Embed Size (px)
Citation preview

2034
Breast Cancer Screening in Older Black Women Noma L. Roberson, Ph.D.
The objective of this study was to report findings about older black women's responses to breast health education and screening. Findings were reported from a commu- nity-based intervention designed to improve breast screening services for women in Erie County, New York. A 34-foot mobile screening and education clinic was used to overcome barriers such as accessibility and cost. Re- sults from a sample of 271 older black women showed that they participated in breast health education pro- grams and received clinical breast examinations when these services were offered in their neighborhoods. How- ever, there was low participation in screening mammog- raphy offered at a local hospital. Low participation was attributed to structural and functional barriers in the de- livery system. This study emphasizes the particular im- portance of education and screening offered as one unit of service. Further, it emphasizes the need to examine older black women's reported experiences after participation in screening. Cancer 1994; 74:2034-41.
Key words: older black women, breast cancer, breast screening, breast health education, clinical breast exam- ination, mammogram, mobile clinic.
Participation of older black women in breast screening activities is a relatively new area of investigation. Little is known about these women's breast cancer screening practices. In addition, there are no studies specifically
From the Department of Cancer Control and Epidemiology, Roswell Park Cancer Institute, Buffalo, New York.
Supported by New York State Department of Health contract C- 010043.
Special thanks to the following staff Martha Oliveras, Vivian Evans, Nina Greene, Loretta Wilson-Fields, R.N., Dorothy Soda, R.N., Grace Turner, Marianne Cam, Angel Rivera, George Nunn, Wil- liam Aungst, M.D.
Address for reprints: Noma L. Roberson, Ph.D., Department of Cancer Control and Epidemiology, Roswell Park Cancer Institute, Elm and Carlton Streets, Buffalo, NY 14263.
The content of this paper are solely the responsibility of the au- thor and does not necessarily represent the official views of the New York State Department of Health.
Received May 24,1994; accepted May 25,1994.
designed to provide data to thoroughly examine the im- pact of breast cancer screening on breast cancer inci- dence and mortality rates among older black women.
What is known is that older women (i.e., those 65 years of age and older), including older black women, underutilize breast screening services.'-j Therefore, there is a need to improve this health practice in an effort to detect breast cancer early.
A beginning step to address this problem is to learn about older black women's responses to breast health education and participation in screening. This paper de- scribes the results from an intervention study, the Breast Cancer Detection Project, which was established through a mobile clinic, that examined older black women's responses to breast health education and screening. The project was designed to improve partici- pation in these areas.
Background
For the past 2 decades, national studies have shown that breast cancer is the most common cancer seen in American women.4z5 Approximately 60% of breast can- cer cases occur in women older than 60 years of age.' Incidence rates rise sharply with age and have increased steadily since 1976.4 Studies suggest that older women are at increased risk of diagnosis with advanced-stage breast cancer.6-8 Overall mortality rates have not changed for the general female population, however, despite apparent advances in early detection methods and treatment.
Black women, despite having a lower incidence of breast cancer than white women, are more likely to ex- perience high mortality and therefore present with ad- vanced disease.g-'' Black women also have lower 5-year survival rates compared with the general popula- tion. '*-"
Higher mortality among black women has empha- sized barriers to breast screening, including problems attributable to the system of health care delivery and problems related to women's own attitudes and behav-

Breast Cancer Screening/Roberson 2035
iors. Barriers attributable to the health care system in- clude ac~essibility,'~~'~-'~ ~ o s t ' ~ , ' ~ and physician atti- tudes toward recommending s~reening . '~~ '~ , '~ One study shows that when accessibility to health care is not a factor and physicians are seen on a regular basis, low- income black women still are not getting adequate breast cancer screening." Among black women, it ap- pears that knowledge'2T16f20,2' and belief^'^,'^^^^ have been found to be key predictors of breast screening be- havior. From a provider's perspective, the presence or absence of active recruitment of low-income black women, rather than reliance on physician referral, ap- pears to be an important predictor of screening behav- ior. 12,1523 Regardless of barriers to screening, black women are less likely than the 31 % of women in the gen- eral U.S. population to follow current breast cancer screen- ing guidelines for early breast cancer
There is the potential to decrease mortality through early detection. Studes show that, with regular use of breast screening (i.e., clinical breast examination and screening mammography), breast cancer mortality could be decreased by approximately 30%.26-28 Al- though breast cancer is a major threat to older women and they have a sixfold risk compared with younger women,29 there remains a critical problem about these women's failure to undergo regular screening and examination.
