Embed Size (px)
Citation preview


ARTICLES COLUMNS DEPARTMENTS
Practice Management .............. 281HIPAA Q&AJoan M. Kiel, PHD
Legal Report ............................ 282Biggest Mistakes—CredentialingCase StudiesMichael A. Cassidy, ESQ
Legal Report ............................ 284Update on Medical Malpractice Mediationin Western Pa.Jacqueline O. Shogan, ESQ
Robert A. Creo, ESQ
Legal Report ............................ 288New Medicare Appeal Rules Draw FireWilliam H. Maruca, ESQ
Special Report .......................... 297State Society Weighs In On EMRDarlene Kauffman
Profile ...................................... 298Bruce L. Wilder, MD, JD—Physician,Attorney, Advocate, VolunteerElizabeth L. Fulton
BULLETIN of the Allegheny County Medical Society
June 2005 ♦ Vol. 94 No. 6
You should never
marry someone
who doesn’t make
you laugh.—Garrison Keillor
“
”Dr. Gopal is a colon and rectal surgeon.
Key 2005 Legislative andRegulatory Initiatives ............... 265
Cover Art:
Nature’s Wonder
by Krishnan A. Gopal, MD
Thoughts from OurMedical Editor .........................266Morals, Social Norms and the Practice ofMedicineSafdar I. Chaudhary, MD
Editorial ...................................268How Electronic Health Records MayChange Health CareIndira P. Jevaji, MD
Getting There: Musings of aMedical Student ....................... 272What You Won’t Find in the SyllabusMatthew Neal
From Where I Sit: Viewpointof a Physician Executive ...........292Progress on Pay for PerformanceCarey T. Vinson, MD, MPM
Legal Perspective ......................294Stop Prescribing Cox-2 Inhibitors?A Medico-legal AnalysisLeslie Tar, MD, ESQ
Karen Tar, MSN, CRNP, ESQ
Society News ........................... 274♦ Photo: Contracts & Negotiations session♦ Photo: Sandra DaCosta works Senior Expo♦ Urologists to meet in June♦ Coding camp here in August♦ Physicians needed for health fair♦ Ob/Gyn society meeting held♦ Photo: Musical moment at surgeon’s meeting♦ Photo: Surgical society lifetime membership♦ Surgeons travel to West Virginia♦ Surgical society meets♦ Health Insurance renewal rates swing wide♦ ACMS calls for nominations♦ Medical ’biz in the ’Burgh
From the Mailbag .................... 277
Dear Doctor ............................ 277
Activities & Accolades ............. 278
Community Notes ................... 279
Continuing Education ............. 280
Calendar .................................. 283
2005 Editorial Index ................ 300
2005 Ad Index ......................... 304
Classifieds ................................ 306

264 u The Bulletin June 2005
2005 OFFICERS and
Executive Committee of the
Board of Directors
President
Mark A. Goodman
President-elect
Terence W. Starz
Vice President
Krishnan A. Gopal
Secretary
Adam J. Gordon
Treasurer
David L. Katz
Board Chair
Edward J. Teeple Jr.
DIRECTORS
2005
Douglas F. Clough
Paul W. Dishart
Carol E. Rose
Rajiv R. Varma
David S. Zorub
2006
Christopher J. Daly
David J. Deitrick
John F. Delaney Jr.
Jerome M. Itzkoff
James E. Wilberger Jr.
2007
Edward M. Barksdale Jr.
Melinda M. Campopiano
Charles N. Lebovitz
Edmund C. Watters
Mark L. Zeidel
PEER REVIEW BOARD
2005
Bernard I. Cohen
Krishnan A. Gopal
John A. Straka
2006
Jeffrey A. Perri
Jan D. Smith
2007
William D. Hetrick
Barbara E. Swan
PMS DISTRICT TRUSTEE
Paul W. Dishart
DISTRICT CENSOR
Phillip R. Levine
Affiliated with the Pennsylvania Medical Society and the American Medical Association
COMMITTEES
Bylaws
Krishnan A. Gopal
Communications
Leo McCafferty
Finance
Paul W. Dishart
Legislative
David J. Deitrick
Medical Legal
Krishnan A. Gopal
Membership
Rajiv R. Varma
Nominating
Carol E. Rose
Child Health
Jeffrey Upperman
Occupational Medicine
Joseph J. Schwerha
BRANCHES
McKeesport
Chair/Secretary
Louis A. DiToppa/
Leslie Silberman
South Hills
Chair
Joseph F. Hakas
Western
Chair/Secretary
Frank H. Rittenhouse/
Leticia Q. Jariwala
Tri-County
Chair/Secretary
Nisantha Banda/
Manmohan S. Luthra
ACMS ALLIANCE
President
Sandra DaCosta
First Vice President
Sally Buchanan
Second Vice President
Patty Barnett
Recording Secretary
Barbara Adelson
Corresponding Secretary
Cherry Woolhandler
Treasurer
Justina Purpura
Assistant Treasurer
Mary Kay Shaner
Visit our websitewww.acms.org
COPYRIGHT 2005:ALLEGHENY COUNTY MEDICALSOCIETYPOSTMASTER—Send addresschanges to: BULLETIN of theAllegheny County MedicalSociety, 713 Ridge Avenue,Pittsburgh, PA 15212.
BULLETIN
Medical Editor
Safdar I. Chaudhary
Associate Editors
Janet A. Chollet
Christopher J. Daly
Robert L. Ferris
Indira P. Jevaji
Timothy G. Lesaca
Basil A. Marryshow
Adam Z. Tobias
Frank T. Vertosick, Jr.
Managing Editor
Linda L. Smith
Contributing Editors
Adam J. Gordon
Ravi Kant
Deval Paranjpe
Melissa A. Somma
Erin A. Sullivan
Richard T.Vagley
Carey T. Vinson
ADMINISTRATIVE STAFF
Executive Director
John G. Krah
Assistant to the Director
Dorothy S. Hostovich
Bookkeeper
Susan L. Osborne
Communications
Director
Christina E. Morton
Assistant
Elizabeth L. Fulton
Assistant Executive Director,
Membership/Information
Services
Director
James D. Ireland
Manager
Dianne K. Meister, R.N.
Assistant
Nadine M. Popovich
E D I T O R I A L / A D V E R T I S I N G
OFFICES: BULLETIN of the Allegheny
County Medical Society, 713 Ridge Av-
enue, Pittsburgh, PA 15212; (412) 321-
5030; fax (412) 321-5323. USPS #072920.
PUBLISHER: Allegheny County Medi-
cal Society at above address.
The BULLETIN of the Allegheny County
Medical Society welcomes contributions
from readers, physicians, medical students,
members of allied professions, spouses,
etc. Items may be letters, informal clinical
reports, editorials, or articles. Contribu-
tions are received with the understanding
that they are not under simultaneous con-
sideration by another publication.
Issued the third Saturday of each month.
Deadline for submission of copy is the
SECOND Wednesday preceding publica-
tion date. Periodical postage paid at Pitts-
burgh, PA.
BULLETIN of the Allegheny County Medi-
cal Society reserves the right to edit all
reader contributions for brevity, clarity,
and length as well as to reject any subject
material submitted.
The opinions expressed in the Editorials
and other opinion pieces are those of the
writer and do not necessarily reflect the
official policy of the Allegheny County
Medical Society, the institution with
which the author is affiliated, or the
opinion of the Editorial Board. Adver-
tisements do not imply sponsorship by or
endorsement of the ACMS, except where
noted.
Publisher reserves the right to exclude any
advertisement which in its opinion does not
conform to the standards of the publication.
The acceptance of advertising in this publi-
cation in no way constitutes approval or
endorsement of products or services by the
Allegheny County Medical Society of any
company or its products.
Subscriptions: $25 nonprofit organizations;
$35 ACMS advertisers, and $45 others.
Single copy $2. Advertising rates and infor-
mation sent upon request by calling (412)
321-5030.

The Bulletin u 265June 2005
release data and research to show the
detrimental effects of low reimbursement and
unfair contracts.
Department of Labor and Industry
Revisions have been proposed to workers’
compensation cost-containment regulations.
If past practices are any indication (and they
usually are), further cost-containment efforts
will disproportionately focus on physicians
and their practices. Therefore, the state
society will carefully scrutinize criteria for
utilization review, collaborate on developing
qualifications for reviewers, and review
requirements for utilization review organiza-
tions. We’ll also work to refine the Notice of
Compensation Payable to providers.
Department of Public Welfare
With budget proposals to cut Medical
Assistance benefit utilization, our scrutiny is
more important than ever. The state society
will monitor implementation of the Access
Plus Enhanced Primary Care Case Manage-
ment and Disease Management Program.
We’ll also review the proposed implementa-
tion of cost-containment strategies for
Medical Assistance such as changes in
reimbursement for pharmaceuticals and
standards for review of increased drug
utilization. Finally, we’ll scrutinize any
proposed provider taxes.
Department of State
(professional licensure)
As noted above, scope of practice expansion
efforts by non-physician practitioners
continue to surface. The state society will
carefully review all of these proposals such
as changes to optometrist practice and
physician assistant practice regulations. We’ll
also review any proposed changes to the
operation of Medical and Osteopathic
Licensure Boards.
Pennsylvania Medical Society’sKey 2005 Legislative and Regulatory Initiatives
This information was provided by thePennsylvania Medical Society. For moreinformation, call (717) 558-7750 or logon to www.pamedsoc.org.
State budget issues
The society will seek increases in funding for
medical schools and Medical Assistance, both
critical to assuring access to health care for
all Pennsylvanians.
Shaping regulations
Bills become laws and laws become
regulations. Our regulatory experts, with
guidance from our Board of Trustees and
various committees, inject the physician
perspective into the process, helping to
shape regulations so they benefit patients
and doctors.
Because we work with numerous arms of the
state government, initiatives are arranged by
department below:
Department of Health
Ambulatory surgery has been restricted by
recent rulings from the Department of Health.
The Pennsylvania Medical Society is working
to reverse the rulings, while assuring the
safety and efficacy of laparoscopic and other
procedures in ambulatory surgery centers.
We hosted a summit with regulators,
ambulatory center representatives and
surgical specialty societies. We’ll also
continue to scrutinize any movement toward
instituting a CON process for existing or new
facilities.
Regarding CON, our regulatory experts will
review the Legislative Budget and Finance
Committee study and recommendations, and
will monitor the Department of Health’s
consideration of CON as part of the hospital
regulation review process. We’ll review any
proposed revisions to the hospital regulations
that are disseminated for public comment.
Through the medical society, physicians will
have stakeholder status to influence
department revisions of the regulations.
Department of Insurance
While fair contracting legislation has been
introduced to the General Assembly, our
regulatory advocates will pursue changes to
bring more fairness to managed care
contracting regulations. We also plan to
Medical liablity reform and McareFund legislation
The society continues to seek meaningful
reforms, including repeal of the medical
liability insurance mandate and limits on
lawyers’ contingency fees. We also seek a
permanent funding source for the Mcare
unfunded liability. And, we will continue to
advocate aggressively for a constitutional
amendment to permit caps on non-economic
damage awards.
In addition to legislation, the society is
developing mediation and other alternative
dispute resolution options as alternatives to
the current medical liability court system.
Fair managed care contracting
We have written and introduced a bill to
promote fairness in managed care contracting
to enhance Pennsylvania’s practice environ-
ment.
Scope of practice
Non-physician allied health practitioners
routinely seek to expand their scope of
practice, often beyond their training and skills.
In 2005 the society will continue to oppose
inappropriate expansion of other medical
professionals’ scope of practice.
Certificate of need
Ambulatory surgery centers, cardiac
catheterization laboratories and other high
technology services could be detrimentally
affected if certificate of need (CON) laws are
reinstated. The society will oppose efforts to
limit access to these growing health care
services.
Workers’ compensation reform
Workers’ compensation reimbursement
includes a required annual fee update. The
society will oppose efforts to make changes
that unfairly target physician compensation.

266 u The Bulletin June 2005
THOUGHTS FROM
OUR MEDICAL EDITOR
Morals, Social Norms andthe Practice of MedicineSAFDAR I. CHAUDHARY, MD
This beautiful and amazing earthhas many facets of expressions.
The geographical landscape changesas we travel around the globe.Traveling to places of comfort andamazing nature brings diversity toour thinking. We enjoy nature andits display of grandeur with humilityand loving care. Taking pictures inour digital minds and sharing storiesof new experiences with our friendsand families is a joyful reminiscentexperience.
As the nature of landscapechanges during any travel from hillsto meadows, pasture lands to ruggedterrains, sand dunes with cactussurviving brutal sun to lush valleys offruit-laden trees with pleasantbreezes, so do the cultures andpeople living in these landscapesdiffer. People adopt cultures andpractices that conform to the moralsand norms acceptable to them.Nations not only adopt laws thatfoster certain thinking as the “rightpractices,” but each nation strugglesto integrate various subcultures todevelop a consensus on issues ofcontention and disagreement.
So goes the lives of societies overthe course of history, the nationsthat bring advancement in theunderstanding of nature with healingand the art of care seem to leave apositive imprint on the history of
humanity. Wars and destructionleave scars on the face of the earth,in people’s psyches and in historybooks. Memorials to death anddestruction are rather somber placesto visit; whereas discoveries of newterrains in the field of medicine, artand our universe bring excitementand joy.
In all times, mankind lives invarious societies that can foster ahealthy mix of morals, tolerateindividual practices and understand-ings and encourage growth ofscience, which is to understandnature without fear of morals.Societies can also choose to becomehostage of their own rigid moralsand decay without observing excit-ing discoveries of their own sur-roundings. Defining “right fromwrong” is often based on religiousmorals of each society. Some issuescan become matters of passion andobsessional political discussions. Inrecent months we lived through theemotional struggles of a family inFlorida, struggling with issues ofdeath, dignity and what might bethe “right thing to do” for a womanin a state of coma. Interpretation of“righteousness” with various moralswas the centerpiece of this discus-sion. This matter of health andsocietal morals had a significantimpact on our legislature and health
providers and sparked nationaldiscussion.
Interestingly, the morals of anysociety when reviewed in depth areas diverse as are the fingerprints ofeach individual. Our interpretationof any “teaching” can be as diverseand unique as our personalities.Being in the field of psychiatry, Ifind it amazing how we all are sounique; there is no one like us everborn nor will there be. This in itselfwas an amazing discovery for me,that we all—having a face, arms,body, legs and essentially similarbasic ingredients of a persona—canbe so distinct. So are our individualthinking and morals on any mattersthat affect us. Even identical twinshave distinct personalities, eventhough they come from the appar-ently same exact genetic makeup.Dolly the sheep’s clone was not quitethe same either.
Having to establish our uniqueidentity does not seem that hard of apoint to argue with. Our minds arelike a container—so unique to eachone of us that when we pour infor-mation and knowledge in it, it takesit own unique “righteousnessshape”—no different than pouringwater into a glass. The “right thing”to do in any matter then is subject toan individual’s interpretation of howwe see the world through lenses of

