Embed Size (px)
Citation preview
05.07.2018
1
Genomics of Lung Cancer:Impact on Molecular Diagnostics Guiding Therapy
Maastricht June 19th, [email protected]
Reinhard BuettnerInstitute for PathologyCIO Cologne Bonnwww.ngm-cancer.com
Disclosures
• Lectures and Advisory boards for: AstraZeneca, Bayer, BMS, Lilly, MSD, Boehringer-Ingelheim, Novartis, Qiagen, Roche, Pfizer
• Co-Founder and Scientific Advisor for TargosMol. Pathol. GmbH
• Testifying Advisor for MSD in GBA-assessmentfor Pembrolizumab
Barretina et al, Nature 483, 2012
The Cancer Cell Line Encyclopediaenables predictive modeling ofanticancer drug sensitivities
Seidel…Wolf, Buettner, Thomas Science Transl Med Oct30th, 2013
~5,000 Lung Cancer Genomesconnected to clinical data (NGM-L)
unknown
KRAS
EGFR
ALKBRAFPIK3CA
HER2 MET RETROS
unknown
FGFR1amp
PTENmut
PTENloss
PIK3CAmut
KRASmut DDR2mut
Adenocarcinoma
Sqamous cell carcinoma
www.lungcancergroup.de
Gene Alteration Frequency
EGFR Mutation 10 – 15%
ALK Rearrangement 3 – 4%
ROS Rearrangement 1%
MET * Ampl/Mut/Rearr. 2-4%
BRAF Mutation 1-3%
HER2 Ampl/Mutation 2-4%
DDR2 Mutation 4%
RET Rearrangement 1%
MEK1 Mutation 1%
FGFR1 Amplification 10%
KRAS Mutation 15-25%
NRAS Mutation 1%
PIK3CA Mutation 1-3%
PTEN Deletion 4%
drugs approved in NSCLCdrugs approved in other cancer
drugs in clinical development
NTRKfusions, NRG-1Immune checkpoint inhibitorsPD-1,PD-L1, CTLR4DLL3-conjugate
* Approval pending
Options for Personalised Therapies for NSCLC
<
<
<
<
<

05.07.2018
2
Molecular Diagnostics Guiding Therapy
What materials are being tested ?
› FFPE from slides orblocks
› Cytology specimens› Peripheral blood
Multiplex PCR panel Hybrid Capture CAIO Panel92 Gene und 14 MSI Marker
Gene Target Gene Target Gene TargetABL1 Exons IDH1 Exons RAC1 Exon 2ALK Breakpoints and Exons IDH2 Exons RAD50 ExonsAPC Exons IGF2R Exons RAD51C ExonsAR Exons JAK2 Exons RB1 Exons
ARAF Exons KDR Exons RET Breakpoints and ExonsATM Exons KEAP1 Exons RHOA Exon 2,3ATR Exons KIF5B Breakpoints RICTOR ExonsBCL6 Exons KIT Exons ROS1 Breakpoints and ExonsBRAF Breakpoints and Exons KNSTRN Exon 1 RPTOR ExonsBRCA1 Exons KRAS Exons SMO ExonsBRCA2 Exons MAP2K1 Exon 2 STK11 ExonsCCND1 Exons MET Breakpoints and Exons TERT ExonsCCNE1 Exons MSH3 Exons TGFBR2 ExonsCD74 Breakpoints MTOR Exons TMPRSS2 Breakpoints CDK4 Exons MYC Exons TP53 ExonsCDK6 Exons MYCL1 Exons TSC1 Exons
CDKN2A Exons MYCN Exons TSC2 ExonsCDKN2B Exons NF1 Exons VHL ExonsCTNNB1 Exons NF2 Exons
EGFR Exons NFE2L2 ExonsEML4 Breakpoints NOTCH1 ExonsERBB2 Exons NOTCH2 ExonsERG Breakpoints NOTCH3 Exons
FGFR1 Whole Gene NR3C1 ExonsFGFR2 Breakpoints and Exons NRAS ExonsFGFR3 Whole Gene NRG1 Whole GeneFLT1 Exons NTRK1 Breakpoints and ExonsFLT4 Exons NTRK2 Breakpoints and Exons
GN A11 Exons NTRK3 Breakpoints and ExonsGN A13 Exons OXA1L Exon 1GNAI2 Exons PDGFRa Breakpoints and ExonsGNAQ Exons PDGFRb Breakpoints and ExonsGNAS Exons PIK3CA ExonsGN AT2 Exons POLD1 ExonsGNG2 Exons POLE3 ExonsHDAC2 Exons PTCH1 ExonsHRAS Exons PTEN Exons
Genpanels: Multiplex PCR versus Hybrid Capture
Heydt et al., Ann Oncol 2016
Detection of Gene Fusions by Hybrid-Capture Panels
Heydt et al., Ann Oncol 2016

05.07.2018
3
The „met-case“Ø High-level amplifications
• MET amplification status in therapy-naïve adeno- and squamous cell carcinomas of the lung.
