Embed Size (px)
Citation preview

C
1
2
A
mvnscBb
T
1h
Critical Reviews in Oncology/Hematology 85 (2013) 239–256
Cancer-associated genodermatoses: Skin neoplasms as clues to hereditarytumor syndromes
Giovanni Ponti a,∗, Giovanni Pellacani b, Stefania Seidenari b, Annamaria Pollio c,Umberto Muscatello d, Aldo Tomasi a
a Department of Clinical and Diagnostic Medicine and Public Health, University Hospital of Modena and Reggio Emilia, Italyb Department of Head and Neck Surgery, Division of Dermatology, University Hospital of Modena and Reggio Emilia, Italy
c Department of Odontostomatological and Maxillofacial Sciences, Oral Medicine Unit, School of Medicine and Surgery, Federico II University of Naples,Italy
d CNR - Nanoscience Institute, S3 Center, University of Modena and Reggio Emilia, Modena, Italy
Accepted 3 July 2012
ontents
. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2401.1. Neurofibromatosis type I . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2401.2. Brooke–Spiegler syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2421.3. Muir–Torre syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2431.4. Gardner’s syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2441.5. Nevoid basal cell carcinoma syndrome (Gorlin syndrome) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2461.6. Cowden syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2481.7. Birt–Hogg–Dubé syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2491.8. Hereditary leiomyomatosis and renal cell cancer (HLRCC) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 250
. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 251Search strategy and selection criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 252Conflict of interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 252Reviewer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 252Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 252References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 252Biographies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 256
bstract
Characteristic skin neoplasms are associated with a large number of hereditary tumor syndromes and their knowledge and early detectionay facilitate the diagnosis of the underlying malignancies. We will review the clinical and dermatopathological aspects of cutaneous and
isceral lesions and the recent progresses in understanding the etiology, pathogenesis and therapies of selected tumor syndromes. The skineoplasms we chose to consider are multiple neurofibromas in neurofibromatosis, cylindromas and trichoepitheliomas in Broke–Spiegleryndrome, sebaceous tumors and keratoacanthomas in Muir–Torre syndrome, Gardner fibromas in Gardner syndrome, multiple basal cellarcinomas in nevoid basal cell carcinoma (Gorlin) syndrome, multiple tricholemmomas in Cowden syndrome, multiple fibrofolliculomas inirt–Hogg–Dubé syndrome and multiple leiomyomas in hereditary leiomyomatosis and renal cell cancer. Hereditary cancers have distinct
nterparts; for this reason, we are now able to experiment new treatment
iological and clinical features as compared to their sporadic cou∗ Corresponding author at: Department of Clinical Pathology, University of Modena and Reggio Emilia, via del Pozzo 7, 41100 Modena, Italy.el.: +39 059 4224748; fax: +39 059 4222647.
E-mail address: [email protected] (G. Ponti).
040-8428/$ – see front matter © 2012 Elsevier Ireland Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.critrevonc.2012.07.001

2
am©
Ks
1
welcicshss(apBlahwwttnaorm[
McBabmlTtptma
cfa
40 G. Ponti et al. / Critical Reviews in Oncology/Hematology 85 (2013) 239–256
pproaches involving not only tumor detection and prevention, but also tailored therapeutic strategies focusing on the peculiar druggableolecular targets.2012 Elsevier Ireland Ltd. All rights reserved.
eywords: Hereditary cancer syndrome; Neurofibromatosis; Broke–Spiegler syndrome; Muir–Torre syndrome; Gardner syndrome; Gorlin syndrome; Cowden
tnneftmma
dpvgdst
1
dcp1crcfiiteoofTwf
smvw
e
yndrome; Birt–Hogg–Dubé syndrome
. Introduction
Several hereditary tumor syndromes are associatedith unique cutaneous findings which may facilitate an
arly diagnosis as a reliable marker for the risk of deve-oping internal malignancies. Hereditary tumor syndromesover a wide phenotypic spectrum ranging from a benignnherited predisposition to develop cutaneous lentiginesonnected with a systemic disease, to associations witheveral syndromes carrying increased risk of developingamartomas, hyperplasias, and other neoplasms. Theseyndromes comprise Muir–Torre syndrome associated withebaceous neoplasms, PTEN hamartoma tumor syndromeBannayan–Riley–Ruvalcaba/Cowden/Proteus disease)ssociated with multiple tricholemmomas, Carney com-lex associated with multiple superficial angiomyxomas,irt–Hogg–Dubé syndrome associated with multiple fibrofo-
liculomas, tuberous sclerosis associated with multiple facialngiofibromas and so-called Koenen tumors, patients withereditary leiomyomatosis and renal cell cancer syndromeith cutaneous leiomyomas, Gardner syndrome associatedith Gardner fibromas, nevoid basal cell carcinoma associa-
ed with multiple basal cell carcinomas in young patients andypes 1 and 2 neurofibromatosis, associated with multipleeurofibromas. Common features of the syndromes include:n autosomal-dominant pattern of inheritance, developmentf cancer at an early age, tumor multiplicity, presence ofare histotypes and occurrence of various extra cutaneousanifestations, which characterize each specific phenotype
1].The clinical aspects of NF1, Broke–Spiegler syndrome,
uir–Torre syndrome, Gardner syndrome, nevoid basal cellarcinoma syndrome (Gorlin syndrome), Cowden syndrome,irt–Hogg–Dubé syndrome and hereditary leiomyomatosisnd renal cell cancer are here reviewed in a personal way,asing on our clinical experience. Despite their rarity, theolecular basis of many of these syndromes has been partia-
ly clarified with the identification of the responsible gene.hese findings contributed (in most syndromes) to support
he relevance of the Knudson’s two-hit hypothesis in theathogenesis of inherited tumors and shed further light onhe peculiar mechanisms involved in the synchronous and/oretachronous tumorigenesis processes of different organs
nd districts.There is no doubt that hereditary tumor syndromes will
ontinue to represent an excellent model for the study ofamilial cancer. The discovery of the molecular mechanismsssociated to hereditary tumors contributed significantly to
eMt
he understanding of the basic mechanisms of sporadic malig-ancies and might be the milestone for the development ofovel tailored treatment strategies. Further research shouldlucidate the genotype–phenotype correlations, the specificunctioning of the genes and proteins involved in the inheri-ed and sporadic tumorigenesis, as well as the role of possible
odifier genes that might be responsible for the great intrafa-ilial and interfamilial phenotypic variability, which remains
n unexplained paradox of several genetic disorders.Tumors arising in patients with hereditary cancer syn-
romes may have peculiar drug sensitivity. While the initialractical interest on cancer genetic research was limited toarious aspects of cancer detection and prevention, it is nowetting increasingly recognized that hereditary tumors haveistinct biological and clinical features as compared to theirporadic counterparts and thus require tailored treatment stra-egies [2].
.1. Neurofibromatosis type I
NF1 (MIM# 162200), also called “von Recklinghausenisease” or “peripheral neurofibromatosis” is one of the mostommon autosomal dominant disorders, with virtually 100%enetrance by adulthood [3]. The prevalence of NF1 is aboutin 3000–4000 live births [4]. Diagnosis is based on the
linical criteria recommended by a NIH Consensus Confe-ence [5], which include multiple café-au-lait spots (CLS),utaneous or subcutaneous neurofibromas, plexiform neuro-bromas, axillary or inguinal freckling, optic gliomas, and
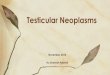
ris Lisch nodules (Table 1). Although the three characteris-ic features (CLS, neurofibromas, and Lisch nodules) occurach in over 90% of all NF1 patients by puberty, the numberf lesions is highly variable (Fig. 1). Approximately 30–40%f NF1 patients may develop larger and more complex plexi-orm neurofibromas associated with major nerve trunks [6].hese congenital benign tumors often grow in associationith the major nerve tracts, where they may involve multiple
ascicles and branches of the nerves (Fig. 7a) [7].NF1 patients are also predisposed to develop dysplastic
keletal lesions, learning difficulties or mental retardation,yeloid leukemias and other malignancies, and may exhibit
ascular abnormalities, thus implicating the NF1 gene in aide variety of tissues and disease processes [8].The NF1 gene is located at 17q11.2, it contains 60
xons spanning approximately 350 kb of genomic DNA, and
ncodes a 12-kb transcript [9] (GDB: 120231; Gen-Bank:82814). The gene product, neurofibromin, has an estima-ed molecular weight of 327 kDa and is a negative regulator of

G.Pontietal./C
riticalReview
sin
Oncology/H
ematology
85(2013)
239–256241
Table 1The main genodermatoses: clinical manifestations and genetics features.
Disease Neurofibromatosis NF1 Brooke–SpieglerBSS
Muir–Torre MTS Gardner GS Gorlin BCNS Cowden CS Birt–Hogg–DubeBHDS
Hereditaryleiomyomato-sis and renalcell cancerHLRCC
MIM 162200 605041 158320 175100 109400 158350 135150 150800Gene/locus/inheritane NF1
17q11.2AD
CYLD16q12-q13AD
MSH2 2p22-p21MLH1 3p21.3MSH6AD
APC 5q21AD
PTCH9q22.3AD
PTEN10q23.31AD
FLCN(folliculin)17p11.2AD
FH1q42-1q44
Skin findings cafe-au-lait spots, cutaneous andsubcutaneous neurofibromas,axillary freckling
Folliculosebaceous-apocrineneoplasms:cylindroma,trichoepitheliomasand spiradenomas;basal cellcarcinomas
Multiple sebaceoustumors (adenoma,epithelioma andcarcinoma) and/orkeratoacanthomas
Epidermoid cysts,fibromas, lipomas,leiomyomas,neurofibromas
Multiple basalcellcarcinomas,palmo-plantarpits, fibroepit-helioma ofPinkus
Facial, acraland oralmucosalpapules;lipomas, hae-mangiomas,pigmentedmacules of theoral mucosa,lips, fingers,and toes
Multipleperifollicularfibromas andtrichodisco-mastrichofollicolomastrichodiscomasacrochordonsfacialangiofibroma
Cutaneousleiomyomas(piloleiomyooma)
Spectrum ofextra-cutaneousneoplasms
Optic gliomas; meningioma;astrocytoma;rhabdomyosar-coma;pheochromocytoma;gastrointestinal autonomic nervetumors (gastrointestinalleiomyomas; neurofibromas;stromal tumor; juvenilemyeloid/myelomonocyticleukemia; tumors throughout thegastrointestinal tract (duodenum,ampulla, pancreas, or bileduct/gallbladder):somatostatinoma, GIST,adenocarcinoma, carcinoid,neurofibroma, schwannoma, organgliocytic paraganglioma ANDadd glomus tumors, MPNSTs
Tumors of themajor and minorsalivary glands:basal cellcarcinoma,adenocarcinoma
Carcinomas of colon,stomach, small bowel,hepatobiliary tract,cancer of the breast,upper gastrointestinaltract, lungs, larynx,parotid gland andhemopoieticmalignancies,genitourinary tract(tumors affecting theendometrium, ovaries,prostate, kidneys,ureters and bladder)
Adenomatous polypsin the small intestine,desmoid, osteomas,craniopharyngioma,ependymoma,gastrointestinalcancer,hepatoblastoma,medulloblastoma,nasal neuromas,nasopharyngealangiofibroma,pancreaticadenocarcinoma,papillary thyroidcancer
Medulloblastoma,ovarianfibrosarcomafetalrhabdomyomacardiacfibroma,ovarianfibroma,odontogenickeratocyst,
Carcinomas ofbreast,thyroid;hamartoma-tous polyposiswith low riskof colonmalignanttransformation
Renal cellcarcinomas(unusualhistologicaltypes); lipoma,melanoma,parathyroidadenoma
Uterineleiomyomas(fibroids)PapillaryRenal tumorsBreast cancer,bladdercancer, adultleydig celltumors of thetestis, massivemacronodularadrenocorticaldisease
Other clinical findings Scoliosis,vertebral/sphenoid/orbitaldysplasia, (tibial)pseudoarthrosis, overgrowth(skeletal abnormalities)
Macrocephaly,calcification offalx cerebri,sindactilia,bifid ribs,facial scoliosis
Macrocephaly,cerebellardysfunction
Spontaneouspneumothora-ces;pulmonarycysts

242 G. Ponti et al. / Critical Reviews in Oncolo
F
tNh[
rppras
awtcsTptomnpwisl
sg
iggtlda[uahoSclogpmgaNnmrsgo
1
nadtdh[cldlt
tsaptions as a deubiquitinating enzyme. The protein contributesto the regulation of cell survival, proliferation and differen-
ig. 1. Multiple neurofibromas of face in patient with NF1 syndrome.
he Ras/mitogen-activated protein kinase (MAPK) pathway.eurofibromin is expressed at low levels in all cells, withigher levels in the central and peripheral nervous system4].