Because the U. S. population is aging, with approx- imately 15% of the population expected to be older than 65 years of age by 2010,30 the importance of breast can- cer as a health problem of older women, including black women, will increase. This is a reason to address barri- ers to screening and to understand the history and ex- periences that may influence older black women's screening practices.
History and Experiences of the Older Black Populations
It is difficult, if not impossible, to understand the elderly black population without an appreciation of their percep- tion of historical events and experiences relative to health care. Particularly, an assessment of black Americans in this country must include a review of their environmental ex- periences. Experiences in slavery is one example.
According to S a ~ i t t , ~ ' the health care system for slaves was based on several concerns. First, slaves were not allowed to malinger. Second, there was concern about the owner's property. Third, preventing the spread of disease was a priority. Finally, there was an actual concern for the health of the slaves. The health care system was controlled and executed primarily by overseers. While slaves often provided care for their
masters, they were not allowed to care for each other. To this end, a law was put into effect forbidding slaves to provide health care to each other under the threat of death. Fear of this law, combined with the concern about medical care provided by the overseer, resulted in the development of an underground health care sys- tem. That system included spiritualism, voodooism, and other appro ache^.^'
In addition to the historical events about the health care system, other situations evolved during slavery that continued to have an impact on the black elderly popula- tion. This was the breakup of the family unit and the loss of the traditional place of honor of the elderly. During the postslavery period of this country, there was an attempt to restore family units and the status of the elderly in black families.32 Unfortunately, throughout this period, poverty and discrimination had a negative impact on the health of blacks, including the aged population. Poor environmental conditions and the virtual absence of health care led to a high prevalence of &ease, disability, and death among blacks in the postslavery era.32
In the virtual absence of health care, the social sup- port network, particularly from the family unit, was viewed as a buffer against environmental stress. This network has been examined for both structural (size, linkages, and compositions) and functional (affective, reciprocal, and instrumental) features.33
Stack34 found networks of kin and friends support- ing each other. Cantor et al.35 found that elderly black women continued to perform instrumental and effective familial roles far beyond the age range custom- ary among whites. Researchers argue that older black women were involved more highly in a mutual assis- tance system among and between family members. In addition, compared with older white women, a sub- stantially greater number of older black women are heads of fa mi lie^,^^,^^ and the extended family pattern persists in the African-American culture.
The aging process of blacks is another area that must be considered when dlscussing health care. Al- though aging can represent a period of increasing free- dom from restricting demands for the black elderly pop- ulation, more often than not, it means increased suscep- tibility to economic loss, chronic health problems, depression and despair, social isolation, and continued employment for survival.38
The health of the aged population has been approached from two perspectives, the medical model and the functional model. The medical model defines health in terms of the presence or absence of disease.39 Tfus model is used more commonly by health care professionals. The functional model defines health in terms of level of functioning (i.e., degree of fitness rather than extent of pa tho log^).^^

2036 CANCER Supplement October 2,2994, Volume 74, No. 7
Impairment of the ability to function independently at home or in one’s community is the common pathway to the array of diseases encountered frequently with age. When there is impairment of ability to function, elderly blacks frequently do not obtain physician exam- inations at the same rate as their white counterparts do.38 Therefore, early recognition of problems does not occur. Often, when an elderly black person seeks med- ical services, his or her condition is usually in a late, advanced stage. The black elderly often identify sick- ness as weakness, and their complaints sometimes are not specific. Rather, their complaints usually are can- tered around their ability to perform the activities of daily living, such as cooking meals, cleaning the house or rooms, or doing the laundry. It is generally when a condition incapacitates them that they will seek care.41 In the process, the black elderly population displays complete confidence in their physician. Unfortunately, the physician attitude toward medical care and treat- ment for this group often is negative and indifferent.
There remain a few elderly blacks who resort to folk cures; those who do frequently do so because these ideas are an element in their particular racial/ethnic id en tit^.^' Ideas about health, illness, and healing are tied so closely to the values and behaviors of people’s lives that knowl- edge about race and ethnicity may provide significant in- sight into the nature of the health practices of the elderly black population in the United States.
