Embed Size (px)
Citation preview
Bronchial thermoplasty or biological targeted therapies for severe uncontrolled asthma
Pascal Chanez,
Aix Marseille Université, Clinique des bronches, allergie et sommeil/ APHM, Marseille
Laboratoire d'Immunologie /INSERM U1067/CNRS UMR 7733
COI DisclosureP.C. has provided consultancy services forSNCF, BI, Centocor, GSK, MSD, AZ, Novartis,Teva, Chiesi, and Boston Sci; has served onadvisory boards for ALK, BI, Centocor, GSK,AZ, Novartis, Teva, Chiesi, and Boston ScMSD; has received lecture fees from ALKl, BI,Centocor, GSK, AZ, Novartis, Teva,Chiesi,,MSD; and has received industry-sponsored grants from Roche, BI, Centocor,
GSK, AZ, Novartis, Teva, Chiesi;.
Severe Asthma Management
Better Understanding
Better Management
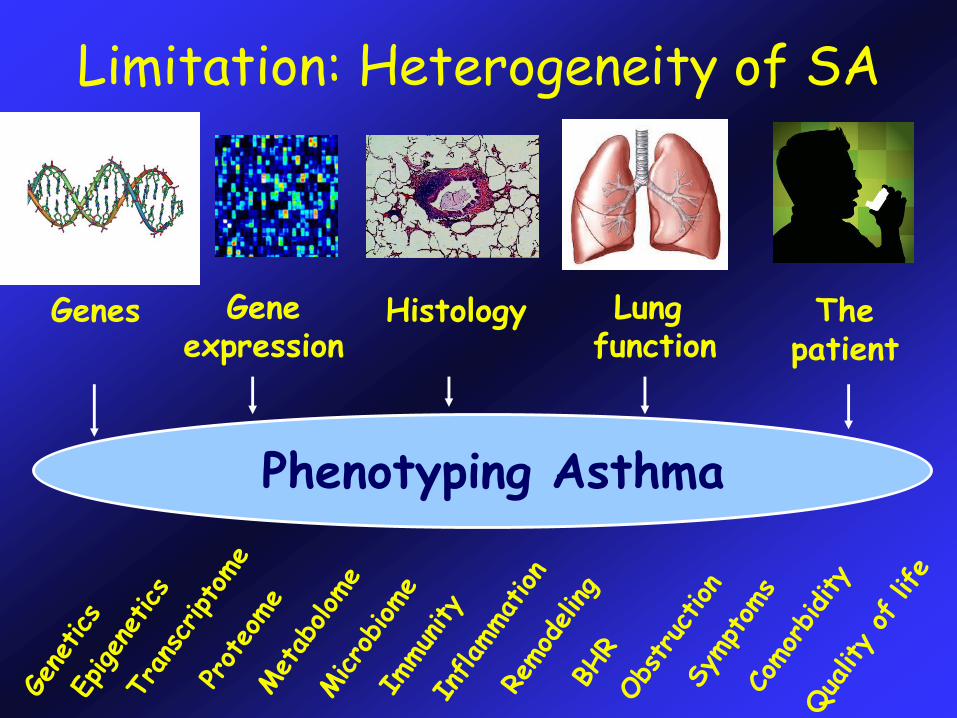
Limitation: Heterogeneity of SA
Genes Geneexpression
Histology Lung function
Thepatient
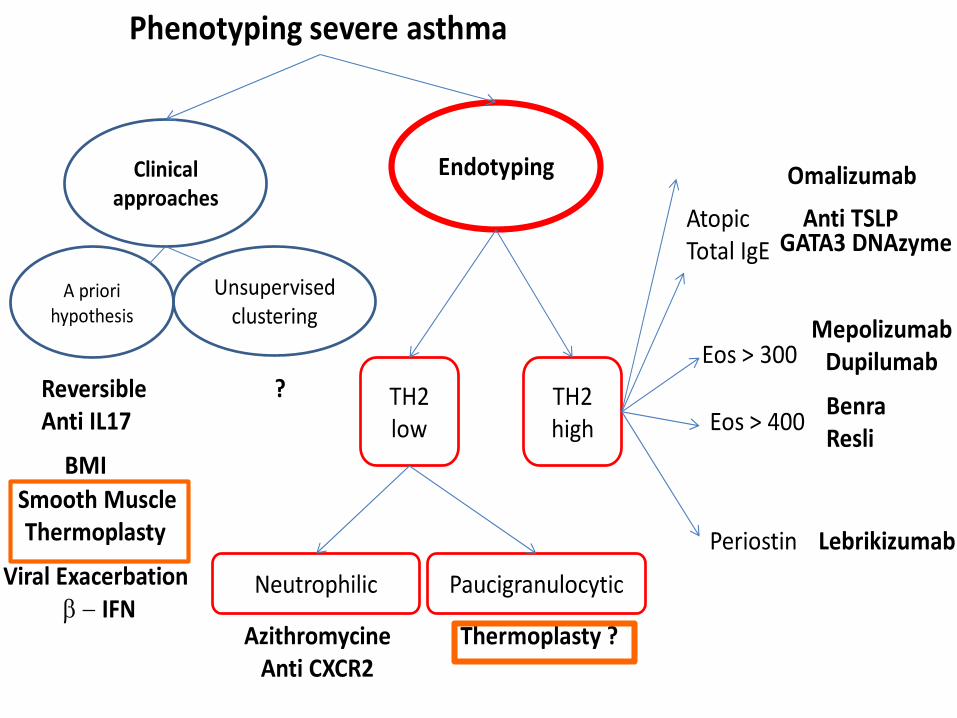
Phenotyping Asthma
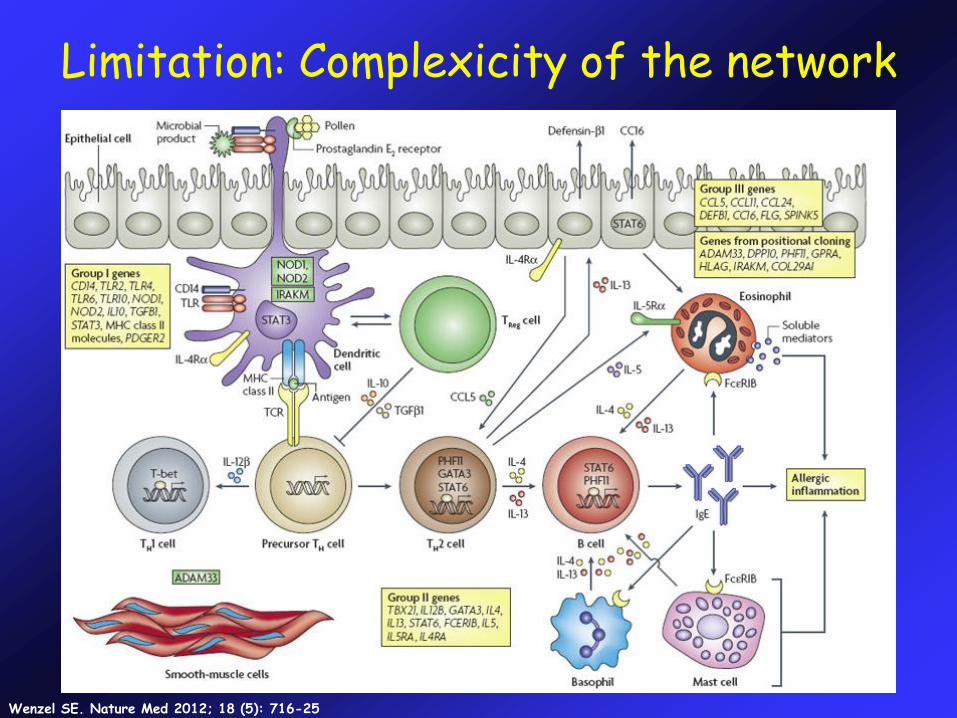
Limitation: Complexicity of the network
Wenzel SE. Nature Med 2012; 18 (5): 716-25
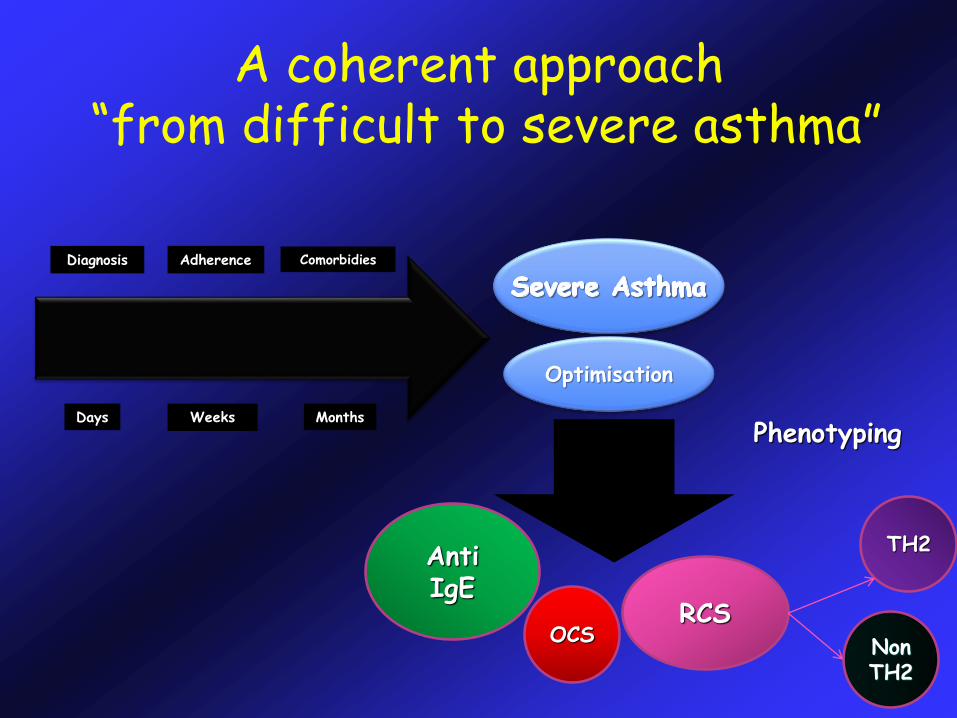
A coherent approach“from difficult to severe asthma”
Diagnosis Adherence Comorbidies
Days Weeks Months
Anti IgE
OCSRCS
TH2
Non TH2
Optimisation
Phenotyping
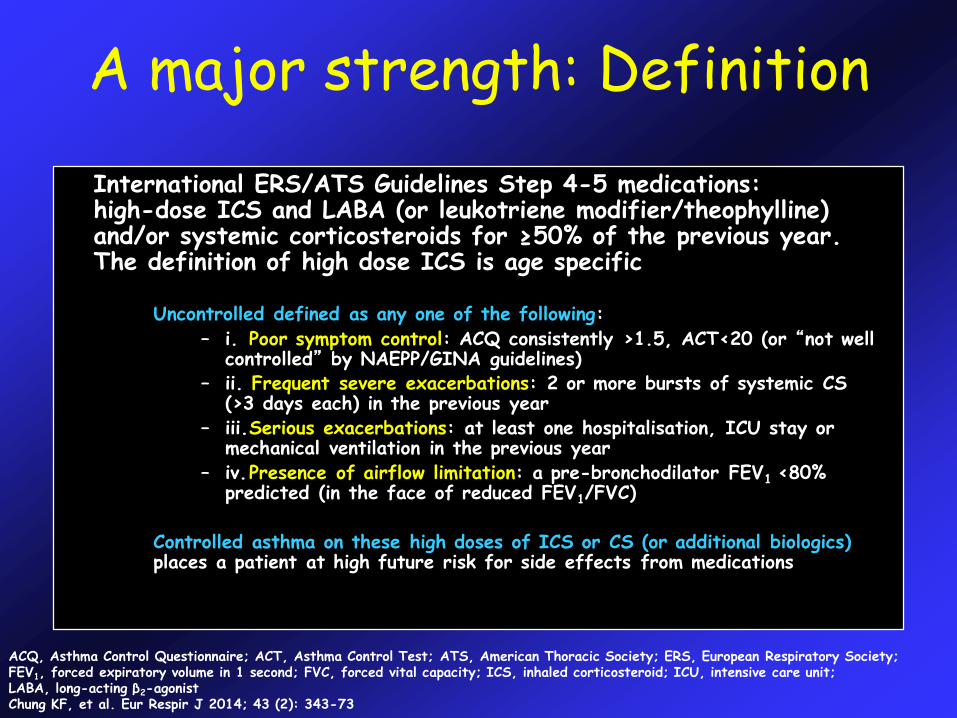
A major strength: Definition
International ERS/ATS Guidelines Step 4-5 medications: high-dose ICS and LABA (or leukotriene modifier/theophylline) and/or systemic corticosteroids for ≥50% of the previous year. The definition of high dose ICS is age specific
Uncontrolled defined as any one of the following:
– i. Poor symptom control: ACQ consistently >1.5, ACT<20 (or “not well controlled” by NAEPP/GINA guidelines)
– ii. Frequent severe exacerbations: 2 or more bursts of systemic CS (>3 days each) in the previous year
– iii.Serious exacerbations: at least one hospitalisation, ICU stay or mechanical ventilation in the previous year
– iv.Presence of airflow limitation: a pre-bronchodilator FEV1 <80% predicted (in the face of reduced FEV1/FVC)
Controlled asthma on these high doses of ICS or CS (or additional biologics) places a patient at high future risk for side effects from medications
ACQ, Asthma Control Questionnaire; ACT, Asthma Control Test; ATS, American Thoracic Society; ERS, European Respiratory Society; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; ICS, inhaled corticosteroid; ICU, intensive care unit; LABA, long-acting β2-agonistChung KF, et al. Eur Respir J 2014; 43 (2): 343-73
Revise the definition of severe asthma;
Discuss phenotypes of severe asthma;
Provide guidance on management, diagnosis,
evaluation and treatment of severe asthma;
Developed according to GRADE methodology
transparent and trustworthy;
Need regular updates for optimal validity
living document PERSONALISED ?
