-
7/24/2019 Cancer Feline
1/13
http://jfm.sagepub.com/Journal of Feline Medicine and
Surgery
http://jfm.sagepub.com/content/15/5/366Theonline version of this
article can be foundat:
DOI: 10.1177/1098612X13483235
2013 15: 366Journal of Feline Medicine and SurgeryLaura
Blackwood
Cats with Cancer : Where to start
technique does not amount to an endorsement of its value or
quality, or the claims made by its manufacturer.those of the
authors and the inclusion in this publication of material relating
to a particular product, method orof animals and interpretation of
published materials lies with the veterinary practitioner. The
opinions expressed arefrom actions or decisions based on
information contained in this publication; ultimate responsibility
for the treatment
arisingcountry. The authors, editors, owners and publishers do
not accept any responsibility for any loss or damageadvertising
material, it is the responsibility of the reader to check that the
product is authorised for use in their ownbear this in mind and be
aware of the prescribing laws pertaining to their own country.
Likewise, in relation toFurthermore, drugs may be mentioned that
are licensed for human use, and not for veterinary use. Readers
need toformulations that are not available or licensed in the
individual reader's own country.The Journal of Feline Medicine and
Surgery is an international journal and authors may discuss
products and
Disclaimer
Published by:
International Society of Feline Medicine
American Association of Feline Practitioners
and
http://www.sagepublications.com
can be found at:Journal of Feline Medicine and SurgeryAdditional
services and information for
http://jfm.sagepub.com/cgi/alertsEmail Alerts:
http://jfm.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Apr 19, 2013Version of Record>>
at FACULTAD DE FILOSOFIA Y LETRA on May 7,
2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/content/15/5/366http://jfm.sagepub.com/content/15/5/366http://jfm.sagepub.com/content/15/5/366http://www.isfm.net/http://www.catvets.com/http://www.sagepublications.com/http://jfm.sagepub.com/cgi/alertshttp://jfm.sagepub.com/cgi/alertshttp://jfm.sagepub.com/subscriptionshttp://jfm.sagepub.com/subscriptionshttp://www.sagepub.com/journalsReprints.navhttp://www.sagepub.com/journalsReprints.navhttp://www.sagepub.com/journalsPermissions.navhttp://online.sagepub.com/site/sphelp/vorhelp.xhtmlhttp://online.sagepub.com/site/sphelp/vorhelp.xhtmlhttp://jfm.sagepub.com/content/15/5/366.full.pdfhttp://jfm.sagepub.com/content/15/5/366.full.pdfhttp://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://online.sagepub.com/site/sphelp/vorhelp.xhtmlhttp://jfm.sagepub.com/content/15/5/366.full.pdfhttp://www.sagepub.com/journalsPermissions.navhttp://www.sagepub.com/journalsReprints.navhttp://jfm.sagepub.com/subscriptionshttp://jfm.sagepub.com/cgi/alertshttp://www.sagepublications.com/http://www.catvets.com/http://www.isfm.net/http://jfm.sagepub.com/content/15/5/366http://jfm.sagepub.com/
-
7/24/2019 Cancer Feline
2/13
366 JFMS CLINICAL PRACTICE DOI: 10.1177/1098612X13483235 ISFM
and AAFP 2013
Journal of Feline Medicine and Surgery (2013) 15, 366377
CATS WITH CANCER
Where to start
Laura Blackwood
Cancer in cats
The most common tumours in cats are summarised with their
pre-senting features and differentials in Table 1, and some are
illustrated onpage 368. Often, there may be non-neoplastic
differentials for masslesions as cats develop more granulomatous
lesions than other species.They can also develop quite marked
lymphadenopathy due to reactiveor infectious causes. Furthermore,
extranodal lymphoma can arise atany site, and is much more common
in feline patients than in theircanine counterparts, as are the
alimentary/abdominal and cranialmediastinal forms of the
disease.
Clinical signs
Patients with cancer may present with a mass lesion (eg, a
palpablemammary lesion) or with signs secondary to a mass such as
halitosis,poor grooming or a malodor-ous coat in those with
oral
masses. The different behav-iour patterns of individual
catsaffect how quickly masslesions are noted and, unfortu-nately,
many cats present latein the disease course. Cats withcancer may
present with non-specific signs, such as alter-ations in appetite,
reducedactivity levels or weight loss(Figure 1). Nonetheless, a
greatdeal of information can beobtained from clinical exami-nation
in cats, as abdominalmasses are often readily palpa-ble, and
changes in thoraciccompressibility may be apparent where there is a
cranial mediastinalmass.
Some cats present with clinical signs of metastatic disease
rather thansigns relating to the primary tumour. This is seen most
often in cases of
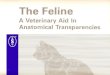
Figure 1 Elderly male neutered (MN) domesticshorthair (DSH) cat,
which presented with weight lossdue to alimentary and renal
lymphoma
Practical relevance: Many cats
develop cancer and may or may not
present with an obvious mass lesion.
As our feline patients are living longer
and their owners are increasingly
seeking veterinary care, the apparent incidence
and prevalence of cancer is increasing.
Clinical challenges: Neoplasia is a differential
for many clinical presentations in cats. Often
tumours are relatively advanced at the point of
presentation, and this can make management
difficult. In addition, many cats find clinic visits
stressful and this can influence owners
decisions about treatment.
Audience: This review provides an overview
of the approach to the feline cancer patient, and
is aimed at all veterinary practitioners that see
cats. It is intended as a starting point for more
detailed discussions in accompanying articlesin this special
issue on feline oncology.
Evidence base: There is limited data on most
feline tumours compared with tumours in canine
or human patients, so a robust evidence base is
often lacking.