The black elderly have many health beliefs and be- haviors that are shaped by both culture and class. These are shaped by education, income, and occupation, as well as other environmental health factors. These be- liefs and attitudes determine when a health event is de- fined as an illness, when help is sought, what type of help is sought, and from whom. The crucial implication of this practice for health care in the elderly is that de- terioration of functional independence is usually a reli- able indicator of inadequately managed d i ~ e a s e . ~ ’ , ~ ~ Those diseases that produce functional impairment in the elderly often are treatable and improvable; how- ever, early detection is essential.
Breast cancer is an example of a disease that is treat- able if detected early. Unfortunately, little is known about older black women’s breast cancer screening practices, which are essential for early detection. His- torical events and experiences may shed some light on the decision to obtain screening.
Methods
Intervention Model
This was a descriptive study designed to determine older black women’s responses to a community-based
intervention. The intervention was a New York State Department of Health’s Breast Cancer Detection Project designed to improve participation in breast health edu- cation and screening among minority women, particu- larly blacks, Hispanics, Native Americans, and other low-income, underserved women in Erie County, New York. Because of the lack of research about older black women’s breast screening practices and the increasing concern to improve mammographic screening, specific emphasis was placed on the study population.
A basic assumption for this study was that older black women encounter carcinogenic exposures similar to those to which other older segments of the popula- tion are subjected, and they therefore would benefit from the same kinds of cancer control measures (e.g., education and screening) that have been useful in other populations. Furthermore, it is believed that historical events and experiences may be associated closely with poverty, which, in turn, is related to limited opportunity and access to health care.44 These are factors that most often are barriers to screening and serve as an indication that these women may be hard to reach. To develop an appropriate strategy for addressing barriers that may affect breast cancer screening in older black women, at- tention must be focused on their screening practices.
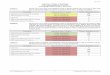
The theoretic model that served as a guiding frame- work to enhance an understanding about overcoming barriers that may influence participation in education and screening is shown in Figure 1. This model integ- rated communication principle^,^^ the Health Belief
and learning theory47 on the basis of the con- tribution each would make toward a rational decision to participate and/or utilize preventive health services focused on breast screening. A combination of these models emphasized that communication is a valuable source for disseminating cancer information that hope- fully increases awareness and knowledge and influence beliefs. The Health Belief Model influences the self-per- ception of being at risk for a disease such as breast can- cer and serves as a cue to action for decisions to adopt breast education and screening as health practices. Through a learning process, participants gained knowl- edge of the proper techniques for adopting these health practices, the ability to perform the practices correctly, and the procedures that encourage examinations for early cancer detection.
The model attempts to explain that women may be likely to adopt breast screening practices when commu- nication, knowledge, and beliefs are in place.
Breast Cancer Detection Project
The Breast Cancer Detection Project was designed and began operation in 1990 in Erie County, New York. Its

Breast Cancer ScreeninglXoberson 2037
TARGET POX'ULATION L.r' Communication
hinfiples
-1-
BEHAVIORAL CHANGE
Figure 1. The theoretic model for guiding the development of cancer screening and education programs in hard-to-reach populations. This is the model that served as a guiding framework to enhance an understanding about overcoming barriers that may influence participation in education and screening. This model integrated communication principle^,'^ the Health Belief theory47 on the basis of the contribution each would make for a rational decision to participate and/or utilize preventive health services focused on breast screening.
and learning
specific objective was to provide breast health educa- tion (i.e., breast self-examination [BSE] instructions) and breast screening (i.e., clinical breast examination and mammography). Although the project was de- signed to provide services to women in Erie County, New York, specific attention was focused on reaching minority women (Le., blacks, Hispanics, Native Ameri- cans, and other low-income, underserved women). This study will report on one segment of the target popula- tion: older black women.
A community assessment, based on a community- mapping procedure, was conducted in census tracts throughout the areas to identify the target population and the community resources and agencies serving this population.
Based on focus group findings from a previous an intervention to target black women was de-
signed and implemented. The central focus of the inter- vention was to eliminate barriers of cost and accessibil- ity to breast screening. To this end, a 34-foot mobile van was purchased and designed to provide free BSE instructions and clinical breast examinations. This mo- bile education and screening clinic traveled throughout neighborhoods, making stops at senior citizen centers, senior housing complexes, health care facilities, churches, community health centers, senior citizens'
outdoor gatherings, and block club events. Approxi- mately four programs per month were devoted to older women.
The mobile clinic consisted of a classroom that seated 15-18 women, an examination room, and a li- brary. The mobile unit was staffed by a driver/security person, outreach workers, nurses, physicians, and community volunteers representative of the targeted communities.
