Embed Size (px)
Citation preview

7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 112
3
Borderline ovarian tumours
Claes Goumlran Tropeacute MD PhD Professor ab Janne Kaern MD PhD SeniorConsultant a Ben Davidson MD PhD Ass Professor bc
a Department of Gynaecological Oncology Oslo University Hospital The Norwegian Radium Hospital PO Box 4953 NydalenN-0424 Oslo Norwayb Institute of Clinical Medicine Faculty of Medicine University of Oslo Oslo Norwayc Division of Pathology Oslo University Hospital The Norwegian Radium Hospital Oslo Norway
Keywords
borderline ovarian tumours
clinical outcome
epidemiology
management
surgery
fertility
prognostic factors
Borderline ovarian tumours account for 10ndash20 of all epithelial
ovarian cancer Historically standard primary surgery has included
borderline ovarian tumours omentectomy peritoneal washing
and multiple biopsies As one-third of borderline ovarian tumours
are diagnosed in women under the age of 40 years fertility-
sparing treatment has been more frequently used in the past 10years Fertility drugs are well tolerated in women with infertility
after fertility-sparing surgery Careful selection of candidates is
necessary Laparoscopic techniques can be used but should be
reserved for oncologic surgeons This conservative treatment
increases the rate of recurrence albeit with no effect on survival
The pregnancy rate is nearly 50 and most are achieved sponta-
neously These women should be closely followed up The question
is whether this is acceptable from a gynaecologic oncologic point
of view For this reason we will discuss recently published studies
and gynaecologic oncologic concerns about the mode of fertility-
sparing surgery and its consequences
2012 Elsevier Ltd All rights reserved
Introduction
Borderline ovarian tumours (BOT) were 1047297rst described as a separate group in 1929 by Taylor1
characterised by histopathologic features and biologic behaviour intermediate between clearly
benign and frankly malignant ovarian tumours
Corresponding author Department of Gynaecological Oncology Oslo University Hospital The Norwegian Radium Hospital
PO Box 4953 Nydalen N-0424 Oslo Norway Tel thorn47 22 93 56 84 Fax thorn47 22 93 42 48E-mail address cgtropemedisinuiono (CG Tropeacute)
Contents lists available at SciVerse ScienceDirect
Best Practice amp Research Clinical
Obstetrics and Gynaecologyj o u r n a l h o m e p a g e w w w e l s e v i e r c o m l o c a t e b p o bg y n
1521-6934$ ndash see front matter 2012 Elsevier Ltd All rights reserved
doi101016jbpobgyn201112006
Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash336
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 212
In 1973 this group of tumours was accepted by the International Federation of Gynecology and
Obstetrics (FIGO) as carcinoma of low malignant potential2 and from 1973 by the World Health
Organization as BOT3 the term we use today MostBOT are comparable to benign cysts but 10ndash15 may
develop a clinical aggressive behaviour as invasive carcinoma and have the potential to spread beyond
the ovary and have the ability to recur as carcinomas resulting in poor patient prognosis
Thehistologicdiagnosisof BOT isbased on criteriadescribed by Hart andNorris4 anddetailedby Scully5epithelial cellular proliferation (strati1047297cation of the epithelial lining of the papillae multi-layering of the
epithelium mitotic activity and nuclear atypia) without stromal invasion The absence of obvious stromal
invasion is the principal diagnostic criteria for BOT The degree of microinvasion lsquoacceptedrsquo however
depends on the individual pathologist with problematic inter- and intra-observer reproducibility
Incidence
Borderline ovarian tumours represent between 10 and 20 of all epithelial ovarian malignancies6
At the Norwegian Radium Hospital and other large institutions the reported prevalence is lower at
1278 probably re1047298ecting that women with BOT are treated at local hospitals Few population-based
studies on BOT are available Between 1970 and 1993 a total of 2343 women were diagnosed with BOTin Norway9 The age-adjusted incidence rate has increased since 1970 to 48 per 100000 persons per
year between 1995 and 2004 Nearly the same trend has been reported in Sweden 10
In a recent review of 6362 women with BOT by Trillsch et al11 789 of women had stage I disease
and few had abdominal spread whereas stage IV disease represented an exception These1047297gures are in
agreement with a large retrospective Norwegian study of 370 women with BOT treated at the
Norwegian Radium Hospital between 1970 and 19828 In the latter study 311 women (84) were
diagnosed with stage I disease 20 women (6) with stage II and 39 women (10) at stage III None had
stage IV disease Median age at diagnosis was 40 years (27 were younger than 40 years of age)
compared with about 60 years for women with invasive carcinoma1213 and the incidence rate
increased with age up to 45ndash49 years after which the rate stabilised Between 1970 and 1993 in
Norway 93 of women were diagnosed with localised tumours The proportion of tumours withdistant metastases increased from 27 between 1970 and 1973 to 66 between 1989 and 1993 9
Epidemiology
Besides age women with BOT do not seem to differ statistically from women with ovarian carci-
noma in epidemiologic characteristics Primary infertility and nulliparity increase the risk of BOT
whereas oral contraceptives pregnancies and breast feeding are protective factors14
Pathogenesis
Recently a new theory has been developed describing a subset of serous ovarian cystadenomas thatevolve through serous BOT to low-grade epithelial ovarian cancer15ndash18 (Fig 1) This lsquolow-gradersquo
pathway involves mutations in the B-raf and K-ras signalling pathway The pathway involves serous
BOT as a precursor mimicking the adenocarcinoma sequence in colorectal cancer in which carcinoma
evolves through a continuum of histological precursor lesions19ndash21 Only 2 of all serous BOT progress
to carcinoma via the lsquolow-gradersquo pathway17
This is in contrary to the lsquohigh-gradersquo pathway that involves frequent TP53 mutations and very
seldom B-raf and K-ras mutations Most serous ovarian carcinomas belong to the typical high-grade
pathway with no known precursor TP53 mutations are most often absent in typical serous BOT and
micropapillary serous BOT compared with 88 prevalence in invasive serous carcinomas22ndash24
The sequence of malignant transformation from benign mucinous tumours to carcinoma represents
transitional stages of mucinous carcinogenesis Three types of ras oncogenes exist (K N and H) andmucinous BOT have a higher frequency of K-ras mutation thanthatof mucinous cystadenoma but a lower
rate than that of mucinous carcinoma Foci suggesting in-situ malignant changes are often identi1047297ed in
mucinous BOT associated with invasion and the transition may be identi1047297ed microscopically in some
cases2425 It is for the moment unclear whether BRCA1 and BRCA2 mutations increase the risk of BOT12
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336326
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 312
Histology
Nearly all BOT are of the mucinous or serous type the remaining 4ndash5 are of endometrioid clear
cell mixed and transitional cell or Brenner type Serous BOT and mucinous BOT make up 43ndash53 and
425ndash
52 of all BOT respectively891126
Serous borderline tumours
Serous borderline tumours are bilateral in about one-third of cases811 Extra-ovarian spread as peri-
toneal implants is frequent (35) Most implants are non-invasive but invasive implants are found in 20ndash
25 of cases27 Bilaterality and non-invasive implants do not predict worse outcome compared with the
presence of invasive implants1127ndash30 Invasive implants may progress to invasive carcinoma whereas
most peritoneal implants will remain stable or regress after removal of the main ovarian tumour2931
Women with serous BOT without invasive implants have 10-year survival of 95 compared with 60ndash
70 for women with invasive implants12 Women with invasive implants develop progressive disease in
about 30 of cases whereas only about 2 of women without invasive implants will progress2432
Controversy exists about whether tumours with invasive implants are more likely to have micro-
papillary features within the primary BOT at diagnosis2829
Mucinous borderline tumours
Mucinous borderline tumours are histologically classi1047297ed as intestinal (85 of mucinous BOT) or
endocervical (15 of mucinous BOT) (former lsquoMuumlllerianrsquo)1130 The ovarian tumours of the intestinal
subtype can be large and are nearly always unilateral In case of bilaterality the woman should be
further examined for a primary intestinal tumour The endocervical subtype might be bilateral and
associated with endometriosis and mixed-BOT Both subtypes can present with intra-epithelial
carcinoma micro-invasion with less than 10 mm
28
Extraovarian spread is infrequent (10ndash
15) andnearly always as pseudomyxoma peritonei The condition may occur in any type of intra-abdominal
mucinous neoplasm but occurs most often in association with mucinous BOT33 Most of these repre-
sent dissemination from a mucinous appendix tumour An appendectomy should be carried out at
primary surgery for intestinal M-BOT All M-BOT might recur as invasive adenocarcinoma especially
Fig 1 Low-grade pathway frequent B-raf and K-ras mutations (61ndash68) lowcellular proliferation gradual 53 mutations (70) high
cellular proliferation high chromosomal instability frequent HLA-Gexpression 5-year survival about 30 APST atypical proliferative
serous tumours MPSC micropapillary serous carcinoma SBT serous borderline ovarian tumour Published with permission 17
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 327
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 412
when only ovarian cystectomy rather than salpingo-oophorectomy has been carried out This might be
explained by missing an invasive component owing to inadequate histopathologic evaluation of these
large tumours Therefore unilateral salpingo-oophorectomy is recommended in mucinous BOT1114
Prognostic factors
As BOT in general has an excellent survival it might be dif 1047297cult to identify variables that improve
survival As many women with BOT are of reproductive age at diagnosis more conservative treatment
preserving thechildbearingability is desirable International Federation of Gynecologyand Obstetrics stage
is thestrongest prognostic factor for recurrence andsurvival for BOT as well as for invasive ovariancancers
Micropapillary histology was reported as an additional risk factor for serous BOT but this issue is contro-
versial as poor prognosis is only seen if this histology is associated with invasive implants2834ndash36 Tumours
with evidence of stromal invasion of less than 10 mm2 behave clinically as BOT and are today classi1047297ed as
BOT222437ndash40 In the retrospective study from the Norwegian Radium Hospital41 370 BOT were treated
between 1970 and 1982 and the follow up was complete with a median follow-up time of 152 months
(range 6ndash354 months) By multivariate analysis the only three independent prognostic factors for disease-
free and long-term survival were FIGO stage (P lt 00001) histologic type (P lt 005) and age (P lt 0005) Inanother study of the same women including DNA ploidy the women could be divided into risk groups41
The low-risk group (100 disease-free survival) was characterised by stage I disease diploid serous BOTor
mucinous BOT and age less than 40 years The high-risk group (75 or higher risk of dying of disease) had
aneuploid serous BOT or mucinous BOT stage II-III disease and age older than 70 years Deoxyribonucleic
acid ploidy was the strongest prognostic factor in BOT in the study by Kaern et al41 but this has unfortu-
nately not been reproduced by others4243 Lymph-node involvement could not convincingly be con1047297rmed
to be an independent risk factor35414445
Symptoms
Limited information exists about symptom registration by women with BOT at diagnosis Mostwomen may be asymptomatic and a pelvic mass discovered at routine pelvic examination Symptoms
are less common compared with symptoms registered for women with invasive ovarian cancer
although 75 of women with BOT may have at lease one symptom as abdominal pain or discomfort
bowel irregularity and persisting fatigue or weight loss4647
Standard treatment
The diagnosis of BOT cannot be determined before surgery Intraoperative frozen section diagnosis
of BOT is often dif 1047297cult even for experienced pathologists Frozen sections may be useful for
discrimination between BOTand epithelial ovarian cancer and benign tumour (over-diagnosis less than
10) but not for discrimination between BOT and epithelial ovarian cancer (under-diagnosis in 25ndash
30of women)4849 Less than 50 of women with BOT will have a complete surgical staging this without
obvious in1047298uence on survival
The standard guidelines for primarysurgery in BOTaresimilar to these for invasive ovarian carcinomas
removal of all macroscopic disease and proper surgical staging hysterectomy with bilateral salpingo-
oophorectomy multiple peritoneal biopsies and peritoneal washing with cytology For mucinous BOT
appendectomy should also be carried out33 Lymph-node sampling has not been part of the standard
procedure A recently published German study reported systematic lymph-node dissection in 189 of
women with BOT11 Involvement of lymph nodes even with upstage do not in1047298uence recurrence or
survival rate850 Lymph-node involvement is rarely seen in M-BOT Lymphadenectomy can be omitted
even for stage II and III disease as there is no difference in the recurrence or survival rate (Fig 2)5051
Restaging procedures
Despite the fact that experts have recommended comprehensive surgical staging for many years most
women referred to university or comprehensive cancer centres after primary surgery have incomplete
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336328
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 512
surgery Another common event is that malignancy is not suspected at the initial operation and therefore
the abdomen is not properly explored Should this woman undergo re-operation Snider et al52 upstaged
1047297ve out of 27 women with stage I disease None of the 12 women with mucinous BOT were upstaged
whereas1047297veoutof 13 women with serous BOTwere upstagedMucinousBOTgrossly con1047297ned to one ovary
are probably unlikely to be upstaged at a restaging procedure If evidence of extra-ovarian disease exists
complete surgical staging and appendectomy are indicated Mucinous BOT with abdominal spread are in50 claimed to arise in the appendix or simultaneously in one or both ovaries5354 For serous BOT it is
reasonable to do a second operation as lymph-node involvement has been reported in about 20 in
apparentstage I tumourswitheven higher incidence in more advanced stages45 At the Norwegian Radium
Hospital we recommend restaging if the women are insuf 1047297ciently staged at primary operation in agree-
ment with Cadron et al51 and Trimble and Trimble55 We also believe that the decision to restage must be
individualised taking into consideration the adequacy of the previous abdominal exploration the tumour
subtype and potential treatment of residual disease as well as thelevel of concern for both thewomanand
the clinician even if there is little proof that restaging operations have an effect on survival115056ndash58
Laparoscopy
Laparoscopic treatment has become an attractive approach for benign ovarian tumours (pelvic
mass) The development of the laparoscopic techniques with the use of endo-bag gives less risk of
spillage during surgery and less port-side metastases For conservatively treated women wishing to
preserve fertility this is a more favourable approach and has short postoperative recovery fewer
adhesions and improved cosmetic results59 Cyst rupture and incomplete staging occur signi1047297cantly
more frequently by laparoscopy compared with laparotomy (339 v 124)6061 but do not in1047298uence
survival The laparoscopic treatment may result in higher recurrence rate which must be discussed
with the woman The woman should agree to close follow up and repeated surgery5162 Other concerns
are port metastases63 and improper staging61
Postoperative treatment of borderline ovarian tumours
Today there is no proven bene1047297t from adjuvant therapy (chemotherapy or radiotherapy) even in
advanced stage disease and in the presence of invasive implants1432 No randomised-controlled studies
Fig 2 Recommendation treatmentof borderline ovarian tumours Modi1047297ed fromTrillsch et al11 and Cadron et al51 with permission
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 329
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 612
have evaluated the ef 1047297cacy of chemotherapy in advanced stage BOT with residual disease Cisplatin-
based therapy in serous BOT with residual disease have shown high response rates but modest
effect on long-term survival1464 In case of recurrences where transformation to an invasive histology
has occurred consideration of platinum-taxane-based chemotherapy is reasonable The molecular
changes transforming BOT to invasive ovarian carcinoma may be clari1047297ed in the future with the
possibility of blocking the different lsquostepsrsquo in the carcinogenesis Today we know that both serous BOTand low-grade serous carcinoma frequently present with B-raf and K-ras mutations11
Survival
Overall survival for women with BOT is excellent 90ndash100 in most reports depending on age at
diagnosis FIGO stage and histologic type112651626566 Trillsch et al11 reported a 5-year overall survival
rate of almost 100 in early stage disease (FIGO I-II) and between 86 and 92 in more advanced
disease (FIGO III-IV) In a Norwegian population-based study67 the age-adjusted 1- 3- 5- and 10-year
relative survival rates of women with mucinous BOT were 98 97 97 and 95 respectively and for
women with serous BOT 96 93 90 and 90 respectively The relative risk of dying increased with
higher age at diagnosis The 5-year relative survival for women aged between 0 and 44 years was 99compared with 85 for women aged 75ndash89 years Nearly the same 1047297gures are reported by Sherman
et al12 with better survival for younger women and slightly better survival for serous tumours
compared with mucinous tumours although mucinous tumours in advanced stage had the poorest
long-term survival (855)12
Seidman and Kurman35 summarised 97 reports including a total of 4129 women with serous BOT
and showed a disease-speci1047297c survival rate of 99 for stage I disease and 953 for stage III disease
(mean follow up of 7 years)35 The 5-year survival was 98 for women with serous BOT with non-
invasive implants and 33 for those with invasive implants68
Conservative surgery
The median age of diagnosis for women with BOT is 40 years and nearly one-third are younger than
40 years Thus preservation of childbearing potential is an important issue for many of these women
To select women for fertility-sparing surgery without risk of reduced long-term survival is a challenge
for the gynaecologic oncologist3069 (Fig 2) Conservative surgery is de1047297ned as complete staging in
which the uterus and at least a part of one ovary are preserved1162 (Fig 2)
Although the standard treatment for all women with BOT is at least bilateral salpingo-
oophorectomy many young women with stage Ia tumours who have not completed childbearing
can be safely treated with unilateral salpingo-oophorectomy after comprehensive surgical staging
thereby preserving the fertility potential At least as important as the fertility issue however is
whether we can reduce the morbidity caused by radical surgery and whether a more conservative
approach is a safe alternative regarding cancer prognosis51
Recent studies from the Norwegian RadiumHospital8 and Gynecologic Oncology Group65 have shown that preservation of reproductive organs is
feasible Relapse rates after bilateral salpingo-oophorectomy range between 0 and 20 This rate
varies between 12 and 58 for cystectomy and between 25 and 57 for radical surgery Relapses
can also occur late and recurrences as late as 39 years after initial treatment have been reported5134
Predictors of relapse are resection margins containing tumour cells70 The frequency of persistence or
recurrence in 35 patients with serous-BOT treated by unilateral cystectomy bilateral cystectomy or
unilateral cystectomy with contralateral oophorectomy or salpingo-oophorectomy was retrospectively
investigated by Lim-Tan et al71 Conservative surgical treatment was carried out either because the
women were young and wanted to preserve their fertility or because the nature of the tumour was not
determined at the time of surgery Thirty-three women had stage I disease (19 stage Ia 10 stage Ib and
four stage Ic) and two had stage III disease Although 60 of the women had additional and in somecases de1047297nitive operations within relative short periods after initial cystectomy or cystectomies 21 had
conservation of ovarian tissue and were followed on average for 75 years All women with stage I
disease were alive without evidence of disease after surgical treatment alone The presence of
persistent or recurrent disease correlated with multifocality and involvement of resection margins
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336330
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 712
Multifocality may be a strong predictor of failure of cystectomy to control the disease No recurrence of
disease was seen in ovaries from which a single cyst had been removed with negative resection
margins Extensive sampling of the resection margins of ovarian cysts is important71
For many women with BOT fertility is an important issue It is therefore essential to discuss with
these young women the advantages and disadvantages between conservative and radical surgery
Conservative surgery preserves fertility and hormonal function but unfortunately with high risk of recurrence
In women with obvious stage I disease unilateral salpingo-oophorectomy or cystectomy has from
previous studies been shown to be safe This has also been con1047297rmed for women with advanced-stage
disease on the assumption of close follow up
Even for women with advanced disease conservative surgery might be considered after informed
consent The recurrence rate is high and invasive and even non-invasive implants may recur up to 15
as invasive OC without negative in1047298uence on survival34567273
Treatment at recurrent disease after conservative treatment
Early detected recurrences are curable with repeated surgery113451 and therefore conservativetreatment might again be considered in women with recurrent disease if fertility still is an issue and the
woman is informed about the high risk of recurrence and agrees on close follow up accepting repeated
surgery5162 If invasive implants are diagnosed this procedure could not be recommended In any case
of recurrent disease secondary debulking surgery is important as women suboptimally debulked have
poor survival115174
Fertility after conservative management of borderline ovarian tumour
Infertility is frequently observed inwomen with BOT A history of infertility beforediagnosis has been
reported in 10ndash35 of women75ndash77 To allow conservative surgery careful evaluation of the extent of
disease by the gynaecologist at the time of operation and meticulous examination of the cystectomyspecimen by the gynaecologist and pathologist are desirable to determine the prognosis after cys-
tectomy In a study by Morris et al76 onewoman who had disease-related deathwasnot staged properly
In a meta-analysis by Maltaris et al78 1483 women had BOT of whom 656 were treated conservatively
(442) A total of 196 women became pregnant and 111 relapsed after unilateral salpingo-
oophorectomy only one woman died from the disease (015) The investigators therefore suggest
that conservative surgery is justi1047297able for some women with a good prognostic index Unilateral
oophorectomy omentectomy and appendectomy in stage Ia diploid mucinous BOT are indicated for
young women who wish to preservefertility (Fig 2) In stage Ia diploid serous BOT thesame procedure is
safe if the contralateral ovary is macroscopically normal Careful inspection of a macroscopically normal
contralateral ovary should be suf 1047297cient inyoung womenwith stageIa disease who wish to remainfertile
Surgery itself can impair the fertility function by loss of ovarian tissue pelvic scarring and adhesionsblocking the fallopian tube Post-surgery fertility factors such as ovulation fallopian tubes and sperm
factors should be investigated and treated if necessary About one-third of women undergoing
conservative surgery for BOT will be able to conceive with no negative in1047298uence of pregnancy on the
disease60727779 Ovulation induction is often required in order to conceive80 The role of ovulation
(in-vitro [IVF] fertilisation) drugs in BOT is currently under debate7780ndash84
Recently a large nationwide cohort study of 19146 subfertile women in the Netherlands who
received IVF drugs between 1983 and 1995 and a comparison group of 6953 subfertile women who
were not treated was published After a median follow up of 15 years a total of 77 ovarian malignancies
were observed in the cohort including 42 women with epithelial ovarian cancer and 35 women with
BOT Sixty-one ovarian malignancies were observed in the IVF-group and 16 in the unexposed (control)
group The ratio hazard for epithelial ovarian cancer and BOT was 167 (074 to 375) and 425 (127 to1418) respectively85 The conclusion of Burger et al85 was that IVF increases the risk of BOT
A worrying1047297nding of their study is the increased risk of epithelial ovarian cancer and BOT even after 15
years of follow up Fasouliotis et al80 found no perceptible negative effect of previous BOT on preg-
nancy rates after IVF The same was shown by Fortin et al84 in a study of 30 women treated with IVF
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 331
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 812
drugs for infertility after conservative surgery Thirteen pregnancies were observed Disease in four
women recurred All recurrences were BOT on a remaining ovary that had been treated by surgery
alone All women are currently disease-free after secondary surgery Fortin et al84 concluded that IVF
drugs can be used safely in womenwho develop infertility after conservative treatment of BOT Because
of the low number of women treated with IVF drugs Norwegian Radium Hospital guidelines are to
proceed with caution and only women with early stage BOT are permitted to be treated with IVF drugsThe latest development regarding reproduction and BOT is cryopreservation 86 Women who have
their ovaries removed because of large stage Ib BOT now have a possibility of becoming pregnant
Biopsies from normal ovarian cortex can be taken during the primary operation In 2004 a live birth
after a fresh ovarian tissue transplant in a primate was reported87 Donnez et al86 described in 2004
a live birth after orthotopic auto-transplantation of cryopreserved ovarian tissue Their1047297ndings opened
new possibilities for young women facing premature ovarian failure
Women with reduced fertility after surgery can consider ovarian stimulation egg retrieval and egg
freezing Ovarian stimulation and exposure to high oestrogen exposure do not seem to increase the risk
for recurrence Nor do pregnancies have negative in1047298uence on survival7277
To assure future fertility preservation in women with BOT the gynaecologic oncologist should
collaborate closely with the reproductive endocrinologists even before surgery Until more mature dataexist the general recommendation is a limited number of stimulation cycles only for stage I patients In
case of bilateral salpingo-oophorectomy cryopreservation of ovarian cortex biopsy from the less
affected ovary could be considered although this is not always technically possible1151
Follow up
Follow up should be long term and lifelong because recurrences may develop after more than 15 years
In conservatively treated womenclose follow up is crucial with special attentionto theremainingovaryIt
is still debated if the remaining ovary (and uterus) should be removed after the family is completed For
low-risk BOT there is no indication for this procedure but in women with high-risk of recurrence the
procedure is optional the alternative being to wait until recurrence or carry out radical surgery Manywomen will choose radical surgery when the family is completed because of psychological stress
The general recommendation is follow up every 3 months during the 1047297rst 2 years and then every 6
months for the next 3 years and annually thereafter The women is followed with pelvic examination
transvaginal ultrasound and calcium 125 measurement1451 (Fig 2)
Future direction of borderline ovarian tumour
A key issue for future research on BOTconcerning epidemiology is the identi1047297cation of risk factors for
invasive implants recurrences and death and also the identi1047297cation of predisposing heritable factors
For clinical management improved methods for preoperative and intraoperative diagnosis should
be considered in addition to the role of laparoscopic surgery in removal of complex cysts improvedmethods for distinguishing metastases from BOT and determination of risk associated with conser-
vative treatment
For pathology and molecular biology molecular studies are needed to assess the relationship
between serous BOT low-grade serous carcinoma and high-grade serous carcinoma Molecular studies
are also needed to aid in the characterisation of implants and studies need to be conducted to
determine the biology of microinvasive BOT and the clinical signi1047297cance of long-term follow up
Conclusion
Borderline ovarian tumours are ovarian tumours with good prognosis that account for 10ndash20 of all
epithelial ovarian cancer Historically standard primarysurgeryincludedbilateral salpingo-oophorectomyomentectomy peritoneal washing and complete peritoneal resection of macroscopic lesions or multiple
biopsies In cases of M-BOT women are also treated with appendectomy As one-third of BOT are diagnosed
inwomenyounger than40 years however fertility-sparingtreatment (ie preservation of the uterus andat
least part of one ovary) has been increasingly used in the past 10 years Fertility drugs are well tolerated in
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336332
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 912
women with infertility after fertility-sparing surgery Careful selection of candidates is necessary Lapa-
roscopic techniques can be used but are reserved for oncologic surgeons This conservative treatment
increases therateof recurrencebutwithoutany effecton survivalThespontaneouspregnancy rate is nearly
50and most are achieved spontaneously Spontaneous pregnancy can occurafter conservative treatment
of advanced-stage BOT (with non-invasive implants) These women should be closely followed up Further
research has to concentrate on clinical risk-factors histopathological markers and pathogenesis to guar-antee the best clinical management for women with BOT
Con1047298ict of interest statement
None declared
Practice points
BOTare ovarian tumours with good prognosis that account for 10ndash20 of all epithelial ovarian
cancer Historically standard primary surgery included bilateral salpingo-oophorectomy omentec-
tomy peritoneal washing and complete peritoneal resection of macroscopic lesions or
multiple biopsies
In case of mucinous BOT women are also treated with appendectomy
Adjuvant therapy for the treatment of BOT has no proven bene1047297t
As one-third of BOT are diagnosed in women younger than 40 years fertility-sparing treat-
ment (ie preservation of the uterus and at least part of one ovary) has been increasingly used
in the past 10 years
Fertility drugs are well tolerated in women with infertility after fertility-sparing surgery
Careful selection of candidates is necessary
Laparoscopic techniques can be used but are reserved for oncologic surgeons Spontaneous pregnancy can occur after conservative treatment of advanced stage BOT (with
non-invasive implants)
These women should be closely followed up
Research agenda
Epidemiology
Identify risk factors for invasive implants recurrences and death
Identify predisposing heritable factors
Clinical management
Improve methods for preoperative and intraoperative diagnosis
Further explore the role of laparoscopic surgery in the removal of complex cysts
Improve methods for distinguishing metastases from BOTand determine risk associated with
conservative treatment
Pathology and molecular biology
Conduct molecular studies to assess the relationship between serous BOT low-grade serous
carcinoma and high-grade serous carcinoma Conduct molecular studies to aid in the characterisation of implants
Conduct studies to determine the biology of microinvasive BOTand the clinical signi1047297cance of
long-term follow up
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 333
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1012
Acknowledgement
We wish to thank Mrs Gry Seppola for technical assistance and gratefully acknowledge the1047297nancial
support from the Inger and John Fredriksen Foundation for Ovarian Cancer Research
References
1 Taylor HC Malignant and semi-malignant tumors of the ovary Surg Gynecol Obstet 1929 48 204ndash2302 Kottmeier HL Kolstad P McGarrity KA Annual report on results of treatment in gynaecologic cancer vol 17 Statements of
results obtained in 1969ndash1972 inclusive FIGO Stockholm Sweden Editorial of 1047297ce Radiumhemmet 19733 Serov SF Scully RE amp Sobin LH International histological classi 1047297cation of tumors no 9 Histoloigcal typing of ovarian tumours
Geneval World Health Organization 19734 Hart WR amp Norris HJ Borderline and malignant mucinous tumors of the ovary Histologic criteria and clinical behavior
Cancer 1973 31 1031ndash10455 Scully RE Tumors of the ovary and maldeveloped gonads Fascicle 16 In Atlas of tumor pathology Second series Wash-
ington DC Armed Forces Institute of Pathology 1979 pp 75ndash906 Lenhard MS Mitterer S Kuumlmper C et al Long-term follow-up after ovarian borderline tumor relapse and survival in
a large patient cohort Eur J Obstet Gynecol Reprod Biol 2009 145 189ndash194
7 Quirk JT amp Natarajan N Ovarian cancer incidence in the United States 1992ndash
1999 Gynecol Oncol 2005 97 519ndash
5238 Kaern J Tropeacute CG amp Abeler VM A retrospective study of 370 borderline tumors of the ovary treated at the NorwegianRadium Hospital from 1970 to 1982 A review of clinicopathologic features and treatment modalities Cancer 1993 711810ndash1820
9 Bjoslashrge T Engeland A Hansen S et al Trends in the incidence of ovarian cancer and borderline tumours in Norway1954ndash1993 Int J Cancer 1997 71 780ndash786
10 Skiacuternisdoacutettir I Garmo H Wilander E et al Borderline ovarian tumors in Sweden 1960ndash2005 trends in incidence and age atdiagnosis compared to ovarian cancer Int J Cancer 2008 123 1897ndash1901
11 Trillsch F Mahner S Ruetzel J et al Clinical management of borderline ovarian tumors Expert Rev Anticancer Ther 2010 101115ndash1124
12 Sherman ME Mink PJ Curtis R et al Survival among women with borderline ovarian tumors and ovarian carcinomaa population-based analysis Cancer 2004 100 1045ndash1052
13 Kramer JL Greene MH Epidemiology of ovarian fallopian tube and primary peritoneal cancer In Gershenson DMMcGuire WP Gore M et al eds Gynecologic cancer Controversies in management 1st ed Philadelphia Elsevier ChurchillLivingstone 2004 pp 327ndash340
14 Tropeacute C Davidson B Paulsen T et al Diagnosis and treatment of borderline ovarian neoplasms lsquothe state of the artrsquo Eur J Gynaecol Oncol 2009 30 471ndash482
15 Kurman RJ amp Shih IeM Pathogenesis of ovarian cancer lessons from morphology and molecular biology and their clinicalimplications Int J Gynecol Pathol 2008 27 151ndash160
16 Kurman RJ Visvanathan K Roden R et al Early detection and treatment of ovarian cancer shifting from early stage tominimal volume of disease based on a new model of carcinogenesis Am J Obstet Gynecol 2008 198 351ndash356
17 Shih IeM amp Kurman RJ Ovarian tumorigenesis a proposed model based on morphological and molecular genetic analysis Am J Pathol 2004 164 1511ndash1518
18 Levanon K Crum C amp Drapkin R New insights into the pathogenesis of serous ovarian cancer and its clinical impact J ClinOncol 2008 26 5284ndash5293
19 Meinhold-Heerlein I Bauerschlag D Hilpert F et al Molecular and prognostic distinction between serous ovarian carci-nomas of varying grade and malignant potential Oncogene 2005 24 1053ndash1065
20 Bonome T Lee JY Park DC et al Expression pro1047297ling of serous low malignant potential low-grade and high-grade tumorsof the ovary Cancer Res 2005 65 10602ndash10612
21 Mahner S Baasch C Schwarz J et al C-Fos expression is a molecular predictor of progression and survival in epithelialovarian carcinoma Br J Cancer 2008 99 1269ndash1275
22 Ortiz BH Ailawadi M Colitti C et al Second primary or recurrence Comparative patterns of p53 and K-ras mutationssuggest that serous borderline ovarian tumors and subsequent serous carcinomas are unrelated tumors Cancer Res 200161 7264ndash7267
23 Lee KR Tavassoli FA Prat J et al Tumours of the ovary and peritoneum In Tavassoli FA amp Devilee P (eds) Pathology and
genetics Tumours of the breast and female genital organs Lyon IARC Press 2003 pp 113ndash20224 Oedegaard E Ovarian carcinomas and borderline ovarian tumors - molecular markers and operative treatment Dissertation
Facutly of Medicine University of Oslo 200825 Mok SC Bell DA Knapp RC et al Mutation of K-ras protooncogene in human ovarian epithelial tumors of borderline