Laura BlackwoodBVMS PhD MVM CertVR DipECVIM-CA (Onc) MRCVSRCVS
& European Specialist in Veterinary Oncology
Small Animal Teaching Hospital,University of Liverpool, Chester
High Road,
Neston, Wirral, CH64 7TE, UKEmail:
[email protected]
C L I N I C A L R E V I E W
at FACULTAD DE FILOSOFIA Y LETRA on May 7,
2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/
-
7/24/2019 Cancer Feline
3/13
JFMS CLINICAL PRACTICE 367
REV IEW/Cancer in cats an introduction
Tumour type Site Signalment/clinical signs/comments
Differentials
LYMPHOMA Alimentary Older catsInsidious weight loss
Anorexia/reduced appetiteDiarrhoeaOccasionally vomiting
Malabsorption/protein-losing enteropathyIf gastric involvement,
secondary gastritis/ulceration
All other causes of weight loss and gastrointestinalsigns
including:
Inflammatory bowel
diseasePancreatitis/triaditisInfectious/antibiotic-responsive
disease
Endocrine diseaseRenal disease
All other causes of mesenteric lymphadenopathyincluding:
Feline infectious peritonitis (FIP)Inflammatory bowel
diseaseMetastatic neoplasiaPancreatitisMycobacterial infection
Multicentric Any ageNon-painful lymph node enlargement (may be
regional)
AnorexiaDepressionNon-specific
malaisePyrexia(Polyuria/polydipsia uncommon)
Retroviral/viral, bacterial, fungal, mycobacterial(and
protozoal) infectionsImmune-mediated diseaseIdiopathic
lymphadenopathyOther haematopoetic malignanciesMetastatic disease
(regional)
Cranialmediastinal
Younger cats, OrientalsRespiratory
distressRegurgitation/dysphagiaWeight lossLethargy, exercise
intolerancePalpable reduction in cranial thoracic
compressibilityCough (uncommon)
ThymomaOther cranial mediastinal lymphadenopathyOther causes of
pleural effusion:
Congestive heart failurePyothoraxFIP(Trauma/haemothorax)
Extranodal:nasal
Nasal dischargeEpistaxisNasal obstructionFacial
distortionExophthalmosReduced appetite
Other nasal tumoursChronic rhinitis/sinusitis
Extranodal:renal
MalaiseAnorexiaRenomegaly (often bilateral)
Azotaemia
Chronic renal failureOther renal tumours
Extranodal:central nervoussystem (CNS)
Signs depend on siteRarely solitary may find other sites on
stagingCNS lymphoma can be difficult to confirm:
Extradural masses: no tumour cells incerebrospinal fluidBone
marrow aspirate?
Other neoplastic CNS disease (especially meningioma)Inflammatory
CNS diseaseInfectious CNS disease:
ToxoplasmosisFIPFeline leukaemia virus
(FeLV)/felineimmunodeficiency virus (FIV) infection
SQUAMOUSCELLCARCINOMA
Oral cavity HalitosisUnkempt coatOral mass lesion (commonly
sublingual)
Dental diseaseFibrosarcomaLymphomaGranulomaOther tumour (eg,
osteosarcoma)
Rhinarium/pinna/eyelid/
other cutaneous
Plaque-like or papillated, scaly, crusty, crateriformor
ulcerated mass
Papillary or fungiform massOften indurated (fixed and firm)
Eosinophilic granulomaActinic keratitis (precursor of squamous
cell carcinoma)
Basal cell tumour
MAMMARYCARCINOMA
Mammaryglands
Mass associated with mammary glandSize has prognostic
significance (3 cm worse prognosis)
SarcomaBenign mammary tumourMammary hypertrophy/fibroadenomatous
hyperplasia
SOFT TISSUESARCOMA
Injection siteOthercutaneous/subcutaneous
Firm, poorly circumscribed massMay be multilobular
Alopecia/ulceration
Cutaneous:Basal cell tumourMast cell tumourSquamous cell
carcinoma
Subcutaneous:Mast cell tumourOther sarcoma
Abscess(Lipoma relatively uncommon)
Table 1 Common tumours in cats clinical signs and
differentials
at FACULTAD DE FILOSOFIA Y LETRA on May 7,
2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/
-
7/24/2019 Cancer Feline
4/13
368 JFMS CLINICAL PRACTICE
REV IEW/ Cancer in cats an introduction
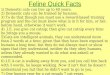
a
b
Intestinal lymphoma, with renal involvement, in the elderly MN
DSH catpictured in Figure 1. This lateral abdominal radiograph
showsgastric/intestinal gravel sign consistent with partial
obstruction, a largemid-ventral abdominal soft tissue mass, and a
rounded irregularenlarged renal shadow. The cat responded well to
cyclophosphamide,vincristine and prednisolone, but on relapse did
not respond to rescuetherapy. Survival time was 7 months
Oral mass, diagnosed as lymphoma, in an adult female
neutered(FN) DSH cat (recently rescued). The cat responded well
tocyclophosphamide, vincristine and prednisolone and had a
survivaltime of more than 2 years
Lymphoma
Squamous cell carcinoma
Soft tissuesarcoma
Unresectable sublingual and lingual squamous cellcarcinoma in an
8-year-old MN DSH cat. There was noresponse to palliative medical
therapy or chemotherapyand the cat was euthanased 3 weeks after
diagnosis
Early cutaneous squamous cellcarcinoma in a 17-year-old FNDSH
cat that presented forpostoperative radiation therapyof a labial
squamous cellcarcinoma. Surgical excision ofthis mass was curative,
but therewas relapse at the site of thelabial squamous cell
carcinomaafter 5 months
Advanced rhinarialsquamous cellcarcinoma in an8-year-old MN DSH
cat,presented for radiationtherapy. Short-termpalliation was
achieved
Maxillary fibrosarcoma causing grossfacial distortion in an
11-year-old FNDSH cat. Suture is present from arecent biopsy
Large soft tissue sarcoma (suspected injection site-associated
sarcoma) in an adult MN DSH cat
C o m m o n f e l i n e t u m o u r s
at FACULTAD DE FILOSOFIA Y LETRA on May 7,
2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/
-
7/24/2019 Cancer Feline
5/13
JFMS CLINICAL PRACTICE 369
lungdigit syndrome (Figure 2), wherepatients present with
metastatic lesions of thedigits (usually multiple) secondary to
primarylung tumours.1,2 Cats may also infrequentlypresent with
signs due to paraneoplastic dis-ease. Cutaneous manifestations of
neoplasiaare uncommon butdramatic (eg, para-neoplastic alopeciain
pancreatic, hepaticor bile duct carcino-ma; exfoliative der-matitis
with thymo-ma), and neoplasiashould be a dif-ferential for cats
pre-senting with thesedermatological com-
plaints (Figure 3).36
REV IEW/Cancer in cats an introduction
Getting a diagnosis
Key to appropriately managing cancer cases ishaving an accurate
diagnosis, so that correcttumour staging can be performed and
thebest treatment recommended. Clinical fea-tures typical of a
malignant tumour includerapid growth, fixation, invasion into deep
tis-sues or overlying skin, ulceration and poorlydefined margins.