The Bulletin u 267June 2005
The opinion expressed in this columnis that of the writer and does notnecessarily reflect the opinion of theEditorial Board, the Bulletin, or theAllegheny County Medical Society.
our minds. Our morals also continueto evolve, as do the shades of ourhair and the shape of our eyeglasses.
The famous scientist GalileoGalilei in Italy, one night in 1609,turned his telescope to the heavenand changed astronomy forever.Telescopes revealed informationabout the celestial entities that noone had previously imagined. Sincethen, astronomershave usedtelescopes tostudy everythingfrom our moonto comets, starclusters and distantgalaxies. It is joyful to understandthe beauties and mysteries of ouruniverse. At one time, however, thesediscoveries by this now famousscientist were not acceptable to themorals of that society. In 1616,during the interval between thepublication of the second and thirdeditions of Nueva Filosofía, GalileoGalilei (1564-1642) was officiallywarned by the Inquisition—and
later reprimanded by Rome—onthe subject of the Copernicanheliocentrism.
Emphasis must be placed ondeveloping the intellectual skills tounderstand nature, and therebyadvance science in the interest of thecommon people. A spiral of birth,growth, maturation, decline anddeath characterizes human nature.Philosophy of medicine is groundedin the avoidance of unnecessarydisease, the living of a normal,healthy life and reaching a peaceful,natural death.
We need to establish the moraland metaphysical foundations forthe knowledge of human nature.The practice of medicine ought tofocus on preventing disease anddisability and planning holistictreatments with particular under-standing of psychology contributingto human and animal susceptibilityto disease and death. The ability todiscuss and understand without fear,human sexuality, women’s health,epidemiology, psychotherapy and
our universe ought to be fosteredand protected from unnecessarypolitical and religious passions thatcan hinder our understandings ofnature to prevent sufferings. Thematters of health care can be best leftto those who are experts in theirrespective domains. The pairs oflenses with ability to focus on nearand far may best serve us now and infuture. Galileo paved the way for thecurrent “Hubble telescope” andunderstanding of earth’s positioningin our solar system against themorals of his days. Maybe we canlearn some lessons from our ownhistory.
Dr. Chaudhary is a psychiatrist and medicaleditor of the Bulletin. He can be reached [email protected] or (412) 427-6828.
REFERENCE
www.exploratorium.edu/.../ tools/before.html
GE’s #1 Distributor for 100% Windows-based,
Award Winning Practice Management and
Electronic Medical Records SystemsRanked #3 of the region’s fastest growing
companies within the Healthcare Industry
Penn Center West
Building III, Suite 320
Pittsburgh, PA 15276
1-888-950-0688
www.virtualofficeware.net
MEDICAL
EDITOR continued

268 u The Bulletin June 2005
How Electronic Health RecordsMay Change Health Care
EDITORIAL
INDIRA P. JEVAJI, MD
President Bush has a vision toimprove America’s health care
system and is committed to his goalof assuring that most Americanshave electronic health records withinthe next 10 years.1 By 2010, thevision is to transform health carefrom an organization-centric modelto a consumer-centric model. Eventhough the president estimates a 20percent reduction in the cost ofhealth care as a result of informationtechnology,2 implementing an EHRis expensive and may increase thecost of health care.
Currently, most health careproviders have a paper medicalrecord on a single patient. Paperrecords cause fragmentation ofhealth care and compromise healthcare quality. Additionally, it increasesthe expense of health care deliverythrough duplication of tests. How-ever, an EHR is a longitudi-nal collection of electronichealth information.3
Preferably, EHRs shouldhave the capability for allproviders participating in thecare of a patient in multiplesettings to quickly access keyinformation—such as pa-tients’ diagnoses, allergies, labtest results and old and newmedications—that would
improve the caregivers’ ability tomake sound clinical decisions in atimely manner and would increasepatient safety and the effectiveness ofcare.4 In addition, EHR empowerspatients to access their healthrecords, provides interactive patienteducation, and helps them carry outhome monitoring and self-testingwhich can improve control ofchronic conditions such as diabetes.5
Payment for EHRConversion to an EHR is expen-
sive. Stand alone EHR (for a singleoffice) ranges from $15,000-$35,000or more per physician6 for initialimplementation. Additionally, thecost of training and regular upgradesfor stand-alone EHR substantiallyincreases practice overhead. At atime when providers are beingsqueezed on payments, should theybe required to bear this expense?
Various suggestions have beenmade to provide incentives forphysicians to adopt EHRs. TheNational Health Information Infra-structure (NHII) suggests the use ofnew codes or modifiers added on tothe current Medicare physician feeschedule.7 Would these include newcodes for ongoing upgrades andtraining after initial implementation?Who pays for non-Medicare patientsand specialists such as pediatriciansand obstetricians/gynecology andothers who do not provide care forMedicare patients? Should privateinsurance companies pay for EHRimplementation by adopting Medi-care codes? After all, they would alsobenefit from the technologicaladvances EHR provides such asaccess to processing claims andelectronic utilization reviews.
One of the key capabilities of anEHR is patient access to “personal
health records.” With aclick, the patient has imme-diate access and the abilityto review his or her healthrecords, not only from aprimary care provider butalso notes from specialistlabs and radiology reportsand other data from acrossthe spectrum of health careproviders. Furthermore,
phot
o by
Don
ald
E. F
ette
rolf,
MD

The Bulletin u 269June 2005
EDITORIAL continued
patients would benefit from EHRcapability of providing interactivepatient education and home healthmonitoring that traditionally wouldbe done in an office.8 Moreover, thisallows patients to partner in theirhealth care decisions—empoweringthem to determine and make anindividualized pathway to theirhealth. In addition to receivingmedical advice, it saves time com-muting and is convenient andaccessible despite weather condi-tions. Should the physicians beallowed to bill the patient for thisextra service? On a flat surcharge forevery patient visit? Or a per-click orper-minute basis?
EHR would improve caregivers’ability to make sound clinicaldecisions in a timely manner andwould increase patient safety and theeffectiveness of care.9 Medicationerror detection and the use ofclinical practice guidelines willimprove safety and quality resultingin better patient satisfaction. This,coupled with the partnership in
decision making it develops, has apotential to decrease medical liabil-ity. Should insurance companiesphase in a discount on malpracticepremiums for physicians implement-ing EHRs? Should patients have anoption to comply with arbitrationand mediation and waive a jury trailin exchange for the benefits andservice of EHR? The reduction inmalpractice premiums and thesavings attained will transfer intoimplementation and maintenance,training and upgrading the system.
Ownership and Retention ofMedical Records
Medical records are an integralpart of a medical practice. A practiceconsiders medical records that areaccurate and complete a significantasset. Typically, the value of a newrecord is $12-$20.10 Depending onthe size of the practice and theduration of the practice’s operation,the number of medical recordsconfers a considerable value to themedical practice. As an owner of themedical record, the practice is alsoresponsible for retaining the medicalrecord for a period depending onstate laws and professional standards.
In Pennsylvania, a physician shallretain a patient’s medical record forat least seven years from the date ofthe last medical service for which amedical record entry is required. Themedical record for a minor patientshall be retained until one year afterthe minor patient reaches majority,even if this means that the physicianretains the record for a period of
continued on page 270
Preferably, EHRs
should have the
capability for all
providers participating
in the care of a patient
in multiple settings to
quickly access key
information.

270 u The Bulletin June 2005
The opinion expressed in this columnis that of the writer and does notnecessarily reflect the opinion of theEditorial Board, the Bulletin, or theAllegheny County Medical Society.
Dr. Jevaji is a pediatrician and associateeditor of the ACMS Bulletin. Dr. Jevaji alsohas a master’s degree in the study of law. Shecan be reached at [email protected].
more than seven years.11 The practiceis also responsible for keeping theinformation confidential so that onlythe patient or patient designees haveaccess to their medical records.Patients are charged a reasonableamount for the cost of copyingmedical records when necessary.12
An ideal EHR is portable; i.e., ithas the ability to access and movepatient information from one pointof care to another.13 Stand-aloneEHRs convert a physician’s officefrom paper to electronic filing.However, they are “islands of datawhere patient information does notflow seamlessly from one clinicalsetting to the next.”14 Therefore, anEHR should be interoperable so thatelectronic exchange of patientinformation is easily available acrossthe nation.15 In order for the EHRto be interoperable and portable,there should be a database to se-curely store data that is electronicallyaccessible through a portal to thoseinvolved with providing care in theircommunity. These databases, coined“Regional Health InformationOrganizations” (RHIOs) requirecollaboration among physicians andhealth care entities in a commu-nity.16 Interconnecting each RHIOwill require an infrastructure knownas a National Health InformationNetwork (NHIN) to facilitateinteroperability between RHIOs.This will allow medical informationto travel anywhere with patients,thus revolutionizing the industry bymaking information more con-sumer-centric.17
However, with EHR the infor-mation is stored in databases, whichare accessible to any health careprovider, insurance company, the
patient, or his designees followingauthorization. The practice losescontrol over the information ormedical records and loses thecapacity to “own the record” whichis now no longer considered to be anasset. Since there are multipleproviders and users of the electronicsystem, who is responsible to paythe fees incurred for accessing orstoring information? Who is respon-sible for retaining the records so thatthey comply with the state laws andwho pays the cost of retention? Whois responsible for the security andprivacy of personal health records?Do we have laws in place that waiveliability on physicians when securityor privacy breach occurs by theentity owning the databases?
An EHR for a physician practicehas many advantages. It can improveclinical care, provide access toimportant lab information, reducemedical errors and decrease adminis-trative hassles to mention a few. Itimproves medical care, safety andsupport to the patient and reducesmedical errors. With an EHR,however, ownership and assetconferred by a paper medical recordis lost. Once the information istransmitted from the physicians’offices into databases, multiple users(and owners) come into play.
Multiple users must have mul-tiple payers. The federal and stategovernment, the private health careand malpractice insurance compa-nies, providers of health care and thepatients should all be a part of thepayers. Suggestions such as includ-ing the use of tax credits, alteringevaluation and management codeswith the use of modifiers, reformingmedical malpractice and antitrust
EDITORIAL continued from page 269
laws, and incorporating a surchargeon every patient visit for EHRimplementation, training andupgrades are worth considering.Transformation of health caredelivery from an organization-centric model to a consumer-centricmodel needs a revamping of thepayers system—from insurance toconsumer payers.
REFERENCES
1http://www.whitehouse.gov/news/releases/2005/01/20050127-2.html
2http://www.whitehouse.gov/news/releases/2005/01/20050127-7.html
3http://books.nap.edu/books/NI000427/html/1.html#pagetop
4see core capabilities of an EHR at http://books.nap.edu/books/NI000427/html/1.html#pagetop
5see core capabilities of an EHR at http://books.nap.edu/books/NI000427/html/1.html#pagetop
6http://www.physiciansnews.com/cover/505.html
7http://www.hsrnet.net/nhii/materials/strategic_framework.pdf page 28.
8http://books.nap.edu/books/NI000427/html/1.html#pagetop
9see core capabilities of an EHR at Seehttp://books.nap.edu/books/NI000427/html/1.html#pagetop
10http://www.irs.gov/pub/irs-tege/eotopicq96.pdf
11http://www.pacode.com/secure/data/049/chapter16/s16.95.html
12http://www.pacode.com/secure/data/028/chapter563/chap563toc.html
13-17http://www.os.dhhs.gov/healthit/goals.html.

The Bulletin u 271June 2005

272 u The Bulletin June 2005
MATTHEW NEAL
What You Won’t Find inthe Syllabus
GETTING THERE:MUSINGS OF A MEDICAL STUDENT
On the very first day of myemergency medicine rotation,
a young patient presented with anklepain following a fall. Having justfinished an elective in sports medi-cine, I was eager to demonstrate myunderstanding of the management ofjoint injuries and, I’ll admit, keen onimpressing my attending. Aftertaking a history and examining thepatient, I presented the case.
Subtlety not being my bestquality, I confidently argued that thepatient did not meet the criteria forimaging set forth by the OttawaAnkle Rules, and I suggested aconservative management plan thatdid not include any imaging stud-ies.1 We subsequently examined thepatient together, and my attending,likely concealing his amusementwith my pretentious display, agreedwith my conclusions. As we left theroom, my pride took a blow as theattending told the nurse that wewould get ankle films before thepatient could leave. Sensing mybewilderment, he assured me that
X-rays were probably not necessary,and he then uttered a statement thathas become disgustingly familiar: “Ijust don’t want to get sued.”
Sometimes it is exceptionallydifficult to identify reality in medicalschool. My guess is that a majorityof the most senior physicians haveonly seen one case of FamilialMediterranean fever and that caselikely appeared as a vignette on theUSMLE. We spend time studyingrare diseases that we are not likely tosee in practice to help us to under-stand general physiology and pathol-ogy. In our current education, welearn evidence-based models forapproaching patient care; we learnhow to be efficiently effective
healers. Our ignorance to reality isbliss in other realms of medicine; weenjoy patient care without beingsubjected to the tortures of insur-ance, billing or managed care.However, from a medical student’sperspective, I can tell you that it hasbecome impossible to ignore theeffects of one particular area onpatient care: the medical liabilityinsurance crisis.
Although I would like to thinkthat I retain that naïve ambition thatled me to this career, my currentperspective is very different fromthat of just three short years ago.When I came to medical school, myfocus was on learning to be the verybest healer, educator and advocatefor my patients. Many experienceshave served to reaffirm my decisionto enter this profession. I have seenthe passion for caring in my teachersas they connect with patients; I havemarveled at the wonders of medicineas a science and as an art; and I havebeen humbled by the awesomeresponsibility of being a physician.These are the tenants of medicinewhich have defined the professionsince antiquity; the difference, in ourcurrent era, is that these interactions
1Stiell IG, Greenbert GH, McKnight RD, Nair RD,McDowell F, Worthington JR. A study to developclinical decision rules for the use of radiographyin acute ankle injuries. Ann Emerg Med 1992,Apr; (21):394-90.

