Embed Size (px)
Citation preview

2010. Patients with pathologic documentation of mesenteric lymphnodes were selected for further review. χ2 analysis was used toidentify clinicopathologic factors associated with mesenteric lym-phatic spread.Results: We found a total of 120 patients in whom mesenteric lymphnodes were isolated by our pathologist. The median age of thesepatients was 57 years (range: 22–77). The median number ofmesenteric nodes was eight (range: 1–37). Eighty-seven of 120(72%) cases had one or more mesenteric lymph node metastases,whereas 33 of 120 (28%) were negative. Among patients withmetastasis to mesenteric lymph nodes the only serosal or subserosalinvolvement was present in 31 of 87 (36%) patients; 31 of 87 (36%)had invasion into the muscolaris propria, 19 of 87 (22%) had invasioninto the submucosa, and six of 87 (6%) presented with full-thicknessinvasion of the bowel wall. The increase in depth of invasion was notcorrelated with the risk of mesenteric lymph node involvement.Retroperitonal evaluation (pelvic and/or paraaortic lymph nodedissection) was performed in 62% of the cases; 86% were positiveand 83% of them showed mesenteric lymph node metastasis. In the87 specimens analyzed, 59 (68%) had positive lymphovascular spaceinvasion (LVSI), while in the other group, LVSI was observed in only11 (33%) patients. Histologic grade did not correlate with the extentof bowel wall invasion or the presence of LVSI.Conclusions: Our results showed that lymph nodes are commonlyinvolved in the main basins draining from the different tumorlocations. Therefore, when ovarian carcinoma involves the rectosig-moid colon, metastases to mesenteric lymph nodes are as common asthose to the pelvic and paraaortic nodes. In patients with advanceddisease, lymph node sites in addition to the pelvic and/or paraaorticshould be considered, especiallywhenoptimal debulking is attempted.
doi:10.1016/j.ygyno.2010.12.151
145C-terminal binding protein 2: A potential marker for response tohistone deacetylase inhibitors in epithelial ovarian cancerL. Barroilhet, J. Yang, K. Hasselblatt, J. Rauh-Hain, W. Welch,R. Berkowitz, S. NgBrigham & Women's Hospital, Boston, MA
Objective: The objective of this study was investigation of theexpression pattern and functional roles of tumor antigen C-terminalbinding protein 2 (CtBP2) in epithelial ovarian cancer.
CtBP2 expression was studied in 105 ovarian tumors byimmunohistochemistry (IHC). Functional assays were performedwith human ovarian cancer cell lines that integrated a CtBP2-targeting short-hairpin RNA (shRNA) construct. Protein expressionin control and knockdown cell lines was examined by Westernblotting. Cell proliferation was determined by seeding cells to 35-mm culture dishes and allowing growth to different time points. ACytoMatrix Screen kit from Millipore was used to evaluate cellularadhesion to specific components of the extracellular matrix. Cellmigration assays were performed with a Boyden chamber-basedassay. β-Catenin activity was measured using a TOPFLASHluciferase reporter assay and cellular sensitivity to HDAC inhibitorswas measured using MTT assays. HDAC activity was measuredusing a colorimetric HDAC activity assay kit. CtBP2 expression wasrescued in the knockdown cell lines with a full-length CtBP2 cDNAexpression construct and empty vector. Overall survivals ofpatients with positive and negative CtBP2 expression wereestimated using the Kaplan–Meier method, and compared with alog rank test.
Results: Our study shows that expression of the transcriptional co-repressor CtBP2 is elevated in human ovarian cancers. Downregula-tion of CtBP2 expression in ovarian cancer cell lines using short-hairpin RNA strategy suppressed the growth rate, adhesion, andmigration of the resultant cancer cells. The knockdown cell lines alsoshowed upregulation of HDAC activity and increased sensitivity toselected HDAC inhibitors. Introduction of a CtBP2 expressionconstruct into the knockdown cell lines to reverse the CtBP2expression was able to partially rescue cellular sensitivity to theHDAC inhibitors. The overall survival of patients with positive CtBP2expression was found to be poorer (Fig. 1) compared with thosepatients with negative CtBP2 expression (P=0.05), based on theKaplan–Meier survival estimation.Conclusions: We propose that CtBP2 is an ovarian cancer oncogenethat regulates gene expression programs by modulating HDACactivity. CtBP2 expression may be a surrogate indicator of cellularsensitivity to HDAC inhibitors.