Clinical criteria can suggesta lesion is malignant, but apparently
lessaggressive behaviour should not result in thelesion being
assumed benign. For example,aggressive mesenchymal tumours may
appear well demarcated due to pseudocap-sule formation. Sampling
of mass lesions bycytology or histology is required.
The advantages and disadvantages ofcytology and histopathology
are summarisedin the box below. Neither technique is 100%sensitive
or specific in the diagnosis oftumours, although histopathology
remainsthe gold standard.
a b
Figure 2 Lungdigitsyndrome in an adult DSHcat. The patient
presentedto the orthopaedic serviceat the authors hospital
forinvestigation of lamenessand digital swellings (a). Apulmonary
mass was foundon thoracic radiography, asdemonstrated by the
rightlateral view shown in (b).Reproduced from Corr andBlackwood
(2003)2
Figure 3 Severe exfoliativedermatitis, seborrhoea andalopecia in
a 14-year-old MNDSH cat that was presentedas a dermatology referral
(a).
A pulmonary mass was foundon thoracic radiography(dorsoventral
view, b) andconfirmed cytologically as anadenocarcinoma. Courtesy
ofDr Tim Nuttall
a
b
Cytology Relatively non-invasive
Minimal restraint often
sufficient
Minimal tissue disruption
Rapidly performed
Results obtained quickly
Cheaper
No architectural detail
Small numbers of cells
examined representative?
Limited assessment of tumour
type/grade
Histopathology More invasive
General anaesthesia (or
sedation) required
Moderate tissue disruption
More time-consuming
Delay in results
More expensive
Architecture apparent
Larger sample size
more representative?
More accurate assessment
of tumour type/grade
Comparison of cytology and histopathology
Key to appropriately managing cancer cases
is having an accurate diagnosis.
at FACULTAD DE FILOSOFIA Y LETRA on May 7,
2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/
-
7/24/2019 Cancer Feline
6/13
370 JFMS CLINICAL PRACTICE
R E V I E W /Cancer in cats an introduction
Sampling by cytology
Cytology will usually differentiate betweenneoplastic and
inflammatory lesions, anddetermine if tumours are malignant or
benign.Cytology will also broadly ascertain tumourtype (epithelial,
mesenchymal or round celltumour) but not the exact histogenesis;
forexample, sarcoma may be diagnosed, but his-
tology will be required to determine the tissueof origin. There
are other pitfalls to be wary oftoo: dysplastic epithelial or
mesenchymal cellsmay mimic neoplastic change, and this
isparticularly problematic where there is con-current
inflammation.
Fine needle aspirates may be non-diagnos-tic due to low yield in
some sarcomas. In cats,fine needle aspirates from lymph nodes
areless likely to be diagnostic of lymphoma thanin dogs, and it may
be impossible for theclinical pathologist to differentiate
lymphomafrom a very reactive node; in many cases,biopsy is
required. However, fine needle aspi-rates are very useful in
extranodal lymphoma,and cytology of bone marrow may helpsupport a
diagnosis of CNS lymphoma asmany affected cats are reported to have
bonemarrow involvement.
Cytology is also very useful in making adiagnosis from fluid
samples. In cases ofsuspected neoplastic effusion, the detection
oftumour cells in samples with low cellularitycan be enhanced by
preparing a sedimentsmear (see box).
Sampling by biopsy
Biopsy is more invasive than harvesting sam-ples for cytology,
and there are increased risksof haemorrhage, transplantation of
tumourcells, compromise of future surgery anddamage to adjacent
structures, although goodtechnique minimises these risks. If
suspiciousof an infectious cause, it is advisable not to fix
all biopsy tissue so the procedure does nothave to be repeated
to perform bacterial,fungal or mycobacterial culture. Tru-cut
biopsies are useful for samplingparenchymatous organs
non-invasively, butsamples are small. Tru-cut biopsies of
lymphnodes are not recommended as they are ofteninsufficient to
allow diagnosis of lymphoma,and may be no more sensitive than
fineneedle aspiration for the detection ofmetastatic disease. Punch
biopsies are most often used forskin lesions, but can be used for
samplingoral masses (although the defect is harder toclose than an
inverted wedge). They are oflittle value for lymph node biopsy.
Grab biopsies tend to be used to sampletissue from the respiratory
and alimentarytracts. Biopsy of suspected nasal tumours isbest
achieved through the external nares witha small set of cup biopsy
forceps. If these arenot available, a sharp bone curette can beused
to try to scoop out tumour, or a cut-offurinary catheter can be
inserted into themass, with gentle rotation and suction
The chances
of detecting
tumour cells
in effusion
samples with
low cellularity
can be
increased by
preparing a
sediment
smear.(a) Line smear from a thoracic effusion. The smear
isprepared in the same way as a blood smear, but instead ofcreating
a feathered edge, the aim is to create a line wherecells are
concentrated together. This is achieved by abruptlystopping
smearing mid-way and lifting the smearing slide off,creating a
line. The technique is illustrated in (b) and (c) using abloody
sample for easy visualisation
b
a
c
A sediment smear can be prepared in practice using the
urine setting on a StatSpin (or similar benchtop)
centrifuge;
the aim is to use the slowest spin to minimise cell
damage/destruction. The majority of the supernatant is
decanted off and the sediment is gently resuspended
before making the smear or line smear (as illustrated here),
and these samples are submitted along with the fluid sam-
ple in EDTA. For very haemorrhagic samples, the laborato-
ry can prepare a buffy coat smear to maximise the
chances of finding tumour cells. Care is required in inter-
preting fluid samples from body cavities, as reactive
mesothelial cells can look similar to neoplastic epithelial
cells; submission to a clinical pathologist is recommended.