The mutation rate in the NF1 gene is one of the highesteported in any human disorder (approx. 1/10,000 gameteser generation) [10], with approximately 50% of all NF1atients having no family history of the disease. In our expe-ience [11], a great phenotypic variability was revealed bothmong unrelated patients and even among members of theame family who had different clinical manifestations.
Malignancies in NF1 usually develop at an earlier agend they represent the main cause of mortality in patients,ith a 10–15-year decreased life expectancy compared to
he general population. Therefore some types of malignan-ies are characterized by a poor prognosis compared to theirporadic counterparts, with an exception of optic gliomas.his finding is probably related to the nonspecific clinicalresentation together with the lack of well-defined screeningests for early detection, that both contribute to a poorerutcome in malignancies associated with NF1 [12]. Theost frequent malignancies in NF1 are malignant peripheral
erve sheath tumors (MPNSTs), high-grade spindle cell neo-lasms with various degrees of Schwann cell differentiation,ith a high propensity for metastasis [13]. Their prevalence
n NF1 patients ranges from 8 to 13% [6] and they may
how divergent differentiation with heterogeneous epithe-ial or mesenchymal components, including skeletal muscle,ts
gy/Hematology 85 (2013) 239–256
mooth muscle, cartilaginous, osseous, angiosarcomatous orlandular differentiation [14–17].
Documented gastrointestinal manifestations of NF1nclude neurofibromas, most commonly in the jejunum,anglioneuromatosis leading to disordered gut motility, gan-liocytic paragangliomas, periampullary duodenal carcinoidumors and GISTs [18,19]. Besides the typical cutaneousesions, the tumor spectrum of our NF1 cohort included theiagnosis of GISTs. The clinical association between GISTsnd type 1 neurofibromatosis has been well characterized20]. However, little is known about the molecular basisnderlying GISTs development in neurofibromatosis [21],s well as in other syndromic settings; it is still unclear whet-er there is a difference between the molecular pathogenesisf sporadic and multi-neoplastic disease associated GISTs.ome investigators have attempted to explain the mutablelinical expression observed in patients with identical germ-ine NF1 mutations. In the case of co-existing GISTs andther gastrointestinal tumors, which mostly arise in the upperastro-intestinal tract, second NF1 somatic mutations mightlay a significant role. Alternatively, inherited or epigeneticodifiers, such as ethnicity or somatic aberrations in other
enes (21), may determine distinct clinical phenotypes. Onlypproximately half of all patients with a clinical diagnosis ofF1 can be classified at the molecular level as affected byeurofibromatosis type 1 (i.e., proven presence of a germlineutation in NF1 gene) [17], thus there must be other genomic
egions that are also responsible for the disease pathogene-is. For this reason it has been hypothesized that mutations inenes other than NF1 may be necessary for the developmentf the full phenotype.
.2. Brooke–Spiegler syndrome
Brooke–Spiegler syndrome (BSS) is an autosomal domi-ant disorder characterized by predisposition toward skinppendage tumors, such as cylindromas, spiradenocylin-romas, spiradenomas and trichoepitheliomas (cribriformrichoblastomas) (Table 1). The exact incidence of this syn-rome is unknown, but it remains uncommon. Several studiesave suggested that the prevalence of BSS is higher in females22–25]. Two dominantly inherited genodermatosis, familialylindromatosis (FC, OMIM 132700) and multiple fami-ial trichoepithelioma (MFT, OMIM 601606) were originallyescribed as distinct entities but are now considered to be alle-ic diseases with the same genetic basis and included withinhe spectrum of BSS [26].
BSS patients have various mutations in the CYLD gene, aumor suppressor gene whose locus was mapped to chromo-ome 16q12-13 by linkage analysis in 1995 [27]; it encodes
cytoplasmic protein with three cytoskeletal-associatedrotein-glycine-conserved (CAP-GLY) domains that func-
iation via its effects on NF-kappa-B activation and on Wntignaling negative regulation.

G. Ponti et al. / Critical Reviews in Oncology/Hematology 85 (2013) 239–256 243
F
7a[amcgv
tbtetcs
ttsvmItlp
tiudmdp
1
cst
Fd
mm[dct
dsrmom
tltrioidgenders, with a slight predominance in men (male to femaleratio of 3 to 2). The age at presentation of the first malignant
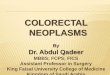
ig. 2. Cylindromas of scalp in patient with Brooke–Spiegler syndrome.
Blake and Toro [25] described 51 germline mutations in3 families in their review of the literature; to our knowledge,total of 66 germline mutations have been identified so far
23–25,35–39]. However, some patients present as CYLDnd PTCH mutation-negative, suggesting that other genesay be implicated and thus further studies are needed to
larify whether these patients may be affected by de novoermline mutations [28]. Inter- and intra-familial phenotypicariability has been documented as well [29].
The cutaneous tumors usually appear from childhood tohe third decade, and tend to gradually grow in size and num-er throughout life; they can be very disfiguring and leado psychological distress (Figs. 2 and 7b,c). Moreover pre-xisting benign adnexal tumors hide a malignant potential ashey can transform into their malignant counterparts, whichan be more aggressive in the syndromic than in the sporadicetting [33].
It is useful to genetically test families and individuals withhe syndrome, while mutation carriers should be informedhat BSS present a high penetrance at increasing age forkin appendageal tumors. These patients need regular sur-eillance in order to detect potential malignant lesions andinimize disfigurement through an early surgical treatment.
n this context, a recent therapeutic attempt has been made toreat single cylindroma in BSS with topically applied salicy-ic acid, which acts by interfering with the NF-�B signalingathway [40].
Moreover, an association of BSS with salivary glandumors has been suggested [29–33]. In this setting, affectedndividuals should be examined, even if the exact risk remainsnknown [33]. Unfortunately it is not always possible toetect the putative mutation due to a variety of alternativeechanisms including unknown mutations, germline large
eletions, deep intronic or promoter mutations and/or incom-lete sensitivity of the technique used [24,34,35].
.3. Muir–Torre syndrome
Muir–Torre syndrome is an autosomal-dominant skin
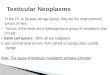
ondition of genetic origin distinguished by tumors of theebaceous glands and/or keratoacanthomas, that are associa-ed (i.e., arise simultaneously or sequentially) with one orig. 3. Multiple sebaceous adenomas of face in patient Muir–Torre syn-rome.
ore visceral malignancies, in particular, colorectal, endo-etrial, urological, and upper gastrointestinal neoplasms
41]. The characteristic sebaceous tumors of Muir–Torre syn-rome include sebaceomas, sebaceous adenomas (Fig. 3) andarcinomas, basal cell carcinomas with sebaceous differen-iation and seboacanthomas [42–44] (Fig. 4).
MTS has been considered a rare variant of Lynch syn-rome, although it has been suggested that the incidence ofebaceous neoplasms among Lynch families has been unde-estimated and that as many as 10% of individuals withismatch repair genes mutations have a sebaceous neoplasm
r a keratoacanthoma detectable through dermatologic exa-ination [45] (Table 1).Muir–Torre syndrome is a rare disease. Consequently,
here is little or no knowledge about the main epidemio-ogical features. It is possible (though not documented)hat Muir–Torre syndrome can escape diagnosis and clinicalecognition. Most clinical reports on Muir–Torre syndromenvolve white patients who live in developed countries. Tour knowledge, there is almost no information on the diseasen Asian and African populations. Following an autosomal-ominant pattern of inheritance, the disease is present in both
Fig. 4. Keratoacanthoma in patient with Muir–Torre syndrome.

2 Oncolo
d5
g((q
McgbaaHsMfgaIt
pigsnrpcKsMniwptmotpvn
ntpcm
ttps
crndd
tp
ihvghvwoiScahrststi
1
sdoIfaat
tvsedamatof
44 G. Ponti et al. / Critical Reviews in
isease ranges from 23 years to 89 years, with a median of3 years [45].
MTS is due to defective DNA mismatch repair (MMR)enes. The MMR proteins mainly related to MTS are MSH2on chromosome 2), MLH1 (on chromosome 3) and MSH6on chromosome 2). MLH3 and PMS2 have been less fre-uently implicated in MTS [44].
In addition to the clear pathogenetic role of MLH1 [46] andSH2 genes in MTS, a few cases of MSH6 mutations asso-
iated with MTS have been recently reported [47,48]. Theeno-phenotype characterization in MTS cases shows thatoth MLH1 and MSH2/MSH6 have an etiopathological rolend that there is no correlation between MTS mutations andny particular functional domains inside these three genes.owever, in contrast to the colorectal carcinomas of HNPCC,
ebaceous neoplasms implicated in MTS display the loss ofSH2 much more commonly than MLH1 [51–54]. There-
ore, the “subordinate” role of MSH6 [47–50] in the MTSenesis has to be re-evaluated and its involvement shouldlways be investigated, together with MSH2, first throughHC analysis, and second through direct sequencing or dele-ion mapping.
Several reports suggest that, whenever a sebaceous neo-lasm is identified, individuals should be screened fornternal malignancies. It is reasonable that dermatopatholo-ists perform immunohistochemical staining on sebaceomas,ebaceous adenomas and carcinomas, on basal cell carci-omas with sebaceous differentiation and seboacanthomas,egardless of the topographic location of the lesion or theatient’s age. Multiple KAs should also be immunohisto-hemically analyzed; additional studies including solitaryAs and further discussion of their results are still neces-
ary [55]. The immunohistochemical analysis should includeLH1, MSH2, MSH6, and PMS2. A lack of nuclear immu-
oreactivity within tumour cells is supportive of a mutationn the tested gene and has been shown to correlate wellith high levels of MSI, as assessed by the gold standard ofolymerase chain reaction-based amplification and chroma-ographic or electrophoretic assessment of multiple, defined
icrosatellite regions of DNA. Depending on the resultsbtained, the dermatopathologist could perform molecularechniques for MSI and MMR or BRAF mutations or sendaraffin-embedded tissue to a reference laboratory. Howe-er, immunohistochemistry for BRAF sounds promising buteeds stronger support in the literature.
This strategy should be followed even in patients withegative family history and absence of other symptoms; upo 60% of affected individuals develop sebaceous neoplasmsreceding visceral malignancies (among those, colorectalarcinoma is the most frequent, accounting for 50% of allalignancies in MTS) (Table 1) [42,45,55].Mutations in the mismatch repair genes may not be
he only mechanism leading to a MTS phenotype. Muta-ions in the MYH gene, inherited in an autosomal recessiveattern, result in an attenuated gastrointestinal polypo-is phenotype with patients showing an increased risk of
tptw
gy/Hematology 85 (2013) 239–256
olorectal carcinoma and other cancers. Several caseeports have recently highlighted the presence of sebaceouseoplasms in patients with MYH-associated polyposis syn-rome, and one paper established that those sebaceous lesionsid not exhibit MSI [56,57].
Lines of evidence further clarifying the pathogenesis ofhe most common sebaceous gland neoplasms may revealotential therapeutic targets [58].
Sebaceous glands are affected through ageing, bothntrinsic and extrinsic, which lead to distinct clinical andistological changes. Reduced androgen levels in aged indi-iduals carry to a slow cellular turnover in the sebaceouslands resulting in hyperplasia: this will be evident in theyperplastic facial sebaceous glands at advanced age. Ultra-iolet radiation and immune suppression (cyclosporin Aith corticosteroids) represent cofactors for the developmentf sebaceous gland hyperplasia. Current molecular findingsndicate that overexpression of the ageing-associated genemad7 and parathormone-related protein correlate with seba-eous gland hyperplasia, whereas c-myc overexpression isssociated with enhanced sebum production. On the otherand, microsatellite instability with a loss of the mismatchepair gene hMSH-2 has been detected in immune suppres-ed patients and under photo-induced DNA damage. Whileopical and systemic oestrogens offer treatment options forkin xerosis in menopausal females, a combination of isotre-inoin and interferon-alpha may prevent tumour developmentn patients with Muir–Torre syndrome [58–60].