The Bulletin u 273June 2005
The opinion expressed in this columnis that of the writer and does notnecessarily reflect the opinion of theEditorial Board, the Bulletin, or theAllegheny County Medical Society.
often occur across a proverbial“battlefield.” The new face of medi-cine, that which is defined in part bypractice in a caustic, litigious envi-ronment, is the only face of medi-cine known to current trainees. As astudent, I hear my preceptors discusstheir frustrations with the system.Frivolous lawsuits and excessiveawards abound. I hear discussionsabout patient care punctuated bylegal concerns. I watch my col-leagues in residency accept jobs instates that have enacted liabilityinsurance reform. Unnecessary testsare ordered to “cover” the legal bases;“CYA” might arguably have becomeone of the most prevalent medicalabbreviations. Physicians alter theirpractices or leave, services at smallerhospitals are abandoned and, mosttragically, quality of care is compro-mised. All of these issues are pre-sented side by side with pathologyand physiology to the ever-impres-sionable minds of medical students.
Oftentimes, the focus surround-ing the medical liability insurancereform debate is only on the present.Mcare abatements are lauded asprogress by some, while others lobbyfor more concrete solutions toaddress a broken system. Regardlessof the debate, the immediacy of theissue is always raised. Although theattempt at immediate reform isabsolutely necessary, I think that theimpact of this issue upon futuregenerations is often neglected.Pennsylvania’s current shortage ofyoung physicians may seem bleak,but the forecast is likely even moregrim. Without significant changes,those of us educated in this environ-ment are not likely to be enticed tostay. With daily mounting debt, this
budding surgeon will certainly beconsidering the liability insurancecosts when choosing a location topractice, not to mention the fact thatno one wants to work in a placewhere they are not made to feelwanted. When the Pennsylvanialegislature fails to enact strongreforms on this issue, this is exactlythe message it conveys.
Recognize, too, the effects of thisissue on the health care system as awhole. Current health care costs aresoaring in a generation of practitio-ners not educated by defensivemedicine. The overall burden ofdefensive medicine is difficult toascertain, but the exposure of currenttrainees and access to evolving,expensive technology available formedical tests will make it impossibleto ignore in the near future. Run-ning extra tests to cover legal bases isan expensive and a dangerouspractice for our patients, yet thecurrent legal environment makes itdifficult to avoid. Defensive medi-cine and evidence-based medicinecan, at times, be mutually exclusive.As a medical student, I am beingtaught both. The choice that I andother students make between thesetwo in our future practices will drivenot only the health care bottom linebut the quality of care delivered toour patients.
Medical students have not beensilent on this issue. Last year, a group
of us circulated a letter that gatheredmore than 1,200 signatures ofmedical students across the state. Inthis letter, we expressed our concernfor the effect of the medical malprac-tice insurance crisis on our patients.We sent this letter to the entirePennsylvania Senate and to thegovernor; in a personal meeting withGovernor Rendell, we warned himthat, without significant reforms,Pennsylvania would not be able tocontinue to recruit or retain youngphysicians. Unfortunately, thePennsylvania legislature did notapprove the bill that would haveenacted a cap on non-economicdamages and would have providedsubstantial relief to Pennsylvaniaphysicians and their patients. Thiswas not an effective recruitment toolfor a state with a rising shortage ofyoung doctors. It is time for reform.Our patients deserve it.
I will graduate in a year with thegoal of becoming the best healer andadvocate that I can be for my pa-tients. I attend a fantastic medicalschool, arguably one of the best, andthe curriculum will prepare me wellfor my practice; however, the realityof modern medicine has also beenpart of my training. The next time Isee a patient with an ankle injury inthe ER, I’ll have a tough decision tomake.
Mr. Neal is a fourth-year medical student atthe University of Pittsburgh School ofMedicine. He can be reached at [email protected].
Defensive medicine and
evidence-based
medicine can, at times,
be mutually exclusive.
MUSINGS continued

274 u The Bulletin June 2005
SOCIETY NEWS
Urologists to meet in JuneThe Pittsburgh Urological Associa-tion will host a meeting on June 20at Morton’s, 625 Liberty Avenue inPittsburgh. Registration beginspromptly at 6 p.m., followed bydinner and program at 6:40 p.m.James M. McKiernan, MD, invitedguest speaker, will talk on Contempo-rary Management of Renal CorticalTumors—A Tale of Two Evolutions.Dr. McKiernan, who is the recipientof numerous honors and awards, isassistant professor of urology atColumbia University College ofPhysicians and Surgeons in NewYork City. His research interestsinclude the characterization andtreatment of high-risk urologicmalignancies; he has authored andco-authored more than 70 articles,book chapters and abstracts.Registration is required for thismeeting; contact Nadine Popovich at(412) 321-5030 or [email protected].
Coding camp here in AugustThe Pennsylvania Medical Society’sannual day-long coding camp isscheduled for August 11 at themedical society headquarters. Thesession is geared to all physicians,administrators and office staff andyields up to 7.5 hours of CME/CEU. Cost is $189 for PMS mem-bers, $169 for front line practice andsecond attendees, and $489 forpotential members. Class size islimited, so register early atwww.pamedsoc.org/shop or call(877) 228-7823.
Physicians needed for health fairThe ACMS is seeking physicians toparticipate in the 2005 Healthy 4Life Expo, scheduled for August 27at the David L. Lawrence Conven-tion Center. Physicians from a rangeof specialties, especially familypractice, internal medicine, derma-tology and ophthalmology, areneeded to provide information andinformal consultations at the Ask the
Doctor booth. (Physicians will not beproviding examinations.)
Healthy 4 Life sponsor, WTAE-TV, will advertise the medicalsociety’s involvement prior to theevent, including the hours whenphysicians will be on hand forconsultations. Approximately 8,000people are expected to attend theone-day interactive event. For moreinformation or to sign up, callChristina Morton at (412) 321-5030 or e-mail [email protected].
Ob/Gyn society meeting heldDr. Eric J. Bieber, chair of theDepartment of Obstetrics & Gyne-cology at the Geisinger MedicalCenter spoke to the members of thePittsburgh Obstetrical & Gynecol-ogy Society at its May 2 meeting onMedical Approach to ManagingAbnormal Uterine Bleeding.The society elected Patrick T.Christy, MD, as its new president tofollow Saul R. Berg, MD; John P.Barrett, MD, took over as president-
Sandra DaCosta, president of the ACMS Alliance speaks to avisitor to the ninth annual Senior Expo sponsored by Pa. SenatorJane Claire Orie. ACMS and the alliance participated in the eventheld on May 13 at the Community College of Allegheny CountyNorth Campus.
William H. Maruca, Esq., speaks to a gathering of medicalstudents and residents at the University of Pittsburgh MedicalCenter on the ins and outs of contracts and negotiations, at amedical society-sponsored session on May 17. Mr. Maruca is apartner with the Pittsburgh office of Fox Rothschild LLP.

The Bulletin u 275June 2005
elect; and Pierce Soffronoff, MD,will continue as secretary/treasurer.
The society’s next meeting willbe held on October 3. A completecalendar of meetings will be mailedto members during the summermonths and will also be availablethrough a link from the medicalsociety’s website, www.acms.org.
Surgeons travel to West VirginiaColin Knight, MD (AlleghenyGeneral Hospital), and John M.Robinson, MD (Mercy Hospital),were selected from among theresidents who presented abstracts atthe January meeting of the Pitts-burgh Surgical Society to attend ajoint meeting of the SW Pennsylva-nia and West Virginia chapters of theAmerican College of Surgeons inearly May.
Also representing the SW Padistrict at the meeting were Laurel A.Omert (formerly of AGH), whopresented Advances in Surgical Care,Tom E. Read (West Penn Hospital),who presented Controversies in RectalCancer Treatment, and Kurt R.Stahlfeld, MD, (Mercy), who pre-
sented The (F)utility of Mammogra-phy and an ACOSOG Update. continued on page 276
Health Insurance Renewal Rates Swing Wide
The annual renewal of Allegheny County Medical Society Health Insurance Programs
takes place on July 5. This year, as in years past, several program changes have
occurred, none of which have had a more serious impact than the change in how
Highmark Blue Cross now demographically rates individual groups within the society’s
programs.
The use of demographic rating is not new within the ACMS health insurance programs.
Highmark has used this rating process for the last several renewals. This year, however,
Highmark included two new demographic factors in the pricing process that impact the
individual group rates, adding age and gender to geographic location, client size and
industry classification. The use of this pricing method has produced a “good news/bad
news” scenario for those members who participate in the ACMS health insurance
programs.
The 2005 renewal premium changes range from a decrease of 25.9 percent to an
astounding increase of 79.5 percent. For the first time in several years, some ACMS
member groups realized a decrease in medical insurance premiums. Premiums for
almost half of the groups (46%) increased by nine percent or less. On the other hand,
42 percent of the insureds participating in these plans saw a premium increase of 21
percent. A smaller group (10.5%) are trying to deal with an increase of 40 percent or
more.
Although the ACMS realizes that some of you are very happy with the renewal rates you
received this year, we know that many of you are disappointed, upset and angry with the
high cost of health care insurance. We ask those of you who are not satisfied with your
current health insurance plan call USI Colburn and explore your alternatives. The ACMS-
sponsored program has more than 19 different plans including qualified and non-qualified
High Deductible Health Plans (HDHP), requires no medical underwriting, and accepts
groups of one that meet the Highmark participation guidelines. USI Colburn can help you
review your medical insurance needs and offer suggestions as which plans and/or
carriers might best fit your needs. Its representatives can be reached at (800) 327-1550.
Resident doctors John Robinson (left),MD, and Colin Knight, MD, pause for amusical moment at a May meeting of theAmerican College of Surgeons.
Pittsburgh Surgical Society President DanJ. Gagne, MD (left), bestows an honorarylifetime membership on guest speakerMichel Gagner, MD, at the society’s May17 meeting.
Surgical Society meetsMichel Gagner, MD, of the WeillCollege of Medicine at CornellUniversity was featured guest speakerat the May 17 meeting of the Pitts-burgh Surgical Society, speaking onLaparoscopic Adrenalectomy: the GoldStandard. Society President Dan J.Gagne, MD, presented him with anhonorary lifetime membership.The society will meet again onNovember 8 when Dr. Timothy R.Billiar will speak on The Future ofGeneral Surgery as a Profession. Dr.Billiar is the George Vance FosterProfessor and chair of the depart-ment of surgery at the University of
SOCIETY NEWS continued

276 u The Bulletin June 2005
SOCIETY NEWS continued from page 275
Pittsburgh Medical Center. Detailswill be mailed directly to membersand will be available through a linkon the medical society’s website atwww.acms.org.
ACMS calls for nominationsThe medical society’s NominatingCommittee is seeking candidates forthe ACMS Board of Directors andother elected offices, includingdelegates to the Pennsylvania Medi-cal Society. The committee is alsolooking for individuals interested inserving on the following ACMScommittees: Child Health, Commu-nications, Legislative, Membership,and Occupational Medicine, as wellas the Bulletin Editorial and PeerReview boards.
The need for physician leader-ship cannot be overstated during thistime of change in the medicalprofession. All appointments aredesigned to maximize expertise andkeep time commitments to anefficient minimum. Please respondby July 15. Nomination forms areavailable for download at www.acms.org. For more information, callDottie Hostovich at (412) 321-5030.
Medical ’biz in the ’BurghNearly $3 of every $100 spent onpatient care in Pa. hospitals goestoward the cost of malpracticeinsurance according to a reportreleased by the Pennsylvania HealthCare Cost Containment Council.The 182 general acute care hospitals
in the state spent $636 million onmalpractice insurance costs duringfiscal 2004, while malpracticeexpenses as a percent of net patientrevenue during fiscal 2004 averaged2.67 percent for hospitals across Pa.Philadelphia lived up to its litigiousreputation, with hospitals in thatcounty spending 3.95 percent of netpatient revenue on malpractice costs;the figure was only 1.6 percent athospitals in the eight counties in thesouthwest corner of the state, mak-ing Pittsburgh the lowest-cost regionin the state. During fiscal 2004,hospitals subsidized the malpracticeexpenses for 5,289 physicians andmedical staff at a total cost of $37.4million, or $7,077 per doctor.
(5/3/05 Pittsburgh Post-Gazette)

The Bulletin u 277June 2005
FROM THE
MAILBAG
May 23, 2005
Melinda (Campopiano, MD),
Good article in the ACMS Bulletin(May 2005, pg. 251, “Consideringthe Move to Electronic MedicalRecords”). I agreed with all you said.Look forward to seeing you at thenext ACMS board meeting.
Best Wishes, Doug Clough, MD
May 23, 2005
To the Editor:
I was very pleased to see Dr. MelindaCampopiano’s article on her decisionto seek out an Open Source elec-tronic medical records system. OpenSource software is exactly the rightchoice for mission-critical applica-tions like EMR, because it guaran-tees that the physician will not beleft at the mercy of the softwarevendor for support or modifications.I hope you will continue to featurearticles from Dr. Campopiano as sheimplements her system—I amconfident that they will highlight thewisdom of her choice!
Alik Widge, Chair-ElectMedical Student SectionAmerican Medical Association
Mike Danoff, MD,cardiovasculardisease, discussedmetabolic syndrome.He wrote thatmetabolic syndromeconsists of at least
three of five elements and can becontrolled with exercise and diet. Insome cases medication may be used.
Joseph Paviglianiti,MD, ophthalmology,wrote about eyesafety for childrenwho are active insports. He wrote thatall children playing
sports should wear eye protectionapproved for their particular sportduring all practices and competi-tions. Children who wear glassesshould also wear eye protectionbecause the frames in glasses canbreak easily and are not protective.
Dr. Danoff
Dr. Paviglianiti
The Dear Doctor column ispublished regularly in thePittsburgh Post-Gazette’sHealth Section. To contribute a Dear Doctorcolumn, call Elizabeth Fulton at (412) 321-5030 or e-mail [email protected].
DEAR
DOCTOR Telecom Audits Saveyou Money!!
(Have you had a
check up lately?)
Telecom Audits help recover
incorrect billing dollars and
lower future billing expenses.
It would be selfish of me to keep myexperience with A to Z Communications asecret! …They are not only knowledgeableand experienced, but only charge you ifthey find and correct problems. … Duringthe first year, we will realize a cost savingsof over $23,000.00!” Linda Chufe,
Manager; Bell, Froman, Orsini and
Associates
The process to manage, reduce andcontrol communication expenses isenormously overwhelming for most officemanagers. Their monthly billing statementsare difficult to read, and often close toimpossible to audit. The simple factremains that these expenses (literallythousands of dollars monthly) are paid “asis”. Telecom providers have a vestedinterest in the status quo. If the averageperson could read and comprehend the bill,most providers would experience adecrease in revenues from the exposure ofhidden fees, rate changes and additionalcharges.
Most business mangers do not have thetime to wait on hold to speak to customerservice representatives in order to clarify ordispute questionable charges on eachseparate bill. Statistics show that compa-nies are spending 25 to 50% more thanthey should for their telecommunications.
Allow us the opportunity to help you reduceyour telecommunications cost. We willcharge you nothing if we do not findsavings.
Professional Audit and Management ofBusiness communications
Impartial - Advisors - Ethical - Thorough - Hard Working
A to Z Communications Management
Linda Paonessa Christine McColpin
412-303-0189
DO YOU VOLUNTEER?The Bulletin is compiling a list of volunteeropportunities in the area that retired physicians maywant to explore. If you have suggestions for the list—which will appear in the August Bulletin—please callLinda Smith, Bulletin managing editor at 412-321-5030, ext. 105 or e-mail [email protected].
278 u The Bulletin June 2005
Send your Activities & Accolades to ElizabethFulton at ACMS, 713 Ridge Ave., Pittsburgh,PA 15212 or e-mail [email protected]. Pleasesend a recent photograph indicating whether ornot it needs to be returned.
ACTIVITIES &ACCOLADES
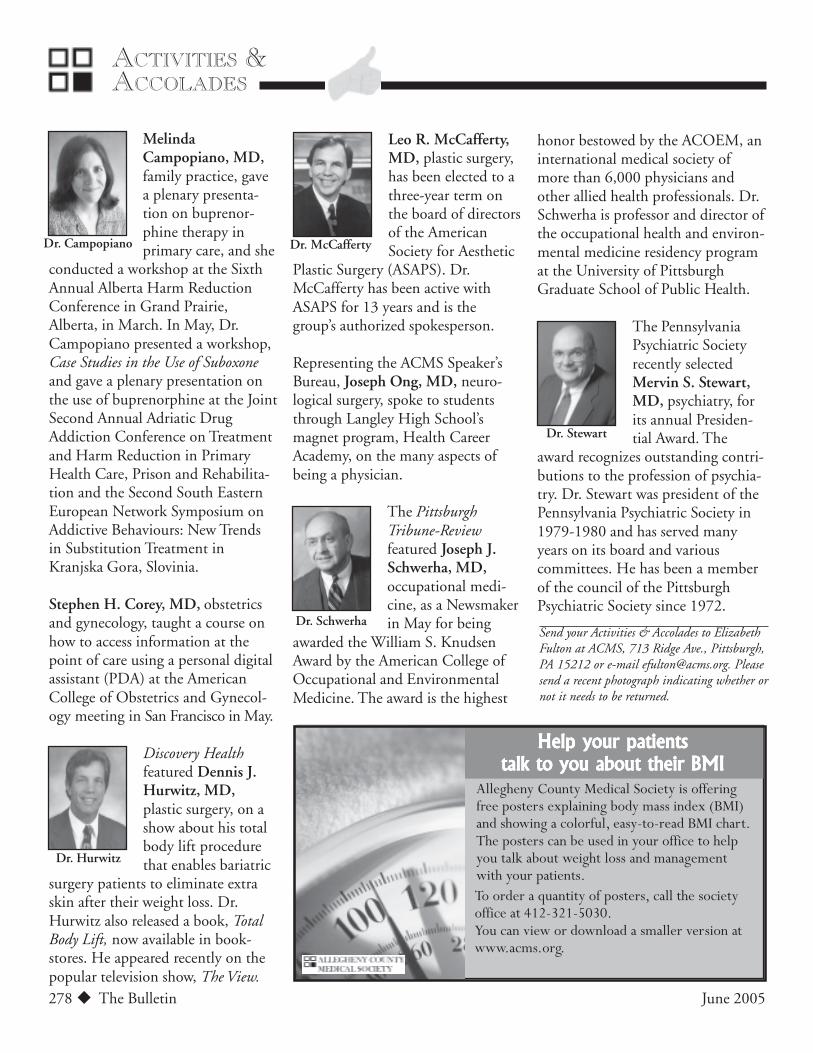
Dr. Campopiano
Dr. Hurwitz
Dr. McCafferty
Dr. Schwerha
Dr. Stewart
MelindaCampopiano, MD,family practice, gavea plenary presenta-tion on buprenor-phine therapy inprimary care, and she
conducted a workshop at the SixthAnnual Alberta Harm ReductionConference in Grand Prairie,Alberta, in March. In May, Dr.Campopiano presented a workshop,Case Studies in the Use of Suboxoneand gave a plenary presentation onthe use of buprenorphine at the JointSecond Annual Adriatic DrugAddiction Conference on Treatmentand Harm Reduction in PrimaryHealth Care, Prison and Rehabilita-tion and the Second South EasternEuropean Network Symposium onAddictive Behaviours: New Trendsin Substitution Treatment inKranjska Gora, Slovinia.
Stephen H. Corey, MD, obstetricsand gynecology, taught a course onhow to access information at thepoint of care using a personal digitalassistant (PDA) at the AmericanCollege of Obstetrics and Gynecol-ogy meeting in San Francisco in May.
Discovery Healthfeatured Dennis J.Hurwitz, MD,plastic surgery, on ashow about his totalbody lift procedurethat enables bariatric
surgery patients to eliminate extraskin after their weight loss. Dr.Hurwitz also released a book, TotalBody Lift, now available in book-stores. He appeared recently on thepopular television show, The View.
Leo R. McCafferty,MD, plastic surgery,has been elected to athree-year term onthe board of directorsof the AmericanSociety for Aesthetic
Plastic Surgery (ASAPS). Dr.McCafferty has been active withASAPS for 13 years and is thegroup’s authorized spokesperson.
Representing the ACMS Speaker’sBureau, Joseph Ong, MD, neuro-logical surgery, spoke to studentsthrough Langley High School’smagnet program, Health CareerAcademy, on the many aspects ofbeing a physician.
The PittsburghTribune-Reviewfeatured Joseph J.Schwerha, MD,occupational medi-cine, as a Newsmakerin May for being
awarded the William S. KnudsenAward by the American College ofOccupational and EnvironmentalMedicine. The award is the highest
honor bestowed by the ACOEM, aninternational medical society ofmore than 6,000 physicians andother allied health professionals. Dr.Schwerha is professor and director ofthe occupational health and environ-mental medicine residency programat the University of PittsburghGraduate School of Public Health.
The PennsylvaniaPsychiatric Societyrecently selectedMervin S. Stewart,MD, psychiatry, forits annual Presiden-tial Award. The
award recognizes outstanding contri-butions to the profession of psychia-try. Dr. Stewart was president of thePennsylvania Psychiatric Society in1979-1980 and has served manyyears on its board and variouscommittees. He has been a memberof the council of the PittsburghPsychiatric Society since 1972.
Help your patientsHelp your patientsHelp your patientsHelp your patientsHelp your patientstalk to you about their BMItalk to you about their BMItalk to you about their BMItalk to you about their BMItalk to you about their BMI
Allegheny County Medical Society is offeringfree posters explaining body mass index (BMI)and showing a colorful, easy-to-read BMI chart.The posters can be used in your office to helpyou talk about weight loss and managementwith your patients.To order a quantity of posters, call the societyoffice at 412-321-5030.You can view or download a smaller version atwww.acms.org.

