Embed Size (px)
Citation preview

2015Vol.1 No.1:8
Review Article
iMedPub Journals
1© Under License of Creative Commons Attribution 3.0 License | This article is available in: http://cellular-molecular-medicine.imedpub.com/
www.imedpub.comCellular & Molecular Medicine: Open access
ISSN 2573-5365
DOI: 10.21767/2573-5365.100008
Calreticulin and JAK2V617F Mutations in Essential Thrombocythemia and Their
Potential Role in Diagnosis and Prognosis
Ahmad Ahmadzadeh1,Reza Shirzad1, Neda Golchin1, Saeid Shahrabi2, Mohammad Shahjahani1,Mohammad Seghatoleslami1 andNajmaldin Saki2
1 Healthresearchinstitute,Research Center of Thalassemia & Hemoglobinopathy,AhvazJundishapurUniversityofMedicalSciences,Ahvaz,Iran
2 Departmentofbiochemistryandhematology,Facultyofmedicine,SemnanUniversityofmedicalsciences,Semnan,Iran
Corresponding author: NajmaldinSaki
HealthResearchCenter,ResearchInstituteofThalassemia and Hemoglobinopathy, AhvazJundishapurUniversityofMedicalSciences,Ahvaz,Iran
Tel: +98.6113738317
Fax: +98.6113738330
Citation: AhmadzadehA,ShirzadR,GolchinN,etal.CalreticulinandJAK2V617FMutationsinEssentialThrombocythemiaandTheirPotentialRoleinDiagnosisandPrognosis.CellMolMed.2015,1:1.
IntroductionET was first recognized in 1934 by the name of hemorrhagicthrombocythemia. ET is characterized by an unusualthrombocytosis and risk of thrombotic and hemorrhagicdisorders.TheannualincidenceofETisapproximately1-2.5per100,000 population [1]. The incidence of ET is higher in those50-70yearsold,and ismostoften incidentallydetectedduringahighplateletcount.Anumberofpatientshavethromboticand
Abstract Introduction: Mutation in calreticulin (CALR) has been recently detected inessentialthrombocythemia(ET)patientslackingJAK2V617Fmutation.TheabsenceofJAK2V617Fmutationin50%ofpatientswithEThasindicatedtheimportanceofnewmarkersfordiseasediagnosis,includingCALR.ConsideringthedetectionofCALRinthesepatients,inthispaperwestudythestructureandfunctionofCALRproteinandJAK2V617FaswellastheirdiagnosticandprognosticroleinETpatients.
Methods: RelevantEnglish-languageliteratureweresearchedandretrievedfromPubMed (1995-2014) using the terms “Essential thrombocythemia, CalreticulinandJAK2”.
Discussion: CALRcanbindthrombospondinandvitaminK-dependentcoagulationfactors.ExperimentshaveshownthatCALRcanincreaseclottingtimeinpresenceofplatelets.Inaddition,CALRindirectlyleadstoactivationoftranscriptionfactorseffectiveuponcelldevelopment.ETpatientswithCALRmutationshowthromboticdisorders,lowerleukocytecountandhemoglobin,ahighplateletcountaswellaslongersurvivalandbetterprognosisthanpatientswithJAK2V617Fmutation.
Conclusion:EvaluationofCALRmutationinETpatientslackingJAK2V617Fmutationcancontributetodecisivediseasediagnosisandprognosis.Moreover,consideringtheimpactofCALRinincreasingtheclottingtimeaswellasotherfunctionsofit,includingcalciumbindingandproteinfolding,studiesonthisproteincanprovidesanoveltherapeuticapproachincontrolofET.
Keywords: Essentialthrombocythemia; Calreticulin; JAK2V617F
Abbreviations: MPNS: Myeloproliferative Neoplasms; ET: EssentialThrombocythemia; CALR: Calreticulin; JAK2: Janus kinase2; BM: BoneMarrow;TPO: Thrombopoietin; EPO: Erythropoietin; PMF: PrimaryMyelofibrosis; MRD:MinimalResidualDisease;MPL:MyeloproliferativeLeukemia
Received: September28,2015, Accepted: December11,2015, Published: December 16,2015
hemorrhagicdisordersandasmallnumberofthemshowdiseasetransformation towards myelofibrosis, myelodysplasia or AML[2]. ET patients rarely show two simultaneous mutations. Forexample,mutation inJAK2V617ForJAK2exon12rarelycoincideswith mutation in exon 10MPL gene in ET [3-6]. Hence, sincethe definite diagnosis of ET is not feasible in patientswithoutmutation in JAK2V617F, new biomarkers are required to identifysuch patients, including the newly discovered CALR protein.Remarkably,mutation inCALRhasbeendetected in29-80%of

2015Vol.1 No.1:8
Cellular & Molecular Medicine: Open access
2 This article is available in: http://cellular-molecular-medicine.imedpub.com/
Cellular & Molecular Medicine: Open access ISSN 2573-5365
ETpatients lackingmutation inJAK2V617F.Moreover,ETpatientswithmutationinCALRshowbetterprognosisthanpatientswithJAK2V617FmutationlackingCALRmutation[7-11].MutationinCALRand JAK2V617F simultaneously occur in approximately 80%of ETpatients.ETpatientslackingmutationinbothCALRandJAK2V617F canlackanymutationorshowmutationinTP53,DNMT3A,TET2,MPL, NFE2, CUX1 and del 7q [12]. As a result, CALRmutationassayinETpatients,especiallythoselackingmutationinJAK2V617F,canbehelpfulindiseaseprognosisanddiagnosis.GiventheroleandfunctionofCALRandJAK2V617FinETpatients,inthisreviewwehaveattemptedtostudythestructureandfunctionofCALRand JAK2V617F, theirmutation and interaction in ET in order tobetterunderstanddiseaseprognosisanddiagnosis. Inaddition,we have attempted to suggest novel CALR-based therapeuticstrategiesaccordingtodifferentfunctionsofCALRtohelpcontrolthediseaseinETpatients,whichrequiresfurtherinvestigations.
Materials and MethodsLiterature search and search strategy GiventherecentdiscoveryofCALRmutationinpatientswithETharboringJAK2V617mutation,PubmedandMedlinesearchenginesweresearchedfrom1995to2014andthepaperswereselectedwith respect to inclusion and exclusion criteria. The keywordsselected for search from MeSH database include Essentialthrombocythemia;JAK2V617Fandcalreticulin.ThediagnosisofETisbasedoncriteriareleasedin2001or2008byWHOandBritishCommitteeforStandardsinHematology(BCSH),respectively[13-15]. In themajorityof studies, ETpatientswere selected frominstitutional databases based on availability of archived bonemarroworperipheralbloodDNAformutationscreening,Sangersequencingorallele-specificPCR (AS-PCR) todetectmutations,includingCALRandJAK2V617F.
