Embed Size (px)
Citation preview

CHAPTER 6
Bullying, Harassment, and Horizontal Violence in the Nursing WorkforceThe State of the Science
Judith A. Vessey, Rosanna DeMarco, and Rachel DiFazio
ABSTRACTIn the complex health care workplace of nurses, intra/interprofessional ideals intersect with the expectations of patients, families, students, and coworkers in a context of managed care environments, academia, and other health care enterprises. Integral to quality assessment, management, and assurance is col-legial and respectful communication. Decades of reported descriptive and anec-dotal data on intra/inter professional and on client communication, describe the antithesis of these ideals. Specifi cally, increasing frequency and rates of persis-tent bullying, harassment, or horizontal violence (BHHV) have shown to yield detrimental effects on workplace satisfaction, workforce retention, and the psy-chological and physical health of nurses as well as implied effects on quality of patient care and risk of poor health outcomes. Persistent BHHV among nurses is a serious concern. In advancing the science of description and explanation to a level of prevention intervention, explanatory models from biology, developmen-tal psychology, intra/interpersonal interactionism are described along with the-oretical explanations for the prevalence of BHHV in nurse workplaces. Making
© 2011 Springer Publishing CompanyDOI: 10.1891/0739-6686.28.133
THE WORKPLACE
Debisette_PTR_CH06_01-04-11_133-158.indd 133Debisette_PTR_CH06_01-04-11_133-158.indd 133 4/1/2011 8:11:45 PM4/1/2011 8:11:45 PM

134 ANNUAL REVIEW OF NURSING RESEARCH
the connection between explanatory models and creative solutions to address BHHV through multiple levels of behavioral infl uence such as individual, envi-ronmental, interpersonal, and cultural contexts is key to advancing the science of the relationship between professional behavior and client/family/community health care outcomes.
Quality patient-centered care requires cooperation among nurses, other health-care personnel, patients, and their families. A prerequisite for such partnerships includes respectful, collaborative, working relationships among members of the nursing workforce. Without these collaborative relationships, the open exchange of health care information is jeopardized, putting patients at risk for negative health outcomes. While there will always be challenges in nurses’ interactions, today’s increasingly complex and stress-laden hospitals can cause poor inter-actions to deteriorate further into persistent bullying, harassment, or horizontal violence (BHHV) among nurses (Clark, Leddy, Drain, & Kaldenberg, 2006). When BHHV occurs, all meaningful communication is essentially stopped.
BHHV is a problem; within and across all health care professional groups the preponderance of evidence supports that BHHV is the greatest problem intra-professionally within nursing, both in its prevalence and level of distress it causes (Farrell, 1997, 1999; Randle, 2003; Woelfl e & McCaffrey, 2007). Intraprofessional BHHV also permits, and even encourages, interprofessional BHHV to fl ourish (Duddle & Boughton, 2007).This review will focus on intraprofessional (nurse to nurse) BHHV, particularly as it is manifested in acute care settings. Its descrip-tion, explanatory models, epidemiology, and impact will be explicated. Finally, the identifi cation of interventions and solutions including primary and second-ary prevention strategies designed to rapidly identify and manage BHHV will be described.
METHODInclusion CriteriaIn order to allow for the greatest representation of BHHV and to later ana-lyze, synthesize, and generalize key constructs (Cooper, Hedges, & Valentine 2009), all articles that were written by nurses or included nurses in their target population in which bullying, harassment, horizontal (lateral) violence, and/or social aggression were key concepts were reviewed. Inclusion criteria were not limited to data-based articles in refereed journals; the nursing literature is replete with clinically focused articles about BHHV in the nursing workforce but actual research evidence is scant. To impose this limitation would severely truncate this
Debisette_PTR_CH06_01-04-11_133-158.indd 134Debisette_PTR_CH06_01-04-11_133-158.indd 134 4/1/2011 8:11:46 PM4/1/2011 8:11:46 PM

Violence in the Nursing Workforce 135
review. Instead, using the rubric of evidence-based practice (Melnyk & Fineout-Overholt, 2005), review and clinically focused refereed articles and professional organizational white papers and briefs were considered to be the evidence of professional expertise. The full array of unpublished studies was not included due to diffi culties with identifi cation and retrieval. Research and reviews pub-lished in refereed electronic journals were included if it was retrievable. Because BHHV occurs across the international nursing workforce, all articles written in English were included, regardless of origin.
Search Strategies and Critique MethodsThe accessible literature base was identifi ed using the following search strate-gies: keyword and author search of journals indexed in the following databases: CINAHL (1982–2010), Medline (1966–2010), and PsycAbstracts/PsycINFO (1987–2010). Manual searches of the reference lists of identifi ed research and review articles were also conducted. Although attempts were made to be as inclusive as possible, the conclusions were drawn only from the retrieved litera-ture and thus may not be totally representative of all aspects of BHHV within the nursing workforce, especially for nurses working outside of the acute care arena where there is signifi cantly less information available.
All articles were reviewed chronologically and conceptually to ascertain how each contributed to our understanding of BHHV. Articles were coded as to whether they were research, and if so, by the conceptual framework that was used, the study methodology, and the analytic techniques employed. Nonresearch literature was evaluated on the evidence provided that supported the authors’ assertions and the quality of the journal in which the article appeared. Finally, in order to better explicate its theoretical underpinnings, supportive literature that addressed explanatory models of BHHV behaviors across biological and psycho-social sciences was reviewed to yield frameworks that described specifi c physio-logical, developmental, intrapersonal and interpersonal aspects of BHHV.
FINDINGS: THE STATE OF THE SCIENCEDefi nitionThe World Health Organization (2002) has defi ned violence as “the intentional use of physical force or power, threatened or actual, against oneself, another person, or against a group or community that either results in or has a high likelihood of resulting in injury, death, psychological harm, mal-development or deprivation.” BHHV are one subset that meets this defi nition. Although there is a considerable literature on workplace violence and BHHV, there is lack of standardized defi nitions among these three terms and numerous other related
Debisette_PTR_CH06_01-04-11_133-158.indd 135Debisette_PTR_CH06_01-04-11_133-158.indd 135 4/1/2011 8:11:46 PM4/1/2011 8:11:46 PM

136 ANNUAL REVIEW OF NURSING RESEARCH
terms (e.g., social, relational, and passive aggression; workplace trauma) that are used in the literature (Broome, 2008; National Advisory Council on Nurse Education and Practice [NACNEP], 2007; Wiskow, 2002). Commonalities across these terms include offensive, abusive, intimidating, or insulting behaviors that cause psychological and/or physical distress to the recipient. Careful concept analyses to distinguish among the terms were conducted and a standardized nomenclature was created by the authors to normalize terms across the litera-ture. For example, horizontal and lateral violence were determined to share all of the same root characteristics; the same can be said for the term bullying, also known as mobbing in the international community.
Bullying differs from horizontal violence in that a real or perceived power differential between the instigator and recipient must be present in bullying, while horizontal violence occurs among peers. With bullying, anyone can be a potential target while harassment generally is associated with the notion of dif-ference—whether due to gender, race, ethnicity, age or disability (Gillen, 2002; Normandale & Davies, 2002). In the literature, these terms are frequently used interchangeably or bullying is used as an umbrella term to describe all interper-sonal violence in the workplace (Gilmour & Hamlin, 2003). Due to the concep-tual overlap and the fact that these terms are often used interchangeably in the literature, for this review, the terms BHHV will be examined together as a single construct. BHHV is then defi ned as repeated, offensive, abusive, intimidating, or insulting behavior, abuse of power, or unfair sanctions that makes recipients upset and feel humiliated, vulnerable, or threatened, creating stress and under-mining their self-confi dence.
Explanatory Models for the Occurrence of BHHVExplanatory models abound in the literature about social contexts that contrib-ute to BHHV; an inclusive view of why BHHV may occur needs to include an understanding of a variety of models that move beyond just defi ning BHHV. Evidence-based explanatory models elucidate the infl uence of human interac-tions in biological, developmental, intrapersonal, and environmental spheres of nurses in the workplace. Models from these three paradigms are critiqued in terms of their explanatory power in explaining the occurrence of BHHV.
Biological ModelsBiologic or biobehavioral models help identify plausible reasons for direct or covert aggressive behaviors in the workplace. These models also can help explain why some individuals could be easy targets. Biologic models that are used to explain the biobehavioral responses of perpetrators or victims of BHHV all have limitations. This is primarily due to the fact that cognitive or mental processes
Debisette_PTR_CH06_01-04-11_133-158.indd 136Debisette_PTR_CH06_01-04-11_133-158.indd 136 4/1/2011 8:11:46 PM4/1/2011 8:11:46 PM