ERS / ATS Guidelines on severe asthma
Chung et al. Eur Respir J 2014
Definitions+++++
Identifies those withhighest unmet needProvides criteria forreferral to expertcentersAllows positioning of newhigh cost therapiesbiologics andthermoplastyFocusses research withattention to phenotypingand personalisedmedicine
LimitationsDoes not identify aspecific severe asthmaendotype is severeasthma a distinct entity?Relies on inadequateresponse to currenttherapyFocus on subjectivemeasures of control andexacerbations
Adapted from CE Brightling
Better Understanding
Better Management
Personalise Phenotype EndotypePartnership
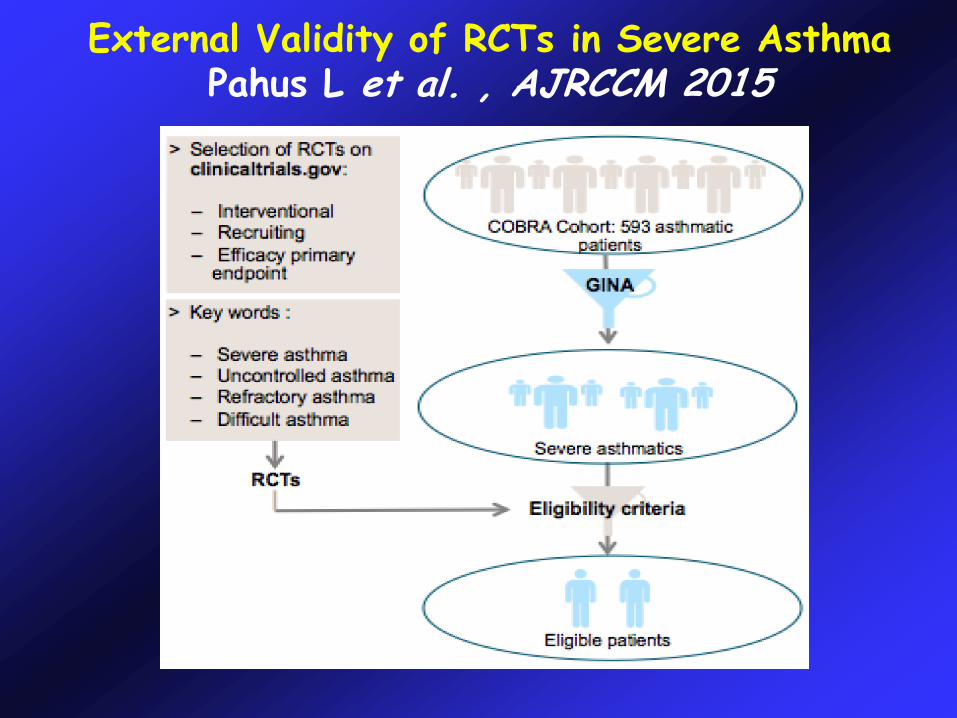
External Validity of RCTs in Severe AsthmaPahus L et al. , AJRCCM 2015
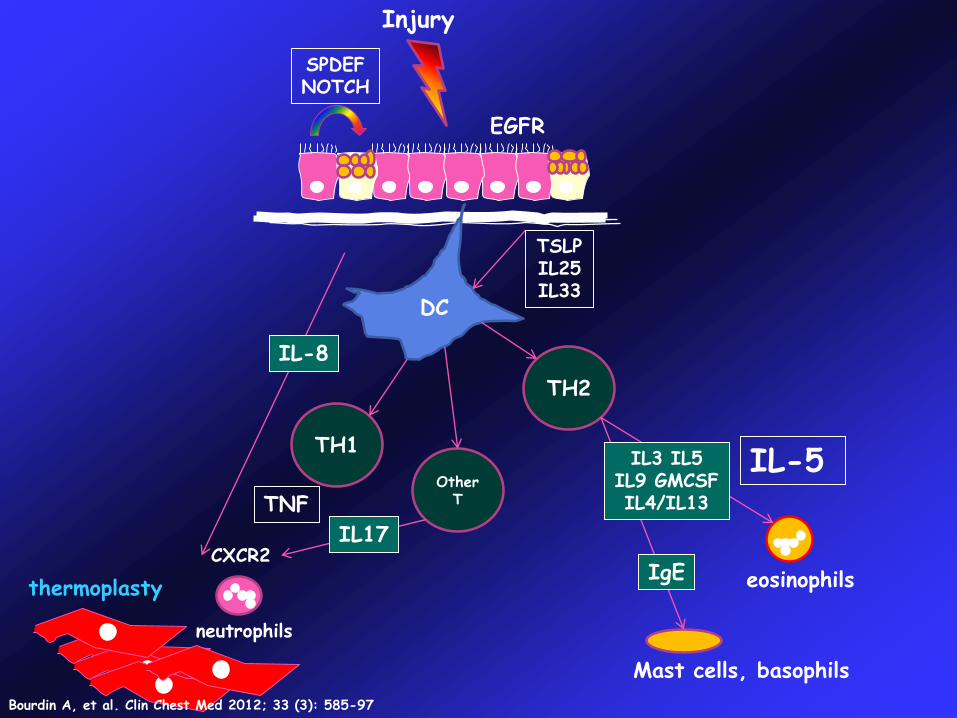
Injury
DC
TH1
OtherT
TH2
IL-5
IL-8
TSLPIL25IL33
IgE
Mast cells, basophils
eosinophilsCXCR2
neutrophils
IL3 IL5IL9 GMCSFIL4/IL13
SPDEFNOTCH
IL17
TNF
EGFR
thermoplasty
Bourdin A, et al. Clin Chest Med 2012; 33 (3): 585-97
TH2-drive
n ast
hma
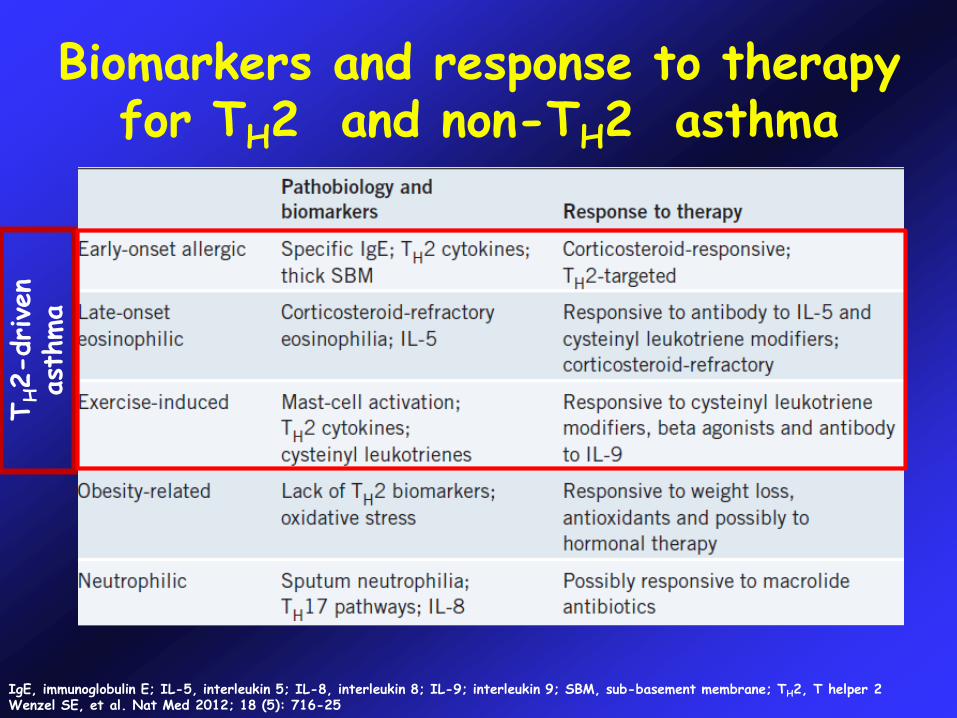
IgE, immunoglobulin E; IL-5, interleukin 5; IL-8, interleukin 8; IL-9; interleukin 9; SBM, sub-basement membrane; TH2, T helper 2Wenzel SE, et al. Nat Med 2012; 18 (5): 716-25
Biomarkers and response to therapy for TH2 and non-TH2 asthma
