Embed Size (px)
Citation preview

Eur J Haematol 1989;43:215-219
Key words: late relapse - leukemia - prognosis
Can late relapse be predicted at initial diagnosis in childhood acute lymphoblastic leukemia?
Jukka Rautonen & Martti A. Siimes Children’s Hospital, University of Helsinki, Helsinki, Finland
We have investigated whether any prognostic factor can be used to identify those children who have a relapse after discontinuation of therapy for acute lymphoblastic leukemia (ALL). Our population-based series comprised 167 children with newly diagnosed ALL. The 3-year event-free survival rate in these children was 65%. Maintenance therapy was electively discontinued for 120 patients, 20 of whom have subsequently had a relapse 1 to 27 months later. In multivariate analysis the risk of late relapse in the 15 patients with initially enlarged kidneys was 4.5-fold (95% confidence limits 1.7-11.8) that of the others (p < 0.01). The risk in the 18 patients with initially elevated CSF protein concentration (> 0.4 g/l) or leukocyte count (> 5 x 106/1), but with no blasts in the CSF, was 3.8-fold (1.5-9.6) that of the others (p < 0.01). Our results indicate that enlarged kidneys or abnormal CSF findings at initial diagnosis are associated with an increased risk of late relapse in children with ALL.
Accepted for publication May I , 1989
Although more than 20 prognostic factors are rec- ognized in childhood acute lymphoblastic leukemia (ALL) (1-3), their predictive value seems to disap- pear soon after therapy is initiated (4-S), making it difficult to identify patients with an increased risk of late relapse. Of the patients whose maintenance therapy is electively discontinued after 2-3 yr of pri- mary remission, 10-20% subsequently have a re- lapse (4, 9-12) which may lead to death. We have investigated whether any of the initial prognostic factors can be used to identify these patients, since modification of their induction or maintenance therapy might be worth studying.
Patients and methods Our population-based series comprised all the 173 chil- dren with newly diagnosed ALL who were admitted to
the Children’s Hospital, University of Helsinki, during the 10-yr period from 1975 to 1984. 6 of these patients had Down’s syndrome and were excluded from the study. The mean age of the remaining 167 patients was 4.9 yr with a range from 3 months to 16 yr. The numbers of boys and girls were 84 and 83, respectively. Therapy could be electively discontinued in 120 pa- tients, 20 of whom have subsequently had a late re- lapse. For the purpose of this study, a late relapse was defined as any relapse occurring after the elective dis- continuation of therapy.
In all cases the diagnosis of ALL was based on a bone marrow aspirate. From 1979, in addition, surface marker and karyotype analyses were performed rou- tinely. The therapeutic regimens used were routine Scandinavian protocols (1 3, 14). Specifically, CNS pro- phylaxis was accomplished with intrathecal methotrex- ate combined with either cranial irradiation (1800 or 2400 rads) in 113 cases or with intermediate-dose meth-

216 RAUTONEN & SIIMES
otrexate (500 or lo00 mg/m2) in 54 cases with standard risk ALL. If a patient remained in remission, mainte- nance therapy was electively discontinued 3 yr after the initial diagnosis.
2 patients were lost to follow-up owing to emigra- tion. Both were in primary remission of 7 and 36 months duration, respectively. All patients were fol- lowed closely during therapy, and seen at least four times a year during the first 2 yr after discontinuation of therapy. The closing date of follow-up for this study was August 31, 1988. Thus, the patients in primary remission had been off therapy for 8-126 months (mean, 61 months).
An intravenous pyelogram was performed on every patient at the time of initial diagnosis prior to the start of chemotherapy. If one or both kidneys were found to be enlarged (> + 2 SD of the normal), one kidney was irradiated (300-500 rads).
Cerebrospinal fluid (CSF) leukocytes were counted manually in Biirker chambers. The CSF protein con- centration was determined with routine methods. The CSF protein concentration from 3 patients had not been studied prior to the initiation of therapy; these patients were excluded from the analyses concerning the prognostic effect of CNS findings. For the pur- poses of this study, the patients were divided into three groups according to the initial CSF findings: 1. those with normal CSF (protein concentration 5 0.4 g/l and leukocyte count 5 5 x 106/1, no blast cells); 2. those with abnormal CSF (protein concentration > 0.4 g/l or leukocyte count > 5 x 106/1, but no blast cells); and 3. those with CNS leukemia (blast cells in the CSF).
100 - normal kidneys (nZl05) 9 - 80
2
v) 0
60 3 enlarged kidneys (n=l5) a
2 0
0 2 4 6 8 10
YEARS AFTER DISCONTINUATION OF THERAPY
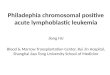
Figure 1. The relation between initial kidney enlargement and the risk of late relapse in children with ALL (p = 0.0003).