S e d i m e n t s m e a r t e c h n i q u e
at FACULTAD DE FILOSOFIA Y LETRA on May 7,
2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/
-
7/24/2019 Cancer Feline
7/13
JFMS CLINICAL PRACTICE 371
REV IEW/Cancer in cats an introduction
applied to harvest a sample. Whichevermethod is employed, the
biopsyforceps/catheter should first be measuredagainst the patient
and the distance from theexternal nares to the medial canthus
markedon the biopsy tool (or the catheter cut justshort of this
length); it is vital that theinstrument is introduced no further
than thispoint, to avoid the risk of biopsying braintissue (Figure
4). Endoscopic grab biopsies from thegastrointestinal tract produce
small,superficial samples composed mainly of
mucosa. Multiple biopsies should be taken.In addition, biopsies
from both duodenumand ileum (ie, using both upper and
lowerendoscopy) are recommended in cases wherethe major
differentials are inflammatorybowel disease or lymphoma, as biopsy
froma single site is likely to fail to identifylymphoma in a
significant proportion of
cases.7 Full thickness biopsies may berequired in feline
intestinal disease. Incisional biopsies allow visualisationof
tissue and harvesting of larger samplesthan Tru-cut, punch or grab
biopsies. Wedgebiopsies are recommended to sampleaccessible masses,
such as oral masses. Whenharvesting incisional biopsies, ulcerated
andnecrotic areas should be avoided, as shouldthe junction between
normal and neoplastictissue, which would otherwise increase
thesurgical field. The biopsy site should beplanned so that the
entire biopsy tract can
be removed at definitive surgery. Excisional biopsy is indicated
for lymphnodes, some intestinal masses and formost mammary tumours
in cats, but isotherwise seldom indicated. This is
becauseinappropriate excisional biopsy canjeopardise future
treatment, and the firstsurgery offers the best chance of cure.
Thisis especially true for cats with soft tissuesarcomas. Reported
recurrence rates for felinesarcoma are in excess of 70%, and every
effortshould be made to avoid inappropriatemanagement.
Clinical staging
Clinical staging involves assessment of theprimary tumour (T),
including involvement ofadjacent structures, and assessment for
metas-tasis to local and regional lymph nodes (N)and distant sites
(M). The aim of TMN stagingis to inform clinical decision making
andensure the best treatment possible under theindividual
circumstances of the case.
Assessment of the primary tumour shouldinclude evaluation of
extent, by clinical exam-ination and appropriate diagnostic
imaging
Figure 4 (a) Unilateral nasal discharge in a2-year-old MN
Siamese cat. Biopsies in thiscase confirmed lymphoma. When
takingbiopsies from nasal tumours, it is important firstto measure
the grab biopsy forceps or cut-offurinary catheter either against
the patient sothat the biopsy/catheter is not inserted anyfurther
than the level of the medial canthus, oragainst a dorsoventral
intraoral radiograph (b) toensure the biopsy/catheter ends within
tumourand cranial to the cribriform plate
a
b
Sampling of feline skin lesionsBenign epithelial tumours and
papillomas are uncom-
mon in cats, and 5060% of skin tumours are malignant.
Non-neoplastic conditions may also present as
proliferative or ulcerative lesions, including eosinophilic
granuloma complex, flea allergic dermatitis, mycoses,
poxvirus, dermatophytoses and immune-mediated disease.
The commonest skin tumours are basal cell tumours
(probably these were over-diagnosed historically),
squamous cell carcinomas, mast cell tumours and
fibrosarcomas.8 Excisional biopsy is generally not
recommended for feline skin tumours. Fine
needle aspiration or biopsy is recommended
to identify those lesions where local
excision is inappropriate.
Inappropriate
excisional
biopsy can
jeopardise
future
treatment.
at FACULTAD DE FILOSOFIA Y LETRA on May 7,
2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/
-
7/24/2019 Cancer Feline
8/13
372 JFMS CLINICAL PRACTICE
REV IEW/Cancer in cats an introduction
or endoscopic techniques, and a diagnosis oftumour type based on
cytology or histology(see earlier). The sensitivity of tests should
beborne in mind. For example, clinical examina-tion of a maxillary
squamous cell carcinomamay suggest a less extensive tumour
thanwould radiography, which in turn is lesssensitive than computed
tomography (CT).
Exploratory laparotomy in a suspected orconfirmed cancer patient
should always con-tribute to tumour staging (see box).
Lymph node evaluation
Carcinomas most commonly metastasise bythe lymphatic route, and
local and regionallymph nodes should be evaluated in cats with
carcinoma by palpation (eg, of axillary andinguinal nodes in
cats with mammarytumours), diagnostic imaging, and aspirationand
cytology. Mast cell tumours also metasta-sise by the lymphatic
route, but reportedmetastatic rates for cutaneous mast celltumours
in cats vary, ranging from 022%,and most histologically
well-differentiatedtumours have a low metastatic potential.Poorly
differentiated tumours are moremalignant. (Visceral mast cell
tumours aregenerally malignant and metastases may bewidespread at
presentation.)
Thoracic radiographs
Primary lung tumours are relatively readilydiagnosed
radiographically (Figures 2 and 3).Compared with dogs, cats less
frequentlydevelop classical well-defined cannon ballmetastases, and
metastatic disease can appearas ill-defined mass lesions or diffuse
alveolar,interstitial or mixed patterns (Figure 5).9 Abronchial
component is relatively commonin metastatic patterns in
bronchoalveolarcarcinoma.10 Cytology of lung aspirates
orbronchoalveolar lavage fluid may be requiredto confirm a
diagnosis.
Abdominal ultrasoundMass lesions and markedly enlarged
lymphnodes may be detectable on abdominal pal-pation, but abdominal
ultrasound allowsdetection of lesions not apparent on
clinicalexamination, including lesions within hepatic,splenic and
renal parenchyma, as well aschanges in layering of the
gastrointestinaltract and more subtle lymph node enlarge-ment.
Advanced imaging
Advanced imaging is increasingly availablefor veterinary
patients, and is very valuable.However, it is expensive, and, as
with anydiagnostic test, should be utilised with full
consideration of the value of the study andthe cost implications
for future managementof the case. When mass lesions are
found,samples should be harvested to allow adiagnosis.
Have a plan: do not perform a peek and shriek!
