Embed Size (px)
DESCRIPTION
Diagnosis: Intraduct papilloma with adjacent DCIS
Citation preview

British/ Arab School of Pathology, June 2008
Slide Seminars

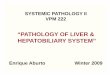
44AF51, Lt breast biopsy

44AF51, Lt breast biopsy
Diagnosis: Intraduct papilloma with adjacent DCIS

49F40, Nipple discharge
Diagnosis: Intraduct papilloma with in situ malignant change

143F46, Rt breast lump
Diagnosis: Solid papillary carcinoma+ Invasive Ductal carcinoma

Solid papillary carcinoma/Immunohistochemistry
Cytokeratin 5/6 CD10
SM Actin

Case No. 152F 64y, Left Breast, Cystic Lump

Case No. 152F 64y, Left Breast, Cystic Lump

Case No. 152F 64y, Left Breast, Cystic Lump

Case No. 152F 64y, Left Breast, Cystic Lump
K5/6 SMA
Diagnosis: Intracystic papillary Carcinoma

Case 184

Case 184 (CK 5/6)

Case 184
SMA ERER
Diagnosis: Intraduct papilloma With usual type hyperplasia

Case 185

Case 185 (CK 5/6)

Case 185
SMA p63
Diagnosis: Benign intraduct papillomas

Core biopsy 54

Core biopsy 54
SMA CK5/6
Diagnosis: Intracystic Papillary Carcinoma (B5)


136FF67, Rt breast lump, 20mm
Diagnosis: Myoid hamartoma
SMA

33 (for 139) F85, Lt breast, Asymmetry M3, US 8mm solid/cystic lesion
Diagnosis: Atypical Apocrine Adenosis (B4)

Case No. 144F 71y, Lt breast Lump, 3cm

Case No. 144F 71y, Lt breast Lump, 3cm
Diagnosis: Malignant phyllodes tumour

145. F58, Lt breast lump
Tubular adenoma rich in myoepithelial cells

150. F53, Rt breast lump, Stopped breast feeding 1 year ago
Extensive sclerosing adenosis (Adenosis tumour)

Case No. 153F 58y, Rt breast Lump, Screen-detected lesion

Case No. 153F 58y, Rt breast Lump, Screen-detected lesion

Case No. 153F 58y, Rt breast Lump, Screen-detected lesion
Diagnosis: Adenomyoepithelioma

Adenomyoepithelioma/Myoepithelial markers
p63

Adenomyoepithelioma/Myoepithelial markers
CD10 SMA

165F 40y, Right Breast Lump
Ductal or Lobular?

165F 40y, Right Breast Lump

E-Cadherin


ER
In situ Invasive

HER2

165F 40y, Right Breast Lump

165F 40y, Right Breast Lump
E-Cadherin
HER2

Case No. 165F 40y, Right Breast Lump
Diagnosis: Pleomorphic in situ & Invasive Lobular Carcinoma+ DCIS

187. F53, Rt breast lump
Benign complex sclerosing lesion


Core 41F44y, Lt breast
microcalcification, ?fibrocystic. M3, U3

41

41
Microcalcification

41
Cysts lined by cuboidal epithelium and containing mucin

41. AB/ PAS
Diagnosis: Mucocele-like lesion (B3)

Mucocele-like lesions First described by Rosen as mucin-filled cysts lined by flat,
cuboidal or columnar epithelium with extrusion of mucin into surrounding stroma (1)
The epithelial lining may show a cribriform or micropapillary atypical proliferative pattern, or even frank in situ malignant change. Detached epithelial cells may be sometimes found within intracystic or extracystic mucin (2)
Most cases present with mammographic coarse calcification. If presenting as mass lesion, malignancy is a high possibility
(1) Rosen PP. Am J Surg Pathol 1986; 10: 464-469 (2) Hoda SA & Rosen PP. Breast J. 2004; 10: 522-527

Excision biopsies of mucocele-like lesions diagnosed on cores P J Carder et al (2004)*
10 cases: Excision: 3 (30%) malignant (2DCIS+ 1 mucinous carcinoma) 3 had ADH 4 benign
R Ramsaroop et al (2005)** 12 cases: Excision:
5 (41%) malignant 1 ADH 6 benign
J Wang et al (2007)*** 11 cases: Excision:
all proved to be benign
*Histopathology 45:148-154 **Breast J 11:321-325***Am J Clin Pathol 127; 124-127

Mucocele-like lesions: B2 or B3? At the moment: Surgical excision seems to
be warranted, hence B3 may be more appropriate