Serum glutamate pyruvate transaminase (SGPT) ac- tivity was measured by routine methods before the initiation of chemotherapy (15). Blast clearance was defined as the time interval from diagnosis to the day when no blast cells could be detected in the differential count of 200 peripheral white blood cells (WBC) (16).
All statistical analyses were performed with the BMDP statistical software package (17). A forward stepping Cox proportional hazards model was used to identify the factors independently associated with prog- nosis. This analysis was used on three groups of pa- tients: one formed by all patients, to study the initial prognostic factors; one comprising those patients who had remained in primary remission for at least 18 months, to see which prognostic factors had retained their value for at least 18 months (or one half of the duration of therapy); and one consisting of the patients in primary remission whose therapy was discontinued 36 months after diagnosis, to study whether by that time there remained any prognostic factors which could be used to predict a late relapse. The 95% confidence limits of risk ratios were calculated as exp (coeffi- cientfl.96 SE). Survival curves were constructed with the product-limit method; the Mantel-Cox test was used for univariate comparisons.
Results The 3-yr event-free survival rate of all children with ALL was 65%. Therapy was electively dis- continued for 120 patients, 20 of whom have subsequently had a relapse 1 to 27 months later. No relapses have occurred in the 64 patients whose primary remission has lasted for 64 months or more.
In univariate analysis, three prognostic factors were associated with an increased risk of late relapse. Of the 49 patients with initial WBC over 10 x 109/1, 13 have had a relapse as compared with 7 of the 71 others (p = 0.012). Closer ins- pection revealed that the worst prognosis was associated with initial WBCs of 10-20 x 109/l. Of these patients, 6 of 15 had a late relapse as compared with 14 of the 105 others, resulting in 2-yr event-free survival rates after discontinua- tion of therapy of 55% and 87% (p = 0.0046), respectively.
Initial kidney enlargement was also associated with an increased risk of late relapse. Of the 15 patients with initially enlarged kidneys, 7 have so

LATE RELAPSE IN CHILDREN WITH ALL 217
100 - relapses in this group, 4 were CNS relapses as
- Normal CSF (n-99) c 80 z u) 1 6 0 1 L Abnormal CSF n=18
a
P
z
f E 20
- 4 0 1 0'
0 2 4 6 8 10
YEARS AFTER PISCONTINUATION OF THERAPY
Figure 2. The relation between initial abnormal CSF findings (protein concentration > 0.4 g/l and/or leukocyte count > 5 x 106/1, but no blast cells) and the risk of late relapse in children with acute lymphoblastic leukemia (p = 0.004).
far had a relapse as compared with 13 of the 105 others. The 2-yr event-free survival rates were 52% and 87% (p = 0.0003), respectively (Figure 1). Of these 15 patients, 6 belonged to low-risk group (age 2-10 yr, WBC < 10 x 1@/1), 2 to high-risk group (WBC > 50 x 109/1), and the re- maining 7 to intermediate-risk group. At discon- tinuation of therapy, kidney size was assessed in 9 of these patients; in none of them were kidneys enlarged. At the time of relapse, 2 patients again had enlarged kidneys; their kidney size had not been assessed at discontinuation of therapy.
All 6 patients with initial CNS leukemia (group 3) died or relapsed before discontinuation of therapy. 7 of the 18 patients with initially elevat- ed CSF protein concentrations (n = 6, 2 relapses) or leukocyte counts (n = 6, 2 relapses) or both (n = 6, 3 relapses), but with no blast cells in the CSF, had a late relapse as compared with 12 of the 99 others, the 2-yr event-free survival rates being 60% and 87% (p = 0.004), respectively (Figure 2). Of the 18 patients with abnormal CSF findings, 8 belonged to low-risk, 4 to high-risk, and the remaining 6 to intermediate risk group. At discontinuation of therapy, all these 18 pa- tients had their CSF leukocyte count and protein concentration within normal limits. Of the 7 late
compared with 5 of the 12 relapses in the other patients.
There were no differences in the timing of late relapses between the patients with and without specific risk factor (Figures 1-2). However, of the 3 patients with both initial kidney enlarge- ment and abnormal CSF findings, 2 had a late relapse soon after discontinuation of therapy (15 and 16 wk, respectively); the 3rd patient has remained in primary remission for 53 months after discontinuation of therapy.
No other factor, such as age at diagnosis, hepatosplenomegaly, mediastinal mass, hemoglo- bin concentration, platelet count, immunologic cell type, karyotype, or FAB classification, was associated with an increased risk of late relapse. Specifically, event-free survival was similar in males (12 of 60 relapsed) and females (8 of the 60 relapsed), the 2-yr event-free survival rates being 78% and 87% (p = 0.28), respectively. Of the 12 late relapses in males, 3 were testicular relapses.
