Embed Size (px)
Citation preview

CAP-HC RFP Cover Sheet 1
Form 1. Cover Sheet
Agency Name:
Director Name:
Director Title: (Executive Director, President, CEO, etc.)
Director Phone:
Director Email:
Agency Administrative Office Address Street Address:
City:
Zip:
Agency Administrative Office Phone:
Agency Website:
Agency Facebook: (if applicable)
Agency Twitter: (if applicable)
Application Contact Name (if different than Director):
Contact Telephone (if different than Director):
Contact Fax Number (if different than Director):
Contact Email Address (if different than Director):
Contact Address (if different than the Agency address):
Federal Tax ID Number (required):
Minnesota Tax ID Number (required):
DUNS Number:
SWIFT Vendor ID Number (if known):
Project Name:
Primary Geographic Area Served (Minneapolis or Suburban Hennepin County)
How Many People Does the Organization Support Each Year (All Programs)
Amount of Funding Requested (All Grant Expenditures Must Be Made Between March 1, 2019 – December 31, 2019)
REQUIRED ATTACHMENTS

CAP-HC RFP Cover Sheet 2
I certify that the information contained herein is true and accurate to the best of my knowledge and that I am
authorized to submit this application on behalf of the applicant.
Authorized Signature: Date:
Title: Executive Director
Form 2: Work Plan
Enter Program Name:
Service Provided (Brief description of how the program addresses the need)
Population(s ) Served
Targeted number of
unduplicated families served
Measurable Outcomes Data collection & analysis methods
Click here to enter text. Click here to
enter text..
Click here
to enter text.
Click here to enter text. Click here to enter
text.
Form 3: Budget
Agency Name:
All grant funds must be expended between March 1, 2019 and December 31st 2019
CAP-HC Sub-Grant
Cost Category # March 1, 2019 - December 31, 2019PROVIDE NARRATIVE FOR EACH BUDGET LINE ITEM
under COLORED Budget Detail SHEET
1
2
3
4
5
6
7
8
TOTALS
Submitter's Signature Date Signed
CAP-HC Approval Signature Date Approved
Community Action Partnership of Hennepin County
Direct Client Services
Personnel
Travel
Supplies
2019 PROPOSED FUNDING BUDGETMarch 1, 2019 to December 31, 2019
Category Description
Consultant & Professional Services
Space and Rentals
Other
The CAP-HC signature below indicates that the above Budget has been accepted and approved and will be attached to the executed grant contract.
Outreach
The signature below indicates that the above Budget has been submitted for approval and if approved will be attached to the executed grant contract.

Agency Name:
CAP-HC Sub-Grant
March 1, 2019 - December 31, 2019
Cost Category # Direct Client Services Description Amounts
18 1
19 1
20 1
21 1
22 1
23 1
Direct Client Services Total:
Narrative- Provide detailed budget calculations (e.g.
amt. of rent X # of clients, mos. etc)
2019 PROPOSED FUNDING BUDGETMarch 1, 2019 to December 31, 2019
Cost Category 1 - Direct Client Services
Agency Name:
Salary Amount Fringe Benefit Amount Total of Salary & Fringe
1 2
2 2
3 2
4 2
5 2
6 2
7 2
8 2
9 2
10 2
11 2
12 2
13 2
14 2
15 2
16 2
17 2
TOTAL PERSONNEL COSTS
Cost Category # Title or Position (Paid Personnel)
CAP-HC Sub-Grant
March 1, 2019 - December 31, 2019 Narrative- Provide detailed budget calculations (e.g. # of
FTEs, wage/fringe, # of weeks/mos., etc)
2019 PROPOSED FUNDING BUDGETMarch 1, 2019 to December 31, 2019
Cost Category 2 - Personnel (Salaries & Fringe)
Agency Name:
CAP-HC Sub-Grant
COST CAT. NO. March 1, 2019 - December 31, 2019
3
Cost Category 3 - Instate Travel
Na
rrat
ive:
Inst
ate
Trav
el
DESCRIPTION
Instate Travel Total:
2019 PROPOSED FUNDING BUDGETMarch 1, 2019 to December 31, 2019