.4. Gardner’s syndrome
Familial gastrointestinal polyposis includes various rareyndromes sharing the common features of an autosomalominant pattern of genetic transmission and numerous andften adenomatous polyps, scattered in the large bowel.n 1951, Gardner described the occurrence of a variant ofamilial adenomatous polyposis (FAP) that presented withdditional extracolonic manifestations: osteomas of the skullnd mandible, epidermoid cysts, desmoids and soft-tissueumors [61,62].
FAP is characterized by the development of hundreds tohousands of adenomatous polyps scattered throughout thearious segments of the colorectum that usually appear in theecond decade of life. The disease is associated with severalxtracolonic manifestations including polyps of the stomach,uodenum and jejuno-ileal tract, typical retinal spots, dentalbnormalities, desmoid tumors, epidermoid cysts, cranial andandibular osteomas, thyroid tumors and nasopharyngeal
ngiofibromas [63] (Table 1). In particular, skin manifesta-ion of GS include: multiple epidermoid, trichilemmal, hybridr pilomatrical cysts or pilomatricomas, developing on theace, the scalp and the limbs of 20–50% of patients; post-
raumatic desmoid tumors of the abdominal wall (12–30% ofatients); nuchal fibroma, manifesting with a diffuse indura-ion and swelling of the back of the neck; “Gardner fibroma”hich appears most commonly on the trunk and consists
Oncology/Hematology 85 (2013) 239–256 245
hgl
fyttkat
sotatOoocchbasprtfbnhcs
5GwaAsiada
waswcscwT
Fh
nme
igtnSmdccotonpp
G. Ponti et al. / Critical Reviews in
istologically of sheets of thick, haphazardly-arranged colla-en bundles with interspersed bland fibroblasts; more rarely,ipomas, leiomyomas and neurofibromas [62,64].
When cutaneous cysts of hair follicle origin are multiple,amilial, located on unusual sites (such as the limbs), affectoung patients or especially when they show uncommon his-ological features (namely a mixture of features belongingo epidermoid, trichilemmal cysts and/or pilomatricomas,nown as hybrid cysts) they may be the hallmark of GS,cancer-prone syndrome that associates (benign) cutaneous
umors and visceral malignancies [62].The extracolonic and extracutaneous manifestations of the
yndrome include gastric and duodenal polyps (80 and 60%f patients respectively) and desmoid tumours. The latterypically arise intra-abdominally (mesentery, small bowel)round the age of 30 years and are associated with muta-ions occurring downstream of codon 1400 of the APC gene.steomas affect about 20% of patients and they usually arisen the mandible and the skull, but may develop in any bonef the body. They may precede the actual development ofolon polyps and are commonly associated with cutaneousysts. Congenital hypertrophy of the retinal pigment epit-elium (CHRPE) affects 60–70% of patients; multiple orilateral patches of CHRPE are highly specific for FAP. Theyre associated with mutations between codons 767 and 1513,imilar to osteomas. Dental lesions are present in 18% ofatients: they include odontomas, absent, supernumerary orudimentary teeth, multiple caries. Other features include:hyroid (namely papillary) carcinomas, that show a strikingemale predominance; brain tumours (astrocytomas, glio-lastomas, medulloblastomas), adrenal adenomas (usuallyon-secreting and often found on autopsy) and pancreatic andepatic carcinomas (hepatoblastomas); however, the asso-iation between the latter tumours and FAP has not beentatistically ascertained [62].
The adenomatous polyposis coli (APC) (chromosomeq21), is the gene that, if mutated, is responsible for theardner’s syndrome. It encodes a 2843-amino acid proteinhich plays significant a role in the cell adhesion process
nd signal trasduction [62]. The effects of a malfunctioningPC gene are not limited to the colorectum, but involve
everal other organs and tissue; thus, this gene is considerednvolved in generalized disorders of tissue growth regulationnd it is responsible for the epidermoid cysts, osteomas andesmoids tumors (Gardner’s phenotype) which accounts forbout 20–40% of patients with FAP [63].
However, on clinical grounds, a sharp distinction bet-een FAP and Gardner’s syndrome is often impossible, sincecareful investigation of families with an initial diagno-
is of classic FAP can lead to the detection of individualsith features of Gardner’s syndrome. The identification and
haracterization of the APC show that FAP and Gardner’s
yndrome are both associated with molecular alterationsonsisting in small deletions, insertions or point mutations,hich introduce premature protein termination signals [64].he available evidence indicates that they are not distincto
pm
ig. 5. Typical face of Gorlin–Goltz patient with ipertelorism, macrocep-aly, frontal bossing and facial scoliosis.
osologic entities, but the latter represents the full-blownanifestation of a spectrum of clinical features due to the
ffect of a pleiotropic gene [65–69].Constitutional mutations of the APC gene are detected
n the large majority (80–90%) of individuals. A peculiarenotype–phenotype correlation is evident in FAP patients:he point at which the APC gene mutation occurs determi-es the manifestations and severity of Gardner syndrome.pecific codon mutations correlate with definite extracolonicanifestations and the number, time frame, and malignant
egeneration of adenomas. APC mutations downstream ofodon 1440 up to codon 1580 (exon 15) are frequently asso-iated with features of Gardner’s syndrome [70] such assteomas, epidermoid cysts and desmoids tumors. Consti-utional mutations occurring within the first 4 coding exonsf the APC gene have been correlated with the so-called atte-uated APC [71], whereas mutations occurring in the centralart of the APC gene are associated with severe polyposishenotype [72], profuse adenomatosis of the colon, early agef onset of adenomas and rapid progression to malignancy.
Regarding the screening and clinical management of GSatients and family members, panoramic dental radiographsay detect several occult radiopaque lesions in Gardner

2 Oncolo
psdo
aloefidcgtaobsrala9fafdfn
1s
#bnarabtds(
c2cpg
c2fD
9btsPvpaptsf
ssj
gWlb
sSatpscadoctalnfvm
mtaf(cvrcoc
46 G. Ponti et al. / Critical Reviews in
atients, such as skull and mandible osteomas, odontomas,upernumerary teeth, dentigerous cysts and abnormal man-ibular bone sculpture. An endoscopic surveillance intervalf 3–5 years is appropriate for the majority of these patients.
Basing on the results of some trials, Celecoxib has beenpproved for the treatment of FAP. However the safety of itsong term-use is questioned by reports revealing a high ratef cardiovascular events in patients receiving therapeuticallyffective drug doses [73]. Earlier studies demonstrated bene-cial effect of Sulindac, a non-steroidal anti-inflammatoryrug, in producing regression of rectal polyps, after totalolectomy. The results of prior trials may then be revisited,iven that the main adverse effect of this drug (gastrointes-inal toxicity) is medically manageable [74]. Tamoxifen haslso been proposed in combination with Sulindac becausef its effects on prostaglandins inhibitions. These two mighte preferable to the use of traditional chemotherapeutic drugsuch as Doxorubicin and Dacarbazine. Oral calcium may alsoeduce the rectal epithelium turn-over. Recent comparativenalysis of serum protein profiles of APC missense germ-ine mutation patients, sporadic colorectal cancer patientsnd healthy patients suggested a relationship between m/z05, belonging to the kininogen-1 precursor, the humanorkhead box protein 01A (FOXO1A) and the developmentnd growth of colorectal cancer. This proposes FOXO1Aragment determination in serum with matrix-assisted laseresorption/ionization mass spectrometry (MALDI/MS) as auture promising approach for early detection of colon carci-oma or for the development of targeted therapies [75].
.5. Nevoid basal cell carcinoma syndrome (Gorlinyndrome)
Nevoid basal cell carcinoma syndrome (NBCC; OMIM109400) is a rare autosomal dominant disorder characterizedy multiple basal cell carcinomas, keratocystic odontoge-ic tumors (KOCTs) of the jaws, palmar and/or plantar pitsnd developmental defects. The latter defects include bifidibs, intracranial calcification, skeletal anomalies (fused, bifidnd splayed ribs, calcifications of the falx cerebri, frontalossing) (Fig. 5). A variety of other benign or malignantumors can be found in association with these developmentalefects, i.e., ovarian fibroma, medulloblastoma, rhabdomyo-arcomas, cardiac fibromas and ameloblastoma (Table 1) [76]Fig. 7d).
The incidence of NBCCS changes widely amongountries from one case per 55,600 [77] to one case per56,000 in population [78]. The prevalence is likely to beonsiderably higher in individuals younger than 20 years whoresent with basal cell carcinomas (BCC) [79]. There is noender predilection [80–82].
Since the discovery in 1996 that NBCCS might be asso-
iated to germline mutations on the PTCH1 gene [49], about80 germline mutations have been described worldwide soar [83]. The PTCH1, or the human homologue 1 of therosophila Patched gene which is mapped on chromosometHih
gy/Hematology 85 (2013) 239–256
q22.3 consists of 23 exons and encodes an integral mem-rane protein of 1447 amino acids, Patched 1 (Ptch1) with 12ransmembrane regions, 2 extracellular loops, and a putativeterol-sensing domain [84]. NBCCS is due to mutations inTCH1, a tumor suppressor gene; the PTCH1 protein ser-es as a receptor for the Secreted Sonic Hedgehog (SHH)rotein, and inhibits the signaling pathway by repressing thectivity of Smoothened (SMO), another transmembranousrotein [80]. The SHH signaling pathway plays an impor-ant role in mammalian embryonic development of structuresuch as the neural tube, axial skeleton, limbs, lungs, skin, hairollicles and teeth [81].
PTCH1 mutations are involved in the formation ofyndromic as well as non-syndromic keratocysts [85]. Non-yndromic KOCTs are common benign cystic tumors of theaws [86].
The vast majority of cysts arise sporadically and in a sin-le form on upper and/or lower jaws of middle-aged people.hen associated with the NBCCS, these lesions appear ear-
ier, often during the first or second decade of life, and maye multiple [87].
Diagnostic criteria were defined by Evans [77] and revi-ed by Kimonis [88], and include major and minor criteria.ince then, further diagnostic criteria have been proposednd vary by source, but there have been no studies to definehe sensitivity and specificity of the most accurate phenoty-ic combination. Recently, Bree and Shah [89] proposed lesstringent criteria for suspected NBCCS diagnosis and dis-ussed that medulloblastoma should be considered a majornd not a minor criterion, as this may lead to increased earlyetection if the tumor was recognized as a potential indicatorf the underlying syndrome, since it typically manifests inhildren aged two years or even younger (Fig. 6). Althoughhere are several reports in the literature regarding NBCCSssociated-ameloblastoma, the latest NBCCS clinical criteriaack of this peculiar odontogenic tumor, which constitutes aeglected criterion [90]. Of note, there is no firm evidenceor genotype/phenotype correlation in NBCCS; phenotypicariations may be related to environmental exposure and/orodifier genes [81].According to the most recent guidelines, the goal of treat-
ent in basal cell carcinoma (BCC) is eradication of theumor, with the intent of maximal preservation of function andesthetics. For this reason, strategies should be individualizedollowing risk factors and preferences. The surgical approachtraditional or Mohs Micrographic surgery in the most diffi-ult lesions) usually represents the first choice, but treatmentsary according to cancer size, depth, and location. Local the-apy with chemotherapeutic and immune-modulating agentsan be considered in some cases, as the FDA approved the usef topical fluorouracil and imiquimod for small and superfi-ial BCCs. Metastatic BCC is usually treated with clinical
rials of systemic platinum-based combination therapy, andedgehog pathway inhibitors might epitomize a promisingnnovation. Recent evidence from in vitro and in vivo studiesas demonstrated that aberrant reactivation of the Sonic Hed-

G. Ponti et al. / Critical Reviews in Oncology/Hematology 85 (2013) 239–256 247
Fig. 6. Genealogic tree of family with Gorlin–Golz syndrome cosegregating PTCH1 germline mutation.
Fig. 7. (a) Histological features of neurofibroma (HE); (b and c) eccrine cylindroma showing accumulation of basement membrane within the tumor lobules(HE, 20×). (d) Histological features of ameloblastoma, a peculiar odontogenic tumor associated to Gorlin–Goltz syndrome.