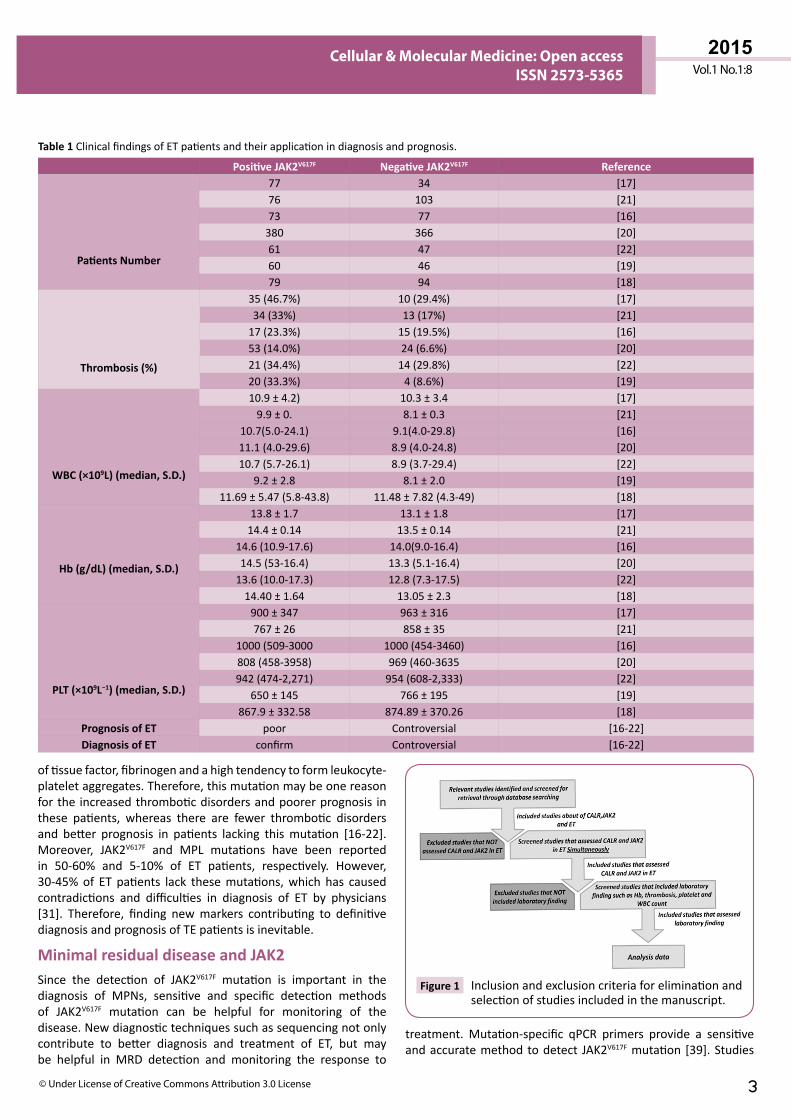
Inclusion criteriaAftersearchingthedatabases,studiesregardingJAK2V617F,CALRand ETwere collected. Then, since evaluation of simultaneousprevalence of JAK2V617F and CALRmutations in ET patientswasthe main inclusion criteria, the papers assessing both CALRand JAK2V617F mutations in ET patients entered into our study.Inaddition,studiesevaluatingthe incidenceof thrombosisandotherlaboratoryfindingssuchasHb,PltandWBCcountsaswellas detecting the above-mentioned mutations were included.Finally,thedatawerecollectedandanalyzed(Figure 1).
Exclusion criteriaStudies dealing with the prevalence of JAK2V617F and CALRmutations in MPNs other than ET were excluded. Afterwards,studies that only measured the prevalence of CALR but notJAK2V617Fandviceversawerealsoexcluded.Anumberofpapershad evaluated JAK2V617F and CALR mutations but no otherlaboratoryfindings likethrombosis,Hb,PltandWBCcountandwerealsoexcluded.
JAK2 as a main biomarker in ET diagnosis and prognosisET patients are divided to two groups: those bearing JAK2V617F
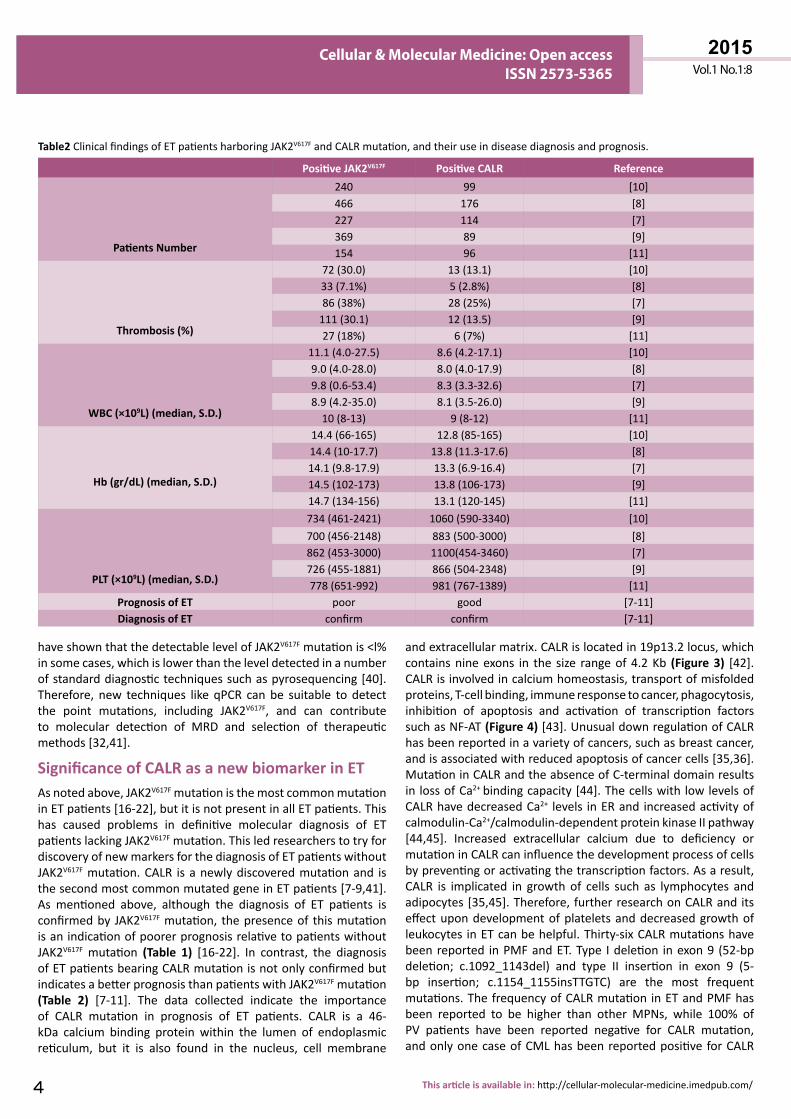
mutation and those lacking it [16-22]. Patients with JAK2V617F mutationcommonlyhavehemoglobinlevelslowerthan16g/dL,WBCcountlowerthan9.0×109/LandBMwithhighercellularity[7-11]. These values are different in ET patients bearing CALRmutation,and lowerHbandWBCvalueswithahigherplateletcount have been reported in them [7-11]. A higher risk ofthrombosis and vascular abnormalities has also been reportedinETpatientsbearingJAK2V617Fmutation[16-22].Therefore,thisgroup of ET patients shows a poorer prognosis than patientslackingthismutation(Tables 1 and 2).