The Bulletin u 279June 2005
COMMUNITY NOTES
Ovarian cancer informationThe National Ovarian CancerCoalition (NOCC) is committed toimproving the overall survival rateand quality of life for women withovarian cancer. It is asking for yourhelp in pursuing early diagnosis bytalking with your patients aboutsymptoms and risks, placing infor-mational brochures in your waitingareas and sharing the NOCC contactinformation with patients who havebeen diagnosed with ovarian cancer.
The NOCC Pittsburgh Divisionconducts outreach and educationalactivities, as well as fund-raisingevents locally; it also supportsresearch and advocates for appropri-ate legislation. To request materials,call (412) 486-4952 or e-mail
pa.pitt.nocc@ovarian cancer. Foradditional information, log on towww.ovarianpgh.org.
Universal provider numbersAccording to the PennsylvaniaMedical Society, effective May 23,you can obtain a new universalprovider identifier number designedto improve efficiency by eliminatingthe need for multiple identifiersfrom different health plans.
You can use your new nationalprovider identifier (NPI) as soon asit is assigned; however, you may stillneed to supply your current providernumbers until May 23, 2007—thenational provider identifier compli-ance date—to transition and achievecompliance. After May 2007, you
Over 35 years experience representing physicians
in medical negligence cases. Fellow, American College of Trial
Lawyers; and member of Federation of Defense and Corporate
Counsel and of the Academy of Trial Lawyers of Southwestern Pa.
• Do you have claims against you for punitive dam-
ages or claims in excess of your insurance limits?
• Are you one of several defendants represented by
the same attorney?
• Do you want to settle your case, but your insurance
company does not?
• Does your insurance company want to settle your
case but you do not?
• Are you uncomfortable with your insurance com-
pany-appointed attorney?
ARE YOU A DEFENDANT
IN A MEDICAL MALPRACTICE CASE?
IF YOU ANSWER YES TO ANY OF THESE QUESTIONS,YOU NEED A SECOND OPINION FROM AN ATTORNEY
OF YOUR CHOOSING. CONTACT:William D. Phillips, Esquire
Phillips & Faldowski, PC
29 East Beau St. Washington, PA 15301
Telephone: 724-225-9933
Fax: 724-225-4712
E-Mail [email protected]
won’t be permitted to use your oldUPINs or numbers from Blue Crossand Blue Shield, CHAMPUS orMedicaid.
Small health plans have untilMay 23, 2008, to comply. After thatdeadline, the only number you’llneed to retain in addition to yourNPI would be your taxpayer identifi-cation number.
Be sure to check your currentbilling software to ensure it canaccommodate this new 10-digitidentifier, which will not containembedded information about theprovider and will never expire.
Check the CMS website atwww.cms.hhs.gov/hipaa/hipaa2 formore information on how to obtainan NPI application.

280 u The Bulletin June 2005
CONTINUING
EDUCATION
BEHAVIORAL HEALTH LEADERSHIP FORUM: RESEARCH, RESOURCES
AND RECOVERY—Sept. 16. Sponsor: Torrance State Hospital, etal. Chestnut Ridge Inn on the Green, Blairsville. CME category1 credits available. For information, contact Nora Carney at(724) 454-7647 or at [email protected].
VIDEOCONFERENCE SERIES. Sponsor: Western Psychiatric Institute& Clinic, et al. CME available. For information, log on towww.wpic.pitt.edu/oerp.
ONGOING CONTINUING EDUCATION PROGRAMS & CONFERENCES.Sponsor: Western Psychiatric Institute & Clinic, et al. CMEavailable. For information, call (412) 624-2523 or log on towww.wpic.pitt.edu/oerp.
ONGOING MENTAL ILLNESS & SUBSTANCE ABUSE (MISA) TRAIN-ING SERIES. Sponsor: Western Psychiatric Institute & Clinic, et al.CME available. For information, call (412) 605-1227 or [email protected].
This listing includes local events that are coming up soon; a morecomplete list is available on the medical society’s website atwww.acms.org or by calling (412) 321-5030.

The Bulletin u 281June 2005
June 27 is National HIV Testing Day, and July is
International Group B Strep Awareness Month.
(Source: U.S. Dept. of Health and Human Services).
JUNE/JULY
CALENDAR
PRACTICE
MANAGEMENT
HIPAA Q & AQ: What are the categories of HIPAA security
policies that were implemented in April 2005?
A: The HIPAA Security Rule has both required and addressable policies. Within those two
general categories are three sub-categories: technical,administrative and physicial security safeguards.Therefore, there are six categories of HIPAA Securitypolicies: required technical, required administrative,required physical, addressable technical, addressableadministrative and addressable physical.
Information for this column was provided by Joan M. Kiel, PhD,who serves as the university HIPAA compliance officer at DuquesneUniversity and is certified in health care privacy and security. Shecan be reached at (412) 396-4419. Submit your questions [email protected]. The column will publish answers to the mostfrequently asked questions; individual questions will not beanswered. Log on to the ACMS website (www.acms.org) forHIPAA events such as training for the new Security Rule.
June 19 .......................... ACMS Family Picnic
Kennywood Amusement Park
June 20, 6 pm ................ Pittsburgh Urological Association
July 4 .............................. Independence Day
ACMS Office Closed
July 11, 5:30 p.m. ........... Pittsburgh Regional Healthcare Initiative
School’s OutPlease
Drive Carefully

282 u The Bulletin June 2005
LEGAL REPORT
Biggest Mistakes—Credentialing CaseStudies
MICHAEL A. CASSIDY, ESQ
The case studies presented below illustrate thepoint made in a previous article, “The 10 BiggestMistakes Physicians Make in the Credentialing
Process” (Bulletin, February 2005, page 80).
1. The Cover-UpA physician was in the midst of the medical staff hear-ings at one hospital. The hospital had summarily sus-pended his privileges; the physician had requested andreceived a medical staff hearing; the medical staff hearingpanel upheld the suspension; and the physician ap-pealed. During this process, the physician applied formedical staff privileges at another hospital and, inresponse to the question on the application that asks ifprivileges had ever been suspended or otherwise cur-tailed at another hospital, the physi-cian answered “no;” his explanationwas that the appeal was pending.However, during the credentialingprocess, medical staff officers atHospital B talked to medicalstaff officers at Hospital A andlearned about the suspension.The physician’s application wasrejected because he attempted toconceal the summary suspension. Denial wasbased on the false application and ignored thedetails of the case at Hospital A.
2. Believing That Collegial is Actually CollegialWhile cooperation and professional courtesy is
important, you must also be cautious when your medicalstaff membership and clinical privileges are at stake. Inanother case, a physician was alleged to have a history ofdisruptive behavior, but there were never any formalinterventions. However, when an adverse peer reviewaction was initiated, the hospital’s evidence consisted ofnumerous statements by medical staff officers aboutcounseling sessions, consisting of call waiting encountersand discussions in the doctor’s lounge. Although thephysician in question could not deny that the discus-sions occurred, she never suspected that the hospital wascreating a record of these encounters to later be usedagainst her.
3. Failure to Secure WitnessesAlthough most medical staff
procedures authorize informalmeetings at which counsel is notpermitted—either from thehospital or on behalf of thephysician—those same proce-dures often permit the physi-cian to bring other medical staffmembers who will support his
or her position. Not only do those medi-cal staff members serve to support the

The Bulletin u 283June 2005
LEGAL
REPORT continued
position at the meeting, they also serve as critical wit-nesses about what happened at a later time. In anothersituation, a physician was threatened with a situationsimilar to the one above, in which there were a numberof statements by other physicians attending the meetingsas to what occurred and what the physician admitted.The fact that there was a witness to rebut the severity ofthe statements that were to be offered as evidence wascritical to a satisfactory resolution of the situation.
4. Failure to Take Peer Review Activity SeriouslyPhysicians sometimes fail to take potential adverse
peer review activity as seriously as they should take it.They don’t really disregard the threat, but they feel thatthey are sufficiently prepared and know their adversecases well enough that they can simply attend themeetings and provide their opinion, which they presumewill not be questioned by their fellow medical staffmembers. Unfortunately, in some of these meetings andin one situation particularly, the Peer Review Committee
had already consulted an outside expert and had volumi-nous critical information about cases in which there wereadverse events. When faced with that information, thephysician’s unprepared remarks were insufficient to swayhis peers.
5. Failure to Obtain CounselThis mistake is a tangent of the mistake about failure
to take peer review activity seriously. Not only do somephysicians believe that they can handle the medicalissues with which they will be confronted withoutoutside help, but they may often believe that counsel isunnecessary until there is an actual hearing. In onesituation in which I was involved, I was not contacteduntil the hospital sent a formal notice that terminationof clinical privileges was going to recommended and thatit was providing an opportunity for a hearing. At thispoint, I met with the physician and reviewed the by-lawsthat provided for notice and an opportunity to discuss
Think practicing medicine is just about being a good doctor?Think practicing medicine is just about being a good doctor?Think practicing medicine is just about being a good doctor?Think practicing medicine is just about being a good doctor?Think practicing medicine is just about being a good doctor?
Tucker Arensberg’s Healthcare Lawyers have decades of experience helping doctors resolve their legal and business problems.
Think reimbursements, medical staff credentialing, restrictive covenants,employee benefits, tax, HIPAA, ERISA, OSHA and HSAs!
THINK AGAIN!
www.tuckerlaw.com
Sign up for our complimentary Quarterly Newsletterand Bi-weekly E-mail Newsletter:
E-mail your contact information to [email protected]
MichaelCassidy
RichardCramer
WilliamHarvey
KentCulley
CharlesVater
ScottLeah
StephenMatthes
CarlRonald
OwenSeman
continued on page 305

284 u The Bulletin June 2005
LEGAL REPORT
Update on MedicalMalpracticeMediation inWestern Pa.JACQUELINE O. SHOGAN, ESQ
ROBERT A. CREO, ESQ
On March 29, 2004, the Pennsylvania SupremeCourt promulgated new statewide rules forpretrial procedures in medical malpractice cases
that allow defendant health care providers to ask for acourt-ordered mediation early in the litigation process.These rules were effective immediately and applied toactions pending on that date. Rule 1042.21 provides:(1) Prior to the exchange of expert reports in a medical
professional liability action, a health care providermay file a motion with the court requesting a settle-ment conference or court-ordered mediation.(a) If the motion is filed without the consent of allother parties, the moving party shall certify that itbelieves there is a realistic possi-bility of settlement.(b) If the motion requestscourt-ordered mediation, themoving party shall describein the motion the media-tion which is sought andshall pay for the mediation.
(2) The court shall considerany objection to the mo-tion before entering anorder.
Also, under Rule 1042.51, the court is directed toinquire whether the parties are willing to participate inmediation when a pretrial conference is held after expertreports as to liability have been exchanged.
Subsequent to the promulgation of these rules, thePennsylvania Supreme Court went one step further andordered that all counties have available to malpracticelitigants a court-supervised mediation program that is inthe process of being established in most counties. De-spite these broad based initiatives by the courts, however,there are still some questions in the medical and legalcommunities regarding the use of mediation in medicalmalpractice cases. This is especially true given the
different models being utilizedthroughout the state. In Philadel-
phia, for example, Drexel Univer-sity College of Medicine has
developed a “Rush-style”mediation program. Thismodel utilizes two co-media-tors who are practicing medicalmalpractice attorneys. TheUniversity of PittsburghMedical Centers (UPMC), onthe other hand, has recentlyadopted the more traditional