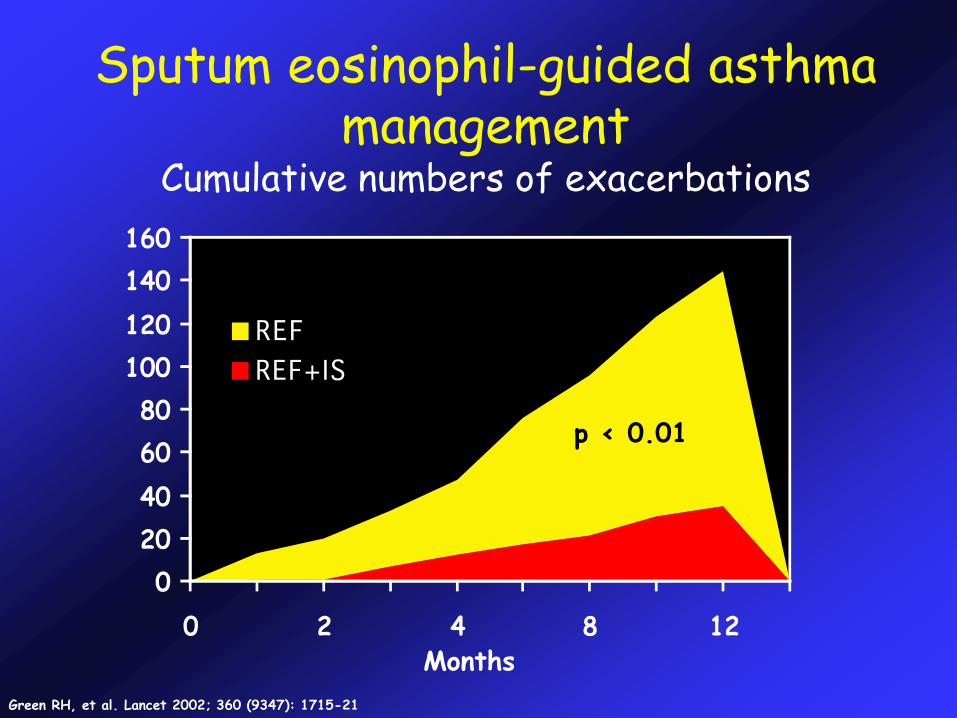
Sputum eosinophil-guided asthma management
Cumulative numbers of exacerbations
p < 0.01
Months
Green RH, et al. Lancet 2002; 360 (9347): 1715-21
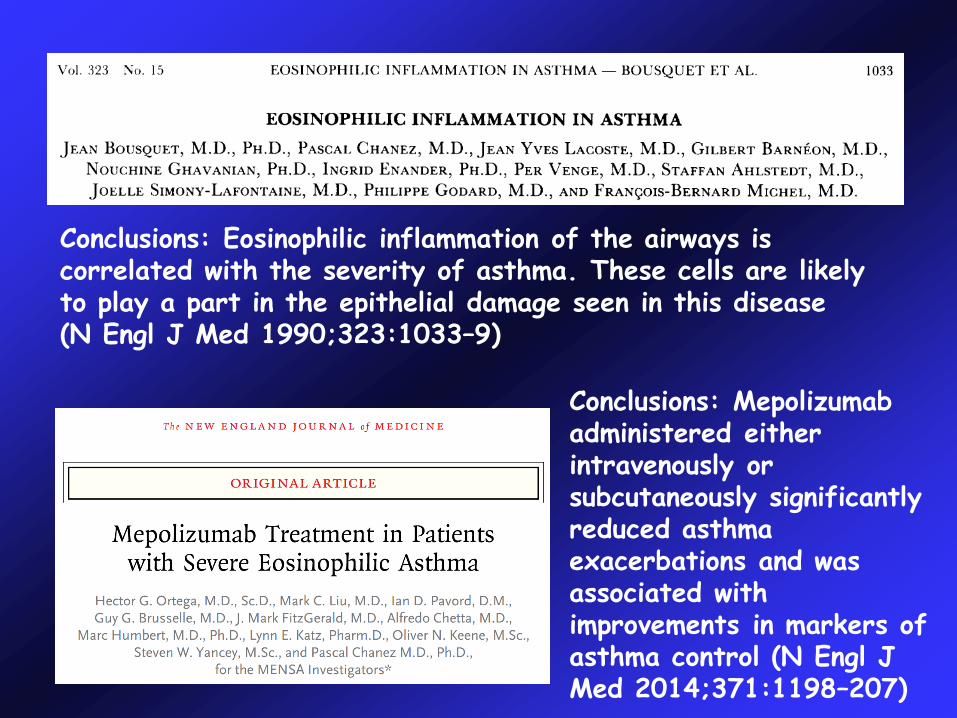
Conclusions: Eosinophilic inflammation of the airways is correlated with the severity of asthma. These cells are likely to play a part in the epithelial damage seen in this disease (N Engl J Med 1990;323:1033–9)
Conclusions: Mepolizumabadministered either intravenously or subcutaneously significantly reduced asthma exacerbations and was associated with improvements in markers of asthma control (N Engl J Med 2014;371:1198–207)
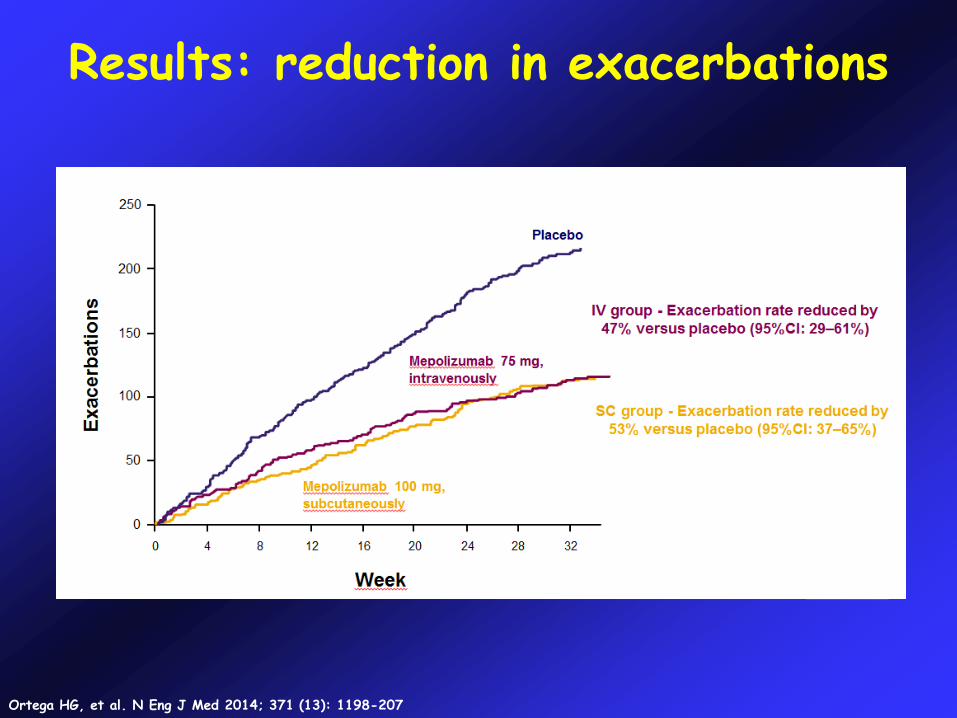
Results: reduction in exacerbations
Ortega HG, et al. N Eng J Med 2014; 371 (13): 1198-207
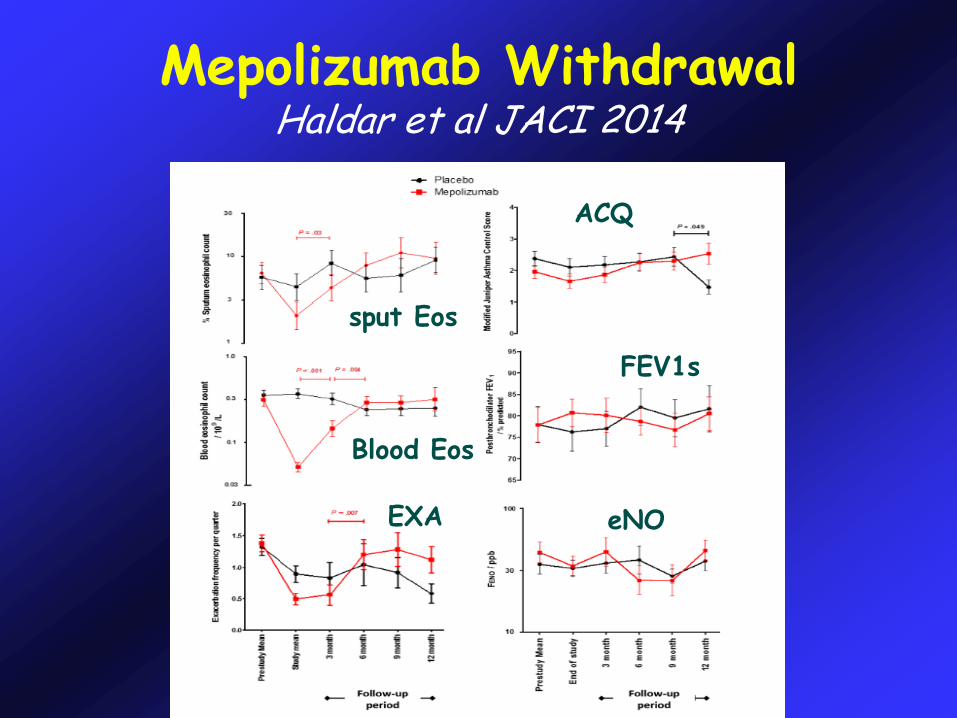
Mepolizumab WithdrawalHaldar et al JACI 2014
Blood Eos
EXA
sput Eos
eNO
FEV1s
ACQ
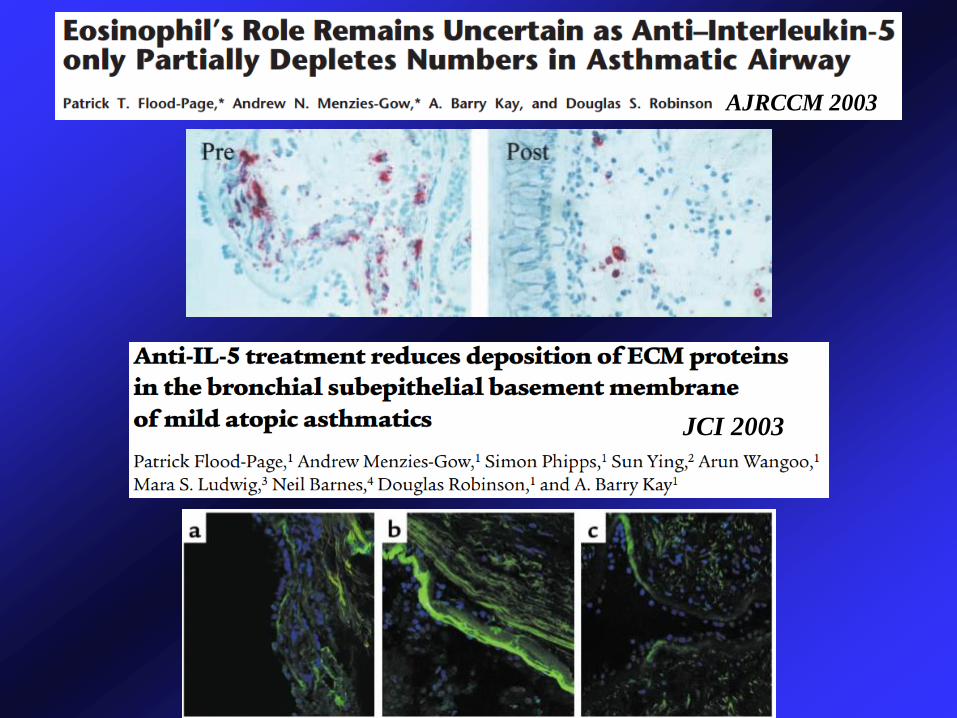
JCI 2003
AJRCCM 2003
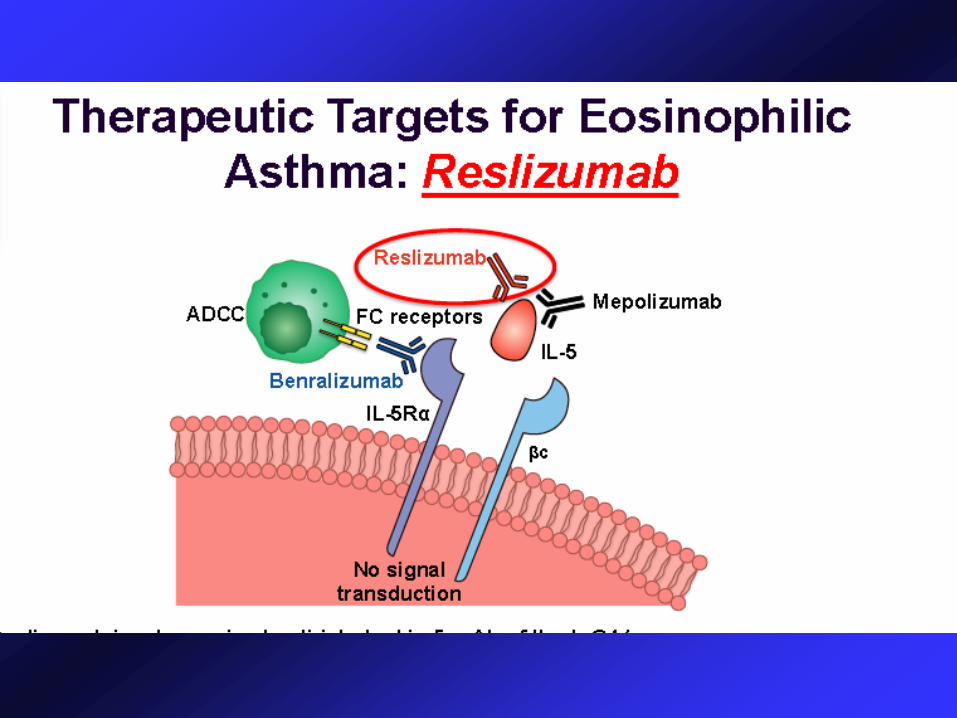
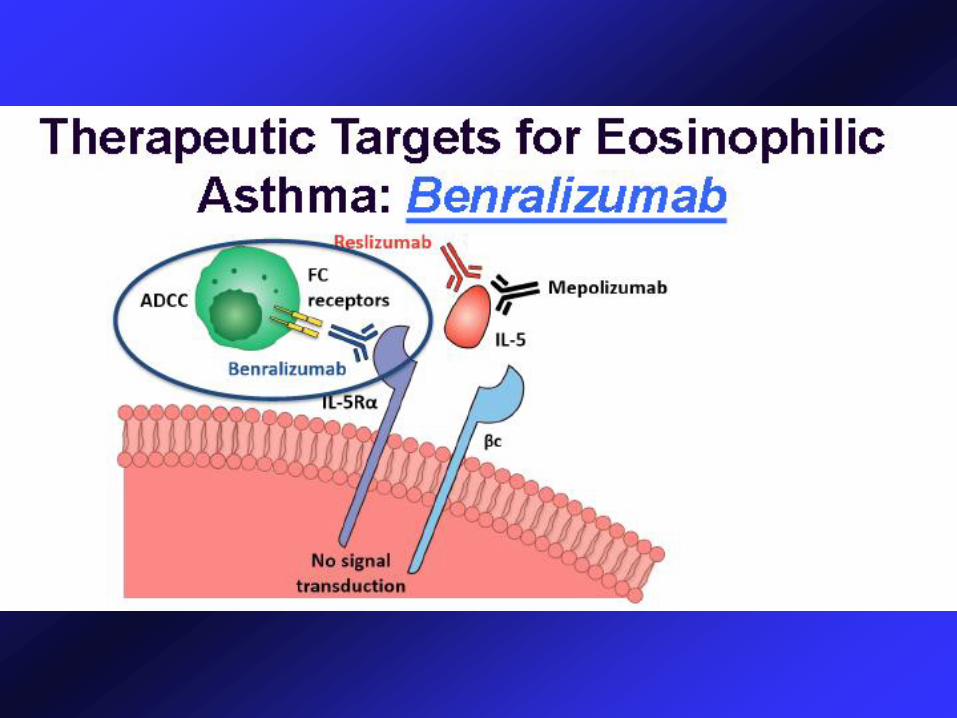
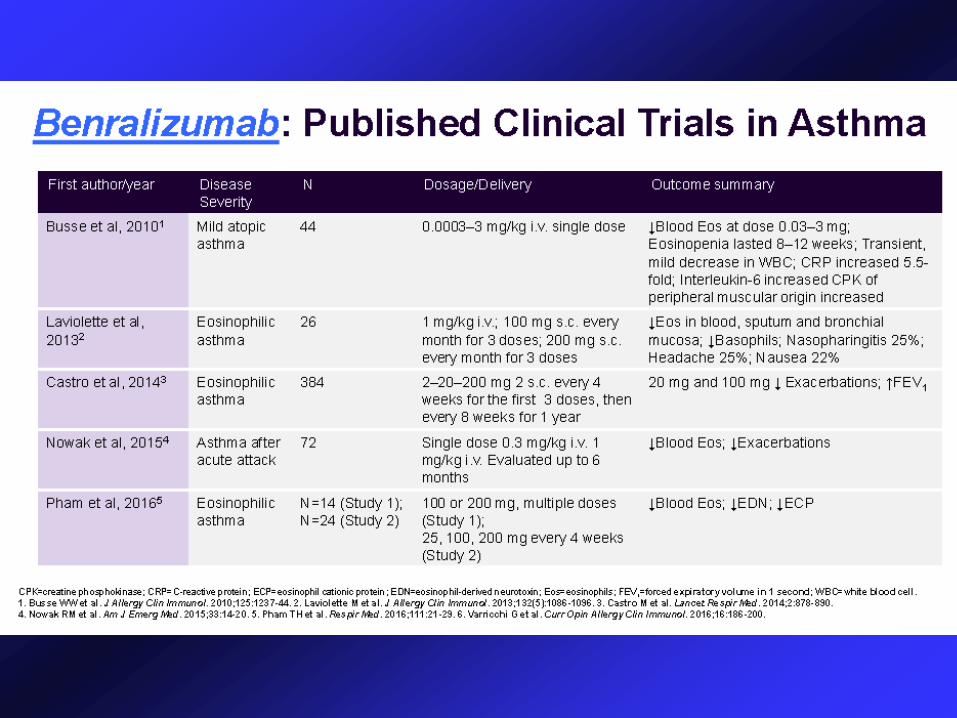
Benralizumab
IL-5 Receptors antagonist
Dosing
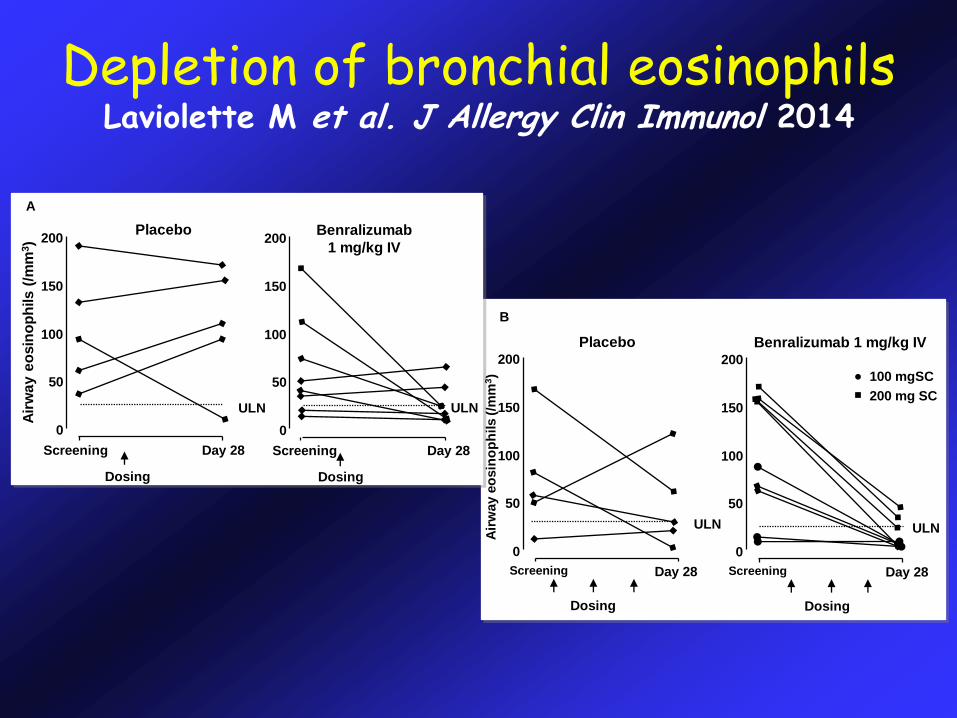
Depletion of bronchial eosinophilsLaviolette M et al. J Allergy Clin Immunol 2014
Screening
Dosing
Day 28
0
50
100
150
200Benralizumab
1 mg/kg IV