malignancy Cancer Res 1993 53 1489ndash149226 du Bois A Ewald-Riegler N du Bois O et al Borderline tumors of the ovary a systematic review [German] Geburtsh
Frauenheilk 2009 69 807ndash83327 Seidman JD Horkayne-Szakaly I Haiba M et al The histologic type and stage distribution of ovarian carcinomas of surface
epithelial origin Int J Gynecol Pathol 2004 23 41ndash44
28 Prat J amp De Nictolis M Serous borderline tumors of the ovary a long-term follow-up study of 137 cases including 18 witha micropapillary pattern and 20 with microinvasion Am J Surg Pathol 2002 26 1111ndash1128
29 Bell DA Weinstock MA amp Scully RE Peritoneal implants of ovarian serous borderline tumors Histologic features andprognosis Cancer 1988 62 2212ndash2222
30 Tinelli R Tinelli A Tinelli FG et al Conservative surgery for borderline ovarian tumors a review Gynecol Oncol 2006 100
185ndash191
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336334
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1112
31 Kurman RJ amp Trimble CL The behavior of serous tumors of low malignant potential are they ever malignant Int J Gynecol
Pathol 1993 12 120ndash12732 Morice P Camatte S Rey A et al Prognostic factors for patients with advanced stage serous borderline tumours of the
ovary Ann Oncol 2003 14 592ndash59833 Bradley RF Stewart 4th JH Russell GB et al Pseudomyxoma peritonei of appendiceal origin a clinicopathologic analysis of
101 patients uniformly treated at a single institution with literature review Am J Surg Pathol 2006 30 551ndash559
34 Silva EG Gershenson DM Malpica A et al The recurrence and the overall survival rates of ovarian serous borderlineneoplasms with noninvasive implants is time dependent Am J Surg Pathol 2006 30 1367ndash137135 Seidman JD amp Kurman RJ Ovarian serous borderline tumors a critical review of the literature with emphasis on prognostic
indicators Hum Pathol 2000 31 539ndash55736 Chang SJ Ryu HS Chang KH et al Prognostic signi1047297cance of the micropapillary pattern in patients with serous borderline
ovarian tumors Acta Obstet Gynecol Scand 2008 87 476ndash48137 Fox H amp Wells M Surface epithelialstromal tumors of the ovary In Fox H amp Wells M (eds) Haines and Taylor Obstetrical and
Gynaecological Pathology 5th ed London Churchill Livingstone 2003 pp 713ndash74338 Ren J Peng Z amp Yang K A clinicopathologic multivariate analysis affecting recurrence of borderline ovarian tumors Gynecol
Oncol 2008 110 162ndash16739 Longacre TA McKenney JK Tazelaar HD et al Ovarian serous tumors of low malignant potential (borderline tumors)
outcome-based study of 276 patients with long-term (gt or frac145-year) follow-up Am J Surg Pathol 2005 29 707ndash72340 Cusidoacute M Balagueroacute L Hernandez G et al Results of the national survey of borderline ovarian tumors in Spain Gynecol
Oncol 2007 104 617ndash62241 Kaern J Tropeacute CG Kristensen GB et al DNA ploidy the most important prognostic factor in patients with borderline
tumors of the ovary Int J Gynecol Cancer 1993 3 349ndash35842 Meyer JS Gersell DJ amp Yim S Cell proliferation in ovarian carcinoma superior accuracy of S-phase fraction (SPF) by DNA
labeling index versus 1047298ow cytometric SPF lack of independent prognostic power for SPF and DNA ploidy and limitedeffect of SPF on tumor growth rate Gynecol Oncol 2001 81 466ndash476
43 Verbruggen MB van Diest PJ Baak JP et al The prognostic and clinical value of morphometry and DNA cytometry inborderline ovarian tumors a prospective study Int J Gynecol Pathol 2009 28 35ndash40
44 Yokoyama Y Moriya T Takano T et al Clinical outcome and risk factors for recurrence in borderline ovarian tumours Br J Cancer 2006 94 1586ndash1591
45 Leake JF Rader JS Woodruff JD et al Retroperitoneal lymphatic involvement with epithelial ovarian tumors of lowmalignant potential Gynecol Oncol 1991 42 124ndash130
46 Paulsen T Kaern J Kjaerheim K et al Symptoms and referral of women with epithelial ovarian tumors Int J Gynaecol Obstet 2005 88 31ndash37
47 Paulsen T Epithelial ovarian cancer A clinical epidemiological approach on diagnosis and treatment Dissertation Faculty of Medicine University of Oslo 2007
48 Tropeacute CG Kristensen G amp Makar A Surgery for borderline tumor of the ovary Semin Surg Oncol 2000 19 69ndash7549 Tempfer CB Polterauer S Bentz EK et al Accuracy of intraoperative frozen section analysis in borderline tumors of the
ovary a retrospective analysis of 96 cases and review of the literature Gynecol Oncol 2007 107 248ndash25250 Camatte S Morice P Thoury A et al Impact of surgical staging in patients with macroscopic lsquostage Irsquo ovarian borderline
tumours analysis of a continuous series of 101 cases Eur J Cancer 2004 40 1842ndash184951 Cadron I Leunen K Van Gorp T et al Management of borderline ovarian neoplasms J Clin Oncol 2007 25 2928ndash293752 Snider DD Stuart GC Nation JG et al Evaluation of surgical staging in stage I low malignant potential ovarian tumors
Gynecol Oncol 1991 40 129ndash13253 Ronnett BM Kurman RJ Zahn CM et al Pseudomyxoma peritonei in women a clinicopathologic analysis of 30 cases with
emphasis on site of origin prognosis and relationship to ovarian mucinous tumors of low malignant potential Hum Pathol
1995 26 509ndash52454 Seidman JD Elsayed AM Sobin LH et al Association of mucinous tumors of the ovary and appendix A clinicopathologic
study of 25 cases Am J Surg Pathol 1993 17 22ndash3455 Trimble EL amp Trimble LC Epithelial ovarian tumors of low malignant potential In Markman M amp Hoskins W (eds) Cancer
of the Ovary New York Raven Press 1993 pp 415ndash429
56 Zanetta G Rota S Chiari S et al Behavior of borderline tumors with particular interest to persistence recurrence andprogression to invasive carcinoma a prospective study J Clin Oncol 2001 19 2658ndash266457 Fauvet R Boccara J Dufournet C et al Restaging surgery for women with borderline ovarian tumors results of a French
multicenter study Cancer 2004 100 1145ndash115158 Zapardiel I Rosenberg P Peiretti M et al The role of restaging borderline ovarian tumors single institution experience and
review of the literature Gynecol Oncol 2010 119 274ndash27759 Def 1047297eux X Morice P Camatte S et al Results after laparoscopic management of serous borderline tumor of the ovary with
peritoneal implants Gynecol Oncol 2005 97 84ndash8960 Fauvet R Boccara J Dufournet C et al Laparoscopic management of borderline ovarian tumors results of a French
multicenter study Ann Oncol 2005 16 403ndash41061 Vandenput I Amant F amp Vergote I Peritoneal recurrences might be less common in advanced stage serous borderline
ovarian tumors that were treated by laparotomy Gynecol Oncol 2005 98 52362 CadronI Amant F VanGorp Tet alThe management of borderline tumours of theovary Curr Opin Oncol 2006 18 488ndash49363 Vergote I De Brabanter J Fyles A et al Prognostic importance of degree of differentiation and cyst rupture in stage I
invasive epithelial ovarian carcinoma Lancet 2001 357 176ndash182
64 Gershenson DM amp Silva EG Serous ovarian tumors of low malignant potential with peritoneal implants Cancer 1990 65578ndash585
65 Gershenson DM Clinical management potential tumours of low malignancy Best Pract Res Clin Obstet Gynaecol 2002 16513ndash527
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 335
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1212
66 Heintz AP Odicino F Maisonneuve P et al Carcinoma of the ovary FIGO 26th Annual Report on the Results of Treatment inGynecological Cancer Int J Gynaecol Obstet 2006 95(Suppl 1) S161ndashS192
67 Bjoslashrge T Engeland A Hansen S et al Prognosis of patients with ovarian cancer and borderline tumours diagnosed inNorway between 1954 and 1993 Int J Cancer 1998 75 663ndash670
68 Seidman JD amp Kurman RJ Subclassi1047297cation of serous borderline tumors of the ovary into benign and malignant typesA clinicopathologic study of 65 advanced stage cases Am J Surg Pathol 1996 20 1331ndash1345
69 Sherman ME Berman J Birrer MJ et al Current challenges and opportunities for research on borderline ovarian tumorsHum Pathol 2004 35 961ndash97070 Leake JF Currie JL Rosenshein NB et al Long-term follow-up of serous ovarian tumors of low malignant potential Gynecol
Oncol 1992 47 150ndash15871 Lim-Tan SK Cajigas HE amp Scully RE Ovarian cystectomy for serous borderline tumors a follow-up study of 35 cases Obstet
Gynecol 1988 72 775ndash78172 Morice P Camatte S El Hassan J et al Clinical outcomes and fertility after conservative treatment of ovarian borderline
tumors Fertil Steril 2001 75 92ndash9673 Camatte S Morice P Pautier P et al Fertility results after conservative treatment of advanced stage serous borderline
tumour of the ovary BJOG 2002 109 376ndash38074 Crispens MA Bodurka D Deavers M et al Response and survival in patients with progressive or recurrent serous ovarian
tumors of low malignant potential Obstet Gynecol 2002 99 3ndash1075 Fauvet R Poncelet C Boccara J et al Fertility after conservative treatment for borderline ovarian tumors a French
multicenter study Fertil Steril 2005 83 284ndash29076 Morris RT Gershenson DM Silva EG et al Outcome and reproductive function after conservative surgery for borderline
ovarian tumors Obstet Gynecol 2000 95 541ndash54777 Gotlieb WH Flikker S Davidson B et al Borderline tumors of the ovary fertility treatment conservative management and
pregnancy outcome Cancer 1998 82 141ndash14678 Maltaris T Boehm D Dittrich R et al Reproduction beyond cancer a message of hope for young women Gynecol Oncol
2006 103 1109ndash112179 Beiner ME Gotlieb WH Davidson B et al Infertility treatment after conservative management of borderline ovarian
tumors Cancer 2001 92 320ndash32580 Fasouliotis SJ Davis O Schattman G et al Safety and ef 1047297cacy of infertility treatment after conservative management of
borderline ovarian tumors a preliminary report Fertil Steril 2004 82 568ndash57281 Kashyap S amp Davis OK Ovarian cancer and fertility medications a critical appraisal Semin Reprod Med 2003 21 65ndash7182 Morice P Camatte S Wicart-Poque F et al Results of conservative management of epithelial malignant and borderline
ovarian tumours Hum Reprod Update 2003 9 185ndash19283 Whittemore AS Harris R amp Itnyre J Characteristics relating to ovarian cancer risk collaborative analysis of 12 US case-
control studies II Invasive epithelial ovarian cancers in white women Collaborative Ovarian Cancer Group Am J Epi-demiol 1992 136 1184ndash1203
84 Fortin A Morice P Thoury A et al Impact of infertility drugs after treatment of borderline ovarian tumors results of a retrospective multicenter study Fertil Steril 2007 87 591ndash596
85 Burger CW van de Swaluw A Mooij TM et al Risk of borderline and invasive ovarian tumors after ovarian stimulation forin vitro fertilization in a large Dutch cohort after 15 years of follow-up Abstracts presented for the 40th Annual Meeting of the Society of Gynecologic Oncologists February 2009 (abstract no 6) Gynecol Oncol 2009 112(Suppl) S4
86 Donnez J Dolmans MM Demylle D et al Livebirth after orthotopic transplantation of cryopreserved ovarian tissue Lancet 2004 364 1405ndash1410
87 Lee DM Yeoman RR Battaglia DE et al Live birth after ovarian tissue transplant Nature 2004 428 137ndash138
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336336

7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 212
In 1973 this group of tumours was accepted by the International Federation of Gynecology and
Obstetrics (FIGO) as carcinoma of low malignant potential2 and from 1973 by the World Health
Organization as BOT3 the term we use today MostBOT are comparable to benign cysts but 10ndash15 may
develop a clinical aggressive behaviour as invasive carcinoma and have the potential to spread beyond
the ovary and have the ability to recur as carcinomas resulting in poor patient prognosis
Thehistologicdiagnosisof BOT isbased on criteriadescribed by Hart andNorris4 anddetailedby Scully5epithelial cellular proliferation (strati1047297cation of the epithelial lining of the papillae multi-layering of the
epithelium mitotic activity and nuclear atypia) without stromal invasion The absence of obvious stromal
invasion is the principal diagnostic criteria for BOT The degree of microinvasion lsquoacceptedrsquo however
depends on the individual pathologist with problematic inter- and intra-observer reproducibility
Incidence
Borderline ovarian tumours represent between 10 and 20 of all epithelial ovarian malignancies6
At the Norwegian Radium Hospital and other large institutions the reported prevalence is lower at
1278 probably re1047298ecting that women with BOT are treated at local hospitals Few population-based
studies on BOT are available Between 1970 and 1993 a total of 2343 women were diagnosed with BOTin Norway9 The age-adjusted incidence rate has increased since 1970 to 48 per 100000 persons per
year between 1995 and 2004 Nearly the same trend has been reported in Sweden 10
In a recent review of 6362 women with BOT by Trillsch et al11 789 of women had stage I disease
and few had abdominal spread whereas stage IV disease represented an exception These1047297gures are in
agreement with a large retrospective Norwegian study of 370 women with BOT treated at the
Norwegian Radium Hospital between 1970 and 19828 In the latter study 311 women (84) were
diagnosed with stage I disease 20 women (6) with stage II and 39 women (10) at stage III None had
stage IV disease Median age at diagnosis was 40 years (27 were younger than 40 years of age)
compared with about 60 years for women with invasive carcinoma1213 and the incidence rate
increased with age up to 45ndash49 years after which the rate stabilised Between 1970 and 1993 in
Norway 93 of women were diagnosed with localised tumours The proportion of tumours withdistant metastases increased from 27 between 1970 and 1973 to 66 between 1989 and 1993 9
Epidemiology
Besides age women with BOT do not seem to differ statistically from women with ovarian carci-
noma in epidemiologic characteristics Primary infertility and nulliparity increase the risk of BOT
whereas oral contraceptives pregnancies and breast feeding are protective factors14
Pathogenesis
Recently a new theory has been developed describing a subset of serous ovarian cystadenomas thatevolve through serous BOT to low-grade epithelial ovarian cancer15ndash18 (Fig 1) This lsquolow-gradersquo
pathway involves mutations in the B-raf and K-ras signalling pathway The pathway involves serous
BOT as a precursor mimicking the adenocarcinoma sequence in colorectal cancer in which carcinoma
evolves through a continuum of histological precursor lesions19ndash21 Only 2 of all serous BOT progress
to carcinoma via the lsquolow-gradersquo pathway17
This is in contrary to the lsquohigh-gradersquo pathway that involves frequent TP53 mutations and very
seldom B-raf and K-ras mutations Most serous ovarian carcinomas belong to the typical high-grade
pathway with no known precursor TP53 mutations are most often absent in typical serous BOT and
micropapillary serous BOT compared with 88 prevalence in invasive serous carcinomas22ndash24
The sequence of malignant transformation from benign mucinous tumours to carcinoma represents
transitional stages of mucinous carcinogenesis Three types of ras oncogenes exist (K N and H) andmucinous BOT have a higher frequency of K-ras mutation thanthatof mucinous cystadenoma but a lower
rate than that of mucinous carcinoma Foci suggesting in-situ malignant changes are often identi1047297ed in
mucinous BOT associated with invasion and the transition may be identi1047297ed microscopically in some
cases2425 It is for the moment unclear whether BRCA1 and BRCA2 mutations increase the risk of BOT12
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336326
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 312
Histology
Nearly all BOT are of the mucinous or serous type the remaining 4ndash5 are of endometrioid clear
cell mixed and transitional cell or Brenner type Serous BOT and mucinous BOT make up 43ndash53 and
425ndash
52 of all BOT respectively891126
Serous borderline tumours
Serous borderline tumours are bilateral in about one-third of cases811 Extra-ovarian spread as peri-
toneal implants is frequent (35) Most implants are non-invasive but invasive implants are found in 20ndash
25 of cases27 Bilaterality and non-invasive implants do not predict worse outcome compared with the
presence of invasive implants1127ndash30 Invasive implants may progress to invasive carcinoma whereas
most peritoneal implants will remain stable or regress after removal of the main ovarian tumour2931
Women with serous BOT without invasive implants have 10-year survival of 95 compared with 60ndash
70 for women with invasive implants12 Women with invasive implants develop progressive disease in
about 30 of cases whereas only about 2 of women without invasive implants will progress2432
Controversy exists about whether tumours with invasive implants are more likely to have micro-
papillary features within the primary BOT at diagnosis2829
Mucinous borderline tumours
Mucinous borderline tumours are histologically classi1047297ed as intestinal (85 of mucinous BOT) or
endocervical (15 of mucinous BOT) (former lsquoMuumlllerianrsquo)1130 The ovarian tumours of the intestinal
subtype can be large and are nearly always unilateral In case of bilaterality the woman should be
further examined for a primary intestinal tumour The endocervical subtype might be bilateral and
associated with endometriosis and mixed-BOT Both subtypes can present with intra-epithelial
carcinoma micro-invasion with less than 10 mm
28
Extraovarian spread is infrequent (10ndash
15) andnearly always as pseudomyxoma peritonei The condition may occur in any type of intra-abdominal
mucinous neoplasm but occurs most often in association with mucinous BOT33 Most of these repre-
sent dissemination from a mucinous appendix tumour An appendectomy should be carried out at
primary surgery for intestinal M-BOT All M-BOT might recur as invasive adenocarcinoma especially
Fig 1 Low-grade pathway frequent B-raf and K-ras mutations (61ndash68) lowcellular proliferation gradual 53 mutations (70) high
cellular proliferation high chromosomal instability frequent HLA-Gexpression 5-year survival about 30 APST atypical proliferative
serous tumours MPSC micropapillary serous carcinoma SBT serous borderline ovarian tumour Published with permission 17
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 327
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 412
when only ovarian cystectomy rather than salpingo-oophorectomy has been carried out This might be
explained by missing an invasive component owing to inadequate histopathologic evaluation of these
large tumours Therefore unilateral salpingo-oophorectomy is recommended in mucinous BOT1114
Prognostic factors
As BOT in general has an excellent survival it might be dif 1047297cult to identify variables that improve
survival As many women with BOT are of reproductive age at diagnosis more conservative treatment
preserving thechildbearingability is desirable International Federation of Gynecologyand Obstetrics stage
is thestrongest prognostic factor for recurrence andsurvival for BOT as well as for invasive ovariancancers
Micropapillary histology was reported as an additional risk factor for serous BOT but this issue is contro-
versial as poor prognosis is only seen if this histology is associated with invasive implants2834ndash36 Tumours
with evidence of stromal invasion of less than 10 mm2 behave clinically as BOT and are today classi1047297ed as
BOT222437ndash40 In the retrospective study from the Norwegian Radium Hospital41 370 BOT were treated
between 1970 and 1982 and the follow up was complete with a median follow-up time of 152 months
(range 6ndash354 months) By multivariate analysis the only three independent prognostic factors for disease-
free and long-term survival were FIGO stage (P lt 00001) histologic type (P lt 005) and age (P lt 0005) Inanother study of the same women including DNA ploidy the women could be divided into risk groups41
The low-risk group (100 disease-free survival) was characterised by stage I disease diploid serous BOTor
mucinous BOT and age less than 40 years The high-risk group (75 or higher risk of dying of disease) had
aneuploid serous BOT or mucinous BOT stage II-III disease and age older than 70 years Deoxyribonucleic
acid ploidy was the strongest prognostic factor in BOT in the study by Kaern et al41 but this has unfortu-
nately not been reproduced by others4243 Lymph-node involvement could not convincingly be con1047297rmed
to be an independent risk factor35414445
Symptoms
Limited information exists about symptom registration by women with BOT at diagnosis Mostwomen may be asymptomatic and a pelvic mass discovered at routine pelvic examination Symptoms
are less common compared with symptoms registered for women with invasive ovarian cancer
although 75 of women with BOT may have at lease one symptom as abdominal pain or discomfort
bowel irregularity and persisting fatigue or weight loss4647
Standard treatment
The diagnosis of BOT cannot be determined before surgery Intraoperative frozen section diagnosis
of BOT is often dif 1047297cult even for experienced pathologists Frozen sections may be useful for
discrimination between BOTand epithelial ovarian cancer and benign tumour (over-diagnosis less than
10) but not for discrimination between BOT and epithelial ovarian cancer (under-diagnosis in 25ndash
30of women)4849 Less than 50 of women with BOT will have a complete surgical staging this without
obvious in1047298uence on survival
The standard guidelines for primarysurgery in BOTaresimilar to these for invasive ovarian carcinomas
removal of all macroscopic disease and proper surgical staging hysterectomy with bilateral salpingo-
oophorectomy multiple peritoneal biopsies and peritoneal washing with cytology For mucinous BOT
appendectomy should also be carried out33 Lymph-node sampling has not been part of the standard
procedure A recently published German study reported systematic lymph-node dissection in 189 of
women with BOT11 Involvement of lymph nodes even with upstage do not in1047298uence recurrence or
survival rate850 Lymph-node involvement is rarely seen in M-BOT Lymphadenectomy can be omitted
even for stage II and III disease as there is no difference in the recurrence or survival rate (Fig 2)5051
Restaging procedures
Despite the fact that experts have recommended comprehensive surgical staging for many years most
women referred to university or comprehensive cancer centres after primary surgery have incomplete
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336328
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 512
surgery Another common event is that malignancy is not suspected at the initial operation and therefore
the abdomen is not properly explored Should this woman undergo re-operation Snider et al52 upstaged
1047297ve out of 27 women with stage I disease None of the 12 women with mucinous BOT were upstaged
whereas1047297veoutof 13 women with serous BOTwere upstagedMucinousBOTgrossly con1047297ned to one ovary
are probably unlikely to be upstaged at a restaging procedure If evidence of extra-ovarian disease exists
complete surgical staging and appendectomy are indicated Mucinous BOT with abdominal spread are in50 claimed to arise in the appendix or simultaneously in one or both ovaries5354 For serous BOT it is
reasonable to do a second operation as lymph-node involvement has been reported in about 20 in
apparentstage I tumourswitheven higher incidence in more advanced stages45 At the Norwegian Radium
Hospital we recommend restaging if the women are insuf 1047297ciently staged at primary operation in agree-
ment with Cadron et al51 and Trimble and Trimble55 We also believe that the decision to restage must be
individualised taking into consideration the adequacy of the previous abdominal exploration the tumour
subtype and potential treatment of residual disease as well as thelevel of concern for both thewomanand
the clinician even if there is little proof that restaging operations have an effect on survival115056ndash58
Laparoscopy
Laparoscopic treatment has become an attractive approach for benign ovarian tumours (pelvic
mass) The development of the laparoscopic techniques with the use of endo-bag gives less risk of
spillage during surgery and less port-side metastases For conservatively treated women wishing to
preserve fertility this is a more favourable approach and has short postoperative recovery fewer
adhesions and improved cosmetic results59 Cyst rupture and incomplete staging occur signi1047297cantly
more frequently by laparoscopy compared with laparotomy (339 v 124)6061 but do not in1047298uence
survival The laparoscopic treatment may result in higher recurrence rate which must be discussed
with the woman The woman should agree to close follow up and repeated surgery5162 Other concerns
are port metastases63 and improper staging61
Postoperative treatment of borderline ovarian tumours
Today there is no proven bene1047297t from adjuvant therapy (chemotherapy or radiotherapy) even in
advanced stage disease and in the presence of invasive implants1432 No randomised-controlled studies
Fig 2 Recommendation treatmentof borderline ovarian tumours Modi1047297ed fromTrillsch et al11 and Cadron et al51 with permission
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 329
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 612
have evaluated the ef 1047297cacy of chemotherapy in advanced stage BOT with residual disease Cisplatin-
based therapy in serous BOT with residual disease have shown high response rates but modest
effect on long-term survival1464 In case of recurrences where transformation to an invasive histology
has occurred consideration of platinum-taxane-based chemotherapy is reasonable The molecular
changes transforming BOT to invasive ovarian carcinoma may be clari1047297ed in the future with the
possibility of blocking the different lsquostepsrsquo in the carcinogenesis Today we know that both serous BOTand low-grade serous carcinoma frequently present with B-raf and K-ras mutations11
Survival
Overall survival for women with BOT is excellent 90ndash100 in most reports depending on age at
diagnosis FIGO stage and histologic type112651626566 Trillsch et al11 reported a 5-year overall survival
rate of almost 100 in early stage disease (FIGO I-II) and between 86 and 92 in more advanced
disease (FIGO III-IV) In a Norwegian population-based study67 the age-adjusted 1- 3- 5- and 10-year
relative survival rates of women with mucinous BOT were 98 97 97 and 95 respectively and for
women with serous BOT 96 93 90 and 90 respectively The relative risk of dying increased with
higher age at diagnosis The 5-year relative survival for women aged between 0 and 44 years was 99compared with 85 for women aged 75ndash89 years Nearly the same 1047297gures are reported by Sherman
et al12 with better survival for younger women and slightly better survival for serous tumours
compared with mucinous tumours although mucinous tumours in advanced stage had the poorest
long-term survival (855)12
Seidman and Kurman35 summarised 97 reports including a total of 4129 women with serous BOT
and showed a disease-speci1047297c survival rate of 99 for stage I disease and 953 for stage III disease
(mean follow up of 7 years)35 The 5-year survival was 98 for women with serous BOT with non-
invasive implants and 33 for those with invasive implants68
Conservative surgery
The median age of diagnosis for women with BOT is 40 years and nearly one-third are younger than
40 years Thus preservation of childbearing potential is an important issue for many of these women
To select women for fertility-sparing surgery without risk of reduced long-term survival is a challenge
for the gynaecologic oncologist3069 (Fig 2) Conservative surgery is de1047297ned as complete staging in
which the uterus and at least a part of one ovary are preserved1162 (Fig 2)
Although the standard treatment for all women with BOT is at least bilateral salpingo-
oophorectomy many young women with stage Ia tumours who have not completed childbearing
can be safely treated with unilateral salpingo-oophorectomy after comprehensive surgical staging
thereby preserving the fertility potential At least as important as the fertility issue however is
whether we can reduce the morbidity caused by radical surgery and whether a more conservative
approach is a safe alternative regarding cancer prognosis51
Recent studies from the Norwegian RadiumHospital8 and Gynecologic Oncology Group65 have shown that preservation of reproductive organs is
feasible Relapse rates after bilateral salpingo-oophorectomy range between 0 and 20 This rate
varies between 12 and 58 for cystectomy and between 25 and 57 for radical surgery Relapses
can also occur late and recurrences as late as 39 years after initial treatment have been reported5134
Predictors of relapse are resection margins containing tumour cells70 The frequency of persistence or
recurrence in 35 patients with serous-BOT treated by unilateral cystectomy bilateral cystectomy or
unilateral cystectomy with contralateral oophorectomy or salpingo-oophorectomy was retrospectively
investigated by Lim-Tan et al71 Conservative surgical treatment was carried out either because the
women were young and wanted to preserve their fertility or because the nature of the tumour was not
determined at the time of surgery Thirty-three women had stage I disease (19 stage Ia 10 stage Ib and
four stage Ic) and two had stage III disease Although 60 of the women had additional and in somecases de1047297nitive operations within relative short periods after initial cystectomy or cystectomies 21 had
conservation of ovarian tissue and were followed on average for 75 years All women with stage I
disease were alive without evidence of disease after surgical treatment alone The presence of
persistent or recurrent disease correlated with multifocality and involvement of resection margins
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336330
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 712
Multifocality may be a strong predictor of failure of cystectomy to control the disease No recurrence of
disease was seen in ovaries from which a single cyst had been removed with negative resection
margins Extensive sampling of the resection margins of ovarian cysts is important71
For many women with BOT fertility is an important issue It is therefore essential to discuss with
these young women the advantages and disadvantages between conservative and radical surgery
Conservative surgery preserves fertility and hormonal function but unfortunately with high risk of recurrence
In women with obvious stage I disease unilateral salpingo-oophorectomy or cystectomy has from
previous studies been shown to be safe This has also been con1047297rmed for women with advanced-stage
disease on the assumption of close follow up
Even for women with advanced disease conservative surgery might be considered after informed
consent The recurrence rate is high and invasive and even non-invasive implants may recur up to 15
as invasive OC without negative in1047298uence on survival34567273
Treatment at recurrent disease after conservative treatment
Early detected recurrences are curable with repeated surgery113451 and therefore conservativetreatment might again be considered in women with recurrent disease if fertility still is an issue and the
woman is informed about the high risk of recurrence and agrees on close follow up accepting repeated
surgery5162 If invasive implants are diagnosed this procedure could not be recommended In any case
of recurrent disease secondary debulking surgery is important as women suboptimally debulked have
poor survival115174
Fertility after conservative management of borderline ovarian tumour
Infertility is frequently observed inwomen with BOT A history of infertility beforediagnosis has been
reported in 10ndash35 of women75ndash77 To allow conservative surgery careful evaluation of the extent of
disease by the gynaecologist at the time of operation and meticulous examination of the cystectomyspecimen by the gynaecologist and pathologist are desirable to determine the prognosis after cys-
tectomy In a study by Morris et al76 onewoman who had disease-related deathwasnot staged properly
In a meta-analysis by Maltaris et al78 1483 women had BOT of whom 656 were treated conservatively
(442) A total of 196 women became pregnant and 111 relapsed after unilateral salpingo-
oophorectomy only one woman died from the disease (015) The investigators therefore suggest
that conservative surgery is justi1047297able for some women with a good prognostic index Unilateral
oophorectomy omentectomy and appendectomy in stage Ia diploid mucinous BOT are indicated for
young women who wish to preservefertility (Fig 2) In stage Ia diploid serous BOT thesame procedure is
safe if the contralateral ovary is macroscopically normal Careful inspection of a macroscopically normal
contralateral ovary should be suf 1047297cient inyoung womenwith stageIa disease who wish to remainfertile
Surgery itself can impair the fertility function by loss of ovarian tissue pelvic scarring and adhesionsblocking the fallopian tube Post-surgery fertility factors such as ovulation fallopian tubes and sperm
factors should be investigated and treated if necessary About one-third of women undergoing
conservative surgery for BOT will be able to conceive with no negative in1047298uence of pregnancy on the
disease60727779 Ovulation induction is often required in order to conceive80 The role of ovulation
(in-vitro [IVF] fertilisation) drugs in BOT is currently under debate7780ndash84
Recently a large nationwide cohort study of 19146 subfertile women in the Netherlands who
received IVF drugs between 1983 and 1995 and a comparison group of 6953 subfertile women who
were not treated was published After a median follow up of 15 years a total of 77 ovarian malignancies
were observed in the cohort including 42 women with epithelial ovarian cancer and 35 women with
BOT Sixty-one ovarian malignancies were observed in the IVF-group and 16 in the unexposed (control)
group The ratio hazard for epithelial ovarian cancer and BOT was 167 (074 to 375) and 425 (127 to1418) respectively85 The conclusion of Burger et al85 was that IVF increases the risk of BOT
A worrying1047297nding of their study is the increased risk of epithelial ovarian cancer and BOT even after 15
years of follow up Fasouliotis et al80 found no perceptible negative effect of previous BOT on preg-
nancy rates after IVF The same was shown by Fortin et al84 in a study of 30 women treated with IVF
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 331
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 812
drugs for infertility after conservative surgery Thirteen pregnancies were observed Disease in four
women recurred All recurrences were BOT on a remaining ovary that had been treated by surgery
alone All women are currently disease-free after secondary surgery Fortin et al84 concluded that IVF
drugs can be used safely in womenwho develop infertility after conservative treatment of BOT Because
of the low number of women treated with IVF drugs Norwegian Radium Hospital guidelines are to
proceed with caution and only women with early stage BOT are permitted to be treated with IVF drugsThe latest development regarding reproduction and BOT is cryopreservation 86 Women who have
their ovaries removed because of large stage Ib BOT now have a possibility of becoming pregnant
Biopsies from normal ovarian cortex can be taken during the primary operation In 2004 a live birth
after a fresh ovarian tissue transplant in a primate was reported87 Donnez et al86 described in 2004
a live birth after orthotopic auto-transplantation of cryopreserved ovarian tissue Their1047297ndings opened
new possibilities for young women facing premature ovarian failure
Women with reduced fertility after surgery can consider ovarian stimulation egg retrieval and egg
freezing Ovarian stimulation and exposure to high oestrogen exposure do not seem to increase the risk
for recurrence Nor do pregnancies have negative in1047298uence on survival7277
To assure future fertility preservation in women with BOT the gynaecologic oncologist should
collaborate closely with the reproductive endocrinologists even before surgery Until more mature dataexist the general recommendation is a limited number of stimulation cycles only for stage I patients In
case of bilateral salpingo-oophorectomy cryopreservation of ovarian cortex biopsy from the less
affected ovary could be considered although this is not always technically possible1151
Follow up
Follow up should be long term and lifelong because recurrences may develop after more than 15 years
In conservatively treated womenclose follow up is crucial with special attentionto theremainingovaryIt
is still debated if the remaining ovary (and uterus) should be removed after the family is completed For
low-risk BOT there is no indication for this procedure but in women with high-risk of recurrence the
procedure is optional the alternative being to wait until recurrence or carry out radical surgery Manywomen will choose radical surgery when the family is completed because of psychological stress
The general recommendation is follow up every 3 months during the 1047297rst 2 years and then every 6
months for the next 3 years and annually thereafter The women is followed with pelvic examination
transvaginal ultrasound and calcium 125 measurement1451 (Fig 2)
Future direction of borderline ovarian tumour
A key issue for future research on BOTconcerning epidemiology is the identi1047297cation of risk factors for
invasive implants recurrences and death and also the identi1047297cation of predisposing heritable factors
For clinical management improved methods for preoperative and intraoperative diagnosis should