Violence in the Nursing Workforce 137
occur as antecedents to biobehavioral responses and effect behavior over time (Lupien, McEwen, Gunnar, & Heim, 2009). Genetics (temperament) and early experiences in growth and development effect neurological development and future cognitive performance (Cirulli et al., 2010); response antecedents may vary as a selective fi lter for different individuals based on their experiences with stress and coping (Olff, Langeland, & Gersons, 2005).
Despite these limitations, early studies demonstrated through animal and human experiments that the removal or lowering of the levels of testosterone decrease aggression and/or dominance and biobehavioral responses to stress. In women, this takes the form of befriending the perpetrator rather than a fi ght or fl ight response that is often connected with the activation of testosterone (Albert, Walsh, Gorzalka, Siemens, & Louie, 1986). Women tend to use attachment behaviors to quell aggression and these are triggered by oxytocin, not testos-terone (Campbell, 2008; Jack, 1993, 1999). Terburg, Morgan, and van Honk (2009) supported the claim that female aggression exists, but that it is less medi-ated by testosterone and thus aggression is not overt but social or relational in nature. For example, adult victims of “mobbing” have altered circadian cycles of cortisol levels which may negatively infl uence the social climate by affecting, sen-sory acuity, learning, and memory in the workplace (Kudielka & Kern, 2004). Finally, dehydroepiandrosterone (DHEA) is an endogenous hormone secreted by the adrenal gland that can protect the individual from exposure to cortisol and thus mitigate its effect on behavior. Testosterone, cortisol, and DHEA in com-bination with environmental infl uences have an interactive role in the develop-ment of behavior (Kudielka, 2004).
Developmental ModelsThe larger domain of social aggression has as a key characteristic the intent on the part of a perpetrator to do social harm while one subtype, relational aggres-sion, focuses on harm directed to the individual or in the case of BHHV the peer specifi cally (Archer & Coyne, 2005). Galen and Underwood (1997) describe relational aggression as a direct or indirect form of social aggression used to dam-age a peer’s self esteem, social status or both. Archer et al. (2005) in analyzing the differences in goals and strategies across indirect, social, and relational aggres-sion state that forms of aggression change across age. In all cases, indirect forms of aggression historically have been used primarily by girls. With the advent of the cyberbullying, a type of indirect aggression, early work suggests that equal gender participation is the norm (Kiriakidis & Kavoura, 2010).
From a developmental perspective, indirect aggression as a learned expe-rience by girls may be reinforced developmentally for women over time. Jack (1999) explored the origins, meanings, and experiences of women’s aggression
Debisette_PTR_CH06_01-04-11_133-158.indd 137Debisette_PTR_CH06_01-04-11_133-158.indd 137 4/1/2011 8:11:46 PM4/1/2011 8:11:46 PM

138 ANNUAL REVIEW OF NURSING RESEARCH
through interviews with women from varying socio-economic backgrounds. She argues that aggression arises from failures in relationships with other people and can take the form of veiled/indirect approaches, control in getting back at others, or indirect resisting victimization. Jack’s main argument is that women are not aggressive because of human nature, but that indirect aggression develops in a cultural and interpersonal context. She states: “the basic pattern behind the differing forms [of aggression in women] remains the same: attempts to hurt, to oppose, or to express anger go underground to reach others through hidden channels, while surface behaviors mask the intent” ( Jack, 1999, p. 188).
Intrapersonal ModelsUnique situational issues that can affect individuals, help explain why BHHV may be a response to situations occurring in the workplace environments. Hershcovis and colleagues (2007) identifi ed use of drugs and alcohol, interpersonal/family and economic stressors outside of the workplace, and circadian effects related to time of day one works (shifts in the case of hospital settings) as key components of aggression in the workplace. Balducci, Alfano, and Fraccaroli (2009) investi-gated the relationships between the individuals’ experience of mobbing (bully-ing) at work (N = 107) and personality traits and symptom patterns as assessed by the Minnesota Multiphasic Personality Inventory (MMPI-2). Individuals who were the recipients of the mobbing scored highly on the neurotic and paranoid components of the MMPI-2. A pattern of positive and signifi cant correlations was found between the frequency of exposure to mobbing behaviors and the MMPI-2 clinical, supplementary, and content scales, including the Post-traumatic Stress Diagnostic Scale (McCarthy, 2008). Half of the participants in this study, and who were recipients of mobbing, showed a level of posttraumatic stress symp-toms consistent with posttraumatic stress disorder. In addition, the frequency of exposure to mobbing predicted suicidal ideation and behavior, with depression only partially mediating this relationship.
Jack’s (1993) seminal research on silencing the self behaviors and Jack and Ali’s (2010) more recent work, explain that women silence or suppress certain thoughts, feelings, and actions that may contradict another’s view. The “other” to which Jack (1993) originally referred to was often an intimate partner, but others have identifi ed the concept and behaviors in the workplace of nurses (DeMarco, 1997, 2002; DeMarco & Roberts, 2003; Roberts, DeMarco, & Griffi n, 2009). “Silencing the self” is an intrapersonal behavior based on a relational situation, i.e., women trying to avoid confl ict to maintain relationships and/or ensure their psychological or physical safety (Jack, 2010). One schema that describes the result of silencing the self is the inner stress and strain women expressed in Jack’s original work (1993) about how divided women often felt about outwardly
Debisette_PTR_CH06_01-04-11_133-158.indd 138Debisette_PTR_CH06_01-04-11_133-158.indd 138 4/1/2011 8:11:46 PM4/1/2011 8:11:46 PM

Violence in the Nursing Workforce 139
trying to keep peace and not disrupt relationships (“not rocking the boat”) while inwardly feeling more and more anger. The anger often comes from a violation of justice in that one is held back from doing the right thing (telling others directly what they need and feel). Over time anger and self-blame become a struggle behind the mask of compliance for women (Jack, 1999).
Interpersonal ModelsBehaviors like aggression or withdrawal can create roles (bully versus victim) and can infl uence how others behave in the context of these roles. Emotional and cognitive reactions to BHHV begin to be part of a work culture in which self-esteem, feelings of injustice, resentment, and frustration results in what Bowling and Beehr (2006) call “reciprocation” (p. 1001) within the work environment. Reciprocation takes the form of retaliatory behaviors that are intended to “get even” with others or the organization. Whether the perpetrator stands alone or is assisted with others in the group or institution directly or indirectly can vary across work environments, cultures, and normative beliefs about behavior.
Each disciplinary perspective appears to recognize that, like in other types of workplaces, BHHV takes on the form of relational aggression in the work-place. Galen and Underwood (1997) defi ne relational aggression as a subtype of social aggression where a perpetrator targets a victim. The key characteristic of social aggression is the intent on the part of a perpetrator of BHHV to do social harm while relational aggression in BHHV focuses on the peer. Social aggression is described as a direct or indirect form of relational aggression used to damage a peer’s self esteem, social status or both.
The process of social aggression is both overt and covert (passive) in nature, as are the responses of the victims. The overriding effects of the interpersonal aggression can be identifi ed at the individual, workgroup, and organizational level in the health care setting. Beyond developmental perspectives of how indi-viduals develop over time and learn to tacitly accept cultural imperatives about appropriate and nonappropriate behavior discussed in the ontogenetic section of the ecological model, Archer and Coyne (2005) found that girls may be just as aggressive as boys when using manipulative forms of aggression, such as gossip-ing and spreading rumors in all types of environmental settings (home, school, and later at work). These forms of aggression are known by the term social aggression including subtypes of relational aggression previously mentioned as indirect or passive aggression. A functional explanation for indirect aggression in the work environment includes behavior that is an alternative strategy to direct aggression, generally used when the costs of direct aggression are high and when the aim of the behavior is to socially exclude, or harm the social status of, a vic-tim while simultaneously infl ating one’s own social status (Jack, 1999). In this
Debisette_PTR_CH06_01-04-11_133-158.indd 139Debisette_PTR_CH06_01-04-11_133-158.indd 139 4/1/2011 8:11:46 PM4/1/2011 8:11:46 PM