ULN
Screening Day 28
0
50
100
150
200
B
Placebo
Air
way e
osin
op
hils (/m
m3)
Screening
Dosing
Day 28
0
50
100
150
200
Benralizumab 1 mg/kg IV
100 mgSC
200 mg SCULNULN
Screening
Dosing
Day 28
0
50
100
150
200
A
Placebo
Air
wa
y e
osin
op
hils (
/mm
3)
ULN
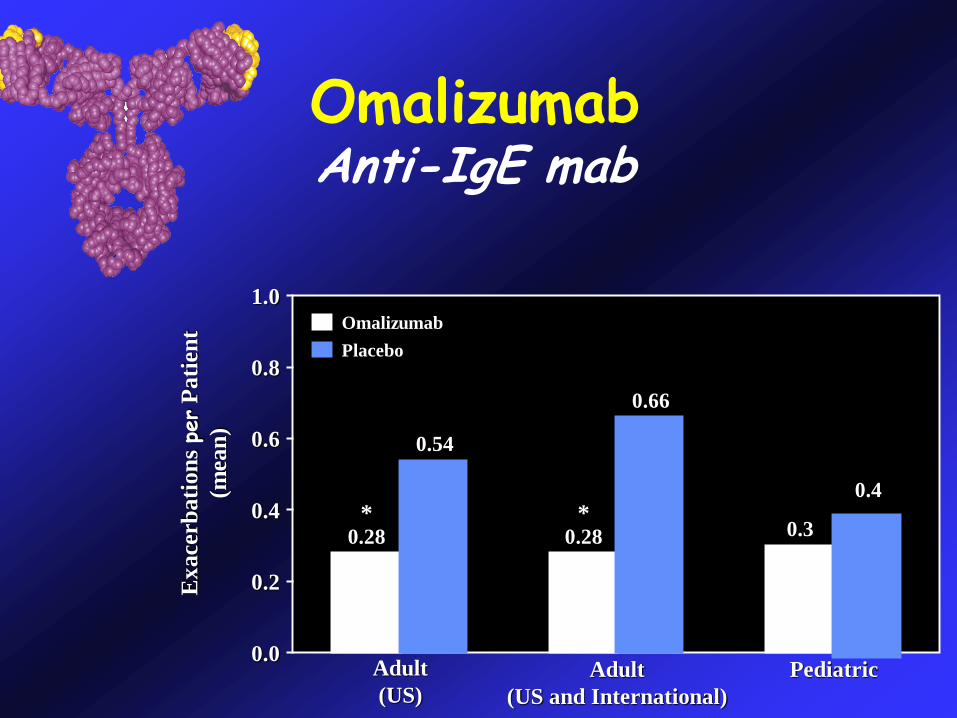
OmalizumabAnti-IgE mab
0.8
0.6
0.4
0.2
0.0Adult
(US)
Adult
(US and International)
Pediatric
Ex
ace
rbati
on
s pe
rP
ati
ent
(mea
n)
1.0Omalizumab
Placebo
0.28 0.28 0.3
0.54
0.66
0.4
**
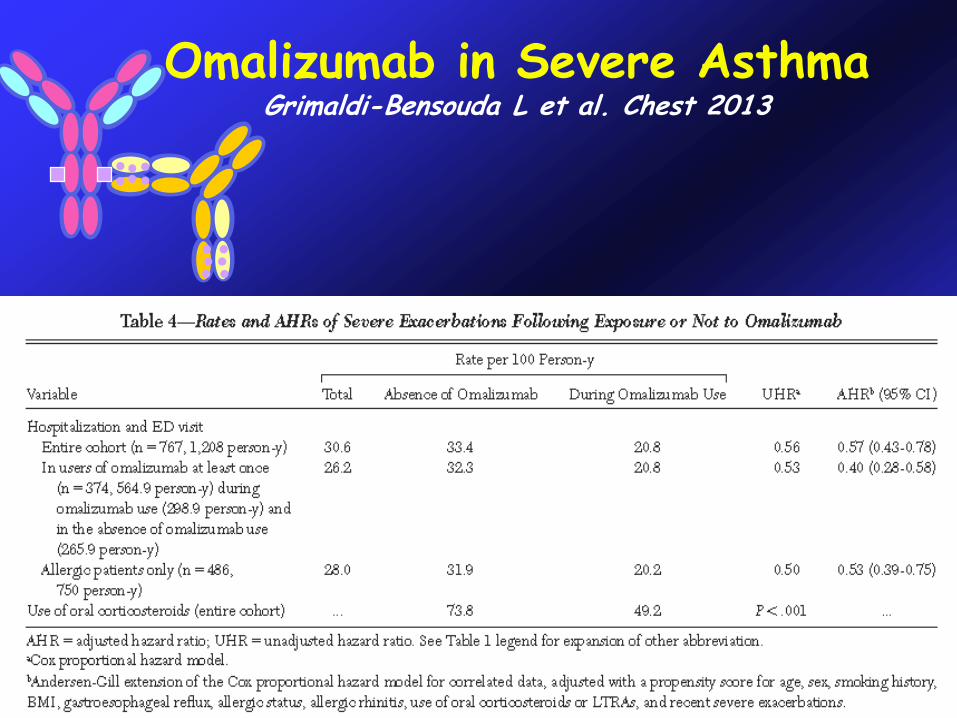
Omalizumab in Severe AsthmaGrimaldi-Bensouda L et al. Chest 2013
-53
-32 -30
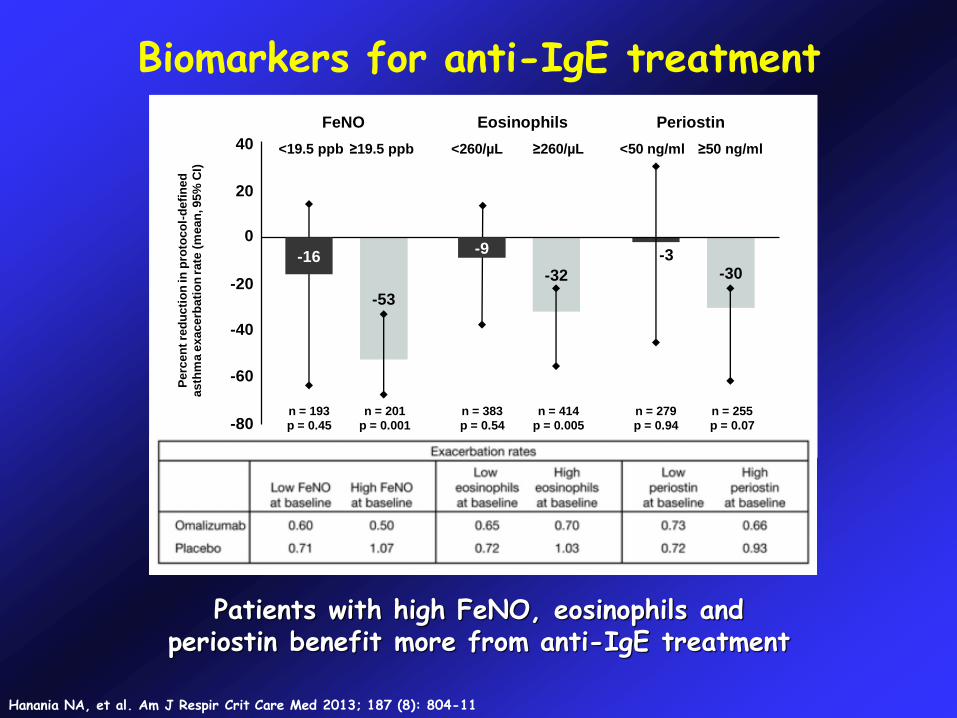
Patients with high FeNO, eosinophils and periostin benefit more from anti-IgE treatment
Biomarkers for anti-IgE treatment
Hanania NA, et al. Am J Respir Crit Care Med 2013; 187 (8): 804-11
-80
-60
-40
-20
0
20
40
FeNO Eosinophils Periostin
<19.5 ppb ≥19.5 ppb <260/µL ≥260/µL <50 ng/ml ≥50 ng/ml
n = 193
p = 0.45
n = 201
p = 0.001
n = 383
p = 0.54
n = 414
p = 0.005
n = 279
p = 0.94
n = 255
p = 0.07
Perc
en
t re
du
cti
on
in
pro
toco
l-d
efi
ned
asth
ma e
xacerb
ati
on
rate
(m
ean
, 95%
CI)
-3-16-9
% o
f P
art
icip
an
ts w
ith
Exacerb
ati
on
s
(n=211)
(n=208)
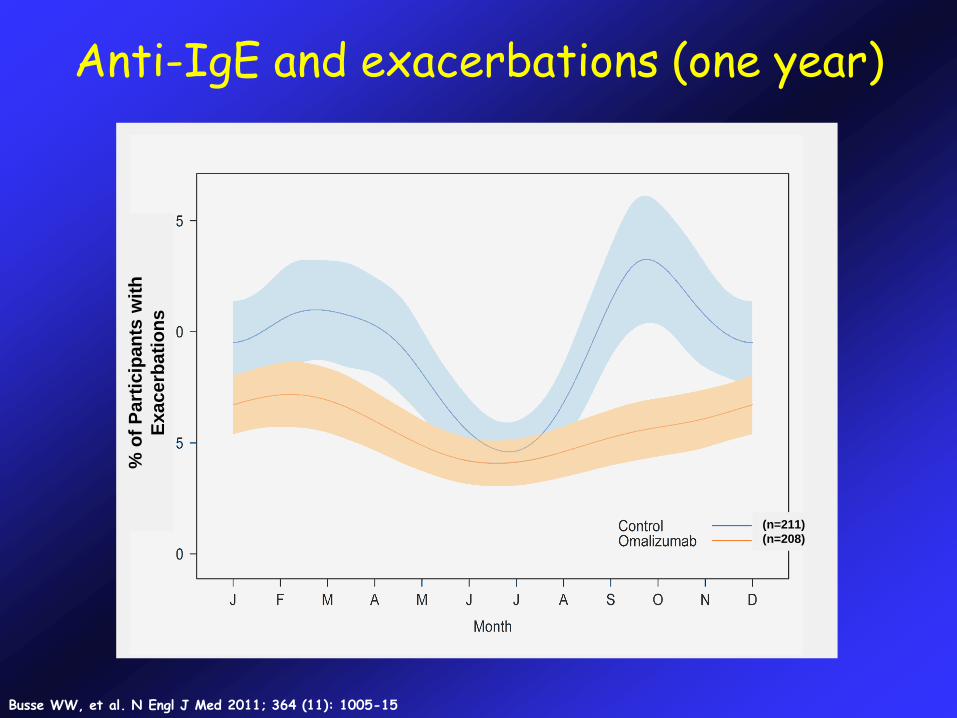
Anti-IgE and exacerbations (one year)