All staff completed a 6-week training program be- fore participating in community activities. Outreach workers provided BSE instructions, including the use of brochures, videos, and silicone breast models. Nurses and physicians performed need assessments and clini- cal breast examinations and made recommendations and/or referrals for mammograms at a comprehensive cancer center, a private practice, or a health clinic.
To ensure that women would schedule and keep appointments for mammograms, outreach workers as- sisted women and sent a reminder message before the scheduled appointment. Transportation was scheduled when required. In addition, outreach workers were available to accompany women to their appointment, if such assistance was requested. Tote bags, pens, pins, and T-shirts were some of the incentives provided for participation.
Data about breast education and screening prac- tices were collected via a client-intake form. It was com- pleted by each program participant before receiving ser- vices. Sampling of convenience was employed for the study because of the practical impossibility of obtaining a truly representative sample. The Statistical Package for the Social Sciences49 was employed to implement statistical procedures.
The study population consisted of 271 older black women, 65 years of age and older, who completed a client-intake form. This was 13% of the total target pop- ulation recruited from the community.
Results
Of the study population, 70% were aged 65-69 years, 20% were 70-74 years of age, and 10% were 75 years and older. Thirty-three percent of the women had com- pleted only elementary school, 28% had less than a high school education, and 20% had completed high school. Seventy-nine percent had household incomes of less than $12,000, and 14% had household incomes between $12,000 and $18,000. Thirty-eight percent of women reported having Medicare only, and 42% had Medicare plus private insurance. The remainder had Medicare and Medicaid.

2038 CANCER Supplement October 2,2994, Volume 74, No. 7
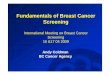
‘EDU ‘CBE ‘MMG Figure 2. The percentage of older black women recruited for education and screening (n = 271). EDU: education; CBE: clinical breast examination; MMG: mammogram.
As shown in Figure 2, 99% of older black women participated in breast health education classes. Less than 20% completed the survey to determine what was learned in the class or how well they performed the technique on the breast model. Seventy-five percent of the women continued through the needs assessment and received a clinical breast examination after educa- tion. Thirteen percent of the women followed the refer- ral and/or recommendation to obtain a mammogram at the local hospital. Less than 5% required transportation for their appointments.
When asked about their BSE practices, only 20% reported that they practiced regularly, 47% of women reported that they performed BSE occasionally, and 33% never practiced. Fifty-seven percent of women re- ported having had at least one mammogram: 10% re- ported receiving a mammogram within the previous year, 14% reported having had a mammogram within the previous 2 years, and 31% said that they had had one mammogram within the previous 5 years.
Discussion
This study of older black women’s responses to breast health education and screening provides a unique view of a population that long has been ignored in cancer control research. Although there have been a few sur- vey s t ~ ~ d i e s ’ ~ , ~ ~ * ~ ~ about breast cancer screening among older women, none have based findings on interven- tions that personalize program activity, increase access to services, limit cost, and facilitate completion, partic- ularly for older black women. In addition, there have been no studies wherein interventions for older black women were guided by a theoretic framework that in- tegrated useful models for program planning and im- plementation. The present study included both of these
factors in an effort to address the underutilization of breast health education and screening.
Findings of the present study show that older black women who participated in education and screening generally have low incomes and less than a high school education. The majority have some type of health insurance.
Older black women’s low income most likely is as- sociated with and is a function of their employment ex- perience. Many older black women had disadvantaged work experiences throughout their employment histo- ries. They are more likely to have worked in low-status jobs, characterized by sporadic unemployment, ex- tremely low earnings, and few, if any, benefits. They also generally have been affected by employers’ last hired, first fired policies. Therefore, the experience of low income is more evident through advanced age.38
Similar to income, limited education is a function of limited opportunities during women’s earlier years. In the past, lifetime experiences were centered primarily around employment for survival of the family; there- fore, education was not a priority. In fact, because of limited education, in addition to some physical impair- ments, additional time and assistance were required for participants to complete data intake forms for this study.
The majority of women in the study had some type of health insurance, whether Medicare, Medicaid, pri- vate, or a combination. Although it would appear that cost would not be a barrier to obtaining breast cancer screening, three important factors must be kept in mind. First, high deductibles for Medicare may be a problem for women with low incomes, as may small payments for services not covered completely by this insurance. Women are required to pay for health care services until deductibles are met. Second, Medicare coverage is pro- vided every other year. Therefore, on odd years, women are required to pay out-of-pocket unless they have private insurance. Third, not all physicians accept Medicare and Medicaid payments for health care services.