140 ANNUAL REVIEW OF NURSING RESEARCH
way, BHHV have the characteristic of being additive in that they accumulate burden on the individual similar to that of a toxin in an unhealthy environment. Although extremely subtle, BHHV may have not only an additive but synergistic effect in relationship to consequent behaviors.
Crick and colleagues (2006) use the term relational aggression to char-acterize girls’ and later women’s indirect practice of “harming others through purposeful manipulation and damage of their peer relationships” by exclusion in the context of the work environment, individuals can withdraw friendship, or control behavior, spreading rumors so peers will reject others. Boys/men use physical, verbal aggression or intimidation as forms of aggression whereas women try to affect the relational space between individuals. Examples of rela-tional aggression in nurse workplaces can include nurses creating “in-groups” that share information, activities, friendship, confi dences and workloads, but clearly do not do the same with others in the workplace who are at the same peer level. Those who are excluded from the “in-group” are put in a position of feeling like outsiders, “less-than,” not welcome and generally feel stigmatized in some way (Underwood, 2003).
In trying to understand why direct or indirect aggression among nurses occurs in the work environment, an explanatory model that intersects gender studies, social science, psychology, and individual/environment interactions is that of Oppressed Group Behaviors (Roberts, 1983). Roberts (1983) was the fi rst nurse who described BHHV as outcomes of structural or social contexts of work environments of nurses based on the original work, Pedagogy of the Oppressed, by Paulo Freire (2000) and conceptualizing her own observations of nurses in the workplace “oppressed group behaviors.” Freire’s (2000) primary contribution to Roberts’ understanding and interpretation of BHHV was in the area of critical pedagogy. As an educator who was highly infl uenced by Marxist principles in Brazil, Friere explored how oppression is often justifi ed in a normative manner by a mutual process between the “oppressor” and the “oppressed.” Freire theorized that the powerless in societies where oppression proliferates can be frightened of freedom, i.e., freedom to address negative behavior of an oppressor as opposed to supporting a culture of BHHV. Friere beckoned those that were oppressed to pursue constantly and responsibly BHHV as defi ned in this paper. According to Freire, freedom is the result of action not inaction. Roberts (1983, 1996, 1997) identifi ed in her work that inaction on the part of nurses when BHHV were pre-sent in the workplace was related to a history of gender oppression as well as marginalization from the discipline of medicine. Using the work of Freire, she described the ability of dominant groups who identify norms as the “right” ones.
Individual, workgroup, and larger work cultures or systems are related and perpetuate acceptance of BHHV as normative while supporting
Debisette_PTR_CH06_01-04-11_133-158.indd 140Debisette_PTR_CH06_01-04-11_133-158.indd 140 4/1/2011 8:11:46 PM4/1/2011 8:11:46 PM

Violence in the Nursing Workforce 141
inaction—decreased acts of freedom—when BHHV are not named and ignored for reasons of maintaining power and control. When nurse managers and admin-istrators do not address BHHV it may lead to “silencing the self” as a force of “inaction” that maintains power and control for nurse managers and administra-tors. It also perpetuates the sub-oppression that Freire (2000) identifi ed when one who was oppressed has power (DeMarco, 2003). Hutchinson, Vickers, Jackson, and Wilkes (2006) developed an organizational model and matching outcome measures to evaluate specifi c domains of the workplace that accounted for antecedents of bullying behavior. These researchers identifi ed organizational tolerance, informal organizational alliances and misuse of legitimate authority processes and procedures as antecedents to bullying acts. These bullying acts were at the personal reputation and competence level as well as attacks through work process. The individual/environmental consequences identifi ed in this model of bullying acts included (1) normalization of bullying, (2) distress and avoidance of bullying in the workplace, (3) negative health effects, and (4) inter-ruption to work and career trajectory.
Prevalence of BHHVThere are incomplete global epidemiologic data of BHHV due to the diffi culty tracking events secondary to defi nitional inconsistencies and measurement problems, including the “the lack of systematic and coordinated data collection procedures and scant research” (NACNEP, 2007, p. 18). Although the exact prev-alence is not known, BHHV is accepted as a common and pernicious problem and a persistent, occupational hazard within the global nursing workforce (Clark, 2006; Farrell, Bobrowski, & Bobrowski, 2006; Gunnarsdottir, Sveinsdottir, Bernburg, Fridriksdottis, & Tomasson, 2006; Hegney, Eley, Plank, Buikstra, & Parker, 2006; Kwok, Law, Li, Ng, Cheung, Fung, et al., 2006; Quine, 2001; Rutherford & Rissel, 2004; Stevens, 2002; Yildirim, 2009).
Five studies conducted in the international arena reveal that between 17% and 76% of professional nurses report experiencing BHHV (Clark, 2006; Farrell, 2006; Gunnarsdottir, 2006; Hegney, 2006; Kwok, 2006; Quine, 2001; Rutherford, 2004; Stevens, 2002); marked differences in study methodolo-gies likely account for this large range. Data for the U.S. nursing workforce is sparse. Simons’ (2008) study of measured negative acts consistent with bul-lying in Massachusetts registered nurses (RNs; N = 511); 31% reported being bullied (with bullying subjectively defi ned as >1 negative act) and bullying was a signifi cant (p < .0005) factor in intent to leave the workplace. Stanley, Martin, Nemeth, Michel, and Welton (2007) studied lateral violence of staff RNs (N = 601) at one hospital; 46% indicated that lateral violence was a very or some-what serious problem, although an explicit defi nition of lateral violence was not
Debisette_PTR_CH06_01-04-11_133-158.indd 141Debisette_PTR_CH06_01-04-11_133-158.indd 141 4/1/2011 8:11:46 PM4/1/2011 8:11:46 PM

142 ANNUAL REVIEW OF NURSING RESEARCH
provided. In a cross-sectional study, Australian nurses (N = 2,487) reported that in across their last fi ve shifts, 1.1% had experienced nurse-on-nurse physical violence, 2% had threats of violence, and another 14.7% experienced emotional abuse (Roche, Diers, Duffi eld, & Catling-Paull, 2010). An American Association of Critical-care Nurses (AACN) study (2006) indicates that 88% of nurses (N = 4,000) work with a colleague that engages in low intensity behaviors (e.g., verbal abuse, gossip, self-promotion at another’s expense) consistent with BHHV. Lastly, new, and as yet unpublished data from a federally funded lateral violence project, reports that 88% of nurses have been recipients of similar low- intensity forms of lateral violence while in a staff nurse position (“Upstate Lateral Violence,” n.d.). More concerning is that 76% report witnessing such behaviors directed at one or more colleagues on a weekly basis; this is supported by Stanley et al.’s (2007) work, where 6% reported frequently observing lateral violence behaviors among coworkers.
These studies, however, lack methodological rigor (AACN, 2006; Stanley et al., 2007; “Upstate Lateral Violence,” n.d.), lack clear defi nitions (AACN, 2006; “Upstate Lateral Violence,” n.d.), did not include the full scope of BHHV behav-iors (AACN, 2006; Simons, 2008; Stanley et al., 2007; “Upstate Lateral Violence,” n.d.), used nonspecifi c sampling criteria (AACN, 2006), used instrumentation with insuffi cient psychometric evaluation (AACN, 2006; Simons, 2008; Stanley et al., 2007; “Upstate Lateral Violence,” n.d.), or had a poor response rates—54.4% (Simons, 2008) and 36% (Stanley et al., 2007) indicating that sampling bias may be an issue. The reason for the absence of robust prevalence studies in not understood although the infl uence of culture, government-controlled or fragmented and competitive health systems, fears of litigation, or acceptance of longstanding attitudes (e.g., “nurses eat their young”) and roles of professional nurses in the larger society cannot be discounted.
As with other forms of victimization, signifi cant underreporting is likely (Ferns & Chojnacka, 2005; NACNEP, 2007). Frequent low-grade BHHV goes unnoticed by others and the recipient may not report such inci-dents for fear of appearing petty. In part, this may be because these behaviors are learned in the schoolyard where most bullying among girls is relational, covert and socially toxic—ostracism, insults, divisive gossip, and so on—the same behaviors that are demonstrated in the workplace (Farrington, 1993; Rayner & Hoel, 1998; Vessey, DeMarco, Gaffney, & Budin, 2009). BHHV, surrounded by a “culture of silence,” fears of retaliation, and the perception that “nothing will be changed,” can also effectively shut down the exchange of information (DeMarco, 1998; 2002; Ferns, 2005; Stearley, 1997). Data support these assertions. Out of two British studies and one U.S. study on bullied nurses who reported that they had tried to take action, only 22–43%
Debisette_PTR_CH06_01-04-11_133-158.indd 142Debisette_PTR_CH06_01-04-11_133-158.indd 142 4/1/2011 8:11:46 PM4/1/2011 8:11:46 PM

