Embed Size (px)
Citation preview

Breathlessness Philip Ryan
Aims Review what you already know
Put some context around it
Show you some Hereford specific information
E.g. care bundles
Answer any questions


Breathlessness
Dyspnoea is very common presenting symptom in ED, CAU and wards
Cough
Sputum Production
Haemoptysis
Wheeze
Chest Pain, oedema, PND, orthopnoea
Fever
Night Sweats
Hoarseness or Stridor

Whilst taking history - observe Inability to speak
Pursed lipped breathing
Accessory muscle use and intercostal recession
Positioning
Extreme tachypnoea (respiratory rate greater than 30 breaths per minute)
Hypoxaemia
Pulse Oximetry (sats< 90%, heart rate)

Examine with purpose i.e. to rule in or rule out diagnoses
temperature
Heart rate and rhthym, BP, valves, oedema
Breathe sounds
Absence
Crepitations
Wheeze
Pleural rub
Common causes of dysnoea COPD
Pneumothorax
Pneumonia
Pulmonary embolism
Asthma
Pleural Effusion
Acute pulmonary oedema
Acute coronary syndrome
Valvular heart disease
Also cause dysnoea Trauma (chest wall injuries and smoke inhalation)
Neurological causes (spinal cord injury, muscular dystrophy, GBS and stroke)
Endocrine causes (DKA)
Metabolic causes (metabolic acidosis from sepsis)
Toxicological causes (salicylate toxicity)
Haematological causes (anaemia)
Gastrointestinal causes (massive ascites)
Psychiatric causes (anxiety)
Investigations You may have some before you start your examination
Pulse oximetry
ABG if sats <92% (make sure you write FiO2)
CXR Write good clinical info
Report it yourself
FBC, CRP +/- blood culture +/- tropinin +/- d-dimer
ECG
Peak flow meter in asthma

Putting it all together https://youtu.be/peNFccdBL3A
Intern Content: Dyspnea - OnlineMedEd

Advice and Tips COPD
Usually a combination of age, smoking history and wheeze
Use the care bundle
Oxygen prescribing is key based on ABG
Make sure decisions about ventilation / ceiling of care are discussed on PTWR if not before
Pneumothorax
Very good BTS guidelines cover nearly all eventualities
Get early respiratoty help
Pneumonia
Use the care bundle
Admisister abx within 1 hour
Pulmonary embolism
Don’t use d-dimer indiscriminantly
If you need a CTPA- make it happen
Asthma
Make sure a peak flow chart is started, put peak flow recording on drug chart if necessary
Airway obstruction
Can be difficult to assess, early CT may be helful
Get early respiratory team help
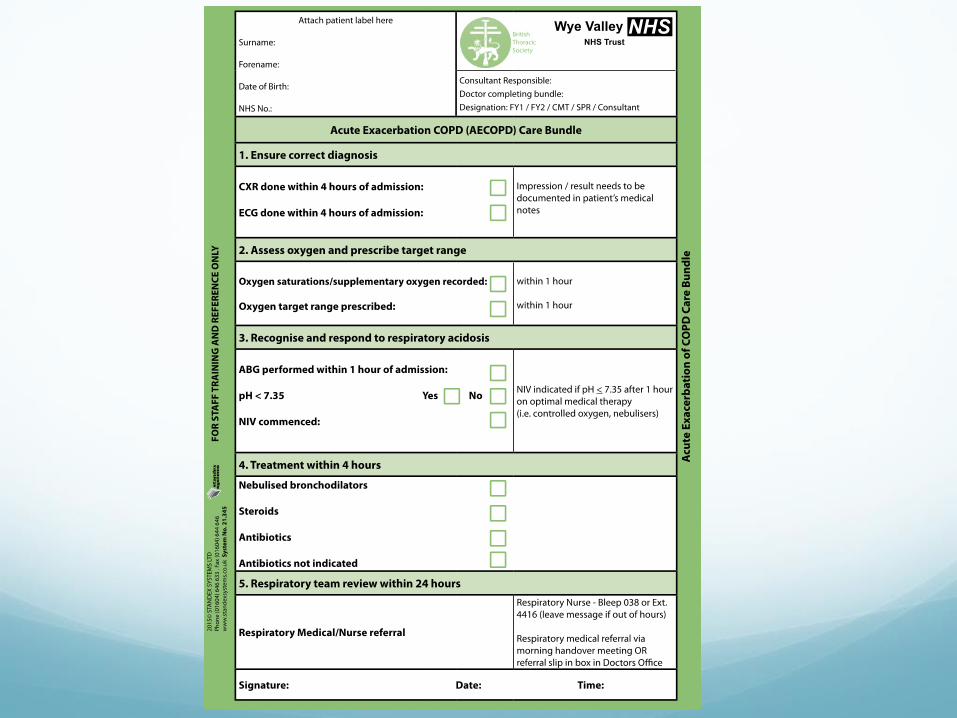
NIV service