be considered in addition to the role of laparoscopic surgery in removal of complex cysts improvedmethods for distinguishing metastases from BOT and determination of risk associated with conser-
vative treatment
For pathology and molecular biology molecular studies are needed to assess the relationship
between serous BOT low-grade serous carcinoma and high-grade serous carcinoma Molecular studies
are also needed to aid in the characterisation of implants and studies need to be conducted to
determine the biology of microinvasive BOT and the clinical signi1047297cance of long-term follow up
Conclusion
Borderline ovarian tumours are ovarian tumours with good prognosis that account for 10ndash20 of all
epithelial ovarian cancer Historically standard primarysurgeryincludedbilateral salpingo-oophorectomyomentectomy peritoneal washing and complete peritoneal resection of macroscopic lesions or multiple
biopsies In cases of M-BOT women are also treated with appendectomy As one-third of BOT are diagnosed
inwomenyounger than40 years however fertility-sparingtreatment (ie preservation of the uterus andat
least part of one ovary) has been increasingly used in the past 10 years Fertility drugs are well tolerated in
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336332
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 912
women with infertility after fertility-sparing surgery Careful selection of candidates is necessary Lapa-
roscopic techniques can be used but are reserved for oncologic surgeons This conservative treatment
increases therateof recurrencebutwithoutany effecton survivalThespontaneouspregnancy rate is nearly
50and most are achieved spontaneously Spontaneous pregnancy can occurafter conservative treatment
of advanced-stage BOT (with non-invasive implants) These women should be closely followed up Further
research has to concentrate on clinical risk-factors histopathological markers and pathogenesis to guar-antee the best clinical management for women with BOT
Con1047298ict of interest statement
None declared
Practice points
BOTare ovarian tumours with good prognosis that account for 10ndash20 of all epithelial ovarian
cancer Historically standard primary surgery included bilateral salpingo-oophorectomy omentec-
tomy peritoneal washing and complete peritoneal resection of macroscopic lesions or
multiple biopsies
In case of mucinous BOT women are also treated with appendectomy
Adjuvant therapy for the treatment of BOT has no proven bene1047297t
As one-third of BOT are diagnosed in women younger than 40 years fertility-sparing treat-
ment (ie preservation of the uterus and at least part of one ovary) has been increasingly used
in the past 10 years
Fertility drugs are well tolerated in women with infertility after fertility-sparing surgery
Careful selection of candidates is necessary
Laparoscopic techniques can be used but are reserved for oncologic surgeons Spontaneous pregnancy can occur after conservative treatment of advanced stage BOT (with
non-invasive implants)
These women should be closely followed up
Research agenda
Epidemiology
Identify risk factors for invasive implants recurrences and death
Identify predisposing heritable factors
Clinical management
Improve methods for preoperative and intraoperative diagnosis
Further explore the role of laparoscopic surgery in the removal of complex cysts
Improve methods for distinguishing metastases from BOTand determine risk associated with
conservative treatment
Pathology and molecular biology
Conduct molecular studies to assess the relationship between serous BOT low-grade serous
carcinoma and high-grade serous carcinoma Conduct molecular studies to aid in the characterisation of implants
Conduct studies to determine the biology of microinvasive BOTand the clinical signi1047297cance of
long-term follow up
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 333
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1012
Acknowledgement
We wish to thank Mrs Gry Seppola for technical assistance and gratefully acknowledge the1047297nancial
support from the Inger and John Fredriksen Foundation for Ovarian Cancer Research
References
1 Taylor HC Malignant and semi-malignant tumors of the ovary Surg Gynecol Obstet 1929 48 204ndash2302 Kottmeier HL Kolstad P McGarrity KA Annual report on results of treatment in gynaecologic cancer vol 17 Statements of
results obtained in 1969ndash1972 inclusive FIGO Stockholm Sweden Editorial of 1047297ce Radiumhemmet 19733 Serov SF Scully RE amp Sobin LH International histological classi 1047297cation of tumors no 9 Histoloigcal typing of ovarian tumours
Geneval World Health Organization 19734 Hart WR amp Norris HJ Borderline and malignant mucinous tumors of the ovary Histologic criteria and clinical behavior
Cancer 1973 31 1031ndash10455 Scully RE Tumors of the ovary and maldeveloped gonads Fascicle 16 In Atlas of tumor pathology Second series Wash-
ington DC Armed Forces Institute of Pathology 1979 pp 75ndash906 Lenhard MS Mitterer S Kuumlmper C et al Long-term follow-up after ovarian borderline tumor relapse and survival in
a large patient cohort Eur J Obstet Gynecol Reprod Biol 2009 145 189ndash194
7 Quirk JT amp Natarajan N Ovarian cancer incidence in the United States 1992ndash
1999 Gynecol Oncol 2005 97 519ndash
5238 Kaern J Tropeacute CG amp Abeler VM A retrospective study of 370 borderline tumors of the ovary treated at the NorwegianRadium Hospital from 1970 to 1982 A review of clinicopathologic features and treatment modalities Cancer 1993 711810ndash1820
9 Bjoslashrge T Engeland A Hansen S et al Trends in the incidence of ovarian cancer and borderline tumours in Norway1954ndash1993 Int J Cancer 1997 71 780ndash786
10 Skiacuternisdoacutettir I Garmo H Wilander E et al Borderline ovarian tumors in Sweden 1960ndash2005 trends in incidence and age atdiagnosis compared to ovarian cancer Int J Cancer 2008 123 1897ndash1901
11 Trillsch F Mahner S Ruetzel J et al Clinical management of borderline ovarian tumors Expert Rev Anticancer Ther 2010 101115ndash1124
12 Sherman ME Mink PJ Curtis R et al Survival among women with borderline ovarian tumors and ovarian carcinomaa population-based analysis Cancer 2004 100 1045ndash1052
13 Kramer JL Greene MH Epidemiology of ovarian fallopian tube and primary peritoneal cancer In Gershenson DMMcGuire WP Gore M et al eds Gynecologic cancer Controversies in management 1st ed Philadelphia Elsevier ChurchillLivingstone 2004 pp 327ndash340
14 Tropeacute C Davidson B Paulsen T et al Diagnosis and treatment of borderline ovarian neoplasms lsquothe state of the artrsquo Eur J Gynaecol Oncol 2009 30 471ndash482
15 Kurman RJ amp Shih IeM Pathogenesis of ovarian cancer lessons from morphology and molecular biology and their clinicalimplications Int J Gynecol Pathol 2008 27 151ndash160
16 Kurman RJ Visvanathan K Roden R et al Early detection and treatment of ovarian cancer shifting from early stage tominimal volume of disease based on a new model of carcinogenesis Am J Obstet Gynecol 2008 198 351ndash356
17 Shih IeM amp Kurman RJ Ovarian tumorigenesis a proposed model based on morphological and molecular genetic analysis Am J Pathol 2004 164 1511ndash1518
18 Levanon K Crum C amp Drapkin R New insights into the pathogenesis of serous ovarian cancer and its clinical impact J ClinOncol 2008 26 5284ndash5293
19 Meinhold-Heerlein I Bauerschlag D Hilpert F et al Molecular and prognostic distinction between serous ovarian carci-nomas of varying grade and malignant potential Oncogene 2005 24 1053ndash1065
20 Bonome T Lee JY Park DC et al Expression pro1047297ling of serous low malignant potential low-grade and high-grade tumorsof the ovary Cancer Res 2005 65 10602ndash10612
21 Mahner S Baasch C Schwarz J et al C-Fos expression is a molecular predictor of progression and survival in epithelialovarian carcinoma Br J Cancer 2008 99 1269ndash1275
22 Ortiz BH Ailawadi M Colitti C et al Second primary or recurrence Comparative patterns of p53 and K-ras mutationssuggest that serous borderline ovarian tumors and subsequent serous carcinomas are unrelated tumors Cancer Res 200161 7264ndash7267
23 Lee KR Tavassoli FA Prat J et al Tumours of the ovary and peritoneum In Tavassoli FA amp Devilee P (eds) Pathology and
genetics Tumours of the breast and female genital organs Lyon IARC Press 2003 pp 113ndash20224 Oedegaard E Ovarian carcinomas and borderline ovarian tumors - molecular markers and operative treatment Dissertation
Facutly of Medicine University of Oslo 200825 Mok SC Bell DA Knapp RC et al Mutation of K-ras protooncogene in human ovarian epithelial tumors of borderline
malignancy Cancer Res 1993 53 1489ndash149226 du Bois A Ewald-Riegler N du Bois O et al Borderline tumors of the ovary a systematic review [German] Geburtsh
Frauenheilk 2009 69 807ndash83327 Seidman JD Horkayne-Szakaly I Haiba M et al The histologic type and stage distribution of ovarian carcinomas of surface
epithelial origin Int J Gynecol Pathol 2004 23 41ndash44
28 Prat J amp De Nictolis M Serous borderline tumors of the ovary a long-term follow-up study of 137 cases including 18 witha micropapillary pattern and 20 with microinvasion Am J Surg Pathol 2002 26 1111ndash1128
29 Bell DA Weinstock MA amp Scully RE Peritoneal implants of ovarian serous borderline tumors Histologic features andprognosis Cancer 1988 62 2212ndash2222
30 Tinelli R Tinelli A Tinelli FG et al Conservative surgery for borderline ovarian tumors a review Gynecol Oncol 2006 100
185ndash191
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336334
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1112
31 Kurman RJ amp Trimble CL The behavior of serous tumors of low malignant potential are they ever malignant Int J Gynecol
Pathol 1993 12 120ndash12732 Morice P Camatte S Rey A et al Prognostic factors for patients with advanced stage serous borderline tumours of the
ovary Ann Oncol 2003 14 592ndash59833 Bradley RF Stewart 4th JH Russell GB et al Pseudomyxoma peritonei of appendiceal origin a clinicopathologic analysis of
101 patients uniformly treated at a single institution with literature review Am J Surg Pathol 2006 30 551ndash559
34 Silva EG Gershenson DM Malpica A et al The recurrence and the overall survival rates of ovarian serous borderlineneoplasms with noninvasive implants is time dependent Am J Surg Pathol 2006 30 1367ndash137135 Seidman JD amp Kurman RJ Ovarian serous borderline tumors a critical review of the literature with emphasis on prognostic
indicators Hum Pathol 2000 31 539ndash55736 Chang SJ Ryu HS Chang KH et al Prognostic signi1047297cance of the micropapillary pattern in patients with serous borderline
ovarian tumors Acta Obstet Gynecol Scand 2008 87 476ndash48137 Fox H amp Wells M Surface epithelialstromal tumors of the ovary In Fox H amp Wells M (eds) Haines and Taylor Obstetrical and
Gynaecological Pathology 5th ed London Churchill Livingstone 2003 pp 713ndash74338 Ren J Peng Z amp Yang K A clinicopathologic multivariate analysis affecting recurrence of borderline ovarian tumors Gynecol
Oncol 2008 110 162ndash16739 Longacre TA McKenney JK Tazelaar HD et al Ovarian serous tumors of low malignant potential (borderline tumors)
outcome-based study of 276 patients with long-term (gt or frac145-year) follow-up Am J Surg Pathol 2005 29 707ndash72340 Cusidoacute M Balagueroacute L Hernandez G et al Results of the national survey of borderline ovarian tumors in Spain Gynecol
Oncol 2007 104 617ndash62241 Kaern J Tropeacute CG Kristensen GB et al DNA ploidy the most important prognostic factor in patients with borderline
tumors of the ovary Int J Gynecol Cancer 1993 3 349ndash35842 Meyer JS Gersell DJ amp Yim S Cell proliferation in ovarian carcinoma superior accuracy of S-phase fraction (SPF) by DNA
labeling index versus 1047298ow cytometric SPF lack of independent prognostic power for SPF and DNA ploidy and limitedeffect of SPF on tumor growth rate Gynecol Oncol 2001 81 466ndash476
43 Verbruggen MB van Diest PJ Baak JP et al The prognostic and clinical value of morphometry and DNA cytometry inborderline ovarian tumors a prospective study Int J Gynecol Pathol 2009 28 35ndash40
44 Yokoyama Y Moriya T Takano T et al Clinical outcome and risk factors for recurrence in borderline ovarian tumours Br J Cancer 2006 94 1586ndash1591
45 Leake JF Rader JS Woodruff JD et al Retroperitoneal lymphatic involvement with epithelial ovarian tumors of lowmalignant potential Gynecol Oncol 1991 42 124ndash130
46 Paulsen T Kaern J Kjaerheim K et al Symptoms and referral of women with epithelial ovarian tumors Int J Gynaecol Obstet 2005 88 31ndash37
47 Paulsen T Epithelial ovarian cancer A clinical epidemiological approach on diagnosis and treatment Dissertation Faculty of Medicine University of Oslo 2007
48 Tropeacute CG Kristensen G amp Makar A Surgery for borderline tumor of the ovary Semin Surg Oncol 2000 19 69ndash7549 Tempfer CB Polterauer S Bentz EK et al Accuracy of intraoperative frozen section analysis in borderline tumors of the
ovary a retrospective analysis of 96 cases and review of the literature Gynecol Oncol 2007 107 248ndash25250 Camatte S Morice P Thoury A et al Impact of surgical staging in patients with macroscopic lsquostage Irsquo ovarian borderline
tumours analysis of a continuous series of 101 cases Eur J Cancer 2004 40 1842ndash184951 Cadron I Leunen K Van Gorp T et al Management of borderline ovarian neoplasms J Clin Oncol 2007 25 2928ndash293752 Snider DD Stuart GC Nation JG et al Evaluation of surgical staging in stage I low malignant potential ovarian tumors
Gynecol Oncol 1991 40 129ndash13253 Ronnett BM Kurman RJ Zahn CM et al Pseudomyxoma peritonei in women a clinicopathologic analysis of 30 cases with
emphasis on site of origin prognosis and relationship to ovarian mucinous tumors of low malignant potential Hum Pathol
1995 26 509ndash52454 Seidman JD Elsayed AM Sobin LH et al Association of mucinous tumors of the ovary and appendix A clinicopathologic
study of 25 cases Am J Surg Pathol 1993 17 22ndash3455 Trimble EL amp Trimble LC Epithelial ovarian tumors of low malignant potential In Markman M amp Hoskins W (eds) Cancer
of the Ovary New York Raven Press 1993 pp 415ndash429
56 Zanetta G Rota S Chiari S et al Behavior of borderline tumors with particular interest to persistence recurrence andprogression to invasive carcinoma a prospective study J Clin Oncol 2001 19 2658ndash266457 Fauvet R Boccara J Dufournet C et al Restaging surgery for women with borderline ovarian tumors results of a French
multicenter study Cancer 2004 100 1145ndash115158 Zapardiel I Rosenberg P Peiretti M et al The role of restaging borderline ovarian tumors single institution experience and
review of the literature Gynecol Oncol 2010 119 274ndash27759 Def 1047297eux X Morice P Camatte S et al Results after laparoscopic management of serous borderline tumor of the ovary with
peritoneal implants Gynecol Oncol 2005 97 84ndash8960 Fauvet R Boccara J Dufournet C et al Laparoscopic management of borderline ovarian tumors results of a French
multicenter study Ann Oncol 2005 16 403ndash41061 Vandenput I Amant F amp Vergote I Peritoneal recurrences might be less common in advanced stage serous borderline
ovarian tumors that were treated by laparotomy Gynecol Oncol 2005 98 52362 CadronI Amant F VanGorp Tet alThe management of borderline tumours of theovary Curr Opin Oncol 2006 18 488ndash49363 Vergote I De Brabanter J Fyles A et al Prognostic importance of degree of differentiation and cyst rupture in stage I
invasive epithelial ovarian carcinoma Lancet 2001 357 176ndash182
64 Gershenson DM amp Silva EG Serous ovarian tumors of low malignant potential with peritoneal implants Cancer 1990 65578ndash585
65 Gershenson DM Clinical management potential tumours of low malignancy Best Pract Res Clin Obstet Gynaecol 2002 16513ndash527
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 335
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1212
66 Heintz AP Odicino F Maisonneuve P et al Carcinoma of the ovary FIGO 26th Annual Report on the Results of Treatment inGynecological Cancer Int J Gynaecol Obstet 2006 95(Suppl 1) S161ndashS192
67 Bjoslashrge T Engeland A Hansen S et al Prognosis of patients with ovarian cancer and borderline tumours diagnosed inNorway between 1954 and 1993 Int J Cancer 1998 75 663ndash670
68 Seidman JD amp Kurman RJ Subclassi1047297cation of serous borderline tumors of the ovary into benign and malignant typesA clinicopathologic study of 65 advanced stage cases Am J Surg Pathol 1996 20 1331ndash1345
69 Sherman ME Berman J Birrer MJ et al Current challenges and opportunities for research on borderline ovarian tumorsHum Pathol 2004 35 961ndash97070 Leake JF Currie JL Rosenshein NB et al Long-term follow-up of serous ovarian tumors of low malignant potential Gynecol
Oncol 1992 47 150ndash15871 Lim-Tan SK Cajigas HE amp Scully RE Ovarian cystectomy for serous borderline tumors a follow-up study of 35 cases Obstet
Gynecol 1988 72 775ndash78172 Morice P Camatte S El Hassan J et al Clinical outcomes and fertility after conservative treatment of ovarian borderline
tumors Fertil Steril 2001 75 92ndash9673 Camatte S Morice P Pautier P et al Fertility results after conservative treatment of advanced stage serous borderline
tumour of the ovary BJOG 2002 109 376ndash38074 Crispens MA Bodurka D Deavers M et al Response and survival in patients with progressive or recurrent serous ovarian
tumors of low malignant potential Obstet Gynecol 2002 99 3ndash1075 Fauvet R Poncelet C Boccara J et al Fertility after conservative treatment for borderline ovarian tumors a French
multicenter study Fertil Steril 2005 83 284ndash29076 Morris RT Gershenson DM Silva EG et al Outcome and reproductive function after conservative surgery for borderline
ovarian tumors Obstet Gynecol 2000 95 541ndash54777 Gotlieb WH Flikker S Davidson B et al Borderline tumors of the ovary fertility treatment conservative management and
pregnancy outcome Cancer 1998 82 141ndash14678 Maltaris T Boehm D Dittrich R et al Reproduction beyond cancer a message of hope for young women Gynecol Oncol
2006 103 1109ndash112179 Beiner ME Gotlieb WH Davidson B et al Infertility treatment after conservative management of borderline ovarian
tumors Cancer 2001 92 320ndash32580 Fasouliotis SJ Davis O Schattman G et al Safety and ef 1047297cacy of infertility treatment after conservative management of
borderline ovarian tumors a preliminary report Fertil Steril 2004 82 568ndash57281 Kashyap S amp Davis OK Ovarian cancer and fertility medications a critical appraisal Semin Reprod Med 2003 21 65ndash7182 Morice P Camatte S Wicart-Poque F et al Results of conservative management of epithelial malignant and borderline
ovarian tumours Hum Reprod Update 2003 9 185ndash19283 Whittemore AS Harris R amp Itnyre J Characteristics relating to ovarian cancer risk collaborative analysis of 12 US case-
control studies II Invasive epithelial ovarian cancers in white women Collaborative Ovarian Cancer Group Am J Epi-demiol 1992 136 1184ndash1203
84 Fortin A Morice P Thoury A et al Impact of infertility drugs after treatment of borderline ovarian tumors results of a retrospective multicenter study Fertil Steril 2007 87 591ndash596
85 Burger CW van de Swaluw A Mooij TM et al Risk of borderline and invasive ovarian tumors after ovarian stimulation forin vitro fertilization in a large Dutch cohort after 15 years of follow-up Abstracts presented for the 40th Annual Meeting of the Society of Gynecologic Oncologists February 2009 (abstract no 6) Gynecol Oncol 2009 112(Suppl) S4
86 Donnez J Dolmans MM Demylle D et al Livebirth after orthotopic transplantation of cryopreserved ovarian tissue Lancet 2004 364 1405ndash1410
87 Lee DM Yeoman RR Battaglia DE et al Live birth after ovarian tissue transplant Nature 2004 428 137ndash138
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336336
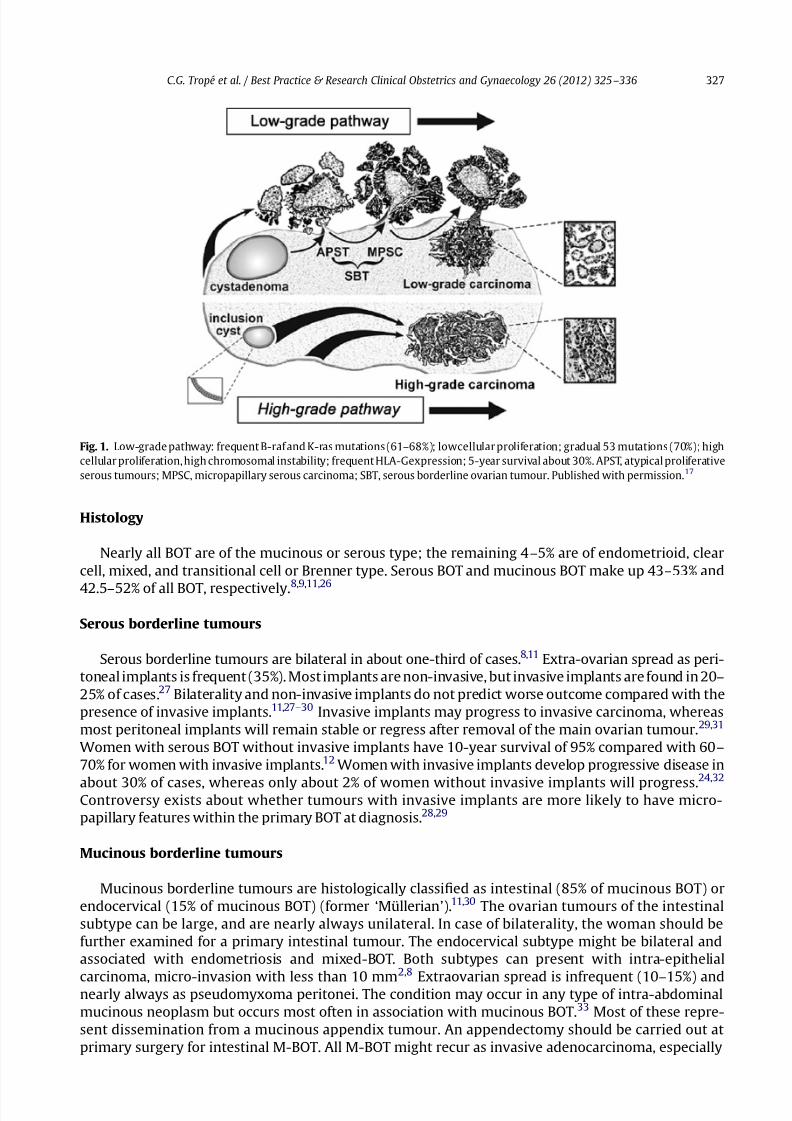
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 312
Histology
Nearly all BOT are of the mucinous or serous type the remaining 4ndash5 are of endometrioid clear
cell mixed and transitional cell or Brenner type Serous BOT and mucinous BOT make up 43ndash53 and
425ndash
52 of all BOT respectively891126
Serous borderline tumours
Serous borderline tumours are bilateral in about one-third of cases811 Extra-ovarian spread as peri-
toneal implants is frequent (35) Most implants are non-invasive but invasive implants are found in 20ndash
25 of cases27 Bilaterality and non-invasive implants do not predict worse outcome compared with the
presence of invasive implants1127ndash30 Invasive implants may progress to invasive carcinoma whereas
most peritoneal implants will remain stable or regress after removal of the main ovarian tumour2931
Women with serous BOT without invasive implants have 10-year survival of 95 compared with 60ndash
70 for women with invasive implants12 Women with invasive implants develop progressive disease in
about 30 of cases whereas only about 2 of women without invasive implants will progress2432
Controversy exists about whether tumours with invasive implants are more likely to have micro-
papillary features within the primary BOT at diagnosis2829
Mucinous borderline tumours
Mucinous borderline tumours are histologically classi1047297ed as intestinal (85 of mucinous BOT) or
endocervical (15 of mucinous BOT) (former lsquoMuumlllerianrsquo)1130 The ovarian tumours of the intestinal
subtype can be large and are nearly always unilateral In case of bilaterality the woman should be
further examined for a primary intestinal tumour The endocervical subtype might be bilateral and
associated with endometriosis and mixed-BOT Both subtypes can present with intra-epithelial
carcinoma micro-invasion with less than 10 mm
28
Extraovarian spread is infrequent (10ndash
15) andnearly always as pseudomyxoma peritonei The condition may occur in any type of intra-abdominal
mucinous neoplasm but occurs most often in association with mucinous BOT33 Most of these repre-
sent dissemination from a mucinous appendix tumour An appendectomy should be carried out at
primary surgery for intestinal M-BOT All M-BOT might recur as invasive adenocarcinoma especially
Fig 1 Low-grade pathway frequent B-raf and K-ras mutations (61ndash68) lowcellular proliferation gradual 53 mutations (70) high
cellular proliferation high chromosomal instability frequent HLA-Gexpression 5-year survival about 30 APST atypical proliferative
serous tumours MPSC micropapillary serous carcinoma SBT serous borderline ovarian tumour Published with permission 17
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 327
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 412
when only ovarian cystectomy rather than salpingo-oophorectomy has been carried out This might be
explained by missing an invasive component owing to inadequate histopathologic evaluation of these
large tumours Therefore unilateral salpingo-oophorectomy is recommended in mucinous BOT1114
Prognostic factors
As BOT in general has an excellent survival it might be dif 1047297cult to identify variables that improve
survival As many women with BOT are of reproductive age at diagnosis more conservative treatment
preserving thechildbearingability is desirable International Federation of Gynecologyand Obstetrics stage
is thestrongest prognostic factor for recurrence andsurvival for BOT as well as for invasive ovariancancers
Micropapillary histology was reported as an additional risk factor for serous BOT but this issue is contro-
versial as poor prognosis is only seen if this histology is associated with invasive implants2834ndash36 Tumours
with evidence of stromal invasion of less than 10 mm2 behave clinically as BOT and are today classi1047297ed as
BOT222437ndash40 In the retrospective study from the Norwegian Radium Hospital41 370 BOT were treated
between 1970 and 1982 and the follow up was complete with a median follow-up time of 152 months
(range 6ndash354 months) By multivariate analysis the only three independent prognostic factors for disease-
free and long-term survival were FIGO stage (P lt 00001) histologic type (P lt 005) and age (P lt 0005) Inanother study of the same women including DNA ploidy the women could be divided into risk groups41
The low-risk group (100 disease-free survival) was characterised by stage I disease diploid serous BOTor
mucinous BOT and age less than 40 years The high-risk group (75 or higher risk of dying of disease) had
aneuploid serous BOT or mucinous BOT stage II-III disease and age older than 70 years Deoxyribonucleic
acid ploidy was the strongest prognostic factor in BOT in the study by Kaern et al41 but this has unfortu-
nately not been reproduced by others4243 Lymph-node involvement could not convincingly be con1047297rmed
to be an independent risk factor35414445
Symptoms
Limited information exists about symptom registration by women with BOT at diagnosis Mostwomen may be asymptomatic and a pelvic mass discovered at routine pelvic examination Symptoms
are less common compared with symptoms registered for women with invasive ovarian cancer
although 75 of women with BOT may have at lease one symptom as abdominal pain or discomfort
bowel irregularity and persisting fatigue or weight loss4647
Standard treatment
The diagnosis of BOT cannot be determined before surgery Intraoperative frozen section diagnosis
of BOT is often dif 1047297cult even for experienced pathologists Frozen sections may be useful for
discrimination between BOTand epithelial ovarian cancer and benign tumour (over-diagnosis less than
10) but not for discrimination between BOT and epithelial ovarian cancer (under-diagnosis in 25ndash
30of women)4849 Less than 50 of women with BOT will have a complete surgical staging this without
obvious in1047298uence on survival
The standard guidelines for primarysurgery in BOTaresimilar to these for invasive ovarian carcinomas
removal of all macroscopic disease and proper surgical staging hysterectomy with bilateral salpingo-
oophorectomy multiple peritoneal biopsies and peritoneal washing with cytology For mucinous BOT
appendectomy should also be carried out33 Lymph-node sampling has not been part of the standard
procedure A recently published German study reported systematic lymph-node dissection in 189 of
women with BOT11 Involvement of lymph nodes even with upstage do not in1047298uence recurrence or
survival rate850 Lymph-node involvement is rarely seen in M-BOT Lymphadenectomy can be omitted
even for stage II and III disease as there is no difference in the recurrence or survival rate (Fig 2)5051
Restaging procedures
Despite the fact that experts have recommended comprehensive surgical staging for many years most
women referred to university or comprehensive cancer centres after primary surgery have incomplete
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336328
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 512
surgery Another common event is that malignancy is not suspected at the initial operation and therefore
the abdomen is not properly explored Should this woman undergo re-operation Snider et al52 upstaged
1047297ve out of 27 women with stage I disease None of the 12 women with mucinous BOT were upstaged
whereas1047297veoutof 13 women with serous BOTwere upstagedMucinousBOTgrossly con1047297ned to one ovary
are probably unlikely to be upstaged at a restaging procedure If evidence of extra-ovarian disease exists
complete surgical staging and appendectomy are indicated Mucinous BOT with abdominal spread are in50 claimed to arise in the appendix or simultaneously in one or both ovaries5354 For serous BOT it is
reasonable to do a second operation as lymph-node involvement has been reported in about 20 in
apparentstage I tumourswitheven higher incidence in more advanced stages45 At the Norwegian Radium
Hospital we recommend restaging if the women are insuf 1047297ciently staged at primary operation in agree-
ment with Cadron et al51 and Trimble and Trimble55 We also believe that the decision to restage must be
individualised taking into consideration the adequacy of the previous abdominal exploration the tumour
subtype and potential treatment of residual disease as well as thelevel of concern for both thewomanand
the clinician even if there is little proof that restaging operations have an effect on survival115056ndash58
Laparoscopy
Laparoscopic treatment has become an attractive approach for benign ovarian tumours (pelvic
mass) The development of the laparoscopic techniques with the use of endo-bag gives less risk of
spillage during surgery and less port-side metastases For conservatively treated women wishing to
preserve fertility this is a more favourable approach and has short postoperative recovery fewer
adhesions and improved cosmetic results59 Cyst rupture and incomplete staging occur signi1047297cantly
more frequently by laparoscopy compared with laparotomy (339 v 124)6061 but do not in1047298uence
survival The laparoscopic treatment may result in higher recurrence rate which must be discussed
with the woman The woman should agree to close follow up and repeated surgery5162 Other concerns
are port metastases63 and improper staging61
Postoperative treatment of borderline ovarian tumours
Today there is no proven bene1047297t from adjuvant therapy (chemotherapy or radiotherapy) even in
advanced stage disease and in the presence of invasive implants1432 No randomised-controlled studies
Fig 2 Recommendation treatmentof borderline ovarian tumours Modi1047297ed fromTrillsch et al11 and Cadron et al51 with permission
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 329
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 612
have evaluated the ef 1047297cacy of chemotherapy in advanced stage BOT with residual disease Cisplatin-
based therapy in serous BOT with residual disease have shown high response rates but modest
effect on long-term survival1464 In case of recurrences where transformation to an invasive histology
has occurred consideration of platinum-taxane-based chemotherapy is reasonable The molecular
changes transforming BOT to invasive ovarian carcinoma may be clari1047297ed in the future with the
possibility of blocking the different lsquostepsrsquo in the carcinogenesis Today we know that both serous BOTand low-grade serous carcinoma frequently present with B-raf and K-ras mutations11
Survival
Overall survival for women with BOT is excellent 90ndash100 in most reports depending on age at
diagnosis FIGO stage and histologic type112651626566 Trillsch et al11 reported a 5-year overall survival
rate of almost 100 in early stage disease (FIGO I-II) and between 86 and 92 in more advanced
disease (FIGO III-IV) In a Norwegian population-based study67 the age-adjusted 1- 3- 5- and 10-year
relative survival rates of women with mucinous BOT were 98 97 97 and 95 respectively and for
women with serous BOT 96 93 90 and 90 respectively The relative risk of dying increased with
higher age at diagnosis The 5-year relative survival for women aged between 0 and 44 years was 99compared with 85 for women aged 75ndash89 years Nearly the same 1047297gures are reported by Sherman
et al12 with better survival for younger women and slightly better survival for serous tumours
compared with mucinous tumours although mucinous tumours in advanced stage had the poorest
long-term survival (855)12
Seidman and Kurman35 summarised 97 reports including a total of 4129 women with serous BOT
and showed a disease-speci1047297c survival rate of 99 for stage I disease and 953 for stage III disease
(mean follow up of 7 years)35 The 5-year survival was 98 for women with serous BOT with non-
invasive implants and 33 for those with invasive implants68
Conservative surgery
The median age of diagnosis for women with BOT is 40 years and nearly one-third are younger than
40 years Thus preservation of childbearing potential is an important issue for many of these women
To select women for fertility-sparing surgery without risk of reduced long-term survival is a challenge
for the gynaecologic oncologist3069 (Fig 2) Conservative surgery is de1047297ned as complete staging in
which the uterus and at least a part of one ovary are preserved1162 (Fig 2)
Although the standard treatment for all women with BOT is at least bilateral salpingo-
oophorectomy many young women with stage Ia tumours who have not completed childbearing
can be safely treated with unilateral salpingo-oophorectomy after comprehensive surgical staging
thereby preserving the fertility potential At least as important as the fertility issue however is
whether we can reduce the morbidity caused by radical surgery and whether a more conservative
approach is a safe alternative regarding cancer prognosis51
Recent studies from the Norwegian RadiumHospital8 and Gynecologic Oncology Group65 have shown that preservation of reproductive organs is
feasible Relapse rates after bilateral salpingo-oophorectomy range between 0 and 20 This rate
varies between 12 and 58 for cystectomy and between 25 and 57 for radical surgery Relapses
can also occur late and recurrences as late as 39 years after initial treatment have been reported5134
Predictors of relapse are resection margins containing tumour cells70 The frequency of persistence or
recurrence in 35 patients with serous-BOT treated by unilateral cystectomy bilateral cystectomy or
unilateral cystectomy with contralateral oophorectomy or salpingo-oophorectomy was retrospectively
investigated by Lim-Tan et al71 Conservative surgical treatment was carried out either because the
women were young and wanted to preserve their fertility or because the nature of the tumour was not
determined at the time of surgery Thirty-three women had stage I disease (19 stage Ia 10 stage Ib and
four stage Ic) and two had stage III disease Although 60 of the women had additional and in somecases de1047297nitive operations within relative short periods after initial cystectomy or cystectomies 21 had
conservation of ovarian tissue and were followed on average for 75 years All women with stage I
disease were alive without evidence of disease after surgical treatment alone The presence of
persistent or recurrent disease correlated with multifocality and involvement of resection margins
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336330
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 712
Multifocality may be a strong predictor of failure of cystectomy to control the disease No recurrence of
disease was seen in ovaries from which a single cyst had been removed with negative resection
margins Extensive sampling of the resection margins of ovarian cysts is important71
For many women with BOT fertility is an important issue It is therefore essential to discuss with
these young women the advantages and disadvantages between conservative and radical surgery
Conservative surgery preserves fertility and hormonal function but unfortunately with high risk of recurrence
In women with obvious stage I disease unilateral salpingo-oophorectomy or cystectomy has from
previous studies been shown to be safe This has also been con1047297rmed for women with advanced-stage
disease on the assumption of close follow up
Even for women with advanced disease conservative surgery might be considered after informed
consent The recurrence rate is high and invasive and even non-invasive implants may recur up to 15
as invasive OC without negative in1047298uence on survival34567273
Treatment at recurrent disease after conservative treatment
Early detected recurrences are curable with repeated surgery113451 and therefore conservativetreatment might again be considered in women with recurrent disease if fertility still is an issue and the
woman is informed about the high risk of recurrence and agrees on close follow up accepting repeated
surgery5162 If invasive implants are diagnosed this procedure could not be recommended In any case
of recurrent disease secondary debulking surgery is important as women suboptimally debulked have
poor survival115174
Fertility after conservative management of borderline ovarian tumour
Infertility is frequently observed inwomen with BOT A history of infertility beforediagnosis has been
reported in 10ndash35 of women75ndash77 To allow conservative surgery careful evaluation of the extent of
disease by the gynaecologist at the time of operation and meticulous examination of the cystectomyspecimen by the gynaecologist and pathologist are desirable to determine the prognosis after cys-
tectomy In a study by Morris et al76 onewoman who had disease-related deathwasnot staged properly
In a meta-analysis by Maltaris et al78 1483 women had BOT of whom 656 were treated conservatively
(442) A total of 196 women became pregnant and 111 relapsed after unilateral salpingo-
oophorectomy only one woman died from the disease (015) The investigators therefore suggest
that conservative surgery is justi1047297able for some women with a good prognostic index Unilateral
oophorectomy omentectomy and appendectomy in stage Ia diploid mucinous BOT are indicated for
young women who wish to preservefertility (Fig 2) In stage Ia diploid serous BOT thesame procedure is
safe if the contralateral ovary is macroscopically normal Careful inspection of a macroscopically normal
contralateral ovary should be suf 1047297cient inyoung womenwith stageIa disease who wish to remainfertile
Surgery itself can impair the fertility function by loss of ovarian tissue pelvic scarring and adhesionsblocking the fallopian tube Post-surgery fertility factors such as ovulation fallopian tubes and sperm
factors should be investigated and treated if necessary About one-third of women undergoing
conservative surgery for BOT will be able to conceive with no negative in1047298uence of pregnancy on the
disease60727779 Ovulation induction is often required in order to conceive80 The role of ovulation
(in-vitro [IVF] fertilisation) drugs in BOT is currently under debate7780ndash84
Recently a large nationwide cohort study of 19146 subfertile women in the Netherlands who