2 Oncolo
gcstttpmsItwmfItf
1
bdtDRp
hBtabSpat
lahagftttKg
cp[omo
ao
ttiab
iTtPapmhtaadtea
otttwPtirPPlost
anwi
ncaf3f
48 G. Ponti et al. / Critical Reviews in
ehog (SHH) signaling pathway regulates genes that promoteellular proliferation in various human cancer stem cells,uch as basocellular carcinoma, medulloblastoma, pancrea-ic adenocarcinoma and small-cell lung cancer. Therefore,he chemotherapeutic agents that inhibit activation of GLIranscription factors have emerged as promising novel thera-eutic drugs. GDC-0449 (Vismodegib), orally administrableolecule belonging to the 2-arylpyridine class, inhibits SHH
ignaling pathway by blocking the activities of Smoothened.n a recent phase II trial, Vismodegib was found to substan-ially shrink tumors or heal visible lesions in 43% of patientsith locally advanced BCC and in 30% of patients withetastatic BCC [91]. Hedgehog pathway inhibitors are there-
ore indicated for non-surgically removable advanced BCCs.ts anti-tumor efficacy has been proved, and the effect seemso be suspensive, which raises the question of its tolerabilityor long term use [92].
.6. Cowden syndrome
Cowden syndrome (CS) is a genodermatosis characterizedy multiple hamartomas, neoplasms of ectodermal, meso-ermal and endodermal origin, and an autosomal dominantype of transmission. CD was first reported by Lloyd andennis in 1963, who named the syndrome after their patientachel Cowden [93]. In a successive report [94], Weary et al.roposed the name of “multiple hamartomas syndrome”.
Cowden syndrome (CS) is part of the PTENamartoma tumor syndrome (PHTS), along withannayan–Riley–Ruvalcaba syndrome (BRRS), Pro-
eus syndrome (PS), and Proteus-like syndrome, comprisingspectrum of lesions that affect skin, mucous membranes,
reast, thyroid gland, kidney and gastrointestinal tract.everal genetic studies revealed the autosomal dominantattern of inheritance with a high prevalence in both gendersnd moderate interfamilial and intrafamilial differences inhe expressivity of signs and symptoms [95,96].
The responsible gene for Cowden’s disease has been loca-ized to chromosome 10q22-23 and subsequently identifieds PTEN (or MMAC1); it encodes a dual-specificity phosp-atase which functions as tumor suppressor. Constitutionalberrations of PTEN, including missense, nonsense and sin-le splice site mutations, have been detected in several CSamilies [97]; moreover, loss of heterozygosity and dele-ions of PTEN were found in fibroadenomas of the breast,hyroid adenomas and various hamartomatous tissues. Theumorogenesis in CS follows the two-hit model suggested bynudson, resulting in biallelic inactivation of this particularene.
99% of affected individuals with CS develop the muco-utaneous stigmata, such as trichilemmomas, papillomatousapules, acral and plantar keratoses, by the third decade of life
95]. Facial lesions are the most typical and peculiar featuresf CS and occur in the majority of patients – these consist ofultiple small and keratotic papules concentrated around therifices and are associated with hair follicles. Hyperkeratotic
satw
gy/Hematology 85 (2013) 239–256
nd verrucous lesions are usually found on the dorsal surfacef the hands and feet, together with palmoplantar keratosis.
Newly described PTEN-related neoplasms include a dis-inctive soft tissue lesion highly associated with PHTS andermed PHOST (PTEN hamartoma of soft tissue). This lesions an overgrowth of mingled soft tissue elements (primarilydipose and dense), myxoid fibrous tissues and abnormallood vessels of various types [98].
The gastrointestinal involvement in CS is represented bysolated or clustered polyps of various histological types.hese can be seen from the esophagus to the rectum, and
heir frequency is of the order of 60–80% of all cases [99].olyp-like lesions with suspected hamartomatous origin havelso been found, by ultrasound, in the gallbladder of CSatients [100]. Gastrointestinal polyps in CS are hamarto-atous; however, adenomatous and carcinomatous changes
ave also been reported [101] in association with hamar-omas. Given the recently described high prevalence ofdenomatous polyps, it has been accordingly suggested thatdenomas may be a manifestation of CS, rather than a coinci-ental finding as previously appreciated [102,103]. Besideshe classical hamartomatous polyposis, diffuse macroscopicsophageal acanthosis and microscopic ganglioneuromatosisre other findings associated with CS [104,105] (Table 1).
Immunohistochemical (IHC) staining for the assessmentf PTEN expression levels can provide additional support tohe diagnosis of CS. Somatic PTEN loss is rare in sporadicrichilemmoma and demonstration of complete PTEN loss inrichilemmoma by IHC is strongly suggestive of associationith CS, but retention of PTEN staining does not exclude CS.TEN IHC in trichilemmomas may be helpful in screening
hese skin tumors for association with CS but should be usedn context with other major and minor defining clinical crite-ia, genetic counseling (family history) and possibly germlineTEN genotyping to confirm a diagnosis of CS [106,107].TEN IHC staining of thyroidectomy specimens and papi-
lary renal cell carcinoma (pRCC) can aid in the recognitionf patients with CS [108]. In particular, the sensitivity andpecificity of PTEN staining in thyroidectomy specimens forhe detection of CS are 100% and 92,3%, respectively [109].
Patients with negative PTEN IHC, patients with papillarynd chromofobe RCC may be referred to cancer genetics cli-ics for personal and family history assessment to determinehether testing for CS or another hereditary syndrome is
ndicated [108].Regarding the PTEN life-time risk for associated malig-
ancies, elevated risk of breast, thyroid, endometrial, kidneyancers and melanoma has been reported. More specifically,ge-related penetrance estimates reveal 85.2% for invasiveemale breast cancer, 35.2% for epithelial thyroid cancer,3.6% for kidney cancer, 28.2% for endometrial cancer, 9.0%or colorectal cancer and 6% for melanoma [110]. Recent
tudies reported that germline mutations of PTEN as wells SDHB-D and KLLN are all associated with a significan-ly higher risk of epithelial thyroid cancer when comparedith the general population. In particular, there was a clear
Oncolo
dgcKghtc
diratsmund2a
prraieo[btt2mg
coweitttrtcpm
1
no
smftcsek
ttfcokc
dpll
tF6icaagbr[
lWtFadafitsgfmvc
pr
G. Ponti et al. / Critical Reviews in
ifference in gene-related clinical presentation: patients withermline PTEN pathogenic mutations develop thyroid can-er at an earlier age compared to patients with SDHB-D orLLN mutations [111]. Moreover, both upper- and lower-astrointestinal polyps are common features of the PTENamartoma tumor syndrome and almost 20% of PTEN muta-ions carriers with colorectal adenomatous polyps developolorectal adenocarcinomas [112].
Regarding the CS management, the NCCN recommen-ations for cancer surveillance [113] have been recentlymproved and include: for children (<18 years): yearly thy-oid ultrasound and skin check with physical examination; fordults: yearly thyroid ultrasound and dermatologic evalua-ion; women beginning at the age of 30 years: monthly breastelf-examination, annual breast screening (at minimum mam-ogram; MRI my also be incorporated) and transvaginal
ltrasound or endometrial biopsy. For men and women: colo-oscopy beginning at age of 35–40 years with frequencyepending on degree of polyposis identified; biennial (everyyears) renal imaging (CT or MRI preferred) beginning at
ge 40 years [95].The analyses and extensive clinical experience in pros-
ective series of patients performed by Tan MH et al.ecommend: (i) biannual renal imaging on the basis of theelatively high incidence of RCC; (ii) endometrial samplings a routine surveillance procedure on the basis of the highncidence of RCC; (iii) a specific starting age for breast andndometrial screening; (iv) surveillance for colorectal cancern the basis of data showing an increase of colorectal cancer110]. For TC surveillance, especially in children with PHTS,aseline thyroid ultrasound is recommend in all patients uponhe genetic diagnosis of PHTS, regardless of their age, andhen repeated annually [114]. For those patients with a family3 history of a particular cancer type at an early age screeningay be initiated five to ten years prior to the youngest dia-
nosis in the family [95,115].Due to the benign nature of cutaneous lesions, no medi-
al treatment is required. Nevertheless, available treatmentptions include CO2-laser ablation, surgical excision, orith topical 5-fluorouracil. Alternative therapies comprise
lectrosurgery, cryosurgery, dermabrasion, topic retinoids,nterferon 2 alpha and bleomycin chemotherapy. Research onhe diverse post-translational alterations of PTEN focusing onheir biological relevance and potential applications to cancerherapy was recently reported [116]. Innovative targeted the-apies may focus on inhibition of the PI3K/Akt/mammalianarget of rapamycin (mTOR) pathway: NSAIDS have beenonsidered on this point, but promising results have been dis-layed by the use of rapamycin in the regression of advanceducocutaneous lesions.
.7. Birt–Hogg–Dubé syndrome
Birt–Hogg–Dubé syndrome is a rare autosomal domi-ant genodermatosis that is characterized by the presencef fibrofolliculomas and/or trichodiscomas, pulmonary cysts,
lpas
gy/Hematology 85 (2013) 239–256 249
pontaneous pneumothorax, and renal tumors [117]. Theost common histological types found in renal tumors
rom patients with the syndrome are hybrid oncocy-ic/chromophobe tumors and pure forms of chromophobearcinoma, clear cell or papillary RCC and oncocytomas. Theyndrome is linked to mutations in the FLCN gene, whichncodes folliculin and is preferentially expressed in the skin,idney, and lung [118].
Although skin neoplasms and pathogenic FLCN muta-ions are the major criteria for setting the diagnosis ofhis syndrome, ‘renal-cancer-only’ and ‘pneumothorax-only’amilies have been described as well [119]. Given the clini-al variability and penetrance, a diagnosis can be made basedn non-cutaneous manifestations, in patients with or withoutnown family history, even in the absence of histologicalonfirmation of fibrofolliculomas or trichodiscomas [120].
Birt–Hogg–Dubé syndrome is very rare; the exact inci-ence is unknown. To date, approximately 200 families withathogenic FCLN mutations have been identified, but this isikely to be an underestimate because of the marked variabi-ity in presentation [121].
In 2002, Zbar’s group was successful in identifying muta-ions in the folliculin (FLCN) gene underlying BHDS [122].olliculin is a cytoplasmic protein with a predicted size of4 kDa. Alternative splicing of the FLCN gene results in twosoforms—a full-length form and one that uses an initiationodon in intron 6. Although the precise function of folliculinnd its alternate splice variant is not clear, it is thought to betumor suppressor with LOH initiating tumor formation. Allermline mutations in patients suffering from BHDS descri-ed so far are splice-site mutations or insertions/deletions thatesult in putative protein truncation and haplo-insufficiency118,120,123].
The differential diagnosis for the multiple facial papu-es seen in BHD includes several familial cancer syndromes.
hile punch biopsy is necessary to establish a defini-ive diagnosis, there are distinguishing clinical features.ibrofolliculomas and trichodiscomas appear as describedbove. Multiple trichilemmomas are seen in Cowden syn-rome: these lesions look similar to fibrofolliculomas andre located around the mouth, nose, and ears. Associatedndings include cobblestoning of the oral mucosa with kera-
oses at acral sites. Multiple trichoepitheliomas are insteadeen in Brooke–Spiegler syndrome. These lesions are lar-er (2–8 mm) firm papules and are located on the nasolabialolds, forehead, upper lip, and scalp. Multiple angiofibro-as are appreciated in tuberous sclerosis. They are pink,
ascular-appearing papules and are located periorally; asso-iated findings include periungual fibromas.
Dermatologic findings may be the presenting signs inatients with BHD syndrome; therefore, it is important toecognize them in order to undertake a further systemic eva-
uation (121). Skin findings usually do not appear before theatient reaches 20 years of age. The characteristic skin lesionsre described as multiple, 2–4 mm, waxy, white, opaque,mooth, dome-shaped papules, most commonly involving
2 Oncolo
ttcfiAtmprlrnipca
2fcddgf
tbidcrmrsad
hhpyisfmcsoa
oinotg
a[
codel
bcgbrifsyo
1(
(ldcr
icglptincHmiiobtta
fit
50 G. Ponti et al. / Critical Reviews in
he head and neck, with less frequent involvement of therunk. Biopsy of these lesions shows fibrofolliculomas or lessommonly trichodiscomas. It is not possible to distinguishbrofolliculomas from trichodiscomas on clinical grounds.crochordon-like lesions have also been noted, localized to
he eyelids, axillae, and skin folds. Biopsy of these lesionsay show fibrofolliculoma or simple fibroepitheliomatous
olyp features. Some may have comedo- or cyst-like featu-es [124]. Some patients manifest only a few lesions in aocalized distribution, while others have hundreds in a gene-alized spreading. The most often involved facial areas are theose, then the cheeks, forehead, and ears. Oral examination ismperative, as these patients may have multiple, discrete, softapules of the lips, gingival and buccal mucosa. Other asso-iated skin findings include connective tissue nevus, lipomas,ngiolipomas, and facial angiofibromas.