• Schildhaus HU, Clin Cancer Res 2015
Ø Exon 14 skipping mutations
• Activation of MET via diverse exon 14 splicing alterations occurs in multiple tumor types and confers clinical sensitivity to MET inhibitors.
• Frampton GM, Cancer Discov 2015
Ø Fusions
• Structural Alterations of MET Trigger Response to MET Kinase Inhibition in Lung Adenocarcinoma Patients.
• Plenker D, Clin Cancer Res 2017
3rd gen. EGFR-TKI as 1st line therapy are superiorto 1st gen. inhibitors
Erlotinib, Gefitinib(8-10m)
PD: rebiopsy
T790M Osimertinib (8-10m) EGFRdel 19L858R
Initial biopsy
Osimertinib (18.9m)
OsimertinibStandard EGFR-TKI
HR 0,46(95%KI 0,37; 0,57)p<0,0001
1,0
PFS
0,2
0,4
0,6
0,8
0,0
0 3 6 9 12 15 18 21 24 27
time since randomisation (months)
Median PFS, months (95%KI)18,9 (15,2; 21,4)10,2 (9,6; 11,1)
Soria et al, NEJM 2018
FLAURAPhase IIIOsimertinib vs. Standard EGFR-TKI
Sequential therapy in EGFRmut NSCLC:increasingly molecularly guided
0 6 12 18 24
1st gen. EGFR-TKIPFS: 10 m
Osimertinib PFS: 10 mT790M+
T790M-ChemoPFS: 5m
2nd gen. EGFR-TKI PFS: 14.7 m (dacom.)
T790M+Osimertinib PFS: 10 m
T790M-ChemoPFS: 5m
alternatively: 1st gen.EGFR TKI + bevacizumab: T790M+: PFS 16m / T790M-: PFS 10m
Osimertinib PFS: 19 m
PD: rebiopsy
EGFRC797S
EGFRG724S
hl METamp.
HER2amp.
KRASMut
Targeted therapies
OS ?
Chemo-therapy
Jana Fassunke et al., Second-generation EGFR inhibitors override EGFRG724S-induced osimertinib resistance in lung adenocarcinoma patients, submitted
Ø Osimertinib first-line suppresses emerging T790M, butØ G724S and C797S are the most frequent resistant mutations after
Osimertinib.
05.07.2018
4
Jana Fassunke,…D. Rauh, M. Sos, submittedPeled N, et al. J Thorac Oncol. 2017:12:e81-84.