The Bulletin u 285June 2005
LEGAL
REPORT continued
single mediator approach for cases currently in litigation.What physicians can expect under the single mediatormodel is the focus of this article.
The single mediator modelUnder the single mediator model, all sides of a
dispute meet with an experienced attorney mediator inan informal setting in an attempt to reach a mutuallyacceptable settlement. The mediator does not have astake in the outcome of a dispute. There are no formalcourt procedures or rules of evidence. Unlike a judge orarbitrator, the mediator has no authority to render adecision or force the parties to accept a settlement if afull resolution is not voluntarily reached. The mediator’srole is to assist the negotiating parties.
All parties to the dispute should be present at themediation session. Within the medical malpracticecontext, this usually means the plaintiff, plaintiff ’sattorney, defendant, defendant’s attorney and someonewith authority from the insurance carrier. Typically, allparties, party representatives, insurance representativesand the mediator meet in a joint session. After introduc-tory remarks by the mediator, the plaintiff ’s attorney isgiven an opportunity to make a short opening state-ment. Plaintiff is then given a chance to explain how heor she has been affected by the occurrence. Everyonepresent may be permitted to ask the plaintiff questions.The defendant’s attorney and defendant are then pro-vided with a similar opportunity to make an openingstatement and presentation.
After the joint session, the mediator meets with eachparty individually. In each caucus, the mediator discussesthe risks of the case, such as best and worst outcomes,the quality of evidence and the costs of litigation. Themediator also discusses possible settlements. These need
not be limited to financial compensation. Creativesettlements such as apologies and changes in policies orprocedures can be considered. It is common for themediator to go back and forth between the parties for anumber of caucuses. However, the mediator does notdisclose what is discussed in each caucus unless autho-rized by the respective party to do so. Furthermore, amediator does not side with any party or argue the factsor law on behalf of any party.
Pennsylvania law and the agreement of the parties tomediate provide for the confidentiality of all mediationcommunications including settlement offers. Finalsettlement positions are not admissible in subsequentlitigation. However, evidence that has an independentbasis of admissibility at trial may still be used, even if itwas discussed during the mediation. The mediator is notinvolved in the litigation of the case and cannot becompelled to testify or produce notes.
If the parties are unable to reach agreement on allissues at mediation, they may explore another alternativedispute resolution process such as binding arbitration toresolve outstanding issues. Arbitration may also be usedto apportion damages between multiple defendants whoare not able to do so themselves.
Preliminary results and trendsMediation is currently being used successfully in
medical malpractice cases throughout Pennsylvania.Among 31 cases in Western Pennsylvania, parties havegenerally agreed to mediation without the need for courtintervention. Mediations have already been conducted in20 of the 31 cases with 18 successfully settling. Settle-ment negotiations are ongoing in the other two caseswith additional mediation sessions to be held. Media-tions have not yet been held in the remaining cases orthey settled before mediation.
Trends within the legal arena support the evengreater use of mediation, including the possible adoptionof an apology rule in Pennsylvania and the use of earlymediation programs within the hospital setting.
The physician’s perspectiveIn a case mediated successfully during fall 2004
involving three physicians as defendants, the case settledwith two physicians consenting and their insurers paying
continued on page 286
Under the single mediator model,
all sides of a dispute meet with an
experienced attorney mediator in
an informal setting in an attempt to
reach a mutually acceptable
settlement.

286 u The Bulletin June 2005
LEGAL REPORT continued from page 285
on their behalf; one physician was dismissed from thecase. One of the consenting physicians said:
“Everyone was, however, very satisfied that areasonable compromise had been reached, thatthe uncertainties of trial were avoided and thatthe issue had finally been put to rest. Thisoutcome would not have been possible withoutthe skills of the mediator who approached theproblems methodically, without apparent bias,calmly, patiently and, above all, with a constantsmile. The mediator showed care and concern forall parties and for all points of view. In medicalsituations wherein damages have occurred andthere were opportunities for physicians, hospitals,nurses or other caregivers to prevent those dam-ages, mediation under the direction of a skilledmediator is clearly superior to the uncertainties ofa jury trial in the threatening environment of acourtroom.”
Mediation is not right for every case. However,where there is at least some merit to the claim and therisk of proceeding to trial is deemed to be too great,mediation should be considered. Physicians benefit byparticipating in the dialogue on all aspects of the case,including the terms of settlement. It is an opportunityfor physicians to directly explain their positions andfeelings to all involved parties and counsel. It may alsoprovide an opportunity to restore prior relations betweenthe defendants. Mediation recognizes and empowersphysician interests.
Ms. Shogan is an attorney with Thorp Reed & Armstrong, LLP, and amediator with JUSTUS Medical Malpractice Group. She can bereached at (412) 394-7721 or [email protected]. Mr. Creo isdirector of JUSTUS Medical Malpractice Group.

The Bulletin u 287June 2005
And we’ll do what we do best. The Allegheny County Medical Society specializes in
providing physicians with the best supplies and services at the best prices. And we only
contract with those vendors who can meet the unique needs of physicians.
Do What You Do Best.
Membership Group Insurance Programs
Blue Cross/Blue Shield, Disability,
Property and Casualty
0 USI Colburn Insurance Service
Bob Cagna (724) 873-8150
Life, HIV Coverage
0 Malachy Whalen & Co.
Malachy Whalen (412) 281-4050
Collection Service
0 IC System, Inc.
Matthew Buffalini (800) 279-6711, ext. 1212
Allegheny MedCare: Medical & Surgical
Office Products, Pharmaceuticals &
Equipment
0 Physician Sales & Services
Mark D. McKenna (800) 472-2791
Banking, Financial & Leasing Services
0 PNC Bank
Kevin Jansma (412) 373-6112
Physician Office VISA/MC Service
0 PNC Bank
Frank Fratangelo (412) 768-6066
Printing Services & Professional Announcement
Service for New Associates, Offices
and Address Changes
0 Allegheny County Medical Society
Susan Osborne (412) 321-5030
Records Management
0 Business Records Management, Inc. (BRM)
Rebecca Whipkey (412) 321-0600
We’ve done our homework
so you can spend more time doing what you do best.
(412) 321-2188

288 u The Bulletin June 2005
LEGAL REPORT
New Medicare AppealRules Draw FireWILLIAM H. MARUCA, ESQ
As the old saying goes, “Be careful what you askfor, because you might get it.” Physicians frus- trated with a lengthy appeal process for Medicare
decisions which included “fair hearing officers” whoseindependence was viewed as suspect, welcomed thechanges enacted by the Benefits Improvement andProtection Act of 2001 (BIPA). Those changes werescheduled to take effect in 2002, but had been delayedby the Centers for Medicare and Medicaid Services(CMS) despite ongoing pressure from organized medicine.
Now CMS has issued an interim final rule to moveforward implementing the changes, and some of theapproaches taken by CMS turn the reform principles ofBIPA on their head. Assuming these rules are imple-mented intact, physicians may have limited access to in-person hearings, may be required toassemble and introduce their entirecase earlier in the process, may facehead-on opposition from CMS athearings, and may be subject toa variety of restrictive proce-dural rules slanted toward thecarriers. Accordingly, severalphysician advocates havesubmitted critical comments toCMS, and two influential U.S.Senators are publicly questioningwhether the system will work.
First, some history: Medicare permits beneficiaries,and by extension, providers, to appeal Part B paymentdecisions though several steps. Prior to BIPA, the firstlevel of appeal was a carrier-based reconsideration, then afair hearing before a carrier-employed or contractedhearing officer. The fair hearing officer was required toapply the carrier’s policies, including Local MedicalReview Policies. Since these policies are often at theheart of the dispute, a fair hearing can be a frustratingstep. The administrative law judges (ALJs) were em-ployed by the Social Security Administration and mayconsider, but are not required to follow, local carrierpolicies. After that, an appeal may be taken by either theprovider or the carrier to the Medicare Appeals Councilunder the Departmental Appeals Board, and finally, an
action may be filed in Federal DistrictCourt. Each step required certain
dollar thresholds be met: $100 for acarrier fair hearing, $500 for an
ALJ appeal (except home health,which is $100), and $1,000 forFederal Court. A separateprocess was in place for Part Aclaims for hospital benefits.
BIPA required a series ofstructural and proceduralchanges to the appeals process,including:

The Bulletin u 289June 2005
LEGAL
REPORT continued
• Uniform appeal procedures for both Part A and Part Bclaims;
• Reduced decision-making time frames for mostadministrative appeals levels, as well as the right toescalate a case that is not decided on time to the nextappeal level;
• The establishment of new entities, Qualified Indepen-dent Contractors (QICs) to replace the hearing officersand conduct reconsiderations of claims denials madeby fiscal intermediaries, carriers and quality improve-ment organizations; and
• Use of QIC review panels, which include medicalprofessionals, to reconsider all cases involving medicalnecessity issues.
So far, what’s not to like? Congress stepped in againby enacting the Medicare Prescription Drug, Improve-ment and Modernization Act of 2003 (MMA) whichadded a number of provisions that affect the Medicareclaim appeals process, including:• Revised redetermination and reconsideration decision-
making time frames;• A reduction in the minimum required number of
QICs from 12 to 4;• A requirement to transfer the ALJ function from
Social Security Administration (SSA) to the Depart-ment of Health and Human Services (HHS) byOctober 1, 2005.
The bad news: The March 8, 2005 rule that imple-mented the changes raises concerns about a variety offairness issues, including:
New evidentiary restrictions: The rule bars a providerfrom introducing any evidence at the ALJ level that was
not introduced at the QIC hearing (which takes theplace of the old fair hearing) absent a showing of “goodcause.” The ALJ is to determine whether good causeexists, and the only guidance in the rule is a singleexample: “An ALJ finds good cause, for example, whenthe new evidence is material to an issue addressed in theQIC’s reconsideration and that issue was not identifiedas a material issue prior to the QIC’s reconsideration.”The end result is that if providers do not have their casesfully prepared at the QIC level, including expert testi-mony, additional medical records, medical literature,etc., they will not be allowed to introduce that evidencelater.
CMS participation in ALJ hearings: The ALJ mayrequest CMS or a carrier to participate in a hearing, orCMS or a carrier may elect to participate. This changesuggests some CMS frustration with the historical resultsof hearings based on their conclusion in the FederalRegister “that [certain prior payment appeal] cases mighthave been resolved more appropriately if CMS or thecontractor had been party to the appeal.” (emphasissupplied). Unlike the providers, CMS and the carriersare not required to have introduced all evidence prior tothe ALJ hearing. The result is not a level playing fieldbut an uneven one favoring the government and itscontractors. At a minimum, the rule should allowproviders to introduce new rebuttal evidence at an ALJhearing where CMS or a carrier has been allowed toparticipate.
Limits on discovery: Providers may only conductdiscovery when CMS or a carrier is a party, and thenonly subject to limitations imposed by the judge. A
continued on page 290

290 u The Bulletin June 2005
LEGAL
REPORT continued from page 289
party may not take the deposition of another partyunless the proposed deponent agrees to the deposition orthe ALJ finds that the proposed deposition is necessaryand appropriate in order to secure the deponent’s testi-mony for an ALJ hearing.
Substantial deference to CMS policies: Under the rule,decisionmakers at all levels are required to give CMSpolicies greater deference than similar informal agencypolicies are typically granted within administrativeappeal processes. The substantial deference standardincorporated in the Interim Claims Appeal Rule essen-tially allows CMS to impose binding obligations onbeneficiaries and providers without a public commentprocess.
Responsibilities of appointed representatives: The ruleimposes an “affirmative duty” on appointed representa-tives, including attorneys, to “Comply with all laws andCMS regulations, CMS Rulings and instructions.” It isnot uncommon for an attorney or other representativeof a provider to challenge the validity of CMS rulings,policies, instructions and other interpretations as incon-sistent with applicable law and regulation. It is unreason-able to require a representative to defer to all suchpolicies to the potential detriment of the provider/appellant.
Geographic distribution of ALJ offices: The new systemreduces in-person hearing sites from numerous localSocial Security offices to only three regional offices(Cleveland, Miami and Irvine, Calif.). Limiting in-person hearings to those locations will force manylitigants to use video-conferencing, an imperfect substi-tute, rather than incur the expense, lost income andinconvenience of traveling to one of these locations withattorneys and witnesses. More critically, it has beenreported that a large percentage of the existing veteranSSA ALJs who have been offered positions at these threeregional locations are declining to relocate. The loss ofthe “institutional memory” and skills of a cadre ofexperienced, knowledgeable and sophisticated ALJs whohave handled Medicare appeals for years will disadvan-tage all parties.
ALJ independence: With the transfer of the ALJs toHHS, safeguards will be necessary to ensure that theALJs are free from influence by or guidance from CMSto provide an objective evaluation. The restrictionsrequiring deference to CMS, the participation by CMS,
the restrictions on discovery, and the change to a moreadversarial approach invite further Congressional actionto maintain the independence contemplated by Con-gress.
The Cleveland Plain Dealer reports that the chair-man and ranking minority member of the Senate Fi-nance Committee warned HHS Secretary Mike Leavittand Social Security Chief Jo Anne Barnhart that the newsystem faces major obstacles, including employee train-ing, location of the field offices and reliance on videoteleconferencing to conduct long-distance hearings.
Chairman Charles Grassley (R-Iowa) and seniorDemocratic member Max Baucus (D-Mont) wrote “Afailure in the implementation of any one of these areasthreatens the integrity of the Medicare program and hasserious consequences for each of the 42 million Ameri-cans that has coverage under Medicare.” They also askedthe General Accounting Office to investigate.
Providers seeking a fair opportunity to disputeMedicare payment issues will be carefully watchingCMS for response to the comments to the March 2005rule as well as any developments that may arise out ofthe actions of Senators Grassley and Baucus. In themeantime, physicians who face such disputes shouldwork with experienced counsel to gear up for the chal-lenges and opportunities presented by the new system.
Mr. Maruca is a partner with the Pittsburgh office of the regional lawfirm of Fox Rothschild LLP, which serves as the counsel to the AlleghenyCounty Medical Society. Fox Rothschild is also a member of the GreatLakes Law alliance, whose health care group submitted comments toCMS regarding the Medicare Appeals Rule. He can be reached [email protected].
Did you know we get calls daily asking forreferrals to physicians? Be sure yourmembership information is up to date sothat you get connected, including:
Physician Referrals
√ Board Certifications√ Hospital Affiliations√ E-mail address
√ Correct phone/fax/address/e-mail
E-mail [email protected] orcall (412) 321-5030 and ask forNadine Popovich (ext. 110) or
Jim Ireland (ext. 101)

The Bulletin u 291June 2005

292 u The Bulletin June 2005
CAREY T. VINSON, MD, MPM
Progress on Pay forPerformance
As medical professionals, wethink the American health care
system is the best in the world andin many ways that certainly is true.Technological diffusion is rapid, andwe have an incredibly resource-richhealth care system. However, avail-ability of technology does not equatewith excellence in quality of care. Agrowing body of empirical evidencehas documented gaps between howhealth care should be delivered toachieve the best possible outcomesand how it is actually delivered.
The Institute of Medicinedramatically called attention to gapsin service in its 2001 report, Crossingthe Quality Chasm. The report hadthe following recommendationsregarding physician payment:• Fair payment should be given for
good clinical management;• Providers should have the opportu-
nity to share in the benefits ofquality improvement;
• Purchasers should have the oppor-tunity to recognize quality differ-ences in health care and directdecisions accordingly;
• Financial incentives should alignwith implementation of careprocess based on best practices andthe achievement of better patientoutcomes;
• Payment should promote bettercoordination of care.
Current physician paymentsystems aren’t designed to promotequality or better outcomes. Fee-for-service, capitation and salariedpayment don’t align compensationwith acceptable results. New meth-ods for paying physicians are neededso that doctors are appropriatelyrewarded for providing high-qualitycare and promoting better outcomesfor their patients.
Health care organizations havealready begun to pay physicians formeeting quality standards, usually inthe form of a pay-for-performancemodel that uses incentives to encour-age and reinforce the delivery ofevidence-based practices. Health caresystem transformation that promotesbetter outcomes as efficiently aspossible is also a key component ofsuch an incentive program.
More than 35 health plansrepresenting 30 million members
FROM WHERE I SIT:VIEWPOINT OF A PHYSICIAN EXECUTIVE
now offer pay-for-performanceprograms. Based on current growthtrends, at least 80 health plans areexpected to offer such programs by2006, covering more than 60 millionmembers.
Companies participating in theBridges to Excellence program, whichbegan in 2003 as a test in Cincinnatiand Louisville, pay doctors $50 to$160 per patient for meeting certainstandards for care they provide forchronic illnesses. In January, theprogram expanded to Massachusettsand upstate New York, where physi-cians have earned about $1 millionin bonus payments. The initiative isin the process of moving into 10states and involving more than twomillion people as employers andinsurers take it into the widermarketplace.
Among the many provisions ofthe Medicare Prescription Drug,Improvement and ModernizationAct of 2003 (MMA) are several
New methods for paying physicians are needed
so that doctors are appropriately rewarded for
providing high-quality care and promoting better
outcomes for their patients.