received IVF drugs between 1983 and 1995 and a comparison group of 6953 subfertile women who
were not treated was published After a median follow up of 15 years a total of 77 ovarian malignancies
were observed in the cohort including 42 women with epithelial ovarian cancer and 35 women with
BOT Sixty-one ovarian malignancies were observed in the IVF-group and 16 in the unexposed (control)
group The ratio hazard for epithelial ovarian cancer and BOT was 167 (074 to 375) and 425 (127 to1418) respectively85 The conclusion of Burger et al85 was that IVF increases the risk of BOT
A worrying1047297nding of their study is the increased risk of epithelial ovarian cancer and BOT even after 15
years of follow up Fasouliotis et al80 found no perceptible negative effect of previous BOT on preg-
nancy rates after IVF The same was shown by Fortin et al84 in a study of 30 women treated with IVF
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 331
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 812
drugs for infertility after conservative surgery Thirteen pregnancies were observed Disease in four
women recurred All recurrences were BOT on a remaining ovary that had been treated by surgery
alone All women are currently disease-free after secondary surgery Fortin et al84 concluded that IVF
drugs can be used safely in womenwho develop infertility after conservative treatment of BOT Because
of the low number of women treated with IVF drugs Norwegian Radium Hospital guidelines are to
proceed with caution and only women with early stage BOT are permitted to be treated with IVF drugsThe latest development regarding reproduction and BOT is cryopreservation 86 Women who have
their ovaries removed because of large stage Ib BOT now have a possibility of becoming pregnant
Biopsies from normal ovarian cortex can be taken during the primary operation In 2004 a live birth
after a fresh ovarian tissue transplant in a primate was reported87 Donnez et al86 described in 2004
a live birth after orthotopic auto-transplantation of cryopreserved ovarian tissue Their1047297ndings opened
new possibilities for young women facing premature ovarian failure
Women with reduced fertility after surgery can consider ovarian stimulation egg retrieval and egg
freezing Ovarian stimulation and exposure to high oestrogen exposure do not seem to increase the risk
for recurrence Nor do pregnancies have negative in1047298uence on survival7277
To assure future fertility preservation in women with BOT the gynaecologic oncologist should
collaborate closely with the reproductive endocrinologists even before surgery Until more mature dataexist the general recommendation is a limited number of stimulation cycles only for stage I patients In
case of bilateral salpingo-oophorectomy cryopreservation of ovarian cortex biopsy from the less
affected ovary could be considered although this is not always technically possible1151
Follow up
Follow up should be long term and lifelong because recurrences may develop after more than 15 years
In conservatively treated womenclose follow up is crucial with special attentionto theremainingovaryIt
is still debated if the remaining ovary (and uterus) should be removed after the family is completed For
low-risk BOT there is no indication for this procedure but in women with high-risk of recurrence the
procedure is optional the alternative being to wait until recurrence or carry out radical surgery Manywomen will choose radical surgery when the family is completed because of psychological stress
The general recommendation is follow up every 3 months during the 1047297rst 2 years and then every 6
months for the next 3 years and annually thereafter The women is followed with pelvic examination
transvaginal ultrasound and calcium 125 measurement1451 (Fig 2)
Future direction of borderline ovarian tumour
A key issue for future research on BOTconcerning epidemiology is the identi1047297cation of risk factors for
invasive implants recurrences and death and also the identi1047297cation of predisposing heritable factors
For clinical management improved methods for preoperative and intraoperative diagnosis should
be considered in addition to the role of laparoscopic surgery in removal of complex cysts improvedmethods for distinguishing metastases from BOT and determination of risk associated with conser-
vative treatment
For pathology and molecular biology molecular studies are needed to assess the relationship
between serous BOT low-grade serous carcinoma and high-grade serous carcinoma Molecular studies
are also needed to aid in the characterisation of implants and studies need to be conducted to
determine the biology of microinvasive BOT and the clinical signi1047297cance of long-term follow up
Conclusion
Borderline ovarian tumours are ovarian tumours with good prognosis that account for 10ndash20 of all
epithelial ovarian cancer Historically standard primarysurgeryincludedbilateral salpingo-oophorectomyomentectomy peritoneal washing and complete peritoneal resection of macroscopic lesions or multiple
biopsies In cases of M-BOT women are also treated with appendectomy As one-third of BOT are diagnosed
inwomenyounger than40 years however fertility-sparingtreatment (ie preservation of the uterus andat
least part of one ovary) has been increasingly used in the past 10 years Fertility drugs are well tolerated in
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336332
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 912
women with infertility after fertility-sparing surgery Careful selection of candidates is necessary Lapa-
roscopic techniques can be used but are reserved for oncologic surgeons This conservative treatment
increases therateof recurrencebutwithoutany effecton survivalThespontaneouspregnancy rate is nearly
50and most are achieved spontaneously Spontaneous pregnancy can occurafter conservative treatment
of advanced-stage BOT (with non-invasive implants) These women should be closely followed up Further
research has to concentrate on clinical risk-factors histopathological markers and pathogenesis to guar-antee the best clinical management for women with BOT
Con1047298ict of interest statement
None declared
Practice points
BOTare ovarian tumours with good prognosis that account for 10ndash20 of all epithelial ovarian
cancer Historically standard primary surgery included bilateral salpingo-oophorectomy omentec-
tomy peritoneal washing and complete peritoneal resection of macroscopic lesions or
multiple biopsies
In case of mucinous BOT women are also treated with appendectomy
Adjuvant therapy for the treatment of BOT has no proven bene1047297t
As one-third of BOT are diagnosed in women younger than 40 years fertility-sparing treat-
ment (ie preservation of the uterus and at least part of one ovary) has been increasingly used
in the past 10 years
Fertility drugs are well tolerated in women with infertility after fertility-sparing surgery
Careful selection of candidates is necessary
Laparoscopic techniques can be used but are reserved for oncologic surgeons Spontaneous pregnancy can occur after conservative treatment of advanced stage BOT (with
non-invasive implants)
These women should be closely followed up
Research agenda
Epidemiology
Identify risk factors for invasive implants recurrences and death
Identify predisposing heritable factors
Clinical management
Improve methods for preoperative and intraoperative diagnosis
Further explore the role of laparoscopic surgery in the removal of complex cysts
Improve methods for distinguishing metastases from BOTand determine risk associated with
conservative treatment
Pathology and molecular biology
Conduct molecular studies to assess the relationship between serous BOT low-grade serous
carcinoma and high-grade serous carcinoma Conduct molecular studies to aid in the characterisation of implants
Conduct studies to determine the biology of microinvasive BOTand the clinical signi1047297cance of
long-term follow up
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 333
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1012
Acknowledgement
We wish to thank Mrs Gry Seppola for technical assistance and gratefully acknowledge the1047297nancial
support from the Inger and John Fredriksen Foundation for Ovarian Cancer Research
References
1 Taylor HC Malignant and semi-malignant tumors of the ovary Surg Gynecol Obstet 1929 48 204ndash2302 Kottmeier HL Kolstad P McGarrity KA Annual report on results of treatment in gynaecologic cancer vol 17 Statements of
results obtained in 1969ndash1972 inclusive FIGO Stockholm Sweden Editorial of 1047297ce Radiumhemmet 19733 Serov SF Scully RE amp Sobin LH International histological classi 1047297cation of tumors no 9 Histoloigcal typing of ovarian tumours
Geneval World Health Organization 19734 Hart WR amp Norris HJ Borderline and malignant mucinous tumors of the ovary Histologic criteria and clinical behavior
Cancer 1973 31 1031ndash10455 Scully RE Tumors of the ovary and maldeveloped gonads Fascicle 16 In Atlas of tumor pathology Second series Wash-
ington DC Armed Forces Institute of Pathology 1979 pp 75ndash906 Lenhard MS Mitterer S Kuumlmper C et al Long-term follow-up after ovarian borderline tumor relapse and survival in
a large patient cohort Eur J Obstet Gynecol Reprod Biol 2009 145 189ndash194
7 Quirk JT amp Natarajan N Ovarian cancer incidence in the United States 1992ndash
1999 Gynecol Oncol 2005 97 519ndash
5238 Kaern J Tropeacute CG amp Abeler VM A retrospective study of 370 borderline tumors of the ovary treated at the NorwegianRadium Hospital from 1970 to 1982 A review of clinicopathologic features and treatment modalities Cancer 1993 711810ndash1820
9 Bjoslashrge T Engeland A Hansen S et al Trends in the incidence of ovarian cancer and borderline tumours in Norway1954ndash1993 Int J Cancer 1997 71 780ndash786
10 Skiacuternisdoacutettir I Garmo H Wilander E et al Borderline ovarian tumors in Sweden 1960ndash2005 trends in incidence and age atdiagnosis compared to ovarian cancer Int J Cancer 2008 123 1897ndash1901
11 Trillsch F Mahner S Ruetzel J et al Clinical management of borderline ovarian tumors Expert Rev Anticancer Ther 2010 101115ndash1124
12 Sherman ME Mink PJ Curtis R et al Survival among women with borderline ovarian tumors and ovarian carcinomaa population-based analysis Cancer 2004 100 1045ndash1052
13 Kramer JL Greene MH Epidemiology of ovarian fallopian tube and primary peritoneal cancer In Gershenson DMMcGuire WP Gore M et al eds Gynecologic cancer Controversies in management 1st ed Philadelphia Elsevier ChurchillLivingstone 2004 pp 327ndash340
14 Tropeacute C Davidson B Paulsen T et al Diagnosis and treatment of borderline ovarian neoplasms lsquothe state of the artrsquo Eur J Gynaecol Oncol 2009 30 471ndash482
15 Kurman RJ amp Shih IeM Pathogenesis of ovarian cancer lessons from morphology and molecular biology and their clinicalimplications Int J Gynecol Pathol 2008 27 151ndash160
16 Kurman RJ Visvanathan K Roden R et al Early detection and treatment of ovarian cancer shifting from early stage tominimal volume of disease based on a new model of carcinogenesis Am J Obstet Gynecol 2008 198 351ndash356
17 Shih IeM amp Kurman RJ Ovarian tumorigenesis a proposed model based on morphological and molecular genetic analysis Am J Pathol 2004 164 1511ndash1518
18 Levanon K Crum C amp Drapkin R New insights into the pathogenesis of serous ovarian cancer and its clinical impact J ClinOncol 2008 26 5284ndash5293
19 Meinhold-Heerlein I Bauerschlag D Hilpert F et al Molecular and prognostic distinction between serous ovarian carci-nomas of varying grade and malignant potential Oncogene 2005 24 1053ndash1065
20 Bonome T Lee JY Park DC et al Expression pro1047297ling of serous low malignant potential low-grade and high-grade tumorsof the ovary Cancer Res 2005 65 10602ndash10612
21 Mahner S Baasch C Schwarz J et al C-Fos expression is a molecular predictor of progression and survival in epithelialovarian carcinoma Br J Cancer 2008 99 1269ndash1275
22 Ortiz BH Ailawadi M Colitti C et al Second primary or recurrence Comparative patterns of p53 and K-ras mutationssuggest that serous borderline ovarian tumors and subsequent serous carcinomas are unrelated tumors Cancer Res 200161 7264ndash7267
23 Lee KR Tavassoli FA Prat J et al Tumours of the ovary and peritoneum In Tavassoli FA amp Devilee P (eds) Pathology and
genetics Tumours of the breast and female genital organs Lyon IARC Press 2003 pp 113ndash20224 Oedegaard E Ovarian carcinomas and borderline ovarian tumors - molecular markers and operative treatment Dissertation
Facutly of Medicine University of Oslo 200825 Mok SC Bell DA Knapp RC et al Mutation of K-ras protooncogene in human ovarian epithelial tumors of borderline
malignancy Cancer Res 1993 53 1489ndash149226 du Bois A Ewald-Riegler N du Bois O et al Borderline tumors of the ovary a systematic review [German] Geburtsh
Frauenheilk 2009 69 807ndash83327 Seidman JD Horkayne-Szakaly I Haiba M et al The histologic type and stage distribution of ovarian carcinomas of surface
epithelial origin Int J Gynecol Pathol 2004 23 41ndash44
28 Prat J amp De Nictolis M Serous borderline tumors of the ovary a long-term follow-up study of 137 cases including 18 witha micropapillary pattern and 20 with microinvasion Am J Surg Pathol 2002 26 1111ndash1128
29 Bell DA Weinstock MA amp Scully RE Peritoneal implants of ovarian serous borderline tumors Histologic features andprognosis Cancer 1988 62 2212ndash2222
30 Tinelli R Tinelli A Tinelli FG et al Conservative surgery for borderline ovarian tumors a review Gynecol Oncol 2006 100
185ndash191
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336334
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1112
31 Kurman RJ amp Trimble CL The behavior of serous tumors of low malignant potential are they ever malignant Int J Gynecol
Pathol 1993 12 120ndash12732 Morice P Camatte S Rey A et al Prognostic factors for patients with advanced stage serous borderline tumours of the
ovary Ann Oncol 2003 14 592ndash59833 Bradley RF Stewart 4th JH Russell GB et al Pseudomyxoma peritonei of appendiceal origin a clinicopathologic analysis of
101 patients uniformly treated at a single institution with literature review Am J Surg Pathol 2006 30 551ndash559
34 Silva EG Gershenson DM Malpica A et al The recurrence and the overall survival rates of ovarian serous borderlineneoplasms with noninvasive implants is time dependent Am J Surg Pathol 2006 30 1367ndash137135 Seidman JD amp Kurman RJ Ovarian serous borderline tumors a critical review of the literature with emphasis on prognostic
indicators Hum Pathol 2000 31 539ndash55736 Chang SJ Ryu HS Chang KH et al Prognostic signi1047297cance of the micropapillary pattern in patients with serous borderline
ovarian tumors Acta Obstet Gynecol Scand 2008 87 476ndash48137 Fox H amp Wells M Surface epithelialstromal tumors of the ovary In Fox H amp Wells M (eds) Haines and Taylor Obstetrical and
Gynaecological Pathology 5th ed London Churchill Livingstone 2003 pp 713ndash74338 Ren J Peng Z amp Yang K A clinicopathologic multivariate analysis affecting recurrence of borderline ovarian tumors Gynecol
Oncol 2008 110 162ndash16739 Longacre TA McKenney JK Tazelaar HD et al Ovarian serous tumors of low malignant potential (borderline tumors)
outcome-based study of 276 patients with long-term (gt or frac145-year) follow-up Am J Surg Pathol 2005 29 707ndash72340 Cusidoacute M Balagueroacute L Hernandez G et al Results of the national survey of borderline ovarian tumors in Spain Gynecol
Oncol 2007 104 617ndash62241 Kaern J Tropeacute CG Kristensen GB et al DNA ploidy the most important prognostic factor in patients with borderline
tumors of the ovary Int J Gynecol Cancer 1993 3 349ndash35842 Meyer JS Gersell DJ amp Yim S Cell proliferation in ovarian carcinoma superior accuracy of S-phase fraction (SPF) by DNA
labeling index versus 1047298ow cytometric SPF lack of independent prognostic power for SPF and DNA ploidy and limitedeffect of SPF on tumor growth rate Gynecol Oncol 2001 81 466ndash476
43 Verbruggen MB van Diest PJ Baak JP et al The prognostic and clinical value of morphometry and DNA cytometry inborderline ovarian tumors a prospective study Int J Gynecol Pathol 2009 28 35ndash40
44 Yokoyama Y Moriya T Takano T et al Clinical outcome and risk factors for recurrence in borderline ovarian tumours Br J Cancer 2006 94 1586ndash1591
45 Leake JF Rader JS Woodruff JD et al Retroperitoneal lymphatic involvement with epithelial ovarian tumors of lowmalignant potential Gynecol Oncol 1991 42 124ndash130
46 Paulsen T Kaern J Kjaerheim K et al Symptoms and referral of women with epithelial ovarian tumors Int J Gynaecol Obstet 2005 88 31ndash37
47 Paulsen T Epithelial ovarian cancer A clinical epidemiological approach on diagnosis and treatment Dissertation Faculty of Medicine University of Oslo 2007
48 Tropeacute CG Kristensen G amp Makar A Surgery for borderline tumor of the ovary Semin Surg Oncol 2000 19 69ndash7549 Tempfer CB Polterauer S Bentz EK et al Accuracy of intraoperative frozen section analysis in borderline tumors of the
ovary a retrospective analysis of 96 cases and review of the literature Gynecol Oncol 2007 107 248ndash25250 Camatte S Morice P Thoury A et al Impact of surgical staging in patients with macroscopic lsquostage Irsquo ovarian borderline
tumours analysis of a continuous series of 101 cases Eur J Cancer 2004 40 1842ndash184951 Cadron I Leunen K Van Gorp T et al Management of borderline ovarian neoplasms J Clin Oncol 2007 25 2928ndash293752 Snider DD Stuart GC Nation JG et al Evaluation of surgical staging in stage I low malignant potential ovarian tumors
Gynecol Oncol 1991 40 129ndash13253 Ronnett BM Kurman RJ Zahn CM et al Pseudomyxoma peritonei in women a clinicopathologic analysis of 30 cases with
emphasis on site of origin prognosis and relationship to ovarian mucinous tumors of low malignant potential Hum Pathol
1995 26 509ndash52454 Seidman JD Elsayed AM Sobin LH et al Association of mucinous tumors of the ovary and appendix A clinicopathologic
study of 25 cases Am J Surg Pathol 1993 17 22ndash3455 Trimble EL amp Trimble LC Epithelial ovarian tumors of low malignant potential In Markman M amp Hoskins W (eds) Cancer
of the Ovary New York Raven Press 1993 pp 415ndash429
56 Zanetta G Rota S Chiari S et al Behavior of borderline tumors with particular interest to persistence recurrence andprogression to invasive carcinoma a prospective study J Clin Oncol 2001 19 2658ndash266457 Fauvet R Boccara J Dufournet C et al Restaging surgery for women with borderline ovarian tumors results of a French
multicenter study Cancer 2004 100 1145ndash115158 Zapardiel I Rosenberg P Peiretti M et al The role of restaging borderline ovarian tumors single institution experience and
review of the literature Gynecol Oncol 2010 119 274ndash27759 Def 1047297eux X Morice P Camatte S et al Results after laparoscopic management of serous borderline tumor of the ovary with
peritoneal implants Gynecol Oncol 2005 97 84ndash8960 Fauvet R Boccara J Dufournet C et al Laparoscopic management of borderline ovarian tumors results of a French
multicenter study Ann Oncol 2005 16 403ndash41061 Vandenput I Amant F amp Vergote I Peritoneal recurrences might be less common in advanced stage serous borderline
ovarian tumors that were treated by laparotomy Gynecol Oncol 2005 98 52362 CadronI Amant F VanGorp Tet alThe management of borderline tumours of theovary Curr Opin Oncol 2006 18 488ndash49363 Vergote I De Brabanter J Fyles A et al Prognostic importance of degree of differentiation and cyst rupture in stage I
invasive epithelial ovarian carcinoma Lancet 2001 357 176ndash182
64 Gershenson DM amp Silva EG Serous ovarian tumors of low malignant potential with peritoneal implants Cancer 1990 65578ndash585
65 Gershenson DM Clinical management potential tumours of low malignancy Best Pract Res Clin Obstet Gynaecol 2002 16513ndash527
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 335
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1212
66 Heintz AP Odicino F Maisonneuve P et al Carcinoma of the ovary FIGO 26th Annual Report on the Results of Treatment inGynecological Cancer Int J Gynaecol Obstet 2006 95(Suppl 1) S161ndashS192
67 Bjoslashrge T Engeland A Hansen S et al Prognosis of patients with ovarian cancer and borderline tumours diagnosed inNorway between 1954 and 1993 Int J Cancer 1998 75 663ndash670
68 Seidman JD amp Kurman RJ Subclassi1047297cation of serous borderline tumors of the ovary into benign and malignant typesA clinicopathologic study of 65 advanced stage cases Am J Surg Pathol 1996 20 1331ndash1345
69 Sherman ME Berman J Birrer MJ et al Current challenges and opportunities for research on borderline ovarian tumorsHum Pathol 2004 35 961ndash97070 Leake JF Currie JL Rosenshein NB et al Long-term follow-up of serous ovarian tumors of low malignant potential Gynecol
Oncol 1992 47 150ndash15871 Lim-Tan SK Cajigas HE amp Scully RE Ovarian cystectomy for serous borderline tumors a follow-up study of 35 cases Obstet
Gynecol 1988 72 775ndash78172 Morice P Camatte S El Hassan J et al Clinical outcomes and fertility after conservative treatment of ovarian borderline
tumors Fertil Steril 2001 75 92ndash9673 Camatte S Morice P Pautier P et al Fertility results after conservative treatment of advanced stage serous borderline
tumour of the ovary BJOG 2002 109 376ndash38074 Crispens MA Bodurka D Deavers M et al Response and survival in patients with progressive or recurrent serous ovarian
tumors of low malignant potential Obstet Gynecol 2002 99 3ndash1075 Fauvet R Poncelet C Boccara J et al Fertility after conservative treatment for borderline ovarian tumors a French
multicenter study Fertil Steril 2005 83 284ndash29076 Morris RT Gershenson DM Silva EG et al Outcome and reproductive function after conservative surgery for borderline
ovarian tumors Obstet Gynecol 2000 95 541ndash54777 Gotlieb WH Flikker S Davidson B et al Borderline tumors of the ovary fertility treatment conservative management and
pregnancy outcome Cancer 1998 82 141ndash14678 Maltaris T Boehm D Dittrich R et al Reproduction beyond cancer a message of hope for young women Gynecol Oncol
2006 103 1109ndash112179 Beiner ME Gotlieb WH Davidson B et al Infertility treatment after conservative management of borderline ovarian
tumors Cancer 2001 92 320ndash32580 Fasouliotis SJ Davis O Schattman G et al Safety and ef 1047297cacy of infertility treatment after conservative management of
borderline ovarian tumors a preliminary report Fertil Steril 2004 82 568ndash57281 Kashyap S amp Davis OK Ovarian cancer and fertility medications a critical appraisal Semin Reprod Med 2003 21 65ndash7182 Morice P Camatte S Wicart-Poque F et al Results of conservative management of epithelial malignant and borderline
ovarian tumours Hum Reprod Update 2003 9 185ndash19283 Whittemore AS Harris R amp Itnyre J Characteristics relating to ovarian cancer risk collaborative analysis of 12 US case-
control studies II Invasive epithelial ovarian cancers in white women Collaborative Ovarian Cancer Group Am J Epi-demiol 1992 136 1184ndash1203
84 Fortin A Morice P Thoury A et al Impact of infertility drugs after treatment of borderline ovarian tumors results of a retrospective multicenter study Fertil Steril 2007 87 591ndash596
85 Burger CW van de Swaluw A Mooij TM et al Risk of borderline and invasive ovarian tumors after ovarian stimulation forin vitro fertilization in a large Dutch cohort after 15 years of follow-up Abstracts presented for the 40th Annual Meeting of the Society of Gynecologic Oncologists February 2009 (abstract no 6) Gynecol Oncol 2009 112(Suppl) S4
86 Donnez J Dolmans MM Demylle D et al Livebirth after orthotopic transplantation of cryopreserved ovarian tissue Lancet 2004 364 1405ndash1410
87 Lee DM Yeoman RR Battaglia DE et al Live birth after ovarian tissue transplant Nature 2004 428 137ndash138
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336336

7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 412
when only ovarian cystectomy rather than salpingo-oophorectomy has been carried out This might be
explained by missing an invasive component owing to inadequate histopathologic evaluation of these
large tumours Therefore unilateral salpingo-oophorectomy is recommended in mucinous BOT1114
Prognostic factors
As BOT in general has an excellent survival it might be dif 1047297cult to identify variables that improve
survival As many women with BOT are of reproductive age at diagnosis more conservative treatment
preserving thechildbearingability is desirable International Federation of Gynecologyand Obstetrics stage
is thestrongest prognostic factor for recurrence andsurvival for BOT as well as for invasive ovariancancers
Micropapillary histology was reported as an additional risk factor for serous BOT but this issue is contro-
versial as poor prognosis is only seen if this histology is associated with invasive implants2834ndash36 Tumours
with evidence of stromal invasion of less than 10 mm2 behave clinically as BOT and are today classi1047297ed as
BOT222437ndash40 In the retrospective study from the Norwegian Radium Hospital41 370 BOT were treated
between 1970 and 1982 and the follow up was complete with a median follow-up time of 152 months
(range 6ndash354 months) By multivariate analysis the only three independent prognostic factors for disease-
free and long-term survival were FIGO stage (P lt 00001) histologic type (P lt 005) and age (P lt 0005) Inanother study of the same women including DNA ploidy the women could be divided into risk groups41
The low-risk group (100 disease-free survival) was characterised by stage I disease diploid serous BOTor
mucinous BOT and age less than 40 years The high-risk group (75 or higher risk of dying of disease) had
aneuploid serous BOT or mucinous BOT stage II-III disease and age older than 70 years Deoxyribonucleic
acid ploidy was the strongest prognostic factor in BOT in the study by Kaern et al41 but this has unfortu-
nately not been reproduced by others4243 Lymph-node involvement could not convincingly be con1047297rmed
to be an independent risk factor35414445
Symptoms
Limited information exists about symptom registration by women with BOT at diagnosis Mostwomen may be asymptomatic and a pelvic mass discovered at routine pelvic examination Symptoms
are less common compared with symptoms registered for women with invasive ovarian cancer
although 75 of women with BOT may have at lease one symptom as abdominal pain or discomfort
bowel irregularity and persisting fatigue or weight loss4647
Standard treatment
The diagnosis of BOT cannot be determined before surgery Intraoperative frozen section diagnosis
of BOT is often dif 1047297cult even for experienced pathologists Frozen sections may be useful for
discrimination between BOTand epithelial ovarian cancer and benign tumour (over-diagnosis less than
10) but not for discrimination between BOT and epithelial ovarian cancer (under-diagnosis in 25ndash
30of women)4849 Less than 50 of women with BOT will have a complete surgical staging this without
obvious in1047298uence on survival
The standard guidelines for primarysurgery in BOTaresimilar to these for invasive ovarian carcinomas
removal of all macroscopic disease and proper surgical staging hysterectomy with bilateral salpingo-
oophorectomy multiple peritoneal biopsies and peritoneal washing with cytology For mucinous BOT
appendectomy should also be carried out33 Lymph-node sampling has not been part of the standard
procedure A recently published German study reported systematic lymph-node dissection in 189 of
women with BOT11 Involvement of lymph nodes even with upstage do not in1047298uence recurrence or
survival rate850 Lymph-node involvement is rarely seen in M-BOT Lymphadenectomy can be omitted
even for stage II and III disease as there is no difference in the recurrence or survival rate (Fig 2)5051
Restaging procedures
Despite the fact that experts have recommended comprehensive surgical staging for many years most
women referred to university or comprehensive cancer centres after primary surgery have incomplete
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336328
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 512
surgery Another common event is that malignancy is not suspected at the initial operation and therefore
the abdomen is not properly explored Should this woman undergo re-operation Snider et al52 upstaged
1047297ve out of 27 women with stage I disease None of the 12 women with mucinous BOT were upstaged
whereas1047297veoutof 13 women with serous BOTwere upstagedMucinousBOTgrossly con1047297ned to one ovary
are probably unlikely to be upstaged at a restaging procedure If evidence of extra-ovarian disease exists
complete surgical staging and appendectomy are indicated Mucinous BOT with abdominal spread are in50 claimed to arise in the appendix or simultaneously in one or both ovaries5354 For serous BOT it is
reasonable to do a second operation as lymph-node involvement has been reported in about 20 in
apparentstage I tumourswitheven higher incidence in more advanced stages45 At the Norwegian Radium
Hospital we recommend restaging if the women are insuf 1047297ciently staged at primary operation in agree-
ment with Cadron et al51 and Trimble and Trimble55 We also believe that the decision to restage must be
individualised taking into consideration the adequacy of the previous abdominal exploration the tumour
subtype and potential treatment of residual disease as well as thelevel of concern for both thewomanand
the clinician even if there is little proof that restaging operations have an effect on survival115056ndash58
Laparoscopy
Laparoscopic treatment has become an attractive approach for benign ovarian tumours (pelvic
mass) The development of the laparoscopic techniques with the use of endo-bag gives less risk of
spillage during surgery and less port-side metastases For conservatively treated women wishing to
preserve fertility this is a more favourable approach and has short postoperative recovery fewer
adhesions and improved cosmetic results59 Cyst rupture and incomplete staging occur signi1047297cantly
more frequently by laparoscopy compared with laparotomy (339 v 124)6061 but do not in1047298uence
survival The laparoscopic treatment may result in higher recurrence rate which must be discussed
with the woman The woman should agree to close follow up and repeated surgery5162 Other concerns
are port metastases63 and improper staging61
Postoperative treatment of borderline ovarian tumours
Today there is no proven bene1047297t from adjuvant therapy (chemotherapy or radiotherapy) even in
advanced stage disease and in the presence of invasive implants1432 No randomised-controlled studies
Fig 2 Recommendation treatmentof borderline ovarian tumours Modi1047297ed fromTrillsch et al11 and Cadron et al51 with permission
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 329
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 612
have evaluated the ef 1047297cacy of chemotherapy in advanced stage BOT with residual disease Cisplatin-
based therapy in serous BOT with residual disease have shown high response rates but modest
effect on long-term survival1464 In case of recurrences where transformation to an invasive histology
has occurred consideration of platinum-taxane-based chemotherapy is reasonable The molecular
changes transforming BOT to invasive ovarian carcinoma may be clari1047297ed in the future with the
possibility of blocking the different lsquostepsrsquo in the carcinogenesis Today we know that both serous BOTand low-grade serous carcinoma frequently present with B-raf and K-ras mutations11
Survival
Overall survival for women with BOT is excellent 90ndash100 in most reports depending on age at
diagnosis FIGO stage and histologic type112651626566 Trillsch et al11 reported a 5-year overall survival
rate of almost 100 in early stage disease (FIGO I-II) and between 86 and 92 in more advanced
disease (FIGO III-IV) In a Norwegian population-based study67 the age-adjusted 1- 3- 5- and 10-year
relative survival rates of women with mucinous BOT were 98 97 97 and 95 respectively and for
women with serous BOT 96 93 90 and 90 respectively The relative risk of dying increased with
higher age at diagnosis The 5-year relative survival for women aged between 0 and 44 years was 99compared with 85 for women aged 75ndash89 years Nearly the same 1047297gures are reported by Sherman
et al12 with better survival for younger women and slightly better survival for serous tumours
compared with mucinous tumours although mucinous tumours in advanced stage had the poorest
long-term survival (855)12
Seidman and Kurman35 summarised 97 reports including a total of 4129 women with serous BOT
and showed a disease-speci1047297c survival rate of 99 for stage I disease and 953 for stage III disease
(mean follow up of 7 years)35 The 5-year survival was 98 for women with serous BOT with non-
invasive implants and 33 for those with invasive implants68
Conservative surgery
The median age of diagnosis for women with BOT is 40 years and nearly one-third are younger than
40 years Thus preservation of childbearing potential is an important issue for many of these women
To select women for fertility-sparing surgery without risk of reduced long-term survival is a challenge
for the gynaecologic oncologist3069 (Fig 2) Conservative surgery is de1047297ned as complete staging in
which the uterus and at least a part of one ovary are preserved1162 (Fig 2)
Although the standard treatment for all women with BOT is at least bilateral salpingo-
oophorectomy many young women with stage Ia tumours who have not completed childbearing
can be safely treated with unilateral salpingo-oophorectomy after comprehensive surgical staging
thereby preserving the fertility potential At least as important as the fertility issue however is
whether we can reduce the morbidity caused by radical surgery and whether a more conservative
approach is a safe alternative regarding cancer prognosis51
Recent studies from the Norwegian RadiumHospital8 and Gynecologic Oncology Group65 have shown that preservation of reproductive organs is
feasible Relapse rates after bilateral salpingo-oophorectomy range between 0 and 20 This rate
varies between 12 and 58 for cystectomy and between 25 and 57 for radical surgery Relapses
can also occur late and recurrences as late as 39 years after initial treatment have been reported5134
Predictors of relapse are resection margins containing tumour cells70 The frequency of persistence or
recurrence in 35 patients with serous-BOT treated by unilateral cystectomy bilateral cystectomy or
unilateral cystectomy with contralateral oophorectomy or salpingo-oophorectomy was retrospectively
investigated by Lim-Tan et al71 Conservative surgical treatment was carried out either because the
women were young and wanted to preserve their fertility or because the nature of the tumour was not
determined at the time of surgery Thirty-three women had stage I disease (19 stage Ia 10 stage Ib and
four stage Ic) and two had stage III disease Although 60 of the women had additional and in somecases de1047297nitive operations within relative short periods after initial cystectomy or cystectomies 21 had
conservation of ovarian tissue and were followed on average for 75 years All women with stage I
disease were alive without evidence of disease after surgical treatment alone The presence of
persistent or recurrent disease correlated with multifocality and involvement of resection margins
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336330
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 712
Multifocality may be a strong predictor of failure of cystectomy to control the disease No recurrence of
disease was seen in ovaries from which a single cyst had been removed with negative resection
margins Extensive sampling of the resection margins of ovarian cysts is important71
For many women with BOT fertility is an important issue It is therefore essential to discuss with
these young women the advantages and disadvantages between conservative and radical surgery
Conservative surgery preserves fertility and hormonal function but unfortunately with high risk of recurrence
In women with obvious stage I disease unilateral salpingo-oophorectomy or cystectomy has from
previous studies been shown to be safe This has also been con1047297rmed for women with advanced-stage
disease on the assumption of close follow up
Even for women with advanced disease conservative surgery might be considered after informed
consent The recurrence rate is high and invasive and even non-invasive implants may recur up to 15
as invasive OC without negative in1047298uence on survival34567273
Treatment at recurrent disease after conservative treatment
Early detected recurrences are curable with repeated surgery113451 and therefore conservativetreatment might again be considered in women with recurrent disease if fertility still is an issue and the
woman is informed about the high risk of recurrence and agrees on close follow up accepting repeated
surgery5162 If invasive implants are diagnosed this procedure could not be recommended In any case
of recurrent disease secondary debulking surgery is important as women suboptimally debulked have
poor survival115174
Fertility after conservative management of borderline ovarian tumour
Infertility is frequently observed inwomen with BOT A history of infertility beforediagnosis has been
reported in 10ndash35 of women75ndash77 To allow conservative surgery careful evaluation of the extent of
disease by the gynaecologist at the time of operation and meticulous examination of the cystectomyspecimen by the gynaecologist and pathologist are desirable to determine the prognosis after cys-
tectomy In a study by Morris et al76 onewoman who had disease-related deathwasnot staged properly
In a meta-analysis by Maltaris et al78 1483 women had BOT of whom 656 were treated conservatively