Mucocele-like lesions: Relationship to invasive mucinous carcinoma It has been suggested that there is a spectrum of
changes representing a pathway progressing through:
mucin-filled ducts to mucinous ADH, mucinous DCIS and ultimately invasive mucinous carcinoma (1,2)
This is supported by recent evidence concerning staining for WT-1
(1) Hamele-Bena D et al. Am J Surg Pathol 1996; 20: 1081-1085 (2) Fisher CJ et al. Histopathology 1992; 21:69-71

Mucinous Carcinoma: WT1 positive

41. Mucocele- like lesion: WT1 positive
Supporting a link between mucinous carcinoma and mucocele-like lesions

Core biopsy 50

Core biopsy 50
ER
Diagnosis: Adenoid cystic carcinoma

Differential diagnosis1. Cribriform DCIS
ER: Uniformly positiveCells: monomorphic

2. Collagenous Spherulosis

Differential diagnosis: Using ER & CD10
Cribriform DCIS Adenoid cystic carcinoma
Collagenous spherulosis
ER
CD10


147F73, Rt breast lump

ER –PgR –HER2 –
Triple Negative (Basal Cell Type) Breast Carcinoma
ER PgR
HER2

CK5/6CK14

SMA

EGFR
EGFR Kinase Inhibitors:LapatinibGefitinib

176F73, Rt breast lump

176F73, Rt breast lump

176F73, Rt breast lump
AE1/AE3 CK5/6 CK5/6
SMA p63 ER
Diagnosis: Metaplastic carcinoma + DCIS

Case No. 157M 58y, Lt breast Lump

CD20CD3


M 58, Lt breast Lump

AE1/AE3

CK5/6

SMA
CD68
CD10

Diagnosis: Diabetic mastopathy

Diabetic Mastopathy
Fibrotic breast lumps presenting in patients with long standing diabetes,
more than 10 years, particularly the insulin-dependent variety.
Patients are relatively young (average 42 years), but a range of 32-66 years
Other diabetic complications are usually present. It has also been described, less commonly, in
patients with: type 2 diabetes patients with auto-immune thyroid and connective
tissue diseases.

Diabetic Mastopathy/ Histopathology
Lesions vary in size between 2-6 cm can be single or multiple and are bilateral in 50% of cases. Histology:
Dense keloid-like fibrosis heavy lobular and peri-vascular lymphocytic
infiltration. ‘Epithelioid fibroblasts’, sometimes
multinucleated, are present in the stroma. Cysts are characteristically absent.

Diabetic Mastopathy
The disease is self-limiting, but can recur. Reported recurrence rates varies between 32-80% of
patients Hence follow up is recommended, and any new lumps
developing examined by FNA or a core biopsy The disease is not associated with an increased risk of
breast carcinoma or lymphoma, although sporadic cases of breast carcinoma developing in association with diabetic mastopathy have been described

164. F72, ‘Eczema’, Rt nipple
Glandular Paget’s disease

182: M 95y, ‘Contents of a breast cyst’

CX3: M 95y, ‘Contents of a breast cyst’
Diagnosis: Mucinous Carcinoma, ?breast ?skin ?Colon
AB/PAS

M 95y, ‘Contents of a breast cyst’
CK7 CK20
ER PgR

M 95y, ‘Contents of a breast cyst’/ HER2/ IH
IHC ++

M 95y, ‘Contents of a breast cyst’/ p63
P63 negativity is in favour of ‘non-skin’ originD.Evans et al. J Cutan Pathol 2007, 34; 474-480

M 95y, ‘Contents of a breast cyst’
Final Diagnosis: Mucinous Carcinoma of breast, ER+, PgR+, HER2-

188. F 43, Rt breast lump

ER
S100
SMA
CD10
Microglandular adenosis


ER
S100
Diagnosis: Microglandular adenosis and matrix producing invasive carcinoma

Case No. 135F 61y, Lt breast haemorrhagic tumour, 11cm. Had Lt Breast Carcinoma, 5y ago
xxxxxxx_

Case No. 135F 61y, Lt breast haemorrhagic tumour, 11cm.

Case No. 135F 61y, Lt breast haemorrhagic tumour, 11cm.

Case No. 135F 61y, Lt breast haemorrhagic tumour, 11cm.

Case No. 135F 61y, Lt breast haemorrhagic tumour, 11cm.

Case No. 135F 61y, Lt breast haemorrhagic tumour, 11cm.
Ae1/AE3

Case No. 135F 61y, Lt breast haemorrhagic tumour, 11cm.
CD31 Factor VIII
Diagnosis: Angiosarcoma

Thank you