Violence in the Nursing Workforce 143
was satisfi ed with the result (Quine, 1999; Royal College of Nursing, 2002; Vessey, 2009).
Perpetrators and Recipients of BHHVFor some nurses, BHHV is viewed as a normal part of the job and therefore tol-erated (Dunn, 2003; Lewis, 2006). This view is reinforced by the hierarchical organizational culture within hospitals which limits reporting of BHHV-related behaviors (Alexy & Hutchins, 2006; Lewis, 2006). What constitutes BHHV var-ies, in part, according to people’s ideas and perceptions about workplace culture. BHHV is commonly a ‘learned behavior’ among practicing nurses (Lewis, 2006). Issues are rarely handled during the early stages of confl ict and when they do emerge, nurse managers try to keep them contained (Lewis, 2006; MacIntosh, 2005). Workplace BHHV thrives on organizationally dysfunctional units. BHHV tends to be more common in settings where technical expertise is valued over interpersonal competence (Cole, 1996; Corr, 2000). Some individuals and unit cultures may support or condone BHHV; staff who thrive in such environments are seen by their colleagues as strong and resilient (Hughes, 2003).
BHHV increases in high-intensity, stressful environments and has become more prevalent among the nursing workforce over the last decade along with escalating patient acuity, attempts to ‘right-size’ the nursing workforce, and sub-sequent increases in staff turnover (Gilmour, 2003; Jackson, Clare, & Mannix, 2002; Long, 1996; Mayhew & Chappell, 2002a, 2002b). Research has demon-strated that nurses who have just entered the workforce are at greater risk of being targeted for BHHV as they are often younger, less experienced, somewhat insecure in their new role, and less aware of the a unit’s cultural norms than their more seasoned colleagues (Griffi n, 2004; McKenna, Smith, Poole, & Coverdale, 2003; Simons & Mawn, 2010). When BHHV is unnoticed or unchecked by nurse managers or supervisors, the instigator considers such behaviors appro-priate (Hughes, 2003). In descriptive studies of nurses working in acute care settings, 50%–76% of nurses report regularly witnessing BHHV (Quine, 2001; Stanley et al., 2007; “Upstate Lateral Violence,” n.d.), but frequently have little idea as to how they might best intervene. In qualitative interviews, nurses (n = 29) revealed that witnessing BHHV between colleagues was actually more distressing than physical assault from patients (Farrell, 1997). Over time, bystanders who observe BHHV but choose not to intervene, even if they abhor BHHV behaviors, it is postulated that they become complicit and begin to create reasons to justify the BHHV they have witnessed (Deans, 2004; Stevens, 2002).
Nursing management is implicated as being the most frequent initiator of BHHV (Deans, 2004; Long, 1996; Quine, 1999; Vessey, 2009). For example, in the Vessey et al. (2009) survey, 37% of U.S. nurses (N = 314) reported nursing
Debisette_PTR_CH06_01-04-11_133-158.indd 143Debisette_PTR_CH06_01-04-11_133-158.indd 143 4/1/2011 8:11:46 PM4/1/2011 8:11:46 PM

144 ANNUAL REVIEW OF NURSING RESEARCH
management engaged in bulling behaviors. Similar fi ndings were reported in the (British) Royal College of Nursing (2002) nationwide survey (N = 778), with fi nd-ings indicating that 41% of the nursing workforce was bullied by management in the six months prior to their study. Lastly, McMillan (1995) reported that 61% of British nurses identifi ed line managers as a source of constant bullying (1995), noting that because managers are in positions of power, they are as likely to target strong as well as weak subordinates just in the process of exercising power and advancing themselves, which may come at the expense of others. The Royal College of Nursing (2002) noted that nurses who found their supervi-sors intimidating became less sensitive and more morally disengaged over time; these nurses’ disenchantment was also contagious to other staff members. A synthesis of available data supports that a crisis of leadership occurs in many hospitals when nurse managers are promoted to their posts based on clinical competence rather than the appropriate educational background and necessary organizational and leadership skills required for the position (Hauge, Skogstad, & Einarsen, 2007; Long, 1996; Pearson et al., 2004).
Psychological and Physical Impact of BHHVBHHV has been shown to be deleterious to the recipient’s psychological and physical health (Cortina & Magley, 2003; Gilmour, 2003; Gunnarsdottir, 2006; MacIntosh, 2005). Recipients of BHHV experience stress directly from the attacks. They constantly edit their behaviors to avoid what they perceive as further aggravation of the instigators; avoidance and withdrawal behaviors have been repeatedly documented (Gilmour, 2003; Graveson, 1998; Hansen et al., 2006; McVicar, 2003) as has the increased use of tobacco, alcohol and other substances (Kivimaki, Elovainio, & Vahtera, 2000; Normandale, 2002). Psychological distress symptoms that have been reported across studies includ-ing anxiety, irritability, panic attacks, tearfulness, depression, loss of confi dence and self-esteem, mood swings, and irritability (Cortina, 2003; Gilmour, 2003; Graveson, 1998; Gunnarsdottir, 2006; Yildirim, 2009). Physical symptoms include sleep disturbances, headaches, increased blood pressure, anorexia, gas-trointestinal upset, and loss of libido. Lastly, sleep disorders, posttraumatic stress disorder, suicide ideation and suicide have been documented in the research literature (Gilmour, 2003; Graveson, 1998; Normandale, 2002; Hansen, 2006; Royal College of Nursing, 2002; Vessey, 2009).
International studies that have explored the biological effects of BHHV underlying psychological and physical symptomatology experienced by on recipients indicate compelling effects on the body. Di Rosa and colleagues (2009) postulated that victims of workplace mobbing were at increased risk for psy-chological diagnosable disorders. Comparing healthy individuals with those
Debisette_PTR_CH06_01-04-11_133-158.indd 144Debisette_PTR_CH06_01-04-11_133-158.indd 144 4/1/2011 8:11:46 PM4/1/2011 8:11:46 PM

Violence in the Nursing Workforce 145
experiencing mobbing by measuring oxidative stress, these researchers found victims of mobbing had higher serum levels of protein carbonyl groups and of nitrosylated proteins which are biological markers of oxidative stress conditions. Monteleone and colleagues (2009) found hypoactivity of the hypothalamo- pituitary-adrenal axis in victims of BHHV and conjectured through further analy-sis that there is a relationship between brain function and victim’s temperament and chronicity of the work-related psychological distress as a result of BHHV.
Cortina and Magley (2003) demonstrated in their large scale survey (n = 1167) of nonnurse public employees, that the impact of BHHV on recipi-ents is exacerbated further if, when seeking redress, recipients experience retali-ation from their supervisors. This has signifi cant implications for nursing as it is known that collectively, symptomatology related to BHHV lowers nurses’ confi -dence and competence (Deans, 2004; Leivers, 2004) and thus can infl uence the quality of nursing care rendered and subsequently, patient care outcomes.
Impact of BHHV on Quality of CareBHHV interrupts critical components of teamwork; communication, the exchange of crucial health information, and collaborative decision-making, all of which are associated with increased medical errors and poorer patient outcomes (Hughes, 2003; ISMP, 2009; Joint Commission, 2008; Longo, 2007; Quine, 2001). However, strong correlational or causal impacts of BHHV on patient safety/quality of care are just beginning to be specifi cally explicated in the empir-ical literature. Nurses’ reactions to BHHV have resulted from situations in which their contributions are ridiculed, their sense of professional mastery threatened, and ultimately, deeply eroding their self-esteem. Nurse recipients report avoid-ing staff interactions that target them for insult and abuse (Macintosh, 2005; McVicar, 2003; Quine, 1999, 2001; Stevens, 2002). Because BHHV is not limited solely to a dysfunctional dyadic relationship, staff who are bystanders are affected and teamwork is undermined (Hughes, 2003). Hutchinson, Wilkes, Jackson & Vickers, (2010) have recently used structural equation modeling and confi r-matory factor analysis to test a multidimensional model of bullying using data from 370 surveys completed by Australian nurses. Organizational characteris-tics, including misuse of authority/policies/procedures, organizational tolerance, and informal alliances were confi rmed as critical antecedents to bullying, its frequency, and intra- and interpersonal consequences.
Results of BHHV—poorer job satisfaction, professional disengagement, and increased turnover—are related to poorer quality of care (American Organization of Nurse Executives [AONE], 2000; Armstrong & Laschinger, 2006; Moyad, Daraiseh, Shell, & Salem, 2006; Rowe & Sherlock, 2005). Numerous studies have consis-tently identifi ed the linkages between BHHV and poor job satisfaction (Graveson,
Debisette_PTR_CH06_01-04-11_133-158.indd 145Debisette_PTR_CH06_01-04-11_133-158.indd 145 4/1/2011 8:11:46 PM4/1/2011 8:11:46 PM

146 ANNUAL REVIEW OF NURSING RESEARCH
1998; Hegney, 2006; Leer, 2006; Mayhew, 2002a, 2002b; Yildririm, 2009). Across studies, recipients of verbal abuse report declines in morale (67–81%), decreased productivity (41–71%), and decreased nursing care delivery (36–54%), although the survey methodologies employed were not particularly rigorous. Other studies have successfully identifi ed the relationship between poor job satisfaction and neg-ative patient outcomes (American Nurses Association [ANA], 2001; Blegen, 1993; Hegyvary & Haussman, 1976; Weisman & Nathanson, 1985). A study conducted by the Institute for Safe Medication Practices (2009), examined the role intimidat-ing behaviors had on medication errors. Within the RN subsample (n = 1,565), 7% stated that intimidation lead to a medication error within the past year (translating to 110 avoidable medication errors); however, the instigator of intimidation (i.e., RN, MD, PharmD) was not specifi ed.
In other studies, nurses self-reported a range of in increase in patient safety errors from 51% to 87%, but the type of error and specifi c antecedents were not explicated (Braun, Christle, Walker, & Tiwanak, 1991; Cox, 1987; Sofi eld & Salmond, 2003). Roche and colleagues (2010) also demonstrated positive corre-lations between workplace violence and patient falls, delayed medication admin-istrations, and medication errors, however, the defi nition of violence employed encompassed more than just nurse to nurse BHHV, including violence between nurses and physicians or patients and their families. All of these organizational, staffi ng, and patient care outcomes consequences result in substantial direct and indirect fi nancial costs, although these are diffi cult to calculate.
Available Evidence-based Interventions and InstrumentationDespite the presence of BHHV and its impact on workforce indicators and as a root cause of preventable medical errors, evidence-based strategies for its detection and prevention have not been specifi cally addressed in organizational white papers/reports/materials that posit solutions for contextual nursing workplace issues associated with BHHV(AACN 2006; American Association of Colleges of Nursing, 2004; American Hospital Association Commission on Workforce for Hospitals and Health Systems, 2002; AONE, 2000; National Institute for Occupational Safety and Health, 2002; U.S. Health Resources Services Administration, 2002). The two exceptions are the Center for American Nurses (2008) policy state-ment on lateral violence and bullying and the Joint Commission’s 2008 Sentinel Event Alert Behaviors that Undermine a Culture of Safety (2008). The American Nurses’ policy statement outlines broad actions that need to be taken at the inter-personal and organizational levels, with specifi c calls for more research on all aspects of BHHV in the workplace. The Joint Commission’s Sentinel Event Alert outlines the need for institutions to develop the following primary and second-ary prevention activities: (1) skills-based training and coaching, (2) ongoing,
Debisette_PTR_CH06_01-04-11_133-158.indd 146Debisette_PTR_CH06_01-04-11_133-158.indd 146 4/1/2011 8:11:46 PM4/1/2011 8:11:46 PM