Multivariate analysis showed that only initial kidney enlargement and abnormal CSF findings were independently associated with the risk of late relapse (Table 1). The third factor identified by the stepping procedure was sex, the risk for males being 2.2-fold (95% confidence limits 0.8-
TABLE 1 The significance of prognostic factors in children with acute lymphoblastic leukemia at diagnosis (0 months) and at 18 and 36 months after diagnosis. The risk ratios of prognostic factors at 36 months (discontinuation of therapy) and their 95% con- fidence limits are given in parentheses
Time after diagnosis ~
0 mos. 18 mos. 36 mos. Risk ratio P P P
Age Sex Enl. kidneys (>2SD)
WBC Blast clearance Abnormal CSP Blasts in CSF SGPTb
ns ns
ns ns
< 0.001 < 0.01 < 0.01
< 0.001
ns ns
ns ns ns ns ns
< 0.05
ns ns
<0.01 (4.5, 1.7-11.8) ns ns
ns ns
< 0.01 (3.8, 1.5-9.6)
a CSF protein concentration > 0.4 g/l and/or CSF leukocyte count > 5 x 106/1, no blasts. SGPT = Serum glutamate pyruvate transaminase.

218 RAUTONEN & SIIMES
5.9) that for females; however, this association did not reach statistical significance (0.1 c p c 0.2).
Additional analyses of the data showed that, of the four initial prognostic factors, only one, SGPT activity, retained its value for 18 months (Table l), and even this lost its significance after 36 months. In contrast, the prognostic value of CSF protein concentration and leukocyte count (without blast cells in the CSF) was evident at diagnosis, the risk for patients with abnormal CSF then being increased 2.0-fold (1.3-3.3); the value had declined after 18 monhts during main- tenance therapy, but became strong again after therapy was electively discontinued. The other factors, blast clearance and unequivocal CNS leukemia (blast cells in the CSF), were significant only at the initial evaluation.
Discussion In the early 1970s, both the initial WBC count and the age of the patient at diagnosis were shown to affect the prognosis for at least 5 yr (18). But, according to some later studies, sex is the only prognostic factor that remains valid for more than 2 yr (6), the risk of late relapse being greater in boys (4, 5 ) , especially those over 10 yr of age (7). However, in a recent British study (8) the only prognostic factor of any significance 4-6 yr after diagnosis was again initial WBC count.
At first glance, our results may seem to contra- dict those of the previous studies. However, ini- tial WBC count was a prognostic factor in our study as well when univariate analyses were per- formed, and lost its significance only in the step- wise multivariate analysis. None of the above- mentioned studies made use of multivariate anal- ysis. Further, it seems that the variables examined in previous studies included neither CSF findings nor kidney size.
Enlarged kidney size was recently shown not to be associated with poor prognosis in children with ALL (19), and the assessment of renal size at initial diagnosis was discouraged. However, even in our material kidney size had no effect in the prognosis at initial diagnosis; instead, the
prognostic effect appeared only after discontin- uation of therapy. It seems that the significance of initial kidney enlargement remains unsettled.
The effect of SGPT, blast clearance, and ab- normal CSF on prognosis at the initial diagnosis have been reported previously (16, 20, 21) and will not be discussed in this context.
We speculate that initially enlarged kidneys or abnormal CSF findings indicate a widespread disease, the eradication of which is not satis- factorily achieved with routine therapy. When treatment is electively discontinued, proliferation of the remaining leukemic cells may continue unhampered and in due time lead to a recog- nizable relapse. This hypothesis is best illustrated by the association between abnormal CSF values and prognosis: at diagnosis the association is significant, because some, if not all, of these patients in fact already have a CNS leukemia, which appears to carry a poor prognosis (21-23). At 18 months no significant association is found because, in those patients who did not have a relapse during the first 18 months after diagnos- is, the on-going maintenance therapy suppresses the proliferation of the remaining blast cells without destroying them. At 36 months the asso- ciation reappears, because in the absence of cy- tostatics the remaining blast cells begin to prolif- erate uninhibitedly.
This pattern was also displayed by the associ- ation between initial WBC and prognosis. The risk of late relapse was not greatest in those patients with the highest WBCs and the most intensive treatment protocols, but in those with intermediate WBCs and less intensive therapy. Of the 16 patients with WBC of > 100 x 109/1, all 7 patients who survived the 1st yr are still in primary remission of 50 to 137 months duration (data not shown), whereas the patients with WBC of 10-20 x 109/1 continued to fail until 5 yr after diagnosis. The hypothesis could perhaps be generalized as follows: patients with a very heavy leukemic burden either fail early or are cured, and patients with a light leukemic burden are mostly cured, but in patients with a moderate leukemic burden routine therapy is able to sup- press all signs of the disease but is not able to

LATE RELAPSE IN CHILDREN WITH ALL 219
eradicate the malignant cells, the result being a late failure after discontinuation of therapy.