Achieve adequate access
Biopsy (or fine needle aspirate) any suspicious
lesions
Examine/fine needle aspirate/biopsy local and
regional nodes
Examine/fine needle aspirate/biopsy
parenchymatous organs
If you resect a mass
Think about your margins
Resect adhesions with the mass
Discard contaminated instruments (tumour
or gastrointestinal contents)
Decide if you should place a feeding tube
(Keep a fresh piece of tissue for culture if
suspicious of a granulomatous lesion)
Figure 5 Lateral thoracic radiograph (inflated) of an elderly FN
DSH cat. Multiple poorlydefined soft tissue opacities are seen,
which represent metastases from an unknown primary.There are also
increased interstitial and bronchial markings
Compared
with dogs, cats
less frequently
develop
classical
well-definedcannon ball
metastases.
E x p l o r a t o r y l a p a r o t o m y a n d t u m o u r s t
a g i n g
The importance of clinical staging is sometimes forgotten during
abdominal surgery, particularly
when exploratory surgery is performed and a mass is discovered.
At the time of surgery, there is the
opportunity to assess the primary tumour/mass and also to
evaluate other organs. Some pointers
for getting the best outcome from exploratory laparotomy are
given below.
at FACULTAD DE FILOSOFIA Y LETRA on May 7,
2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/
-
7/24/2019 Cancer Feline
9/13
JFMS CLINICAL PRACTICE 373
REV IEW/Cancer in cats an introduction
Computed tomography is most useful forevaluation of tumours
where there is likely
to be skeletal involvement, and is generallyrequired for
radiation planning (Figure 6).CT is also useful for the
identificationand staging of pulmonary neoplasia(including
evaluation of bronchial nodes)and pulmonary metastatic disease.
Magnetic resonance imaging is usefulfor the evaluation of soft
tissue lesions andlesions in the CNS. It is particularly valuablein
planning surgery in cases of soft tissuesarcoma.
Blood testsMost blood tests do not help to make a diag-nosis of
cancer in cats, but they can help toidentify common co-morbidities,
and this canbe very important in decision making.
On haematology, there may be a mildnon-regenerative anaemia and
a stress haem -ogram. These are the commonest findingsin lymphoma
patients.11 Abnormal circulatingcells and/or lymphocytosis is
relatively
uncommon. Even in cats with leukaemia, theremay be no abnormal
circulating cells on
haematology.On biochemistry, changes are often non-
specific and may reflect stress (eg, hyper-glycaemia),
co-morbidity or organ involve-ment (eg, hypoalbuminaemia in
diffusealimentary lymphoma). Urine specific gravityshould be
measured in azotaemic patients toconfirm renal or pre-renal origin.
(Urinespecific gravity will be low in azotaemichypercalcaemic
patients even if the renal con-centrating ability is normal because
of antago-nism of antidiuretic hormone.)
Paraneoplastichypercalcaemia is uncommon in cases offeline
lymphoma, and is more commonly seenin patients with myeloma.
Hypercalcaemiacan also be seen with other tumours, particu-larly
carcinomas.
In the UK, most cats with lymphoma noware FeLV antigen negative
on ELISA.However, testing is valid where there is aninfection risk
to others, and where concurrentdisease may affect treatment
decision making.
Figure 6 (a) Transverse CTscan of an 8-year-old MNDSH cat with
poorlycontrolled diabetes mellitusdue to acromegaly, showing
a mass in the pituitary fossa.The positioning device seenis a
thermoplastic mould,which is shaped round thepatient, whose head
issupported on a mouldablepillow (not visible on thiswindow). The
mould issecured to a baseplate.(b) CT scan of a 7-year-oldFN cat
with a nasal tumour(extending into the orbit)after positioning in
the samemould system (c)
a
cb
The aim of staging is to inform clinical decision making and
ensure
the best treatment possible under the individual circumstances
of the case.
PItuitary tumour
Thermoplasticmould
Baseplate
at FACULTAD DE FILOSOFIA Y LETRA on May 7,
2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/
-
7/24/2019 Cancer Feline
10/13
374 JFMS CLINICAL PRACTICE
R E V I E W /Cancer in cats an introduction
Treatment options andconsiderations
In broad terms, surgery and radiotherapy canbe considered as
local treatments for primarydisease or primary disease with local
lymphnode involvment, and chemotherapy as sys-temic treatment for
disseminated disease.
Surgery
In cats, treatment of primary mass lesionsmay be limited by
small patient size and dif-ficulties in achieving wide local
excision.However, surgery remains the mainstay oftreatment for
solid tumours.
Mammary tumours are most often resectedby radical mastectomy, as
most feline mamma-ry tumours are malignant. Both axillary
andinguinal lymph nodes on the affected sideshould be resected en
bloc with the mammary
tissue, but often the axillary nodes are notremoved if deemed
normal as they are lessreadily identifiable than the inguinal
nodes.Local excision of malignant mammary tumoursis associated with
a high rate of recurrence.
Oral tumours are often unresectable by thetime of presentation:
the overall cure rate fororal squamous cell carcinoma is less than
5%.Where excision is possible, considerationshould be given to
placing a feeding tube at thetime of surgery to facilitate
postoperative careand recovery, as cats may cope less well with,for
example, mandibulectomy than dogs do,particularly in the immediate
postoperativeperiod. Cosmetic and functional results may bevery
good in the longer term (Figure 7).
Excision of soft tissue sarcomas, which mayhave extensive fronds
of invading tumourcells, is particularly challenging in
smallpatients, and compartmental excision is onlyachievable for
tumours on (distal) limbs.
Radiotherapy
Radiation therapy is most often used either as apostoperative
adjunctive therapy, ideally in aminimal residual disease setting,
or palliativelyin the face of unresectable gross disease. When
radiation is used postoperatively, it is veryimportant to ensure
that the radiation therapistis aware of the original tumour site,
extent anddimensions, or the planned radiation field maynot include
all of the affected tissue. This canresult in a geographical miss,
where microscop-ic residual disease is not included in the
treatedarea. The risk of geographical miss increases asrepeat
surgeries are performed and normalanatomy becomes increasingly
distorted.
The best results are likely to be achieved ifradiotherapy is
considered prior to surgery,and presurgical measurements and images
areavailable (ie, photographs with measurements,drawings,
radiographic or other images) tohelp plan the treatment. Placement
of metalsurgical clips at the margins of the surgical bedalso helps
to avoid geographical miss duringradiotherapy, as there may be
migration ofsubcutaneous tissues that may contain residual
tumour (Figure 8).