JAK2V617F mutation in exon 14 of chromosome 9 is a commonmutationinidentificationofMPNs,includingET,whichplaysanimportantroleinsignalingofcytokines(includingTPO)affectinghematopoietic cells [23]. This pathway is involved in cellularmechanisms, including proliferation, survival, hematopoiesisand immune function [24]. Each JAK2V617F protein includes anactive tyrosine kinasedomainof JAK2V617F homology1 (JH1), aninactivecatalyticdomainof JH2,Srchomologydomain2 (SH2)anda4-point-1erzinradixinmoesin(FERM)domainintheamineterminal (Figure 2A) [23,24]. A point mutation in exon 14 ofJAK2V617Fgeneresults insubstitutionofcodon617(valine)withphenylalanine in the JH2 domain,which causes inactivation ofits inhibitory effecton JAK2V617F, throughwhich tyrosine kinaseactivity in JAK2V617F is induced in the absence of TPO and EPOligands. The expression of JAK2V617F mutation causes sustainedactivityof JAK2V617Fsignalingpathwayaswellasothersignalingpathways,resultinginincreasedsensitivityofmegakaryocyteandleukocyte precursors to growth factors, causing their cytokineindependent proliferation [25]. This mutation triggers thecytokine-independentactivationofJAK/STAT,PI3,AKTandMEK/ERKpathways(Figure 2B),allofwhichare involvedinsignalingof hematopoietic factors such as TPO, EPO and Granulocyte-Colony Stimulating Factor [26]. JAK2V617F signal transductionpathwayplaysanimportantroleincellsignaling,andmutationsin it canbeofclinical importance [27].Since JAK2V617Fpathwaycauses ineffectivehematopoiesis andmegakaryopoiesis aswellassplenomegaly inpatients,thepatientsbearingthismutationhave a higher incidence of thrombotic disorders with higherleukocytecountandhemoglobinconcentrationthaninpatientslackingmutation.JAK2V617FinhibitorslikeRuxolitinibareinvolvedin reducing ineffective hematopoiesis, megakaryopoiesis andsplenomegaly in ET patients [25]. Mutation in JAK2V617F is present in 80-90% of patients with Polycythemia Vera (PV),50-58%ofpatientswithET, 50-65%ofpatientswith idiopathicPMFand20%ofnon-classifiedMPNpatients [28-31]. It isalsoobserved inasmallgroupofmyelodysplasticsyndromes,acutemyelomonocytic leukemia, acute myeloid leukemia (AML),chronic myelogenous leukemia (CML) and other MPNs suchas Philadelphia negative myeloid leukemia [32]. AlthoughJAK2V617FmutationwasfirstreportedtobenegativeinCMLwithPhiladelphia positive chromosome, subsequent studies haveconfirmed the presence ofmutant JAK2V617F in CML [33-36]. Inpresenceofthismutation,overactiveJAK2V617Fcausesincreasedproductionofmegakaryocyte,erythroidandgranulocyticserieswith the expansion of erythron associated with splenomegaly[37,38].ETpatientsbearingJAK2V617Fmutationshowastrongerprothromboticstatusduetosignificantincreaseintheexpression
2015Vol.1 No.1:8
3© Under License of Creative Commons Attribution 3.0 License
Cellular & Molecular Medicine: Open access ISSN 2573-5365
oftissuefactor,fibrinogenandahightendencytoformleukocyte-plateletaggregates.Therefore,thismutationmaybeonereasonforthe increasedthromboticdisordersandpoorerprognosis inthese patients, whereas there are fewer thrombotic disordersand better prognosis in patients lacking thismutation [16-22].Moreover, JAK2V617F and MPL mutations have been reportedin 50-60% and 5-10% of ET patients, respectively. However,30-45%of ET patients lack thesemutations,which has causedcontradictions and difficulties in diagnosis of ET by physicians[31]. Therefore, finding newmarkers contributing to definitivediagnosisandprognosisofTEpatientsisinevitable.
Minimal residual disease and JAK2Since the detection of JAK2V617F mutation is important in thediagnosis of MPNs, sensitive and specific detection methodsof JAK2V617F mutation can be helpful for monitoring of thedisease.Newdiagnostictechniquessuchassequencingnotonlycontribute to better diagnosis and treatment of ET, but maybe helpful in MRD detection and monitoring the response to
treatment. Mutation-specific qPCR primers provide a sensitiveandaccuratemethodtodetect JAK2V617Fmutation[39].Studies
Positive JAK2V617F Negative JAK2V617F Reference
Patients Number
77 34 [17]76 103 [21]73 77 [16]380 366 [20]61 47 [22]60 46 [19]79 94 [18]
Thrombosis (%)
35(46.7%) 10(29.4%) [17]34(33%) 13(17%) [21]17(23.3%) 15(19.5%) [16]53(14.0%) 24(6.6%) [20]21(34.4%) 14(29.8%) [22]20(33.3%) 4(8.6%) [19]
WBC (×109L) (median, S.D.)
10.9±4.2) 10.3±3.4 [17]9.9±0. 8.1±0.3 [21]
10.7(5.0-24.1) 9.1(4.0-29.8) [16]11.1(4.0-29.6) 8.9(4.0-24.8) [20]10.7(5.7-26.1) 8.9(3.7-29.4) [22]
9.2±2.8 8.1±2.0 [19]11.69±5.47(5.8-43.8) 11.48±7.82(4.3-49) [18]
Hb (g/dL) (median, S.D.)
13.8±1.7 13.1±1.8 [17]14.4±0.14 13.5±0.14 [21]
14.6(10.9-17.6) 14.0(9.0-16.4) [16]14.5(53-16.4) 13.3(5.1-16.4) [20]13.6(10.0-17.3) 12.8(7.3-17.5) [22]14.40±1.64 13.05±2.3 [18]
PLT (×109L−1) (median, S.D.)
900±347 963±316 [17]767±26 858±35 [21]
1000(509-3000 1000(454-3460) [16]808(458-3958) 969(460-3635 [20]942(474-2,271) 954(608-2,333) [22]
650±145 766±195 [19]867.9±332.58 874.89±370.26 [18]
Prognosis of ET poor Controversial [16-22]Diagnosis of ET confirm Controversial [16-22]
Table 1ClinicalfindingsofETpatientsandtheirapplicationindiagnosisandprognosis.
Figure 1 Inclusionandexclusioncriteriaforeliminationandselectionofstudiesincludedinthemanuscript.
2015Vol.1 No.1:8
Cellular & Molecular Medicine: Open access
4 This article is available in: http://cellular-molecular-medicine.imedpub.com/
Cellular & Molecular Medicine: Open access ISSN 2573-5365
haveshownthatthedetectablelevelofJAK2V617Fmutationis<l%insomecases,whichislowerthantheleveldetectedinanumberofstandarddiagnostictechniquessuchaspyrosequencing[40].Therefore, new techniques like qPCR canbe suitable to detectthe point mutations, including JAK2V617F, and can contributeto molecular detection of MRD and selection of therapeuticmethods[32,41].