ALK TKI ROS1 activity
Status Ongoing Studies
Ceritinib Yes FDA approved (4-29-14)EMA approved (5-8-15)
Phase 3(vs chemo)
Alectinib No Approved in Japan(7-4-2014)
FDA Breakthrough TherapyDesignation
Phase 3(vs crizotinib)
Brigatinib* Yes InvestigationalFDA Breakthrough Therapy
Designation
Phase 2
X-396* Yes Investigational Phase 1
TSR-011* No Investigational Phase 1/2a
Entrectinib* Yes Investigational Phase 1/2a
CEP-37440* Unk Investigational Phase 1
Next Gen - ALK inhibitors
*Not licenced in EMA
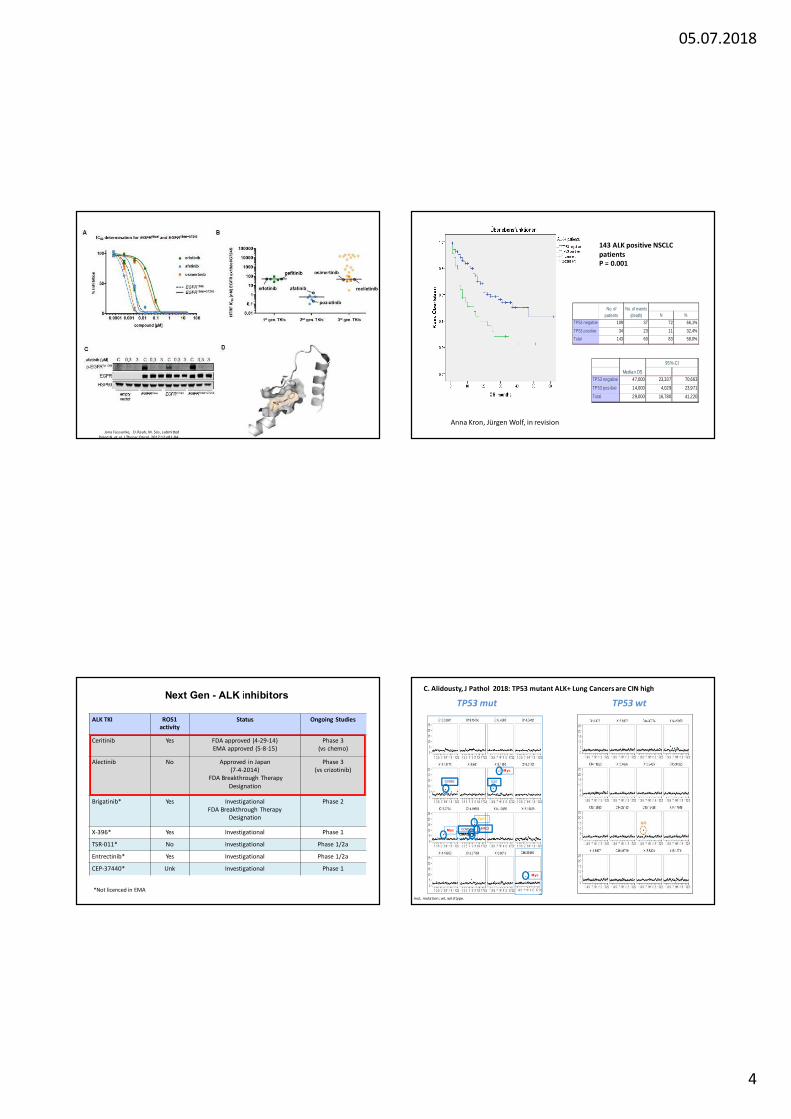
N %TP53 negative 109 37 72 66,1%
TP53 positive 34 23 11 32,4%Total 143 60 83 58,0%
No. of patients
No. of events (death)
TP53 negative 47,000 23,337 70,663TP53 pos itive 14,000 4,029 23,971Total 29,000 16,780 41,220
Median OS
95%-CI
143 ALK positive NSCLC patientsP = 0.001
Anna Kron, Jürgen Wolf, in revision
TP53 mut TP53 wtC. Alidousty, J Pathol 2018: TP53 mutant ALK+ Lung Cancers are CIN high
Myc
CCND1 TERT
Myc
Myc
YAP1
BIRC2CCND1ORAOV1
mut, mutation; wt, wild type.
05.07.2018
5
ALK+ p53 wt:
remain chromosomally stable
ALK+ p53 mut:
reveal high chromosomal instabilityreveal higher TMBreveal shorter responses to TKIs and shorter survival
ALK+ p53 wt:
remain chromosomally stable
ALK+ p53 mut:
reveal high chromosomal instabilityreveal higher TMBreveal shorter responses to TKIs and shorter survival
Do we need to measure
chromosomal instabilitytumor mutational burden ???