Regarding the specific neoplastic risk, approximately5–35% of BHDS patients develop kidney tumors of dif-erent histological type [119,125]. Hybrid tumors are mostharacteristic of this condition, since several lesions initiallyiagnosed as oncocytomas or chromophobe RCCs have beenefined as hybrid tumors upon reappraisal. Various histolo-ical types of renal tumors can be found in the same BHDSamily, in the same patient or even in the same kidney.
Multiple pulmonary cysts in the setting of BHDS are dis-inctively different in histopathology from other pulmonaryullous lesions. Histopathologic examination shows that thenner surface of cysts was lined by epithelial cells, with a pre-ominance of type II pneumocyte-like cuboidal cells. Theells constituting the cysts stained positive for phospho-S6ibosomal protein expression, suggesting activation of theammalian target of rapamycin (mTOR) pathway that inte-
act with FLCN to mediate the cellular activities. The BHDyndrome associated pulmonary cysts may be consideredhamartoma-like cystic alveolar formation associated with
eranged mTOR signaling [126].There is a link of spontaneous pneumothorax with this
ereditary tumor syndrome, since the patients with BHDave 50 times the population risk of primary spontaneousneumothorax, and cases have been reported in patients asoung as 7 years [122,125]. These evidences highlight themportance of considering BHD in patients with primarypontaneous pneumothorax, even in the absence of cutaneouseatures for the syndrome [120]. The mean age of first pneu-othorax is earlier than that of the development of renal
arcinoma (38*0 years vs 50*7 years); therefore, this pre-entation provides physicians a critical opportunity to affectutcomes in later life, not only for the presenting patient, butlso for other family members who may be mutation carriers.
There are numerous reports that describe a wide spectrumf phenotypic neoplastic manifestations in BHD-affectedndividuals, including lipomas, melanomas, parathyroid ade-
omas [127] or thyroid gland alterations, but the significancef these associations has not been statistically substan-iated. Potential association with other malignancies andenotype–phenotype correlation between FLCN mutationsouts
gy/Hematology 85 (2013) 239–256
nd risk of colon or breast cancer have been recently reported128].
Due to the benign nature of the skin neoplasm no spe-ific medical treatment exists for the cutaneous lesionsf BHDS, Surgical removal has always represented theefinitive treatment of solitary perifollicular fibromas, andlectrodessication may be helpful in removing multipleesions.
Once a FLCN mutation has been demonstrated in a pro-and, genetic testing may be offered to at-risk relatives andlinical follow-up has to be initiated for carriers of the familialerm-line mutation. Contrast-enhanced CT and MRI are theest imaging techniques for surveillance and assessment ofenal lesions. However, there are no clear evidences regardingmaging follow-up: the latter can be very different, rangingrom every 3–6 months to every 2–3 years, depending on theize of lesions [129]. Surveillance could be started at 30–35ears of age and/or 10 years before the earlier age of onsetf an RCC in a given family [119].
.8. Hereditary leiomyomatosis and renal cell cancerHLRCC)
Hereditary leiomyomatosis and renal cell cancerHLRCC, also known as multiple cutaneous and uterineeiomyomatosis, MCUL) is a highly penetrant autosomalominant tumor predisposing syndrome characterized byutaneous leiomyomata, uterine leiomyomata, and/o singleenal tumor [130,131].
Regarding cutaneous tumors, the majority (76%) ofndividuals with HLRCC present with single or multipleutaneous leiomyomas (piloleiomyomas), suggested to ori-inate from hair erector pili muscles. Clinically, cutaneouseiomyomas (CLM) appear as skin-colored to light brownapules or nodules distributed over the trunk and extremi-ies, and occasionally on the face. The different presentationsnclude: single, grouped/clustered, segmental, and dissemi-ated. Forty percent of individuals with HLRCC have mildutaneous manifestations with five or fewer lesions [132].istologically, proliferation of interlacing bundles of smoothuscle fibers with centrally located, long blunt-edged nuclei
s observed [133]. These tumors typically cause pain, usuallyn response to temperature changes and touch. The penetrancef CLM is higher in men harboring a FH mutation becausey the age of 35 all men but only 55% of women result affec-ed [134]. The prevalence in woman increases with age, upo 76–80% [134,135]. The mean age of developing CML ispproximately 24 years (range 9–47) [134,136].
Uterine leiomyomas (fibroids) are benign tumors that ariserom the smooth-muscle cells of the uterus. They are presentn almost all females with HLRCC [132,134,136]. Fibroidsend to be numerous and large. In females the presence
f cutaneous leiomyomata correlates with the presence ofterine fibroids [134,136]. Behind the well known associa-ion of early onset uterine leiomyosarcoma (UMLS) in theetting of HLRCC with FH germline mutation [137,138],
Oncolo
tos[
clre[
[mcdlanttcocla
btficpfmtcigH
kbcv8fipih
nfesolw
swPercbshri
itucntgtdgpry[
2
taccubcp
Gcsaognpmswa
G. Ponti et al. / Critical Reviews in
hese mutations can occur in seemingly nonsyndromic casesf ULMS. Seventeen percent of patients with early onsetporadic ULMS showed allelic imbalance at the FH locus138,139].
FH mutation screening should be recommended by gyne-ologists for the families with multiple severe uterineeiomyomas cases. The early detection of FH mutation allowsegular screening of high risk individuals and enables thearly identification of possible highly aggressive renal tumors140].
Ten to 16% of individuals with HLRCC have renal tumors136]. RCC is found in approximately 20–25% of the FHutation positive families worldwide [141]. Most tumors are
lassified as ‘type 2’ papillary renal cancer, which displaysistinct papillary architecture and characteristic histopatho-ogy [137,142]. Other types of reported renal tumors includespectrum of tumors from tubulo-papillary renal cell carci-omas to collecting-duct renal cell carcinomas [132]. RCCumors can present a variety of patterns such as cystic,ubule-papillary, tubular and solid architecture, as well as aombination of them. The most important histologic featurer the hallmark of these RCC tumor is the presence of aharacteristic large nucleus with a very prominent inclusionike orangiophilic or eosinophilic nucleolus, surrounded byclear halo [143–145].
While diagnostic criteria for HLRCC have not been esta-lished yet, Smit et al. [133] have listed practical criteria forhe clinical diagnosis of HLRCC. Histopathologically con-rmed CLM was proposed as a major criterion, and minorriteria suggestive of HLRCC include: uterine leiomyomas,apillary type RCC or positive family history. If the clinicaleatures are indicative of HLRCC, genetic counseling andolecular genetic testing should be conducted to confirm
he diagnosis. The testing is performed by direct sequen-ing of the fumarate hydratase (FH) coding region (includingntron–exon boundaries), a method which reveals underlyingenetic alterations in approximately 90% of the suggestiveLRCC cases/families [142].The FH gene (chromosome 1q42.1) and encodes the 50-
Da subunit of the homotetramer, is the only gene known toe associated with hereditary leiomyomatosis and renal cellancer (HLRCC). More than 200 families with HLRCC fromarious populations have been described [141,146]. Between0% and 100% [136] of individuals with HLRCC have identi-able sequence variants in FH. Multiplex ligation-dependentrobe amplification (MLPA) identified a whole-gene deletionn one of 20 index cases from families in which no mutationad been identified on sequence analysis [133,146,147].
FH heterozygotes and at-risk family members who haveot been tested should undergo molecular genetic testing; theollow-up should include: every one to two years full skinxamination to evaluate for changes suggestive of leiomyo-
arcoma; annual gynecologic consultation to assess severityf uterine fibroids and to evaluate for changes suggestive ofeiomyosarcoma; every two years abdominal/pelvic CT scanith contrast or MRI to evaluate for renal lesions if previoustgB
gy/Hematology 85 (2013) 239–256 251
cans are normal; once a renal lesion is identified, CT scanith and without contrast and renal ultrasound examination,ET-CT scan to identify metabolically active lesions, andvaluation by a urologic oncology surgeon familiar with theenal cancer of HLRCC. Recently, the immunohistochemi-al evaluation of 2SC proteins has been proposed as robustiomarkers of FH mutation status [148]. Detection of proteinuccination is likely to provide a sensitive and specific met-od for pathologists to recognize the proportion of papillaryenal carcinoma that are associated with germline mutationsn the FH gene [144,149].
Since CLMs are typically benign, their management onlyncludes alleviation of cosmetic and pain related complica-ions. General guidelines can be applied in the treatment ofterine leiomyomas, though more radical surgical approa-hes, i.e., hysterectomy is typically needed due to the largeumber and size of the tumors and the severity of the symp-oms they cause [132–136]. As pharmaceutical treatment,onadotropin-releasing hormone agonists have been reportedo decrease the volume of the myomas and reduce blee-ing. In addition, novel treatments will be likely to includerowth factor or collagen production blockers. One exam-le is CP8947, a novel non-steroidal selective progesteroneeceptor modulator which seems to specifically inhibit leiom-oma cell proliferation and decrease collagen production150].
. Conclusions
An early detection of the peculiar cutaneous stigmata ofhese syndromes (malignant and benign neoplasms as wells innocent lentigines) may represent a significant help in thelinical practice for oncologists, dermatologists and geneti-ists, since these lesions can be recognized as a clue to annderlying cancer predisposition. Such an approach mightring to the early identification of hidden visceral malignan-ies together with tight surveillance screening and follow-uprotocols.
It is evident that, with the exception of APC gene inardner’s syndrome, a characteristic phenotype-genotype
orrelation has not been established for other genodermato-is. Moreover, a wide phenotypic variability is reported, evenmong patients belonging to the same family. Future studiesf the specific proteomic profiles associated to the distinctermline mutations, as well as of the phenotypes determi-ed by (until recently) unknown mutations, may reveal newrognostic markers. These should permit the detection of theolecular pathways which are responsible for cancerogene-
is in the cases not associated to acknowledged mutations, asell as the recognition of specific lifetime risk levels and the
dditional elaboration of personalized follow-up strategies.
Furthermore, it is becoming increasingly recognized thatumors diagnosed in hereditary settings have a distinct biolo-ical behavior, when compared to their sporadic counterpart.esides, they show a different chemo/radiosensitivity and

2 Oncolo
hhopnchmta
S
1tssdssb
C
R
CN
A
nPCalUHst
R
52 G. Ponti et al. / Critical Reviews in
ave dissimilar prognosis. Successful treatment protocolsave often developed starting from a druggable target that,nce inhibited, led to the regression of a specific type of neo-lasm. This is going to be true for many cancers, although it isecessary to analyze drug resistance, which can develop as aonsequence of second mutations and/or genetic polymorp-isms. Therefore heredo-familial tumors constitute uniqueodels for understanding the post translational mechanisms
hat underlie different cancer biological behavior, prognosisnd drug response.
earch strategy and selection criteria
We searched MEDLINE for articles published between963 and February 2012, using the keywords “genoderma-osis”, “familial cancer”, “Muir–Torre syndrome”, “Gorlinyndrome”, “Brooke–Spiegler syndrome”, “NF1”, “Cowdenyndrome”, “Birt–Hogg–Dubè syndrome”, “Gardner syn-rome”, “Hereditary leiomyomatosis and renal cell canceryndrome”, “Hereditary cancers and drug-sensitivity”. Weubsequently searched the reference lists of articles identifiedy our search strategy.
onflict of interest
We declare no conflicts of interest.
eviewer
Thomas Papathomas, MD, Erasmus MC, Department oflinical Pathology, Dr. Molewaterplein 50, NL-Rotterdam,etherlands.
cknowledgments
We thank Cristel Ruini, Carmelo Guarneri, Cristina Mag-oni, Caterina Longo, Giorgia Bertazzoni, Stefania Giudice,aola Azzoni, Luisa Benassi, Cristina Vaschieri, Silvanaiardo, Sara Bassoli, Francesca Giusti (Department of Headnd Neck Surgery, Division of Dermatology; Molecular Bio-ogy Laboratories), Lorenza Pastorino (Molecular Geneticsnit, University-Hospital of Genoa; Laboratory of Rareereditary Cancers, San Martino Hospital, Genoa, Univer-
ity of Genova) for the assistance and Sandro Radeghieri forhe preparation of illustrations.
eferences
[1] Ponder BAJ. Inherited predisposition to cancer. Trends in Genetics1990;6:213–8.
gy/Hematology 85 (2013) 239–256
[2] Evgeny N, Imyanitov, Moiseyenko VM. Drug therapy for hereditarycancers. Hereditary Cancer in Clinical Practice 2011;9:5.