Significance of CALR as a new biomarker in ETAsnotedabove,JAK2V617FmutationisthemostcommonmutationinETpatients[16-22],butitisnotpresentinallETpatients.Thishas caused problems in definitive molecular diagnosis of ETpatientslackingJAK2V617Fmutation.ThisledresearcherstotryfordiscoveryofnewmarkersforthediagnosisofETpatientswithoutJAK2V617Fmutation.CALR isanewlydiscoveredmutationand isthesecondmostcommonmutatedgeneinETpatients[7-9,41].As mentioned above, although the diagnosis of ET patients isconfirmedby JAK2V617Fmutation, thepresenceof thismutationisanindicationofpoorerprognosisrelativetopatientswithoutJAK2V617F mutation (Table 1) [16-22]. In contrast, the diagnosisofETpatientsbearingCALRmutationisnotonlyconfirmedbutindicatesabetterprognosisthanpatientswithJAK2V617Fmutation(Table 2) [7-11]. The data collected indicate the importanceof CALR mutation in prognosis of ET patients. CALR is a 46-kDa calcium binding protein within the lumen of endoplasmicreticulum, but it is also found in the nucleus, cell membrane
andextracellularmatrix.CALRislocatedin19p13.2 locus,whichcontainsnineexons in the size rangeof4.2Kb (Figure 3) [42].CALRisinvolvedincalciumhomeostasis,transportofmisfoldedproteins,T-cellbinding,immuneresponsetocancer,phagocytosis,inhibition of apoptosis and activation of transcription factorssuchasNF-AT(Figure 4) [43].UnusualdownregulationofCALRhasbeenreportedinavarietyofcancers,suchasbreastcancer,andisassociatedwithreducedapoptosisofcancercells[35,36].MutationinCALRandtheabsenceofC-terminaldomainresultsin loss of Ca2+ bindingcapacity[44].ThecellswithlowlevelsofCALRhavedecreasedCa2+ levels inERand increasedactivityofcalmodulin-Ca2+/calmodulin-dependentproteinkinaseIIpathway[44,45]. Increased extracellular calcium due to deficiency ormutationinCALRcaninfluencethedevelopmentprocessofcellsbypreventingoractivatingthetranscriptionfactors.Asaresult,CALR is implicated in growth of cells such as lymphocytes andadipocytes[35,45].Therefore,furtherresearchonCALRanditseffectupondevelopmentofplateletsanddecreasedgrowthofleukocytes inETcanbehelpful.Thirty-sixCALRmutationshavebeenreported inPMFandET.Type Ideletion inexon9 (52-bpdeletion; c.1092_1143del) and type II insertion in exon 9 (5-bp insertion; c.1154_1155insTTGTC) are the most frequentmutations.ThefrequencyofCALRmutationinETandPMFhasbeen reported to be higher than other MPNs, while 100% ofPV patients have been reported negative for CALR mutation,andonlyonecaseofCMLhasbeenreportedpositiveforCALR
Positive JAK2V617F Positive CALR Reference
Patients Number
240 99 [10]466 176 [8]227 114 [7]369 89 [9]154 96 [11]
Thrombosis (%)
72(30.0) 13(13.1) [10]33(7.1%) 5(2.8%) [8]86(38%) 28(25%) [7]111(30.1) 12(13.5) [9]27(18%) 6(7%) [11]
WBC (×109L) (median, S.D.)
11.1(4.0-27.5) 8.6(4.2-17.1) [10]9.0(4.0-28.0) 8.0(4.0-17.9) [8]9.8(0.6-53.4) 8.3(3.3-32.6) [7]8.9(4.2-35.0) 8.1(3.5-26.0) [9]10(8-13) 9(8-12) [11]
Hb (gr/dL) (median, S.D.)
14.4(66-165) 12.8(85-165) [10]14.4(10-17.7) 13.8(11.3-17.6) [8]14.1(9.8-17.9) 13.3(6.9-16.4) [7]14.5(102-173) 13.8(106-173) [9]14.7(134-156) 13.1(120-145) [11]
PLT (×109L) (median, S.D.)
734(461-2421) 1060(590-3340) [10]700(456-2148) 883(500-3000) [8]862(453-3000) 1100(454-3460) [7]726(455-1881) 866(504-2348) [9]778(651-992) 981(767-1389) [11]
Prognosis of ET poor good [7-11]Diagnosis of ET confirm confirm [7-11]
Table2ClinicalfindingsofETpatientsharboringJAK2V617FandCALRmutation,andtheiruseindiseasediagnosisandprognosis.

2015Vol.1 No.1:8
5© Under License of Creative Commons Attribution 3.0 License
Cellular & Molecular Medicine: Open access ISSN 2573-5365
mutation [31,41]. The frequency of CALRmutation in patientswithET(regardlessofpositiveornegativemutationofJAK2V617F)isestimated tobe15-30%.The frequencyofCALRmutation inpatients with ET is shown in Table 3 and Figure 5. Moreover,recent studies on 10 cases of familial MPN with a history ofmyeloproliferativediseaseshowedthat2outof10ETpatientshadamutationinCALR,whichindicatedthatthemutationisnot
ETpatients CALRmutation(%) References
745 176(24%) [8]
250 80(31.2%) [41]
62 18(34.4%) [41]69 17(25%) [12]436 99(22.7%) [10]402 114(28%) [7]576 89(15.5%) [9]311 78(25%) [31]289 96(33%) [11]
Table 3 FrequencyofCALRmutationinEntireETcohort.
restrictedtosporadicMPNsandcanalsooccurinfamilialcases[46].ComparingTables 1 and 2showsthatplateletcountishigherinETpatientswithCALRmutationthan thosebearing JAK2V617F mutation. WBC and hemoglobin levels as well as thrombosisoccurrencearehigher inETpatientsbearingJAK2V617Fmutationthan patients with CALR mutation (Figure 6). These resultsandmutation diagrams along with laboratory data of patientsfrom diagnosis through treatment can contribute to diagnosis,monitoringandprognosisofpatientsaswellasMRDdetection,offeringanovelmethodtohelppatients,whichrequiresfurtherinvestigations.
Coagulation disorders in ET and prognostic role of CALRMostETpatientsareasymptomaticandarefortuitouslydetectedduringCBC.AstrongassociationhasbeenfoundbetweenJAK2V617F
mutationandthromboticdisordersinET[21],whichareamongETmanifestations.Thenatureofarterialandvenousthrombosisisdifferentinthesepatients.Arterialthrombosismainlyincludesplatelets (whiteclot)butvenous thrombosismostly consistsoffibrinandredbloodcells(redclot);however,severalsimilaritiesbetween these two trends of thrombosis have been recentlynoted[47].Studieshaveshownthatleukocytecountisabetterindex for predicting thrombosis comparedwith platelet count,RBC and hematocrit [48]. In these patients, prothromboticcirculatingendothelialcellshavebeenreported,themajorityofwhichbeartheJAK2V617Fmutation[49].Cardiovasculardisordersand thrombosis are more frequent in patients with mutantJAK2V617F compared to patients without the mutation [50,51].Other symptoms of ET patients include deep vein thrombosisand pulmonary embolism [52-54]. ET patients bearing CALRmutationshowlowerhemoglobinandWBCthanETpatientswithJAK2V617Fmutation,whereastheplateletcounthasbeenreportedtobehigher inETpatientswithCALRmutation comparedwiththosewith JAK2V617Fmutation (Figure 7). Studies indicated that
Figure 2 A) Location of JAK2V617F mutation and other exon 14mutations(fromSH2domain)inJAK2.Januskinase(JAK2)mutationscouldexistaspointmutations,duplicationsandinsertions in essential thrombocythemia (ET) and otherMPNs. Location of these mutations is the regulatory Nterminal of pseudokinase, namely SH2 (Src-homologydomain).JAK2V617Fmutationisthemostfrequentmutationinthesepatients.B)SchematicfigureofJAK2V617Fmutationand TPO signaling. JAK2V617F mutation activates thetranscriptionfactorsinvolvedinmyeloidandmegakaryocyticproliferation,andcanbeassumedastheoriginalcauseofMPNSsuchasET.ActivatedJAK2 kinasephosphorylatesthetyrosineofSTAT,whichisdimerizedandentersthenucleus,bindingtheregulatorysequenceoftargetgenetoregulateitstranscriptionandincreasetheproliferationofmyeloidandmegakaryocyticprogenitors.Ontheotherhand,JAK2
phosphorylatesRas/MEK/ERKmoleculesthatresultincellproliferation. Therefore, JAK2V617Fmutation by STAT, Ras/MEK/ERKandPI3K/AktpathwaysresultsinproliferationofmyeloidandmegakaryocyticprogenitorsintheabsenceofTPO.JAK2inhibitors(e.g.Ruxolitinib)inhibitbothmutatedandnon-mutatedJAK2anddonotdiscriminatebetweenthem.