The Bulletin u 293June 2005
Centers for Medicare and MedicaidServices (CMS) demonstrationprojects intended to test potentialfuture improvements in Medicareexpenditures and quality of care.One project is a three-year demon-stration involving 10 physiciangroup practices, including theGeisinger Health System inDanville, Pa. The demonstration willinvolve more than 5,000 physiciansand 200,000 patients. CMS will paythe groups a five percent incentivewhen they can demonstrate im-proved quality of care and lower costmeasures.
This year, Highmark launchedQualityBLUE™, a physician pay-for-performance program, whichintroduces an incentive program forfee-for-service payment in westernand central Pennsylvania. Theprogram is an expansion of theexisting Quality Incentive PaymentSystem (QIPS), originally imple-mented in 1993 in western Pennsyl-vania for the Keystone Health PlanWest (KHPW) network primarycare physician (PCP) practices thatreceive capitation payment for theirmanaged care members.
For the new fee-for-servicecomponent of the program, incen-tive payments to eligible KHPWnetwork primary care physicians—internal medicine, family practice,general practice and pediatrics—inthe 29-county western region willbegin with applicable claims thathave service dates of July 1, 2005, orlater. A similar incentive programwill be introduced for thePremierBlue Shield network PCPpractices located in the 21-countycentral region beginning with servicedates of April 1, 2006, or later.
The QualityBLUE physicianpay-for-performance program isreimbursed as a fixed flat dollaramount paid as an add-on to desig-nated evaluation and management(E&M) services billed by the PCPpractice. E&M services includeservices such as office visits, inpa-tient hospital visits and newborncare, among others. To be eligiblefor the incentive program, PCPpractices must meet certain eligibil-ity requirements, such as beingNaviNet SM enabled, and meeting athreshold for the electronic submis-sion of claims.
When compared with QIPS,QualityBLUE’s components includetwo new additional measures for2005: best practices and implemen-tation of electronic health records.The best practices indicator allowspractices to get credit for the devel-opment and implementation of awork plan to improve quality ofclinical care and service to theirpatients. The electronic healthrecords indicator provides an incen-tive for the practice to implement anelectronic health record. Otherprogram components includeclinical quality indicators, use ofgeneric pharmaceuticals, electronicconnectivity and member access.
Dr. Vinson, a family practitioner, is medicaldirector for quality and medical performancemanagement at Highmark Blue Cross BlueShield. He can be reached at [email protected].
It’s no secret that, in recent years,consumer demand has shifted awayfrom managed care insurance prod-ucts and more toward fee-for-serviceplans. Consumers simply want morechoice and greater flexibility inaccessing care.
To complement this growingshift in membership, insurers mustkeep pace by rethinking and rede-signing their physician incentiveprograms. Such efforts will not onlyreward physicians for deliveringhigh-quality care both appropriatelyand efficiently, but by featuringincentives tied to the adoption ofelectronic information technologiesand the consistent use of evidence-based care practices to treat chronicconditions, they also may very wellunlock the potential for America’shealth care system to truly live up tothe billing as “the best the world hasto offer.”
The opinion expressed in this columnis that of the writer and does notnecessarily reflect the opinion of theEditorial Board, the Bulletin, or theAllegheny County Medical Society.
Contributors are needed for one of the Bulletin’s newest columns, “From
Where I Sit: Viewpoint of a Physician Executive.” If you are a physician
in a leadership position at a hospital, managed care firm or other
healthcare entity, please consider sharing your experience with your
peers by writing an occasional column on a topic of your choice for
our readers (approximately 500-1,000 words in length). E- mail the
Bulletin’s medical editor, Safdar I. Chaudhary, MD, at
[email protected], indicating your interest or call 412-427-6828.
From Where I Sit: Viewpoint of a Physician Executive
PHYSICIAN
EXECUTIVE continued

294 u The Bulletin June 2005
LEGAL PERSPECTIVE
Stop Prescribing Cox-2 Inhibitors?A Medico-legal AnalysisLESLIE TAR, MD, ESQ
KAREN TAR, MSN, CRNP, ESQ
The following is part two of a two-partreview on the use of Cox-2 inhibitors. Lastmonth’s review addressed the medicalindications for use of such agents. Thebasis for potential physician liability inuse of these agents will be reviewed here.
Cox-2 inhibitors are the newestgroup of NSAIDs to come to
the market. Unfortunately they haverecently been associated with anincreased risk of cardiovasculardisease. On April 7, 2005, theFederal Drug Administration (FDA)asked Pfizer to suspend its sales ofBextra. Celebrex and all other olderNSAIDs will now be marketed with“black box” warnings intended towarn consumers of the potentialassociated cardiovascular risks.Furthermore, the FDA intends toextend “black box” labeling to theover-the-counter versions of theseagents. While intended to putconsumers on notice, the aggregateimpact of this move may be tomerely desensitize consumers. Asover the counter medications con-tinue to be regarded as generally safeby consumers, finding such cardio-vascular warnings on Advil andMotrin IB labels may have the effect
of undermining such warning onprescription equivalents, much assuch warnings are ignored on packsof cigarettes. Many physicians haveshied away from prescribing Cox-2agents, given the current litigiousclimate. Whether physicians will feelcomforted with “black box warn-ings” prompting a resurgence ofCelebrex sales is yet to be deter-mined. It is likely that such warningswill benefit pharmaceutical manu-facturers more than it will providers.
Duty to warn and the learnedintermediary doctrine
For years, the pharmaceuticalindustry has, on the one hand,emulated physicians for their fund of
medical knowledge, while shieldingthemselves from liability by standingbehind the learned intermediarydoctrine. A drug manufacturer has aduty to warn of side effects of a drugwhen such effects are understood tooccur, but is not expected to warn ofunknown dangers. Often the manu-facturer discharges this duty byproviding the necessary informationto the patient’s prescribing physicianor to the pharmacist. The drugmanufacturer is considered an expertin its field; as such, it has a continu-ing duty to keep abreast of knowl-edge regarding its products and totake all reasonable steps to updatemedical professionals on theirpotential adverse effects. There is noduty to warn of possible reactions inunusually susceptible consumers,however, but just because a reactionis rare does not mean the manufac-turer has no duty to warn about it orthat the persons experiencing thereaction are unusually susceptible.For instance, though the allergicreactions to sulfonamides likeCelebrex are rare, Pfizer warnsphysicians that sulfa-sensitive pa-tients should not take Celebrex.
The learned intermediary

The Bulletin u 295June 2005
doctrine has been an incrediblyclever means for the pharmaceuticalindustry to shift product liability riskto physicians. The doctrine origi-nated in a 1966 suit against theproducer of chloroquine, sometimesused by rheumatologists in treatingrheumatoid arthritis, for failing towarn physicians of its potential tocause irreversible retinopathy.1 Byproviding physician’s with informa-tion about their product (albeit,usually in the form of marketinghype), the manufacturer has shieldeditself from liability, leaving it tophysicians to adequately inform theend user-patient. This defense shiftsthe focus for any failure to warnabout the medication’s risk from themanufacturer to the prescribingphysician. Furthermore, if theprescribing physician is aware of therisks associated with the use of themedication, any failure to warn bythe manufacturer cannot be a causeof the patient’s injury.
Most recently, the FDA hasreversed its position prohibiting thepharmaceutical industry fromengaging in direct-to-consumeradvertising. Whether this cameabout through successful lobbyingafter the industry experienced sales
decline in the managed care environ-ment, is not clear. However, in orderto create consumer demand to offsetmanaged care cost containment, itran the risk of losing protectionunder the learned intermediarydoctrine. In Perez v. Wyeth Labora-tories Inc., the court argued that thelearned intermediary doctrine doesnot apply when companies engage indirect-to-consumer advertising.2 Inthis case, female users of theNorplant contraceptive systemclaimed that Wyeth Laboratoriesfailed to provide adequate warningabout the adverse effects and surgicalcomplications of this heavily adver-tised product. The court found thatcompanies engaging in direct-to-consumer advertising were legallyresponsible for providing adequatewarnings to consumers about thepotential dangers of their products.After Perez, Id., television adsprovide more information about sideeffects, with a further disclaimer,“Only your doctor can say whetherthis product is for you,” a retreat tothe learned intermediary shield.
While direct-to-consumeradvertising seems to continue to rise,physicians in Pennsylvania shouldnot be comforted. Pennsylvania
courts have not abandoned thelearned intermediary doctrine in faceof direct-to-consumer advertisingunless the information imparted tothe physician was inadequate for thephysician to warn the patient. InIncollingo v. Ewing (1971), theSupreme Court acknowledged thatinformation imparted to physiciansby the company’s sales force in theform of “over promotion” by drugdetail marketers, which contradictedthat found in the PDR, cancelledout the product warnings in the PDR.
Pennsylvania physicians,strapped with the duty to warnconsumers, must know when thisduty is met. The duty to warn isachieved, not when the prescribingprovider has provided the warning,but when the reasonable patientwould have comprehended it. “Blackbox” warnings on cigarettes have notbeen a bullet proof shield for R.J.Reynolds; nor should such warningsprovide false reassurance to providersthat they are now relieved of theirduty to warn. Furthermore, theperfunctory motions of merelyproviding an informed consent formfor a patient’s signature is inadequateif the consumer can argue that he
continued on page 296
LEGAL PERSPECTIVE continued
Gloria Caroll
REALTOR®
and Team(412) 367-8000 Ext. 242
Hampton - $899,900
Elegance & style. Surrounded by oneacre of beautifully landscapedgrounds, this impeccable Tudor in aprivate cul-de-sac offers a world ofpleasant surprises with expansive liv-ing & entertainment areas. Sevenspacious rooms on the first flooralone.
Franklin Park - $939.900
New Price! Rarely is a home withthis character available. This 5BRbrick Provincial offers 4 full & 2 par-tial Baths, 2 FPs, lofty ceilings, 1stfloor MBR, an open floor plan & 4-car attached garage all on a beauti-ful 2.1 acre lot at the end of a cul-de-sac.
Marshall - $925,000
New Price! The open, airy designof this brick Provincial featuresmarble flooring, natural maplecabinetry & flooring, two-story FR& foyer, butler’s pantry, sunroom,cathedral ceiling & built-in cabinetry.6 BRs, 4.5 BAs, 2 fireplaces, 3 cargarage.

296 u The Bulletin June 2005
LEGAL PERSPECTIVE continued from page 295
did not understand its contents orimplications, or that the providernever discussed the contents. On theother hand, if the form was designedby the pharmaceutical company, asRoche Inc. has done in the distribu-tion of its consent form to derma-tologists prescribing Accutane, andthe prescribing dermatologistreviews its contents with the patientor provides the patient an Accutanevideo outlining the teratogenic risksof this acne drug to women of childbearing age, and documents that thevideo was given to the patient, hehas likely met his duty. As RocheInc. has provided the video andconsent form to be given to thepatient, the physician is arguablyshielded by providing “all of theinformation” that the pharmaceuti-cal manufacturer felt was relevant toconsumers prior to use of its product.
ConclusionCox-2 inhibitors are not likely to
go away. In fact, there are moreready to be released. These medica-tions provide physicians and patientsoptions that were not previouslyavailable. Class removal of thesedrugs is not likely to occur. Whilecardiovascular risk appears to beassociated with the entire class, suchagents have potential use in differentsettings. Whether any such agent isuseful for your patient will requiredeliberation with your patient on acase-by-case basis. Though informedconsent in writing is not requiredwith use of these drugs, I haveemployed the consent form belowwith surprisingly little consumeralarm. You may find it useful indocumenting your cardiovascularconcern and your communicationon the issue with your patient. Iwould like it if the FDA required
The opinion expressed in this columnis that of the writer and does notnecessarily reflect the opinion of theEditorial Board, the Bulletin, or theAllegheny County Medical Society.
Dr. Tar, a practicing rheumatologist, and wifeKaren, a rheumatology nurse practitioner, arealso attorneys and members of MyLawDoc,LLC. They can be reached at (412) 488-0218, or you can e-mail Dr. Tar at [email protected].
manufacturers to provide their ownconsent form, requiring providers toreview them with patients as acondition precedent to obtaining aprescription for these products. Asthis has not occurred, remember thatwritten documentation is your bestdefense against liability.
COX-2 INHIBITOR CONSENT FORM
Your medical provider has considered the use of Celebrex/other (circle one) as part of your care. Such “Cox-2 inhibitor” drugs appear to
be associated with an increased risk of strokes and/or heart attacks, occurring in about 1-1.2% of individuals who take them for periods
of about three years compared to 0.3% of patients taking only sugar pills. Traditional arthritis drugs such as naproxen/Aleve also appear
to be associated with lesser but increased risks of stroke and heart attacks than previously recognized.
Cox-2 inhibitor drugs are no stronger for pain control than traditional arthritis medications like ibuprofen/Advil. While they are associated
with less risk of stomach ulcers and bleeding, such problems can still occur.
In all other ways, Cox-2 inhibitors share the same risks of side effects as traditional arthritis medications.
My medical provider has reviewed this matter with me. I understand and accept such risks and I have asked my provider toprescribe this medication for me.
Date ______________ Signature ______________________________________________
Print name _____________________________________________
Date ______________ Signature ______________________________________________
Print provider’s name ____________________________________
REFERENCES
1Sterling Drug Inc. v. Cornish, 370 F2d 82,85(9th Cir 1966).
2Perez v. Wyeth Laboratories Inc, NJ Super.Ct. App. Div., No A-16-98 (August 19, 1999)

