Embed Size (px)
Citation preview

Slide 1
Calcaneus FracturesCalcaneus Fractures
Anthony J Longo M.D.Anthony J Longo M.D.University of Texas Medical BranchUniversity of Texas Medical Branch

Slide 2
IntroductionIntroduction
Most frequently fractured tarsal boneMost frequently fractured tarsal boneSixty % of all tarsal fractures and 1Sixty % of all tarsal fractures and 1--2% 2% of all fracturesof all fracturesSeventySeventy--five% are intrafive% are intra--articulararticular10% are Bilateral10% are BilateralSeventy % occur in the work placeSeventy % occur in the work placeMajority occur in men age 25Majority occur in men age 25--4545

Slide 3
IntroductionIntroduction
Treatment is controversial, with mixed Treatment is controversial, with mixed outcomes for both surgical and outcomes for both surgical and nonsurgical management. nonsurgical management. Very severe injury, this was recognized Very severe injury, this was recognized earlyearlyInitially all were treated nonsurgically. Initially all were treated nonsurgically. Initial surgical treatment was a primary Initial surgical treatment was a primary subtalar fusionsubtalar fusion

Slide 4
Second surgical method was closed Second surgical method was closed reduction and pins with plasterreduction and pins with plasterContinue to have problems with Continue to have problems with morning stiffness, subtalar motion and morning stiffness, subtalar motion and long term runninglong term running

Slide 5
AnatomyAnatomy
Largest tarsal boneLargest tarsal boneCalcaneus has been Calcaneus has been described as being described as being like an egglike an eggThree articular Three articular facetsfacetsPosterior, Middle Posterior, Middle and Anteriorand AnteriorAll articulate with All articulate with the talusthe talus

Slide 6
AnatomyAnatomy
Lateral anatomy is Lateral anatomy is important because it important because it is exposed during is exposed during the most common the most common surgical approachsurgical approachLateral process of Lateral process of the the tuberositytuberosity, origin , origin of the plantar fasciaof the plantar fasciaPeronealPeroneal trochleatrochleaView of the posterior View of the posterior facetfacet

Slide 7
Mechanism of injuryMechanism of injury
EssexEssex--LoprestiLopresti -- described two basic described two basic fracture types: joint depressed and fracture types: joint depressed and tongue type. tongue type. Axial compression with an oblique Axial compression with an oblique primary fracture line.primary fracture line.AnteriorAnterior--lateral superior to posteriorlateral superior to posterior--medial inferiormedial inferiorInvolving some portion of the posterior Involving some portion of the posterior facetfacetLateral process acts as a wedgeLateral process acts as a wedge

Slide 8
MechanismMechanism
Fracture is caused by a shearing forceFracture is caused by a shearing force
The posterior The posterior tuberositytuberosity is lateral to the is lateral to the mechanical axis of the legmechanical axis of the leg
This primary fracture line divides the This primary fracture line divides the calcaneuscalcaneus into a into a sustenaculumsustenaculum piece piece and a and a tuberositytuberosity piece.piece.
The secondary fracture line determines The secondary fracture line determines joint depression versus tongue typejoint depression versus tongue type

Slide 9
Joint DepressionJoint Depression
Secondary fracture line runs superior from the Secondary fracture line runs superior from the primary fracture line and exits behind the primary fracture line and exits behind the posterior facetposterior facet

Slide 10
Tongue typeTongue type
Secondary fracture line runs posterior to the Secondary fracture line runs posterior to the primary fracture line and exits out the back of primary fracture line and exits out the back of the the tuberositytuberosity

Slide 11
Physical ExamPhysical Exam
Heel appears shorter and wider and at Heel appears shorter and wider and at times in a times in a varusvarus positionposition
SuralSural nerve injury is commonnerve injury is common
High incidence of associated injuresHigh incidence of associated injures

Slide 12
Physical ExaminationPhysical ExaminationSignificant swelling with rapid onset of Significant swelling with rapid onset of fracture blisters and fracture blisters and ecchymosisecchymosis to the heel to the heel and archand arch

Slide 13
Associated injuriesAssociated injuries
70% of 70% of calcaneuscalcaneus fractures have an fractures have an associated injuryassociated injury
L spine 10% (3L spine 10% (3--12%)12%)
IpsilateralIpsilateral lower extremity fracture 10%lower extremity fracture 10%
Compartment syndrome 10%Compartment syndrome 10%

Slide 14
Radiographic EvaluationRadiographic Evaluation
Plain filmsPlain films
Lateral of the foot Lateral of the foot and ankleand ankle
Harris axial view Harris axial view
BrodenBroden ViewView

Slide 15
Lateral of the CalcaneusLateral of the Calcaneus
BohlerBohler angleangle
Insertion of a line Insertion of a line from posterior from posterior tuberositytuberosity to the to the posterior facet and posterior facet and anterior process to anterior process to the posterior facetthe posterior facet
2525--40 degrees40 degrees
Crucial angle of Crucial angle of GissaneGissane

Slide 16
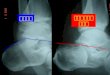
Broden’sBroden’s ViewView
Evaluates reduction of the posterior facetEvaluates reduction of the posterior facet
IR foot to 45 degreesIR foot to 45 degrees
Angle the xAngle the x--ray beam vertically toward the horizontal in ray beam vertically toward the horizontal in 10 degree increments form 1010 degree increments form 10--40 degrees40 degrees

Slide 17
Broden’sBroden’s ViewView

Slide 18
Harris ViewHarris ViewPassively Passively dorsiflexdorsiflex the ankle to achieve a the ankle to achieve a tangential radiograph across the plantar tangential radiograph across the plantar aspect of the heelaspect of the heel