[3] Halliday AL, Sobel RA, Martuza RL. Benign spinal nerve sheathtumors: their occurrence sporadically and in neurofibromatosis type1 and 2. Journal of Neurosurgery 1991;74:248–53.
[4] Laycock-van Spyk S, Thomas N, Cooper DN, Upadhyaya M. Neu-rofibromatosis type 1-associated tumours: their somatic mutationalspectrum and pathogenesis. Human Genomics 2011;5:623–90.
[5] National Institutes of Health Consensus Development Conference:neurofibromatosis: conference statement. Archives of Neurology1988;45:575–8.
[6] Evans DG, Baser ME, McGaughran J, Sharif S, Howard E, MoranA. Malignant peripheral nerve sheath tumors in neurofibromatosis 1.Journal of Medical Genetics 2002;39:311–4.
[7] Korf BR, Schneider G, Poussaint TY. Structural anomalies revealed byneuroimaging studies in the brains of patients with neurofibromatosistype 1 and large deletions. Genetics in Medicine 1999;1:136–40.
[8] Ferner RE, Huson SM, Thomas N, et al. Guidelines for the diagnosisand management of individuals with neurofibromatosis 1. Journal ofMedical Genetics 2007;44:81–8.
[9] Upadhyaya M, Osborn MJ, Maynard J, Kim MR, Tamanoi F, CooperDN. Mutational and functional analysis of the neurofibromatosis type1 (NF1) gene. Human Genetics 1997;99:88–92.
[10] Li Y, O’Connell P, Breidenbach HH, et al. Genomic organization ofthe neurofibromatosis 1 gene (NF1). Genomics 1995;25:9–18.
[11] Ponti G, Losi L, Martorana D, et al. Clinico-pathological andbiomolecular findings in Italian patients with multiple cutaneous neu-rofibromas. Hereditary Cancer in Clinical Practice 2011;12(9):6.
[12] Patil S, Chamberlain RS. Neoplasms associated with germline andsomatic NF1 gene mutations. Oncologist 2012;17:101–16.
[13] Rodriguez FJ, Stratakis CA, Evans DG. Genetic predisposition toperipheral nerve neoplasia: diagnostic criteria and pathogenesis ofneurofibromatoses Carney complex, and related syndromes. ActaNeuropathologica 2012;123:349–67.
[14] Ducatman BS, Scheithauer BW. Malignant peripheral nerve sheathtumors with divergent differentiation. Cancer 1984;54:1049–57.
[15] Rodriguez FJ, Scheithauer BW, Abell-Aleff PC, Elamin E, ErlandsonRA. Low grade malignant peripheral nerve sheath tumor with smoothmuscle differentiation. Acta Neuropathologica 2007;113:705–9.
[16] Woodruff JM, Christensen WN. Glandular peripheral nerve sheathtumors. Cancer 1993;72:3618–28.
[17] Li H, Velasco-Migual S, Vass WC, et al. Epidermal growth factorreceptor signaling pathways are associated with tumorigenesis in theNF1: p53 mouse tumor model. Cancer Research 2002;62:4507–13.
[18] Relles D, Baek J, Witkiewicz A, Yeo CJ. Periampullary and duode-nal neoplasms in neurofibromatosis type 1: two cases and an updated20-year review of the literature yielding 76 cases. Journal of Gastro-intestinal Surgery 2010;14:1052–61.
[19] Fuller CE, Williams GT. Gastrointestinal manifestations of type 1neurofibromatosis (von Recklinghausen’s disease). Histopathology1991;19:1–11.
[20] Takazawa Y, Sakurai S, Sakuma Y, et al. Gastrointestinal stromaltumors of neurofibromatosis type 1 (von Recklighausen’s disease).American Journal of Surgical Pathology 2005;29:755–63.
[21] Wang JH, Lasota J, Miettinen M. Succinate dehydrogenase subunit B(SDHB) is expressed in neurofibromatosis 1-associated gastrointes-tinal stromal tumors (Gists): implications for the SDHB expressionbased classification of Gists. Journal of Cancer 2011;16(2):90–3.
[22] van Balkom ID, Hennekam RC. Dermal eccrine cylindromatosis.Journal of Medical Genetics 1994;31:321–4.
[23] Sima R, Vanecek T, Kacerovska D, et al. Brooke–Spiegler syndrome:report of 10 patients from 8 families with novel germline mutations:evidence of diverse somatic mutations in the same patient regardless
of tumor type. Diagnostic Molecular Pathology 2010;19:83–91.[24] van den Ouweland AM, Elfferich P, Lamping R, et al. Identification ofa large rearrangement in CYLD as a cause of familial cylindromatosis.Familial Cancer 2011;10:127–32.

Oncolo
G. Ponti et al. / Critical Reviews in[25] Blake PW, Toro JR. Update of cylindromatosis gene (CYLD)mutations in Brooke–Spiegler syndrome: novel insights intothe role of deubiquitination in cell signaling. Human Mutation2009;30:1025–36.
[26] Biggs PJ, Wooster R, Ford D, et al. Familial cylindromatosis (tur-ban tumour syndrome) gene localised to chromosome 16q12-q13:evidence for its role as a tumour suppressor gene. Nature Genetics1995;11:441–3.
[27] Young AL, Kellermayer R, Szigeti R, Tészás A, Azmi S, Celebi JT.CYLD mutations underlie Brooke–Spiegler, familial cylindromatosis,and multiple familial trichoepithelioma syndromes. Clinical Genetics2006;70:246–9.
[28] Ponti G, Nasti S, Losi L, et al. Brooke–Spiegler syndrome: reportof two cases not associated with a mutation in the CYLD andPTCH tumor-suppressor genes. Journal of Cutaneous Pathology2012;39:366–71.
[29] Bowen S, Gill M, Lee DA, et al. Mutations in the CYLD gene inBrooke–Spiegler syndrome, familial cylindromatosis, and multiplefamilial trichoepithelioma: lack of genotype–phenotype correlation.Journal of Investigative Dermatology 2005;124:919–20.
[30] Saggar S, Chernoff KA, Lodha S, et al. CYLD mutations infamilial skin appendage tumours. Journal of Medical Genetics2008;45:298–302.
[31] Baican A, Has C, Crisan C, Orasan R, Petrescu M, Machet L. Multi-ple cutaneous cylindromas associated with parotid and submandibulargland cylindromas. Annales de Dermatologie et de Venereologie1998;125:909–11.
[32] Kazakov DV, Benkova K, Michal M, Vanecek T, Kacerovska D, Ska-lova A. Skin type spiradenoma of the parotid gland with malignanttransformation: report of a case with analysis of the CYLD gene.Human Pathology 2009;40:1499–503.
[33] Kazakov DV, Zelger B, Rütten A, et al. Morphologic diversity ofmalignant neoplasms arising in preexisting spiradenoma, cylindroma,and spiradenocylindroma based on the study of 24 cases, sporadicor occurring in the setting of Brooke–Spiegler syndrome. AmericanJournal of Surgical Pathology 2009;33:705–19.
[34] Bignell GR, Warren W, Seal S, et al. Identification of the familial cylin-dromatosis tumour suppressor gene. Nature Genetics 2000;25:160–5.
[35] Kazakov DV, Thoma-Uszynski S, Vanecek T, Kacerovska D, Gross-mann P, Michal M. A case of Brooke–Spiegler syndrome with a novelgermline deep intronic mutation in the CYLD gene leading to intro-nic exonization, diverse somatic mutations, and unusual histology.American Journal of Dermatopathology 2009;31:664–73.
[36] Kazakov DV, Vanecek T, Zelger B, et al. Multiple (familial) trichoe-pitheliomas: a clinicopathological and molecular biological study,including CYLD and PTCH gene analysis, of a series of 16 patients.American Journal of Dermatopathology 2011;33:251–65.
[37] Kazakov DV, Schaller J, Vanecek T, Kacerovska D, Michal M.Brooke–Spiegler syndrome: report of a case with a novel mutation inthe CYLD gene and different types of somatic mutations in benign andmalignant tumors. Journal of Cutaneous Pathology 2010;37:886–90.
[38] Amaro C, Freitas I, Lamarão P, Afonso A, Skrzypczak M, HeinritzW. Multiple trichoepitheliomas—a novel mutation in the CYLD gene.Journal of the European Academy of Dermatology and Venereology2010;24:844–6.
[39] Scholz IM, Nümann A, Froster UG, Helmbold P, Enk AH,Näher H. New mutation in the CYLD gene within a family withBrooke–Spiegler syndrome. Journal der Deutschen Dermatologis-chen Gesellschaft 2010;8:99–101.
[40] Parren LJ, Bauer B, Hamm H, Frank J. Brooke–Spiegler syndromecomplicated by unilateral hearing loss. International Journal of Der-matology 2008;47(Suppl. 1):56–9.
[41] Muir EG, Bell AJY, Barlow KA. Multiple primary carcinomata of the
colon, duodenum and larynx associated with keratoacanthoma of theface. British Journal of Surgery 1967;54:191–5.[42] Ponti G, Losi L, Di Gregorio C, et al. Identification of Muir–Torre syn-drome among patient with sebaceous tumors and keratoacanthomas:
gy/Hematology 85 (2013) 239–256 253
role of clinical features, microsatellite instability and immunohisto-chemistry. Cancer 2005;103:1018–25.
[43] Fernandez-Flores A. Considerations on the performance of immu-nohistochemistry for mismatch repair gene proteins in casessebaceous neoplasms and keratoacanthomas with reference toMuir–Torre syndrome. American Journal of Dermatopathology2011;(November):23.
[44] Kanitakis J. Adnexal tumours of the skin as markers of cancer-pronesyndromes. Histopathology 2010;56:133–47.
[45] Ponti G, Losi L, Pedroni M, et al. Value of MLH1 and MSH2mutations in the appearance of Muir–Torre syndrome phenotype inHNPCC patients presenting sebaceous gland tumors or keratoacant-homas. Journal of Investigative Dermatology 2006;126:2302–7.
[46] Losi L, Scarselli A, Benatti P, et al. Relationship between MUC5ACand alterated expression of MLH1 protein in mucinous and non-mucinous colorectal carcinomas. Pathology, Research and Practice2004;200:371–7.
[47] Arnold A, Payne S, Fisher S, et al. An individual with Muir–Torresyndrome found to have a pathogenic MSH6 gene mutation. FamilialCancer 2007;6:317–21.
[48] Chhibber V, Dresser K, Mahalingam M. MSH-6: extending the relia-bility of immunohistochemistry as a screening tool in Muir–Torresyndrome. Modern Pathology 2008;21:159.
[49] Roncari B, Pedroni M, Maffei S, et al. Frequency of constitutionalMSH6 mutations in a consecutive series of families with clinicalsuspicion of HNPCC. Clinical Genetics 2007;72:230–7.
[50] Chhibber V, Dresser K, Mahalingam M. MSH-6: extending the relia-bility of immunohistochemistry as a screening tool in Muir–Torresyndrome. Modern Pathology 2008;21:159–64.
[51] Shalin SC, Lyle S, Calonje E, Lazar AJ. Sebaceous neoplasia and theMuir–Torre syndrome: important connections with clinical implica-tions. Histopathology 2010;56:133–47.
[52] Mangold E, Pagenstecher C, Leister M, et al. A genotype–phenotypecorrelation in HNPCC: strong predominance of msh2 mutations in41 patients with Muir–Torre syndrome. Journal of Medical Genetics2004;41:567–72.
[53] Singh RS, Grayson W, Redston M, et al. Site and tumor type pre-dicts DNA mismatch repair status in cutaneous sebaceous neoplasia.American Journal of Surgical Pathology 2008;32:936–42.
[54] Ponti G, Ponz de Leon M, Losi L, et al. Different phenotypesin Muir–Torre syndrome: clinical and biomolecular characteri-zation in two Italian families. British Journal of Dermatology2005;152:1335–8.
[55] Ponti G, Ponz de Leon M. Muir–Torre syndrome. The Lancet Onco-logy 2005;12:980–7.