Findings showed that older black women were re- cruited for and participated in education sessions to learn about the BSE technique. Approximately three fourths of these women were given a clinical breast ex- amination. The favorable response to education and clinical breast examination may be attributed to the elimination of barriers associated with access and avail- ability of services. The mobile screening clinic appeared to be a useful strategy for providing services in women’s neighborhoods. Recruitment messages designed to target older women and outreach workers representa-

Breast Cancer ScreeninglRoberson 2039
tive of their communities were likely to be key factors in communicating with these women.
Study results showed that women were less likely to obtain a screening mammography than education and clinical breast examination. As shown in Figure 2, only 13% of older black women who completed educa- tion obtained a mammogram. Low participation in screening mammography perhaps could be attributed to the structure of the program and the health delivery system (i.e., the appointment system). Women were re- quired to take additional steps to make appointments and obtain mammograms at a local hospital. Mammo- grams were not provided at the mobile clinic; however, every effort was made to assist women in scheduling appointments. At the local hospital, the structure of the appointment system was such that women were sub- jected to a 2-4-week waiting period. The system was not designed to be flexible enough to accommodate cli- ents from a community program in a timely fashion. The ideal approach would have been to schedule ap- pointments within 2-3 days of participating in an education program and undergoing a clinical breast examination.
Long waiting periods for appointments increases the probability of noncompliance. It is likely that non- compliance would result in more serious problems for older women than for the general population. First, in the case of breast cancer screening, clients were intro- duced to a relatively new medical test they were re- quired to undergo. Second, they were likely to have had some reservations about going to a new or unfamiliar facility to receive services. For this population, there may also have been some reservations about receiving services at a specialized hospital, such as a cancer cen- ter. Third, it is not evident what influence the providers at the mobile clinic had on women’s decisions to follow through on referrals and/or recommendations. Fourth, it is not known what importance women placed on ob- taining a mammogram. Fifth, it is not evident what physical impairments or other environmental circum- stances may have prevented older women from keeping appointments.
Transportation was not an impediment to screen- ing, because van services were provided. For those women who kept appointments, family and/or friends usually provided transportation and accompanied them to the clinic. This demonstration of support may be con- sidered a factor that enhanced compliance.
According to study findings, the majority of older black women were not practicing BSE monthly. It was likely women were not aware of the technique and its importance. For those women who reported practicing occasionally, it was uncertain what the quality of the
technique was. Most women failed to complete the sur- vey that would have provided data about knowledge and performance of the correct steps for BSE. Observa- tions showed that women experienced some difficulty completing intake forms and, more often than not, needed some assistance. It appeared that this was at- tributed to their educational level.
Findings showed that more than one half of the women reported that they had received a mammogram at least sometime within the previous 5 years. This was an indication that these women were knowledgeable about mammograms and had taken the initiative to be screened. The critical question was whether women ac- tually knew what a mammogram was. It was possible that they were confusing a mammogram with another medical test such as an electrocardiogram. Results from focus group sessions for a national study (Worden K, per- sonal communication, August 1991) showed that this was the case in a study of older black women’s reports on obtaining screening mammography. When asked to describe the mammograms that they had received, women described an electrocardiogram.
Several limitations of this study should be consid- ered in assessing its results. First, cancer control and be- havioral science data on racial/ethnic older populations are sparse; therefore, caution is warranted when com- paring the responses of this population segment to those of the general population. Second, there is a per- sistent use of small samples of blacks in this study, par- ticularly segments of the older black population, such as older black women. Third, this study was limited to findings from a relatively small sample size. Lastly, findings relied on data from self-reports.
Conclusions
Overall, these results suggest that older black women will participate in breast health education programs and undergo clinical breast examination when these ser- vices are provided in their neighborhoods. The use of a mobile screening clinic appeared to be a useful strategy for this intervention.
Participation in screening mammography was less evident, particularly because women were required to receive this service at a different location. It was the structure and function of the delivery system, not barri- ers to cost and accessibility, that appeared to be attrib- uting factors to low participation.