Violence in the Nursing Workforce 147
nonconfrontational surveillance, (3) a system for assessing staff perceptions of the seriousness and extent of unprofessional behaviors, and (4) policies that sup-port early reporting without fear of intimidation.
There is little evidence that organizational leadership has the tools to rou-tinely employ interventions to thwart the development of BHHV or engage in system-wide screening when BHHV is most amenable to intervention. While a plethora of articles (>130) describe the problem of BHHV; a review of the literature revealed fi ve instruments to measure constructs related to BHHV, all of which have limitations (see Table 6.1). None of these instruments embrace the full range of behaviors seen in BHHV. Additionally, such ‘stand-alone’, single construct instruments, while appropriate for research, may not be amenable for clinical use due to their negative tone and possible ramifi cations that could negatively infl uence the workplace climate. In the era of multiple staff surveys to continuous quality assessment, hospital administrators may be reluctant to employ them for ongoing surveillance due to their costs respondent fatigue resulting in poor response rates.
A variety of interventions strategies have been proposed including no tolerance policies (Bigony et al., 2009) and application of restorative/shared responsibility approaches (Hutchinson, 2009). Documentation of the num-ber of health care facilities that have policies specifi c to BHHV is limited. In some countries, there are specifi c laws that address BHHV and the organization’s responsibility for monitoring and addressing such incidents (Rocker, 2008). In the United States, federal legislation prohibits harassment based on the notion of difference—race, ethnicity, gender—but not for bullying per se. In a small study conducted on nursing administrators (N = 108) in New York, 55% of the facilities that they represented had policies that addressed horizontal violence but they were only enforced approximately 43% of the time (Sellers, Millenbach, Kovach, & Yingling, 2009–2010).
In addition, only three small studies were identifi ed that focused on inter-vention. Griffi n (2004) investigated the use of cognitive rehearsal with newly licensed RNs (N = 26). After a two hour didactic teaching session, cueing cards for handling lateral violence were provided to the participants. At one year postint-ervention, qualitative data indicated that cognitive rehearsal helped them deal with lateral violence; no quantitative data were collected. DeMarco, Roberts, and Chandler (2005) pilot-tested a group writing intervention designed to decrease negative workplace behaviors with a sample of graduate nursing students (N = 5).The goal was to evaluate the effi cacy of the intervention; no data regard-ing the effectiveness of the intervention was documented.
The third study by Barrett, Piatek, Korber, and Padula (2009) used a quasi-experimental, pretest/posttest design. The researchers implemented two team
Debisette_PTR_CH06_01-04-11_133-158.indd 147Debisette_PTR_CH06_01-04-11_133-158.indd 147 4/1/2011 8:11:47 PM4/1/2011 8:11:47 PM

TABLE 6.1Instruments to Measure Constructs Related to BHHV
Instrument Construct Description and Psychometric Properties
Bullying Acts Inventory for the Nursing Workplace (Hutchinson, Wilkes, Vickers, & Jackson, 2008)
Bullying • 17 items, 7-point Likert scale, 3 subscales: attack upon competence/reputation (6 items), personal attack (6 items), attack through work tasks (5 items)
• Normed on nurses (N = 102) of varying ages, race/ethnicity n/a; diverse practice areas; 20% response rate
• Overall Cronbach’s � = .83; 93, .89, & .88 for respective subscales
• Content Validity by expert panel• Used to test a multidimensional model of
bullying in the workplace. Results indicated that the characteristics of the organization are antecedents of bullying and infl uence the occurrence of bullying and the resultant consequences (Hutchinson et al., 2010).
Lateral Violence in Nursing Survey (Stanley et al., 2007)
Lateral violence
• 23 dichotomous items organized by perceived seriousness, oppressors, mediators, and open-ended questions
• Normed on RNs (n = 601) from 1 U.S. SE hospital; licensed from <1 to >30 years, race/ethnicity: 82% White; 36% response rate
• No reliability or validity reported• No reports of the use of this tool in other
studies identifi ed
Negative Acts Questionnaire–Revised (Simons, 2008)
Horizontal violence
• Adapted from Norwegian Negative Acts Questionnaire
• 22 items descriptive of bullying behaviors if repetitive over time, 3-point Likert scale
• Trialed with MA RNs (n = 511), 78% licensed w/in past 3 years; race/ethnicity: 84% White; 6.7% male
• Cronbach’s � = .88; no validity indicated• Note: Original scale also revised for use in Japan
(Abe & Henly, 2010)
(Continued)
148
Debisette_PTR_CH06_01-04-11_133-158.indd 148Debisette_PTR_CH06_01-04-11_133-158.indd 148 4/1/2011 8:11:47 PM4/1/2011 8:11:47 PM

Violence in the Nursing Workforce 149
building sessions, each lasting two hours with RNs (N = 145) from four diverse patient care areas. Each unit served as their own control. Signifi cant (p = .037) differences were noted between pre- and posttest scores on the Group Cohesion Scale using the Mann-Whitney U test. No statistical fi ndings were reported for the differences in the pre- and posttest scores for the RN-RN interaction subscale of the NDNQI Adapted Index of Work Satisfaction, although the authors state that some improvements on the units were seen. Unfortunately, the response rates on pre- and posttest measures were only 41% and 31% in the pre- and posttest measures respectively, indicating potential sampling bias. Moreover, the dose of intervention was not likely to result in long-term change as BHHV is an engrained problem, rarely responsive to brief interventions. The reasons for the lack of intervention research are complex and include but are not limited to methodological diffi culties, lack of standardized and measurable defi nitions, the lack of reliable and valid instrumentation, diffi culty achieving institutional access, and limited available funding.
TABLE 6.1Instruments to Measure Constructs Related to BHHV (Continued)
Instrument Construct Description and Psychometric Properties
Sabotage Savvy Questionnaire (Briles, 1999)
Sabotage • 40 items, 3-point scoring; victim & saboteur subscales
• Perioperative RNs (n = 145). Race/ethnicity: 86.2% White
• No initial reliability and validity reported• Used in one other study, Dunn, 2003; reported
Cronbach’s � .86 & .72 for victim & saboteur subscales
Violence Climate Survey (Kessler, Spector, Chang, & Parr, 2008)
Safety/violence
• 18-item measure assessing workplace climate; 3 subscales: policies, practices, pressures
• Full-time employees (n = 216), diverse work settings not specifi c to nursing; 82% female, race/ethnicity data not provided
• Cronbach’s �’s for policies, practices, & pressures subscales: .95, .90, & .90 respectively; Face validity indicated
• No reports of the use of this tool in other studies identifi ed
Debisette_PTR_CH06_01-04-11_133-158.indd 149Debisette_PTR_CH06_01-04-11_133-158.indd 149 4/1/2011 8:11:47 PM4/1/2011 8:11:47 PM