Figure 7 An 8-year-old MNDSH cat, which presentedwith an early
mandibularfibrosarcoma. A partialmandibulectomy wasperformed, and a
feedingtube placed, visible in (a),which shows the patient2 days
postsurgery.(b) The cat 6 months later.In this case, surgery
wascurative, but complete
excision of feline oraltumours is frequentlyimpossible
ba
Surgery
remains the
mainstay of
treatment for
solid tumours
Figure 8 Dorsoventral radiograph obtained to check the radiation
field in an adult MN DSH catreceiving postoperative adjunctive
radiation therapy for an incompletely resected soft tissuesarcoma.
The solid line is the scar, and dots represent a margin round this
of 5 cm. Two of the dotsalong the caudal margin are joined by a
dotted line to show where the caudal edge of the treatmentfield
lies. Two clips are positioned beyond (caudal to) this margin,
indicating that a larger marginmust be used. This illustrates the
limitations of basing radiation treatment fields on surgical
scars
at FACULTAD DE FILOSOFIA Y LETRA on May 7,
2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/
-
7/24/2019 Cancer Feline
11/13
JFMS CLINICAL PRACTICE 375
REV IEW/Cancer in cats an introduction
In the clinic, radiation therapy is used to treatfeline patients
in a variety of ways (see box). Pituitary tumours in acromegalic
cats(Figure 6) are one of the most commonindications for
teletherapy. Soft tissue sarcomas (Figures 8 and 9)are also
commonly treated using teletherapy,mostly following surgical
resection. The
majority of the published work in this areahas focused on
injection site-associatedsarcomas. Good presurgical tumourrecording
is essential for these patients, andthe risk of recurrence is
greater if radiation iscarried out after multiple surgeries. Nasal
and paranasal tumours (Figure 6b,c)may be treated with
radiotherapy, and this isthe treatment of choice for nasal
carcinomas. Itsuse in nasal lymphoma is controversial as thesecats
may relapse with lymphoma in other sites.In the authors hospital,
patients with nasallymphoma are most often treated
withchemotherapy, with radiation used as a rescuetherapy if there
is relapse of the nasal disease.A study comparing survival in
patients treatedwith radiotherapy alone, chemotherapy alone,or both
modalities, showed no difference inoutcome between groups.12
Abdominal cavity lymphoma has morerecently been treated with
radiation therapyused in conjunction with chemotherapy or asa
rescue therapy.13,14
Oral squamous cell carcinoma (Figure 10)has been treated with a
variety of radiationtherapy protocols, but results have been
fairlydisappointing, with short median survival
times (2 or 3 months in most studies).1517
Oncologists continue to try to find aneffective protocol for
this disease, withlimited success, though a recent pilot studyof
multimodality therapy reported survivalof greater than a year in
3/6 cats.18
Superficial cutaneous or rhinarialsquamous cell carcinoma may be
treatedusing electrons of different energies, withtheir variable
penetrations, though treatmentwith strontium is preferred as this
can bedelivered as a single treatment rather thanmultiple
fractions. Photodynamic therapy(PDT) may also be appropriate for
superficiallesions, but recurrence is common. Eitherradiotherapy or
PDT may achieve long-termcontrol after a single treatment in
very
superficial lesions,19but relapse is morecommon after PDT.20,21
Topical imiquimodhas also been reported to produce
clinicalremission. For invasive tumours, surgicalexcision is the
treatment of choice.
Figure 9 A 9-year-old MN Birman being prepared forpostoperative
adjunctive radiation therapy using electrons,for treatment of an
incompletely excised, high grade injectionsite-associated sarcoma.
The electron applicator has acut out made to shape the field for
the individual patient.The treatment field is illuminated on the
patient.Unfortunately, this cat, which also received
chemotherapywith epirubicin, developed widespread metastatic
disease(but no local recurrence) 18 months after radiotherapy
Figure 10 A 14-year-old MNDSH cat with a maxillarysquamous cell
carcinomaat the beginning (a) andend (b) of a course
ofhypofractionated radiationtherapy for a gingivalsquamous cell
carcinoma.
After an initial favourableresponse, the tumourrecurred and the
patientwas euthanased just over3 months after radiotherapy
b
Radiationtherapy is most
often used as a
postoperative
adjunctive
therapy, or
palliatively
in the face of
unresectablegross disease.
R a d i o t h e r a p y m e t h o d s u s e d i n c a t s
Systemic administration of iodine 131 (gamma and beta emitter)
is used,
for example, to treat hyperthyroidism.
Brachytherapy (internal radiation therapy) using a strontium 90
wand,
which produces beta particles with a maximum penetration of 34
mm, is
used to treat superficial (non-oral) squamous cell
carcinoma.
Teletherapy (external beam radiation) is delivered using
linear
accelerators producing x-rays (photons) at 420 MV. These high
energy x-rays are deeply penetrating, and high energy beams allow a
more uniform
distribution of dose, particularly for deep tumours and those
involving bone.
Some linear accelerators also produce electrons in a range of
energies,
which are variably penetrating, allowing treatment of
superficial lesions and
avoidance of toxicity to deep structures, which is useful in
small patients
like cats. Radiation therapy using these sources requires
multiple treatments
(usually between three and 20) delivered under general
anaesthesia.
a
Applicator
Cut out
Treatment field
(illuminated)
at FACULTAD DE FILOSOFIA Y LETRA on May 7,
2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/
-
7/24/2019 Cancer Feline
12/13
376 JFMS CLINICAL PRACTICE
R E V I E W /Cancer in cats an introduction
Chemotherapy
Chemotherapy is used where systemic deliv-ery of treatment is
required to treat widelydisseminated but chemoresponsive
disease(eg, lymphoma) or where there is a high riskof development
of metastatic disease andmicrometastases are likely to be present
(eg,some high grade sarcomas). It is generally not
a suitable option as the primary treatment fora large solid
non-lymphoid tumour, which islikely to be poorly chemosensitive.