doi:10.1016/j.ygyno.2010.12.152
146CA-125 changes can predict optimal interval cytoreduction inpatients with advanced-stage epithelial ovarian cancer treatedwith neoadjuvant chemotherapyN. Rodriguez1, J. Rauh-Hain1,2, C. Feltmate1, M. Del Carmen2,3,R. Penson2,3, A. Goodman2,3, U. Matulonis4, M. Muto1,J. Schorge2,3, N. Horowitz11Brigham & Women's Hospital, Boston, MA, 2Massachusetts GeneralHospital, Boston, MA, 3Harvard University, Boston, MA, 4Dana–FarberCancer Institute, Boston, MA
Objective: The purpose of this studywas to evaluate the predictive powerof CA-125 changes in the management of patients undergoing neoadju-vant chemotherapy followedby interval debulking surgery (NACT-IDS) fora new diagnosis of ovarian, fallopian tube or peritoneal cancer.
Using the Cancer Registry databases from our institutions, aretrospective review of patients with FIGO stage IIIC and IV epithelialdisease who were treated with NACT-IDS between January 2006 andDecember 2009was conducted. All patients received carboplatin (AUC4 or 5) and paclitaxel (175 mg/m2). The Mann–Whitney U test wasused to compare data. Receiver operator characteristic curves weregenerated.Results: Fifty-seven patients met study criteria. Median age was66 years (range: 44–85). Median number of neoadjuvant cycles was 3
S63ABSTRACTS / Gynecologic Oncology 120 (2011) S2–S133

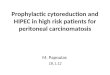
(range: 1–8). Optimal interval cytoreduction (defined as disease<1 cm) was achieved in 52 patients (91%). The median CA-125 levelat diagnosis and before IDS was 545 U/mL (range: 38–10,150) and63 U/mL (range: 5–2945), respectively. When patients with intervaloptimal cytoreduction were compared with patients with suboptimalcytoreduction, there was no statistical difference in the mean CA-125level at diagnosis (1326 U/mL vs 589 U/mL, P=0.3) or before IDS(227 U/mL vs 570 U/mL, P=0.1). The mean percentage drop betweenthe CA-125 obtained before NACT and the pre-IDS CA-125 differedsignificantly between patients who had optimal and those who hadsuboptimal cytoreduction (82% vs 41%, P<0.001). All patients(n=33) with a CA-125 drop greater than 80% by the third cycle oftherapy had an optimal cytoreduction. In comparison, four of the fivepatients who had suboptimal cytoreduction had a CA-125 drop≤50%.This ≤50% CA-125 drop was seen in only three of 52 patients withoptimal cytoreduction. An 80% drop in CA-125 was able to predictoptimal versus suboptimal cytoreduction with a sensitivity of 62%,specificity of 100%, positive predictive value of 100%, and negativepredictive value of 17%. The table outlines a comparison of thepercentage drop between the CA-125 obtained before NACT and thepre-IDS CA-125.Conclusions: Percentage change in CA-125 from the time of diagnosisto IDS is predictive of surgical outcome. In our study, patients whoachieved a ≥80% drop in CA-125 by cycle 3 of NACT achieved optimalcytoreduction. A ≤50% drop was predictive of a suboptimalcytoreduction, but did not exclude optimal cytoreduction. If ourfindings are confirmed in a larger cohort, a <50% drop in CA-125 mayencourage alternative management strategies.
Comparison of the sensitivity, specificity, PPV, and NPV atdifferent percentage changes between the CA-125 obtained beforethe first cycle of chemotherapy and the preoperative CA-125 forprediction of optimal cytoreduction.
doi:10.1016/j.ygyno.2010.12.153
147CA-125 surveillance for women with ovarian, fallopian tube orprimary peritoneal cancers: What do survivors think?L. Boyd, S. Bedell, J. Curtin, R. Wallach, B. Pothuri, F. Muggia,A. Tiersten, S. BlankNew York University School of Medicine, New York, NY
Objective: Monitoring CA-125 levels is an expected part of patientcare for women with ovarian, fallopian tube or primary peritonealcancers. Recent evidence calls into question whether CA-125 levelsshould be monitored in surveillance in the absence of symptoms. Wesought to determine if patients would accept no longer obtaining CA-125 levels as part of routine surveillance.