150 ANNUAL REVIEW OF NURSING RESEARCH
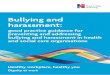
STRATEGIES FOR ADDRESSING BHHVA model (see Figure 6.1) that can advance incremental and signifi cant traction to address the challenge of BHHV is the stages of prevention model (Wallace, 2008). When applied to BHHV, primary prevention refers to reducing the number of BHHV incidents by intervening before BHHV occurs. Primary pre-vention requires identifying the risk and protective factors for BHHV, elimi-nating or against the development of BHHV and its adverse consequences; an approach advocated by nursing leaders (Embree & White, 2010). Organization wide awareness reducing associated risks and strengthening those individual, interpersonal, and organizational factors, campaigns, policy development, and the use of risk markers to target high-risk groups and/or individuals for educa-tional interventions and follow up are exemplars of such activities.
Secondary prevention focuses on early problem detection of BHHV when these behaviors are still ‘under the radar’. It helps stop BHHV from worsening and prevents or ameliorates long-term sequelae from developing. Lead time is the time for potential discovery of BHHV by screening compared to the time when BHHV becomes obvious. Screening allows for early detection of BHHV when it is most amenable to intervention. The longer the lead-time, the greater the opportunity for screening. No empirical data are available regarding lead time of BHHV, but anecdotal reports indicate that due to its subtle nature, it is often years before it is addressed, if ever (Cortina, 2003; ISMP, 2009; MacIntosh, 2005; Stevens, 2002). Screening tools would help nursing leadership teams and occupational health nurses who may speculate about which nursing units are experiencing BHHV, but have limited options for objectively identifying them and for tracking improvements after interventions have been initiated.
Tertiary prevention is required when there is failure to address issues of BHHV until after full-blown problems have erupted. Such interventions,
Primaryprevention
Secondaryprevention
Tertiaryprevention
Screening time
Educational awareness campaigns
Policies
Risk markers for ID of potential target areas
Monitoring:RN satisfaction surveys
Site-specific interventions
Personnel actions
Unit dissolution
Exa
mpl
es
Lead time
FIGURE 6.1 The prevention model as the study’s guiding framework.© Judith A. Vessey.
Debisette_PTR_CH06_01-04-11_133-158.indd 150Debisette_PTR_CH06_01-04-11_133-158.indd 150 4/1/2011 8:11:47 PM4/1/2011 8:11:47 PM

Violence in the Nursing Workforce 151
including disciplinary action, terminations, and in the worst case scenario, unit reorganization or dissolution, are palliative in nature, result in suboptimal out-comes. Tertiary prevention activities can usually be avoided with appropriate primary and secondary prevention.
SUMMARYIntraprofessional BHHV is a global issue. It is detrimental to nurses’ well-being and organizational culture. It results in nursing dissatisfaction, increasing disengagement and absenteeism, intent to leave, and interrupts intraprofes-sional communication, and is a crucial component in medical errors and patient outcomes. The overall quality of available evidence on BHHV is lim-ited; there particularly are few data-based intervention studies that provide foundational information useful for adoption by clinical settings. Although the reasons for this are open to conjecture, in part it may be due to the historic lack of public acknowledgement and/or unwillingness by hospital administrators to recognize or address BHHV. Future well-conducted studies are needed.
REFERENCESAbe, K., & Henly, S. J. (2010). Bullying (ijime) among Japanese hospital nurses: Modeling responses
to the revised Negative Acts Questionnaire. Nursing Research, 59(2), 110–118.Albert, D. J., Walsh, M. L., Gorzalka, B. B., Siemens, Y., & Louie, H. (1986). Testosterone removal
in rats results in a decrease in social aggression and a loss of social dominance. Physiology & Behavior, 36(3), 401–407.
Alexy, E. M., & Hutchins, J. A. (2006). Workplace violence: A primer for critical care nurses. Critical Care Nursing Clinics of North America, 18(3), 305–312.
American Association of Colleges of Nursing. (2004). Hallmarks of quality and patient safety. Retrieved from http://www.aacn.nche.edu/publications/pdf/Qual&PatientSafety.pdf
American Association of Critical-care Nurses. (2006). Silence kills. The seven crucial conversations for healthcare. Retrieved February 9, 2009, from www.aacn.org/WD/Practice/Docs/PublicPolicy/SilenceKills.pdf
American Hospital Association Commission on Workforce for Hospitals and Health Systems. (2002). In our hands: How hospital leaders can build a thriving workforce. Retrieved from http://www.eric.ed.gov/ERICDocs/data/ericdocs2sql/content_storage_01/0000019b/80/1b/03/62.pdf
American Nurses Association. (2001). Analysis of the American Nurses Association staffi ng survey. Warwick, RI: Cornerstone Communications Group.
American Organization of Nurse Executives. (2000). Perspectives on the nursing shortage: A blueprint for action. Washington, DC: Author.
Archer, J., & Coyne, S. M. (2005). An integrated review of indirect, relational, and social aggression. Personality and Social Psychology Review, 9(3), 212–230.
Armstrong, K. J., & Laschinger, H. (2006). Structural empowerment, Magnet hospital character-istics, and patient safety culture: Making the link. Journal of Nursing Care Quality, 21(2), 124–32, quiz 133.
Debisette_PTR_CH06_01-04-11_133-158.indd 151Debisette_PTR_CH06_01-04-11_133-158.indd 151 4/1/2011 8:11:47 PM4/1/2011 8:11:47 PM

152 ANNUAL REVIEW OF NURSING RESEARCH
Balducci, C., Alfano, V., & Fraccaroli, F. (2009). Relationships between mobbing at work and MMPI-2 personality profi le, posttraumatic stress symptoms, and suicidal ideation and behav-ior. Violence and Victims, 24(1), 52–67.
Barrett, A., Piatek, C., Korber, S., & Padula, C. (2009). Lessons learned from a lateral violence and team-building intervention. Nursing Administration Quarterly, 33(4), 342–351.
Bigony, L., Lipke, T. G., Lundberg, A., McGraw, C. A., Pagac, G. L., & Rogers, A. (2009). Lateral vio-lence in the perioperative setting. AORN Journal, 89(4), 688–96; quiz 697.
Blegen, M. A. (1993). Nurses’ job satisfaction: A meta-analysis of related variables. Nursing Research, 42(1), 36–41.
Bowling, N. A., & Beehr, T. A. (2006). Workplace harassment from the victim’s perspective: A theo-retical model and meta-analysis. The Journal of Applied Psychology, 91(5), 998–1012.
Braun, K., Christle, D., Walker, D., & Tiwanak, G. (1991). Verbal abuse of nurses and non-nurses. Nursing Management, 22(3), 72–76.
Briles, J. (1999). Women to women 2000: Becoming sabotage savvy in the new millennium. Far Hills, NJ: New Horizon Press.
Broome, B. A. (2008). Dealing with sharks and bullies in the workplace. The ABNF (Association of Black Nursing Faculty) Journal, 19(1), 28–30.
Campbell, A. (2008). Attachment, aggression and affi liation: The role of oxytocin in female social behavior. Biological Psychology, 77(1), 1–10.
Center for American Nurses. (2008). Bullying and lateral violence in the workplace. Retrieved from http://centerforamericannurses.org/associations/9102/files/Position%20StatementLateral%20Violence%20and%20Bullying.pdf
Cirulli, E. T., Kasperaviciute, D., Attix, D. K., Need, A. C., Ge, D., Gibson, G., & Goldstein, D. B. (2010). Common genetic variation and performance on standardized cognitive tests. European Journal of Human Genetics, 18(7), 815–820.
Clark, P. A., Leddy, K., Drain, M., & Kaldenberg, D. (2007). State nursing shortages and patient satisfaction: More RNs–better patient experiences. Journal of Nursing Care Quality, 22(2), 119–27; quiz 128.
Cole, A. (1996). Fighting the bully. The Health Service Journal, 106(5485), 22–24.Cooper, H. M., Hedges, L. V., & Valentine, J. C. (2009). The handbook of research synthesis and meta-
analysis (2nd ed.). New York, NY: Russell Sage Foundation.Corr, M. (2000). Reducing occupational stress in intensive care. Nursing in Critical Care, 5(2),
76–81.Cortina, L. M., & Magley, V. J. (2003). Raising voice, risking retaliation: Events following inter-
personal mistreatment in the workplace. Journal of Occupational Health Psychology, 8(4), 247–265.
Cox, H. C. (1987). Verbal abuse in nursing: Report of a study. Nursing Management, 18(11), 47–50.
Crick, N. R., Ostrov, J. M., & Werner, N. E. (2006). A longitudinal study of relational aggres-sion, physical aggression, and children’s social-psychological adjustment. Journal of Abnormal Child Psychology, 34(2), 131–142.
Deans, C. (2004). Nurses and occupational violence: The role of organizational support in moderat-ing professional competence. Australian Journal of Advanced Nursing, 22(2), 15–18.
DeMarco, R. (1997). The relationship between family life and workplace behaviors: Exploring the gendered perceptions of staff nurses through the framework of systemic organization. (Doctoral Dissertation, Wayne State University, 1997). Dissertation Abstracts International, 58 (3B), 9725823.
DeMarco, R. F. (1998). Caring to confront in the workplace: An ethical perspective for nurses. Nursing Outlook, 46(3), 130–135.
Debisette_PTR_CH06_01-04-11_133-158.indd 152Debisette_PTR_CH06_01-04-11_133-158.indd 152 4/1/2011 8:11:47 PM4/1/2011 8:11:47 PM