[56] Ponti G, Ponz de Leon M, Maffei S, et al. Attenuated familialadenomatous polyposis and Muir–Torre syndrome linked to com-pound biallelic constitutional MYH gene mutations. Clinical Genetics2005;68:442–7.
[57] Ponti G, Venesio T, Losi L, et al. BRAF mutations inmultiple sebaceous hyperplasias of patients belonging to MYH-associated polyposis pedigrees. Journal of Investigative Dermatology2007;127:1387–91.
[58] Zampeli VA, Makrantonaki E, Tzellos T, Zouboulis CC. New pharma-ceutical concepts for sebaceous gland diseases: implementing today’spre-clinical data into tomorrow’s daily clinical practice. Current Phar-maceutical Biotechnology 2012;(January) [Epub ahead of print].
[59] Zouboulis CC, Boschnakow A. Chronological ageing and photoa-geing of the human sebaceous gland. Clinical and ExperimentalDermatology 2001;26:600–7.
[60] Zouboulis CC. Acne and sebaceous gland function. Clinics in Der-matology 2004;22:360–6.
[61] Alm T, Dencker H, Lunderquist A, et al. Gardner’s syndrome. Acta
Chirurgica Scandinavica 1973;139:660–5.[62] Kanitakis J. Adnexal tumours of the skin as markers of cancer-pronesyndromes. Journal of the European Academy of Dermatology andVenereology 2010;24:379–87.

2 Oncolo
54 G. Ponti et al. / Critical Reviews in[63] Ponti G, Losi L, Pellacani G, et al. Wnt pathway, angiogenetic andhormonal markers in sporadic and familial adenomatous polyposisassociated juvenile nasopharyngeal angiofibromas (JNA). AppliedImmunohistochemistry and Molecular Morphology 2008;16:173–8.
[64] Nakamura Y. The role of the adenomatous polyposis coli (APC) genein human cancers. Advances in Cancer Research 1993:621.
[65] Lipkin M, Winawer SJ, Sherlok P. Early identification of individualsat increased risk for cancer of the large intestine. Clinical Bulletin1981;11:13–21.
[66] Jarviven HJ. Epidemiology of familial adenomatous polyposis inFinland: impact of family screening on the colorectal cancer rate andsurvival. Gut 1992;33:357–60.
[67] Houlston R, Crabtree M, Phillips R, Crabtree M, Tomlinson I. Explai-ning differences in the severity of familial adenomatous polyposis andthe search for modifier genes. Gut 2001;48:1–5.
[68] Mitry E, Benhamiche AM, Jouve JL, Clinard F, Finn-Faivre C,Faivre J. Colorectal adenocarcinoma in the patients under 45years of age: comparison with older patients in a well-definedFrench population. Diseases of the Colon and Rectum 2001;44:380–7.
[69] De Pietri S, Sassatelli R, Roncucci L, et al. Clinical and biologicalfeatures of adenomatosis coli in Northern Italy. Scandinavian Journalof Gastroenterology 1995;30:771–9.
[70] Caspari R, Olschwang S, Friedl W, et al. Familial adenomatous poly-posis: desmoids tumors and lack of ophthalmic lesions (CHRPE)associated with APC mutations beyond codon 1,444. Human Mole-cular Genetics 1995;4:337–40.
[71] Spirio L, Green J, Robertson J, et al. The identical 5′ splice-siteacceptor mutation in five attenuated APC families from Newfound-land demonstrates a founder effect. Human Genetics 1999;105:388–98.
[72] Caspari R, Friedl W, Mandl M, et al. Familial adenomatous polypo-sis: mutation at codon 1309 and early onset of colon cancer. Lancet1994;343:629–32.
[73] Bertagnolli MM, Eagle CJ, Zauber AG, et al. Adenoma Preven-tion with Celecoxib Study Investigators: five-year efficacy and safetyanalysis of the adenoma prevention with celecoxib trial. Cancer Pre-vention Research (Philadelphia) 2009;2:310–21.
[74] Vasen HF, Möslein G, Alonso A, et al. Guidelines for the cli-nical management of familial adenomatous polyposis (FAP). Gut2008;57:704–13.
[75] Agostini M, Bedin C, Pucciarelli S, et al. APC I1307K mutationsand forkhead box gene (FOXO1A): another piece of an interestingcorrelation. The International Journal of Biological Markers 2011;13,http://dx.doi.org/10.5301/JBM.2011.8908 [Epub ahead of print].
[76] Gorlin RJ. Nevoid basal cell carcinoma syndrome. Dermatologic Cli-nics 1995;13:113–25.
[77] Evans DG, Ladusans EJ, Rimmer S, Burnell LD, Thakker N, FarndonPA. Complications of the naevoid basal cell carcinoma syndrome:results of a population based study. Journal of Medical Genetics1993;30:460–4.
[78] Pastorino L, Cusano R, Nasti S, et al. Molecular characterizationof Italian nevoid basal cell carcinoma syndrome patients. HumanMutation 2005;25:322–3.
[79] Stone DM, Hynes M, Armanini M, et al. The tumour-suppressor genepatched encodes a candidate receptor for Sonic hedgehog. Nature1996;384:129–34.
[80] Lo Muzio L. Nevoid basal cell carcinoma syndrome (Gorlin syn-drome). Orphanet Journal of Rare Diseases 2008;3(November):32.
[81] Jones EA, Sajid MI, Shenton A, Evans DG. Basal cell carcinomas inGorlin syndrome: a review of 202 patients. Journal of Skin Cancer2011:217378.
[82] Johnson RL, Rothman AL, Xie J, et al. Human homolog of pat-
ched, a candidate gene for the basal cell nevus syndrome. Science1996;272:1668–71.[83] Diniz MG, Borges ER, Guimarães AL, et al. PTCH1 isoforms inodontogenic keratocysts. Oral Oncology 2009;45:291–5.
gy/Hematology 85 (2013) 239–256
[84] Wicking C, Shanley S, Smyth I, et al. Most germ-line mutations in thenevoid basal cell carcinoma syndrome lead to a premature terminationof the PATCHED protein, and no genotype–phenotype correla-tions are evident. American Journal of Human Genetics 1997;60:21–6.
[85] Barreto DC, Gomez RS, Bale AE, Boson WL, De Marco L.PTCH gene mutations in odontogenic keratocysts. Journal of DentalResearch 2000;79:1418–22.
[86] Woolgar JA, Rippin JW, Browne RM. The odontogenic kera-tocyst and its occurrence in the nevoid basal cell carcinomasyndrome. Oral Surgery, Oral Medicine, Oral Pathology 1987;64:727–30.
[87] Lench NJ, Telford EA, High AS, Markham AF, Wicking C,Wainwright BJ. Characterization of human patched germ line muta-tions in nevoid basal cell carcinoma syndrome. Human Genetics1997;100:497–502.
[88] Kimonis VE, Goldstein AM, Pastakia B, et al. Clinical manifestationsin 105 persons with nevoid basal cell carcinoma syndrome. AmericanJournal of Medical Genetics 1997;69:299–308.
[89] Bree AF, Shah MR, BCNS Colloquium Group. Consensus state-ment from the first international colloquium on basal cell nevussyndrome (BCNS). American Journal of Medical Genetics Part A2011;155A:2091–7, http://dx.doi.org/10.1002/ajmg.a.34128.
[90] Ponti G, Pastorino L, Pollio A, et al. Ameloblastoma: a neglectedcriterion for nevoid basal cell carcinoma (Gorlin) syndrome. FamCancer1 2012;May [Epub ahead of print].
[91] Scales SJ, de Sauvage FJ. Mechanisms of Hedgehog pathway activa-tion in cancer and implications for therapy. Trends in PharmacologicScience 2009;30(6):303–12.
[92] Kasper M, Jaks V, Hohl D, Toftgård R. Basal cellcarcinoma—molecular biology and potential new therapies.Journal of Clinical Investigation 2012;122:455–63.
[93] Starink TM, van der Veen JP, Arwert F, et al. The Cowden syn-drome: a clinical and genetic study in 21 patients. Clinical Genetics1986;29:222–33.
[94] Weary PE, Gorlin RJ, Gentry WC, Comer JE, Greer KE. Multiplehamartoma syndrome (Cowden’s disease). Archives of Dermatology1972;106:682–90.
[95] Eng C. In: Pagon RA, Bird TD, Dolan CR, Stephens K, Adam MP,editors. GeneReviewsT [Internet]. PTEN hamartoma tumor syndrome(PHTS). Seattle, WA: University of Washington, Seattle; 1993–2001,November [updated 2011 July 21].
[96] Salem OS, Steck WD. Cowden’s disease (multiple hamartoma andneoplasia syndrome). Journal of the American Academy of Derma-tology 1983;8:686–96.
[97] Frayling IM, Bodmer WF, Tomlinson IP. Allele loss in colorectalcancer at the Cowden disease/juvenile polyposis locus on 10q. CancerGenetics and Cytogenetics 1997;97:64–9.
[98] Kurek KC, Howard E, Tenant L, et al. PTEN hamartoma of soft tissue:a distinctive lesion in PTEN syndromes. American Journal of SurgicalPathology 2012;(March) [Epub ahead of print].
[99] Haggitt RC, Reed BJ. Hereditary gastrointestinal polyposis syndro-mes. American Journal of Pathology 1986;12:871–87.
[100] Christensen AH, Ishak KG. Benign tumors and pseudotumorsof the gallbladder Report of 180 cases. Archives of Pathology1970;90:423–32.
[101] Marra G, Armelao F, Vecchio FM, Percesepe A, Anti M. Cowden’sdisease with extensive gastrointestinal polyposis. Journal of ClinicalGastroenterology 1993;16:1–6.
[102] Stanich PP, Owens VL, Sweetser S, et al. Colonic polyposisand neoplasia in Cowden syndrome. Mayo Clinic Proceedings2011;86:489–92.
[103] Pilarski R. Cowden syndrome: a critical review of the clinical litera-
ture. Journal of Genetic Counseling 2009;18:13–27.[104] Coriat R, Mozer M, Caux F, et al. Endoscopic findings in Cow-den syndrome. Endoscopy 2011;43(August (8)):723–6 [Erratum in:Endoscopy 2011;43:1096, Epub 2011 March 24].

Oncolo
G. Ponti et al. / Critical Reviews in[105] Williard W, Borgen P, Bol R, Tiwari R, Osborne M. Cowden’sdisease. A case report with analysis at the molecular level. Cancer1992;69:2969–74.
[106] Al-Zaid T, Ditelberg JS, Prieto VG, et al. Trichilemmomas showloss of PTEN in Cowden syndrome but only rarely in spo-radic tumors. Journal of Cutaneous Pathology 2012;(February),http://dx.doi.org/10.1111/j.1600-0560.2012.01888.x [Epub ahead ofprint].
[107] Zabetian S, Mehregan D. Cowden syndrome: report of two caseswith immunohistochemical analysis for PTEN expression. AmericanJournal of Dermatopathology 2012;(April) [Epub ahead of print].
[108] Mester JL, Zhou M, Prescott N, Eng C. Papillary renal cell carci-noma is associated with PTEN hamartoma tumor syndrome. Urology2012;(February) [Epub ahead of print].
[109] Barletta JA, Bellizzi AM, Hornick JL. Immunohistochemical stainingof thyroidectomy specimens for PTEN can aid in the identificationof patients with Cowden syndrome. American Journal of SurgicalPathology 2011;35:1505–11.
[110] Tan MH, Mester JL, Ngeow J, Rybicki LA, Orloff MS, Eng C.Lifetime cancer risks in individuals with germline PTEN mutations.Clinical Cancer Research 2012;18:400–7.
[111] Ngeow J, Mester J, Rybicki LA, Ni Y, Milas M, Eng C. Incidenceand clinical characteristics of thyroid cancer in prospective series ofindividuals with Cowden and Cowden-like syndrome characterizedby germline PTEN SDH, or KLLN alterations. Journal of ClinicalEndocrinology and Metabolism 2011;96(12):E2063–71.
[112] Heald B, Mester J, Rybicki L, Orloff MS, Burke CA, Eng C.Frequent gastrointestinal polyps and colorectal adenocarcinomas ina prospective series of PTEN mutation carriers. Gastroenterology2010;139(6):1927–33.
[113] Nelen MR, Padberg GW, Peeters EA, et al. Localization of thegene for Cowden disease to chromosome 10q22-23. Nature Genetics1996;13:114–6.
