Embed Size (px)
Citation preview

CAMPUS CLL
Chronic Lymphocytic LeukemiaRoma, 7-8 Maggio 2018
MALATTIA MINIMA RESIDUA IMMUNOFENOTIPICA
Anna Guarini
Università «Sapienza», Roma

Chronic Lymphocytic Leukemiaand
Minimal Residual Disease
1 July 2016
The European Medicine Agency (EMA) approved the use of undectectable MRD in CLL patients as an intermediate endpoint for licensure in well controlled randomized phase 3 clinical trials

Chronic Lymphocytic Leukemiaand
Minimal Residual Disease
Eliminating minimal residual disease as a therapeutic endpoint: working toward cure for patients with CLL
Philip A. Thompson and William G. Wierda
Blood 2016 127:279-286

MRD negative remission=defined as PB or BM with <1 cell/10,000 leukocytes. PB can generally be used for making this assessment; however, for treatments that preferentially clear the blood (for example MoAbs) it is important to confirm the BM is also MRD negative.
Thompson & Wierda, Blood 2016
Hallek M, iwCLL 2017Hallek M, et al. Blood 2018
Undetectable MRD in CLL patients in clinical CR (= MRD response rate) after induction therapy may be used as an intermediate endpoint for licensure in randomised well controlled studies designed to show superiority in terms of PFS [EMA, European Medicines Agency, dec 2015].
MRD eradication in CLL is possible
Still investigational, but…

Thompson M et al. Minimal Residual Disease in Chronic Lymphocytic Leukemia in the Era
of Novel Agents. A Review. JAMA Oncol. 2018
MRD Diagnostic
Tools:
Advantages and
Disadvantages

Flow cytometry (FC) MRD assay in CLL
✓ ERIC (European Research Initiative on CLL): standardized and reproducible 4-color FC, 4 tubes
✓ Sensitivity: 0.01% or 10-4 mononuclear cells (at least 500,000 events)
✓ Results as % of CLL cells on nucleated cellsMRD pos: at least 20 CLL cells/tube in at least 2 tubes
✓ 6-color: CD3/CD38/CD5/CD19/CD79b/CD20; CD81/CD22/CD5/CD19/CD43/CD20
✓8-color FC, 10-color FC (CD160, CD200): 1 tube
Rawstron A et al. Leukemia 2007Rawstron A et al. Leukemia 2013 & 2016Farren TW et al. Blood Cancer Journal 2015

Minimal residual disease monitoring in chroniclymphocytic leukaemia patients. A comparative analysis of flow cytometry and ASO IgH RQ-PCR
Raponi S et al, Br J Haematol 2014
1) Basic 4-color analysis: CD20/CD5/CD3/CD19; CD20/CD38/CD19/CD5
kappa/lambda/CD19/CD5
2) ERIC consensus panel: CD20/CD3/CD19/CD5; CD20/CD38/CD19/CD5
CD43/CD79b/CD19/CD5; CD81/CD22/CD19/CD5
CD45/CD14/CD19/CD5
3) 8-color analysis: CD81/CD38/CD20/CD43/CD5/CD45/CD19/CD3

Comparison of the three flow cytometric minimal residual disease methods in 10 samples from five patients with chronic lymphocytic leukaemia.
(ERIC, European Research Initiative in chronic lymphocytic leukaemia)Raponi et al, Br J Haemato 2014
Basic 4-color analysis
ERIC consensus analysis
8-color analysis

PFS of 87 CLL patients grouped by flow minimal residual disease (MRD) levels assessed (A) in the peripheral blood (PB) and (B) in
the bone marrow (BM) at the end of induction
(A) (B)
Raponi et al, Br J Haematol 2014

MRD+ (0.084%) of CLL patient (Pb)

MRD+ (1.59%) of CLL patient (BM)

Case 7: MRD- of CLL patient (Pb)

Raponi S, Della Starza I, De Propris MS, Del Giudice I, Mauro FR, Marinelli M, Di Maio V, Piciocchi A, Foà R, Guarini A. Minimal residual diseasemonitoring in chronic lymphocyticleukaemia patients. A comparative analysis of flow cytometry and ASO IgH RQ-PCR. Br J Haematol. 2014 166:360-8.
PFS of CLL patients stratified by minimal residual disease (MRD) assessed by both flow cytometry (FC) and PCR at the end of induction therapy (i.e. FC+ MRD versus FC-/PCR-MRD versus FC-/PCR+ MRD). (A) Peripheral Blood; (B) Bone Marrow
B
A

1 2 3 4 5
CGCAAGGGATGTTTATACTCATACA
CCCAGGAGGTGGAGCTGGATATTGA
GACTGCAAAATCTAATTGAAAATGA
TTCTGGGGTCTATTACTGTGCCACCT
GGGACTTACCCCATTAACGGGTTGG
TTCAAGATATTTGCTGAAGGGACTA
AGCTCATAGTAACTTCACCTGGTAA
GTAACTTTTCTTTCTGTTTTT
FR1 FR2 FR4FR3CDR1 CDR2L CDR3
primer 5’ patientspecific
primer 3’ patientspecific
Consensus/ specific probe derived from FR3
QR
STRATEGIA TAQMAN
Methods: molecular analysis

FITC PE PerCP PECy7 APC APC-Cy7 V450 V500
Lambda Kappa CD20 CD5 CD19 CD3 CD38 CD45
FITC PE PerCP PECy7 APC APC-Cy7 V450 V500
CD81 CD5 CD20 CD19 CD43 CD45 CD3 HLA-DR

Esordio PZ WW

Esordio Pz WW PB
MMR Pz WW , PB : 0.02%

Esordio Pz WW PB
MMR Pz WW 0.2% PB

MMR Pz WW BM : 0.3%

Esordio Pz XX PB
MMR Pz XX PB : 0.01%

MMR PZ XX PB: 0.01%
Esordio Pz XX PB

Esordio Pz ZZ PB
MMR Pz ZZ SP: NEGATIVA.