The Bulletin u 297June 2005
SPECIAL REPORT
State Society Weighs In On EMRDARLENE KAUFFMAN
Where does the Pennsylvania Medical Society(PMS) stand on electronic medical records(EMRs)? The state medical society is taking
the lead in expanding health information technology inPennsylvania while supporting physicians through therigorous process of EMR adoption.
Health care and information technology profession-als are working on development of the electronic healthrecord (EHR), a term that encompasses subsets ofelectronic records, including electronic medical recordssystems used by physician practices, hospitals and otherhealth care providers, and personal health records(PHRs)—records developed for patients that mayinclude transactions in a doctor’s office, a hospital andmedication records. Regardless of the particular termi-nology used, the prospect of using electronic records forpatients causes many Pennsylvania physicians a greatdeal of consternation. In many cases, the cost anddaunting process of converting from paper records to afully functional EMR system overshadows the potentialbenefits of such systems-patient safety, practice efficiencyand, typically, greater peace of mind.
Recognizing the challenges associated with imple-menting an EMR system, the Board of Trustees of thePennsylvania Medical Society appointed a task force toidentify ways the society could encourage and assist itsmembers in the use of information technology. The firststep is EMRs; long-term goals are to improve medicalpractice, patient care and the patient-physician relation-ship. The task force, dubbed the “Techies,” was chairedby Bruce A. MacLeod, MD, FACP, chair of the Depart-ment of Emergency Medicine at Mercy Hospital inPittsburgh and a member of the state society’s board.Task force members included physicians, practice ad-ministrators and physician-hospital organization repre-sentatives from across the commonwealth.
On May 18, 2005, the Board of Trustees approvedthe Techies’ final report that spelled out a comprehensive
plan to address health information technology at twolevels.
At a macro level, the society is actively involved in astatewide effort on health information technology. It iscritical that electronic health information be transfer-able. It is not enough to simply create a digitized record.Health care providers must be able to exchange pro-tected health information in a secure manner. Some havecompared building a regional health information net-work to building a road. You do not build the businessesand restaurants and then build the road. The road isbuilt first, followed by commercial expansion. Likewise,once the information network is established, providers,payers and other organizations will be better able todesign or purchase systems that are compatible with thenetwork. It is essential that the state society be activelyengaged in the development of a health informationnetwork for Pennsylvania.
To facilitate the development of a statewide networkfor the exchange of electronic health information, thePennsylvania Medical Society has partnered with QualityInsights of Pennsylvania (QIP), the quality improvementorganization for the commonwealth. The two organiza-tions founded the Pennsylvania eHealth Initiative, acollaborative of more than 30 major stakeholders in theexchange of electronic health records. The PennsylvaniaeHealth Initiative has won the enthusiastic support ofsuch stakeholders as the Hospital & HealthsystemAssociation of Pennsylvania (HAP), Health InformationManagement Systems Society (HIMSS), academicmedical centers, insurance companies, state and federallegislators, state government, private practice physiciansand professional membership organizations. By repre-senting physicians’ interests in the initiative, the societyhopes to reduce the risk of EMR investment for Pennsyl-vania physicians by advocating for interoperabilityamong EMR systems.
continued on page 305

298 u The Bulletin June 2005
ELIZABETH L. FULTON
Bruce L. Wilder, MD, JD—Physician, Attorney,Advocate, Volunteer
PROFILE
Dr. Wilder
Bruce L. Wilder, MD, JD, neurological surgery,received his medical degree from Tufts UniversitySchool of Medicine in Boston in 1966. He held
several residencies following his graduation, eventuallyending up in Pittsburgh for a residency in the 1970s. Heearned a law degree from the University of Pittsburgh in1986. (Author’s note: the following answers have beenparaphrased.)
Who inspired you to become a physician?My father was a physician, a general practitioner. He
was primarily my inspiration, but I was a little bitunfocused. When I worked for a neurosurgeon at Tuftsbefore I went to medical school, I got to see surgery andwork in a lab. That really got me interested. The neuro-surgeon was Dr. Bertram Silverstone, who was fairly wellknown at the time.
What made you decide to get a law degree?I was thinking about it as a high school student. I
took an interest in Clarence Darrow. I saw the play,Inherit the Wind, when I was about 12 years old. Theplay was about teaching evolution and Darwin, whichincidentally is being played out again in Kansas now.That got me excited about law and standing in front ofthe court. I went to medical school early. I had alsoapplied to law school, but before I went I worked for aneurosurgeon and got reoriented to a medical career.
Later, while working in medicine, I became interested intopics of legal significance, so I went to law school.
How has having both a law and medical degree helpedyou?
It helps me in doing things that I like to do. I alwayswanted to do both. Having a medical degree has helpedme a little with my law practice. People notice when youhave a medical degree. They tend to listen to you morethan if you didn’t have it.
What are some of your interests outside the office?My biggest interest is music. I’ve been involved with
the Pittsburgh New Music Ensemble for many years,and I’m the president of the board. The Pittsburgh NewMusic Ensemble is a small group of nationally recruitedmusicians. It was started by David Stock, a composerwho is a Pittsburgher. What we do is commissioning ofnew work by composers. That is our forte. Our perfor-mance is high level as well.
Tell me a little about your family.My wife Joanne is a well known divorce attorney/
family law attorney. She was really the one who helpedme decide to go to law school. She has been a mentor aswell as my wife. My son Charlie is almost 24 and anarchitect in Philadelphia. My mother was quite anaccomplished musician.
The Bulletin u 299June 2005
What else would you like the Bulletin readers to knowabout you?
I don’t make a lot of money practicing law, but I’mpretty active in various organizations including theAllegheny County Bar Association, Pennsylvania BarAssociation and American Bar Association. I’ve been thechair of several committees. I’m on a special committeefor bio-ethics and law, and I’m also on a committeedrafting a model act on genetic and reproductive tech-nology. We are working on getting the revised UniformParentage Act passed in Pennsylvania. It was revised toinclude assistive reproductive technology such as frozenembryos and in vitro fertilization.
I also do volunteer work. I’m on the legal committeefor the Pittsburgh AIDS Task Force. I also belong toPhysicians for Human Rights; I’m part of its AsylumNetwork, which are physicians who give exams to peoplewho may have been tortured or abused in their homecountry who are seeking asylum in the United States. Ihaven’t done many exams through the network, but Ibelieve I’m helping people.
Many people ask if I do medical malpractice. Mypractice involves mostly physicians and deals with thingslike medical staff issues. I’ve thought about doingmedical malpractice, but I’ve not done it. I have a hardtime advocating against physicians, and I also have ahard time advocating against patients. But I am active inmany organizations, including the Bar Association, totry to find a solution to the medical malpractice issue.
Ms. Fulton is communications assistant for the Allegheny CountyMedical Society. She can be reached at [email protected].
www.acms.orgIf you haven’t logged on to our web site recently,
guess what you’re missing?
√ Daily updates on legislative actionimportant to physicians
√ Online petitions√ Physician Placement√ Resumes and Position Postings√ Reaching other ACMS members√ Sponsorship Opportunities√ Activity Announcements√ And More!
ExperienceA combined 310 years of Physician Healthcare Serviceand solution experience in Pittsburgh. That means wehave the knowledge base to provide the best in medicalsolution and service!
Commitment22,000 square foot Pittsburgh warehouse means acommitment to our community to provide the bestservice, solutions, quality and price to your practice.
Timely DeliverySame-day delivery service for emergency orders andnext-day delivery for orders received before 6 p.m.means reducing inventory on your shelves, saving space,reducing overheads and not tying up your cash.
ProfessionalismMedical supplies delivered and instant credit returnswith our dedicated, knowledgeable and service-orienteddrivers—professionals who know your products andwhere you want them placed to save you time.
No Hidden CostsNo minimum orders and no shipping charge! Ever!
OUR MISSION is to serve eachcustomer as if he or she were the onlycustomer by providing each office withthe best healthcare services andsolutions for quality patient care.
We value your partnership in helping us to serveyou. Thank you, physicians, administrators andoffice staff, for directing and advising us on medicalsupply products, services and costs.
Allegheny MedCare
Endorsed by the Allegheny County Medical Society
Group Purchasing Program
Mark D. McKenna
Toll Free (800) 472-2791
www.pssd.com

300 u The Bulletin June 2005
2005 BULLETIN EDITORIAL INDEX: JANUARY-JUNE
Volume 94 No. 1 ................ January 2005 ........................Pages 1-52Volume 94 No. 2 ................ February 2005 ..................Pages 53-100Volume 94 No. 3 ................ March 2005 ....................Pages 101-156Volume 94 No. 4 ................ April 2005 ......................Pages 157-208Volume 94 No. 5 ................ May 2005 ....................... Pages 209-260Volume 94 No. 6 ................ June 2005 ....................... Pages 261-308
A
ACMS Calendar ................. 25, 73, 128, 177, 231, 281Academic Perspectives:
Match Day – When the Future Finally ComesInto Focus ............................................................ 252
Arthur S. Levine, MDA New Year, A New Home for BiomedicalResearch................................................................. 12
Arthur S. Levine, MDPolio Legacy Endures in Pitt’s ResearchPriorities .............................................................. 144
Arthur S. Levine, MDActivities and Accolades ..... 21, 68, 125, 174, 226, 278Applications for Membership ........... 96, 152, 199, 257
B
Board of Directors .................................... 47, 149, 254
C
Classified Advertising ......... 50, 98, 154, 206, 258, 306Community Notes ............ 23, 70, 126, 127, 172, 173,225, 279Continuing Education ........ 24, 72, 129, 176, 230, 280
D
Dear Doctor ..................................... 22, 175, 224, 277
E
Editorials:The Care and Feeding of Physician Assistants ...... 216
Christopher J. Daly, MDFree Lunch or Forbidden Fruit ............................. 164
Adam Z. TobiasDoctor, Is There a Draft in the House? .................. 60
Timothy G. Lesaca, MDHow Electronic Health Records May ChangeHealth Care ......................................................... 268
Indira P. Jevaji, MD
On the Question of Religion and Medicine ............. 8Janet A. Chollet, MD
The Smith Principle ............................................. 112Basil A. Marryshow, MD
F
Features:2004 ACMS Award Winners ................................. 42
Elizabeth L. Fulton2004 – Year in Review............................................ 322005 ACMS President and Officers ....................... 41Medical Society’s Contributions to the Effortto Eradicate Polio ................................................. 188
Linda L. SmithPhoto Feature: 2005 ACMS InaugurationDinner ................................................................. 138Specialty Society Update 2005 ............................. 180
From the Mailbag ....................... 24, 69, 124, 223, 277From Where I Sit: Viewpoint of a Physician Executive:
Progress on Pay for Performance .......................... 292Carey T. Vinson, MD, MPM
G
Getting There: Musings of a Medical Student:The Heads-Up About Epistaxis ............................ 166
John L. FalconeHow to Feel Good About Yourself ......................... 62
Emily BrownThe Scholarly Project: A New Part of MedicalEducation ............................................................ 118
Cyrus RajiTime to Fight for Our Patients ............................... 10
Adam Z. TobiasWhat You Won’t Find in the Syllabus ................... 272
Matthew Neal
H

The Bulletin u 301June 2005
EDITORIAL INDEX continued
continued on page 302
I
Important Notice on Reporting MedicalLiability Suits .......................................................... 235In Memoriam ......................................... 124, 175, 229
A Tribute to Penna Drew ..................................... 229Macy I. Levine, MD
J
K
Key 2005 Legislative and Regulatory Initiatives ...... 265
L
Legal Perspective:Stop Prescribing Cox-2 Inhibitors?A Medico-legal Analysis (Parts 1 & 2) .......... 238, 294
Leslie Tar, MD, Esq.Karen Tar, MSN, CRNP, Esq.
Legal Reports:Biggest Mistakes—Credentialing Case Studies ..... 282
Michael A. Cassidy, Esq.The 10 Biggest Mistakes Physicians Make in theCredentialing Process ............................................. 80
Michael A. Cassidy, Esq.Getting the Bad with the Good—SuccessorLiability ............................................................... 242
Robert A. Galanter, Esq.Medical Staff Disputes Intensify ........................... 133
Edward J. Kabala, Esq.William H. Maruca, Esq.
New Legal Requirements for NonqualifiedDeferred Compensation Plans ............................. 184
Michelle L. Kopnski, Esq.New Medicare Appeal Rules Draw Fire ................ 288
William H. Maruca, Esq.Update on Medical Malpractice Mediation inWestern Pa. .......................................................... 284
Jacqueline O. Shogan, Esq.Robert A. Creo, Esq.
Looking Back in Time .............................. 13, 187, 206
M
N
O
P
Perspectives:Butterfly Power: A Fresh Meaning forInfection Control ................................................... 92
Diane Dean, MA, RN-C, LPCConsidering the Move to ElectronicMedical Records .................................................. 251
Melinda M. Campopiano, MDSometimes We Forget (Guest Perspective) .............. 45
T. Hayes Woolen Jr., MDTsunami: A View from Ground Zero ................... 204
Brahma Sharma, MD, FACCPhysicians’ Personal Pearls ............................... 71, 175Pill Box:
Beta-Blockers Post Myocardial Infarction—IsTreatment Ending Too Soon? ................................. 76
Siva Kedar, MDDonald Polito, RN, MBA
Contemporary Management of Chemotherapy-Induced Nausea and Vomiting ............................. 130
Thomas L. Rihn, PharmDCOX-2 Inhibitors: The Past, Present and Future .. 232
Thomas L. Rihn, PharmDNicole K. Remaley, PharmDCynthia S. Niccolai, PharmD
Ethinyl Estradiol/Levonorgestrel (Seasonale) forOral Contraception.............................................. 178
Heather A. Kudis, PharmDStephen A. Wilson, MD
New Approvals by the FDA in 2004 ...................... 26Tucker Freedy, PharmD, BCPS
Practice Management:Claims Rejections: When the Beneficiary Can’t BeIdentified ............................................................. 244
Amy Ascher, CPCEncouraging Overweight Patients to Make BehaviorChanges ............................................................... 196
Karen K. Davis, CPHRMHIPAA Q&A................................. 31, 137, 241, 281
Joan M. Kiel, PhDJust How Expensive is the Market? ......................... 86
Louis P. Stanasolovich, CFP

302 u The Bulletin June 2005
EDITORIAL INDEX continued from page 301
President’s Message:President’s Inaugural Address ............................... 114
Mark A. Goodman, MDProfiles:
Bruce L. Wilder, MD – Physician, Attorney,Advocate, Volunteer ............................................. 298
Elizabeth L. FultonMark A. Goodman, MD – Physician, Husband,Father, World Traveler .......................................... 142
Elizabeth L. Fulton
Q
R
S
Society News:2005 Reproduction Fees released ........................... 65ACMS announces award winners ........................... 19ACMS calls for nominations .......................... 64, 276ACMS provides career assistance ............................ 65ACMSA to celebrate Doctors’ Day ...................... 122Alliance continues hand program ......................... 123AMA organizes tsunami relief ................................ 66Associate editors appointed .................................. 121Call for nominations ............................................ 120Coding camp here in August ................................ 274Correction to Dec. Bulletin item ............................ 20EMR seminar scheduled June 1 ........................... 218EOL program set for Feb. 18 ................................. 19Geriatrics society holds update ............................. 218Geriatric update set for April .......................... 64, 120Geriatric update to be held in April ........................ 19Health insurance renewal rates swing wide ........... 275Media changes noted ........................................... 221Medical ’biz in the ’Burgh ............... 20, 69, 123, 168,221, 276Most Interesting Cases presented ........................... 64Ob/Gyn society meeting held .............................. 274Ob/Gyn society meets .......................................... 168Ob/Gyn society presents update .......................... 122Ophthalmology society speakers ............................ 65Ophthalmology spring meeting ............................. 64Ophthalmology spring meeting held .................... 168OSHA Update draws crowd................................. 218Pediatrics meeting held in February ..................... 121
Photo: 2005 Inauguration ...................................... 64Photo: Benjamin Rush Award .............................. 122Photo: Career night program ............................... 169Photo: Child Health Committee ......................... 220Photo: Contract & Negotiations session .............. 274Photo: EPEC Program ......................................... 120Photo: Focus on the Issues ...................................... 120Photo: Gerontology’s annual clinical update ........ 220Photo: Henry the Hand......................................... 123Photo: Musical moment ....................................... 275Photo: Occupational Health/OSHA Update ........ 219Photo: Ophthalmology Society ............................ 168Photo: Pittsburgh Ophthalmology Society ........... 122Photo: Pittsburgh Surgical Society ....................... 221Photo: Senior Expo .............................................. 274Photo: Surgical society lifetime membership ........ 275Photo: Urologists and ob/gyns meet together ....... 219Photos: Science Fair winners ................................ 218Physician Career Center launched ........................ 123Physicians needed for health fair .......................... 274PMS develops new services .................................. 168PMS looking for nominations .............................. 218School Health Update held .................................. 220Surgeons travel to West Virginia .......................... 275Surgical Society meets .......................................... 275Urologists host guest speaker ................................ 168Urologists to meet in June.................................... 274Urologists to meet on June 20 .............................. 218
Special Reports:CCAC’s Center for Health Careers: A“Smorgasboard” of Programs ............................... 202
Elizabeth L. FultonFacing the Facts About Child Abuse ..................... 148Highmark Caring Place ........................................ 146
Elizabeth L. FultonImportant Tips for Performing Emergency Self-Surgery ................................................................ 256MIND Your Health: The Co-occurrence of Depres-sion with Medical Disorders ................................. 246National Alcohol Screening Day 2005—Thursday, April 7 ................................................... 85PTSD Among Returning Veterans andTheir Families ........................................................ 88
Ravi Kant, MD