Figure 3 StructureofCalreticulin.CALRhas threedomainswithstructuralandfunctionalviability.Nterminaldomaininred(containingNdomainandsignalsequenceshowninblack),Pdomain(blue),Cdomain(green)arethethreedomainofCALR.CdomainisabindingsiteforCa2+andcontains KDEL signal. P and N domains are chaperondomains of CALR. N domain contains three cysteineresidues.Thunderboltyellowarrowshowsglycosylationsites in N and C domain (residues 162 and 327,respectively).RepetitivesequenceinPdomaincontainsPXXIXDPDAXKPEDWDE(orangelozengeandlettera)andGXWXPPXIXNPXYX (orange square and letter b) aminoacids.

2015Vol.1 No.1:8
Cellular & Molecular Medicine: Open access
6 This article is available in: http://cellular-molecular-medicine.imedpub.com/
Cellular & Molecular Medicine: Open access ISSN 2573-5365
Figure 4 Schematic figure of CALR functions CALR is involved inprocessingofERproteinsandpeptidesinvolvedinantigenpresentation and processing. However, other moleculesuch as calnexin, Transporter associated with antigenprocessing(TAP),tapasinandβ2macroglobulinplayarolein thisprocess.Binding toCa2+ in ER is another functionofCALRbutmutatedCALR losesthiscapacity; therefore,Ca2+ release in ER by sarco/endoplasmic reticulum Ca2+ ATPase(SERCA)channel isprevented,andfreeCa2+ inERentersintocytoplasmthrough1,4,5-triphosphatereceptor(InsP3R) channel. Increased Ca2+ activates calcineurin,which dephosphorylates nuclear factor of activatedt-cells (NF-AT), resulting in the transcription of targetgeneinDNA.IfCALRtranslocatesoutsidethecell,itmayhavea role inwoundhealing.CALRcouldact likea trapfor opsonins like C1q that is a site for antibody bindingrecognizedbyFCRonphagocyticcellsurface.Ontheotherhand,CALRandCD91/LRPhaveahomologytobindC1q.CALRactslikealigandtobindCD91/LRPonmacrophagesto help in phagocytosis of the apoptotic cell. CALR canbindendothelialcells,Thrombospondin(TSP)andvitaminK-dependentcoagulationfactorsbutdoesnotchangetheircoagulantpropertiesandprolongsthebloodclottingtime.
GraphofCALRmutationfrequencyinET.Figure 5
Figure 6 Graphof laboratoryfindings in JAK2positive/negativeandCALRpositivemutationinET.Theleftgraphsshowthe TBR, Hb, Plt and WBC in JAK2 positive/negativecases.RightgraphsshowtheTBR,Hb,PltandWBC inCALR positive/negative cases. These data could helpin diagnosis, prognosis and determination of MRDin ET in correlation with qPCR data from diagnosisto CR. Abbreviations: Minimal residual disease(MRD), Complete remission (CR), Thrombosis (TBR),Hemoglobin(Hb),Platelet(Plt),Whitebloodcell(WBC).Quantitativepolymerasechainreaction(qPCR).
ET patientswith CALRmutation have a better thrombosis-freesurvivalthanpatientswith JAK2V617Fmutation[55].Forexample,among 300Mayo Clinic ET patients, incidence of JAK2V617F andCALR mutations was reported 53% and 32%, respectively. Inthis study, ET patients with CALR mutation displayed betterthrombosis-free survival compared to patients with JAK2V617F
mutation[55].Thereductioninthromboembolicdisordersmaybe due to decreased hemoglobin concentration and leukocytecount inETpatientswithCALRmutationcomparedwith those
bearing JAK2V617Fmutation[31,56,57].CALRhasbeenrecognizedasacalcium-bindingproteinsinceadecadeago.CALRbindsthe

2015Vol.1 No.1:8
7© Under License of Creative Commons Attribution 3.0 License
Cellular & Molecular Medicine: Open access ISSN 2573-5365
Figure 7 Schematic ET death risk scale. As shown in the Figure,in ET patientswith JAK2mutation,WBC count, Hb andthrombosisrisk(TBR)ishigherandplateletratioislowerthan the ET patients with CALR mutation but withoutJAK2 mutation. Patients with CALR mutation have abetterprognosisandlowerdeathriskthanpatientswithJAK2mutation.Inotherwords,inthepatientswithJAK2mutation,theriskofdeathishighandprognosisispoor,unlikeETpatientswithCALRmutation.
Figure 8 Diagnosis and prognosis algorithm of ET with JAK2negative mutation by CALR. Distinction between MPNandCMLispossiblethroughtheexistenceofPhiladelphia(Ph) chromosome, which is the hallmark of CML. If Phchromosomeisabsent,JAK2mutationshouldbeassessedin these patients. JAK2 mutation is present in most PhnegativeMPNdiseasessuchasET,Primarymyelofibrosis(PMF)andPV.Inrecentstudies,CALRmutationhasbeenassessedinPhandJAK2 negativecasesofMPNdisorders.CALRmutationiscompletelynegativeand60-80%positiveinPhandJAK2negativePVandETpatients,respectively,andcouldbehelpfulfordiagnosisofthesepatients.
endothelialcellsandvitaminKdependentcoagulationfactors(IX,X,VIIand II)butcausesnochange in theircoagulationactivity(Figure 4).Moreover,CALRcaninteractwithfactorVIII andthis interactionappearstoberequiredforfactorVIIIsecretion[58]. In animalmodelsofthrombosisinducedbyelectricity,KuwabaraetalfoundthatintravascularinjectionofCALRhelpspreventbloodvesselocclusion[59].Furthermore,CALRpromotesangiogenesisvia activating nitric oxide signaling pathway [60]. This activityis relatedtoC-terminaldomainofCALR,which isalso found inplateletsandmaybeassociatedwithintegrins[59].ThestudyofCALRasananti-coagulanthasshownthathumanandrabbitCALRdramatically prolong the whole blood clotting time. A similarincreasewasobservedinclottingtimeofplatelet-richplasmabutplatelet poor plasma showed no difference in clotting timeupto300seconds inthepresenceorabsenceofCALR.Therefore,CALRislikelytohaveanti-coagulationeffectinassociationwithplatelet glycoproteins [59,61]. CALR acts as an anti-thromboticagent [62,63].AsCALRcanincreasetheclottingtime,mutationinitcausesabetterprognosisinpatients.Therefore,thepossibilityofahigher tendencyof thismolecule forvitaminKdependentcoagulation factors and the resulting reduction in thromboticdisorders in ET patients could be one reason for the betterprognosisinpatientswiththismutation,whichrequiresfurtherinvestigations. Several drugs like aspirin, hydroxyurea (HU),
AnagrelideandJAK2inhibitorsareusedtotreatandcontrolET.Aspirindecreasesbothvenousandarterial thrombosis [64,65].Studies have shown that in patients with JAK2V617F mutationwithriskfactors(high-riskET),prescriptionofaspirincanaffectthe incidence of venous thrombosis [66,67]. Studies haveindicated that aspirin use prevents venous thrombosis in low-riskETpatientsbearing JAK2V617Fmutation[66].However, inETpatientslackingJAK2V617Fmutationandbearing JAK2V617Fmutationwithoutriskfactors(low-riskET),cardiovascularriskfactorsandthromboticdisorderscanbereducedbyaspirinprescription [66].HU halts DNA synthesis and decreases the platelet productionandthrombosisinhigh-riskETpatients[68].Anagrelidetherapyinthesepatientscausesdecreasedproductionofplatelets[33,69].JAK2V617F inhibitors suchas INC18424 (Ruxolitinib) suppress thesignalinducedby JAK2V617Fanddecreasetheplateletcount[70]. Thecombinationofoldtechniqueswithnewmethodscanhelpimprove the ET patients. The study of new molecules, theirfunctionandinactivationcanpresentnoveltreatmentapproachesforcontrolofET.Hence,accordingtotheanti-coagulanteffects

2015Vol.1 No.1:8
Cellular & Molecular Medicine: Open access
8 This article is available in: http://cellular-molecular-medicine.imedpub.com/
Cellular & Molecular Medicine: Open access ISSN 2573-5365
ofCALR,furtherstudiesonthismoleculeandunderstandingitsmodeofactioncanbeafuturetreatmentapproachforET.