WVT: TP01: Ratified: June 2016 Updated: June 2016 (V. 1) Review Date: June 2018
Pulmonary Embolism Pathway
Symptoms and Signs of PE
Dyspnoea, pleuritic chest pain, haemoptysis, syncope, cough
Tachypnoea, tachycardia, fever, pleural rub
If massive PE suspected with haemodynamic instability consider thrombolysis (see note 1) and leave pathway
Request CXR, ECG, FBC, U&E, LFT, coagulation screen, bone profile, TropT, ABG if SpO2 <94%
Calculate Wells score (except in pregnant patients)
High probability of PE (pregnant patients or Wells
score >4) Low probability of PE (Wells score 4 or less)
Start treatment with low molecular weight heparin
relevant to body weight, renal function, pregnancy
status. If at high risk of bleeding seek senior advice.
For pregnant patients (note 3) request bilateral leg
Doppler ultrasound if leg symptoms/signs of DVT and,
if negative, low dose perfusion scan
All other patients request CTPA (if eGFR permits,
otherwise VQ)
Consider ambulatory management (see PESI score
and exclusion criteria (see note 2))
Check d-dimer
D-dimer positive D-dimer negative
PE excluded. Consider alternative
diagnosis and assess suitability for
discharge
PE confirmed
on CTPA (or VQ
high
probability)
Diagnostic doubt
(VQ moderate
probability) Perform
CTPA or treat as PE
PE excluded on
CTPA (or low
probability on VQ)
Consider oral anticoagulation (note 4)
Continue LMWH in patients with active cancer (note 5)
Continue LMWH in pregnant patients (note 6)
If unprovoked investigate according to NICE guidelines (note 7)
file:///.file/id=657136
7.13920318

Fluid, free in the
pleural cavity
Lung
Ribs
Anatomy of the Pleural Space

Pleural
Adhesions
Loculated
Effusion
Rib
Lung
Pleural Adhesion
Rib
Lung
Pleural
Adhesions
Loculated vs Free Pleural Effusion (Air or Liquid)

CT scan showing lung cancer
tumour


WVT: TP02: Ratified: June 2016 Updated: June 2016 (V. 1) Review Date: June 2018
Possible Cardiac Chest Pain Pathway
Pain or discomfort that sounds like unstable
angina or myocardial infarction
Observations including BP in both arms
Oxygen aim saturations 94-98% (if risk of CO2 retention then aim 88-92%)
Obtain 12 lead ECG
Obtain IV access
Bloods FBC, U&E, LFT, TropT, glucose, CRP, coagulation
CXR (but do not delay other treatment to obtain CXR)
Give aspirin 300mg stat if no contraindications and not given pre hospital
STEMI PATHWAY
TREAT AS STEMI
ACS PATHWAY
New ECG changes
(not meeting STEMI criteria)
Or on-going cardiac sounding
chest pain
Or positive initial TropT
NB. Consider other causes of
raised TropT (see note 1)
TREAT AS ACS
LOW RISK PATHWAY
Normal or non-diagnostic
ECG
Chest pain resolved
Initial TropT negative
(<17 male, <14 female)

Asbestosis

Asbestos pleural plaques

more Pleural Effusion
Unilateral usually requires either diagnostic tap, therapeutic aspiration or chest drainage (pH, protein, LDH, Cytology & Culture)
Bilateral usually due totransudate but not always
Acute pulmonary oedema Iv diuretic, oxygenation
Acute coronary syndrome Care bundle
Valvular heart disease Echo-make it happen

Most important slide If you are not sure about anything ask for help
If you are still not sure ask again
If you are getting an answer you are still unhappy with
ask someone more senior

Questions

ABCDE approach Airway
Causes of airway obstruction
CNS depression
blood
vomit
foreign body
direct trauma
infection
inflammation
laryngospasm
bronchospasm
blocked tracheostomy

ABCDE approach Airway
Recognition of airway obstruction
talking/not talking
difficulty breathing, distressed, choking
Short of breath, tired
see-saw respiratory pattern, accessory muscles
partial obstruction - noisy breathing
stridor, wheeze, gurgling
complete obstruction - silence

ABCDE approach Airway
Treatment of airway obstruction
high flow oxygen
airway opening
head tilt, chin lift, jaw thrust
simple adjuncts
oropharyngeal or nasal airway
advanced techniques
e.g. supraglottic airway device, tracheal tube

ABCDE approach Breathing
decreased respiratory drive
CNS depression
decreased respiratory effort muscle weakness
nerve damage
restrictive chest defect
pain from fractured ribs
lung disorders
pneumothorax
haemothorax
infection
acute exacerbation COPD
asthma
pulmonary embolus
pulmonary oedema
Causes of breathing problems

ABCDE approach Breathing
Recognition of breathing problems
Look Respiratory distress, accessory
muscles, cyanosis, respiratory rate, chest deformity, conscious level
Listen Noisy breathing, breath sounds
Feel Expansion, percussion

ABCDE approach Breathing
Treatment of breathing problems
airway opening
oxygen guided by pulse oximetry
treat underlying cause e.g. antibiotics for pneumonia
support breathing if inadequate e.g. ventilate with bag-mask















![[Int. med] dyspnoea](https://img.dokumen.tips/doc/110x75/55ce4f2cbb61eb4d528b4758/int-med-dyspnoea.jpg)