Busse WW, et al. N Engl J Med 2011; 364 (11): 1005-15
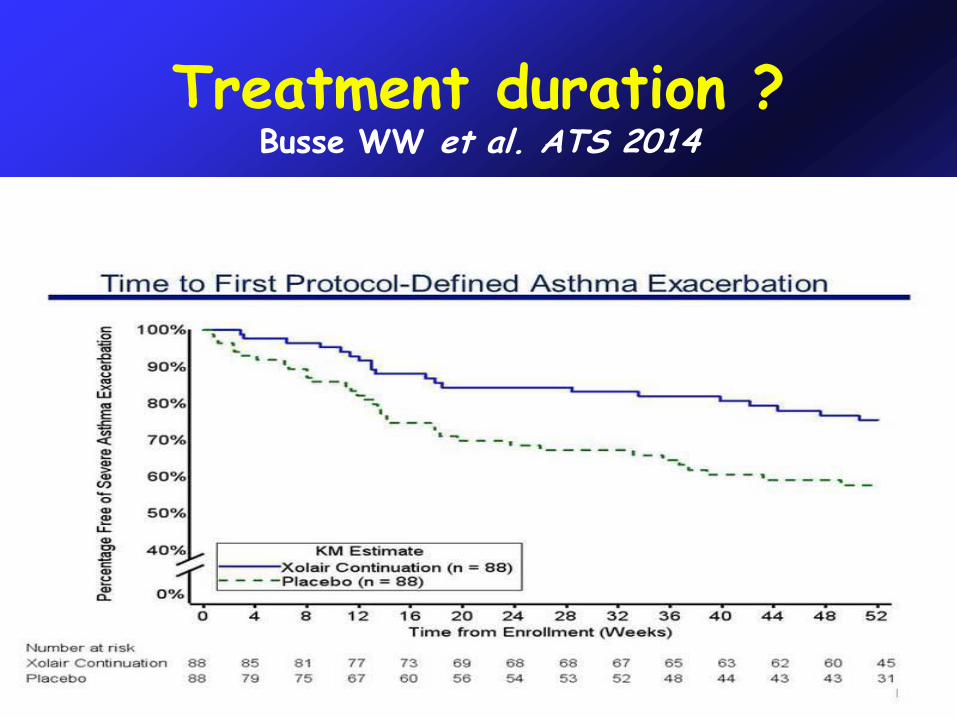
Treatment duration ?Busse WW et al. ATS 2014
LebrikizumabTralokinumab
m-AB anti-IL13
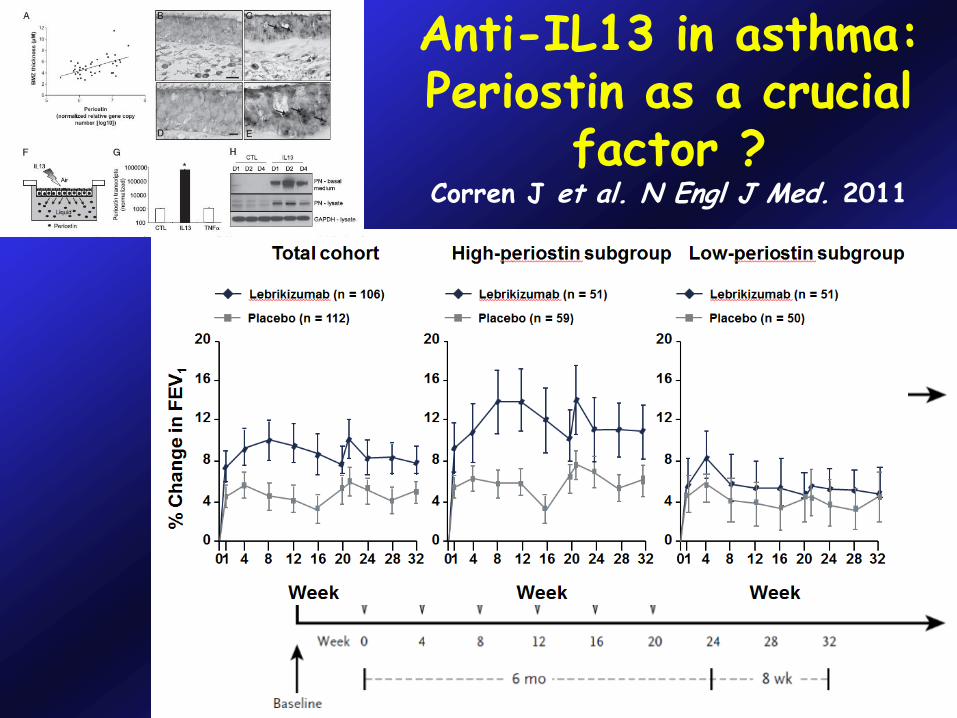
Anti-IL13 in asthma:Periostin as a crucial
factor ?Corren J et al. N Engl J Med. 2011
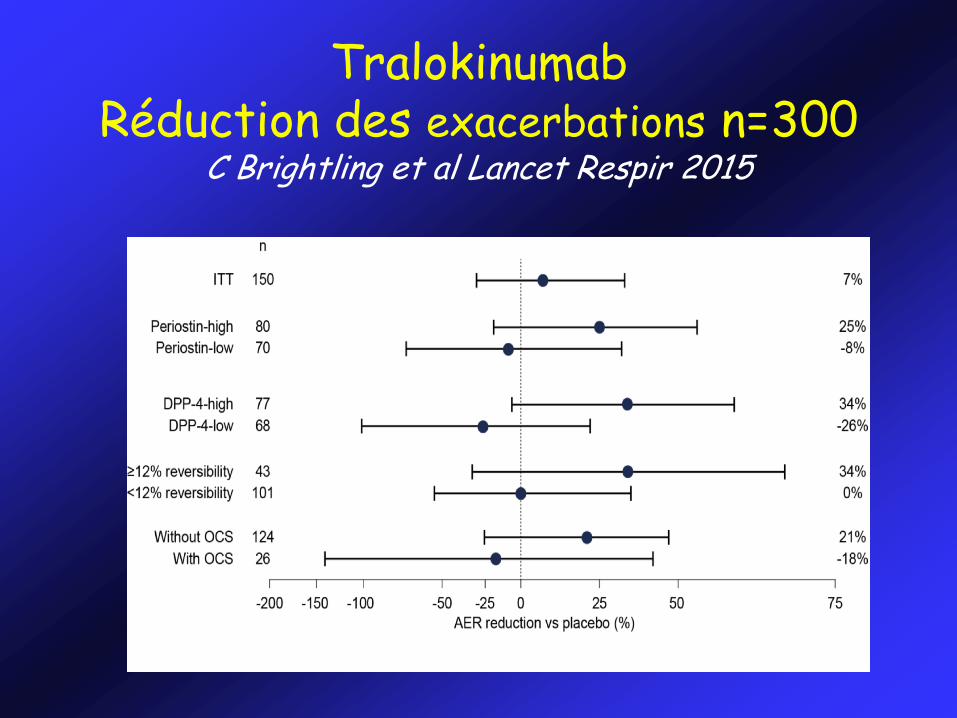
Tralokinumab Réduction des exacerbations n=300
C Brightling et al Lancet Respir 2015
Dupilumab
m-AB anti-IL-4R
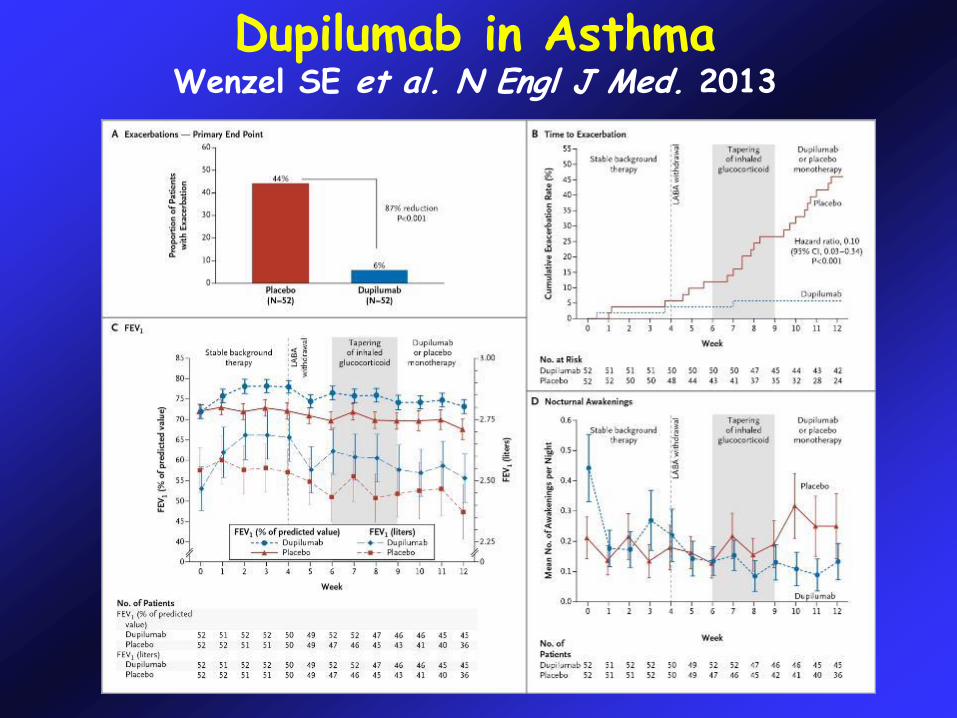
Dupilumab in AsthmaWenzel SE et al. N Engl J Med. 2013
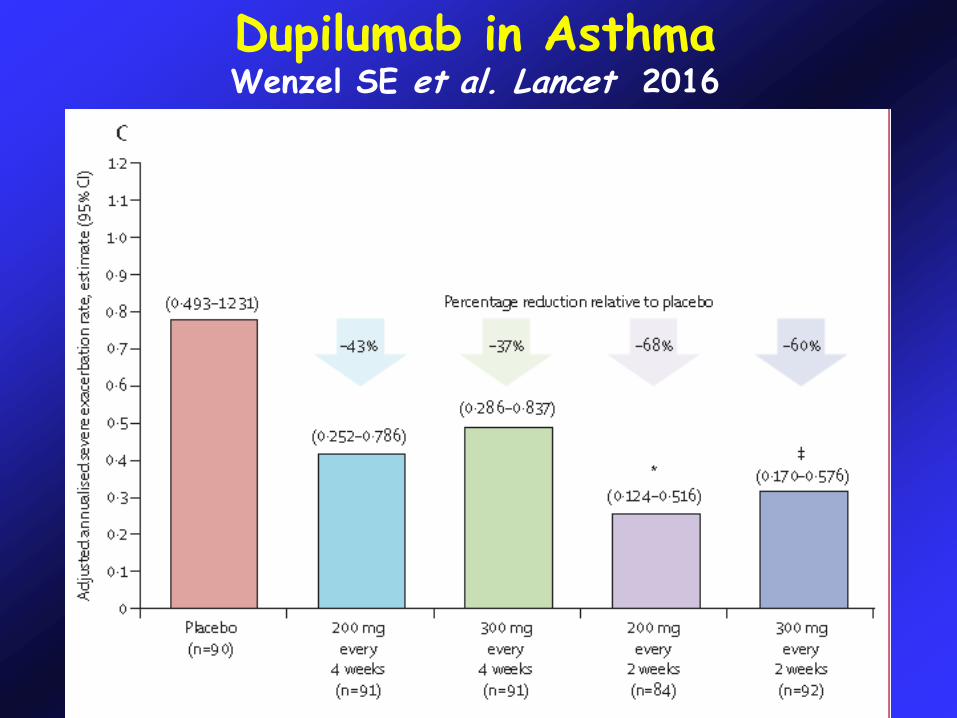
Dupilumab in AsthmaWenzel SE et al. Lancet 2016
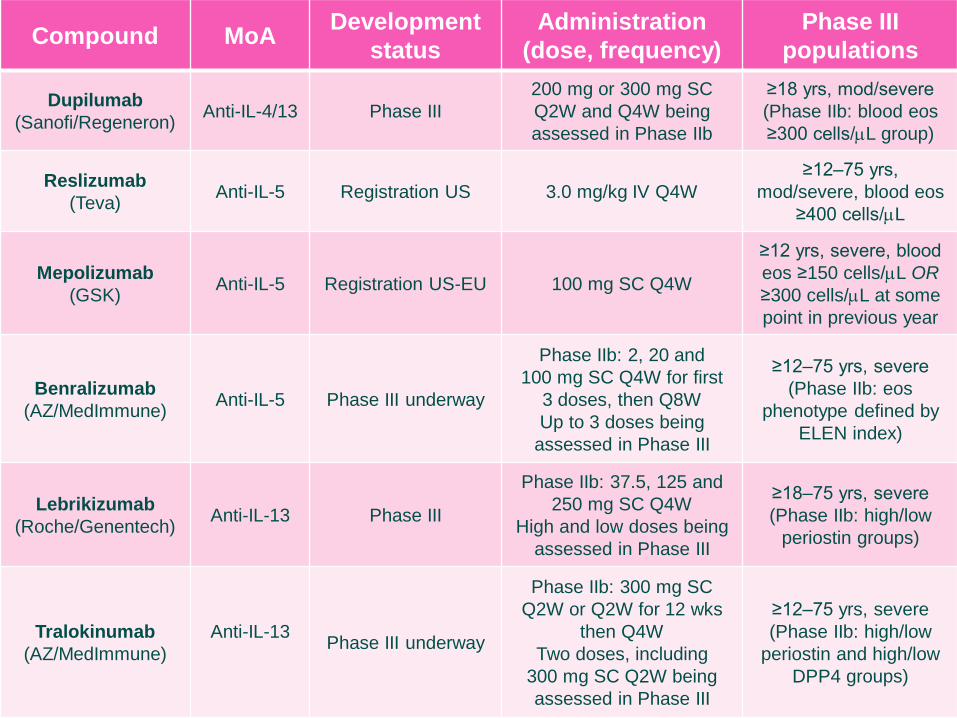
Compound MoADevelopment
status
Administration
(dose, frequency)
Phase III
populations
Dupilumab
(Sanofi/Regeneron)Anti-IL-4/13 Phase III
200 mg or 300 mg SC
Q2W and Q4W being
assessed in Phase IIb
≥18 yrs, mod/severe
(Phase IIb: blood eos
≥300 cells/L group)
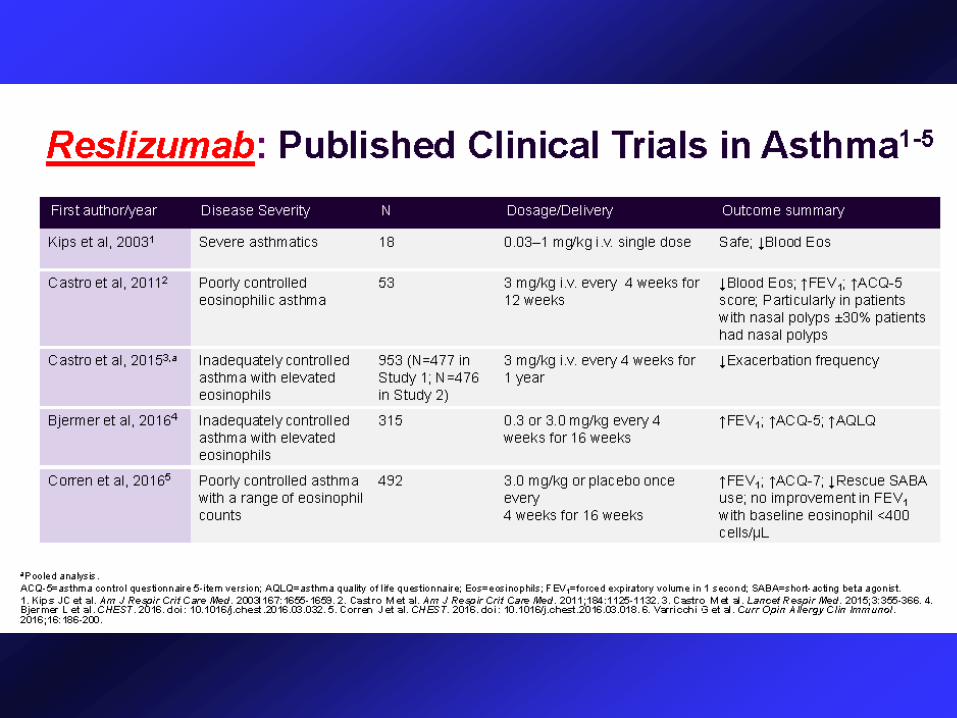
Reslizumab
(Teva)Anti-IL-5 Registration US 3.0 mg/kg IV Q4W
≥12‒75 yrs,
mod/severe, blood eos
≥400 cells/L
Mepolizumab
(GSK)Anti-IL-5 Registration US-EU 100 mg SC Q4W
≥12 yrs, severe, blood
eos ≥150 cells/L OR
≥300 cells/L at some
point in previous year
Benralizumab
(AZ/MedImmune)Anti-IL-5 Phase III underway
Phase IIb: 2, 20 and
100 mg SC Q4W for first