These results emphasize the particular importance of education and screening being offered as one unit of service. In addition, it identified areas that warrant further investigation in this population segment. In par- ticular, there is a need to examine older black women’s

2040 CANCER Supplement October I , 1994, Volume 74, No. 7
knowledge and beliefs about education and screening. Furthermore, there is a need to design interventions that address structural and functional barriers in the de- livery of breast cancer screening. These interventions should be implemented and evaluated to determine the program impact on older black women’s behavior and
older racial/ethnic minorities and whites: bamers to early detec- tion. J Gerontol 1992; 47(Special Issue):101-10. Whitman S, Ansell D, Lacey LP, et al. Patterns of breast and cervical cancer screening at three public health centers in an in- ner-city urban area. A m ]Public Health 1991; 81:1651-3.
20. Burack RC, Liang J. The acceptance and completion of mam- mography by older black women. Am ] Public Health 1989; 79:
19.
- - experiences as a result of participation,
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10
11
12
13
14
15
16
17
18
NCI Breast Screening Consortium. Screening mammography: a missed clinical opportunity? National Health Interview Survey Series. JAMA 1990; 264:54-8. Centers for Disease Control. Trends in screening mammograms for women 50 years of age or older: behavioral risk factor sur- veillance system, 1987. MMWR Morb Mortal Wkly Rep 1989; 38:
Costanza ME. Breast cancer screening in older women: Over- view. JGerontol 1992; 47:l-3. Boring CC, Squires TS, Tong T, Montgomery S. Cancer statistics, 1994. CA CancerJClin 1994; 44:7-26. National Cancer Institute. Division of Cancer Prevention and Control. 1987 Annual Cancer Statistics Review. Including can- cer trends: 1950-1985. Bethesda, MD: 1988 NIH Report No. 88- 2789. Goodwin JS, Samet JM, Key CR, Humble C, Kutvirt D, Hunt C. Stage at diagnosis of cancer vanes with age of the patient. ] A m Geriatr Soc 1986; 34:20-6. Holmes FF, Heame E. Cancer stage-to-age relationship: implica- tions for cancer screening in the elderly. J Am Geriatr Soc 1981; 2955-7. Mueller CB, Ames F, Anderson GD. Breast cancer in 3,558 women: age as a significant determinant in the rate of dying and causes of death. Surgery 1978; 83:123-32. Jacob TC, Penn NE, Brown M. Breast self-examination: knowl- edge, attitudes and performance among black women. J Natl Med Assoc 1989; 81:769-76. Polednak AP. Breast Cancer in black and white women in New York State. Cancer 1986; 582307-15. Satariano WA, Belle SH, Swanson GM. The severity of breast cancer at diagnosis: a comparison of age and extent of disease in black and white women. Am 1 Public Health 1986; 76:779-82. Ansell DA, Dillard J, Rothenberg M, et al. Breast cancer screen- ing in an urban black population. Cancer 1988; 62:425-8. Lacey LP, Phillips CW, Ansell D, Whitman S, Edie N, Chen E. An urban community-based cancer prevention screening and health education intervention in Chicago. Public Health Rep
Valanis B, Wirman J, Hertzberg VS. Social and biological factors in relation to survival among black vs. white women with breast cancer. Breast Cancer Res Treat 1987; 9:135-44. Bloom JR, Grazier K, Hodge F, Hayes WA. Factors affecting the use of screening mammography among African American women. Cancer Epidemiol Biomarkers Preu 1991; 1:75-82. Rimer BK, Keintz MK, Kessler HB, Engstrom PK, Rosan JR. Why women resist screening mammography: patient-related bamers. Radiology 1989; 172:243-6. Vernon SW, Vogel VG, Halabi S, Jackson GL, Lundy RO, Peters GN. Breast cancer screening behaviors and attitudes in three ra- cial/ethnic groups. Cancer 1992; 69:165-74. Caplan LS, Wells BL, Haynes S. Breast cancer screening among
137-40.
1989; 104:536-41.
721-6. 21. Jepson C, Kessler LG, Portnoy B, Gibbs T. Black-white differ-
ences in cancer prevention knowledge and behavior. Am J Public Health 1991; 81:501-4.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32. 33.
34.
35.
36.
37.
38.
39.
40.