Simultaneous assessment of CALR and JAK2 in ET diagnosis and prognosisETpatientsaregroupedbasedonriskfactors,andprevioushistoryofthrombosisandageover60yearsarethemostimportantriskfactors. Increased leukocyte count at diagnosis is a predictivefactor for thrombosis in ET and PV patients. ET patients with JAK2V617F mutationshowahigherincidenceofvenousandarterialthrombosis compared with patients without this mutation,and this is also true in somepatientswithMPLmutation [51].IncreasedBMreticulinfibrosisisapredictivefactorforthromboticandhemorrhagicdisorders[33].ThestudyofBMandperipheralblood,applicationofWHOandBCSHcriteriaaswellas JAK2V617F andMPLmutationsarediagnosticapproachesforET.Hence,thediscoveryofnewmarkerscanhelpdiagnosethesepatients.Sincenot allMPN patients bear the JAK2V617Fmutation, detection ofnewmutationswithahigherfrequency(includingCALR)canbehelpfultobetteridentifythesepatients.Aspreviouslymentioned(Figure 7),patientsbearingCALRmutationsshowbettersurvivalandprognosisthanETpatientslackingthismutation[55],whichcan help in the treatment and monitoring of these patients(Figure 8).
Conclusion and future perspectiveGiven that the classification of hematopoietic and lymphatictumors is undergoing developments by WHO revision, newfindings and mutations like CALR and their interaction withother mutations such as JAK2V617F can help in classification,diagnosis, treatmentmonitoring and choice of clinical ET testsin otherMPNs such as IMP and PV. CALRhas been implicatedincoagulationthroughbindingplateletsandtheirglycoproteinsaswellasvitaminKdependentcoagulationfactors.ETpatientswithincreasedplateletcountandmutationinCALRshowbetterprognosis and survival with a lower frequency of thromboticdisordersrelativetothoselackingthismutation,whichisanother
indication of the association between CALR and coagulation.Therefore,sinceCALRbindstovitaminKdependentcoagulationfactorsandincreasesthewholeclottingtime[59,61],wesuggestthe treatment or alleviation of symptoms in patients withthrombotic disorders via inhibition of CALR. Furthermore, theuseofantibodiesagainstCALRmaybehelpful forhemorrhagiccomplications in other disorders due to the role of CALR inincreasingtheclottingtime.MutatedCALRcanindirectlyactivatecalcineurin via increased calcium levels. Mutated CALR has alowercapacityofCa2+ binding,thusCa2+ enters the cytoplasm from ER.Thiscausescalcineurinactivation,whichcausestranscriptionof NF-AT and affects the development process of the cells[36,43,44]. Considering lowWBC count in ET patients bearingCALRmutationbuthighcountsinthosewithJAK2V617Fmutation,CALRmaybeimplicatedindevelopment,growthandapoptosisof lymphocytes, adipocytes and cancer cells. Further studiesontheroleofCALRinthedevelopmentprocessofWBCcanbehelpfulinbetterrecognitionofETanditstreatment.CombinednewandoldtreatmentsaswellasJAK2V617Finhibitors,monitoringandcomparisonwithCALRand its inhibitorscanpresentnovelmethodsfortreatmentofthesepatients.Detectionoflowlevelsofmutated JAK2V617F using sensitive and specificmethods (e.g.qPCR), laboratoryfindingsof ETpatients and their comparisoncancontributetoMRDdetectionanddiseasemonitoringduringtherapy.
AuthorshipAllauthorsdraftedandapprovedthismanuscript.
AcknowledgmentsThisworkwasfinanciallysupportedbygrant:Th94/3fromvice-chancellorforResearchAffairsofAhvazJundishapurUniversityofSciences.ThisstudyispartofMScthesisforRezaShirzad.
Conflict of InterestTheauthorsdeclarenoconflictofinterest.

2015Vol.1 No.1:8
9© Under License of Creative Commons Attribution 3.0 License
Cellular & Molecular Medicine: Open access ISSN 2573-5365
References1 Campo E, Swerdlow SH, Harris NL, Pileri S, Stein H et al. (2011)
The2008WHOclassificationof lymphoid neoplasms andbeyond:evolvingconceptsandpracticalapplications.Blood117:5019-5032.
2 Vardiman JW,Thiele J,ArberDA,BrunningRD,BorowitzMJ,etal.(2009)The2008revisionof theWorldHealthOrganization(WHO)classification ofmyeloid neoplasms and acute leukemia: rationaleandimportantchanges.Blood114:937-951.
3 BoydEM,BenchAJ,Goday-FernandezA,AnandS,VaghelaKJ,etal.(2010)ClinicalutilityofroutineMPLexon10analysisinthediagnosisof essential thrombocythaemia and primary myelofibrosis. Britishjournalofhaematology149:250-257.
4 Dos Santos MT, Mitne-Neto M, Miyashiro K, Chauffaille Mde L,Rizzatti EG (2014)Molecular genetic tests for JAK2V617F, Exon12_JAK2andMPLW515K/Larehighly informative in theevaluationofpatients suspected to have BCR-ABL1-negative myeloproliferativeneoplasms.Journalofclinicalpathology67:176-178.
5 Kim HJ, Jang JH, Yoo EH, Kim HJ, Ki CS, et al. (2010) JAK2 V617Fand MPL W515L/K mutations in Korean patients with essentialthrombocythemia. The Korean journal of laboratorymedicine 30:474-476.
6 ZhangSJ,QiuHX,LiJY,ShiJY,XuW(2010)TheanalysisofJAK2andMPLmutationsandJAK2singlenucleotidepolymorphisms inMPNpatients by MassARRAY assay. International journal of laboratoryhematology32:381-386.
7 TefferiA,WassieEA,GuglielmelliP,GangatN,BelachewAA,etal.(2014) Type 1 versus Type 2 calreticulin mutations in essentialthrombocythemia:acollaborativestudyof1027patients.Americanjournalofhematology89:E121-4.
8 Rumi E, Pietra D, Ferretti V, Klampfl T, Harutyunyan AS, et al.(2014) JAK2orCALRmutationstatusdefinessubtypesofessentialthrombocythemia with substantially different clinical course andoutcomes.Blood123:1544-1551.
9 RotunnoG,MannarelliC,GuglielmelliP,PacilliA,PancrazziA,etal.(2014)Impactofcalreticulinmutationsonclinicalandhematologicalphenotypeandoutcomeinessentialthrombocythemia.Blood123:1552-1555.
10 FuR,XuanM,ZhouY,SunT,BaiJ,etal.(2014)Analysisofcalreticulinmutations in Chinese patients with essential thrombocythemia:clinicalimplicationsindiagnosis,prognosisandtreatment.Leukemia28:1912-1914.