Violence in the Nursing Workforce 153
DeMarco, R. F. (2002). Two theories/a sharper lens: The staff nurse voice in the workplace. Journal of Advanced Nursing, 38(6), 1–8.
DeMarco, R. F., & Roberts, S. J. (2003). Negative behaviors in nursing. The American Journal of Nursing, 103(3), 113–116.
DeMarco, R. F., Roberts, S. J., & Chandler, G. E. (2005). The use of a writing group to enhance voice and connection among staff nurses. Journal for Nurses in Staff Development, 21(3), 85–90; quiz 91.
Di Rosa, A. E., Gangemi, S., Cristani, M., Fenga, C., Saitta, S., Abenavoli, E., . . . Cimino, F. (2009). Serum levels of carbonylated and nitrosylated proteins in mobbing victims with workplace adjustment disorders. Biological Psychology, 82(3), 308–311.
Duddle, M., & Boughton, M. (2007). Intraprofessional relations in nursing. Journal of Advanced Nursing, 59(1), 29–37.
Dunn, H. (2003). Horizontal violence among nurses in the operating room. AORN Journal, 78(6), 977–988.
Embree, J. L., & White, A. H. (2010). Concept analysis: Nurse-to-nurse lateral violence. Nursing Forum, 45(3), 166–173.
Farrell, G. A. (1997). Aggression in clinical settings: Nurses’ views. Journal of Advanced Nursing, 25(3), 501–508.
Farrell, G. A. (1999). Aggression in clinical settings: Nurses’ views—A follow-up study. Journal of Advanced Nursing, 29(3), 532–541.
Farrell, G. A., Bobrowski, C., & Bobrowski, P. (2006). Scoping workplace aggression in nursing: Findings from an Australian study. Journal of Advanced Nursing, 55(6), 778–787.
Farrington, D. (1993). Understanding and preventing bullying. Crime and Justice, 17, 381–458.Ferns, T., & Chojnacka, I. (2005). Reporting incidents of violence and aggression towards NHS
staff. Nursing Standard (Royal College of Nursing [Great Britain]: 1987), 19(38), 51–56.Freire, P. (2000). Pedagogy of the oppressed. New York, NY: Continuum.Galen, B. R., & Underwood, M. K. (1997). A developmental investigation of social aggression
among children. Developmental Psychology, 33(4), 589–600.Gillen, P. (2002). A concept analysis of bullying in midwifery. Midwifery, 2(2), 46–51.Gilmour, D., & Hamlin, L. (2003). Bullying and harassment in perioperative settings. British
Journal of Perioperative Nursing: the Journal of the National Association of Theatre Nurses, 13(2), 79–85.
Graveson, G. (1998). Workplace bullying–the abuse of power. The British Journal of Theatre Nursing, 7(11), 21–23.
Griffi n, M. (2004). Teaching cognitive rehearsal as a shield for lateral violence: An intervention for newly licensed nurses. Journal of Continuing Education in Nursing, 35(6), 257–263.
Gunnarsdottir, H. K., Sveinsdottir, H., Bernburg, J. G., Fridriksdottir, H., & Tomasson, K. (2006). Lifestyle, harassment at work and self-assessed health of female fl ight attendants, nurses and teachers. Work (Reading, Mass.), 27(2), 165–172.
Hansen, A. M., Hogh, A., Persson, R., Karlson, B., Garde, A. H., & Ørbaek, P. (2006). Bullying at work, health outcomes, and physiological stress response. Journal of Psychosomatic Research, 60(1), 63–72.
Hauge, L. J., Skogstad, A., & Einarsen, S. (2007) Relationships between stressful work environ-ments and bullying: Results of a large representative study. Work & Stress, 21, 220–242.
Hegney, D., Eley, R., Plank, A., Buikstra, E., & Parker, V. (2006). Workplace violence in Queensland, Australia: The results of a comparative study. International Journal of Nursing Practice, 12(4), 220–231.
Hegyvary, S. T., & Haussman, R. K. (1976). Correlates of the quality of nursing care. The Journal of Nursing Administration, 6(9), 22–27.
Debisette_PTR_CH06_01-04-11_133-158.indd 153Debisette_PTR_CH06_01-04-11_133-158.indd 153 4/1/2011 8:11:47 PM4/1/2011 8:11:47 PM

154 ANNUAL REVIEW OF NURSING RESEARCH
Hershcovis, M. S., Turner, N., Barling, J., Arnold, K. A., Dupré, K. E., Inness, M., . . . Sivanathan, N. (2007). Predicting workplace aggression: A meta-analysis. The Journal of Applied Psychology, 92(1), 228–238.
Hughes, A. (2003). Being bullied what an insight. British Journal of Perioperative Nursing, 13(4), 166–8, 171.
Hutchinson, M. (2009). Restorative approaches to workplace bullying: Educating nurses towards shared responsibility. Contemporary Nurse: A Journal for the Australian Nursing Profession, 32(1–2), 147–155.
Hutchinson, M., Vickers, M., Jackson, D., & Wilkes, L. (2006). Workplace bullying in nursing: Towards a more critical organisational perspective. Nursing Inquiry, 13(2), 118–126.
Hutchinson, M., Wilkes, L., Vickers, M., & Jackson, D. (2008). The development and validation of a bullying inventory for the nursing workplace. Nurse Researcher, 15(2), 19–29.
Hutchinson, M., Wilkes, L., Jackson, D., & Vickers, M. H. (2010). Integrating individual, work group and organizational factors: Testing a multidimensional model of bullying in the nurs-ing workplace. Journal of Nursing Management, 18(2), 173–181.
Institute for Safe Medication Practices. (2009). Results from ISMP Survey on Workplace Intimidation. Retrieved January 9, 2009, from https://www.ismp.org/Survey/surveyResults/Survey0311.asp
Jack, D. C. (1993). Silencing the self: Women and depression. New York, NY: Harper Perennial.Jack, D. C. (1999). Behind the mask: Destruction and creativity in women’s aggression. Cambridge, MA:
Harvard University.Jack, D. C., & Ali, A. (2010). Silencing the self across cultures: Depression and gender in the social world.
New York, NY: Oxford.Jackson, D., Clare, J., & Mannix, J. (2002). Who would want to be a nurse? Violence in the work-
place–a factor in recruitment and retention. Journal of Nursing Management, 10(1), 13–20.Joint Commission. (2008, July 9). Sentinel Event alert. Behaviors that undermine a culture of
safety. Retrieved August 10, 2008, from http://www.jointcommission.org/SentinelEvents/SentinelEventAlert/sea_40.htm
Kessler, S. R., Spector, P. E., Chang, C., & Parr, A. D. (2008). Organizational violence and aggres-sion: Development of the three-factor violence climate survey. Work and Stress, 108–224.
Kiriakidis, S. P., & Kavoura, A. (2010). Cyberbullying: A review of the literature on harassment through the internet and other electronic means. Family & Community Health, 33(2), 82–93.
Kivimäki, M., Elovainio, M., & Vahtera, J. (2000). Workplace bullying and sickness absence in hos-pital staff. Occupational and Environmental Medicine, 57(10), 656–660.
Kudielka, B. M., & Kern S. (2004). Cortisol day profi les in victims of mobbing (bullying at the work place): Preliminary results of a fi rst psychobiological fi eld study. Journal of Psychosomatic Research, 56(1), 149–50.
Kwok, R. P., Law, Y. K., Li, K. E., Ng, Y. C., Cheung, M. H., Fung, V. K., . . . Leung, W. C. (2006). Prevalence of workplace violence against nurses in Hong Kong. Hong Kong Medical Journal, 12(1), 6–9.
Leer, R. E. (2006). Effective nursing management: A solution for nurses’ job dissatisfaction and low retention rate? Doctoral dissertation, Capella University, Minneapolis.
Leivers, G. (2004). Harassment by staff in the workplace: The experiences of midwives. MIDRS Midwifery Digest, 14, 19–24.
Lewis, M. A. (2006). Nurse bullying: Organizational considerations in the maintenance and perpe-tration of health care bullying cultures. Journal of Nursing Management, 14(1), 52–58.
Long, J. (1996). Battle of the bullies. Nursing Management, 3(6), 10–11.Longo, J. (2007). Bullying in the workplace: Reversing a culture. Silver Spring, MD: Center for American
Nurses.
Debisette_PTR_CH06_01-04-11_133-158.indd 154Debisette_PTR_CH06_01-04-11_133-158.indd 154 4/1/2011 8:11:47 PM4/1/2011 8:11:47 PM