3 doses, then Q8W
Up to 3 doses being
assessed in Phase III
≥12‒75 yrs, severe
(Phase IIb: eos
phenotype defined by
ELEN index)
Lebrikizumab
(Roche/Genentech)Anti-IL-13 Phase III
Phase IIb: 37.5, 125 and
250 mg SC Q4W
High and low doses being
assessed in Phase III
≥18‒75 yrs, severe
(Phase IIb: high/low
periostin groups)
Tralokinumab
(AZ/MedImmune)
Anti-IL-13Phase III underway
Phase IIb: 300 mg SC
Q2W or Q2W for 12 wks
then Q4W
Two doses, including
300 mg SC Q2W being
assessed in Phase III
≥12‒75 yrs, severe
(Phase IIb: high/low
periostin and high/low
DPP4 groups)
NON T
H2-
drive
n ast
hma
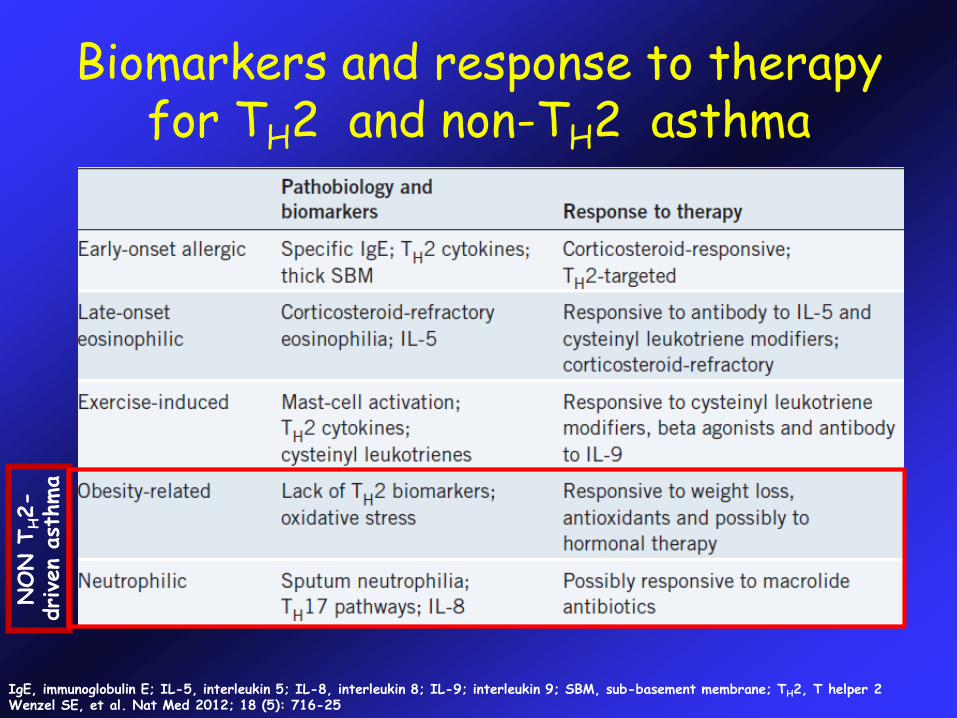
IgE, immunoglobulin E; IL-5, interleukin 5; IL-8, interleukin 8; IL-9; interleukin 9; SBM, sub-basement membrane; TH2, T helper 2Wenzel SE, et al. Nat Med 2012; 18 (5): 716-25
Biomarkers and response to therapy for TH2 and non-TH2 asthma
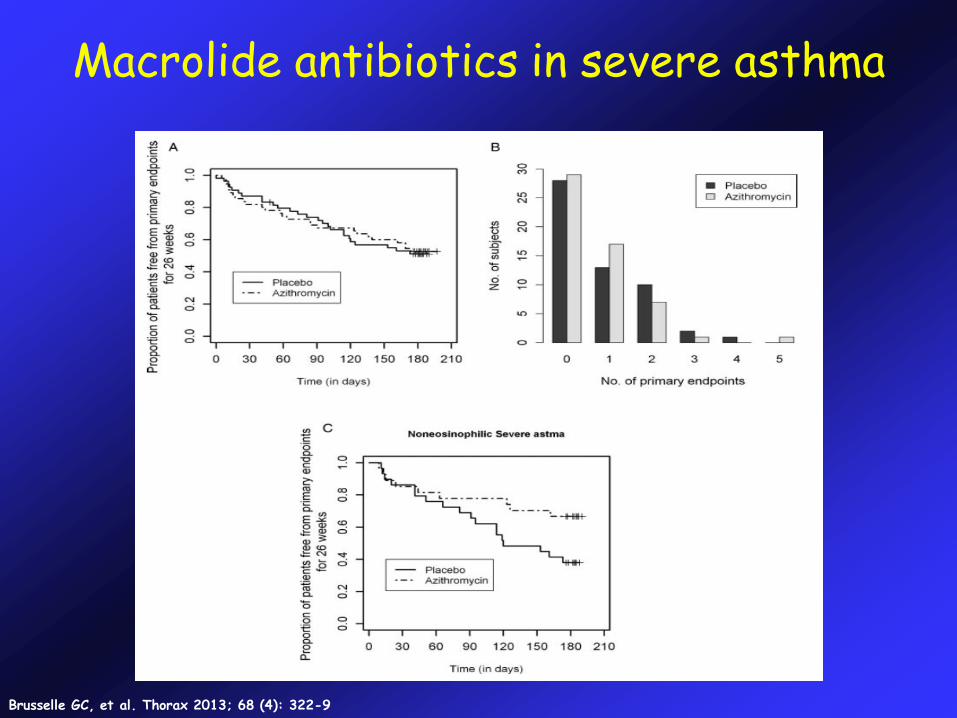
Macrolide antibiotics in severe asthma
Brusselle GC, et al. Thorax 2013; 68 (4): 322-9
No specific intervention on bronchial epithelium and mucus production
No specific intervention on bronchial nerves
No specific intervention on vascular remodeling
No specific action on SM Cells
Limitations of Endotypes
40
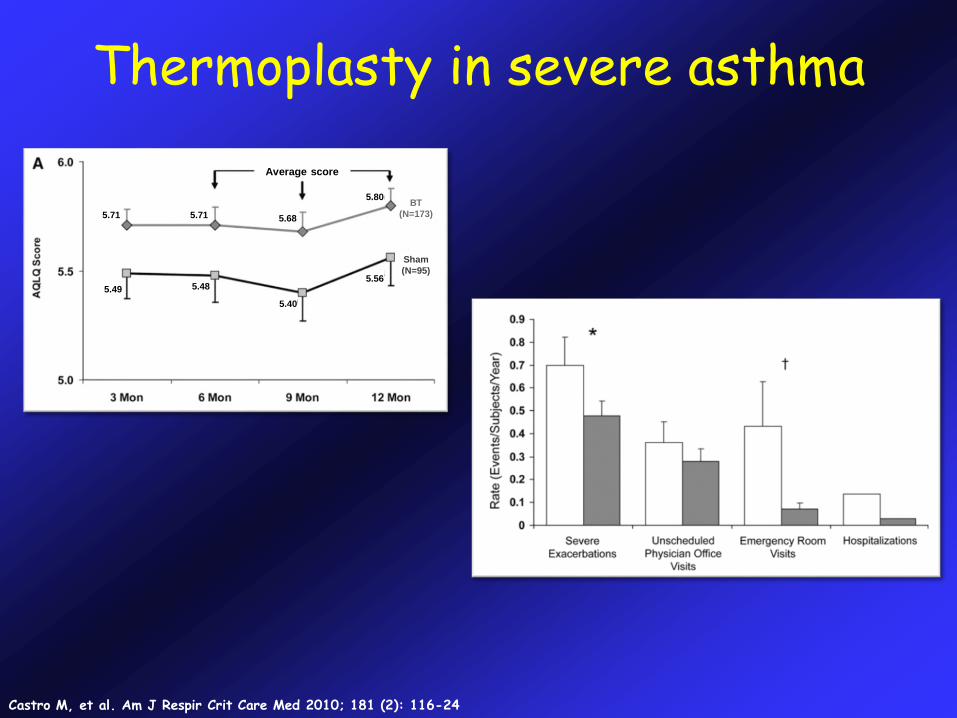
Thermoplasty in severe asthma