11 AndrikovicsH, Krahling T, Balassa K,HalmG, BorsA, et al. (2014)Distinctclinicalcharacteristicsofmyeloproliferativeneoplasmswithcalreticulinmutations.Haematologica99:1184-1190
12 LundbergP,KarowA,NienholdR,LooserR,Hao-ShenH,etal.(2014)Clonal evolution and clinical correlates of somatic mutations inmyeloproliferativeneoplasms.Blood123:2220-2228
13 Vardiman JW, Harris NL, Brunning RD (2002) The World HealthOrganization(WHO)classificationofthemyeloidneoplasms.Blood100:2292-302.
14 SabattiniE,BacciF,SagramosoC,PileriS(2008)WHOclassificationoftumoursofhaematopoieticandlymphoidtissuesin:anoverview.Pathologica102:83-87.
15 HarrisonCN,BarefordD,ButtN,CampbellP,ConneallyE,etal.(2010)Guidelineforinvestigationandmanagementofadultsandchildrenpresenting with a thrombocytosis. British journal of haematology149:352-375.
16 WolanskyjAP,LashoTL,SchwagerSM,McClureRF,WadleighM,etal.(2005)JAK2V617Fmutationinessentialthrombocythaemia:clinicalassociationsand long termprognostic relevance.British journalofhaematology131:208-213.
17 SpeletasM, Katodritou E,Daiou C,Mandala E, Papadakis E, et al.(2007) Correlations of JAK2-V617F mutation with clinical andlaboratory findings in patients with myeloproliferative disorders.LeukRes31:1053-1062.
18 PoopakB,HaghMF,SakiN,ElahiF,RezvaniH,etal.(2013)JAK2V617Fmutation in Iranian patients with myeloproliferative neoplasms:clinicalandlaboratoryfindings.TurkishJournalofMedicalSciences347-353.
19 PatriarcaA,PompettiF,MaliziaR,IulianiO,DiMarzioI,etal.(2010)IstheabsenceofJAK2mutationariskfactorforbleedinginessentialthrombocythemia? An analysis of 106 patients. Blood transfusionTrasfusionedelsangue8:21-27.
20 FuR,XuanM,LvC,ZhangL, LiH,etal. (2014)Externalvalidationand clinical evaluation of the International Prognostic Score ofThrombosisforEssentialThrombocythemia(IPSET-thrombosis)inalargecohortofChinesepatients.Europeanjournalofhaematology92:502-509.
21 Finazzi G, Rambaldi A, Guerini V, Carobbo A, Barbui T (2007) Riskof thrombosis in patients with essential thrombocythemia andpolycythemiaveraaccordingtoJAK2V617Fmutationstatus135-136.
22 ChoYU,ChiHS, LeeEH, Jang S, ParkCJ, et al. (2009)Comparisonof clinicopathologic findings according to JAK2 V617Fmutation inpatients with essential thrombocythemia. International journal ofhematology89:39-44.
23 McLornan D, PercyM,McMullinMF (2006) JAK2 V617F: a singlemutation in themyeloproliferative group of disorders. The Ulstermedicaljournal75:112-119.
24 Liu PC, Caulder E, Li J,Waeltz P,Margulis A, et al. (2009) Combinedinhibitionof Januskinase1/2 for the treatmentof JAK2V617F-drivenneoplasms: selective effects on mutant cells and improvements inmeasuresofdiseaseseverity.Clinicalcancerresearch:anofficialjournaloftheAmericanAssociationforCancerResearch15:6891-6900.
25 LiWX(2008)Canonicalandnon-canonicalJAK-STATsignaling.Trendsincellbiology18:545-551.
26 TaherA,ShammaaD,BazarbachiA,ItaniD,ZaatariG,etal.(2009)AbsenceofJAK2V617Fmutationinthalassemiaintermediapatients.Molecularbiologyreports36:1555-1557.
27 Zhao R, Xing S, Li Z, Fu X, Li Q, et al. (2005) Identification of anacquired JAK2 mutation in polycythemia vera. The Journal ofbiologicalchemistry280:22788-22792.
28 XiaJ,LuMZ,JiangYQ,YangGH,ZhuangY,etal.(2012)JAK2V617F,MPLW515Land JAK2Exon12Mutations inChinesePatientswithPrimaryMyelofibrosis.Chinese journalof cancer research Chung-kuoyenchengyenchiu24:72-76.
29 TefferiA, LashoTL,FinkeCM,KnudsonRA,KetterlingR,etal. (2014)CALRvsJAK2vsMPL-mutatedortriple-negativemyelofibrosis:clinical,cytogeneticandmolecularcomparisons.Leukemia28:1472-1477.
30 RumiE,PietraD,PascuttoC,GuglielmelliP,Martinez-TrillosA,etal.(2014)Clinicaleffectofdrivermutationsof JAK2,CALR,orMPL inprimarymyelofibrosis.Blood124:1062-1069.
31 KlampflT,GisslingerH,HarutyunyanAS,NivarthiH,RumiE, et al.(2013) Somatic mutations of calreticulin in myeloproliferativeneoplasms.TheNewEnglandjournalofmedicine369:2379-2390.

2015Vol.1 No.1:8
Cellular & Molecular Medicine: Open access
10 This article is available in: http://cellular-molecular-medicine.imedpub.com/
Cellular & Molecular Medicine: Open access ISSN 2573-5365
32 JovanovicJV,IveyA,VannucchiAM,LippertE,OppligerLeibundgutE,etal. (2013)Establishingoptimalquantitative-polymerasechainreactionassaysforroutinediagnosisandtrackingofminimalresidualdisease in JAK2-V617F-associated myeloproliferative neoplasms:a joint European LeukemiaNet/MPN&MPNr-EuroNet (COST actionBM0902)study.Leukemia27:2032-2039.
33 CampbellPJ,BarefordD,ErberWN,WilkinsBS,WrightP,etal.(2009)Reticulin accumulation in essential thrombocythemia: prognosticsignificanceand relationship to therapy. Journalof clinicaloncology :official journaloftheAmericanSocietyofClinicalOncology27:2991-2999.
34 GlynnRJ,DanielsonE, FonsecaFA,Genest J,GottoAM,etal. (2009)A randomized trial of rosuvastatin in the prevention of venousthromboembolism.TheNewEngland journalofmedicine360:1851-1861.
35 LeeD,OkaT,HunterB,RobinsonA,PappS,etal.(2013)Correction:CalreticulinInducesDilatedCardiomyopathy.PloSone.
36 WangW-A,GroenendykJ,MichalakM(2012)Calreticulinsignalinginhealthanddisease.The international journalofbiochemistry&cellbiology44:842-846.
37 Da Silva RR, Domingues Hatzlhofer BL,Machado CG, Lima AS, deAlbuquerqueDM,etal.(2012)JAK2V617FmutationprevalenceinmyeloproliferativeneoplasmsinPernambuco,Brazil.Genetictestingandmolecularbiomarkers16:802-805.
38 ReutherGW(2008)JAK2activationinmyeloproliferativeneoplasms:apotentialroleforheterodimericreceptors.Cellcycle7:714-719.
39 LippertE,GirodonF,HammondE,JelinekJ,ReadingNS,,etal(2009)ConcordanceofassaysdesignedforthequantificationofJAK2V617F:amulticenterstudy.Haematologica94:38-45.
40 BenchAJ,WhiteHE,ForoniL,GodfreyAL,GerrardG,etal. (2013)Molecular diagnosis of the myeloproliferative neoplasms: UKguidelines for the detection of JAK2 V617F and other relevantmutations.Britishjournalofhaematology160:25-34.