Slide 19
CT ScanCT ScanCoronal and axial viewsCoronal and axial viewsCommonly Commonly saggitalsaggital reconstructionsreconstructionsThree dimensional reconstructions are Three dimensional reconstructions are availableavailableKnee flexed at 90 degrees and foot flat on the Knee flexed at 90 degrees and foot flat on the tabletableBoth feet simultaneously Both feet simultaneously

Slide 20
Classification based on Plain Classification based on Plain RadiographsRadiographs
Essex Essex LoprestiLopresti 19501950
Rowe in 1963 further subdivided into Rowe in 1963 further subdivided into comminuted and those that were notcomminuted and those that were not
SoeurSoeur and Remy and Remy –– 1975 1975 nonthalamicnonthalamicand thalamicand thalamic-- subdivided in to vertical subdivided in to vertical compression and shearing and compression and shearing and compressioncompression

Slide 21
Classification based on CT ScansClassification based on CT Scans
CrosbyCrosby--FitzgibbonsFitzgibbons–– 19901990
–– Type I Type I ––nondisplacednondisplaced
–– Type II Type II ––displacement of displacement of posterior facetposterior facet
–– Type III Type III ––comminuted intracomminuted intra--articular articular fx
SandersSanders–– 19931993
–– Type I Type I nondiplacednondiplaced
–– Type II 2 intraType II 2 intra--articular fragments articular fragments subtype into A/B/Csubtype into A/B/C
–– Type III 3 intraType III 3 intra--articular fragmentsarticular fragments
–– Type IV 4 fracture Type IV 4 fracture fragments
fxfragments

Slide 22
Sanders ClassificationSanders Classification
choose the coronal choose the coronal CT image that CT image that shows the posterior shows the posterior facet in widest facet in widest profile profile mark two vertical mark two vertical lines to divide the lines to divide the posterior facet into posterior facet into three equal sections three equal sections final line marks the final line marks the vertical border of the vertical border of the sustentaculumsustentaculum

Slide 23
Treatment OptionsTreatment Options
ControversialControversial
Best surgical outcomes are in Sanders Best surgical outcomes are in Sanders type II and tongue typetype II and tongue type
Poorer outcome associated with male Poorer outcome associated with male patients, men, overweight, and patients, men, overweight, and workman compensation casesworkman compensation cases

Slide 24
Surgical TechniquesSurgical Techniques
Multiple approaches described including Multiple approaches described including medial, lateral, combined, sinus tarsi, and medial, lateral, combined, sinus tarsi, and extensile lateralextensile lateralExtensile lateral approach in the most Extensile lateral approach in the most preferred preferred

Slide 25
ConsiderationsConsiderationsSoft tissue swellingSoft tissue swelling
Initially treat in a bulky Jones splintInitially treat in a bulky Jones splint
Goal of surgery is anatomic reduction Goal of surgery is anatomic reduction of posterior facet and the of posterior facet and the calcaneocuboidcalcaneocuboid jointjoint
Bone grafting, also controversial, some Bone grafting, also controversial, some studies show no benefit with lateral studies show no benefit with lateral plateplate

Slide 26
Surgical techniqueSurgical technique
Positioning Positioning -- Unilateral, then lateral Unilateral, then lateral decubitusdecubitus; ; Bilateral, then prone.Bilateral, then prone.No touch technique with the skin, K wires in No touch technique with the skin, K wires in the the talartalar neck, fibula and neck, fibula and cuboidcuboidStiemanStieman pin in the posterior pin in the posterior tuberositytuberosity to to indirectly reduce posterior facet indirectly reduce posterior facet

Slide 27
Surgical TechniqueSurgical Technique
Anterior Anterior calcaneuscalcaneusand posterior facet and posterior facet reduced and held reduced and held with k wireswith k wiresLow profile plate to Low profile plate to hold reductionhold reductionCC--arm with arm with flouroscopicflouroscopicBroden’sBroden’s view to view to visualize reductionvisualize reduction

Slide 28
Post operative carePost operative care
Immobilize for 3 weeks, until wound Immobilize for 3 weeks, until wound has healedhas healedEarly ROM, some recommend out of Early ROM, some recommend out of splint at week onesplint at week oneNonweightNonweight bearing 10bearing 10--12 weeks, 12 weeks, trabeculatrabecula bone formation on plain filmsbone formation on plain filmsProgression to full weight bearing Progression to full weight bearing without assistive deviceswithout assistive devicesMaximal medical improvement at 18 Maximal medical improvement at 18 monthsmonths

Slide 29
Primary Primary arthrodesisarthrodesisRecommended for some Sanders type IV fracturesRecommended for some Sanders type IV fracturesPoor results in type IV with both surgical and Poor results in type IV with both surgical and nonsurgical treatmentnonsurgical treatmentSanders et al reported only one good to excellent result Sanders et al reported only one good to excellent result in 11 type IV fractures treated with ORIFin 11 type IV fractures treated with ORIF

Slide 30
Primary Primary arthrodesisarthrodesis
Similar to Similar to ORIF,ORIF, restoration of anatomyrestoration of anatomyRemoval of the cartilage for the Removal of the cartilage for the undersurface of the talus and remnants undersurface of the talus and remnants of the posterior facet.of the posterior facet.Iliac crest bone grafting versus allograftIliac crest bone grafting versus allograftFusion with large fully threaded Fusion with large fully threaded canulatedcanulated screw from the posterior screw from the posterior facet into the talusfacet into the talus16 weeks or longer before complete 16 weeks or longer before complete fusionfusion