Castro M, et al. Am J Respir Crit Care Med 2010; 181 (2): 116-24
5.71 5.71 5.68
5.80BT
(N=173)
Sham
(N=95)
5.49 5.48
5.40
5.56
Average score
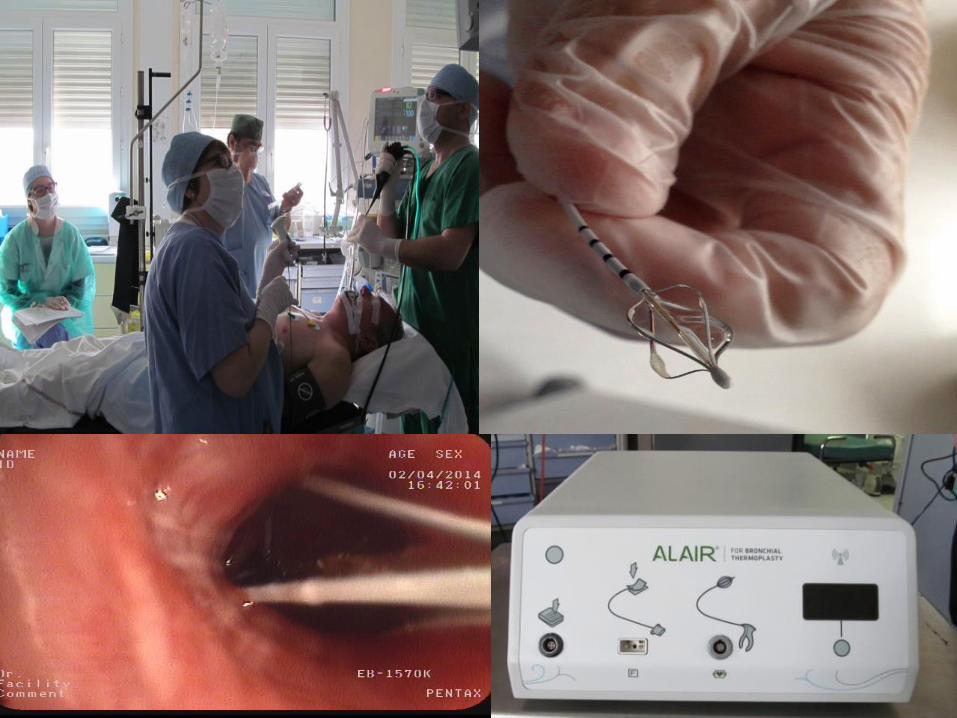
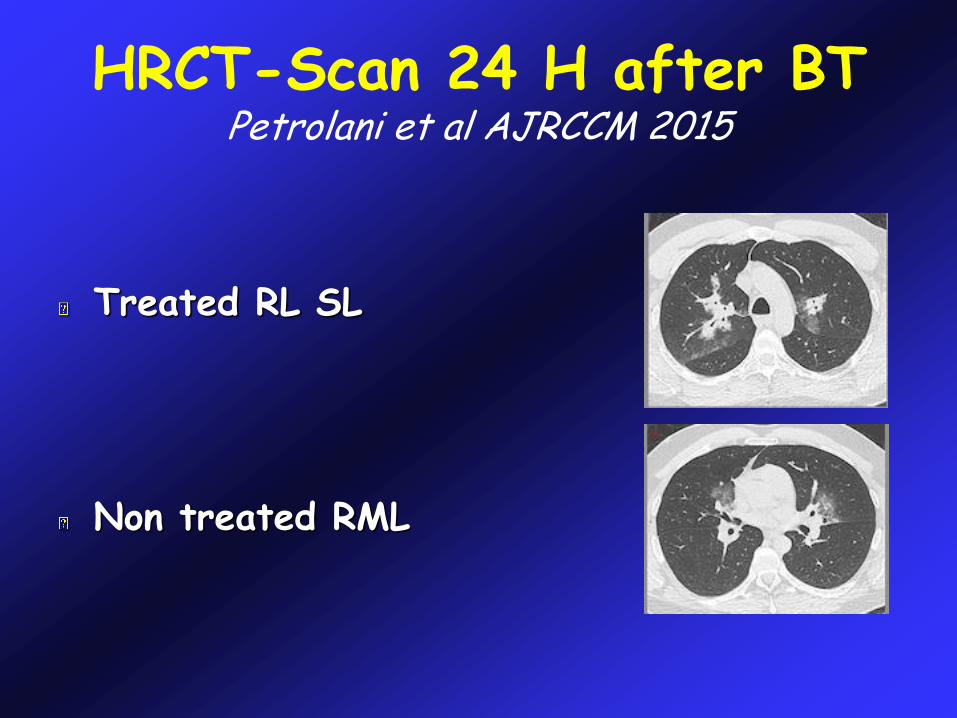
HRCT-Scan 24 H after BTPetrolani et al AJRCCM 2015
Treated RL SL
Non treated RML
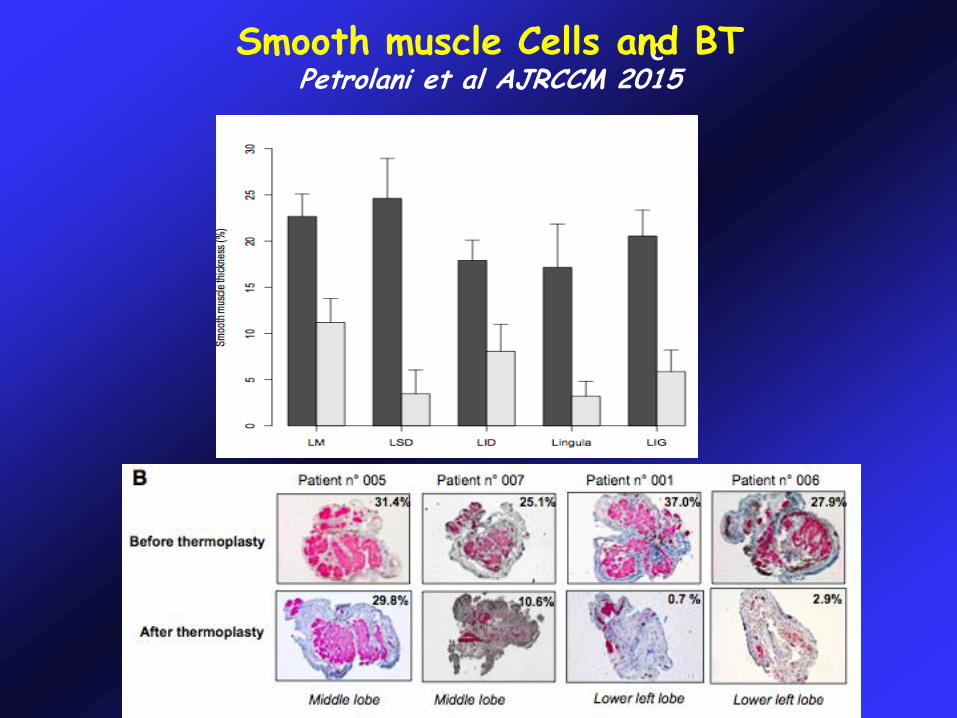
CSmooth muscle Cells and BTPetrolani et al AJRCCM 2015
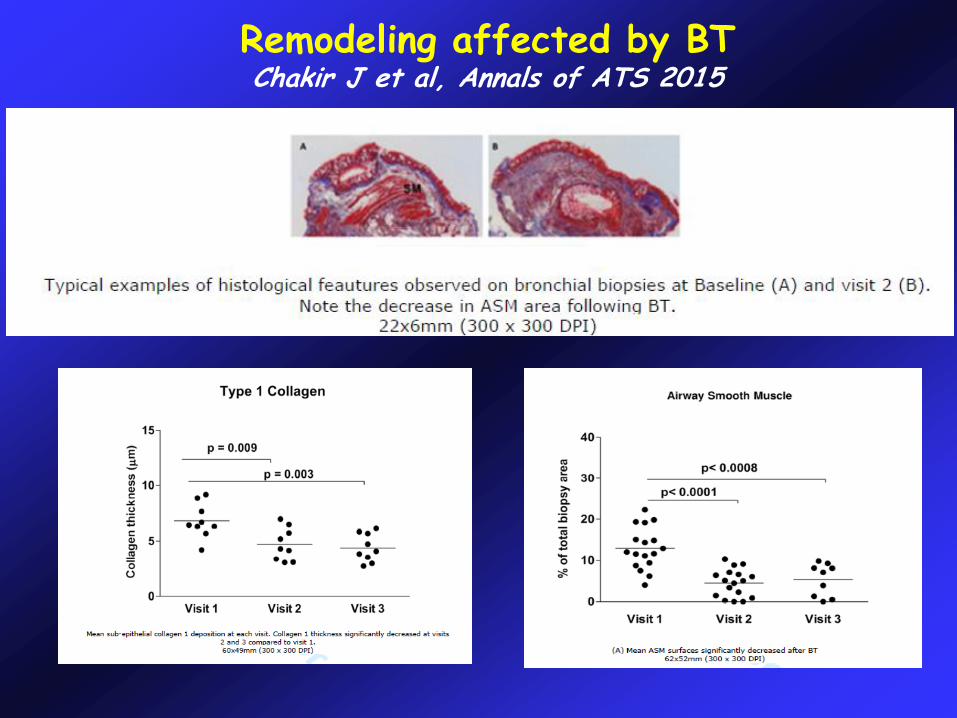
Remodeling affected by BTChakir J et al, Annals of ATS 2015
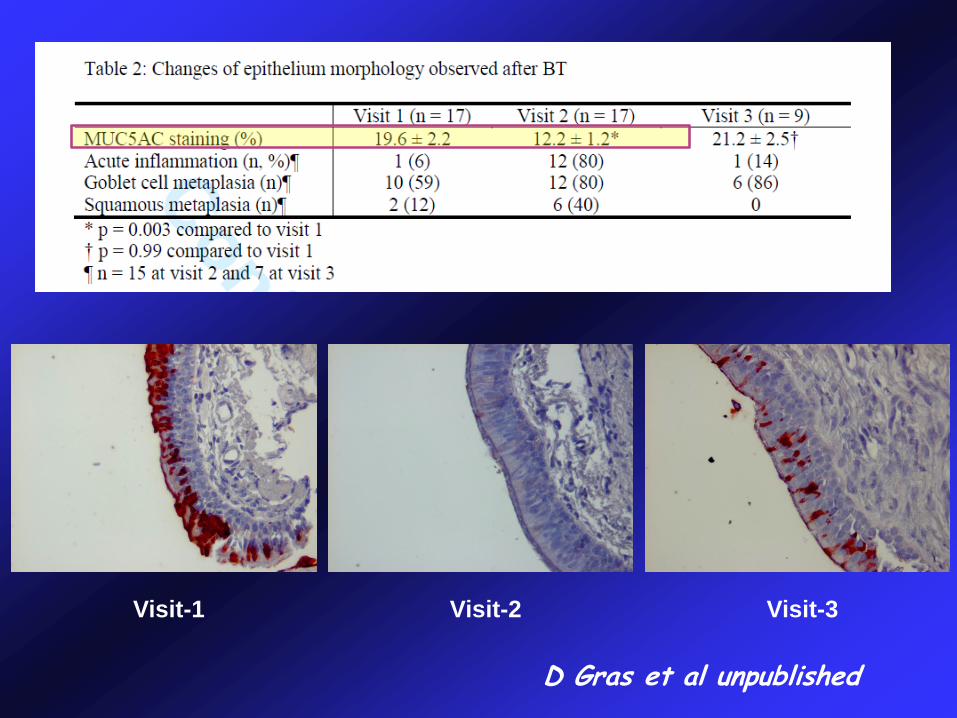
D Gras et al unpublished
Visit-1 Visit-2 Visit-3
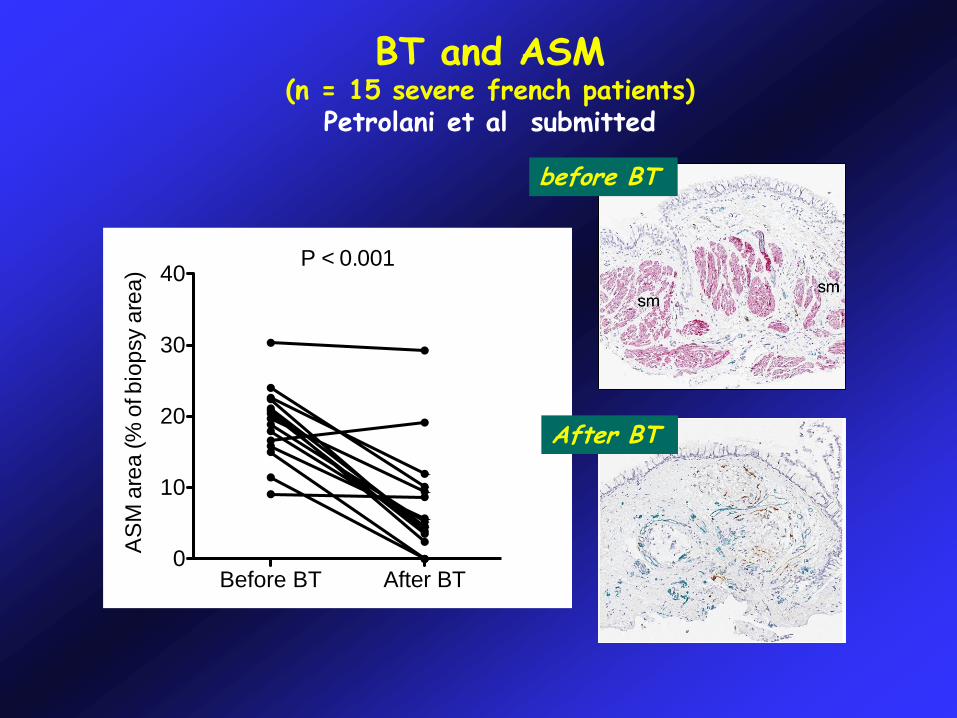
BT and ASM(n = 15 severe french patients)
Petrolani et al submitted
P < 0.001
Before BT After BT0
10
20
30
40
AS
M a
rea (%
of bio
psy a
rea)
before BT
After BT
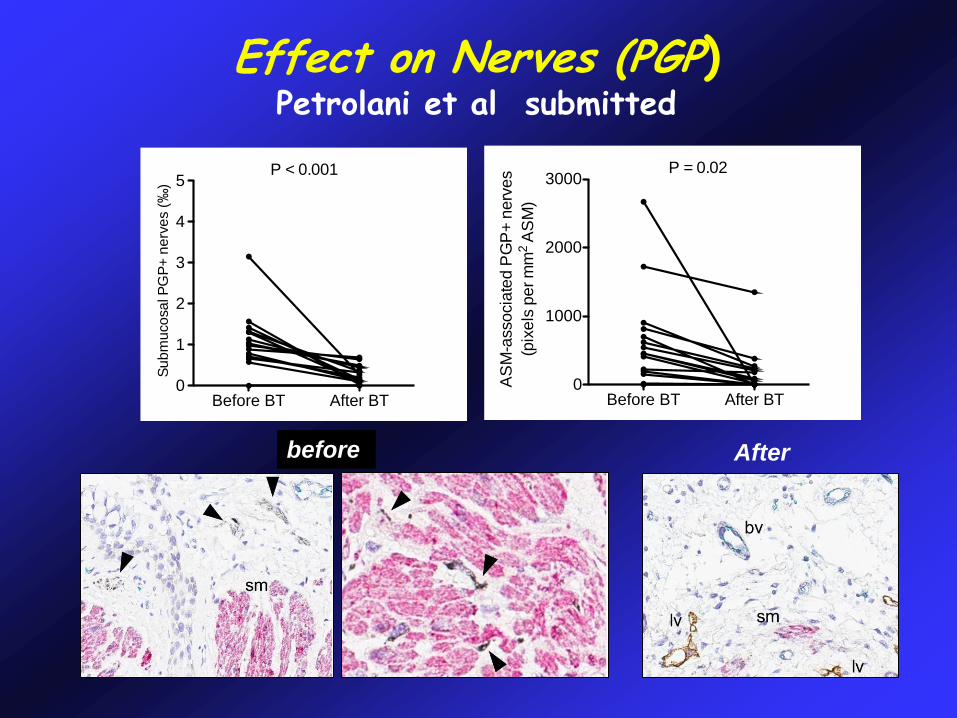
Effect on Nerves (PGP)Petrolani et al submitted
P < 0.001
Before BT After BT0
1
2
3
4
5S
ub
mu
co
sa
l P
GP
+ n
erv
es (‰
)P = 0.02
Before BT After BT0
1000
2000
3000
AS
M-a
ssocia
ted P
GP
+ n
erv
es
(pix
els
per m
m2
AS
M)
before After
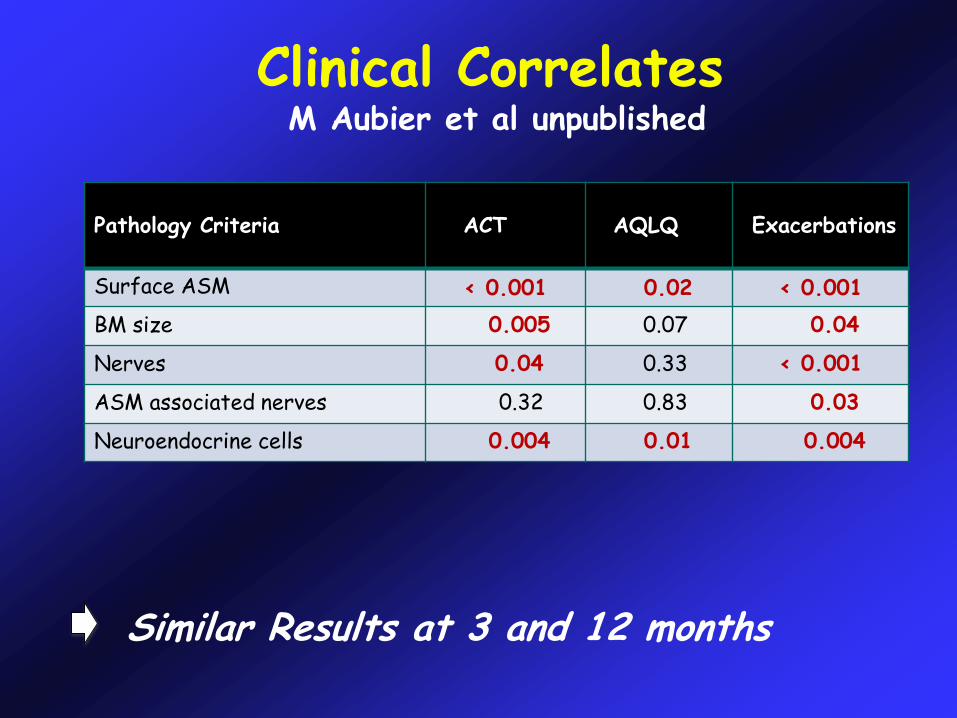
Clinical CorrelatesM Aubier et al unpublished
Pathology Criteria ACT AQLQ Exacerbations
Surface ASM < 0.001 0.02 < 0.001
BM size 0.005 0.07 0.04
Nerves 0.04 0.33 < 0.001
ASM associated nerves 0.32 0.83 0.03