Lymphoma The optimum protocolfor feline lymphoma remains to
bedetermined.2224 This, at least in part, reflectsthe larger
variation in clinical forms oflymphoma seen in cats compared with
dogs.The role of doxorubicin/epirubicin
remainscontroversial.22,24,25 Lymphoma is reviewedelsewhere2630 and
extranodal disease withinthe current special issue. Some cats
withlymphoma will respond very well tochemotherapy, and the best
prognosticindicator is achieving complete remission.Individual cats
may need more adjustmentof their protocol than dogs, but this is
notinsurmountable. The major challenge intreating feline lymphoma
remains the poorresponse of cats to rescue therapy comparedwith
dogs, though some cats will do wellwith lomustine as a rescue
agent.31
Soft tissue sarcoma The impact ofchemotherapy on survival of
cats with highgrade (grade 3) soft tissue sarcomas isunproven, with
most work concentratingon injection site/vaccine-associated
sarcomas.32,33 However, there may be apositive impact on
disease-free interval andpossibly local tumour control in
patientsreceiving radiotherapy and chemotherapywith
doxorubicin,33,34 and multimodalitytreatment is recommended.35
Mast cell tumour Chemotherapy is lesscommonly used for the other
tumours that
readers may be familiar with in dogs(eg, metastatic mast cell
tumours,osteosarcoma), because of differing biologicalbehaviour of
the tumours, and differingresponses and drug toxicities across
species.The role of chemotherapy for palliative oradjuvant
treatment of feline mast celltumours has not been clearly
established,36
and chemotherapy is generally reserved forcats with
histologically poorly differentiated,locally invasive and/or
metastatic tumours.Vinblastine, chlorambucil and lomustine havebeen
used. One study reports an overallresponse rate of 50% in cats with
measurabledisease treated with lomustine, and a medianduration of
response of 168 days.37 There isno proven role for corticosteroids
in thetreatment of feline mast cell tumours.
Further discussion on the use of chemother-apy and targeted
therapies in cats, with aparticular focus on the idiosyncracies of
felinepatients, is provided in an accompanyingarticle in this
special issue.
Funding
The author received no specific grant from anyfunding agency in
the public, commercial or not-for-profit sectors for the
preparation of this article.
Conflict of interest
The author does not have any potential conflicts ofinterest to
declare.
Cancer is a differential for cats with
mass lesions and many non-specific
clinical signs.
For many cancers in cats, early
treatment holds the only chance of cure:
raising awareness is important,
particularly for squamous cell
carcinomas and soft tissue sarcomas.
Diagnosis and staging inform clinical
decision making; tests should be chosen
sensibly (and cost effectively when
funds are limited), based on the
information required.
Inappropriate excisional biopsy can
jeopardise future treatment, particularly
for soft tissue sarcomas.
Radiotherapy and chemotherapy are
evolving fields in feline medicine and
there is still much to learn.
KEYPOINTS
Chemotherapy
is used to treat
widely
disseminated but
chemoresponsive
disease
(eg, lymphoma)
or where there is
a high risk of
development of
metastatic
disease.
Targeted therapiesTyrosine kinase inhibitors (TKIs) have been
used to
treat cats with cancer, though neither masitinib nor
toceranib is licensed in this species. There is limited data
on toxicity and efficacy. The main target tumours are
mast cell tumours, injection site/vaccine-associated
sarcomas and possibly squamous cell carcinoma.
Combination TKI and radiation therapy is being
investigated in the treatment of sarcomas and oral
squamous cell carcinomas. The main potential
toxicities of the TKIs are gastrointestinal
toxicity and myelosuppression, and
nephrotoxicity should also be
monitored for.
at FACULTAD DE FILOSOFIA Y LETRA on May 7,
2013jfm.sagepub.comDownloaded from
http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/
-
7/24/2019 Cancer Feline
13/13
JFMS CLINICAL PRACTICE 377
REV IEW/Cancer in cats an introduction
References
1 Goldfinch N and Argyle DJ. Feline lungdigit syndrome:
unusu-
al metastatic patterns of primary lung tumours in cats. J
Feline
Med Surg 2012; 14: 202208.
2 Corr SA and Blackwood L. What is your diagnosis? Primary
pulmonary tumour (carcinoma) with digital metastases.J Small
Anim Pract 2003; 44: 201, 240xiii.
3 Kasabalis D, Mylonakis ME, Patsikas MN, Petanides T
andKoutinas AF. Paraneoplastic exfoliative erythroderma in a
cat
with thymoma.J Hellenic Vet Med Soc 2011; 62: 229234.
4 Smits B and Reid MM. Feline paraneoplastic syndrome
associat-
ed with thymoma. N Z Vet J 2003; 51: 244247.
5 Tasker S, Griffon DJ, Nutttall TJ and Hill PB. Resolution of
para-
neoplastic alopecia following surgical removal of a
pancreatic
carcinoma in a cat.J Small Anim Pract 1999; 40: 1619.
6 Marconato L, Albanese F, Viacava P, Marchetti V and Abramo
F.
Paraneoplastic alopecia associated with hepatocellular
carcino-
ma in a cat. Vet Dermatol 2007; 18: 267271.
7 Scott KD, Zoran DL, Mansell J, Norby B and Willard MD.
Utility
of endoscopic biopsies of the duodenum and ileum for diagno-
sis of inflammatory bowel disease and small cell lymphoma in
cats.J Vet Intern Med 2011; 25: 12531257.
8 Murphy S. Skin neoplasia in small animals 3. Common canine
tumours. In Pract 2006; 28: 398402.
9 Forrest LJ and Graybush CA. Radiographic patterns of pul-
monary metastasis in 25 cats. Vet Radiol Ultrasound 1998; 39:
48.
10 Ballegeer EA, Forrest LJ and Stepien RL. Radiographic
appear-
ance of bronchoalveolar carcinoma in nine cats. Vet Radiol
Ultrasound 2002; 43: 267271.
11 Gabor LJ, Canfield PJ and Malik R. Haematological and
bio-
chemical findings in cats in Australia with lymphosarcoma.
Aust Vet J2000; 78: 456461.
12 Haney SM, Beaver L, Turrel J, Clifford CA, Klein MK, Crawford
S,
et al. Survival analysis of 97 cats with nasal lymphoma: a
multi-
institutional retrospective study (19862006). J Vet Intern
Med2009; 23: 287294.
13 Parshley DL, LaRue SM, Kitchell B, Heller D and Dhaliwal
RS.
Abdominal irradiation as a rescue therapy for feline gastro-
intestinal lymphoma: a retrospective study of 11 cats
(20012008). J Feline Med Surg 2011; 13: 6368.
