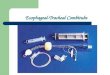
BOUGIE , COMBITUBE , LARYNGEAL TUBE , I-GEL , TRACHLITE ,
TRUVIEW
BOUGIE TRACHLITE , LARYNGEAL TUBE , COMBITUBE , I-GEL ,
TRUVIEW
MODERATOR :- Dr. Sushil Bhati
PRESENTOR :- Dr. Rini Gupta
BOUGIE
Endotracheal tube introducer or intubation catheter
It is important for the clinician, performing intubation and
having the epiglottis-only view, on the first attempt
BOUGIE (Contd.)
Originally produced by Portex and called the Eschmann Stylet
Often called the gum elastic bougie, it is neither made of gum
nor is it elastic; the original design is made of beige colored
resin covering a fiberglass core
The total length of the original version is 60 cm and the distal
tip bends at an angle of30-45 degrees
BOUGIE (Contd.)
Bent distal end makes bougie easier to pass under the epiglottis
and prevents it from advancing too far
narrow diameter (5 mm) provides easier target visualization
compared with a cuffed tracheal tube
It may be solid or hollow.
Hollow bougie allows verification of correct positioning by
fibre optic endoscope , and aids to monitor CO2
TECHNIQUES OF USE
Technique 1:
Do laryngoscopy
Hold bougie in pen like manner
Introduce the lubricated tip of bougie, pointing anteriorly
If tip gets stuck in ant. commisure , rotate it 180 degree and
then advance
As it advances over tracheal rings , clicking sensation is
observed
Contd.
In lightly anaesthetised pt. a cough reflex suggests tracheal
placement
Once the bougie is believed to be in trachea , an assistant
gently advances the ETT over the bougie in railroad like
fashion
Bougie is then withdrawn
Contd.
Connect ETT to breathing system
During nasal intubation, bougie is advanced through nostril into
the larynx. Laryngoscopy is then done and bougie is directed toward
vocal cord under direct vision
Contd.
Technique 2:
- Preinsert the ETT in bougie so that the tip protrudes approx.
5 cm beyond tube
#It saves few seconds in intubation #But makes steering the tip
more difficult
INDICATIONS OF BOUGIE
As an aid to difficult intubation, bougie is considered superior
to stylet
Esp. useful in pt with severly compromised upper airway,
anterior larynx or limited mouth opening
OTHER USES
- For exchanging a ETT : insert a bougie through the existing
tube. Existing tube is then removed and new tube is inserted over
the bougie
- To direct LMA or change existing LMA.
PROBLEMS WITH BOUGIE
TRAUMA : by the force exerted by the tip or by the chipped/
fractured outer layer of bougie
CONTAMINATION
TRACHLITE
It is light-guided intubation device
Uses the principle of transillumination
TRACHLIGHT (CONTD.)
When the tip of the lightwand is placed inside the glottis, a
bright light glow can be seen easily in the soft tissue of the
anterior neck.
No transillumination can be seen, if the lightwand is in
oesophagus
PARTS OF TRACHLIGHT
Consists of 3 parts:
REUSABLE HANDLE-
-made of plastic
-lodges alkaline batteries at one end
-locking clamp on front to secure ETT connector
PARTS OF TRACHLIGHT (contd.)
2) FLEXIBLE WAND-
-:Comes in 3 diff sizes.
-:Its a plastic shaft with bulb at distal end which blinks off
after 30 sec.(to save heat production and to depict apnoea
time)
-:Connector at proximal end ,for attachment of the wand in the
groves of handle.
-The length of the wand can be adjusted by sliding the connector
along the handle.
3) RETRACTABLE STYLET-
allows the wand to be shaped in a J shape or "hockey stick"
configuration
Intubation technique with the TL Preparation
Lubricate the internal stylet and introduced it in the wand
Wand is now mounted on the handle.
The length of the wand is adjusted so that the lightbulb is at
the tip of the ETT
The ETT-TL unit should then be bent at a 90 angle just proximal
to the ETT cuff in the "hockey stick" configuration
Oral intubation
Pt positioned in sniffing position.
The jaw is lifted upward to elevate the epiglottis.
TL is introduced from the lateral corner of the mouth and
repositioned in the midline after entering into the oropharynx.
The midline position is maintained while the device is gently
advanced forward in a rocking motion
The device should not be forced against any resistance
Contd..
A faint glow seen above the thyroid prominence indicates that
the tip of the ETT-TL is located in the glosso-epiglottic fold
.
If the ETT-TL enters the esophagus, no glow can be detected.
A bright glow observed in the lateral aspect of the larynx
indicates that the tip of the ETT-TL is placed in the piriform
fossa, a redirection to the midline is then required.
5 A central, clear and bright transillumination on the
cricothyroid membrane suggests a correct positioning of the
TrachlightTM tip into the laryngeal inlet: it is now safe to
intubate the trachea
Nasal intubation
The most difficult aspect of a blind nasal intubation is to
align the tip of the ETT with the glottis
Transillumination can assist nasal intubation
Remove stylet before insertion of the TL which makes the ETT-TL
more pliable.
Lubricate the nostril
After advancing the tip of the ETT-TL into the oropharynx, the
light is switched on and nasal intubation is performed as described
in the oral intubating technique
Clinical uses of the Trachlight
Useful option in the case of a difficult laryngoscopic
intubations like ,
Congenital abnormalities of upper airway
Acquired abnormalities of upper airway (trauma, etc.)
Limited mandibular protrusion
Short mentohyoid distance
Short neck
Mallampati grade 3, 4
Secretions or blood in the oropharynx
The TL can also be used together with other devices, such as
LMA, the intubating LMA and Direct Laryngoscopy
Limitations, difficulties and contraindications of the
TrachlightTM
LimitationsDifficultiesContraindicationsNo visualization of
pharyngeal and laryngeal structuresSuboptimal transillumination in
grossly obese ptsMistaken tracheal intubation in very thin pts even
if light wand is in oesophagusDifficulties in controlling the tip
of the device in case of accidental partial withdrawal of the
styletUnintentional switching off of the light Difficulties in
withdrawing styletDisturbing effects of the blinking light after 30
sec from switching onTumours of the upper airwayInfections of the
upper airwayForeign body in the upper airway
LARYNGEAL TUBE
Newly developed supraglottic airway device, introduced in U.S.
markets in 2003.
Latex free, silicone made and are easy to insert resulting in
minimal airway trauma.
There are six sizes,
-size 0,1,2 for pt. weighing