(442) A total of 196 women became pregnant and 111 relapsed after unilateral salpingo-
oophorectomy only one woman died from the disease (015) The investigators therefore suggest
that conservative surgery is justi1047297able for some women with a good prognostic index Unilateral
oophorectomy omentectomy and appendectomy in stage Ia diploid mucinous BOT are indicated for
young women who wish to preservefertility (Fig 2) In stage Ia diploid serous BOT thesame procedure is
safe if the contralateral ovary is macroscopically normal Careful inspection of a macroscopically normal
contralateral ovary should be suf 1047297cient inyoung womenwith stageIa disease who wish to remainfertile
Surgery itself can impair the fertility function by loss of ovarian tissue pelvic scarring and adhesionsblocking the fallopian tube Post-surgery fertility factors such as ovulation fallopian tubes and sperm
factors should be investigated and treated if necessary About one-third of women undergoing
conservative surgery for BOT will be able to conceive with no negative in1047298uence of pregnancy on the
disease60727779 Ovulation induction is often required in order to conceive80 The role of ovulation
(in-vitro [IVF] fertilisation) drugs in BOT is currently under debate7780ndash84
Recently a large nationwide cohort study of 19146 subfertile women in the Netherlands who
received IVF drugs between 1983 and 1995 and a comparison group of 6953 subfertile women who
were not treated was published After a median follow up of 15 years a total of 77 ovarian malignancies
were observed in the cohort including 42 women with epithelial ovarian cancer and 35 women with
BOT Sixty-one ovarian malignancies were observed in the IVF-group and 16 in the unexposed (control)
group The ratio hazard for epithelial ovarian cancer and BOT was 167 (074 to 375) and 425 (127 to1418) respectively85 The conclusion of Burger et al85 was that IVF increases the risk of BOT
A worrying1047297nding of their study is the increased risk of epithelial ovarian cancer and BOT even after 15
years of follow up Fasouliotis et al80 found no perceptible negative effect of previous BOT on preg-
nancy rates after IVF The same was shown by Fortin et al84 in a study of 30 women treated with IVF
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 331
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 812
drugs for infertility after conservative surgery Thirteen pregnancies were observed Disease in four
women recurred All recurrences were BOT on a remaining ovary that had been treated by surgery
alone All women are currently disease-free after secondary surgery Fortin et al84 concluded that IVF
drugs can be used safely in womenwho develop infertility after conservative treatment of BOT Because
of the low number of women treated with IVF drugs Norwegian Radium Hospital guidelines are to
proceed with caution and only women with early stage BOT are permitted to be treated with IVF drugsThe latest development regarding reproduction and BOT is cryopreservation 86 Women who have
their ovaries removed because of large stage Ib BOT now have a possibility of becoming pregnant
Biopsies from normal ovarian cortex can be taken during the primary operation In 2004 a live birth
after a fresh ovarian tissue transplant in a primate was reported87 Donnez et al86 described in 2004
a live birth after orthotopic auto-transplantation of cryopreserved ovarian tissue Their1047297ndings opened
new possibilities for young women facing premature ovarian failure
Women with reduced fertility after surgery can consider ovarian stimulation egg retrieval and egg
freezing Ovarian stimulation and exposure to high oestrogen exposure do not seem to increase the risk
for recurrence Nor do pregnancies have negative in1047298uence on survival7277
To assure future fertility preservation in women with BOT the gynaecologic oncologist should
collaborate closely with the reproductive endocrinologists even before surgery Until more mature dataexist the general recommendation is a limited number of stimulation cycles only for stage I patients In
case of bilateral salpingo-oophorectomy cryopreservation of ovarian cortex biopsy from the less
affected ovary could be considered although this is not always technically possible1151
Follow up
Follow up should be long term and lifelong because recurrences may develop after more than 15 years
In conservatively treated womenclose follow up is crucial with special attentionto theremainingovaryIt
is still debated if the remaining ovary (and uterus) should be removed after the family is completed For
low-risk BOT there is no indication for this procedure but in women with high-risk of recurrence the
procedure is optional the alternative being to wait until recurrence or carry out radical surgery Manywomen will choose radical surgery when the family is completed because of psychological stress
The general recommendation is follow up every 3 months during the 1047297rst 2 years and then every 6
months for the next 3 years and annually thereafter The women is followed with pelvic examination
transvaginal ultrasound and calcium 125 measurement1451 (Fig 2)
Future direction of borderline ovarian tumour
A key issue for future research on BOTconcerning epidemiology is the identi1047297cation of risk factors for
invasive implants recurrences and death and also the identi1047297cation of predisposing heritable factors
For clinical management improved methods for preoperative and intraoperative diagnosis should
be considered in addition to the role of laparoscopic surgery in removal of complex cysts improvedmethods for distinguishing metastases from BOT and determination of risk associated with conser-
vative treatment
For pathology and molecular biology molecular studies are needed to assess the relationship
between serous BOT low-grade serous carcinoma and high-grade serous carcinoma Molecular studies
are also needed to aid in the characterisation of implants and studies need to be conducted to
determine the biology of microinvasive BOT and the clinical signi1047297cance of long-term follow up
Conclusion
Borderline ovarian tumours are ovarian tumours with good prognosis that account for 10ndash20 of all
epithelial ovarian cancer Historically standard primarysurgeryincludedbilateral salpingo-oophorectomyomentectomy peritoneal washing and complete peritoneal resection of macroscopic lesions or multiple
biopsies In cases of M-BOT women are also treated with appendectomy As one-third of BOT are diagnosed
inwomenyounger than40 years however fertility-sparingtreatment (ie preservation of the uterus andat
least part of one ovary) has been increasingly used in the past 10 years Fertility drugs are well tolerated in
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336332
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 912
women with infertility after fertility-sparing surgery Careful selection of candidates is necessary Lapa-
roscopic techniques can be used but are reserved for oncologic surgeons This conservative treatment
increases therateof recurrencebutwithoutany effecton survivalThespontaneouspregnancy rate is nearly
50and most are achieved spontaneously Spontaneous pregnancy can occurafter conservative treatment
of advanced-stage BOT (with non-invasive implants) These women should be closely followed up Further
research has to concentrate on clinical risk-factors histopathological markers and pathogenesis to guar-antee the best clinical management for women with BOT
Con1047298ict of interest statement
None declared
Practice points
BOTare ovarian tumours with good prognosis that account for 10ndash20 of all epithelial ovarian
cancer Historically standard primary surgery included bilateral salpingo-oophorectomy omentec-
tomy peritoneal washing and complete peritoneal resection of macroscopic lesions or
multiple biopsies
In case of mucinous BOT women are also treated with appendectomy
Adjuvant therapy for the treatment of BOT has no proven bene1047297t
As one-third of BOT are diagnosed in women younger than 40 years fertility-sparing treat-
ment (ie preservation of the uterus and at least part of one ovary) has been increasingly used
in the past 10 years
Fertility drugs are well tolerated in women with infertility after fertility-sparing surgery
Careful selection of candidates is necessary
Laparoscopic techniques can be used but are reserved for oncologic surgeons Spontaneous pregnancy can occur after conservative treatment of advanced stage BOT (with
non-invasive implants)
These women should be closely followed up
Research agenda
Epidemiology
Identify risk factors for invasive implants recurrences and death
Identify predisposing heritable factors
Clinical management
Improve methods for preoperative and intraoperative diagnosis
Further explore the role of laparoscopic surgery in the removal of complex cysts
Improve methods for distinguishing metastases from BOTand determine risk associated with
conservative treatment
Pathology and molecular biology
Conduct molecular studies to assess the relationship between serous BOT low-grade serous
carcinoma and high-grade serous carcinoma Conduct molecular studies to aid in the characterisation of implants
Conduct studies to determine the biology of microinvasive BOTand the clinical signi1047297cance of
long-term follow up
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 333
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1012
Acknowledgement
We wish to thank Mrs Gry Seppola for technical assistance and gratefully acknowledge the1047297nancial
support from the Inger and John Fredriksen Foundation for Ovarian Cancer Research
References
1 Taylor HC Malignant and semi-malignant tumors of the ovary Surg Gynecol Obstet 1929 48 204ndash2302 Kottmeier HL Kolstad P McGarrity KA Annual report on results of treatment in gynaecologic cancer vol 17 Statements of
results obtained in 1969ndash1972 inclusive FIGO Stockholm Sweden Editorial of 1047297ce Radiumhemmet 19733 Serov SF Scully RE amp Sobin LH International histological classi 1047297cation of tumors no 9 Histoloigcal typing of ovarian tumours
Geneval World Health Organization 19734 Hart WR amp Norris HJ Borderline and malignant mucinous tumors of the ovary Histologic criteria and clinical behavior
Cancer 1973 31 1031ndash10455 Scully RE Tumors of the ovary and maldeveloped gonads Fascicle 16 In Atlas of tumor pathology Second series Wash-
ington DC Armed Forces Institute of Pathology 1979 pp 75ndash906 Lenhard MS Mitterer S Kuumlmper C et al Long-term follow-up after ovarian borderline tumor relapse and survival in
a large patient cohort Eur J Obstet Gynecol Reprod Biol 2009 145 189ndash194
7 Quirk JT amp Natarajan N Ovarian cancer incidence in the United States 1992ndash
1999 Gynecol Oncol 2005 97 519ndash
5238 Kaern J Tropeacute CG amp Abeler VM A retrospective study of 370 borderline tumors of the ovary treated at the NorwegianRadium Hospital from 1970 to 1982 A review of clinicopathologic features and treatment modalities Cancer 1993 711810ndash1820
9 Bjoslashrge T Engeland A Hansen S et al Trends in the incidence of ovarian cancer and borderline tumours in Norway1954ndash1993 Int J Cancer 1997 71 780ndash786
10 Skiacuternisdoacutettir I Garmo H Wilander E et al Borderline ovarian tumors in Sweden 1960ndash2005 trends in incidence and age atdiagnosis compared to ovarian cancer Int J Cancer 2008 123 1897ndash1901
11 Trillsch F Mahner S Ruetzel J et al Clinical management of borderline ovarian tumors Expert Rev Anticancer Ther 2010 101115ndash1124
12 Sherman ME Mink PJ Curtis R et al Survival among women with borderline ovarian tumors and ovarian carcinomaa population-based analysis Cancer 2004 100 1045ndash1052
13 Kramer JL Greene MH Epidemiology of ovarian fallopian tube and primary peritoneal cancer In Gershenson DMMcGuire WP Gore M et al eds Gynecologic cancer Controversies in management 1st ed Philadelphia Elsevier ChurchillLivingstone 2004 pp 327ndash340
14 Tropeacute C Davidson B Paulsen T et al Diagnosis and treatment of borderline ovarian neoplasms lsquothe state of the artrsquo Eur J Gynaecol Oncol 2009 30 471ndash482
15 Kurman RJ amp Shih IeM Pathogenesis of ovarian cancer lessons from morphology and molecular biology and their clinicalimplications Int J Gynecol Pathol 2008 27 151ndash160
16 Kurman RJ Visvanathan K Roden R et al Early detection and treatment of ovarian cancer shifting from early stage tominimal volume of disease based on a new model of carcinogenesis Am J Obstet Gynecol 2008 198 351ndash356
17 Shih IeM amp Kurman RJ Ovarian tumorigenesis a proposed model based on morphological and molecular genetic analysis Am J Pathol 2004 164 1511ndash1518
18 Levanon K Crum C amp Drapkin R New insights into the pathogenesis of serous ovarian cancer and its clinical impact J ClinOncol 2008 26 5284ndash5293
19 Meinhold-Heerlein I Bauerschlag D Hilpert F et al Molecular and prognostic distinction between serous ovarian carci-nomas of varying grade and malignant potential Oncogene 2005 24 1053ndash1065
20 Bonome T Lee JY Park DC et al Expression pro1047297ling of serous low malignant potential low-grade and high-grade tumorsof the ovary Cancer Res 2005 65 10602ndash10612
21 Mahner S Baasch C Schwarz J et al C-Fos expression is a molecular predictor of progression and survival in epithelialovarian carcinoma Br J Cancer 2008 99 1269ndash1275
22 Ortiz BH Ailawadi M Colitti C et al Second primary or recurrence Comparative patterns of p53 and K-ras mutationssuggest that serous borderline ovarian tumors and subsequent serous carcinomas are unrelated tumors Cancer Res 200161 7264ndash7267
23 Lee KR Tavassoli FA Prat J et al Tumours of the ovary and peritoneum In Tavassoli FA amp Devilee P (eds) Pathology and
genetics Tumours of the breast and female genital organs Lyon IARC Press 2003 pp 113ndash20224 Oedegaard E Ovarian carcinomas and borderline ovarian tumors - molecular markers and operative treatment Dissertation
Facutly of Medicine University of Oslo 200825 Mok SC Bell DA Knapp RC et al Mutation of K-ras protooncogene in human ovarian epithelial tumors of borderline
malignancy Cancer Res 1993 53 1489ndash149226 du Bois A Ewald-Riegler N du Bois O et al Borderline tumors of the ovary a systematic review [German] Geburtsh
Frauenheilk 2009 69 807ndash83327 Seidman JD Horkayne-Szakaly I Haiba M et al The histologic type and stage distribution of ovarian carcinomas of surface
epithelial origin Int J Gynecol Pathol 2004 23 41ndash44
28 Prat J amp De Nictolis M Serous borderline tumors of the ovary a long-term follow-up study of 137 cases including 18 witha micropapillary pattern and 20 with microinvasion Am J Surg Pathol 2002 26 1111ndash1128
29 Bell DA Weinstock MA amp Scully RE Peritoneal implants of ovarian serous borderline tumors Histologic features andprognosis Cancer 1988 62 2212ndash2222
30 Tinelli R Tinelli A Tinelli FG et al Conservative surgery for borderline ovarian tumors a review Gynecol Oncol 2006 100
185ndash191
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336334
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1112
31 Kurman RJ amp Trimble CL The behavior of serous tumors of low malignant potential are they ever malignant Int J Gynecol
Pathol 1993 12 120ndash12732 Morice P Camatte S Rey A et al Prognostic factors for patients with advanced stage serous borderline tumours of the
ovary Ann Oncol 2003 14 592ndash59833 Bradley RF Stewart 4th JH Russell GB et al Pseudomyxoma peritonei of appendiceal origin a clinicopathologic analysis of
101 patients uniformly treated at a single institution with literature review Am J Surg Pathol 2006 30 551ndash559
34 Silva EG Gershenson DM Malpica A et al The recurrence and the overall survival rates of ovarian serous borderlineneoplasms with noninvasive implants is time dependent Am J Surg Pathol 2006 30 1367ndash137135 Seidman JD amp Kurman RJ Ovarian serous borderline tumors a critical review of the literature with emphasis on prognostic
indicators Hum Pathol 2000 31 539ndash55736 Chang SJ Ryu HS Chang KH et al Prognostic signi1047297cance of the micropapillary pattern in patients with serous borderline
ovarian tumors Acta Obstet Gynecol Scand 2008 87 476ndash48137 Fox H amp Wells M Surface epithelialstromal tumors of the ovary In Fox H amp Wells M (eds) Haines and Taylor Obstetrical and
Gynaecological Pathology 5th ed London Churchill Livingstone 2003 pp 713ndash74338 Ren J Peng Z amp Yang K A clinicopathologic multivariate analysis affecting recurrence of borderline ovarian tumors Gynecol
Oncol 2008 110 162ndash16739 Longacre TA McKenney JK Tazelaar HD et al Ovarian serous tumors of low malignant potential (borderline tumors)
outcome-based study of 276 patients with long-term (gt or frac145-year) follow-up Am J Surg Pathol 2005 29 707ndash72340 Cusidoacute M Balagueroacute L Hernandez G et al Results of the national survey of borderline ovarian tumors in Spain Gynecol
Oncol 2007 104 617ndash62241 Kaern J Tropeacute CG Kristensen GB et al DNA ploidy the most important prognostic factor in patients with borderline
tumors of the ovary Int J Gynecol Cancer 1993 3 349ndash35842 Meyer JS Gersell DJ amp Yim S Cell proliferation in ovarian carcinoma superior accuracy of S-phase fraction (SPF) by DNA
labeling index versus 1047298ow cytometric SPF lack of independent prognostic power for SPF and DNA ploidy and limitedeffect of SPF on tumor growth rate Gynecol Oncol 2001 81 466ndash476
43 Verbruggen MB van Diest PJ Baak JP et al The prognostic and clinical value of morphometry and DNA cytometry inborderline ovarian tumors a prospective study Int J Gynecol Pathol 2009 28 35ndash40
44 Yokoyama Y Moriya T Takano T et al Clinical outcome and risk factors for recurrence in borderline ovarian tumours Br J Cancer 2006 94 1586ndash1591
45 Leake JF Rader JS Woodruff JD et al Retroperitoneal lymphatic involvement with epithelial ovarian tumors of lowmalignant potential Gynecol Oncol 1991 42 124ndash130
46 Paulsen T Kaern J Kjaerheim K et al Symptoms and referral of women with epithelial ovarian tumors Int J Gynaecol Obstet 2005 88 31ndash37
47 Paulsen T Epithelial ovarian cancer A clinical epidemiological approach on diagnosis and treatment Dissertation Faculty of Medicine University of Oslo 2007
48 Tropeacute CG Kristensen G amp Makar A Surgery for borderline tumor of the ovary Semin Surg Oncol 2000 19 69ndash7549 Tempfer CB Polterauer S Bentz EK et al Accuracy of intraoperative frozen section analysis in borderline tumors of the
ovary a retrospective analysis of 96 cases and review of the literature Gynecol Oncol 2007 107 248ndash25250 Camatte S Morice P Thoury A et al Impact of surgical staging in patients with macroscopic lsquostage Irsquo ovarian borderline
tumours analysis of a continuous series of 101 cases Eur J Cancer 2004 40 1842ndash184951 Cadron I Leunen K Van Gorp T et al Management of borderline ovarian neoplasms J Clin Oncol 2007 25 2928ndash293752 Snider DD Stuart GC Nation JG et al Evaluation of surgical staging in stage I low malignant potential ovarian tumors
Gynecol Oncol 1991 40 129ndash13253 Ronnett BM Kurman RJ Zahn CM et al Pseudomyxoma peritonei in women a clinicopathologic analysis of 30 cases with
emphasis on site of origin prognosis and relationship to ovarian mucinous tumors of low malignant potential Hum Pathol
1995 26 509ndash52454 Seidman JD Elsayed AM Sobin LH et al Association of mucinous tumors of the ovary and appendix A clinicopathologic
study of 25 cases Am J Surg Pathol 1993 17 22ndash3455 Trimble EL amp Trimble LC Epithelial ovarian tumors of low malignant potential In Markman M amp Hoskins W (eds) Cancer
of the Ovary New York Raven Press 1993 pp 415ndash429
56 Zanetta G Rota S Chiari S et al Behavior of borderline tumors with particular interest to persistence recurrence andprogression to invasive carcinoma a prospective study J Clin Oncol 2001 19 2658ndash266457 Fauvet R Boccara J Dufournet C et al Restaging surgery for women with borderline ovarian tumors results of a French
multicenter study Cancer 2004 100 1145ndash115158 Zapardiel I Rosenberg P Peiretti M et al The role of restaging borderline ovarian tumors single institution experience and
review of the literature Gynecol Oncol 2010 119 274ndash27759 Def 1047297eux X Morice P Camatte S et al Results after laparoscopic management of serous borderline tumor of the ovary with
peritoneal implants Gynecol Oncol 2005 97 84ndash8960 Fauvet R Boccara J Dufournet C et al Laparoscopic management of borderline ovarian tumors results of a French
multicenter study Ann Oncol 2005 16 403ndash41061 Vandenput I Amant F amp Vergote I Peritoneal recurrences might be less common in advanced stage serous borderline
ovarian tumors that were treated by laparotomy Gynecol Oncol 2005 98 52362 CadronI Amant F VanGorp Tet alThe management of borderline tumours of theovary Curr Opin Oncol 2006 18 488ndash49363 Vergote I De Brabanter J Fyles A et al Prognostic importance of degree of differentiation and cyst rupture in stage I
invasive epithelial ovarian carcinoma Lancet 2001 357 176ndash182
64 Gershenson DM amp Silva EG Serous ovarian tumors of low malignant potential with peritoneal implants Cancer 1990 65578ndash585
65 Gershenson DM Clinical management potential tumours of low malignancy Best Pract Res Clin Obstet Gynaecol 2002 16513ndash527
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 335
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1212
66 Heintz AP Odicino F Maisonneuve P et al Carcinoma of the ovary FIGO 26th Annual Report on the Results of Treatment inGynecological Cancer Int J Gynaecol Obstet 2006 95(Suppl 1) S161ndashS192
67 Bjoslashrge T Engeland A Hansen S et al Prognosis of patients with ovarian cancer and borderline tumours diagnosed inNorway between 1954 and 1993 Int J Cancer 1998 75 663ndash670
68 Seidman JD amp Kurman RJ Subclassi1047297cation of serous borderline tumors of the ovary into benign and malignant typesA clinicopathologic study of 65 advanced stage cases Am J Surg Pathol 1996 20 1331ndash1345
69 Sherman ME Berman J Birrer MJ et al Current challenges and opportunities for research on borderline ovarian tumorsHum Pathol 2004 35 961ndash97070 Leake JF Currie JL Rosenshein NB et al Long-term follow-up of serous ovarian tumors of low malignant potential Gynecol
Oncol 1992 47 150ndash15871 Lim-Tan SK Cajigas HE amp Scully RE Ovarian cystectomy for serous borderline tumors a follow-up study of 35 cases Obstet
Gynecol 1988 72 775ndash78172 Morice P Camatte S El Hassan J et al Clinical outcomes and fertility after conservative treatment of ovarian borderline
tumors Fertil Steril 2001 75 92ndash9673 Camatte S Morice P Pautier P et al Fertility results after conservative treatment of advanced stage serous borderline
tumour of the ovary BJOG 2002 109 376ndash38074 Crispens MA Bodurka D Deavers M et al Response and survival in patients with progressive or recurrent serous ovarian
tumors of low malignant potential Obstet Gynecol 2002 99 3ndash1075 Fauvet R Poncelet C Boccara J et al Fertility after conservative treatment for borderline ovarian tumors a French
multicenter study Fertil Steril 2005 83 284ndash29076 Morris RT Gershenson DM Silva EG et al Outcome and reproductive function after conservative surgery for borderline
ovarian tumors Obstet Gynecol 2000 95 541ndash54777 Gotlieb WH Flikker S Davidson B et al Borderline tumors of the ovary fertility treatment conservative management and
pregnancy outcome Cancer 1998 82 141ndash14678 Maltaris T Boehm D Dittrich R et al Reproduction beyond cancer a message of hope for young women Gynecol Oncol
2006 103 1109ndash112179 Beiner ME Gotlieb WH Davidson B et al Infertility treatment after conservative management of borderline ovarian
tumors Cancer 2001 92 320ndash32580 Fasouliotis SJ Davis O Schattman G et al Safety and ef 1047297cacy of infertility treatment after conservative management of
borderline ovarian tumors a preliminary report Fertil Steril 2004 82 568ndash57281 Kashyap S amp Davis OK Ovarian cancer and fertility medications a critical appraisal Semin Reprod Med 2003 21 65ndash7182 Morice P Camatte S Wicart-Poque F et al Results of conservative management of epithelial malignant and borderline
ovarian tumours Hum Reprod Update 2003 9 185ndash19283 Whittemore AS Harris R amp Itnyre J Characteristics relating to ovarian cancer risk collaborative analysis of 12 US case-
control studies II Invasive epithelial ovarian cancers in white women Collaborative Ovarian Cancer Group Am J Epi-demiol 1992 136 1184ndash1203
84 Fortin A Morice P Thoury A et al Impact of infertility drugs after treatment of borderline ovarian tumors results of a retrospective multicenter study Fertil Steril 2007 87 591ndash596
85 Burger CW van de Swaluw A Mooij TM et al Risk of borderline and invasive ovarian tumors after ovarian stimulation forin vitro fertilization in a large Dutch cohort after 15 years of follow-up Abstracts presented for the 40th Annual Meeting of the Society of Gynecologic Oncologists February 2009 (abstract no 6) Gynecol Oncol 2009 112(Suppl) S4
86 Donnez J Dolmans MM Demylle D et al Livebirth after orthotopic transplantation of cryopreserved ovarian tissue Lancet 2004 364 1405ndash1410
87 Lee DM Yeoman RR Battaglia DE et al Live birth after ovarian tissue transplant Nature 2004 428 137ndash138
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336336

7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 512
surgery Another common event is that malignancy is not suspected at the initial operation and therefore
the abdomen is not properly explored Should this woman undergo re-operation Snider et al52 upstaged
1047297ve out of 27 women with stage I disease None of the 12 women with mucinous BOT were upstaged
whereas1047297veoutof 13 women with serous BOTwere upstagedMucinousBOTgrossly con1047297ned to one ovary
are probably unlikely to be upstaged at a restaging procedure If evidence of extra-ovarian disease exists
complete surgical staging and appendectomy are indicated Mucinous BOT with abdominal spread are in50 claimed to arise in the appendix or simultaneously in one or both ovaries5354 For serous BOT it is
reasonable to do a second operation as lymph-node involvement has been reported in about 20 in
apparentstage I tumourswitheven higher incidence in more advanced stages45 At the Norwegian Radium
Hospital we recommend restaging if the women are insuf 1047297ciently staged at primary operation in agree-
ment with Cadron et al51 and Trimble and Trimble55 We also believe that the decision to restage must be
individualised taking into consideration the adequacy of the previous abdominal exploration the tumour
subtype and potential treatment of residual disease as well as thelevel of concern for both thewomanand
the clinician even if there is little proof that restaging operations have an effect on survival115056ndash58
Laparoscopy
Laparoscopic treatment has become an attractive approach for benign ovarian tumours (pelvic
mass) The development of the laparoscopic techniques with the use of endo-bag gives less risk of
spillage during surgery and less port-side metastases For conservatively treated women wishing to
preserve fertility this is a more favourable approach and has short postoperative recovery fewer
adhesions and improved cosmetic results59 Cyst rupture and incomplete staging occur signi1047297cantly
more frequently by laparoscopy compared with laparotomy (339 v 124)6061 but do not in1047298uence
survival The laparoscopic treatment may result in higher recurrence rate which must be discussed
with the woman The woman should agree to close follow up and repeated surgery5162 Other concerns
are port metastases63 and improper staging61
Postoperative treatment of borderline ovarian tumours
Today there is no proven bene1047297t from adjuvant therapy (chemotherapy or radiotherapy) even in
advanced stage disease and in the presence of invasive implants1432 No randomised-controlled studies
Fig 2 Recommendation treatmentof borderline ovarian tumours Modi1047297ed fromTrillsch et al11 and Cadron et al51 with permission
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 329
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 612
have evaluated the ef 1047297cacy of chemotherapy in advanced stage BOT with residual disease Cisplatin-
based therapy in serous BOT with residual disease have shown high response rates but modest
effect on long-term survival1464 In case of recurrences where transformation to an invasive histology
has occurred consideration of platinum-taxane-based chemotherapy is reasonable The molecular
changes transforming BOT to invasive ovarian carcinoma may be clari1047297ed in the future with the
possibility of blocking the different lsquostepsrsquo in the carcinogenesis Today we know that both serous BOTand low-grade serous carcinoma frequently present with B-raf and K-ras mutations11
Survival
Overall survival for women with BOT is excellent 90ndash100 in most reports depending on age at
diagnosis FIGO stage and histologic type112651626566 Trillsch et al11 reported a 5-year overall survival
rate of almost 100 in early stage disease (FIGO I-II) and between 86 and 92 in more advanced
disease (FIGO III-IV) In a Norwegian population-based study67 the age-adjusted 1- 3- 5- and 10-year
relative survival rates of women with mucinous BOT were 98 97 97 and 95 respectively and for
women with serous BOT 96 93 90 and 90 respectively The relative risk of dying increased with
higher age at diagnosis The 5-year relative survival for women aged between 0 and 44 years was 99compared with 85 for women aged 75ndash89 years Nearly the same 1047297gures are reported by Sherman
et al12 with better survival for younger women and slightly better survival for serous tumours
compared with mucinous tumours although mucinous tumours in advanced stage had the poorest
long-term survival (855)12
Seidman and Kurman35 summarised 97 reports including a total of 4129 women with serous BOT
and showed a disease-speci1047297c survival rate of 99 for stage I disease and 953 for stage III disease
(mean follow up of 7 years)35 The 5-year survival was 98 for women with serous BOT with non-
invasive implants and 33 for those with invasive implants68
Conservative surgery
The median age of diagnosis for women with BOT is 40 years and nearly one-third are younger than
40 years Thus preservation of childbearing potential is an important issue for many of these women
To select women for fertility-sparing surgery without risk of reduced long-term survival is a challenge
for the gynaecologic oncologist3069 (Fig 2) Conservative surgery is de1047297ned as complete staging in
which the uterus and at least a part of one ovary are preserved1162 (Fig 2)
Although the standard treatment for all women with BOT is at least bilateral salpingo-
oophorectomy many young women with stage Ia tumours who have not completed childbearing
can be safely treated with unilateral salpingo-oophorectomy after comprehensive surgical staging
thereby preserving the fertility potential At least as important as the fertility issue however is
whether we can reduce the morbidity caused by radical surgery and whether a more conservative
approach is a safe alternative regarding cancer prognosis51
Recent studies from the Norwegian RadiumHospital8 and Gynecologic Oncology Group65 have shown that preservation of reproductive organs is
feasible Relapse rates after bilateral salpingo-oophorectomy range between 0 and 20 This rate
varies between 12 and 58 for cystectomy and between 25 and 57 for radical surgery Relapses
can also occur late and recurrences as late as 39 years after initial treatment have been reported5134
Predictors of relapse are resection margins containing tumour cells70 The frequency of persistence or
recurrence in 35 patients with serous-BOT treated by unilateral cystectomy bilateral cystectomy or
unilateral cystectomy with contralateral oophorectomy or salpingo-oophorectomy was retrospectively
investigated by Lim-Tan et al71 Conservative surgical treatment was carried out either because the
women were young and wanted to preserve their fertility or because the nature of the tumour was not
determined at the time of surgery Thirty-three women had stage I disease (19 stage Ia 10 stage Ib and
four stage Ic) and two had stage III disease Although 60 of the women had additional and in somecases de1047297nitive operations within relative short periods after initial cystectomy or cystectomies 21 had
conservation of ovarian tissue and were followed on average for 75 years All women with stage I
disease were alive without evidence of disease after surgical treatment alone The presence of
persistent or recurrent disease correlated with multifocality and involvement of resection margins
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336330
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 712
Multifocality may be a strong predictor of failure of cystectomy to control the disease No recurrence of
disease was seen in ovaries from which a single cyst had been removed with negative resection
margins Extensive sampling of the resection margins of ovarian cysts is important71
For many women with BOT fertility is an important issue It is therefore essential to discuss with
these young women the advantages and disadvantages between conservative and radical surgery
Conservative surgery preserves fertility and hormonal function but unfortunately with high risk of recurrence
In women with obvious stage I disease unilateral salpingo-oophorectomy or cystectomy has from
previous studies been shown to be safe This has also been con1047297rmed for women with advanced-stage
disease on the assumption of close follow up
Even for women with advanced disease conservative surgery might be considered after informed
consent The recurrence rate is high and invasive and even non-invasive implants may recur up to 15
as invasive OC without negative in1047298uence on survival34567273
Treatment at recurrent disease after conservative treatment
Early detected recurrences are curable with repeated surgery113451 and therefore conservativetreatment might again be considered in women with recurrent disease if fertility still is an issue and the
woman is informed about the high risk of recurrence and agrees on close follow up accepting repeated
surgery5162 If invasive implants are diagnosed this procedure could not be recommended In any case
of recurrent disease secondary debulking surgery is important as women suboptimally debulked have
poor survival115174
Fertility after conservative management of borderline ovarian tumour
Infertility is frequently observed inwomen with BOT A history of infertility beforediagnosis has been
reported in 10ndash35 of women75ndash77 To allow conservative surgery careful evaluation of the extent of
disease by the gynaecologist at the time of operation and meticulous examination of the cystectomyspecimen by the gynaecologist and pathologist are desirable to determine the prognosis after cys-
tectomy In a study by Morris et al76 onewoman who had disease-related deathwasnot staged properly
In a meta-analysis by Maltaris et al78 1483 women had BOT of whom 656 were treated conservatively
(442) A total of 196 women became pregnant and 111 relapsed after unilateral salpingo-
oophorectomy only one woman died from the disease (015) The investigators therefore suggest
that conservative surgery is justi1047297able for some women with a good prognostic index Unilateral
oophorectomy omentectomy and appendectomy in stage Ia diploid mucinous BOT are indicated for
young women who wish to preservefertility (Fig 2) In stage Ia diploid serous BOT thesame procedure is
safe if the contralateral ovary is macroscopically normal Careful inspection of a macroscopically normal
contralateral ovary should be suf 1047297cient inyoung womenwith stageIa disease who wish to remainfertile
Surgery itself can impair the fertility function by loss of ovarian tissue pelvic scarring and adhesionsblocking the fallopian tube Post-surgery fertility factors such as ovulation fallopian tubes and sperm
factors should be investigated and treated if necessary About one-third of women undergoing
conservative surgery for BOT will be able to conceive with no negative in1047298uence of pregnancy on the
disease60727779 Ovulation induction is often required in order to conceive80 The role of ovulation
(in-vitro [IVF] fertilisation) drugs in BOT is currently under debate7780ndash84
Recently a large nationwide cohort study of 19146 subfertile women in the Netherlands who
received IVF drugs between 1983 and 1995 and a comparison group of 6953 subfertile women who
were not treated was published After a median follow up of 15 years a total of 77 ovarian malignancies
were observed in the cohort including 42 women with epithelial ovarian cancer and 35 women with
BOT Sixty-one ovarian malignancies were observed in the IVF-group and 16 in the unexposed (control)
group The ratio hazard for epithelial ovarian cancer and BOT was 167 (074 to 375) and 425 (127 to1418) respectively85 The conclusion of Burger et al85 was that IVF increases the risk of BOT
A worrying1047297nding of their study is the increased risk of epithelial ovarian cancer and BOT even after 15
years of follow up Fasouliotis et al80 found no perceptible negative effect of previous BOT on preg-
nancy rates after IVF The same was shown by Fortin et al84 in a study of 30 women treated with IVF
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 331
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 812
drugs for infertility after conservative surgery Thirteen pregnancies were observed Disease in four
women recurred All recurrences were BOT on a remaining ovary that had been treated by surgery
alone All women are currently disease-free after secondary surgery Fortin et al84 concluded that IVF
drugs can be used safely in womenwho develop infertility after conservative treatment of BOT Because