14 Williams LE, Pruitt AF and Thrall DE. Chemotherapy
followed
by abdominal cavity irradiation for feline lymphoblastic
lym-
phoma. Vet Radiol Ultrasound 2010; 51: 681687.
15 Fidel JL, Sellon RK, Houston RK and Wheeler BA. A
nine-day
accelerated radiation protocol for feline squamous cell
carcino-
ma. Vet Radiol Ultrasound 2007; 48: 482485.
16 Bregazzi VS, LaRue SM, Powers BE, Fettman MJ, Ogilvie GK
and
Withrow SJ. Response of feline oral squamous cell carcinoma
to
palliative radiation therapy. Vet Radiol Ultrasound 2001; 42:
7779.
17 McDonald C, Looper J and Greene S. Response rate and
duration
associated with a 4gy 5 fraction palliative radiation protocol.
Vet
Radiol Ultrasound 2012; 53: 358364.
18 Marconato L, Buchholz J, Keller M, Bettini G, Valenti P and
Kaser-
Hotz B. Multimodal therapeutic approach and
interdisciplinary
challenge for the treatment of unresectable head and neck
squa-
mous cell carcinoma in six cats: a pilot study. Vet Comp Oncol.
Epub
ahead of print 23 March 2012. DOI:
10.1111/j.1476-5829.2011.00304.x.
19 Hammond GM, Gordon IK, Theon AP and Kent MS. Evaluation
of strontium Sr 90 for the treatment of superficial squamous
cell
carcinoma of the nasal planum in cats: 49 cases (19902006).J
Am
Vet Med Assoc 2007; 231: 736741.
20 Buchholz J, Wergin M, Walt H, Grfe S, Bley CR and
Kaser-Hotz
B. Photodynamic therapy of feline cutaneous squamous cell
car-
cinoma using a newly developed liposomal photosensitizer:
preliminary results concerning drug safety and efficacy. J
Vet
Intern Med 2007; 21: 770775.
21 Bexfield NH, Stell AJ, Gear RN and Dobson JM.
Photodynamic
therapy of superficial nasal planum squamous cell carcinomas
in cats: 55 cases.J Vet Intern Med 2008; 22: 13851389.
22 Milner RJ, Peyton J, Cooke K, Fox LE, Gallagher A, Gordon P,
et al.Response rates and survival times for cats with lymphoma
treat-
ed with the University of WisconsinMadison chemotherapy pro-
tocol: 38 cases (19962003).J Am Vet Med Assoc2005; 227:
11181122.
23 Teske E, Van Straten G, Van Noort R and Rutteman GR.
Chemotherapy with cyclophosphamide, vincristine, and pred-
nisolone (COP) in cats with malignant lymphoma: new results
with an old protocol.J Vet Intern Med 2002; 16: 179186.
24 Simon D, Eberle N, Laacke-Singer L and Nolte I.
Combination
chemotherapy in feline lymphoma: treatment outcome, tolera-
bility, and duration in 23 cats.J Vet Intern Med 2008; 22:
394400.
25 Oberthaler KT, Mauldin E, McManus PM, Shofer FS and
Sorenmo
KU. Rescue therapy with doxorubicin-based chemotherapy for
relapsing or refractory feline lymphoma: a retrospective
study
of 23 cases.J Feline Med Surg 2009; 11: 259265.
26 Hayes A. Feline lymphoma 1. Principles of diagnosis and
man-
agement. In Pract 2006; 28: 516524.
27 Hayes A. Feline lymphoma 2. Specific disease
presentations.
In Pract 2006; 28: 578585.
28 Lingard AE, Briscoe K, Beatty JA, Moore AS, Crowley AM,
Krockenberger M, et al. Low-grade alimentary lymphoma:
clini-
copathological findings and response to treatment in 17 cases
.
J Feline Med Surg 2009; 11: 692700.
29 Barrs VR and Beatty JA. Feline alimentary lymphoma: 1.
Classification, risk factors, clinical signs and non-invasive
diag-
nostics.J Feline Med Surg 2012; 14: 182190.
30 Barrs VR and Beatty JA. Feline alimentary lymphoma: 2.
Further
diagnostics, therapy and prognosis. J Feline Med Surg 2012;
14:191201.
31 Dutelle AL, Bulman-Fleming JC, Lewis CA and Rosenberg MP.
Evaluation of lomustine as a rescue agent for cats with
resistant
lymphoma.J Feline Med Surg 2012; 14: 694700.
32 Eckstein C, Guscetti F, Roos M, Martn de Las Mulas J,
Kaser-Hotz
B and Rohrer Bley C. A retrospective analysis of radiation
therapy for the treatment of feline vaccine-associated
sarcoma.
Vet Comp Oncol 2009; 7: 5468.
33 Hahn KA, Endicott MM, King GK and Harris-King FD.
Evaluation of radiotherapy alone or in combination with dox-
orubicin chemotherapy for the treatment of cats with incom-
pletely excised soft tissue sarcomas: 71 cases (19891999). J
Am
Vet Med Assoc 2007; 231: 742745.
34 Poirier VJ, Thamm DH, Kurzman ID, Jeglum KA, Chun R,
Obradovich JE, et al. Liposome-encapsulated doxorubicin
(Doxil) and doxorubicin in the treatment of
vaccine-associated
sarcoma in cats.J Vet Intern Med 2002; 16: 726731.
35 Martano M, Morello E and Buracco P. Feline injection-site
sarcoma: past, present and future perspectives. Vet J2011;
188:
136141.
36 Henry CJ and Herrera CL. Mast cell tumors in cats:
clinical
update and possible new treatment avenues. J Feline Med Surg
2013; 15: 4147.
37 Rassnick KM, Williams LE, Kristal O, Al-Sarraf R, Baez JL,
Zwahlen
CH, et al. Lomustine for treatment of mast cell tumors in
cats:
38 cases (19992005).J Am Vet Med Assoc 2008; 232: 12001205.
Available online at jfms com t FACULTAD DE FILOSOFIA Y LETRA M 7
2013jf bD l d d f
http://localhost/var/www/apps/conversion/tmp/scratch_7/jfms.comhttp://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://jfm.sagepub.com/http://localhost/var/www/apps/conversion/tmp/scratch_7/jfms.com