[114] Smith JR, Marqusee E, Webb S, et al. Thyroid nodules and cancer inchildren with PTEN hamartoma tumor syndrome. Journal of ClinicalEndocrinology and Metabolism 2011;96:34–7.
[115] Laury AR, Bongiovanni M, Tille JC, Kozakewich H, Nosé V. Thy-roid pathology in PTEN-hamartoma tumor syndrome: characteristicfindings of a distinct entity. Thyroid 2011;21:135–44.
[116] Singh G, Chan AM. Post-translational modifications of PTEN andtheir potential therapeutic implications. Current Cancer Drug Targets2011;11:536–47.
[117] Lindor NM, Hand J, Burch PA, Gibson LE. Birt–Hogg–Dube syn-drome: an autosomal dominant disorder with predisposition to cancersof the kidney, fibrofolliculomas, and focal cutaneous mucinosis. Inter-national Journal of Dermatology 2001;40:653–6.
[118] Nickerson ML, Warren MB, Toro JR, et al. Mutations in a novel genelead to kidney tumors, lung wall defects, and benign tumors of thehair follicle in patients with the Birt–Hogg–Dube syndrome. CancerCell 2002;2:157–64.
[119] Verine J, Pluvinage A, Bousquet G, et al. Hereditary renal cancersyndromes: an update of a systematic review. European Urology2010;58(November (5)):701–10.
[120] Houweling AC, Gijezen LM, Jonker MA, et al. Renal can-cer and pneumothorax risk in Birt–Hogg–Dubé syndrome; ananalysis of 115 FLCN mutation carriers from 35 BHD fami-lies. British Journal of Cancer 2011;105(December (12)):1912–9,http://dx.doi.org/10.1038/bjc.2011.463.
[121] Baba M, Hong SB, Sharma N, et al. Folliculin encoded by theBHD gene interacts with a binding protein FNIP1, and AMPK,and is involved in AMPK and mTOR signaling. Proceedings ofthe National Academy of Sciences of the United States of America2006;103:15552–7.
[122] Hopkins TG, Maher ER, Reid E, Marciniak SJ. Recurrent pneumot-horax. Lancet 2011;377(9777):1624.
[123] Zbar B, Alvord WG, Glenn G, et al. Risk of renal and colonicneoplasms and spontaneous pneumothorax in the Birt–Hogg–Dubé
gy/Hematology 85 (2013) 239–256 255
syndrome. Cancer Epidemiology, Biomarkers and Prevention2002;11:393–400.
[124] Birt AR, Hogg GR, Dube J. Hereditary multiple fibrofolliculomaswith trichodiscomas and acrochordons. Archives of Dermatology1977;113:1674–7.
[125] Pavlovich CP, Walther MM, Eyler RA, et al. Renal tumors in theBirt–Hogg–Dubé syndrome. American Journal of Surgical Pathology2002;26:1542–52.
[126] Furuya M, Tanaka R, Koga S, et al. Pulmonary cysts ofBirt–Hogg–Dubé syndrome: a clinicopathologic and immunohisto-chemical study of 9 families. American Journal of Surgical Pathology2012;36:589–600.
[127] Adley B, Smith N, Nayar R, Yang X. Birt Hogg Dubè syndrome clin-copathological findings and genetic alterations. Archives of Pathologyand Laboratory Medicine 2006;130:1865–70.
[128] Palmirotta R, Savonarola A, Ludovici G, et al. Association betweenBirt Hogg Dube syndrome and cancer predisposition. AnticancerResearch 2010;30:751–7.
[129] Cohen HT, McGovern FJ. Renal-cell carcinoma. New England Jour-nal of Medicine 2005;353:2477–90.
[130] Badeloe S, Frank J. Clinical and molecular genetic aspectsof hereditary multiple cutaneous leiomyomatosis. EuropeanJournal of Dermatology 2009;19(November–December (6)):545–51.
[131] Pithukpakorn M, Toro JR, Hereditary leiomyomatosis and renal cellcancer. In: Pagon RA, Birt TD, Dolan CR, Stephens K, Adam MP,editors. GeneReviewsT [Internet]. Seattle, WA: University of Was-hington, Seattle; 1993–2006 July [update 2010 November 02].
[132] Wei MH, Toure O, Glenn GM, et al. Novel mutation in FH andexpansion of the spectrum of phenotypes expressed in families withhereditary leiomyomatosis and renal cell cancer. Journal of MedicalGenetics 2006;43:18–27.
[133] Smit DL, Mensenkamp AR, Badeloe S, et al. Hereditary leiomyoma-tosis and renal cell cancer in families referred for fumarate hydratasegermline mutation analysis. Clinical Genetics 2011;79:49–59.
[134] Alam NA, Barelay E, Rowan AJ, et al. Clinical features of multi-ple cutaneous and uterine leiomyomatosis: an underdiagnosed tumorsyndrome. Archives of Dermatology 2005;141:199–206.
[135] Stewart L, Glenn GM, Stratton P, et al. Association of germline muta-tions in the fumarate hydratase gene and uterine fibroids in womanwith hereditary leiomyomatosis and renal cell cancer. Archives ofDermatology 2008;144:1584–92.
[136] Toro JR, Nickerson ML, Wei MH, et al. Mutations in the fuma-rate hydratase gene cause hereditary leiomyomatosis and renal cellcancer in North America. American Journal of Human Genetics2003;73:95–106.
[137] Lehtonen HJ, Kiuru M, Ylisaukko-Oja SK, et al. Increased risk ofcancer in patients with fumarate hydratase germline mutation. Journalof Medical Genetics 2006;43:523–6.
[138] Launonen V, Vierina O, Kiuru M, et al. Inherited susceptibility touterine leiomyomatosis and renal cell cancer. Proceedings of theNational Academy of Sciences of the United States of America2001;98:3387–92.
[139] Ylisaukko-oja SK, Kiuru M, Lehtonen HJ, et al. Analysis of fuma-rate hydratase mutations in a population-based series of early onsetuterine leiomyosarcoma patients. International Journal of Cancer2006;119:283–7.
[140] Tolvanen J, Uimari O, Ryynänen M, Aaltonen LA, VahteristoP. Strong family history of uterine leiomyomatosis warrantsfumarate hydratase mutation screening. Human Reproduction2012;27:1865–9.
[141] Lehtonen HJ. Hereditary leiomyomatosis and renal cell cancer:update on clinical and molecular characteristics. Familial Cancer
2011;10:397–411.[142] Gardie B, Remenieras A, Kattygnarath D, et al. Novel FH muta-tions in families with hereditary leiomyomatosis and renal cell cancer

2 Oncolo
B
cItcpotrhec
mEotmein
mamcla
tao2ooctd
tOMplpn
rIocsmomIo
MnAsasrottrt
56 G. Ponti et al. / Critical Reviews in
(HLRCC) and patients with isolated type 2 papillary renal cell carci-noma. Journal of Medical Genetics 2011;48:226–34.
[143] Merino MJ, Torres-Cabala C, Pinto P, Linehan WM. The morphologicspectrum of kidney tumors in hereditary leiomyomatosis and renalcell carcinoma (HLRCC) syndrome. American Journal of SurgicalPathology 2007;31:1578–85.
[144] Lehtonen HJ, Blanco I, Piulats JM, Herva R, Launonen V, AaltonenLA. Conventional renal cancer in a patient with fumarate hydratasemutation. Human Pathology 2007;38:793–6.
[145] Gatalica Z, Lilleberg SL, Monzon FA, et al. Renal medullary carci-nomas: histopathologic phenotype associated with diverse genotypes.Human Pathology 2011;42:1979–88.
[146] Ahvenainen T, Lehtonen HJ, Lehtonen R, et al. Mutation screening offumarate hydratase by multiplex ligation-dependent probe amplifica-tion: detection of exonic deletion in a patient with leiomyomatosis andrenal cell cancer. Cancer Genetics and Cytogenetics 2008;183:83–8.
[147] Tomlinson IP, Alam NA, Rowan AJ, et al. Multiple leiomyoma con-sortium germline mutations in FH predispose to dominantly inheriteduterine fibroids, skin leiomyomata and papillary renal cell cancer.Nature Genetics 2002;30:406–10.
[148] Bardella C, El-Bahrawy M, Frizzell N, et al. Aberrant succina-tion of proteins in fumarate hydratase-deficient mice and HLRCCpatients is a robust biomarker of mutation status. Journal of Pathology2011;225:4–11.
[149] Maxwell PH. Seeing the smoking gun: a sensitive and specific methodto visualize loss of the tumour suppressor, fumarate hydratase, inhuman tissues. Journal of Pathology 2011;225:1–3.
[150] Catherino WH, Malik M, Driggers P, et al. Novel, orally active selec-tive progesterone reception modulator CP8947 inhibits leiomyomacell proliferation without adversely affecting endometrium or myo-metrium. Journal of Steroid Biochemistry and Molecular Biology2010;122:279–86.
iographies
Giovanni Ponti, M.D., Ph.D. is assistant professor of clini-al pathology at the University of Modena and Reggio Emilia,taly. His primary research goals are directed toward unders-anding the clinical and genetic background of the hereditaryancer syndromes, the cancer genetics, the prevention of neo-lastic diseases and their targeted therapy. He is involved inngoing clinical trials and studies evaluating new oncologicreatments based on experimental targeted-therapies and inesearch projects regarding cells cultures obtained by bothealthy and gene-carriers patients. His main areas of inter-st are the molecular mechanisms and genetics of hereditaryancer syndromes and rare tumors.
Giovanni Pellacani, D., Ph.D. is chairman of the Depart-ent of Dermatology at the University of Modena and Reggiomila. He is professor of dermatology in the Medical Facultyf same University and Director of the School of Derma-ology and Venereology. Since 1995 he practices researchainly in the field of cutaneous physiopathology, skin bio-
ngineering for the evaluation of inflammatory diseases, nonnvasive diagnosis in dermato-oncology. In particular, mela-oma and pigmented skin lesions, their early identification by
otg
gy/Hematology 85 (2013) 239–256
eans of dermoscopy in combination with system for imagenalysis and automated diagnosis, and in vivo reflectance-ode confocal scanning laser microscopy for the study of
ytological and architectural aspects of the skin and of skinesions, in correlation with dermoscopy and histopathologyre the present fields of research.
Stefania Seidenari, M.D., Ph.D., is contract professor ofhe Department of Dermatology at the University of Modenand Reggio Emila. She obtained his Ph.D. She was Directorf the School of Specialization in Dermatology from 2000 to011 and Head of the Department of Dermatology, Universityf Modena from Nov 2010 to September 2011. Main fieldsf her research is Melanoma (familial melanoma; hereditaryancer syndrome; genodermatosis), Allergic contact dermati-is; irritant contact dermatitis; atopic dermatitis; non invasiveiagnosis and image analysis.
Annamaria Pollio, D.M.D. is oral medicine specialist ofhe Advanced Program in Oral Medicine at the Department ofdontostomatological and Maxillofacial Sciences, School ofedicine and Surgery, Federico II University of Naples. Her
rimary research areas are: the hereditary cancer syndromesinked to maxillofacial and oral stigmata, oral cancer andre-neoplastic oral lesions, prevention of rare odontogeniceoplastic diseases and their immunologic targeted therapies.
Umberto Muscatello, M.D. is emeritus professor of gene-al Pathology at the University of Modena and Reggio Emilia,taly. He was Dean of the Medical Faculty and Full Professorf Molecular and Cell Pathology in the Faculty of Bios-iences and Biotechnology in the same University. His maincientific interests were focused on the study of the funda-ental mechanisms of disease through an integrated analysis
f molecular and structural properties of cell components inodel systems. At the present he is associated member at the
nstitute of Nanosciences of the National Research Councilf Italy.
Aldo Tomasi, M.D., Ph.D. is rector of the University ofodena and Reggio Emilia, Italy. He is professor of cli-
ical pathology in the medical faculty of same University.fter graduation in medicine and surgery in Modena Univer-
ity. He obtained his Ph.D. in biochemistry and biophysicst Brunel University of London, U.K. in 1985. His maincientific interests were first focused on the role of freeadicals and of oxidative stress in the aethio-pathogensisf spontaneous and model diseases. Founding Member ofhe Society for Free Radical Research (1981), he was elec-ed secretary of the Society from 1998 to 2002. In moreecent years, his main research interests are focused onhe potential role of proteomic analysis in the diagnosis
f various pathological situations including the differen-iation between benign and potentially malignant tumourrowth.