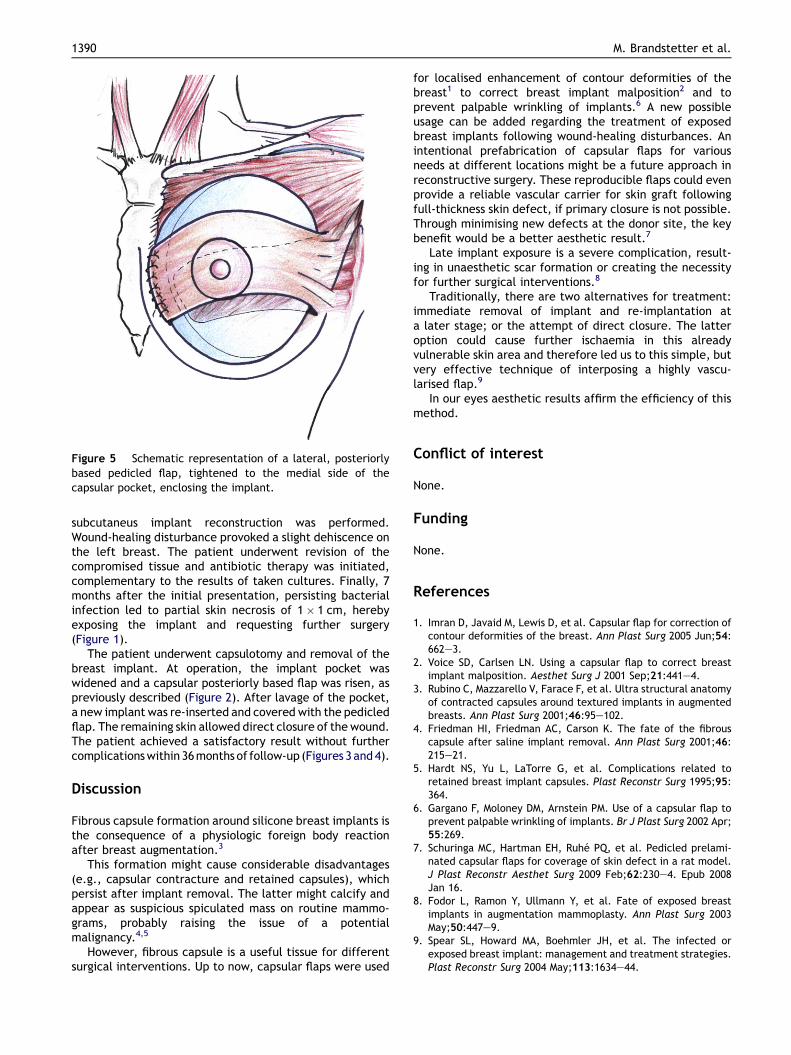
Figure 5 Schematic representation of a lateral, posteriorlybased pedicled flap, tightened to the medial side of thecapsular pocket, enclosing the implant.
1390 M. Brandstetter et al.
subcutaneus implant reconstruction was performed.Wound-healing disturbance provoked a slight dehiscence onthe left breast. The patient underwent revision of thecompromised tissue and antibiotic therapy was initiated,complementary to the results of taken cultures. Finally, 7months after the initial presentation, persisting bacterialinfection led to partial skin necrosis of 1� 1 cm, herebyexposing the implant and requesting further surgery(Figure 1).
The patient underwent capsulotomy and removal of thebreast implant. At operation, the implant pocket waswidened and a capsular posteriorly based flap was risen, aspreviously described (Figure 2). After lavage of the pocket,a new implant was re-inserted and covered with the pedicledflap. The remaining skin allowed direct closure of the wound.The patient achieved a satisfactory result without furthercomplicationswithin36monthsof follow-up (Figures 3 and 4).
Discussion
Fibrous capsule formation around silicone breast implants isthe consequence of a physiologic foreign body reactionafter breast augmentation.3
This formation might cause considerable disadvantages(e.g., capsular contracture and retained capsules), whichpersist after implant removal. The latter might calcify andappear as suspicious spiculated mass on routine mammo-grams, probably raising the issue of a potentialmalignancy.4,5
However, fibrous capsule is a useful tissue for differentsurgical interventions. Up to now, capsular flaps were used
for localised enhancement of contour deformities of thebreast1 to correct breast implant malposition2 and toprevent palpable wrinkling of implants.6 A new possibleusage can be added regarding the treatment of exposedbreast implants following wound-healing disturbances. Anintentional prefabrication of capsular flaps for variousneeds at different locations might be a future approach inreconstructive surgery. These reproducible flaps could evenprovide a reliable vascular carrier for skin graft followingfull-thickness skin defect, if primary closure is not possible.Through minimising new defects at the donor site, the keybenefit would be a better aesthetic result.7
Late implant exposure is a severe complication, result-ing in unaesthetic scar formation or creating the necessityfor further surgical interventions.8
Traditionally, there are two alternatives for treatment:immediate removal of implant and re-implantation ata later stage; or the attempt of direct closure. The latteroption could cause further ischaemia in this alreadyvulnerable skin area and therefore led us to this simple, butvery effective technique of interposing a highly vascu-larised flap.9
In our eyes aesthetic results affirm the efficiency of thismethod.
Conflict of interest
None.
Funding
None.
References
1. Imran D, Javaid M, Lewis D, et al. Capsular flap for correction ofcontour deformities of the breast. Ann Plast Surg 2005 Jun;54:662e3.
2. Voice SD, Carlsen LN. Using a capsular flap to correct breastimplant malposition. Aesthet Surg J 2001 Sep;21:441e4.
3. Rubino C, Mazzarello V, Farace F, et al. Ultra structural anatomyof contracted capsules around textured implants in augmentedbreasts. Ann Plast Surg 2001;46:95e102.
4. Friedman HI, Friedman AC, Carson K. The fate of the fibrouscapsule after saline implant removal. Ann Plast Surg 2001;46:215e21.
5. Hardt NS, Yu L, LaTorre G, et al. Complications related toretained breast implant capsules. Plast Reconstr Surg 1995;95:364.
6. Gargano F, Moloney DM, Arnstein PM. Use of a capsular flap toprevent palpable wrinkling of implants. Br J Plast Surg 2002 Apr;55:269.
7. Schuringa MC, Hartman EH, Ruhe PQ, et al. Pedicled prelami-nated capsular flaps for coverage of skin defect in a rat model.J Plast Reconstr Aesthet Surg 2009 Feb;62:230e4. Epub 2008Jan 16.
8. Fodor L, Ramon Y, Ullmann Y, et al. Fate of exposed breastimplants in augmentation mammoplasty. Ann Plast Surg 2003May;50:447e9.
9. Spear SL, Howard MA, Boehmler JH, et al. The infected orexposed breast implant: management and treatment strategies.Plast Reconstr Surg 2004 May;113:1634e44.





