The Bulletin u 303June 2005
Reportable Diseases ........................................ 91, 237State Society Weighs In On EMR ........................ 297
Darlene KauffmanU.S. Public Sharply Divided on Privacy Risks ofElectronic Medical Records .................................. 248
T
Technology and Medicine:Disease Prevention and Management viaReal Time Integration .......................................... 200
Riffat S. Chughtai, MATechnology’s Role in the “Greater Good” ............... 74
Riffat S. Chughtai, MAThoughts From Our Medical Editor:
Safdar I. Chaudhary, MDMaking Choices of Clinical Care ......................... 162Morals, Social Norms and the Practice ofMedicine .............................................................. 266Our Kids, School Systems and Public HealthConcerns ................................................................. 6Our Prescription Writing Habits .......................... 110Universe, Earth, Tsunami and Us: CurrentMayans .................................................................. 58“You feel me?” – The World of Teens ................... 214
Tsunami Relief .......................................................... 31
U
V
W
X
Y
Your Executive Committee:Obesity: Where We Have Been and WhereWe are Going ......................................................... 14
Terence W. Starz, MD
Z
DOUGLAS A. CHEN, M.D.
is pleased to announce that
TODD A. HILLMAN, M.D.
will join him in the practice of
Otology & Neurotology
June 2005
420 E. North Ave. 2380 McGinley Rd. 11676 Perry Hwy.
Suite 402 1st Floor Suite 2201
Pittsburgh, PA Monroeville, PA Wexford, PA
15212 15146 15090
(412) 321-2480
(412) 321-3229 Fax
www.pittsburghear.com

304 u The Bulletin June 2005
2005 BULLETIN ADVERTISING INDEX: JANUARY-JUNE
Accounting firmsCase/Sabatini .................................... (412) 881-4411
Billing/claims/collectionsFenner Corporation .......................... (412) 788-8007I.C. System ....................................... (800) 279-3511Pinnacle Management ServicesOrganization ..................................... (412) 481-1791
CateringStrictly Business Catering .................. (412) 781-6668
Financial Institutions/AdvisorsThe Fragasso Group Inc. ................... (412) 227-3200National City .................................... (412) 355-4844Wachovia Securities ........................... (800) 545-0480
InsuranceGE Medical Protective ....................... (800) 4MedProMalachy Whalen & Co. .................... (412) 281-4050PMSLIC ........................................... (800) 445-1212USI Colburn Insurance Service ......... (724) 873-8150
Legal FirmsDickie, McCamey & Chilcote .......... (800) 243-5412Phillips & Faldowski ......................... (724) 225-9933Tucker Arensberg .............................. (412) 566-1212
Medical Record StorageBusiness Records Mangement Inc. .... (412) 321-0600
Medical Supplies/EquipmentAllegheny MedCare—PSS Sales ........ (412) 472-2791Nations Innovations .......................... (724) 272-0842
Organizations/InstitutionsAct One Theatre School .................... (412) 487-5613Allegheny Physicians ServiceCorporation ...................................... (412) 321-2188American Cancer Society ................. (800) ACS-2345Chatham College .............................. (800) 837-1290National Toll-Free Poison Help ......... (800) 222-1222Physicians Health Program ............... (717) 558-7819Providence Heights Alpha School ..... (412) 366-4455Shady Side Academy ......................... (412) 968-3180Tobacco Free Allegheny .................... (412) 578-7910
U.S. Army: AMEDD ........................ (800) 784-8867Western Pennsylvania School forthe Deaf ............................................ (412) 371-7000Winchester Thurston School ............. (412) 578-7518
Payroll/Human ResourcesPaychex ............................. (412) 921-9797, ext. 3527
Practice Management ServicesAlpern Rosenthal ................. (412) 281-7692 ext. 351A to Z CommunicationsManagement ..................................... (412) 303-0189MBSS ............................................... (724) 731-0200PMSCO ........................................... (888) 294-4336Virtual OfficeWare Inc. ..................... (412) 261-3790
Real Estate/DevelopmentKossman Development Company ..... (412) 921-6100Lake MacLeod .................................. (724) 625-1277Prudential Preferred Realty,Gloria Caroll ........................ (412) 367-8000 ext. 242Re/Max Heritage, Jill DeRiggi .......... (412) 241-4200Roy F. Johns, Associates .................... (412) 264-8383Spartan Health .................................. (412) 469-6955Zangrilli Realty Group ........... (877) 530-7355 ext. 82
StaffingACMS Physician Career Center ........ (888) 884-8242Liken Health Care ............................ (412) 816-0113Maxim Staffing Solutions .................. (877) 704-2345
Tailors/ClothingMontaj Hong Kong Downtown ........ (412) 391-9333Montaj Hong Kong Monroeville ...... (412) 824-9565
The medical society appreciates and dependson its advertisers. Please remember to tell
them you saw their ad in the Bulletin.

The Bulletin u 305June 2005
Mr. Cassidy is a shareholder with Tucker Arensberg and chair of thefirm’s Healthcare Practice Group. He can be reached at (412) 594-5515 or at [email protected].
this situation before any adverse action would be recom-mended. When that opportunity was requested, thephysician was advised that he had already had thatopportunity in the guise of a conference call. At thispoint, the physician wanted to explore opportunities toresolve the situation without a termination, but since theinvestigation had already commenced, any type of avoluntary withdrawal or resignation would be reportedto the National Practitioners Data Bank and, in fact, wasreported. That physician failed to realize that there wereformal proceedings underway with which he had notprior experience.
These case studies are not isolated events. In fact,they are frequent occurrences, and you should be awareof these whenever your medical staff membership orclinical privileges are threatened.
LEGAL
REPORT continued from page 283
On a more practical level, the society will address theissues of the individual physician. It is the society’s goalto provide individual physicians and practices with thesupport and information they need to confidentlyevaluate, purchase and implement EMR systems. Al-though the federal government has not mandated thatphysicians adopt electronic medical records, the groundswell was phenomenal following President Bush’s an-nouncement in April 2004 that every American wouldhave an electronic health record within 10 years. If thisfederal initiative continues to snowball, as we expect itwill, even the most reluctant physician may feel morecomfortable in taking the EMR leap.
With these concerns in mind, the society is planninga full spectrum of projects to assist its members. Theprojects are directed at providing software information,education and physician networking on EMR topics.The society will also advocate for its members in theareas of financial incentives for EMR adoption, fundingopportunities, backwards compatibility of existing EMRsystems and universal broadband access throughout thecommonwealth.
As a first step, the Pennsylvania Medical Society willconduct a survey this summer of physician practicesregarding their use of broadband and other healthinformation technologies, their success with implement-ing and incorporating technology into their practice andany barriers to adopting such technologies. The results ofthe survey will help the PMS precisely target the needsof physicians in specific geographic regions or specialties.In addition, QIP will use the survey results to determinethe penetration of health information technology inPennsylvania and report its findings to the Centers forMedicare and Medicaid Service (CMS).
The commitment of resources by the PennsylvaniaMedical Society to health information technologyadvocacy, products and services is significant. It willremain a strong advocate for the expansion of EMRacross the state and within your office.
Ms. Kauffman is an associate director in the practice economics andpayer relations division of the Pennsylvania Medical Society, where shehas primary responsibility for HIPAA and health care informationtechnology, including the electronic health record (EHR) ande-Prescribing. She can be reached at (800) 228-7823, ext. 1446, or [email protected].
SPECIAL
REPORT continued from page 297
ACMS PhysicianCareer Centerwww.acms.org
A unique interactive online recruitmenttool provided by the Allegheny CountyMedical Society, a member of theHEALTHeCAREERSTM Network
An integrated network of dozens of the
most prestigious health care associations
Questions? Contact HEALTHeCAREERS
Network at 888/884-8242
Candidates:♦ View national, regional and local job listings 24 hours a
day, 7 days a week—free of charge.
♦ Post resume free of charge where it will be visable tothousands of health care employers nationwide. Postconfidentially or openly—depending on candidate’spreference.
♦ Receive e-mail notification of new job postings.
♦ Track current and past activity, with toll-free access topersonal assistance.
Employers:♦ Access nationwide market of qualified candidates.
♦ Resume Alert automatically e-mails notices of potentialcandidate postings.
♦ Enjoy exceptional customer service and consultation.♦ Use online tracking.

306 u The Bulletin June 2005
CLASSIFIEDS
Help Wanted
MEDICAL DIRECTOR–Rap-idly growing Pittsburgh-basedmulti-state managed care organi-zation seeks Pennsylvania li-censed board certified familyphysicians, geriatricians, or inter-nists to serve as Medical Direc-tors. Under the leadership of ourSenior Medical Director, Medi-cal Directors assist with utiliza-tion and quality management,credentialing, and other medicalmatters in a collegial atmospherethat fosters professional experi-ences. Part time and full timeopportunities are possible. If youdesire to make a diference inhealth care, send your CV toRecruiter, Three Rivers Admin-istrative Services, LLC, 300 Ox-ford Drive, Monroeville, PA15146; or fax to 412-457-1391;or e-mail to [email protected]. AnEqual Opportunity Employer.
PSYCHIATRIST–Part-time(10-12 hours per week) salariedposition available at CMHC inSouth Hills to provide outpatientpsychiatric services to adults.Board certification with DEA #and Highmark/Medicare creden-tialed required. To apply send re-sume to: Human Resources De-partment, Dept. A., ChartiersMH/MR Center, 437 RailroadStreet, Bridgeville, PA 15017.EOE M/F/V/D
PSYCHIATRIST–SewickleyValley Hospital, a member ofHeritage Valley Health System,has an immediate opening for a
full time Adult & Child Psychia-trist to work in Staunton Clinic.Staunton Clinic is a comprehen-sive hospital based program of-fering a wide range of private andpublic mental health and mentalretardation services. Primaryresponsiblilities involve providingongoing care to outpatients at theBellevue, West Park andSewickley Vally Hospital officelocations. Credentialing withmajor payors is required. We of-fer a highly competitive compen-sation package consisting of anexcellent salary and flexible ben-efits program. Interested candi-dates may respond in confidenceto: Sewickley Valley Hospital,Human Resources Department,720 Blackburn Road, Sewickley,PA 15143, or fax to 412-749-7428. Apply online: www.heritagevalley.org
PHYSICIAN–Any specialty, re-tired with active license okay,malpractice provided. 412-232-3555
PART-TIME M.D.–Are youtired of the hospital environment?Are you looking for a careerchange? Why not try research!Novum Pharmaceutical ResearchServices is looking for a Part TimeM.D. or D.O. to oversee clinicalinvestigations. Qualified candi-dates will possess a current medi-cal license and current D.E.A. &ACLS certification. Interestedcandidates please forward yourresume w/cover letter & salaryrequirements to [email protected].
For Sale
FOX CHAPEL–MLS#537671–$975,000–This large and brightTudor home rests on a flat acrein popular Fox Chapel Manor.The many fine features includearched doorways, hardwoodfloors, sunken living room withfireplace, second floor study plussunken family room and so muchmore! Please call for details andan appointment to see. BunnyWolff and Lucy Oliver 412-782-3700 ext. 238 or 210.
FOX CHAPEL–MLS#557352–$1,190,000–Newly listed! Gra-cious Tudor in Fox Chapel Manorwith sunken living room withfireplace, formal dining room,new kitchen, first floor sunroomplus den, first floor laundry, 4bedrooms, 3 1/2 baths. Thisproperty offers over one level acreof beautiful landscaping and gar-dens including an inviting freeform pool. For more informationand appointments to see, pleasecontact: Bunny Wolff or LucyOliver at 412-782-3700 at ext.238 or 210.
THRIVING CARDIOLOGYPRACTICE in heart of Pitts-burgh, Pennsylvania. Large loyalpatient base. Grossing 500K peryear. Relocating after 29 years tosemi-retire. Please reply to Box 6/18-A.
For Rent
FOR RENT–Spacious threestory beautifully decoratedtownhouse in South Sea PinesPlantation, Hilton Head, SouthCarolina. Ocean front, 4 bed-room/4 baths, large family roomlooks out on a spectacular oceanview, adjacent to marina, com-mon swimming pool. For furtherinformation call 412-963-6802.
For Sublease
SUBLEASE–SOUTH HILLS:Manor Oak Two–new, fullyequipped medical office locatednear St. Clair Hospital. Free park-ing, space available for half daysor full days on Tuesdays andThursdays. For additional infor-mation contact Shirley at 412-687-2100.
Professional Services
THE DOCTOR’S LAWYER ISA DOCTOR–Professional licen-sure defense, Social Security Dis-ability for your patients, RiskManagement for Hospitals,Stark, employment contract for-mation/review, Wills, Trusts, andEstates. Don’t pay to teach alawyer your practice. Call theattorneys engaged in the practiceof law and medicine.MYLAWDOC, LLC: 412-488-0218. Leslie Tar, MD, JD, MPHand Judy Orie, MD, JD atwww.mylawdoc.com.
Box Replies:ACMS/box number
713 Ridge Avenue
Pittsburgh PA 15212

The Bulletin u 307June 2005
We are always available as
your insurance consultants.
Please call us at any time if
you have questions about
your existing coverage or
new options you may have
heard about. We assure
prompt response, realistic
advice and no sales pressure.
♦♦♦♦♦ Log on to www.malachy.com
♦♦♦♦♦ Read the details and premiums
♦♦♦♦♦ Download the application
♦♦♦♦♦ Complete and FAX to me at (412) 261-5955
Clark [email protected]
Malachy [email protected]
21st century technology combined
with our true personal service!
Our Special Plan is back! We are able to offer
$500,000 of term life insurance with NO
blood, NO exam and NO specimen.
Just click, read and apply!
Peggy [email protected]
Visit www.malachy.com(412) 281-4050(800) 343-5382FAX (412) 261-5955
Endorsed by the
Malachy Whalen & Co., Inc.
www.malachy.com
Endorsed agent for life/HIV indemnity since 1968