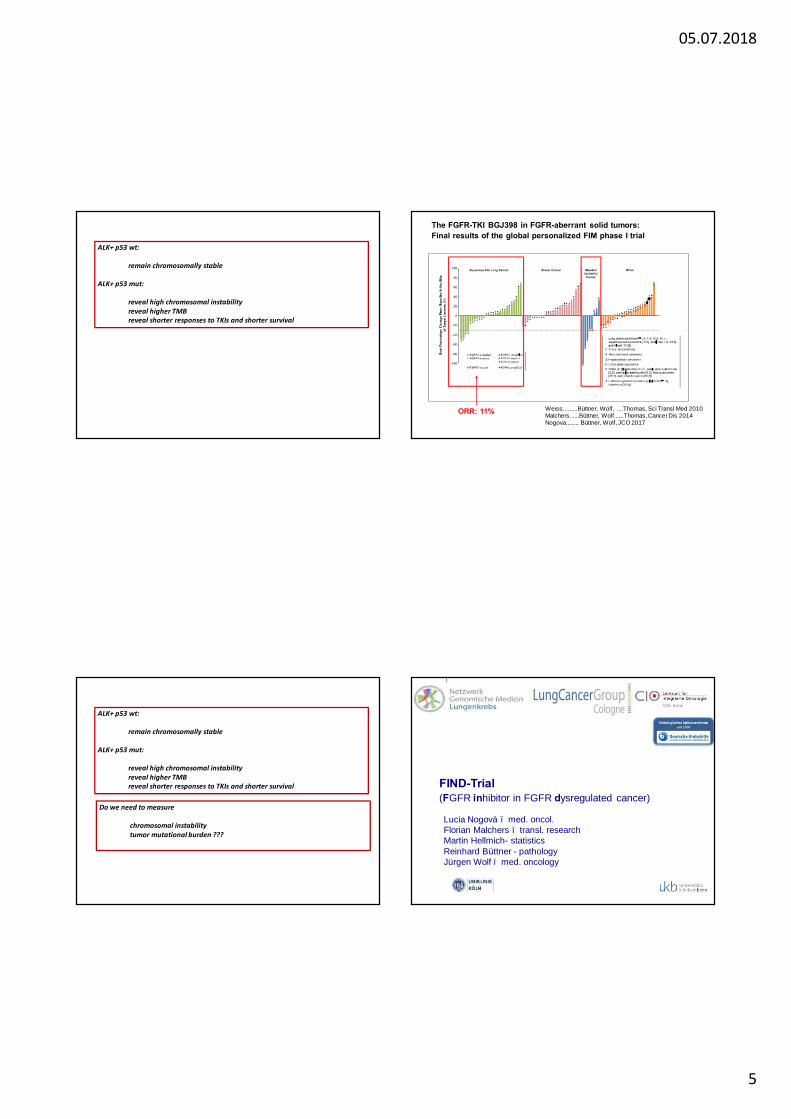
The FGFR-TKI BGJ398 in FGFR-aberrant solid tumors: Final results of the global personalized FIM phase I trial
Weiss, ........Büttner, Wolf, ....Thomas, Sci Transl Med 2010Malchers......Büttner, Wolf......Thomas, Cancer Dis 2014Nogova........ Büttner, Wolf, JCO 2017
ORR: 11%
FIND-Trial (FGFR inhibitor in FGFR dysregulated cancer)
Lucia Nogová – med. oncol. Florian Malchers – transl. researchMartin Hellmich- statisticsReinhard Büttner - pathologyJürgen Wolf – med. oncology

05.07.2018
6
Results of the first German Harmonization-Study PD-L1 IHC09/2016 | Institute of Pathology, University CologneScheel AH et al., Mod Pathol, July2016Scheel AH et al., Histopathology, 2018Scheel AH et al., Der Pathologe, 2016
PD-L1 Harmonization-StudyCologne | 09/2016
PD-L1 Scoring
Scheel AH et al., Der Pathologe 2016. 37(6):557-567
≥1% ≥50%
Harmonization of PD-L1 Assays in German Pathology
• Scheel AH, Harmonized PD-L1 immunohistochemistry for pulmonary squamous-cell andadenocarcinomas. Mod Pathol. 2016 Oct 29.
• Scheel AH, Interlaboratory-concordanceof PD-L1 immunohistochemistry for non-smallcell lung cancer. Histopathology. 2017 Aug 29.
• Scheel AH, Current stateof the art and experiences of the first German harmonizationstudy. Pathologe. 2016 Nov. Review. German.
• George J .. Scheel AH, Genomic Amplification of (CD274/ PD-L1) in Small-Cell Lung Cancer. Clin Cancer Res. 2017 Mar 1.
• Buettner R, …Tsao M. PD-L1 immunohistochemistry testing: a review on analytical assays and clinical implementation in non-small cell lung cancer. J Clin Oncol, Dec 1, 2017.