of the low number of women treated with IVF drugs Norwegian Radium Hospital guidelines are to
proceed with caution and only women with early stage BOT are permitted to be treated with IVF drugsThe latest development regarding reproduction and BOT is cryopreservation 86 Women who have
their ovaries removed because of large stage Ib BOT now have a possibility of becoming pregnant
Biopsies from normal ovarian cortex can be taken during the primary operation In 2004 a live birth
after a fresh ovarian tissue transplant in a primate was reported87 Donnez et al86 described in 2004
a live birth after orthotopic auto-transplantation of cryopreserved ovarian tissue Their1047297ndings opened
new possibilities for young women facing premature ovarian failure
Women with reduced fertility after surgery can consider ovarian stimulation egg retrieval and egg
freezing Ovarian stimulation and exposure to high oestrogen exposure do not seem to increase the risk
for recurrence Nor do pregnancies have negative in1047298uence on survival7277
To assure future fertility preservation in women with BOT the gynaecologic oncologist should
collaborate closely with the reproductive endocrinologists even before surgery Until more mature dataexist the general recommendation is a limited number of stimulation cycles only for stage I patients In
case of bilateral salpingo-oophorectomy cryopreservation of ovarian cortex biopsy from the less
affected ovary could be considered although this is not always technically possible1151
Follow up
Follow up should be long term and lifelong because recurrences may develop after more than 15 years
In conservatively treated womenclose follow up is crucial with special attentionto theremainingovaryIt
is still debated if the remaining ovary (and uterus) should be removed after the family is completed For
low-risk BOT there is no indication for this procedure but in women with high-risk of recurrence the
procedure is optional the alternative being to wait until recurrence or carry out radical surgery Manywomen will choose radical surgery when the family is completed because of psychological stress
The general recommendation is follow up every 3 months during the 1047297rst 2 years and then every 6
months for the next 3 years and annually thereafter The women is followed with pelvic examination
transvaginal ultrasound and calcium 125 measurement1451 (Fig 2)
Future direction of borderline ovarian tumour
A key issue for future research on BOTconcerning epidemiology is the identi1047297cation of risk factors for
invasive implants recurrences and death and also the identi1047297cation of predisposing heritable factors
For clinical management improved methods for preoperative and intraoperative diagnosis should
be considered in addition to the role of laparoscopic surgery in removal of complex cysts improvedmethods for distinguishing metastases from BOT and determination of risk associated with conser-
vative treatment
For pathology and molecular biology molecular studies are needed to assess the relationship
between serous BOT low-grade serous carcinoma and high-grade serous carcinoma Molecular studies
are also needed to aid in the characterisation of implants and studies need to be conducted to
determine the biology of microinvasive BOT and the clinical signi1047297cance of long-term follow up
Conclusion
Borderline ovarian tumours are ovarian tumours with good prognosis that account for 10ndash20 of all
epithelial ovarian cancer Historically standard primarysurgeryincludedbilateral salpingo-oophorectomyomentectomy peritoneal washing and complete peritoneal resection of macroscopic lesions or multiple
biopsies In cases of M-BOT women are also treated with appendectomy As one-third of BOT are diagnosed
inwomenyounger than40 years however fertility-sparingtreatment (ie preservation of the uterus andat
least part of one ovary) has been increasingly used in the past 10 years Fertility drugs are well tolerated in
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336332
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 912
women with infertility after fertility-sparing surgery Careful selection of candidates is necessary Lapa-
roscopic techniques can be used but are reserved for oncologic surgeons This conservative treatment
increases therateof recurrencebutwithoutany effecton survivalThespontaneouspregnancy rate is nearly
50and most are achieved spontaneously Spontaneous pregnancy can occurafter conservative treatment
of advanced-stage BOT (with non-invasive implants) These women should be closely followed up Further
research has to concentrate on clinical risk-factors histopathological markers and pathogenesis to guar-antee the best clinical management for women with BOT
Con1047298ict of interest statement
None declared
Practice points
BOTare ovarian tumours with good prognosis that account for 10ndash20 of all epithelial ovarian
cancer Historically standard primary surgery included bilateral salpingo-oophorectomy omentec-
tomy peritoneal washing and complete peritoneal resection of macroscopic lesions or
multiple biopsies
In case of mucinous BOT women are also treated with appendectomy
Adjuvant therapy for the treatment of BOT has no proven bene1047297t
As one-third of BOT are diagnosed in women younger than 40 years fertility-sparing treat-
ment (ie preservation of the uterus and at least part of one ovary) has been increasingly used
in the past 10 years
Fertility drugs are well tolerated in women with infertility after fertility-sparing surgery
Careful selection of candidates is necessary
Laparoscopic techniques can be used but are reserved for oncologic surgeons Spontaneous pregnancy can occur after conservative treatment of advanced stage BOT (with
non-invasive implants)
These women should be closely followed up
Research agenda
Epidemiology
Identify risk factors for invasive implants recurrences and death
Identify predisposing heritable factors
Clinical management
Improve methods for preoperative and intraoperative diagnosis
Further explore the role of laparoscopic surgery in the removal of complex cysts
Improve methods for distinguishing metastases from BOTand determine risk associated with
conservative treatment
Pathology and molecular biology
Conduct molecular studies to assess the relationship between serous BOT low-grade serous
carcinoma and high-grade serous carcinoma Conduct molecular studies to aid in the characterisation of implants
Conduct studies to determine the biology of microinvasive BOTand the clinical signi1047297cance of
long-term follow up
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 333
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1012
Acknowledgement
We wish to thank Mrs Gry Seppola for technical assistance and gratefully acknowledge the1047297nancial
support from the Inger and John Fredriksen Foundation for Ovarian Cancer Research
References
1 Taylor HC Malignant and semi-malignant tumors of the ovary Surg Gynecol Obstet 1929 48 204ndash2302 Kottmeier HL Kolstad P McGarrity KA Annual report on results of treatment in gynaecologic cancer vol 17 Statements of
results obtained in 1969ndash1972 inclusive FIGO Stockholm Sweden Editorial of 1047297ce Radiumhemmet 19733 Serov SF Scully RE amp Sobin LH International histological classi 1047297cation of tumors no 9 Histoloigcal typing of ovarian tumours
Geneval World Health Organization 19734 Hart WR amp Norris HJ Borderline and malignant mucinous tumors of the ovary Histologic criteria and clinical behavior
Cancer 1973 31 1031ndash10455 Scully RE Tumors of the ovary and maldeveloped gonads Fascicle 16 In Atlas of tumor pathology Second series Wash-
ington DC Armed Forces Institute of Pathology 1979 pp 75ndash906 Lenhard MS Mitterer S Kuumlmper C et al Long-term follow-up after ovarian borderline tumor relapse and survival in
a large patient cohort Eur J Obstet Gynecol Reprod Biol 2009 145 189ndash194
7 Quirk JT amp Natarajan N Ovarian cancer incidence in the United States 1992ndash
1999 Gynecol Oncol 2005 97 519ndash
5238 Kaern J Tropeacute CG amp Abeler VM A retrospective study of 370 borderline tumors of the ovary treated at the NorwegianRadium Hospital from 1970 to 1982 A review of clinicopathologic features and treatment modalities Cancer 1993 711810ndash1820
9 Bjoslashrge T Engeland A Hansen S et al Trends in the incidence of ovarian cancer and borderline tumours in Norway1954ndash1993 Int J Cancer 1997 71 780ndash786
10 Skiacuternisdoacutettir I Garmo H Wilander E et al Borderline ovarian tumors in Sweden 1960ndash2005 trends in incidence and age atdiagnosis compared to ovarian cancer Int J Cancer 2008 123 1897ndash1901
11 Trillsch F Mahner S Ruetzel J et al Clinical management of borderline ovarian tumors Expert Rev Anticancer Ther 2010 101115ndash1124
12 Sherman ME Mink PJ Curtis R et al Survival among women with borderline ovarian tumors and ovarian carcinomaa population-based analysis Cancer 2004 100 1045ndash1052
13 Kramer JL Greene MH Epidemiology of ovarian fallopian tube and primary peritoneal cancer In Gershenson DMMcGuire WP Gore M et al eds Gynecologic cancer Controversies in management 1st ed Philadelphia Elsevier ChurchillLivingstone 2004 pp 327ndash340
14 Tropeacute C Davidson B Paulsen T et al Diagnosis and treatment of borderline ovarian neoplasms lsquothe state of the artrsquo Eur J Gynaecol Oncol 2009 30 471ndash482
15 Kurman RJ amp Shih IeM Pathogenesis of ovarian cancer lessons from morphology and molecular biology and their clinicalimplications Int J Gynecol Pathol 2008 27 151ndash160
16 Kurman RJ Visvanathan K Roden R et al Early detection and treatment of ovarian cancer shifting from early stage tominimal volume of disease based on a new model of carcinogenesis Am J Obstet Gynecol 2008 198 351ndash356
17 Shih IeM amp Kurman RJ Ovarian tumorigenesis a proposed model based on morphological and molecular genetic analysis Am J Pathol 2004 164 1511ndash1518
18 Levanon K Crum C amp Drapkin R New insights into the pathogenesis of serous ovarian cancer and its clinical impact J ClinOncol 2008 26 5284ndash5293
19 Meinhold-Heerlein I Bauerschlag D Hilpert F et al Molecular and prognostic distinction between serous ovarian carci-nomas of varying grade and malignant potential Oncogene 2005 24 1053ndash1065
20 Bonome T Lee JY Park DC et al Expression pro1047297ling of serous low malignant potential low-grade and high-grade tumorsof the ovary Cancer Res 2005 65 10602ndash10612
21 Mahner S Baasch C Schwarz J et al C-Fos expression is a molecular predictor of progression and survival in epithelialovarian carcinoma Br J Cancer 2008 99 1269ndash1275
22 Ortiz BH Ailawadi M Colitti C et al Second primary or recurrence Comparative patterns of p53 and K-ras mutationssuggest that serous borderline ovarian tumors and subsequent serous carcinomas are unrelated tumors Cancer Res 200161 7264ndash7267
23 Lee KR Tavassoli FA Prat J et al Tumours of the ovary and peritoneum In Tavassoli FA amp Devilee P (eds) Pathology and
genetics Tumours of the breast and female genital organs Lyon IARC Press 2003 pp 113ndash20224 Oedegaard E Ovarian carcinomas and borderline ovarian tumors - molecular markers and operative treatment Dissertation
Facutly of Medicine University of Oslo 200825 Mok SC Bell DA Knapp RC et al Mutation of K-ras protooncogene in human ovarian epithelial tumors of borderline
malignancy Cancer Res 1993 53 1489ndash149226 du Bois A Ewald-Riegler N du Bois O et al Borderline tumors of the ovary a systematic review [German] Geburtsh
Frauenheilk 2009 69 807ndash83327 Seidman JD Horkayne-Szakaly I Haiba M et al The histologic type and stage distribution of ovarian carcinomas of surface
epithelial origin Int J Gynecol Pathol 2004 23 41ndash44
28 Prat J amp De Nictolis M Serous borderline tumors of the ovary a long-term follow-up study of 137 cases including 18 witha micropapillary pattern and 20 with microinvasion Am J Surg Pathol 2002 26 1111ndash1128
29 Bell DA Weinstock MA amp Scully RE Peritoneal implants of ovarian serous borderline tumors Histologic features andprognosis Cancer 1988 62 2212ndash2222
30 Tinelli R Tinelli A Tinelli FG et al Conservative surgery for borderline ovarian tumors a review Gynecol Oncol 2006 100
185ndash191
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336334
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1112
31 Kurman RJ amp Trimble CL The behavior of serous tumors of low malignant potential are they ever malignant Int J Gynecol
Pathol 1993 12 120ndash12732 Morice P Camatte S Rey A et al Prognostic factors for patients with advanced stage serous borderline tumours of the
ovary Ann Oncol 2003 14 592ndash59833 Bradley RF Stewart 4th JH Russell GB et al Pseudomyxoma peritonei of appendiceal origin a clinicopathologic analysis of
101 patients uniformly treated at a single institution with literature review Am J Surg Pathol 2006 30 551ndash559
34 Silva EG Gershenson DM Malpica A et al The recurrence and the overall survival rates of ovarian serous borderlineneoplasms with noninvasive implants is time dependent Am J Surg Pathol 2006 30 1367ndash137135 Seidman JD amp Kurman RJ Ovarian serous borderline tumors a critical review of the literature with emphasis on prognostic
indicators Hum Pathol 2000 31 539ndash55736 Chang SJ Ryu HS Chang KH et al Prognostic signi1047297cance of the micropapillary pattern in patients with serous borderline
ovarian tumors Acta Obstet Gynecol Scand 2008 87 476ndash48137 Fox H amp Wells M Surface epithelialstromal tumors of the ovary In Fox H amp Wells M (eds) Haines and Taylor Obstetrical and
Gynaecological Pathology 5th ed London Churchill Livingstone 2003 pp 713ndash74338 Ren J Peng Z amp Yang K A clinicopathologic multivariate analysis affecting recurrence of borderline ovarian tumors Gynecol
Oncol 2008 110 162ndash16739 Longacre TA McKenney JK Tazelaar HD et al Ovarian serous tumors of low malignant potential (borderline tumors)
outcome-based study of 276 patients with long-term (gt or frac145-year) follow-up Am J Surg Pathol 2005 29 707ndash72340 Cusidoacute M Balagueroacute L Hernandez G et al Results of the national survey of borderline ovarian tumors in Spain Gynecol
Oncol 2007 104 617ndash62241 Kaern J Tropeacute CG Kristensen GB et al DNA ploidy the most important prognostic factor in patients with borderline
tumors of the ovary Int J Gynecol Cancer 1993 3 349ndash35842 Meyer JS Gersell DJ amp Yim S Cell proliferation in ovarian carcinoma superior accuracy of S-phase fraction (SPF) by DNA
labeling index versus 1047298ow cytometric SPF lack of independent prognostic power for SPF and DNA ploidy and limitedeffect of SPF on tumor growth rate Gynecol Oncol 2001 81 466ndash476
43 Verbruggen MB van Diest PJ Baak JP et al The prognostic and clinical value of morphometry and DNA cytometry inborderline ovarian tumors a prospective study Int J Gynecol Pathol 2009 28 35ndash40
44 Yokoyama Y Moriya T Takano T et al Clinical outcome and risk factors for recurrence in borderline ovarian tumours Br J Cancer 2006 94 1586ndash1591
45 Leake JF Rader JS Woodruff JD et al Retroperitoneal lymphatic involvement with epithelial ovarian tumors of lowmalignant potential Gynecol Oncol 1991 42 124ndash130
46 Paulsen T Kaern J Kjaerheim K et al Symptoms and referral of women with epithelial ovarian tumors Int J Gynaecol Obstet 2005 88 31ndash37
47 Paulsen T Epithelial ovarian cancer A clinical epidemiological approach on diagnosis and treatment Dissertation Faculty of Medicine University of Oslo 2007
48 Tropeacute CG Kristensen G amp Makar A Surgery for borderline tumor of the ovary Semin Surg Oncol 2000 19 69ndash7549 Tempfer CB Polterauer S Bentz EK et al Accuracy of intraoperative frozen section analysis in borderline tumors of the
ovary a retrospective analysis of 96 cases and review of the literature Gynecol Oncol 2007 107 248ndash25250 Camatte S Morice P Thoury A et al Impact of surgical staging in patients with macroscopic lsquostage Irsquo ovarian borderline
tumours analysis of a continuous series of 101 cases Eur J Cancer 2004 40 1842ndash184951 Cadron I Leunen K Van Gorp T et al Management of borderline ovarian neoplasms J Clin Oncol 2007 25 2928ndash293752 Snider DD Stuart GC Nation JG et al Evaluation of surgical staging in stage I low malignant potential ovarian tumors
Gynecol Oncol 1991 40 129ndash13253 Ronnett BM Kurman RJ Zahn CM et al Pseudomyxoma peritonei in women a clinicopathologic analysis of 30 cases with
emphasis on site of origin prognosis and relationship to ovarian mucinous tumors of low malignant potential Hum Pathol
1995 26 509ndash52454 Seidman JD Elsayed AM Sobin LH et al Association of mucinous tumors of the ovary and appendix A clinicopathologic
study of 25 cases Am J Surg Pathol 1993 17 22ndash3455 Trimble EL amp Trimble LC Epithelial ovarian tumors of low malignant potential In Markman M amp Hoskins W (eds) Cancer
of the Ovary New York Raven Press 1993 pp 415ndash429
56 Zanetta G Rota S Chiari S et al Behavior of borderline tumors with particular interest to persistence recurrence andprogression to invasive carcinoma a prospective study J Clin Oncol 2001 19 2658ndash266457 Fauvet R Boccara J Dufournet C et al Restaging surgery for women with borderline ovarian tumors results of a French
multicenter study Cancer 2004 100 1145ndash115158 Zapardiel I Rosenberg P Peiretti M et al The role of restaging borderline ovarian tumors single institution experience and
review of the literature Gynecol Oncol 2010 119 274ndash27759 Def 1047297eux X Morice P Camatte S et al Results after laparoscopic management of serous borderline tumor of the ovary with
peritoneal implants Gynecol Oncol 2005 97 84ndash8960 Fauvet R Boccara J Dufournet C et al Laparoscopic management of borderline ovarian tumors results of a French
multicenter study Ann Oncol 2005 16 403ndash41061 Vandenput I Amant F amp Vergote I Peritoneal recurrences might be less common in advanced stage serous borderline
ovarian tumors that were treated by laparotomy Gynecol Oncol 2005 98 52362 CadronI Amant F VanGorp Tet alThe management of borderline tumours of theovary Curr Opin Oncol 2006 18 488ndash49363 Vergote I De Brabanter J Fyles A et al Prognostic importance of degree of differentiation and cyst rupture in stage I
invasive epithelial ovarian carcinoma Lancet 2001 357 176ndash182
64 Gershenson DM amp Silva EG Serous ovarian tumors of low malignant potential with peritoneal implants Cancer 1990 65578ndash585
65 Gershenson DM Clinical management potential tumours of low malignancy Best Pract Res Clin Obstet Gynaecol 2002 16513ndash527
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 335
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1212
66 Heintz AP Odicino F Maisonneuve P et al Carcinoma of the ovary FIGO 26th Annual Report on the Results of Treatment inGynecological Cancer Int J Gynaecol Obstet 2006 95(Suppl 1) S161ndashS192
67 Bjoslashrge T Engeland A Hansen S et al Prognosis of patients with ovarian cancer and borderline tumours diagnosed inNorway between 1954 and 1993 Int J Cancer 1998 75 663ndash670
68 Seidman JD amp Kurman RJ Subclassi1047297cation of serous borderline tumors of the ovary into benign and malignant typesA clinicopathologic study of 65 advanced stage cases Am J Surg Pathol 1996 20 1331ndash1345
69 Sherman ME Berman J Birrer MJ et al Current challenges and opportunities for research on borderline ovarian tumorsHum Pathol 2004 35 961ndash97070 Leake JF Currie JL Rosenshein NB et al Long-term follow-up of serous ovarian tumors of low malignant potential Gynecol
Oncol 1992 47 150ndash15871 Lim-Tan SK Cajigas HE amp Scully RE Ovarian cystectomy for serous borderline tumors a follow-up study of 35 cases Obstet
Gynecol 1988 72 775ndash78172 Morice P Camatte S El Hassan J et al Clinical outcomes and fertility after conservative treatment of ovarian borderline
tumors Fertil Steril 2001 75 92ndash9673 Camatte S Morice P Pautier P et al Fertility results after conservative treatment of advanced stage serous borderline
tumour of the ovary BJOG 2002 109 376ndash38074 Crispens MA Bodurka D Deavers M et al Response and survival in patients with progressive or recurrent serous ovarian
tumors of low malignant potential Obstet Gynecol 2002 99 3ndash1075 Fauvet R Poncelet C Boccara J et al Fertility after conservative treatment for borderline ovarian tumors a French
multicenter study Fertil Steril 2005 83 284ndash29076 Morris RT Gershenson DM Silva EG et al Outcome and reproductive function after conservative surgery for borderline
ovarian tumors Obstet Gynecol 2000 95 541ndash54777 Gotlieb WH Flikker S Davidson B et al Borderline tumors of the ovary fertility treatment conservative management and
pregnancy outcome Cancer 1998 82 141ndash14678 Maltaris T Boehm D Dittrich R et al Reproduction beyond cancer a message of hope for young women Gynecol Oncol
2006 103 1109ndash112179 Beiner ME Gotlieb WH Davidson B et al Infertility treatment after conservative management of borderline ovarian
tumors Cancer 2001 92 320ndash32580 Fasouliotis SJ Davis O Schattman G et al Safety and ef 1047297cacy of infertility treatment after conservative management of
borderline ovarian tumors a preliminary report Fertil Steril 2004 82 568ndash57281 Kashyap S amp Davis OK Ovarian cancer and fertility medications a critical appraisal Semin Reprod Med 2003 21 65ndash7182 Morice P Camatte S Wicart-Poque F et al Results of conservative management of epithelial malignant and borderline
ovarian tumours Hum Reprod Update 2003 9 185ndash19283 Whittemore AS Harris R amp Itnyre J Characteristics relating to ovarian cancer risk collaborative analysis of 12 US case-
control studies II Invasive epithelial ovarian cancers in white women Collaborative Ovarian Cancer Group Am J Epi-demiol 1992 136 1184ndash1203
84 Fortin A Morice P Thoury A et al Impact of infertility drugs after treatment of borderline ovarian tumors results of a retrospective multicenter study Fertil Steril 2007 87 591ndash596
85 Burger CW van de Swaluw A Mooij TM et al Risk of borderline and invasive ovarian tumors after ovarian stimulation forin vitro fertilization in a large Dutch cohort after 15 years of follow-up Abstracts presented for the 40th Annual Meeting of the Society of Gynecologic Oncologists February 2009 (abstract no 6) Gynecol Oncol 2009 112(Suppl) S4
86 Donnez J Dolmans MM Demylle D et al Livebirth after orthotopic transplantation of cryopreserved ovarian tissue Lancet 2004 364 1405ndash1410
87 Lee DM Yeoman RR Battaglia DE et al Live birth after ovarian tissue transplant Nature 2004 428 137ndash138
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336336

7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 612
have evaluated the ef 1047297cacy of chemotherapy in advanced stage BOT with residual disease Cisplatin-
based therapy in serous BOT with residual disease have shown high response rates but modest
effect on long-term survival1464 In case of recurrences where transformation to an invasive histology
has occurred consideration of platinum-taxane-based chemotherapy is reasonable The molecular
changes transforming BOT to invasive ovarian carcinoma may be clari1047297ed in the future with the
possibility of blocking the different lsquostepsrsquo in the carcinogenesis Today we know that both serous BOTand low-grade serous carcinoma frequently present with B-raf and K-ras mutations11
Survival
Overall survival for women with BOT is excellent 90ndash100 in most reports depending on age at
diagnosis FIGO stage and histologic type112651626566 Trillsch et al11 reported a 5-year overall survival
rate of almost 100 in early stage disease (FIGO I-II) and between 86 and 92 in more advanced
disease (FIGO III-IV) In a Norwegian population-based study67 the age-adjusted 1- 3- 5- and 10-year
relative survival rates of women with mucinous BOT were 98 97 97 and 95 respectively and for
women with serous BOT 96 93 90 and 90 respectively The relative risk of dying increased with
higher age at diagnosis The 5-year relative survival for women aged between 0 and 44 years was 99compared with 85 for women aged 75ndash89 years Nearly the same 1047297gures are reported by Sherman
et al12 with better survival for younger women and slightly better survival for serous tumours
compared with mucinous tumours although mucinous tumours in advanced stage had the poorest
long-term survival (855)12
Seidman and Kurman35 summarised 97 reports including a total of 4129 women with serous BOT
and showed a disease-speci1047297c survival rate of 99 for stage I disease and 953 for stage III disease
(mean follow up of 7 years)35 The 5-year survival was 98 for women with serous BOT with non-
invasive implants and 33 for those with invasive implants68
Conservative surgery
The median age of diagnosis for women with BOT is 40 years and nearly one-third are younger than
40 years Thus preservation of childbearing potential is an important issue for many of these women
To select women for fertility-sparing surgery without risk of reduced long-term survival is a challenge
for the gynaecologic oncologist3069 (Fig 2) Conservative surgery is de1047297ned as complete staging in
which the uterus and at least a part of one ovary are preserved1162 (Fig 2)
Although the standard treatment for all women with BOT is at least bilateral salpingo-
oophorectomy many young women with stage Ia tumours who have not completed childbearing
can be safely treated with unilateral salpingo-oophorectomy after comprehensive surgical staging
thereby preserving the fertility potential At least as important as the fertility issue however is
whether we can reduce the morbidity caused by radical surgery and whether a more conservative
approach is a safe alternative regarding cancer prognosis51
Recent studies from the Norwegian RadiumHospital8 and Gynecologic Oncology Group65 have shown that preservation of reproductive organs is
feasible Relapse rates after bilateral salpingo-oophorectomy range between 0 and 20 This rate
varies between 12 and 58 for cystectomy and between 25 and 57 for radical surgery Relapses
can also occur late and recurrences as late as 39 years after initial treatment have been reported5134
Predictors of relapse are resection margins containing tumour cells70 The frequency of persistence or
recurrence in 35 patients with serous-BOT treated by unilateral cystectomy bilateral cystectomy or
unilateral cystectomy with contralateral oophorectomy or salpingo-oophorectomy was retrospectively
investigated by Lim-Tan et al71 Conservative surgical treatment was carried out either because the
women were young and wanted to preserve their fertility or because the nature of the tumour was not
determined at the time of surgery Thirty-three women had stage I disease (19 stage Ia 10 stage Ib and
four stage Ic) and two had stage III disease Although 60 of the women had additional and in somecases de1047297nitive operations within relative short periods after initial cystectomy or cystectomies 21 had
conservation of ovarian tissue and were followed on average for 75 years All women with stage I
disease were alive without evidence of disease after surgical treatment alone The presence of
persistent or recurrent disease correlated with multifocality and involvement of resection margins
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336330
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 712
Multifocality may be a strong predictor of failure of cystectomy to control the disease No recurrence of
disease was seen in ovaries from which a single cyst had been removed with negative resection
margins Extensive sampling of the resection margins of ovarian cysts is important71
For many women with BOT fertility is an important issue It is therefore essential to discuss with
these young women the advantages and disadvantages between conservative and radical surgery
Conservative surgery preserves fertility and hormonal function but unfortunately with high risk of recurrence
In women with obvious stage I disease unilateral salpingo-oophorectomy or cystectomy has from
previous studies been shown to be safe This has also been con1047297rmed for women with advanced-stage
disease on the assumption of close follow up
Even for women with advanced disease conservative surgery might be considered after informed
consent The recurrence rate is high and invasive and even non-invasive implants may recur up to 15
as invasive OC without negative in1047298uence on survival34567273
Treatment at recurrent disease after conservative treatment
Early detected recurrences are curable with repeated surgery113451 and therefore conservativetreatment might again be considered in women with recurrent disease if fertility still is an issue and the
woman is informed about the high risk of recurrence and agrees on close follow up accepting repeated
surgery5162 If invasive implants are diagnosed this procedure could not be recommended In any case
of recurrent disease secondary debulking surgery is important as women suboptimally debulked have
poor survival115174
Fertility after conservative management of borderline ovarian tumour
Infertility is frequently observed inwomen with BOT A history of infertility beforediagnosis has been
reported in 10ndash35 of women75ndash77 To allow conservative surgery careful evaluation of the extent of
disease by the gynaecologist at the time of operation and meticulous examination of the cystectomyspecimen by the gynaecologist and pathologist are desirable to determine the prognosis after cys-
tectomy In a study by Morris et al76 onewoman who had disease-related deathwasnot staged properly
In a meta-analysis by Maltaris et al78 1483 women had BOT of whom 656 were treated conservatively
(442) A total of 196 women became pregnant and 111 relapsed after unilateral salpingo-
oophorectomy only one woman died from the disease (015) The investigators therefore suggest
that conservative surgery is justi1047297able for some women with a good prognostic index Unilateral
oophorectomy omentectomy and appendectomy in stage Ia diploid mucinous BOT are indicated for
young women who wish to preservefertility (Fig 2) In stage Ia diploid serous BOT thesame procedure is
safe if the contralateral ovary is macroscopically normal Careful inspection of a macroscopically normal
contralateral ovary should be suf 1047297cient inyoung womenwith stageIa disease who wish to remainfertile
Surgery itself can impair the fertility function by loss of ovarian tissue pelvic scarring and adhesionsblocking the fallopian tube Post-surgery fertility factors such as ovulation fallopian tubes and sperm
factors should be investigated and treated if necessary About one-third of women undergoing
conservative surgery for BOT will be able to conceive with no negative in1047298uence of pregnancy on the
disease60727779 Ovulation induction is often required in order to conceive80 The role of ovulation
(in-vitro [IVF] fertilisation) drugs in BOT is currently under debate7780ndash84
Recently a large nationwide cohort study of 19146 subfertile women in the Netherlands who
received IVF drugs between 1983 and 1995 and a comparison group of 6953 subfertile women who
were not treated was published After a median follow up of 15 years a total of 77 ovarian malignancies
were observed in the cohort including 42 women with epithelial ovarian cancer and 35 women with
BOT Sixty-one ovarian malignancies were observed in the IVF-group and 16 in the unexposed (control)
group The ratio hazard for epithelial ovarian cancer and BOT was 167 (074 to 375) and 425 (127 to1418) respectively85 The conclusion of Burger et al85 was that IVF increases the risk of BOT
A worrying1047297nding of their study is the increased risk of epithelial ovarian cancer and BOT even after 15
years of follow up Fasouliotis et al80 found no perceptible negative effect of previous BOT on preg-
nancy rates after IVF The same was shown by Fortin et al84 in a study of 30 women treated with IVF
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 331
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 812
drugs for infertility after conservative surgery Thirteen pregnancies were observed Disease in four
women recurred All recurrences were BOT on a remaining ovary that had been treated by surgery
alone All women are currently disease-free after secondary surgery Fortin et al84 concluded that IVF
drugs can be used safely in womenwho develop infertility after conservative treatment of BOT Because
of the low number of women treated with IVF drugs Norwegian Radium Hospital guidelines are to
proceed with caution and only women with early stage BOT are permitted to be treated with IVF drugsThe latest development regarding reproduction and BOT is cryopreservation 86 Women who have
their ovaries removed because of large stage Ib BOT now have a possibility of becoming pregnant
Biopsies from normal ovarian cortex can be taken during the primary operation In 2004 a live birth
after a fresh ovarian tissue transplant in a primate was reported87 Donnez et al86 described in 2004
a live birth after orthotopic auto-transplantation of cryopreserved ovarian tissue Their1047297ndings opened
new possibilities for young women facing premature ovarian failure
Women with reduced fertility after surgery can consider ovarian stimulation egg retrieval and egg
freezing Ovarian stimulation and exposure to high oestrogen exposure do not seem to increase the risk
for recurrence Nor do pregnancies have negative in1047298uence on survival7277
To assure future fertility preservation in women with BOT the gynaecologic oncologist should
collaborate closely with the reproductive endocrinologists even before surgery Until more mature dataexist the general recommendation is a limited number of stimulation cycles only for stage I patients In
case of bilateral salpingo-oophorectomy cryopreservation of ovarian cortex biopsy from the less
affected ovary could be considered although this is not always technically possible1151
Follow up
Follow up should be long term and lifelong because recurrences may develop after more than 15 years
In conservatively treated womenclose follow up is crucial with special attentionto theremainingovaryIt
is still debated if the remaining ovary (and uterus) should be removed after the family is completed For
low-risk BOT there is no indication for this procedure but in women with high-risk of recurrence the
procedure is optional the alternative being to wait until recurrence or carry out radical surgery Manywomen will choose radical surgery when the family is completed because of psychological stress
The general recommendation is follow up every 3 months during the 1047297rst 2 years and then every 6
months for the next 3 years and annually thereafter The women is followed with pelvic examination
transvaginal ultrasound and calcium 125 measurement1451 (Fig 2)
Future direction of borderline ovarian tumour
A key issue for future research on BOTconcerning epidemiology is the identi1047297cation of risk factors for
invasive implants recurrences and death and also the identi1047297cation of predisposing heritable factors
For clinical management improved methods for preoperative and intraoperative diagnosis should
be considered in addition to the role of laparoscopic surgery in removal of complex cysts improvedmethods for distinguishing metastases from BOT and determination of risk associated with conser-
vative treatment
For pathology and molecular biology molecular studies are needed to assess the relationship
between serous BOT low-grade serous carcinoma and high-grade serous carcinoma Molecular studies
are also needed to aid in the characterisation of implants and studies need to be conducted to
determine the biology of microinvasive BOT and the clinical signi1047297cance of long-term follow up
Conclusion
Borderline ovarian tumours are ovarian tumours with good prognosis that account for 10ndash20 of all
epithelial ovarian cancer Historically standard primarysurgeryincludedbilateral salpingo-oophorectomyomentectomy peritoneal washing and complete peritoneal resection of macroscopic lesions or multiple
biopsies In cases of M-BOT women are also treated with appendectomy As one-third of BOT are diagnosed
inwomenyounger than40 years however fertility-sparingtreatment (ie preservation of the uterus andat
least part of one ovary) has been increasingly used in the past 10 years Fertility drugs are well tolerated in
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336332
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 912
women with infertility after fertility-sparing surgery Careful selection of candidates is necessary Lapa-
roscopic techniques can be used but are reserved for oncologic surgeons This conservative treatment
increases therateof recurrencebutwithoutany effecton survivalThespontaneouspregnancy rate is nearly
50and most are achieved spontaneously Spontaneous pregnancy can occurafter conservative treatment
of advanced-stage BOT (with non-invasive implants) These women should be closely followed up Further
research has to concentrate on clinical risk-factors histopathological markers and pathogenesis to guar-antee the best clinical management for women with BOT
Con1047298ict of interest statement
None declared
Practice points
BOTare ovarian tumours with good prognosis that account for 10ndash20 of all epithelial ovarian
cancer Historically standard primary surgery included bilateral salpingo-oophorectomy omentec-
tomy peritoneal washing and complete peritoneal resection of macroscopic lesions or
multiple biopsies
In case of mucinous BOT women are also treated with appendectomy
Adjuvant therapy for the treatment of BOT has no proven bene1047297t
As one-third of BOT are diagnosed in women younger than 40 years fertility-sparing treat-
ment (ie preservation of the uterus and at least part of one ovary) has been increasingly used
in the past 10 years
Fertility drugs are well tolerated in women with infertility after fertility-sparing surgery
Careful selection of candidates is necessary