Violence in the Nursing Workforce 155
Lupien, S. J., McEwen, B. S., Gunnar, M. R., & Heim, C. (2009). Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nature Reviews Neuroscience, 10, 434–445.
MacIntosh, J. (2005). Experiences of workplace bullying in a rural area. Issues in Mental Health Nursing, 26(9), 893–910.
Mayhew, C., & Chappell, D. (2002a). Bullying and the healthcare workforce. Lamp, 59(7), 29–30.Mayhew, C., & Chappell, D. (2002b). Occupational violence in the NSW health workforce: Establishment
of baseline data, report to the Taskforce on the Prevention and Management of Violence in the Health Workforce. NSW Department of Health, Sydney.
McCarthy, S. (2008). Post-traumatic Stress Diagnostic Scale (PDS). Occupational Medicine (Oxford, England), 58(5), 379.
McKenna, B. G., Smith, N. A., Poole, S. J., & Coverdale, J. H. (2003). Horizontal violence: Experiences of Registered Nurses in their fi rst year of practice. Journal of Advanced Nursing, 42(1), 90–96.
McMillan, J. (1995). Losing control. Nursing Times, 91, 40–43.McVicar, A. (2003). Workplace stress in nursing: A literature review. Journal of Advanced Nursing,
44(6), 633–642.Melnyk, B. M., & Fineout-Overholt, E. (2005). Evidence-based practice in nursing & healthcare: A
guide to best practice. Philadelphia, PA: Lippincott Williams & Wilkins.Monteleone, P., Nolfe, G., Serritella, C., Milano, V., Di Cerbo, A., Blasi, F., . . . Maj, M. (2009).
Hypoactivity of the hypothalamo-pituitary-adrenal axis in victims of mobbing: Role of the subjects’ temperament and chronicity of the work-related psychological distress. Psychotherapy and Psychosomatics, 78(6), 381–383.
Moyad, F. A., Daraiseh, N., Shell, R. & Salem, S. (2006). Workplace bullying: A systematic review of risk factors and outcomes. Theoretical Issues in Ergonomics Science, 7, 311–327.
National Advisory Council on Nurse Education and Practice. (2007). Violence against nurses. An assessment of the causes and impacts of violence in nursing education and practice (5th ed.). Retrieved February 1, 2009, from http://bhpr.hrsa.gov/nursing/NACNEP/reports/fi fth/status.htm
National Institute for Occupational Safety and Health. (2002). Violence. Occupational hazards in hospitals (DHHS [NIOSH] Publication # 2002–101). Retrieved from http://www.cdc.gov/niosh/2002-101.html
Normandale, S., & Davies, J. (2002). Bullying at work. Community Practitioner, 75, 474–477.Olff, M., Langeland, W., & Gersons, B. P. (2005). Effects of appraisal and coping on the neuroendo-
crine response to extreme stress. Neuroscience and Biobehavioral Reviews, 29(3), 457–467.Pearson, A., Laschinger, J., Porritt, K., Jordan, Z., Tucker, D., & Long, L. (2004). A comprehensive
systematic review of evidence on developing and sustaining nursing leadership that fosters a healthy work environment in health care. Health Care Reports, 2(7), 129–192.
Quine, L. (1999). Workplace bullying in NHS community trust: Staff questionnaire survey. BMJ (Clinical Research Ed.), 318(7178), 228–232.
Quine, L. (2001). Workplace bullying in nurses. Journal of Health Psychology, 6, 73–84.Randle, J. (2003). Bullying in the nursing profession. Journal of Advanced Nursing, 43(4), 395–401.Rayner, C., & Hoel, H. (1998). A summary review of literature relating to workplace bullying.
Journal of Community and Applied Social Psychology, 7, 181–191.Roberts, S. J. (1983). Oppressed group behavior: Implications for nursing. ANS. Advances in Nursing
Science, 5(4), 21–30.Roberts, S. J. (1996). Breaking the cycle of oppression: Lessons for nurse practitioners? Journal of the
American Academy of Nurse Practitioners, 8(5), 209–214.Roberts, S. J. (1997). Nurse executives in the 1990s: Empowered or oppressed? Nursing
Administration Quarterly, 22(1), 64–71.
Debisette_PTR_CH06_01-04-11_133-158.indd 155Debisette_PTR_CH06_01-04-11_133-158.indd 155 4/1/2011 8:11:47 PM4/1/2011 8:11:47 PM

156 ANNUAL REVIEW OF NURSING RESEARCH
Roberts, S., DeMarco, R. F., & Griffi n, M. (2009). The effect of oppressed group behavior on the culture of the nursing workplace: A review of evidence and interventions for change. Journal of Nursing Management, 17(3), 288–293.
Roche, M., Diers, D., Duffi eld, C., & Catling-Paull, C. (2010). Violence toward nurses, the work environment, and patient outcomes. Journal of Nursing Scholarship, 42(1), 13–22.
Rocker, C. F. (2008). Addressing nurse-to-nurse bullying to promote nurse retention. Online Journal of Issues in Nursing, 13(3). Retrieved from http://www.nursingworld.org/MainMenuCategories/ANAMarketplace/ANAPeriodicals/OJIN/TableofContents/vol132008/No3Sept08/ArticlePreviousTopic/NursetoNurseBullying.aspx
Rowe, M. M., & Sherlock, H. (2005). Stress and verbal abuse in nursing: Do burned out nurses eat their young? Journal of Nursing Management, 13(3), 242–248.
Royal College of Nursing. (2002). Working well: A call to employers. A summary of the RCN’s Working well survey into the wellbeing and working lives of nurses. London: RCN.
Rutherford, A., & Rissel, C. (2004). A survey of workplace bullying in a health sector organisation. Australian Health Review, 28(1), 65–72.
Sellers, K., Millenbach, L., Kovach, N., & Yingling, J. K. (2009). The prevalence of horizontal vio-lence in New York State registered nurses. The Journal of the New York State Nurses’ Association, 40(2), 20–25.
Simons, S. (2008). Workplace bullying experienced by Massachusetts registered nurses and the relationship to intention to leave the organization. ANS. Advances in Nursing Science, 31(2), E48–E59.
Simons, S. R., & Mawn, B. (2010). Bullying in the workplace—A qualitative study of newly licensed registered nurses. American Association of Occupational Health Nurses, 58(7), 305–311.
Sofi eld, L., & Salmond, S. W. (2003). Workplace violence. A focus on verbal abuse and intent to leave the organization. Orthopaedic Nursing/National Association of Orthopaedic Nurses, 22(4), 274–283.
Stanley, K. M., Martin, M. M., Nemeth, L. S., Michel, Y., & Welton, J. M. (2007). Examining lateral violence in the nursing workforce. Issues in Mental Health Nursing, 28(11), 1247–1265.
Stearley, H. (1997). Desensitization to nurse abuse. Revolution (Staten Island, NY), 7(4), 23–27.Stevens, S. (2002). Nursing workforce retention: Challenging a bullying culture. Health Affairs
(Project Hope), 21(5), 189–193.Terburg, D., Morgan, B., & van Honk, J. (2009). The testosterone-cortisol ratio: A hormonal
marker for proneness to social aggression. International Journal of Law and Psychiatry, 32(4), 216–223.
Underwood, M. K. (2003). Social aggression among girls. New York: The Guilford Press.Upstate Lateral Violence in Nursing Project (C. Luciano, PD). Department of Health and Human
Services, Health Services Resource Administration, Bureau of Health Professions, Nurses Education, Practice, and Research (NEPR) grant (award # is 5 D11HP08361).
U.S. Health Resources Services Administration. (2002). Projected supply, demand, and shortages of reg-istered nurses: 2000–2020. Retrieved from http://bhpr.hrsa.gov/healthworkforce/rnproject
Vessey, J. A., Demarco, R. F., Gaffney, D. A., & Budin, W. C. (2009). Bullying of staff registered nurses in the workplace: A preliminary study for developing personal and organizational strategies for the transformation of hostile to healthy workplace environments. Journal of Professional Nursing, 25(5), 299–306.
Wallace, R. B. (Ed.). (2008). Wallace/Maxcy-Rosenau-Last public health & preventive medicine (15th ed.). Philadelphia, PA: McGraw-Hill.
Weisman, C. S., & Nathanson, C. A. (1985). Professional satisfaction and client outcomes. A com-parative organizational analysis. Medical Care, 23(10), 1179–1192.
Debisette_PTR_CH06_01-04-11_133-158.indd 156Debisette_PTR_CH06_01-04-11_133-158.indd 156 4/1/2011 8:11:47 PM4/1/2011 8:11:47 PM

Violence in the Nursing Workforce 157
Wiskow, C. (2002). Framework guidelines for addressing workplace violence in the health sector. Geneva, Switzerland: The International Labour Offi ce, the World Health Organization, The International Council of Nurses, and Public Services International. Retrieved January 22, 2009, from http://www.ilo.org/public/english/dialogue/sector/papers/health/guidelines.pdf
Woelfl e, C. Y., & McCaffrey, R. (2007). Nurse on nurse. Nursing Forum, 42(3), 123–131.World Health Organization. (2002). World report on violence and health. Geneva, Switzerland:
Author.Yildirim, D. (2009). Bullying among nurses and its effects. International Nursing Review, 56(4),
504–511.
Debisette_PTR_CH06_01-04-11_133-158.indd 157Debisette_PTR_CH06_01-04-11_133-158.indd 157 4/1/2011 8:11:47 PM4/1/2011 8:11:47 PM

Copyright of Annual Review of Nursing Research is the property of Springer Publishing Company, Inc. and its
content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's
express written permission. However, users may print, download, or email articles for individual use.