Institutional review board approval was obtained. With theuse of billing codes, patients with ovarian, fallopian tube orprimary peritoneal cancer were identified. From February 2010to July 2010, an anonymous, self-administered survey wasdistributed to patients carrying one of these diagnoses. Descrip-tive statistics were performed and Fisher's exact test was
applied to compare groups, with two-tailed P<0.05 consideredsignificant.Results: A total of 70 patients returned the survey. The average age ofrespondents was 61, and the majority were white (59/70) and non-Hispanic (66/70). The average time from diagnosis was 48 months,and 52 of 70 (74%) had stage III or IV disease. Thirty-one of 70 (44%)had received treatment for recurrent disease.When asked, "do you askfor your CA-125 results never, rarely, sometimes, most times oralways," 63 of 70 (76%) responded "most times or always." Thirty-fourof 70 (49%) responded that they were "most times" or "always"anxious about the results. Fifty-nine of 70 (84%) believed CA-125 canbeused todetect cancer earlier, and44of 70 (63%) believedCA-125 canbe used to start treatment earlier. Eighteen of 70 (26%) believed thatCA-125 can be used to "decrease the treatment time needed," and 17 of70 (24%) believed that CA-125 "can decrease the likelihood of dyingfrom cancer." Fifty-one of 70 (73%) believed that CA-125 should bechecked "every three to six months" or "more frequently than everythree months." Only one of 70 (1%) believed that CA-125 should bechecked "only with symptoms." Forty-one of 70 (59%) would "mildly"(3/70) or "strongly" (38/70) disagree if their physicians stoppedchecking CA-125 on a routine basis. Patients with advanced-stagedisease were more likely to want frequent CA-125 testing (P=0.03).Conclusions: The majority of ovarian cancer survivors are stronglyinterested in following their CA-125 results despite the fact thatthree-quarters have realistic expectations about its overall lack ofeffect on eventual outcome. A policy of testing CA-125 only whensymptoms develop would likely have poor acceptance, particularlyfor patients with advanced-stage disease.
doi:10.1016/j.ygyno.2010.12.154
148Calretinin as a prognostic indicator in granulosa cell tumorH. Arabi1, R. Ali-Fehmi2, L. Solomon2, Z. Al-Wahab2, A. Semaan2,S. Bandyopadhyay2, A. Munkarah3, R. Morris21Detroit Medical Center, Detroit, MI, 2Karmanos Cancer Institute, Detroit,MI, 3Henry Ford Health System, Detroit, MI
Objective: Granulosa cell tumor (GCT) is a rare neoplasm hallmarkedby an indolent clinical course and late recurrences. Although multipleclinical and pathologic parameters have been implicated as prog-nostic indicators for GCT, their predictive significance remainscontroversial. Calretinin is a calcium-binding protein primarilyexpressed by selected neurons in the peripheral and central nervoussystems. Its expression in mesotheliomas has made it the primaryconfirmatory antibody in standard mesothelioma immunohistochem-ical panels. Recently, calretinin has been evaluated and studied as anovel diagnostic/prognostic marker of ovarian sex cord–stromaltumors including granulosa cell tumors. The aim of the study wasto evaluate whether calretinin expression is correlated with theclinicopathologic parameters and prognosis in granulosa cell tumor.
Using our institutional database, we identified 51 patientsdiagnosed with GCT between 1975 and 2010 on whom archivaltissue was available. Tumors were histologically classified intojuvenile and adult subtypes. Follow-up data were obtained fromour institutional record and the national SEER registry. Immunohis-tochemical staining for calretinin was performed on tissue micro-array of all tumors. Immunoreactivity was semiquantitatively scoredbased on percentage of stained cells. Statistical correlation betweenimmunostaining results, pathologic parameters, and survival wasassessed using the t test.
Sensitivity Specificity PPV NPV
50% 94 80 98 5760% 90 80 98 4470% 82 80 98 4480% 62 100 100 1790% 48 100 100 15
S64 ABSTRACTS / Gynecologic Oncology 120 (2011) S2–S133