Laparoscopic techniques can be used but are reserved for oncologic surgeons Spontaneous pregnancy can occur after conservative treatment of advanced stage BOT (with
non-invasive implants)
These women should be closely followed up
Research agenda
Epidemiology
Identify risk factors for invasive implants recurrences and death
Identify predisposing heritable factors
Clinical management
Improve methods for preoperative and intraoperative diagnosis
Further explore the role of laparoscopic surgery in the removal of complex cysts
Improve methods for distinguishing metastases from BOTand determine risk associated with
conservative treatment
Pathology and molecular biology
Conduct molecular studies to assess the relationship between serous BOT low-grade serous
carcinoma and high-grade serous carcinoma Conduct molecular studies to aid in the characterisation of implants
Conduct studies to determine the biology of microinvasive BOTand the clinical signi1047297cance of
long-term follow up
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 333
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1012
Acknowledgement
We wish to thank Mrs Gry Seppola for technical assistance and gratefully acknowledge the1047297nancial
support from the Inger and John Fredriksen Foundation for Ovarian Cancer Research
References
1 Taylor HC Malignant and semi-malignant tumors of the ovary Surg Gynecol Obstet 1929 48 204ndash2302 Kottmeier HL Kolstad P McGarrity KA Annual report on results of treatment in gynaecologic cancer vol 17 Statements of
results obtained in 1969ndash1972 inclusive FIGO Stockholm Sweden Editorial of 1047297ce Radiumhemmet 19733 Serov SF Scully RE amp Sobin LH International histological classi 1047297cation of tumors no 9 Histoloigcal typing of ovarian tumours
Geneval World Health Organization 19734 Hart WR amp Norris HJ Borderline and malignant mucinous tumors of the ovary Histologic criteria and clinical behavior
Cancer 1973 31 1031ndash10455 Scully RE Tumors of the ovary and maldeveloped gonads Fascicle 16 In Atlas of tumor pathology Second series Wash-
ington DC Armed Forces Institute of Pathology 1979 pp 75ndash906 Lenhard MS Mitterer S Kuumlmper C et al Long-term follow-up after ovarian borderline tumor relapse and survival in
a large patient cohort Eur J Obstet Gynecol Reprod Biol 2009 145 189ndash194
7 Quirk JT amp Natarajan N Ovarian cancer incidence in the United States 1992ndash
1999 Gynecol Oncol 2005 97 519ndash
5238 Kaern J Tropeacute CG amp Abeler VM A retrospective study of 370 borderline tumors of the ovary treated at the NorwegianRadium Hospital from 1970 to 1982 A review of clinicopathologic features and treatment modalities Cancer 1993 711810ndash1820
9 Bjoslashrge T Engeland A Hansen S et al Trends in the incidence of ovarian cancer and borderline tumours in Norway1954ndash1993 Int J Cancer 1997 71 780ndash786
10 Skiacuternisdoacutettir I Garmo H Wilander E et al Borderline ovarian tumors in Sweden 1960ndash2005 trends in incidence and age atdiagnosis compared to ovarian cancer Int J Cancer 2008 123 1897ndash1901
11 Trillsch F Mahner S Ruetzel J et al Clinical management of borderline ovarian tumors Expert Rev Anticancer Ther 2010 101115ndash1124
12 Sherman ME Mink PJ Curtis R et al Survival among women with borderline ovarian tumors and ovarian carcinomaa population-based analysis Cancer 2004 100 1045ndash1052
13 Kramer JL Greene MH Epidemiology of ovarian fallopian tube and primary peritoneal cancer In Gershenson DMMcGuire WP Gore M et al eds Gynecologic cancer Controversies in management 1st ed Philadelphia Elsevier ChurchillLivingstone 2004 pp 327ndash340
14 Tropeacute C Davidson B Paulsen T et al Diagnosis and treatment of borderline ovarian neoplasms lsquothe state of the artrsquo Eur J Gynaecol Oncol 2009 30 471ndash482
15 Kurman RJ amp Shih IeM Pathogenesis of ovarian cancer lessons from morphology and molecular biology and their clinicalimplications Int J Gynecol Pathol 2008 27 151ndash160
16 Kurman RJ Visvanathan K Roden R et al Early detection and treatment of ovarian cancer shifting from early stage tominimal volume of disease based on a new model of carcinogenesis Am J Obstet Gynecol 2008 198 351ndash356
17 Shih IeM amp Kurman RJ Ovarian tumorigenesis a proposed model based on morphological and molecular genetic analysis Am J Pathol 2004 164 1511ndash1518
18 Levanon K Crum C amp Drapkin R New insights into the pathogenesis of serous ovarian cancer and its clinical impact J ClinOncol 2008 26 5284ndash5293
19 Meinhold-Heerlein I Bauerschlag D Hilpert F et al Molecular and prognostic distinction between serous ovarian carci-nomas of varying grade and malignant potential Oncogene 2005 24 1053ndash1065
20 Bonome T Lee JY Park DC et al Expression pro1047297ling of serous low malignant potential low-grade and high-grade tumorsof the ovary Cancer Res 2005 65 10602ndash10612
21 Mahner S Baasch C Schwarz J et al C-Fos expression is a molecular predictor of progression and survival in epithelialovarian carcinoma Br J Cancer 2008 99 1269ndash1275
22 Ortiz BH Ailawadi M Colitti C et al Second primary or recurrence Comparative patterns of p53 and K-ras mutationssuggest that serous borderline ovarian tumors and subsequent serous carcinomas are unrelated tumors Cancer Res 200161 7264ndash7267
23 Lee KR Tavassoli FA Prat J et al Tumours of the ovary and peritoneum In Tavassoli FA amp Devilee P (eds) Pathology and
genetics Tumours of the breast and female genital organs Lyon IARC Press 2003 pp 113ndash20224 Oedegaard E Ovarian carcinomas and borderline ovarian tumors - molecular markers and operative treatment Dissertation
Facutly of Medicine University of Oslo 200825 Mok SC Bell DA Knapp RC et al Mutation of K-ras protooncogene in human ovarian epithelial tumors of borderline
malignancy Cancer Res 1993 53 1489ndash149226 du Bois A Ewald-Riegler N du Bois O et al Borderline tumors of the ovary a systematic review [German] Geburtsh
Frauenheilk 2009 69 807ndash83327 Seidman JD Horkayne-Szakaly I Haiba M et al The histologic type and stage distribution of ovarian carcinomas of surface
epithelial origin Int J Gynecol Pathol 2004 23 41ndash44
28 Prat J amp De Nictolis M Serous borderline tumors of the ovary a long-term follow-up study of 137 cases including 18 witha micropapillary pattern and 20 with microinvasion Am J Surg Pathol 2002 26 1111ndash1128
29 Bell DA Weinstock MA amp Scully RE Peritoneal implants of ovarian serous borderline tumors Histologic features andprognosis Cancer 1988 62 2212ndash2222
30 Tinelli R Tinelli A Tinelli FG et al Conservative surgery for borderline ovarian tumors a review Gynecol Oncol 2006 100
185ndash191
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336334
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1112
31 Kurman RJ amp Trimble CL The behavior of serous tumors of low malignant potential are they ever malignant Int J Gynecol
Pathol 1993 12 120ndash12732 Morice P Camatte S Rey A et al Prognostic factors for patients with advanced stage serous borderline tumours of the
ovary Ann Oncol 2003 14 592ndash59833 Bradley RF Stewart 4th JH Russell GB et al Pseudomyxoma peritonei of appendiceal origin a clinicopathologic analysis of
101 patients uniformly treated at a single institution with literature review Am J Surg Pathol 2006 30 551ndash559
34 Silva EG Gershenson DM Malpica A et al The recurrence and the overall survival rates of ovarian serous borderlineneoplasms with noninvasive implants is time dependent Am J Surg Pathol 2006 30 1367ndash137135 Seidman JD amp Kurman RJ Ovarian serous borderline tumors a critical review of the literature with emphasis on prognostic
indicators Hum Pathol 2000 31 539ndash55736 Chang SJ Ryu HS Chang KH et al Prognostic signi1047297cance of the micropapillary pattern in patients with serous borderline
ovarian tumors Acta Obstet Gynecol Scand 2008 87 476ndash48137 Fox H amp Wells M Surface epithelialstromal tumors of the ovary In Fox H amp Wells M (eds) Haines and Taylor Obstetrical and
Gynaecological Pathology 5th ed London Churchill Livingstone 2003 pp 713ndash74338 Ren J Peng Z amp Yang K A clinicopathologic multivariate analysis affecting recurrence of borderline ovarian tumors Gynecol
Oncol 2008 110 162ndash16739 Longacre TA McKenney JK Tazelaar HD et al Ovarian serous tumors of low malignant potential (borderline tumors)
outcome-based study of 276 patients with long-term (gt or frac145-year) follow-up Am J Surg Pathol 2005 29 707ndash72340 Cusidoacute M Balagueroacute L Hernandez G et al Results of the national survey of borderline ovarian tumors in Spain Gynecol
Oncol 2007 104 617ndash62241 Kaern J Tropeacute CG Kristensen GB et al DNA ploidy the most important prognostic factor in patients with borderline
tumors of the ovary Int J Gynecol Cancer 1993 3 349ndash35842 Meyer JS Gersell DJ amp Yim S Cell proliferation in ovarian carcinoma superior accuracy of S-phase fraction (SPF) by DNA
labeling index versus 1047298ow cytometric SPF lack of independent prognostic power for SPF and DNA ploidy and limitedeffect of SPF on tumor growth rate Gynecol Oncol 2001 81 466ndash476
43 Verbruggen MB van Diest PJ Baak JP et al The prognostic and clinical value of morphometry and DNA cytometry inborderline ovarian tumors a prospective study Int J Gynecol Pathol 2009 28 35ndash40
44 Yokoyama Y Moriya T Takano T et al Clinical outcome and risk factors for recurrence in borderline ovarian tumours Br J Cancer 2006 94 1586ndash1591
45 Leake JF Rader JS Woodruff JD et al Retroperitoneal lymphatic involvement with epithelial ovarian tumors of lowmalignant potential Gynecol Oncol 1991 42 124ndash130
46 Paulsen T Kaern J Kjaerheim K et al Symptoms and referral of women with epithelial ovarian tumors Int J Gynaecol Obstet 2005 88 31ndash37
47 Paulsen T Epithelial ovarian cancer A clinical epidemiological approach on diagnosis and treatment Dissertation Faculty of Medicine University of Oslo 2007
48 Tropeacute CG Kristensen G amp Makar A Surgery for borderline tumor of the ovary Semin Surg Oncol 2000 19 69ndash7549 Tempfer CB Polterauer S Bentz EK et al Accuracy of intraoperative frozen section analysis in borderline tumors of the
ovary a retrospective analysis of 96 cases and review of the literature Gynecol Oncol 2007 107 248ndash25250 Camatte S Morice P Thoury A et al Impact of surgical staging in patients with macroscopic lsquostage Irsquo ovarian borderline
tumours analysis of a continuous series of 101 cases Eur J Cancer 2004 40 1842ndash184951 Cadron I Leunen K Van Gorp T et al Management of borderline ovarian neoplasms J Clin Oncol 2007 25 2928ndash293752 Snider DD Stuart GC Nation JG et al Evaluation of surgical staging in stage I low malignant potential ovarian tumors
Gynecol Oncol 1991 40 129ndash13253 Ronnett BM Kurman RJ Zahn CM et al Pseudomyxoma peritonei in women a clinicopathologic analysis of 30 cases with
emphasis on site of origin prognosis and relationship to ovarian mucinous tumors of low malignant potential Hum Pathol
1995 26 509ndash52454 Seidman JD Elsayed AM Sobin LH et al Association of mucinous tumors of the ovary and appendix A clinicopathologic
study of 25 cases Am J Surg Pathol 1993 17 22ndash3455 Trimble EL amp Trimble LC Epithelial ovarian tumors of low malignant potential In Markman M amp Hoskins W (eds) Cancer
of the Ovary New York Raven Press 1993 pp 415ndash429
56 Zanetta G Rota S Chiari S et al Behavior of borderline tumors with particular interest to persistence recurrence andprogression to invasive carcinoma a prospective study J Clin Oncol 2001 19 2658ndash266457 Fauvet R Boccara J Dufournet C et al Restaging surgery for women with borderline ovarian tumors results of a French
multicenter study Cancer 2004 100 1145ndash115158 Zapardiel I Rosenberg P Peiretti M et al The role of restaging borderline ovarian tumors single institution experience and
review of the literature Gynecol Oncol 2010 119 274ndash27759 Def 1047297eux X Morice P Camatte S et al Results after laparoscopic management of serous borderline tumor of the ovary with
peritoneal implants Gynecol Oncol 2005 97 84ndash8960 Fauvet R Boccara J Dufournet C et al Laparoscopic management of borderline ovarian tumors results of a French
multicenter study Ann Oncol 2005 16 403ndash41061 Vandenput I Amant F amp Vergote I Peritoneal recurrences might be less common in advanced stage serous borderline
ovarian tumors that were treated by laparotomy Gynecol Oncol 2005 98 52362 CadronI Amant F VanGorp Tet alThe management of borderline tumours of theovary Curr Opin Oncol 2006 18 488ndash49363 Vergote I De Brabanter J Fyles A et al Prognostic importance of degree of differentiation and cyst rupture in stage I
invasive epithelial ovarian carcinoma Lancet 2001 357 176ndash182
64 Gershenson DM amp Silva EG Serous ovarian tumors of low malignant potential with peritoneal implants Cancer 1990 65578ndash585
65 Gershenson DM Clinical management potential tumours of low malignancy Best Pract Res Clin Obstet Gynaecol 2002 16513ndash527
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 335
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1212
66 Heintz AP Odicino F Maisonneuve P et al Carcinoma of the ovary FIGO 26th Annual Report on the Results of Treatment inGynecological Cancer Int J Gynaecol Obstet 2006 95(Suppl 1) S161ndashS192
67 Bjoslashrge T Engeland A Hansen S et al Prognosis of patients with ovarian cancer and borderline tumours diagnosed inNorway between 1954 and 1993 Int J Cancer 1998 75 663ndash670
68 Seidman JD amp Kurman RJ Subclassi1047297cation of serous borderline tumors of the ovary into benign and malignant typesA clinicopathologic study of 65 advanced stage cases Am J Surg Pathol 1996 20 1331ndash1345
69 Sherman ME Berman J Birrer MJ et al Current challenges and opportunities for research on borderline ovarian tumorsHum Pathol 2004 35 961ndash97070 Leake JF Currie JL Rosenshein NB et al Long-term follow-up of serous ovarian tumors of low malignant potential Gynecol
Oncol 1992 47 150ndash15871 Lim-Tan SK Cajigas HE amp Scully RE Ovarian cystectomy for serous borderline tumors a follow-up study of 35 cases Obstet
Gynecol 1988 72 775ndash78172 Morice P Camatte S El Hassan J et al Clinical outcomes and fertility after conservative treatment of ovarian borderline
tumors Fertil Steril 2001 75 92ndash9673 Camatte S Morice P Pautier P et al Fertility results after conservative treatment of advanced stage serous borderline
tumour of the ovary BJOG 2002 109 376ndash38074 Crispens MA Bodurka D Deavers M et al Response and survival in patients with progressive or recurrent serous ovarian
tumors of low malignant potential Obstet Gynecol 2002 99 3ndash1075 Fauvet R Poncelet C Boccara J et al Fertility after conservative treatment for borderline ovarian tumors a French
multicenter study Fertil Steril 2005 83 284ndash29076 Morris RT Gershenson DM Silva EG et al Outcome and reproductive function after conservative surgery for borderline
ovarian tumors Obstet Gynecol 2000 95 541ndash54777 Gotlieb WH Flikker S Davidson B et al Borderline tumors of the ovary fertility treatment conservative management and
pregnancy outcome Cancer 1998 82 141ndash14678 Maltaris T Boehm D Dittrich R et al Reproduction beyond cancer a message of hope for young women Gynecol Oncol
2006 103 1109ndash112179 Beiner ME Gotlieb WH Davidson B et al Infertility treatment after conservative management of borderline ovarian
tumors Cancer 2001 92 320ndash32580 Fasouliotis SJ Davis O Schattman G et al Safety and ef 1047297cacy of infertility treatment after conservative management of
borderline ovarian tumors a preliminary report Fertil Steril 2004 82 568ndash57281 Kashyap S amp Davis OK Ovarian cancer and fertility medications a critical appraisal Semin Reprod Med 2003 21 65ndash7182 Morice P Camatte S Wicart-Poque F et al Results of conservative management of epithelial malignant and borderline
ovarian tumours Hum Reprod Update 2003 9 185ndash19283 Whittemore AS Harris R amp Itnyre J Characteristics relating to ovarian cancer risk collaborative analysis of 12 US case-
control studies II Invasive epithelial ovarian cancers in white women Collaborative Ovarian Cancer Group Am J Epi-demiol 1992 136 1184ndash1203
84 Fortin A Morice P Thoury A et al Impact of infertility drugs after treatment of borderline ovarian tumors results of a retrospective multicenter study Fertil Steril 2007 87 591ndash596
85 Burger CW van de Swaluw A Mooij TM et al Risk of borderline and invasive ovarian tumors after ovarian stimulation forin vitro fertilization in a large Dutch cohort after 15 years of follow-up Abstracts presented for the 40th Annual Meeting of the Society of Gynecologic Oncologists February 2009 (abstract no 6) Gynecol Oncol 2009 112(Suppl) S4
86 Donnez J Dolmans MM Demylle D et al Livebirth after orthotopic transplantation of cryopreserved ovarian tissue Lancet 2004 364 1405ndash1410
87 Lee DM Yeoman RR Battaglia DE et al Live birth after ovarian tissue transplant Nature 2004 428 137ndash138
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336336

7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 712
Multifocality may be a strong predictor of failure of cystectomy to control the disease No recurrence of
disease was seen in ovaries from which a single cyst had been removed with negative resection
margins Extensive sampling of the resection margins of ovarian cysts is important71
For many women with BOT fertility is an important issue It is therefore essential to discuss with
these young women the advantages and disadvantages between conservative and radical surgery
Conservative surgery preserves fertility and hormonal function but unfortunately with high risk of recurrence
In women with obvious stage I disease unilateral salpingo-oophorectomy or cystectomy has from
previous studies been shown to be safe This has also been con1047297rmed for women with advanced-stage
disease on the assumption of close follow up
Even for women with advanced disease conservative surgery might be considered after informed
consent The recurrence rate is high and invasive and even non-invasive implants may recur up to 15
as invasive OC without negative in1047298uence on survival34567273
Treatment at recurrent disease after conservative treatment
Early detected recurrences are curable with repeated surgery113451 and therefore conservativetreatment might again be considered in women with recurrent disease if fertility still is an issue and the
woman is informed about the high risk of recurrence and agrees on close follow up accepting repeated
surgery5162 If invasive implants are diagnosed this procedure could not be recommended In any case
of recurrent disease secondary debulking surgery is important as women suboptimally debulked have
poor survival115174
Fertility after conservative management of borderline ovarian tumour
Infertility is frequently observed inwomen with BOT A history of infertility beforediagnosis has been
reported in 10ndash35 of women75ndash77 To allow conservative surgery careful evaluation of the extent of
disease by the gynaecologist at the time of operation and meticulous examination of the cystectomyspecimen by the gynaecologist and pathologist are desirable to determine the prognosis after cys-
tectomy In a study by Morris et al76 onewoman who had disease-related deathwasnot staged properly
In a meta-analysis by Maltaris et al78 1483 women had BOT of whom 656 were treated conservatively
(442) A total of 196 women became pregnant and 111 relapsed after unilateral salpingo-
oophorectomy only one woman died from the disease (015) The investigators therefore suggest
that conservative surgery is justi1047297able for some women with a good prognostic index Unilateral
oophorectomy omentectomy and appendectomy in stage Ia diploid mucinous BOT are indicated for
young women who wish to preservefertility (Fig 2) In stage Ia diploid serous BOT thesame procedure is
safe if the contralateral ovary is macroscopically normal Careful inspection of a macroscopically normal
contralateral ovary should be suf 1047297cient inyoung womenwith stageIa disease who wish to remainfertile
Surgery itself can impair the fertility function by loss of ovarian tissue pelvic scarring and adhesionsblocking the fallopian tube Post-surgery fertility factors such as ovulation fallopian tubes and sperm
factors should be investigated and treated if necessary About one-third of women undergoing
conservative surgery for BOT will be able to conceive with no negative in1047298uence of pregnancy on the
disease60727779 Ovulation induction is often required in order to conceive80 The role of ovulation
(in-vitro [IVF] fertilisation) drugs in BOT is currently under debate7780ndash84
Recently a large nationwide cohort study of 19146 subfertile women in the Netherlands who
received IVF drugs between 1983 and 1995 and a comparison group of 6953 subfertile women who
were not treated was published After a median follow up of 15 years a total of 77 ovarian malignancies
were observed in the cohort including 42 women with epithelial ovarian cancer and 35 women with
BOT Sixty-one ovarian malignancies were observed in the IVF-group and 16 in the unexposed (control)
group The ratio hazard for epithelial ovarian cancer and BOT was 167 (074 to 375) and 425 (127 to1418) respectively85 The conclusion of Burger et al85 was that IVF increases the risk of BOT
A worrying1047297nding of their study is the increased risk of epithelial ovarian cancer and BOT even after 15
years of follow up Fasouliotis et al80 found no perceptible negative effect of previous BOT on preg-
nancy rates after IVF The same was shown by Fortin et al84 in a study of 30 women treated with IVF
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 331
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 812
drugs for infertility after conservative surgery Thirteen pregnancies were observed Disease in four
women recurred All recurrences were BOT on a remaining ovary that had been treated by surgery
alone All women are currently disease-free after secondary surgery Fortin et al84 concluded that IVF
drugs can be used safely in womenwho develop infertility after conservative treatment of BOT Because
of the low number of women treated with IVF drugs Norwegian Radium Hospital guidelines are to
proceed with caution and only women with early stage BOT are permitted to be treated with IVF drugsThe latest development regarding reproduction and BOT is cryopreservation 86 Women who have
their ovaries removed because of large stage Ib BOT now have a possibility of becoming pregnant
Biopsies from normal ovarian cortex can be taken during the primary operation In 2004 a live birth
after a fresh ovarian tissue transplant in a primate was reported87 Donnez et al86 described in 2004
a live birth after orthotopic auto-transplantation of cryopreserved ovarian tissue Their1047297ndings opened
new possibilities for young women facing premature ovarian failure
Women with reduced fertility after surgery can consider ovarian stimulation egg retrieval and egg
freezing Ovarian stimulation and exposure to high oestrogen exposure do not seem to increase the risk
for recurrence Nor do pregnancies have negative in1047298uence on survival7277
To assure future fertility preservation in women with BOT the gynaecologic oncologist should
collaborate closely with the reproductive endocrinologists even before surgery Until more mature dataexist the general recommendation is a limited number of stimulation cycles only for stage I patients In
case of bilateral salpingo-oophorectomy cryopreservation of ovarian cortex biopsy from the less
affected ovary could be considered although this is not always technically possible1151
Follow up
Follow up should be long term and lifelong because recurrences may develop after more than 15 years
In conservatively treated womenclose follow up is crucial with special attentionto theremainingovaryIt
is still debated if the remaining ovary (and uterus) should be removed after the family is completed For
low-risk BOT there is no indication for this procedure but in women with high-risk of recurrence the
procedure is optional the alternative being to wait until recurrence or carry out radical surgery Manywomen will choose radical surgery when the family is completed because of psychological stress
The general recommendation is follow up every 3 months during the 1047297rst 2 years and then every 6
months for the next 3 years and annually thereafter The women is followed with pelvic examination
transvaginal ultrasound and calcium 125 measurement1451 (Fig 2)
Future direction of borderline ovarian tumour
A key issue for future research on BOTconcerning epidemiology is the identi1047297cation of risk factors for
invasive implants recurrences and death and also the identi1047297cation of predisposing heritable factors
For clinical management improved methods for preoperative and intraoperative diagnosis should
be considered in addition to the role of laparoscopic surgery in removal of complex cysts improvedmethods for distinguishing metastases from BOT and determination of risk associated with conser-
vative treatment
For pathology and molecular biology molecular studies are needed to assess the relationship
between serous BOT low-grade serous carcinoma and high-grade serous carcinoma Molecular studies
are also needed to aid in the characterisation of implants and studies need to be conducted to
determine the biology of microinvasive BOT and the clinical signi1047297cance of long-term follow up
Conclusion
Borderline ovarian tumours are ovarian tumours with good prognosis that account for 10ndash20 of all
epithelial ovarian cancer Historically standard primarysurgeryincludedbilateral salpingo-oophorectomyomentectomy peritoneal washing and complete peritoneal resection of macroscopic lesions or multiple
biopsies In cases of M-BOT women are also treated with appendectomy As one-third of BOT are diagnosed
inwomenyounger than40 years however fertility-sparingtreatment (ie preservation of the uterus andat
least part of one ovary) has been increasingly used in the past 10 years Fertility drugs are well tolerated in
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336332
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 912
women with infertility after fertility-sparing surgery Careful selection of candidates is necessary Lapa-
roscopic techniques can be used but are reserved for oncologic surgeons This conservative treatment
increases therateof recurrencebutwithoutany effecton survivalThespontaneouspregnancy rate is nearly
50and most are achieved spontaneously Spontaneous pregnancy can occurafter conservative treatment
of advanced-stage BOT (with non-invasive implants) These women should be closely followed up Further
research has to concentrate on clinical risk-factors histopathological markers and pathogenesis to guar-antee the best clinical management for women with BOT
Con1047298ict of interest statement
None declared
Practice points
BOTare ovarian tumours with good prognosis that account for 10ndash20 of all epithelial ovarian
cancer Historically standard primary surgery included bilateral salpingo-oophorectomy omentec-
tomy peritoneal washing and complete peritoneal resection of macroscopic lesions or
multiple biopsies
In case of mucinous BOT women are also treated with appendectomy
Adjuvant therapy for the treatment of BOT has no proven bene1047297t
As one-third of BOT are diagnosed in women younger than 40 years fertility-sparing treat-
ment (ie preservation of the uterus and at least part of one ovary) has been increasingly used
in the past 10 years
Fertility drugs are well tolerated in women with infertility after fertility-sparing surgery
Careful selection of candidates is necessary
Laparoscopic techniques can be used but are reserved for oncologic surgeons Spontaneous pregnancy can occur after conservative treatment of advanced stage BOT (with
non-invasive implants)
These women should be closely followed up
Research agenda
Epidemiology
Identify risk factors for invasive implants recurrences and death
Identify predisposing heritable factors
Clinical management
Improve methods for preoperative and intraoperative diagnosis
Further explore the role of laparoscopic surgery in the removal of complex cysts
Improve methods for distinguishing metastases from BOTand determine risk associated with
conservative treatment
Pathology and molecular biology
Conduct molecular studies to assess the relationship between serous BOT low-grade serous
carcinoma and high-grade serous carcinoma Conduct molecular studies to aid in the characterisation of implants
Conduct studies to determine the biology of microinvasive BOTand the clinical signi1047297cance of
long-term follow up
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 333
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1012
Acknowledgement
We wish to thank Mrs Gry Seppola for technical assistance and gratefully acknowledge the1047297nancial
support from the Inger and John Fredriksen Foundation for Ovarian Cancer Research
References
1 Taylor HC Malignant and semi-malignant tumors of the ovary Surg Gynecol Obstet 1929 48 204ndash2302 Kottmeier HL Kolstad P McGarrity KA Annual report on results of treatment in gynaecologic cancer vol 17 Statements of
results obtained in 1969ndash1972 inclusive FIGO Stockholm Sweden Editorial of 1047297ce Radiumhemmet 19733 Serov SF Scully RE amp Sobin LH International histological classi 1047297cation of tumors no 9 Histoloigcal typing of ovarian tumours
Geneval World Health Organization 19734 Hart WR amp Norris HJ Borderline and malignant mucinous tumors of the ovary Histologic criteria and clinical behavior
Cancer 1973 31 1031ndash10455 Scully RE Tumors of the ovary and maldeveloped gonads Fascicle 16 In Atlas of tumor pathology Second series Wash-
ington DC Armed Forces Institute of Pathology 1979 pp 75ndash906 Lenhard MS Mitterer S Kuumlmper C et al Long-term follow-up after ovarian borderline tumor relapse and survival in
a large patient cohort Eur J Obstet Gynecol Reprod Biol 2009 145 189ndash194
7 Quirk JT amp Natarajan N Ovarian cancer incidence in the United States 1992ndash
1999 Gynecol Oncol 2005 97 519ndash
5238 Kaern J Tropeacute CG amp Abeler VM A retrospective study of 370 borderline tumors of the ovary treated at the NorwegianRadium Hospital from 1970 to 1982 A review of clinicopathologic features and treatment modalities Cancer 1993 711810ndash1820
9 Bjoslashrge T Engeland A Hansen S et al Trends in the incidence of ovarian cancer and borderline tumours in Norway1954ndash1993 Int J Cancer 1997 71 780ndash786
10 Skiacuternisdoacutettir I Garmo H Wilander E et al Borderline ovarian tumors in Sweden 1960ndash2005 trends in incidence and age atdiagnosis compared to ovarian cancer Int J Cancer 2008 123 1897ndash1901
11 Trillsch F Mahner S Ruetzel J et al Clinical management of borderline ovarian tumors Expert Rev Anticancer Ther 2010 101115ndash1124
12 Sherman ME Mink PJ Curtis R et al Survival among women with borderline ovarian tumors and ovarian carcinomaa population-based analysis Cancer 2004 100 1045ndash1052
13 Kramer JL Greene MH Epidemiology of ovarian fallopian tube and primary peritoneal cancer In Gershenson DMMcGuire WP Gore M et al eds Gynecologic cancer Controversies in management 1st ed Philadelphia Elsevier ChurchillLivingstone 2004 pp 327ndash340
14 Tropeacute C Davidson B Paulsen T et al Diagnosis and treatment of borderline ovarian neoplasms lsquothe state of the artrsquo Eur J Gynaecol Oncol 2009 30 471ndash482
15 Kurman RJ amp Shih IeM Pathogenesis of ovarian cancer lessons from morphology and molecular biology and their clinicalimplications Int J Gynecol Pathol 2008 27 151ndash160
16 Kurman RJ Visvanathan K Roden R et al Early detection and treatment of ovarian cancer shifting from early stage tominimal volume of disease based on a new model of carcinogenesis Am J Obstet Gynecol 2008 198 351ndash356
17 Shih IeM amp Kurman RJ Ovarian tumorigenesis a proposed model based on morphological and molecular genetic analysis Am J Pathol 2004 164 1511ndash1518
18 Levanon K Crum C amp Drapkin R New insights into the pathogenesis of serous ovarian cancer and its clinical impact J ClinOncol 2008 26 5284ndash5293
19 Meinhold-Heerlein I Bauerschlag D Hilpert F et al Molecular and prognostic distinction between serous ovarian carci-nomas of varying grade and malignant potential Oncogene 2005 24 1053ndash1065
20 Bonome T Lee JY Park DC et al Expression pro1047297ling of serous low malignant potential low-grade and high-grade tumorsof the ovary Cancer Res 2005 65 10602ndash10612
21 Mahner S Baasch C Schwarz J et al C-Fos expression is a molecular predictor of progression and survival in epithelialovarian carcinoma Br J Cancer 2008 99 1269ndash1275
22 Ortiz BH Ailawadi M Colitti C et al Second primary or recurrence Comparative patterns of p53 and K-ras mutationssuggest that serous borderline ovarian tumors and subsequent serous carcinomas are unrelated tumors Cancer Res 200161 7264ndash7267
23 Lee KR Tavassoli FA Prat J et al Tumours of the ovary and peritoneum In Tavassoli FA amp Devilee P (eds) Pathology and
genetics Tumours of the breast and female genital organs Lyon IARC Press 2003 pp 113ndash20224 Oedegaard E Ovarian carcinomas and borderline ovarian tumors - molecular markers and operative treatment Dissertation
Facutly of Medicine University of Oslo 200825 Mok SC Bell DA Knapp RC et al Mutation of K-ras protooncogene in human ovarian epithelial tumors of borderline
malignancy Cancer Res 1993 53 1489ndash149226 du Bois A Ewald-Riegler N du Bois O et al Borderline tumors of the ovary a systematic review [German] Geburtsh
Frauenheilk 2009 69 807ndash83327 Seidman JD Horkayne-Szakaly I Haiba M et al The histologic type and stage distribution of ovarian carcinomas of surface
epithelial origin Int J Gynecol Pathol 2004 23 41ndash44
28 Prat J amp De Nictolis M Serous borderline tumors of the ovary a long-term follow-up study of 137 cases including 18 witha micropapillary pattern and 20 with microinvasion Am J Surg Pathol 2002 26 1111ndash1128
29 Bell DA Weinstock MA amp Scully RE Peritoneal implants of ovarian serous borderline tumors Histologic features andprognosis Cancer 1988 62 2212ndash2222
30 Tinelli R Tinelli A Tinelli FG et al Conservative surgery for borderline ovarian tumors a review Gynecol Oncol 2006 100
185ndash191
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336334
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1112
31 Kurman RJ amp Trimble CL The behavior of serous tumors of low malignant potential are they ever malignant Int J Gynecol
Pathol 1993 12 120ndash12732 Morice P Camatte S Rey A et al Prognostic factors for patients with advanced stage serous borderline tumours of the
ovary Ann Oncol 2003 14 592ndash59833 Bradley RF Stewart 4th JH Russell GB et al Pseudomyxoma peritonei of appendiceal origin a clinicopathologic analysis of
101 patients uniformly treated at a single institution with literature review Am J Surg Pathol 2006 30 551ndash559
34 Silva EG Gershenson DM Malpica A et al The recurrence and the overall survival rates of ovarian serous borderlineneoplasms with noninvasive implants is time dependent Am J Surg Pathol 2006 30 1367ndash137135 Seidman JD amp Kurman RJ Ovarian serous borderline tumors a critical review of the literature with emphasis on prognostic
indicators Hum Pathol 2000 31 539ndash55736 Chang SJ Ryu HS Chang KH et al Prognostic signi1047297cance of the micropapillary pattern in patients with serous borderline
ovarian tumors Acta Obstet Gynecol Scand 2008 87 476ndash48137 Fox H amp Wells M Surface epithelialstromal tumors of the ovary In Fox H amp Wells M (eds) Haines and Taylor Obstetrical and
Gynaecological Pathology 5th ed London Churchill Livingstone 2003 pp 713ndash74338 Ren J Peng Z amp Yang K A clinicopathologic multivariate analysis affecting recurrence of borderline ovarian tumors Gynecol
Oncol 2008 110 162ndash16739 Longacre TA McKenney JK Tazelaar HD et al Ovarian serous tumors of low malignant potential (borderline tumors)
outcome-based study of 276 patients with long-term (gt or frac145-year) follow-up Am J Surg Pathol 2005 29 707ndash72340 Cusidoacute M Balagueroacute L Hernandez G et al Results of the national survey of borderline ovarian tumors in Spain Gynecol
Oncol 2007 104 617ndash62241 Kaern J Tropeacute CG Kristensen GB et al DNA ploidy the most important prognostic factor in patients with borderline
tumors of the ovary Int J Gynecol Cancer 1993 3 349ndash35842 Meyer JS Gersell DJ amp Yim S Cell proliferation in ovarian carcinoma superior accuracy of S-phase fraction (SPF) by DNA
labeling index versus 1047298ow cytometric SPF lack of independent prognostic power for SPF and DNA ploidy and limitedeffect of SPF on tumor growth rate Gynecol Oncol 2001 81 466ndash476
43 Verbruggen MB van Diest PJ Baak JP et al The prognostic and clinical value of morphometry and DNA cytometry inborderline ovarian tumors a prospective study Int J Gynecol Pathol 2009 28 35ndash40
44 Yokoyama Y Moriya T Takano T et al Clinical outcome and risk factors for recurrence in borderline ovarian tumours Br J Cancer 2006 94 1586ndash1591
45 Leake JF Rader JS Woodruff JD et al Retroperitoneal lymphatic involvement with epithelial ovarian tumors of lowmalignant potential Gynecol Oncol 1991 42 124ndash130
46 Paulsen T Kaern J Kjaerheim K et al Symptoms and referral of women with epithelial ovarian tumors Int J Gynaecol Obstet 2005 88 31ndash37
47 Paulsen T Epithelial ovarian cancer A clinical epidemiological approach on diagnosis and treatment Dissertation Faculty of Medicine University of Oslo 2007
48 Tropeacute CG Kristensen G amp Makar A Surgery for borderline tumor of the ovary Semin Surg Oncol 2000 19 69ndash7549 Tempfer CB Polterauer S Bentz EK et al Accuracy of intraoperative frozen section analysis in borderline tumors of the