• Scheel AH: www.pdl1.de
Berlin - Cologne - Dresden - Erlangen - Halle - Hannover - Heidelberg - MunichTargos/Kassel; QuIP/Berlin
05.07.2018
7
Potential New Therapeutic Options
• Pembrolizumab plus Chemotherapy in Metastatic NSCLC, L Gandhi NEJM 2018 KEYNOTE-189.
• > 50% Pembro Monotherapy• 1-49% Pembro + Chemo
• Negative ?? Nivo + Ipi
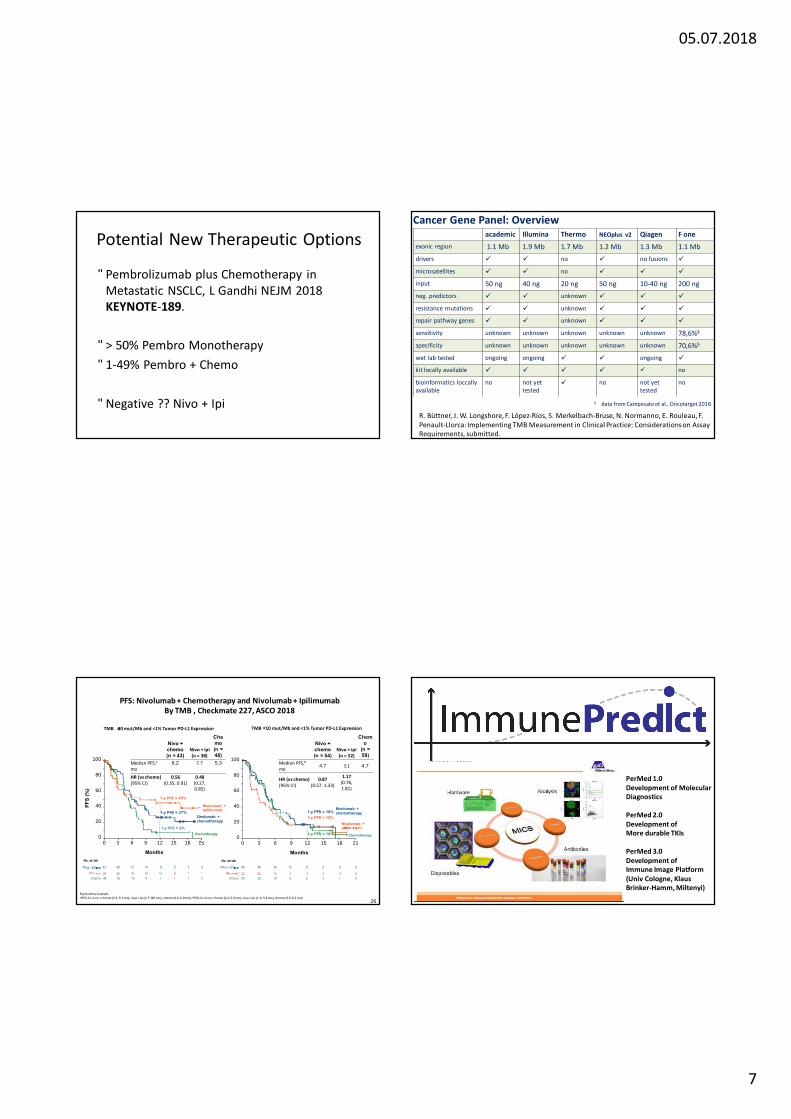
PFS: Nivolumab + Chemotherapy and Nivolumab + Ipilimumab By TMB , Checkmate 227, ASCO 2018
26Exploratory analysisa95% CI: nivo + chemo (4.3, 9.1 mo), nivo + ipi (2.7, NR mo), chemo (4.0, 6.8 mo); b95% CI: nivo + chemo (4.2, 6.9 mo), nivo + ipi (1.6, 5.4 mo), chemo (3.9, 6.2 mo)
Nivolumab + chemotherapy
Nivo + chemo(n = 54)
Nivo + ipi(n = 52)
Chemo
(n = 59)
Median PFS,bmo 4.7 3.1 4.7
HR (vs chemo)(95% CI)
0.87 (0.57, 1.33)
1.17(0.76, 1.81)
Nivolumab + ipilimumab
1-y PFS = 18%1-y PFS = 18%
Months
Chemotherapy1-y PFS = 16%
TMB <10 mut/Mb and <1% Tumor PD-L1 ExpressionTMB ≥10 mut/Mb and <1% Tumor PD-L1 Expression
Nivolumab + chemotherapy
Months
1-y PFS = 45%
1-y PFS = 27%
Nivo + chemo(n = 43)
Nivo + ipi(n = 38)
Chemo(n = 48)
Median PFS,amo
6.2 7.7 5.3
HR (vs chemo)(95% CI)
0.56(0.35, 0.91)
0.48 (0.27, 0.85)
Niv o + chemo
No. at risk
Niv o + ipi 38 20 16 15 10 8 4 143 36 21 14 9 5 2 0
48 30 16 4 1 1 1 0Chemo
0
20
40
60
80
100
0 6 12 183 9 15 21
Chemotherapy1-y PFS = 8%
PFS
(%)
No. at risk
Niv o + ipi 52 22 12 7 5 3 1 059 39 16 6 6 3 1 0Chemo
Niv o + chemo 54 38 19 13 6 3 0 0
Nivolumab + ipilimumab
0
20
40
60
80
100
0 6 12 183 9 15 21
Cancer Gene Panel: Overviewacademic Illumina Thermo NEOplus v2 Qiagen F one
exonic region 1.1 Mb 1.9 Mb 1.7 Mb 1.2 Mb 1.3 Mb 1.1 Mbdrivers ü ü no ü no fusions ü
microsatellites ü ü no ü ü ü
input 50 ng 40 ng 20 ng 50 ng 10-40 ng 200 ngneg. predictors ü ü unknown ü ü ü
resistance mutations ü ü unknown ü ü ü
repair pathway genes ü ü unknown ü ü ü
sensitivity unknown unknown unknown unknown unknown 78,6%§