Agency Name:
CAP-HC Sub-Grant
COST
CAT.
NO.
March 1, 2019 - December 31, 2019
4
2019 PROPOSED FUNDING BUDGETMarch 1, 2019 to December 31, 2019
Cost Categories 4 - Supplies
DESCRIPTION
Supplies: Total:
Nar
rati
ve:
Su
pp
lies
Agency Name:
CAP-HC Sub-Grant
COST CAT.
NO.March 1, 2019 - December 31, 2019
5
6
7
Nar
rati
ve:
Co
nsu
ltan
ts &
Pro
fess
ial S
erv
ices
Nar
rati
ve:
Ou
trea
ch
2019 PROPOSED FUNDING BUDGETMarch 1, 2019 to December 31, 2019
Nar
rati
ve:
Spac
e C
ost
s an
d
Re
nta
ls
Consultant & Prof. Services TOTAL:
DESCRIPTION
Cost Categories 5 - Consultant & Professional Services, 6 - Space and Rentals, & 7 - Outreach
Outreach
Space and Rentals TOTAL:
Agency Name:
CAP-HC Sub-Grant
March 1, 2019 - December 31, 2019
Cost Category # Description of Other Costs AmountsNarrative - Please provide information to support
expense
8
8
8
8
8
8
8
8
8
8
8
8
8
8
8
8
8
TOTAL OTHER
2019 PROPOSED FUNDING BUDGETMarch 1, 2019 to December 31, 2019
Cost Category 8 - Other
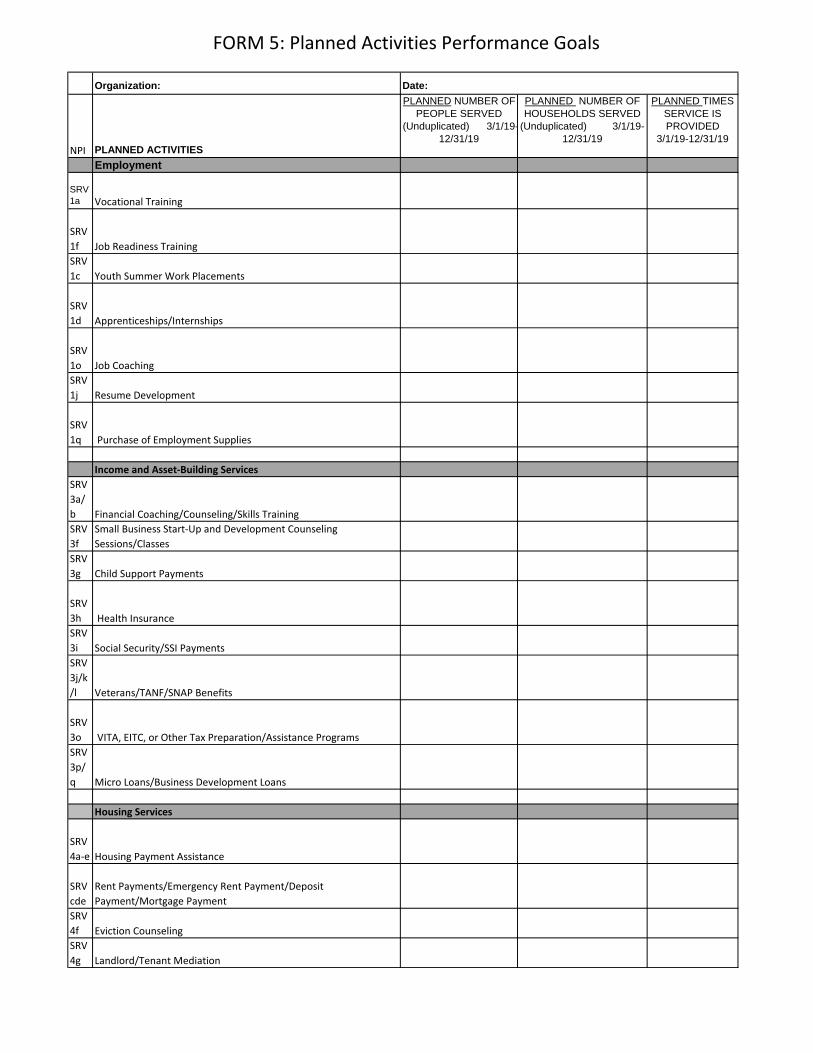
FORM 5: Planned Activities Performance Goals
Organization:
NPI PLANNED ACTIVITIES
PLANNED NUMBER OF
PEOPLE SERVED
(Unduplicated) 3/1/19-
12/31/19
PLANNED NUMBER OF
HOUSEHOLDS SERVED
(Unduplicated) 3/1/19-
12/31/19
PLANNED TIMES
SERVICE IS
PROVIDED
3/1/19-12/31/19
Employment
SRV
1a Vocational Training
SRV
1f Job Readiness Training
SRV
1c Youth Summer Work Placements
SRV
1d Apprenticeships/Internships
SRV
1o Job Coaching
SRV
1j Resume Development
SRV
1q Purchase of Employment Supplies
Income and Asset-Building Services
SRV
3a/
b Financial Coaching/Counseling/Skills Training
SRV
3f
Small Business Start-Up and Development Counseling
Sessions/Classes
SRV
3g Child Support Payments
SRV
3h Health Insurance
SRV
3i Social Security/SSI Payments
SRV
3j/k
/l Veterans/TANF/SNAP Benefits
SRV
3o VITA, EITC, or Other Tax Preparation/Assistance Programs
SRV
3p/
q Micro Loans/Business Development Loans
Housing Services
SRV
4a-e Housing Payment Assistance
SRV
cde
Rent Payments/Emergency Rent Payment/Deposit
Payment/Mortgage Payment
SRV
4f Eviction Counseling
SRV
4g Landlord/Tenant Mediation
Date:

FORM 5: Planned Activities Performance Goals
SRV
4i-l Utility Payment Assistance
SRV
4m-
p Housing Placement/Rapid Re-Housing
SRV
4q Housing Maintenance and Improvements
Health and Social/Behavioral Development Services
SRV
5a-j
Health Services, Screening and Assessments
SRV
5e/f
Prescription Payments/Doctor Visit Payments
SRV
5g Maternal/Child Health
SRV
5k-o
Reproductive Health Services
SRV
5n
STI/HIV Screenings/Prevention Counseling Services
SRV
5r-x
Mental Behavioral Health
SRV
5tSubstance Abuse Counseling
SRV
5bb-
ee
Dental Services, Screening and Exams
SRV
5nn-
oo
Emergency Hygiene Assistance
Education and Cognitive Development
SRV
a-j
Child/Young Adult Education Programs
SRV
2b
Head Start
SRV
2d
K-12 Education
SRV
2h
College-Readiness Prep/Support
SRV
2k School Supplies
SRV
2l-q
Extra-Curricular Programs
SRV
2m
Summer Youth Recreational Opportunities

FORM 5: Planned Activities Performance Goals
SRV
2r-z
Adult Education Programs
SRV
2yPost-Secondary Education Supports

FORM 5: Planned Activities Performance Goals
Performance Indicators
PLANNED # of Program
Participants
(3/1/19-12/31/19)
PLANNED # of Participants Achieving Outcome
(3/1/19-12/31/19)
Employment
The number of unemployed adults who obtained employment
The number of unemployed adults who obtained and
maintained employment for at least 90 days
The number of youth who obtained employment to gain skills or
income
The number of employed participants in a career-advancement
related program who entered or transitioned into a position
that provided increased income or benefits
Income and Asset Building Services
The number of individuals who achieved and maintained
capacity to meet basic needs for 90 days
The number of individuals who opened a savings account or IDA
The number of individuals who increased their savings
The number of individuals who used their savings to purchase
an asset
The number of individuals who improved their credit scores
Housing Services
The number of households experiencing homelessness who
obtained safe temporary shelter
The number of households who obtained safe and affordable
housing
The number of households who avoided eviction
The number of households who avoided foreclosure
FORM 5: PLANNED Performance Goals

FORM 5: Planned Activities Performance Goals
The number of households who experienced improved health
and safety due to improvements within their home (e.g.
reduction or elimination of lead, radon, carbon dioxide and/or
fire hazards or electrical issues, etc.)
Health and Social/Behavioral Development Services
The number of individuals who demonstrated improved physical
health and well-being
The number of individuals who demonstrated improved mental
and behavioral health and well-being
The number of individuals with chronic illness who maintained
an independent living situation
The number of individuals who improved skills related to the
adult role of parents/ caregivers
Education and Cognitive Development Services
The number of children (0 to 5) who demonstrated skills for
school readiness
The number of children and youth who are achieving at basic
grade level (academic, social, and other school success skills)
The number of adults who demonstrated improved basic
education
The number of individuals who obtained a high school diploma
and/or obtained an equivalency certificate or diploma
The number of individuals who obtained a recognized
credential, certificate, or degree relating to the achievement of
educational or vocational skills.




























![HD Видеокамера HC-V770 HC-V760 HC-VX870 HC-VX870M · hc-v770 [v770] Серияv770 / серия [v770] hc-v770m [v770m] hc-v760 [v760] – Данная инструкция](https://img.dokumen.tips/doc/110x75/5e697831d35b2b14c40ee20b/hd-hc-v770-hc-v760-hc-vx870-hc-vx870m-hc-v770-v770-v770.jpg)