Neuroendocrine cells 0.004 0.01 0.004
Similar Results at 3 and 12 months
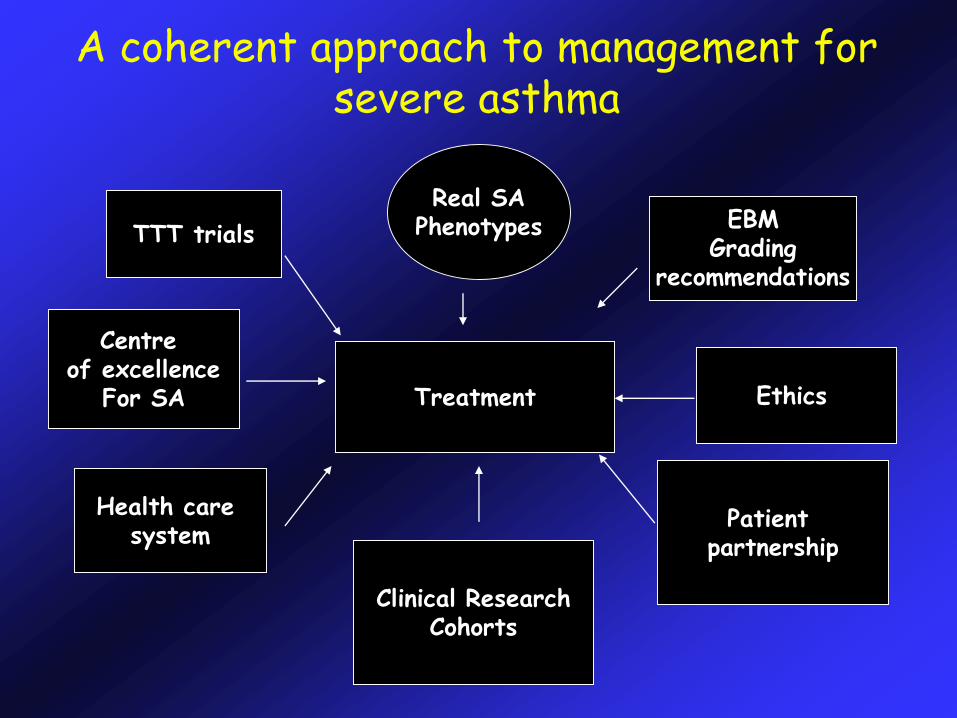
A coherent approach to management for severe asthma
Treatment
Real SAPhenotypes EBM
Gradingrecommendations
Ethics
Patient partnership
TTT trials
Centre of excellence
For SA
Clinical ResearchCohorts
Health care system
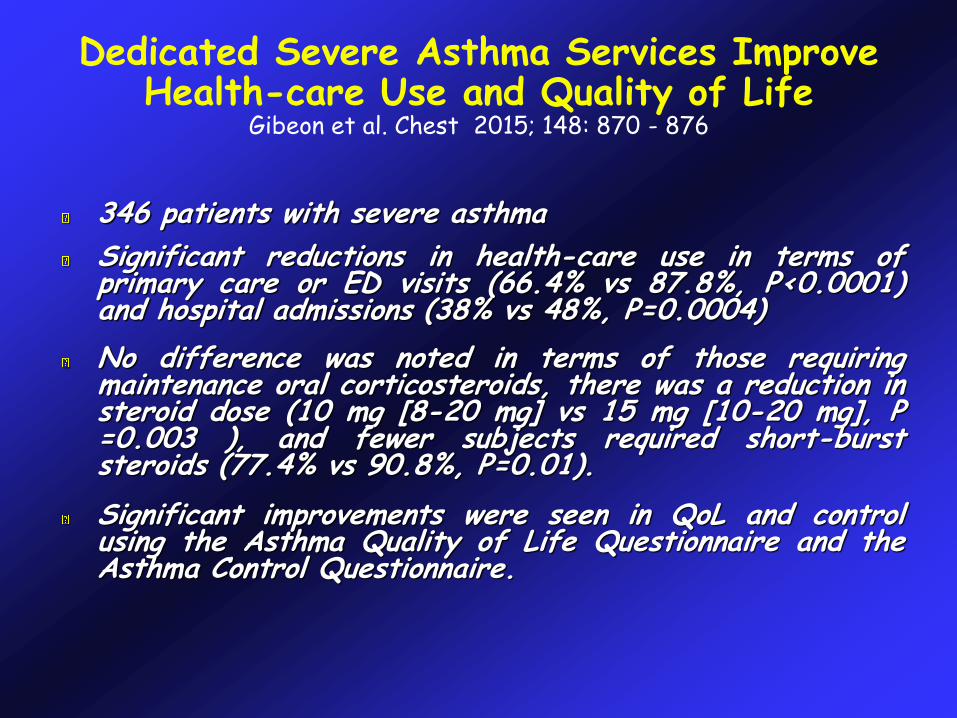
Dedicated Severe Asthma Services ImproveHealth-care Use and Quality of Life
Gibeon et al. Chest 2015; 148: 870 - 876
346 patients with severe asthma
Significant reductions in health-care use in terms ofprimary care or ED visits (66.4% vs 87.8%, P<0.0001)and hospital admissions (38% vs 48%, P=0.0004)
No difference was noted in terms of those requiringmaintenance oral corticosteroids, there was a reduction insteroid dose (10 mg [8-20 mg] vs 15 mg [10-20 mg], P=0.003 ), and fewer subjects required short-burststeroids (77.4% vs 90.8%, P=0.01).
Significant improvements were seen in QoL and controlusing the Asthma Quality of Life Questionnaire and theAsthma Control Questionnaire.
New approaches in severe asthma ?
• Customization of health care• Tailored to individual patient
• New innovative treatments:• Optimized prescribing
Right doseRight drug or interventionRight time

Rugby
Personalised Passion
Thank you !!!!!