specificity unknown unknown unknown unknown unknown 70,6%§
wet lab tested ongoing ongoing ü ü ongoing ü
kit locally available ü ü ü ü ü no
bioinformatics loccally available
no not yet tested
ü no not yet tested
no
§ data from Campesato et al., Oncotarget 2016
R. Büttner, J. W. Longshore, F. López-Ríos, S. Merkelbach-Bruse, N. Normanno, E. Rouleau, F. Penault-Llorca: Implementing TMB Measurement in Clinical Practice: Considerations on Assay Requirements, submitted.
PerMed 1.0Development of MolecularDiagnostics
PerMed 2.0Development ofMore durable TKIs
PerMed 3.0Development ofImmune Image Platform(Univ Cologne, Klaus Brinker-Hamm, Miltenyi)

05.07.2018
8
UK-Köln: Patho, Jürgen Wolf, Christiane Bruns, Jens KlussmannMiltenyiFHS-Hamm-Lippe: Klaus Brinker
CD3 (0-2000/mm2): PD1
SummaryEGFR: Osimertinib 1L, EGF816 NGM trialsALK: AlectinibEGF/HER2: exon 20, TAK788MET: Capmatinib
KN 189: 1+49% PD-L1 Pembro/Chemo
Checkmate 227: Ipi, Nivo in TMB high
Predictive Diagnostics for Selection of Patients for Lung Cancer Therapies:
Immune Markers: PD-L1Comprehensive Molecular Hybrid Capture PanelsTME Markers, ImmunePredict
Task Force 1a/bMol. DiagnosticsQC
Task Force 2DocumentationEvaluation
Task Force 3Medical ReportsCouncelling
Task Force 4
Clinical TrialsTask Force 5ReimbursementHC Providers
Task Force 6
Research

05.07.2018
9
Teaming up for ROSBärbel Söhlke | Facebookhttps://de-de.facebook.com/barbel.sohlkeCIO-KölnBonn
Thank you for your attention
Molecular Pathology Diagnostics Group CologneSabine Merkelbach-Bruse, Axel Hillmer,Jürgen Wolf, Roman Thomas – DKH, BMBF, LifeSciences-NRW














![Topoisomerase II-Alpha Index Predicts the Efficacy of ......expressions nor gene amplifications of HER2 and TOPOIIα had any correlation with the therapeutic effect [12]. Meanwhile,](https://img.dokumen.tips/doc/110x75/5f9b91d85176e551ec794be8/topoisomerase-ii-alpha-index-predicts-the-efficacy-of-expressions-nor-gene.jpg)