41 NangaliaJ,MassieCE,BaxterEJ,NiceFL,GundemG,etal.(2013)SomaticCALR mutations in myeloproliferative neoplasms with nonmutatedJAK2.TheNewEnglandjournalofmedicine369:2391-405.
42 NakamuraK,ZuppiniA,ArnaudeauS,LynchJ,AhsanI,etal.(2001)Functionalspecializationofcalreticulindomains.TheJournalofcellbiology154:961-972.
43 RaghavanM,WijeyesakereSJ,PetersLR,DelCidN(2013)Calreticulinintheimmunesystem:insandouts.Trendsinimmunology34:13-21.
44 BibiA,AgarwalNK,DihaziGH, EltoweissyM,VanNguyenP, et al.(2011) Calreticulin is crucial for calcium homeostasis mediatedadaptationandsurvivalofthickascendinglimbofHenle'sloopcellsunder osmotic stress. The international journal of biochemistry&cellbiology43:1187-1197.
45 Szabo E, Qiu Y, Baksh S, MichalakM, OpasM (2008) Calreticulininhibitscommitmenttoadipocytedifferentiation.TheJournalofcellbiology182:103-116.
46 MaffioliM,GenoniA,CaramazzaD,MoraB,BussiniA,etal.(2014)LookingforCALRmutationsinfamilialmyeloproliferativeneoplasms.Leukemia28:1357-1360.
47 Green D (2009) Risk of future arterial cardiovascular events inpatientswithidiopathicvenousthromboembolism.Hematology/theEducationProgramoftheAmericanSocietyofHematologyAmericanSocietyofHematologyEducationProgram259-266.
48 BarbuiT,CarobbioA,RambaldiA,FinazziG(2009)Perspectivesonthrombosisinessentialthrombocythemiaandpolycythemiavera:isleukocytosisacausativefactor?Blood114:759-763.
49 SozerS,FielMI,SchianoT,XuM,MascarenhasJ,etal.(2009)Thepresence of JAK2V617F mutation in the liver endothelial cells ofpatientswithBudd-Chiarisyndrome.Blood113:5246-5249.
50 AntonioliE,GuglielmelliP,PoliG,BoganiC,PancrazziA,etal.(2008)Influence of JAK2V617F allele burden on phenotype in essentialthrombocythemia.Haematologica93:41-48.
51 VannucchiAM,AntonioliE,GuglielmelliP,PancrazziA,GueriniV,etal. (2008)CharacteristicsandclinicalcorrelatesofMPL515W>L/Kmutationinessentialthrombocythemia.Blood112:844-847.
52 ReginaS,HeraultO,D'AlterocheL,BinetC,GruelY(2007)JAK2V617Fisspecificallyassociatedwithidiopathicsplanchnicveinthrombosis.JTH5:859-861.
53 RossiD,CrestaS,DestroT,VendraminC,BocchettaS,etal. (2007)JAK2V617Finidiopathicvenousthromboembolismoccurringintheabsence of inherited or acquired thrombophilia. British journal ofhaematology138:813-814.
54 Vannucchi AM, Antonioli E, Guglielmelli P, Rambaldi A, Barosi G,etal. (2007)Clinicalprofileofhomozygous JAK2617V>Fmutationin patientswith polycythemia vera or essential thrombocythemia.Blood110:840-846.
55 GangatN,WassieEA,LashoTL,FinkeC,KetterlingRP,etal.(2014)Mutationsandthrombosisinessentialthrombocythemia:prognosticinteraction with age and thrombosis history. European journal ofhaematology94:34-36.
56 CampbellPJ,GriesshammerM,DohnerK,DohnerH,KusecR,etal.(2006)V617FmutationinJAK2isassociatedwithpoorersurvivalinidiopathicmyelofibrosis.Blood107:2098-2100.
57 Rumi E, PietraD, Guglielmelli P, Bordoni R, Casetti I, et al. (2013)Acquiredcopy-neutral lossofheterozygosityofchromosome1pasamoleculareventassociatedwithmarrowfibrosisinMPL-mutatedmyeloproliferativeneoplasms.Blood121:4388-4395.
58 KaufmanRJ,PipeSW,TagliavaccaL,SwaroopM,MoussalliM(1997)Biosynthesis,assemblyandsecretionofcoagulationfactorVIII.Bloodcoagulation&fibrinolysis :an international journal inhaemostasisandthrombosis2:S3-14.
59 Kuwabara K, Pinsky DJ, Schmidt AM, Benedict C, Brett J, et al.(1995)Calreticulin,anantithromboticagentwhichbindstovitaminK-dependentcoagulationfactors,stimulatesendothelialnitricoxideproduction,and limits thrombosis incaninecoronaryarteries.TheJournalofbiologicalchemistry270:8179-8187.
60 DingH,HongC,WangY,LiuJ,ZhangN,ShenC,etal.(2014)Calreticulinpromotesangiogenesisviaactivatingnitricoxidesignallingpathwayinrheumatoidarthritis.Clinicalandexperimentalimmunology178:236-244.
61 Dai E, Stewart M, Ritchie B, Mesaeli N, Raha S, et al. (1997)Calreticulin,apotentialvascularregulatoryprotein,reducesintimalhyperplasia after arterial injury. Arteriosclerosis, thrombosis, andvascularbiology17:2359-2368.
62 PinskyDJ,KuwabaraK,SchmidtAM,LawsonCA,BenedictC,etal.(1996)CalreticulinandThrombosis.Calreticulin:Springer155-168.
63 SternDM,KuwabaraK,BenedictC,RyanJ(1995)Calreticulin:anovelantithromboticagent.GooglePatents.
64 Griesshammer M, Bangerter M, van Vliet HH, Michiels JJ (1997)Aspirin in essential thrombocythemia: status quo and quo vadis.Seminarsinthrombosisandhemostasis23:371-377.

2015Vol.1 No.1:8
11© Under License of Creative Commons Attribution 3.0 License
Cellular & Molecular Medicine: Open access ISSN 2573-5365
65 LandolfiR,MarchioliR,KuttiJ,GisslingerH,TognoniG,etal.(2004)EfficacyandSafetyofLow-DoseAspirininPolycythemiaVera.NewEnglandJournalofMedicine350:114-124.
66 Alvarez-Larran A, Cervantes F, Pereira A, Arellano-Rodrigo E,Perez-Andreu V, et al. (2010 ) Observation versus antiplatelettherapyasprimaryprophylaxisforthrombosis in low-riskessentialthrombocythemia.Blood116:1205-1210.
67 ReikvamH,TiuRV(2012)Venousthromboembolisminpatientswithessential thrombocythemia and polycythemia vera. Leukemia 26:563-571.
68 Cortelazzo S, FinazziG, RuggeriM, VestriO,GalliM, et al. (1995)Hydroxyureaforpatientswithessentialthrombocythemiaandahighriskofthrombosis.TheNewEnglandjournalofmedicine332:1132-1136.
69 HarrisonCN,CampbellPJ,BuckG,WheatleyK,EastCL,etal.(2005)Hydroxyurea compared with anagrelide in high-risk essentialthrombocythemia.TheNewEnglandjournalofmedicine353:33-45.
70 Baskin R, Majumder A, Sayeski PP (2010) The recent medicinalchemistry development of Jak2 tyrosine kinase small moleculeinhibitors.Currentmedicinalchemistry17:4551-4558.





