Presently, there is no direct evidence that the abnormal CSF findings indicate CNS leukemia. Nevertheless, recommendations concerning pos- sible therapeutic intervention strategies for pa- tients with initially abnormal CSF findings or enlarged kidneys are needed. It is possible that enlarged kidneys and pathologic CSF findings at initial diagnosis should be considered indicators of a heavy leukemic burden, necessitating use of more intensive treatment protocols.
References 1.
2.
3.
4.
5 .
6.
7.
8.
9.
10.
11.
Palmer MK, Hann IM, Jones PM, Evans DIK. A score at diagnosis for predicting length of remission in childhood acute lymphoblastic leukaemia. Br J Cancer 1980;42:841-9. Chessells JM. Acute lymphoblastic leukemia. Semin He- matol 1982; 19: 155-71. Poplack DG. Acute lymphoblastic leukemia in childhood. Pediatr Clin North Am 1985;32:669-98. S h o n e JV, Aur RJA, Hustu HO, Verzosa MS, Pinkel D. Three to ten years after cessation of therapy in children with leukemia. Cancer 1978;42:839-44. George SL, Aur RJA, Mauer AM, Simone JV. A reap- praisal of the results of stopping therapy in childhood leukemia. N Engl J Med 1979;300:269-73. Sather H, Coccia P, Nesbit M, Level C, Hammond D. Disappearance of the predictive value of prognostic varia- bles in childhood acute lymphoblastic leukemia. Cancer 1981;48:370-6. Woodcock BE, Anderson LM, Lilleyman JS. Age, sex and late relapse in childhood lymphoblastic leukaemia. Scand J Haematol 1984;33:323-5. Chessells JM, Hardisty RM, Richards S. Long survival in childhood lymphoblastic leukaemia. Br J Cancer 1987;55:315-9. Johansen OJ, Moe PJ. Relapse rate after cessation of therapy in childhood leukemia. Acta Paediatr Scand 1980;69:663-6. Chessells JM, Breatnach F. Late marrow recurrences in childhood acute lymphoblastic leukaemia. Br Med J 1981;283:749-5 I. Rivera GK, Simone JV. Long term survivors in ‘total therapy’ studies of childhood acute lymphocytic leukemia (ALL). Proc Am SOC Clin Oncol 1985;4:161(abstr).
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
Aur RJA, Simone JV, Hustu HO, Verzosa MS, Pinkel D. Cessation of therapy during complete remission of child- hood acute leukemia. N Engl J Med 1974;291:1230-4. Gustafsson G, Kreuger A. Prognosis after relapse in acute lymphoblastic leukemia in childhood. Pediatr Hematol On- col 1986;3:119-26. Gustafsson G, Garwicz S, Hertz H, et al. Childhood acute lymphoblastic leukemia in the Nordic countries: a survey of children diagnosed July 1981 to July 1985. Acta Pae- diatr Scand 1987;76:781-8. Editorial. Experiences with the Scandinavian recommend- ed methods for determinations of enzymes in blood. Scand J Clin Lab Invest 1981;41:107-16. Rautonen J, Hovi L, Siimes MA. Slow disappearance of peripheral blast cells: an independent risk factor indicating poor prognosis in children with acute lymphoblastic leuke- mia. Blood 1988;71:989-91. Dixon WJ, ed. BMDP statistical software (1983 revised printing). Los Angeles, California: University of Califor- nia Press, 1983. George SL, Fernbach DJ, Vietti TJ, et al. Factors influen- cing survival in pediatric acute lekemia. Cancer 1980;46:241-52. Neglia JP, Day DL, Swanson TV, Ramsay NKC, Robison LL, Nesbit ME. Kidney size at diagnosis of childhood acute lymphocytic leukemia: lack of prognostic signifi- cance for outcome. Am J Pediatr Hematol Oncol 1988; 10:296-300. Rautonen J, Siimes MA. Elevated serum transaminase activity at diagnosis is associated with rapidly progressing disease in children with acute lymphoblastic leukemia. Cancer 1988;61:754-7. Rautonen J. Elevated cerebrospinal fluid leukocyte count and protein concentration at diagnosis: independent risk factors in children with acute lymphoblastic leukemia. Blut 1988;56:265-8. Miller DR, Leikin S, Albo V, et al. Use of prognostic factors in improving the design and efficiency of clinical trials in childhood leukemia. Cancer Treat Rep 1980;64:381-92. Miller DR, Leikin S, Albo V, Sather H, Karon M, Ham- mond D. Prognostic factors and therapy in acute lympho- blastic leukemia of childhood: CCG-141. Cancer 1983;51:1041-9.
Correspondence to: Jukka Rautonen, MD Children’s Hospital, University of Helsinki Stenbackinkatu 11 SF-00290 Helsinki Finland