Nemcek MA. Health beliefs and breast self-examination among Black women. Health Values 1990; 14:41-52. Price JH, Desmond SM, Slenker S, Smith D, Stewart PW. Urban black women’s perceptions of breast cancer and mammography. ] Community Health 1992; 17:191-204. Marchant DJ, Sutton SM. Use of mammography-United States. MMWR Morb Mortal Wkly Rep 1990; 339:621-30. Escarce JJ, Epstein KR, Colby DC, Schwartz JS. Racial differences in the elderly’s use of medical procedures and diagnostic tests. Am ] Public Health 1993; 83:948-54. Baker LH. Breast cancer detection demonstration project: five year summary report. Cancer 1982; 32(4):194-225. Shapiro S, Strax P, Venet L, Rosen R. Ten-to-fourteen years effect of screening on breast cancer mortality. J Natl Cancer lnst
Tabar L, Gad A, Holmquist U, et al. Reduction from breast can- cer after mass screening with mammography. Randomized trial from the Breast Cancer Working Group of the Swedish National Board of Health and Welfare. Lancet 1985; 8433:829-32. Ries LAG, Hankey BF, Miller BA, Hartman AM, Edwards BK. Cancer statistics review 1973-1988. Bethesda, MD: National Cancer Institute. 1991 NIH Publication No. 91-2789. Healthy People 2000. Washington, DC: Public Health Services. 1991 U.S. Dept. of Health and Human Services publication
Savitt TL. Medicine and slavery: the diseases and health care of blacks in antebellum Virginia, Chicago: University of Illinois Press, 1978. Clavon A. The black elderly. J Gerontol Nurs 1986; 5:6-12. Wyche KF. Psychology and African-American women: findings from applied research. Appl Preu Psycho1 1993; 2:l 15-21. Stack C. All our kin: strategies for survival in a Black community. New York: Harper and Row, 1974. Cantor MH, Rosenthal K, Wilker L. Social and family relation- ships of Black aged women in New York City. ] Minor Aging
Mindel CH. Multigenerational family households: recent trends and implications for the future. Gerontologist 1979; 19:456-63. OHara WP, Pollard KM, Mann TL, Kent MM. African Ameri- cans in the 1990’s. Popul Bull 1991; 42:ll. U.S. Department of Health and Human Services. Minority aging: essential curricula content for selected health and allied health professions. Washington, DC: Public Health Services; 1990: 193-321, Publication No. HRS-P-DV 90-4. Shanas E, Maddox GL. Health, health resources and the utiliza- tion of care. In: Benstock RH, Shanas E, editors. Handbook on Aging. 2nd ed. New York: Van Nostrand Reinhold, 1985:696- 726. World Health Organization, Regional Office of Europe. The pub- lic health aspect of the aging population. Report of an Advisory group. Copenhagen: World Health Organization, 1959.
1982; 69:349-55.
(PHS) 91-50213.
1979; 4~50-61.

Breast Cancer Screening/Roberson 2041
41. William J, Stokes IH, Geay S. Old people at home: their unre- ported needs. Lancet 1964; 1117-24.
42. Christman NJ, Kleinman A. Health beliefs and practices among American ethnic groups. In: Threnstrom S, editor. Harvard en- cyclopedia of American ethnic groups. Boston: Auburn House, 1980. Besdine RW. The data base of geriatric medicine. In: Rowe JW, Besdine RW, editors. Health and disease in old age. Boston: Lit- tle, Brown, 1983: 1-14.
44. US. Department of Health and Human Services, Office of the Secretary. Report of the Secretary's Task Force on Black and Mi- nority Health. Executive Summary vol. l, Washington, D.C. 1985.
45. Rogers EM, Shoemaker EF. Communication of Innovations: A Cross-cultural approach. New York: Free Press, 1971.
43.
46. Rosenstock IM. The health belief model and preventive health behavior. Health Educ Monogr 1974; 2(9):354-86.
47. Maslow AH. Toward a psychology of being. New Jersey: D. Van Nostrand Co., 1962.
48. Roberson NL. A community cancer control intervention for Black Americans in Buffalo, New York: a case study. [disserta- tion]. Buffalo, NY: State University of New York at Buffalo, 1985.
49. Norusis MT. SPSS for Windows, release 6.0. Chicago, IL: SPSS Inc., 1993.
50. Mor V, Pacala JT, Rakowski W. Mammography for older women: who uses, who benefits? J Gerontol 1992; 47(Special Is- sue):43-9. Kopans DB. Screening mammography in women over age 65. J Gerontol 1992; 47(Special Issue):59-67.
51.















![Screening for Breast Cancer[1]](https://img.dokumen.tips/doc/110x75/577d2c841a28ab4e1eac7094/screening-for-breast-cancer1.jpg)