Esordio Pz ZZ PB
MMR Pz ZZ SP: NEGATIVA
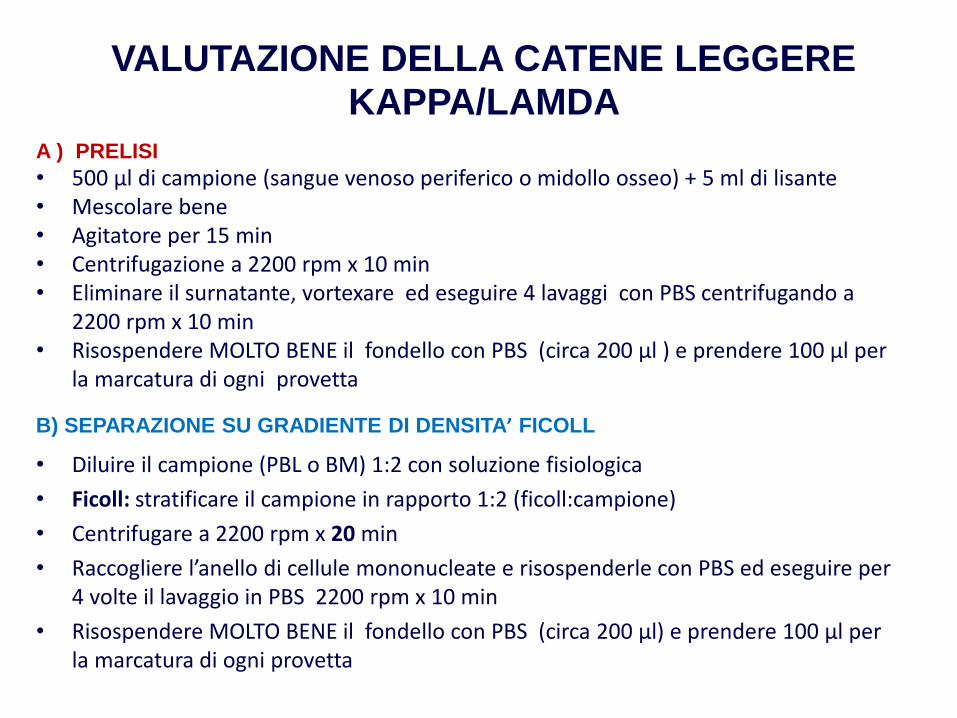
VALUTAZIONE DELLA CATENE LEGGERE KAPPA/LAMDA
A ) PRELISI
• 500 μl di campione (sangue venoso periferico o midollo osseo) + 5 ml di lisante • Mescolare bene • Agitatore per 15 min• Centrifugazione a 2200 rpm x 10 min• Eliminare il surnatante, vortexare ed eseguire 4 lavaggi con PBS centrifugando a
2200 rpm x 10 min• Risospendere MOLTO BENE il fondello con PBS (circa 200 μl ) e prendere 100 μl per
la marcatura di ogni provetta
B) SEPARAZIONE SU GRADIENTE DI DENSITA’ FICOLL
• Diluire il campione (PBL o BM) 1:2 con soluzione fisiologica
• Ficoll: stratificare il campione in rapporto 1:2 (ficoll:campione)
• Centrifugare a 2200 rpm x 20 min
• Raccogliere l’anello di cellule mononucleate e risospenderle con PBS ed eseguire per 4 volte il lavaggio in PBS 2200 rpm x 10 min
• Risospendere MOLTO BENE il fondello con PBS (circa 200 μl) e prendere 100 μl per la marcatura di ogni provetta

PFS by treatment and MRD response in the CLL8,
CLL10 and CLL11 trials
Natalie Dimier et al. Blood 2018;131:955-962
©2018 by American Society of Hematology

MRD in CLL Damier N et al, Blood 2018
• //CD5/CD19,
CD38/CD5/CD19/CD23,
CD81/CD22/CD19/CD5,
CD79b/CD20/CD19/CD5
OR
• //CD5/CD19,
CD38/CD5/CD19/CD23,
CD20/CD5/CD19/CD43,
CD20/CD79b/CD19/CD5

CONCLUSIONSThompson et al JAMA ONCOL.2018
“The use of MRD in CLL holds tremendous promise asa tool to estimate prognosis and influence decisionmaking during the course of treatment. However, there is no 1 MRD approach that is standardizedacross centers, and each method has uniqueadvantages and disadvantages to be considered. MRD as an endpoint must be validated prospectively priorto being used as a surrigate for survival, and given the heterogeneity of CLL biology and therapies, thisvalidation must be regimen specific in a sufficientlyrepresentative CLL population.”

MRD has a role.PROBLEMS:
▪ The method: FLOW OR RT-PCR or DD-PCR or CF-DNA?
▪ FLOW: how many events?
▪ When?
▪ Which compartment?

Morphology F Mancini, MG NardacciImmunophenotype,CD38, MS De Propris,
ZAP-70, CD49d ML Milani, S IntoppaFISH, Karyotype M Mancini, M NanniMRD – Flow Cytometry MS De Propris, ML Milani, S
IntoppaMRD – Molecular Biology I Della Starza, M Cavalli, L DenoviIgVH status C Ilari, L Cafforio S RaponiTP53 sequence and function S Raponi, C Ilari, N PeragineBTK pathway N Peragine, C PuzzoloGene profiling, SNIP, WES, S Chiaretti, I Del Giudice, SNGS, (TP53,NOTCH1, SF3B1, BIRC3, etc) Raponi, M Messina, L Cafforio,
C Ilari