ovary a retrospective analysis of 96 cases and review of the literature Gynecol Oncol 2007 107 248ndash25250 Camatte S Morice P Thoury A et al Impact of surgical staging in patients with macroscopic lsquostage Irsquo ovarian borderline
tumours analysis of a continuous series of 101 cases Eur J Cancer 2004 40 1842ndash184951 Cadron I Leunen K Van Gorp T et al Management of borderline ovarian neoplasms J Clin Oncol 2007 25 2928ndash293752 Snider DD Stuart GC Nation JG et al Evaluation of surgical staging in stage I low malignant potential ovarian tumors
Gynecol Oncol 1991 40 129ndash13253 Ronnett BM Kurman RJ Zahn CM et al Pseudomyxoma peritonei in women a clinicopathologic analysis of 30 cases with
emphasis on site of origin prognosis and relationship to ovarian mucinous tumors of low malignant potential Hum Pathol
1995 26 509ndash52454 Seidman JD Elsayed AM Sobin LH et al Association of mucinous tumors of the ovary and appendix A clinicopathologic
study of 25 cases Am J Surg Pathol 1993 17 22ndash3455 Trimble EL amp Trimble LC Epithelial ovarian tumors of low malignant potential In Markman M amp Hoskins W (eds) Cancer
of the Ovary New York Raven Press 1993 pp 415ndash429
56 Zanetta G Rota S Chiari S et al Behavior of borderline tumors with particular interest to persistence recurrence andprogression to invasive carcinoma a prospective study J Clin Oncol 2001 19 2658ndash266457 Fauvet R Boccara J Dufournet C et al Restaging surgery for women with borderline ovarian tumors results of a French
multicenter study Cancer 2004 100 1145ndash115158 Zapardiel I Rosenberg P Peiretti M et al The role of restaging borderline ovarian tumors single institution experience and
review of the literature Gynecol Oncol 2010 119 274ndash27759 Def 1047297eux X Morice P Camatte S et al Results after laparoscopic management of serous borderline tumor of the ovary with
peritoneal implants Gynecol Oncol 2005 97 84ndash8960 Fauvet R Boccara J Dufournet C et al Laparoscopic management of borderline ovarian tumors results of a French
multicenter study Ann Oncol 2005 16 403ndash41061 Vandenput I Amant F amp Vergote I Peritoneal recurrences might be less common in advanced stage serous borderline
ovarian tumors that were treated by laparotomy Gynecol Oncol 2005 98 52362 CadronI Amant F VanGorp Tet alThe management of borderline tumours of theovary Curr Opin Oncol 2006 18 488ndash49363 Vergote I De Brabanter J Fyles A et al Prognostic importance of degree of differentiation and cyst rupture in stage I
invasive epithelial ovarian carcinoma Lancet 2001 357 176ndash182
64 Gershenson DM amp Silva EG Serous ovarian tumors of low malignant potential with peritoneal implants Cancer 1990 65578ndash585
65 Gershenson DM Clinical management potential tumours of low malignancy Best Pract Res Clin Obstet Gynaecol 2002 16513ndash527
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 335
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1212
66 Heintz AP Odicino F Maisonneuve P et al Carcinoma of the ovary FIGO 26th Annual Report on the Results of Treatment inGynecological Cancer Int J Gynaecol Obstet 2006 95(Suppl 1) S161ndashS192
67 Bjoslashrge T Engeland A Hansen S et al Prognosis of patients with ovarian cancer and borderline tumours diagnosed inNorway between 1954 and 1993 Int J Cancer 1998 75 663ndash670
68 Seidman JD amp Kurman RJ Subclassi1047297cation of serous borderline tumors of the ovary into benign and malignant typesA clinicopathologic study of 65 advanced stage cases Am J Surg Pathol 1996 20 1331ndash1345
69 Sherman ME Berman J Birrer MJ et al Current challenges and opportunities for research on borderline ovarian tumorsHum Pathol 2004 35 961ndash97070 Leake JF Currie JL Rosenshein NB et al Long-term follow-up of serous ovarian tumors of low malignant potential Gynecol
Oncol 1992 47 150ndash15871 Lim-Tan SK Cajigas HE amp Scully RE Ovarian cystectomy for serous borderline tumors a follow-up study of 35 cases Obstet
Gynecol 1988 72 775ndash78172 Morice P Camatte S El Hassan J et al Clinical outcomes and fertility after conservative treatment of ovarian borderline
tumors Fertil Steril 2001 75 92ndash9673 Camatte S Morice P Pautier P et al Fertility results after conservative treatment of advanced stage serous borderline
tumour of the ovary BJOG 2002 109 376ndash38074 Crispens MA Bodurka D Deavers M et al Response and survival in patients with progressive or recurrent serous ovarian
tumors of low malignant potential Obstet Gynecol 2002 99 3ndash1075 Fauvet R Poncelet C Boccara J et al Fertility after conservative treatment for borderline ovarian tumors a French
multicenter study Fertil Steril 2005 83 284ndash29076 Morris RT Gershenson DM Silva EG et al Outcome and reproductive function after conservative surgery for borderline
ovarian tumors Obstet Gynecol 2000 95 541ndash54777 Gotlieb WH Flikker S Davidson B et al Borderline tumors of the ovary fertility treatment conservative management and
pregnancy outcome Cancer 1998 82 141ndash14678 Maltaris T Boehm D Dittrich R et al Reproduction beyond cancer a message of hope for young women Gynecol Oncol
2006 103 1109ndash112179 Beiner ME Gotlieb WH Davidson B et al Infertility treatment after conservative management of borderline ovarian
tumors Cancer 2001 92 320ndash32580 Fasouliotis SJ Davis O Schattman G et al Safety and ef 1047297cacy of infertility treatment after conservative management of
borderline ovarian tumors a preliminary report Fertil Steril 2004 82 568ndash57281 Kashyap S amp Davis OK Ovarian cancer and fertility medications a critical appraisal Semin Reprod Med 2003 21 65ndash7182 Morice P Camatte S Wicart-Poque F et al Results of conservative management of epithelial malignant and borderline
ovarian tumours Hum Reprod Update 2003 9 185ndash19283 Whittemore AS Harris R amp Itnyre J Characteristics relating to ovarian cancer risk collaborative analysis of 12 US case-
control studies II Invasive epithelial ovarian cancers in white women Collaborative Ovarian Cancer Group Am J Epi-demiol 1992 136 1184ndash1203
84 Fortin A Morice P Thoury A et al Impact of infertility drugs after treatment of borderline ovarian tumors results of a retrospective multicenter study Fertil Steril 2007 87 591ndash596
85 Burger CW van de Swaluw A Mooij TM et al Risk of borderline and invasive ovarian tumors after ovarian stimulation forin vitro fertilization in a large Dutch cohort after 15 years of follow-up Abstracts presented for the 40th Annual Meeting of the Society of Gynecologic Oncologists February 2009 (abstract no 6) Gynecol Oncol 2009 112(Suppl) S4
86 Donnez J Dolmans MM Demylle D et al Livebirth after orthotopic transplantation of cryopreserved ovarian tissue Lancet 2004 364 1405ndash1410
87 Lee DM Yeoman RR Battaglia DE et al Live birth after ovarian tissue transplant Nature 2004 428 137ndash138
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336336

7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 812
drugs for infertility after conservative surgery Thirteen pregnancies were observed Disease in four
women recurred All recurrences were BOT on a remaining ovary that had been treated by surgery
alone All women are currently disease-free after secondary surgery Fortin et al84 concluded that IVF
drugs can be used safely in womenwho develop infertility after conservative treatment of BOT Because
of the low number of women treated with IVF drugs Norwegian Radium Hospital guidelines are to
proceed with caution and only women with early stage BOT are permitted to be treated with IVF drugsThe latest development regarding reproduction and BOT is cryopreservation 86 Women who have
their ovaries removed because of large stage Ib BOT now have a possibility of becoming pregnant
Biopsies from normal ovarian cortex can be taken during the primary operation In 2004 a live birth
after a fresh ovarian tissue transplant in a primate was reported87 Donnez et al86 described in 2004
a live birth after orthotopic auto-transplantation of cryopreserved ovarian tissue Their1047297ndings opened
new possibilities for young women facing premature ovarian failure
Women with reduced fertility after surgery can consider ovarian stimulation egg retrieval and egg
freezing Ovarian stimulation and exposure to high oestrogen exposure do not seem to increase the risk
for recurrence Nor do pregnancies have negative in1047298uence on survival7277
To assure future fertility preservation in women with BOT the gynaecologic oncologist should
collaborate closely with the reproductive endocrinologists even before surgery Until more mature dataexist the general recommendation is a limited number of stimulation cycles only for stage I patients In
case of bilateral salpingo-oophorectomy cryopreservation of ovarian cortex biopsy from the less
affected ovary could be considered although this is not always technically possible1151
Follow up
Follow up should be long term and lifelong because recurrences may develop after more than 15 years
In conservatively treated womenclose follow up is crucial with special attentionto theremainingovaryIt
is still debated if the remaining ovary (and uterus) should be removed after the family is completed For
low-risk BOT there is no indication for this procedure but in women with high-risk of recurrence the
procedure is optional the alternative being to wait until recurrence or carry out radical surgery Manywomen will choose radical surgery when the family is completed because of psychological stress
The general recommendation is follow up every 3 months during the 1047297rst 2 years and then every 6
months for the next 3 years and annually thereafter The women is followed with pelvic examination
transvaginal ultrasound and calcium 125 measurement1451 (Fig 2)
Future direction of borderline ovarian tumour
A key issue for future research on BOTconcerning epidemiology is the identi1047297cation of risk factors for
invasive implants recurrences and death and also the identi1047297cation of predisposing heritable factors
For clinical management improved methods for preoperative and intraoperative diagnosis should
be considered in addition to the role of laparoscopic surgery in removal of complex cysts improvedmethods for distinguishing metastases from BOT and determination of risk associated with conser-
vative treatment
For pathology and molecular biology molecular studies are needed to assess the relationship
between serous BOT low-grade serous carcinoma and high-grade serous carcinoma Molecular studies
are also needed to aid in the characterisation of implants and studies need to be conducted to
determine the biology of microinvasive BOT and the clinical signi1047297cance of long-term follow up
Conclusion
Borderline ovarian tumours are ovarian tumours with good prognosis that account for 10ndash20 of all
epithelial ovarian cancer Historically standard primarysurgeryincludedbilateral salpingo-oophorectomyomentectomy peritoneal washing and complete peritoneal resection of macroscopic lesions or multiple
biopsies In cases of M-BOT women are also treated with appendectomy As one-third of BOT are diagnosed
inwomenyounger than40 years however fertility-sparingtreatment (ie preservation of the uterus andat
least part of one ovary) has been increasingly used in the past 10 years Fertility drugs are well tolerated in
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336332
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 912
women with infertility after fertility-sparing surgery Careful selection of candidates is necessary Lapa-
roscopic techniques can be used but are reserved for oncologic surgeons This conservative treatment
increases therateof recurrencebutwithoutany effecton survivalThespontaneouspregnancy rate is nearly
50and most are achieved spontaneously Spontaneous pregnancy can occurafter conservative treatment
of advanced-stage BOT (with non-invasive implants) These women should be closely followed up Further
research has to concentrate on clinical risk-factors histopathological markers and pathogenesis to guar-antee the best clinical management for women with BOT
Con1047298ict of interest statement
None declared
Practice points
BOTare ovarian tumours with good prognosis that account for 10ndash20 of all epithelial ovarian
cancer Historically standard primary surgery included bilateral salpingo-oophorectomy omentec-
tomy peritoneal washing and complete peritoneal resection of macroscopic lesions or
multiple biopsies
In case of mucinous BOT women are also treated with appendectomy
Adjuvant therapy for the treatment of BOT has no proven bene1047297t
As one-third of BOT are diagnosed in women younger than 40 years fertility-sparing treat-
ment (ie preservation of the uterus and at least part of one ovary) has been increasingly used
in the past 10 years
Fertility drugs are well tolerated in women with infertility after fertility-sparing surgery
Careful selection of candidates is necessary
Laparoscopic techniques can be used but are reserved for oncologic surgeons Spontaneous pregnancy can occur after conservative treatment of advanced stage BOT (with
non-invasive implants)
These women should be closely followed up
Research agenda
Epidemiology
Identify risk factors for invasive implants recurrences and death
Identify predisposing heritable factors
Clinical management
Improve methods for preoperative and intraoperative diagnosis
Further explore the role of laparoscopic surgery in the removal of complex cysts
Improve methods for distinguishing metastases from BOTand determine risk associated with
conservative treatment
Pathology and molecular biology
Conduct molecular studies to assess the relationship between serous BOT low-grade serous
carcinoma and high-grade serous carcinoma Conduct molecular studies to aid in the characterisation of implants
Conduct studies to determine the biology of microinvasive BOTand the clinical signi1047297cance of
long-term follow up
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 333
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1012
Acknowledgement
We wish to thank Mrs Gry Seppola for technical assistance and gratefully acknowledge the1047297nancial
support from the Inger and John Fredriksen Foundation for Ovarian Cancer Research
References
1 Taylor HC Malignant and semi-malignant tumors of the ovary Surg Gynecol Obstet 1929 48 204ndash2302 Kottmeier HL Kolstad P McGarrity KA Annual report on results of treatment in gynaecologic cancer vol 17 Statements of
results obtained in 1969ndash1972 inclusive FIGO Stockholm Sweden Editorial of 1047297ce Radiumhemmet 19733 Serov SF Scully RE amp Sobin LH International histological classi 1047297cation of tumors no 9 Histoloigcal typing of ovarian tumours
Geneval World Health Organization 19734 Hart WR amp Norris HJ Borderline and malignant mucinous tumors of the ovary Histologic criteria and clinical behavior
Cancer 1973 31 1031ndash10455 Scully RE Tumors of the ovary and maldeveloped gonads Fascicle 16 In Atlas of tumor pathology Second series Wash-
ington DC Armed Forces Institute of Pathology 1979 pp 75ndash906 Lenhard MS Mitterer S Kuumlmper C et al Long-term follow-up after ovarian borderline tumor relapse and survival in
a large patient cohort Eur J Obstet Gynecol Reprod Biol 2009 145 189ndash194
7 Quirk JT amp Natarajan N Ovarian cancer incidence in the United States 1992ndash
1999 Gynecol Oncol 2005 97 519ndash
5238 Kaern J Tropeacute CG amp Abeler VM A retrospective study of 370 borderline tumors of the ovary treated at the NorwegianRadium Hospital from 1970 to 1982 A review of clinicopathologic features and treatment modalities Cancer 1993 711810ndash1820
9 Bjoslashrge T Engeland A Hansen S et al Trends in the incidence of ovarian cancer and borderline tumours in Norway1954ndash1993 Int J Cancer 1997 71 780ndash786
10 Skiacuternisdoacutettir I Garmo H Wilander E et al Borderline ovarian tumors in Sweden 1960ndash2005 trends in incidence and age atdiagnosis compared to ovarian cancer Int J Cancer 2008 123 1897ndash1901
11 Trillsch F Mahner S Ruetzel J et al Clinical management of borderline ovarian tumors Expert Rev Anticancer Ther 2010 101115ndash1124
12 Sherman ME Mink PJ Curtis R et al Survival among women with borderline ovarian tumors and ovarian carcinomaa population-based analysis Cancer 2004 100 1045ndash1052
13 Kramer JL Greene MH Epidemiology of ovarian fallopian tube and primary peritoneal cancer In Gershenson DMMcGuire WP Gore M et al eds Gynecologic cancer Controversies in management 1st ed Philadelphia Elsevier ChurchillLivingstone 2004 pp 327ndash340
14 Tropeacute C Davidson B Paulsen T et al Diagnosis and treatment of borderline ovarian neoplasms lsquothe state of the artrsquo Eur J Gynaecol Oncol 2009 30 471ndash482
15 Kurman RJ amp Shih IeM Pathogenesis of ovarian cancer lessons from morphology and molecular biology and their clinicalimplications Int J Gynecol Pathol 2008 27 151ndash160
16 Kurman RJ Visvanathan K Roden R et al Early detection and treatment of ovarian cancer shifting from early stage tominimal volume of disease based on a new model of carcinogenesis Am J Obstet Gynecol 2008 198 351ndash356
17 Shih IeM amp Kurman RJ Ovarian tumorigenesis a proposed model based on morphological and molecular genetic analysis Am J Pathol 2004 164 1511ndash1518
18 Levanon K Crum C amp Drapkin R New insights into the pathogenesis of serous ovarian cancer and its clinical impact J ClinOncol 2008 26 5284ndash5293
19 Meinhold-Heerlein I Bauerschlag D Hilpert F et al Molecular and prognostic distinction between serous ovarian carci-nomas of varying grade and malignant potential Oncogene 2005 24 1053ndash1065
20 Bonome T Lee JY Park DC et al Expression pro1047297ling of serous low malignant potential low-grade and high-grade tumorsof the ovary Cancer Res 2005 65 10602ndash10612
21 Mahner S Baasch C Schwarz J et al C-Fos expression is a molecular predictor of progression and survival in epithelialovarian carcinoma Br J Cancer 2008 99 1269ndash1275
22 Ortiz BH Ailawadi M Colitti C et al Second primary or recurrence Comparative patterns of p53 and K-ras mutationssuggest that serous borderline ovarian tumors and subsequent serous carcinomas are unrelated tumors Cancer Res 200161 7264ndash7267
23 Lee KR Tavassoli FA Prat J et al Tumours of the ovary and peritoneum In Tavassoli FA amp Devilee P (eds) Pathology and
genetics Tumours of the breast and female genital organs Lyon IARC Press 2003 pp 113ndash20224 Oedegaard E Ovarian carcinomas and borderline ovarian tumors - molecular markers and operative treatment Dissertation
Facutly of Medicine University of Oslo 200825 Mok SC Bell DA Knapp RC et al Mutation of K-ras protooncogene in human ovarian epithelial tumors of borderline
malignancy Cancer Res 1993 53 1489ndash149226 du Bois A Ewald-Riegler N du Bois O et al Borderline tumors of the ovary a systematic review [German] Geburtsh
Frauenheilk 2009 69 807ndash83327 Seidman JD Horkayne-Szakaly I Haiba M et al The histologic type and stage distribution of ovarian carcinomas of surface
epithelial origin Int J Gynecol Pathol 2004 23 41ndash44
28 Prat J amp De Nictolis M Serous borderline tumors of the ovary a long-term follow-up study of 137 cases including 18 witha micropapillary pattern and 20 with microinvasion Am J Surg Pathol 2002 26 1111ndash1128
29 Bell DA Weinstock MA amp Scully RE Peritoneal implants of ovarian serous borderline tumors Histologic features andprognosis Cancer 1988 62 2212ndash2222
30 Tinelli R Tinelli A Tinelli FG et al Conservative surgery for borderline ovarian tumors a review Gynecol Oncol 2006 100
185ndash191
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336334
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1112
31 Kurman RJ amp Trimble CL The behavior of serous tumors of low malignant potential are they ever malignant Int J Gynecol
Pathol 1993 12 120ndash12732 Morice P Camatte S Rey A et al Prognostic factors for patients with advanced stage serous borderline tumours of the
ovary Ann Oncol 2003 14 592ndash59833 Bradley RF Stewart 4th JH Russell GB et al Pseudomyxoma peritonei of appendiceal origin a clinicopathologic analysis of
101 patients uniformly treated at a single institution with literature review Am J Surg Pathol 2006 30 551ndash559
34 Silva EG Gershenson DM Malpica A et al The recurrence and the overall survival rates of ovarian serous borderlineneoplasms with noninvasive implants is time dependent Am J Surg Pathol 2006 30 1367ndash137135 Seidman JD amp Kurman RJ Ovarian serous borderline tumors a critical review of the literature with emphasis on prognostic
indicators Hum Pathol 2000 31 539ndash55736 Chang SJ Ryu HS Chang KH et al Prognostic signi1047297cance of the micropapillary pattern in patients with serous borderline
ovarian tumors Acta Obstet Gynecol Scand 2008 87 476ndash48137 Fox H amp Wells M Surface epithelialstromal tumors of the ovary In Fox H amp Wells M (eds) Haines and Taylor Obstetrical and
Gynaecological Pathology 5th ed London Churchill Livingstone 2003 pp 713ndash74338 Ren J Peng Z amp Yang K A clinicopathologic multivariate analysis affecting recurrence of borderline ovarian tumors Gynecol
Oncol 2008 110 162ndash16739 Longacre TA McKenney JK Tazelaar HD et al Ovarian serous tumors of low malignant potential (borderline tumors)
outcome-based study of 276 patients with long-term (gt or frac145-year) follow-up Am J Surg Pathol 2005 29 707ndash72340 Cusidoacute M Balagueroacute L Hernandez G et al Results of the national survey of borderline ovarian tumors in Spain Gynecol
Oncol 2007 104 617ndash62241 Kaern J Tropeacute CG Kristensen GB et al DNA ploidy the most important prognostic factor in patients with borderline
tumors of the ovary Int J Gynecol Cancer 1993 3 349ndash35842 Meyer JS Gersell DJ amp Yim S Cell proliferation in ovarian carcinoma superior accuracy of S-phase fraction (SPF) by DNA
labeling index versus 1047298ow cytometric SPF lack of independent prognostic power for SPF and DNA ploidy and limitedeffect of SPF on tumor growth rate Gynecol Oncol 2001 81 466ndash476
43 Verbruggen MB van Diest PJ Baak JP et al The prognostic and clinical value of morphometry and DNA cytometry inborderline ovarian tumors a prospective study Int J Gynecol Pathol 2009 28 35ndash40
44 Yokoyama Y Moriya T Takano T et al Clinical outcome and risk factors for recurrence in borderline ovarian tumours Br J Cancer 2006 94 1586ndash1591
45 Leake JF Rader JS Woodruff JD et al Retroperitoneal lymphatic involvement with epithelial ovarian tumors of lowmalignant potential Gynecol Oncol 1991 42 124ndash130
46 Paulsen T Kaern J Kjaerheim K et al Symptoms and referral of women with epithelial ovarian tumors Int J Gynaecol Obstet 2005 88 31ndash37
47 Paulsen T Epithelial ovarian cancer A clinical epidemiological approach on diagnosis and treatment Dissertation Faculty of Medicine University of Oslo 2007
48 Tropeacute CG Kristensen G amp Makar A Surgery for borderline tumor of the ovary Semin Surg Oncol 2000 19 69ndash7549 Tempfer CB Polterauer S Bentz EK et al Accuracy of intraoperative frozen section analysis in borderline tumors of the
ovary a retrospective analysis of 96 cases and review of the literature Gynecol Oncol 2007 107 248ndash25250 Camatte S Morice P Thoury A et al Impact of surgical staging in patients with macroscopic lsquostage Irsquo ovarian borderline
tumours analysis of a continuous series of 101 cases Eur J Cancer 2004 40 1842ndash184951 Cadron I Leunen K Van Gorp T et al Management of borderline ovarian neoplasms J Clin Oncol 2007 25 2928ndash293752 Snider DD Stuart GC Nation JG et al Evaluation of surgical staging in stage I low malignant potential ovarian tumors
Gynecol Oncol 1991 40 129ndash13253 Ronnett BM Kurman RJ Zahn CM et al Pseudomyxoma peritonei in women a clinicopathologic analysis of 30 cases with
emphasis on site of origin prognosis and relationship to ovarian mucinous tumors of low malignant potential Hum Pathol
1995 26 509ndash52454 Seidman JD Elsayed AM Sobin LH et al Association of mucinous tumors of the ovary and appendix A clinicopathologic
study of 25 cases Am J Surg Pathol 1993 17 22ndash3455 Trimble EL amp Trimble LC Epithelial ovarian tumors of low malignant potential In Markman M amp Hoskins W (eds) Cancer
of the Ovary New York Raven Press 1993 pp 415ndash429
56 Zanetta G Rota S Chiari S et al Behavior of borderline tumors with particular interest to persistence recurrence andprogression to invasive carcinoma a prospective study J Clin Oncol 2001 19 2658ndash266457 Fauvet R Boccara J Dufournet C et al Restaging surgery for women with borderline ovarian tumors results of a French
multicenter study Cancer 2004 100 1145ndash115158 Zapardiel I Rosenberg P Peiretti M et al The role of restaging borderline ovarian tumors single institution experience and
review of the literature Gynecol Oncol 2010 119 274ndash27759 Def 1047297eux X Morice P Camatte S et al Results after laparoscopic management of serous borderline tumor of the ovary with
peritoneal implants Gynecol Oncol 2005 97 84ndash8960 Fauvet R Boccara J Dufournet C et al Laparoscopic management of borderline ovarian tumors results of a French
multicenter study Ann Oncol 2005 16 403ndash41061 Vandenput I Amant F amp Vergote I Peritoneal recurrences might be less common in advanced stage serous borderline
ovarian tumors that were treated by laparotomy Gynecol Oncol 2005 98 52362 CadronI Amant F VanGorp Tet alThe management of borderline tumours of theovary Curr Opin Oncol 2006 18 488ndash49363 Vergote I De Brabanter J Fyles A et al Prognostic importance of degree of differentiation and cyst rupture in stage I
invasive epithelial ovarian carcinoma Lancet 2001 357 176ndash182
64 Gershenson DM amp Silva EG Serous ovarian tumors of low malignant potential with peritoneal implants Cancer 1990 65578ndash585
65 Gershenson DM Clinical management potential tumours of low malignancy Best Pract Res Clin Obstet Gynaecol 2002 16513ndash527
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 335
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1212
66 Heintz AP Odicino F Maisonneuve P et al Carcinoma of the ovary FIGO 26th Annual Report on the Results of Treatment inGynecological Cancer Int J Gynaecol Obstet 2006 95(Suppl 1) S161ndashS192
67 Bjoslashrge T Engeland A Hansen S et al Prognosis of patients with ovarian cancer and borderline tumours diagnosed inNorway between 1954 and 1993 Int J Cancer 1998 75 663ndash670
68 Seidman JD amp Kurman RJ Subclassi1047297cation of serous borderline tumors of the ovary into benign and malignant typesA clinicopathologic study of 65 advanced stage cases Am J Surg Pathol 1996 20 1331ndash1345
69 Sherman ME Berman J Birrer MJ et al Current challenges and opportunities for research on borderline ovarian tumorsHum Pathol 2004 35 961ndash97070 Leake JF Currie JL Rosenshein NB et al Long-term follow-up of serous ovarian tumors of low malignant potential Gynecol
Oncol 1992 47 150ndash15871 Lim-Tan SK Cajigas HE amp Scully RE Ovarian cystectomy for serous borderline tumors a follow-up study of 35 cases Obstet
Gynecol 1988 72 775ndash78172 Morice P Camatte S El Hassan J et al Clinical outcomes and fertility after conservative treatment of ovarian borderline
tumors Fertil Steril 2001 75 92ndash9673 Camatte S Morice P Pautier P et al Fertility results after conservative treatment of advanced stage serous borderline
tumour of the ovary BJOG 2002 109 376ndash38074 Crispens MA Bodurka D Deavers M et al Response and survival in patients with progressive or recurrent serous ovarian
tumors of low malignant potential Obstet Gynecol 2002 99 3ndash1075 Fauvet R Poncelet C Boccara J et al Fertility after conservative treatment for borderline ovarian tumors a French
multicenter study Fertil Steril 2005 83 284ndash29076 Morris RT Gershenson DM Silva EG et al Outcome and reproductive function after conservative surgery for borderline
ovarian tumors Obstet Gynecol 2000 95 541ndash54777 Gotlieb WH Flikker S Davidson B et al Borderline tumors of the ovary fertility treatment conservative management and
pregnancy outcome Cancer 1998 82 141ndash14678 Maltaris T Boehm D Dittrich R et al Reproduction beyond cancer a message of hope for young women Gynecol Oncol
2006 103 1109ndash112179 Beiner ME Gotlieb WH Davidson B et al Infertility treatment after conservative management of borderline ovarian
tumors Cancer 2001 92 320ndash32580 Fasouliotis SJ Davis O Schattman G et al Safety and ef 1047297cacy of infertility treatment after conservative management of
borderline ovarian tumors a preliminary report Fertil Steril 2004 82 568ndash57281 Kashyap S amp Davis OK Ovarian cancer and fertility medications a critical appraisal Semin Reprod Med 2003 21 65ndash7182 Morice P Camatte S Wicart-Poque F et al Results of conservative management of epithelial malignant and borderline
ovarian tumours Hum Reprod Update 2003 9 185ndash19283 Whittemore AS Harris R amp Itnyre J Characteristics relating to ovarian cancer risk collaborative analysis of 12 US case-
control studies II Invasive epithelial ovarian cancers in white women Collaborative Ovarian Cancer Group Am J Epi-demiol 1992 136 1184ndash1203
84 Fortin A Morice P Thoury A et al Impact of infertility drugs after treatment of borderline ovarian tumors results of a retrospective multicenter study Fertil Steril 2007 87 591ndash596
85 Burger CW van de Swaluw A Mooij TM et al Risk of borderline and invasive ovarian tumors after ovarian stimulation forin vitro fertilization in a large Dutch cohort after 15 years of follow-up Abstracts presented for the 40th Annual Meeting of the Society of Gynecologic Oncologists February 2009 (abstract no 6) Gynecol Oncol 2009 112(Suppl) S4
86 Donnez J Dolmans MM Demylle D et al Livebirth after orthotopic transplantation of cryopreserved ovarian tissue Lancet 2004 364 1405ndash1410
87 Lee DM Yeoman RR Battaglia DE et al Live birth after ovarian tissue transplant Nature 2004 428 137ndash138
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336336

7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 912
women with infertility after fertility-sparing surgery Careful selection of candidates is necessary Lapa-
roscopic techniques can be used but are reserved for oncologic surgeons This conservative treatment
increases therateof recurrencebutwithoutany effecton survivalThespontaneouspregnancy rate is nearly
50and most are achieved spontaneously Spontaneous pregnancy can occurafter conservative treatment
of advanced-stage BOT (with non-invasive implants) These women should be closely followed up Further
research has to concentrate on clinical risk-factors histopathological markers and pathogenesis to guar-antee the best clinical management for women with BOT
Con1047298ict of interest statement
None declared
Practice points
BOTare ovarian tumours with good prognosis that account for 10ndash20 of all epithelial ovarian
cancer Historically standard primary surgery included bilateral salpingo-oophorectomy omentec-
tomy peritoneal washing and complete peritoneal resection of macroscopic lesions or
multiple biopsies
In case of mucinous BOT women are also treated with appendectomy
Adjuvant therapy for the treatment of BOT has no proven bene1047297t
As one-third of BOT are diagnosed in women younger than 40 years fertility-sparing treat-
ment (ie preservation of the uterus and at least part of one ovary) has been increasingly used
in the past 10 years
Fertility drugs are well tolerated in women with infertility after fertility-sparing surgery
Careful selection of candidates is necessary
Laparoscopic techniques can be used but are reserved for oncologic surgeons Spontaneous pregnancy can occur after conservative treatment of advanced stage BOT (with
non-invasive implants)
These women should be closely followed up
Research agenda
Epidemiology
Identify risk factors for invasive implants recurrences and death
Identify predisposing heritable factors
Clinical management
Improve methods for preoperative and intraoperative diagnosis
Further explore the role of laparoscopic surgery in the removal of complex cysts
Improve methods for distinguishing metastases from BOTand determine risk associated with
conservative treatment
Pathology and molecular biology
Conduct molecular studies to assess the relationship between serous BOT low-grade serous
carcinoma and high-grade serous carcinoma Conduct molecular studies to aid in the characterisation of implants
Conduct studies to determine the biology of microinvasive BOTand the clinical signi1047297cance of
long-term follow up
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 333
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1012
Acknowledgement
We wish to thank Mrs Gry Seppola for technical assistance and gratefully acknowledge the1047297nancial
support from the Inger and John Fredriksen Foundation for Ovarian Cancer Research
References
1 Taylor HC Malignant and semi-malignant tumors of the ovary Surg Gynecol Obstet 1929 48 204ndash2302 Kottmeier HL Kolstad P McGarrity KA Annual report on results of treatment in gynaecologic cancer vol 17 Statements of
results obtained in 1969ndash1972 inclusive FIGO Stockholm Sweden Editorial of 1047297ce Radiumhemmet 19733 Serov SF Scully RE amp Sobin LH International histological classi 1047297cation of tumors no 9 Histoloigcal typing of ovarian tumours
Geneval World Health Organization 19734 Hart WR amp Norris HJ Borderline and malignant mucinous tumors of the ovary Histologic criteria and clinical behavior
Cancer 1973 31 1031ndash10455 Scully RE Tumors of the ovary and maldeveloped gonads Fascicle 16 In Atlas of tumor pathology Second series Wash-
ington DC Armed Forces Institute of Pathology 1979 pp 75ndash906 Lenhard MS Mitterer S Kuumlmper C et al Long-term follow-up after ovarian borderline tumor relapse and survival in
a large patient cohort Eur J Obstet Gynecol Reprod Biol 2009 145 189ndash194
7 Quirk JT amp Natarajan N Ovarian cancer incidence in the United States 1992ndash
1999 Gynecol Oncol 2005 97 519ndash
5238 Kaern J Tropeacute CG amp Abeler VM A retrospective study of 370 borderline tumors of the ovary treated at the NorwegianRadium Hospital from 1970 to 1982 A review of clinicopathologic features and treatment modalities Cancer 1993 711810ndash1820
9 Bjoslashrge T Engeland A Hansen S et al Trends in the incidence of ovarian cancer and borderline tumours in Norway1954ndash1993 Int J Cancer 1997 71 780ndash786
10 Skiacuternisdoacutettir I Garmo H Wilander E et al Borderline ovarian tumors in Sweden 1960ndash2005 trends in incidence and age atdiagnosis compared to ovarian cancer Int J Cancer 2008 123 1897ndash1901
11 Trillsch F Mahner S Ruetzel J et al Clinical management of borderline ovarian tumors Expert Rev Anticancer Ther 2010 101115ndash1124
12 Sherman ME Mink PJ Curtis R et al Survival among women with borderline ovarian tumors and ovarian carcinomaa population-based analysis Cancer 2004 100 1045ndash1052
13 Kramer JL Greene MH Epidemiology of ovarian fallopian tube and primary peritoneal cancer In Gershenson DMMcGuire WP Gore M et al eds Gynecologic cancer Controversies in management 1st ed Philadelphia Elsevier ChurchillLivingstone 2004 pp 327ndash340
14 Tropeacute C Davidson B Paulsen T et al Diagnosis and treatment of borderline ovarian neoplasms lsquothe state of the artrsquo Eur J Gynaecol Oncol 2009 30 471ndash482
15 Kurman RJ amp Shih IeM Pathogenesis of ovarian cancer lessons from morphology and molecular biology and their clinicalimplications Int J Gynecol Pathol 2008 27 151ndash160
16 Kurman RJ Visvanathan K Roden R et al Early detection and treatment of ovarian cancer shifting from early stage tominimal volume of disease based on a new model of carcinogenesis Am J Obstet Gynecol 2008 198 351ndash356
17 Shih IeM amp Kurman RJ Ovarian tumorigenesis a proposed model based on morphological and molecular genetic analysis Am J Pathol 2004 164 1511ndash1518
18 Levanon K Crum C amp Drapkin R New insights into the pathogenesis of serous ovarian cancer and its clinical impact J ClinOncol 2008 26 5284ndash5293
19 Meinhold-Heerlein I Bauerschlag D Hilpert F et al Molecular and prognostic distinction between serous ovarian carci-nomas of varying grade and malignant potential Oncogene 2005 24 1053ndash1065
20 Bonome T Lee JY Park DC et al Expression pro1047297ling of serous low malignant potential low-grade and high-grade tumorsof the ovary Cancer Res 2005 65 10602ndash10612
21 Mahner S Baasch C Schwarz J et al C-Fos expression is a molecular predictor of progression and survival in epithelialovarian carcinoma Br J Cancer 2008 99 1269ndash1275
22 Ortiz BH Ailawadi M Colitti C et al Second primary or recurrence Comparative patterns of p53 and K-ras mutationssuggest that serous borderline ovarian tumors and subsequent serous carcinomas are unrelated tumors Cancer Res 200161 7264ndash7267
23 Lee KR Tavassoli FA Prat J et al Tumours of the ovary and peritoneum In Tavassoli FA amp Devilee P (eds) Pathology and
genetics Tumours of the breast and female genital organs Lyon IARC Press 2003 pp 113ndash20224 Oedegaard E Ovarian carcinomas and borderline ovarian tumors - molecular markers and operative treatment Dissertation
Facutly of Medicine University of Oslo 200825 Mok SC Bell DA Knapp RC et al Mutation of K-ras protooncogene in human ovarian epithelial tumors of borderline
malignancy Cancer Res 1993 53 1489ndash149226 du Bois A Ewald-Riegler N du Bois O et al Borderline tumors of the ovary a systematic review [German] Geburtsh
Frauenheilk 2009 69 807ndash83327 Seidman JD Horkayne-Szakaly I Haiba M et al The histologic type and stage distribution of ovarian carcinomas of surface
epithelial origin Int J Gynecol Pathol 2004 23 41ndash44
28 Prat J amp De Nictolis M Serous borderline tumors of the ovary a long-term follow-up study of 137 cases including 18 witha micropapillary pattern and 20 with microinvasion Am J Surg Pathol 2002 26 1111ndash1128
29 Bell DA Weinstock MA amp Scully RE Peritoneal implants of ovarian serous borderline tumors Histologic features andprognosis Cancer 1988 62 2212ndash2222
30 Tinelli R Tinelli A Tinelli FG et al Conservative surgery for borderline ovarian tumors a review Gynecol Oncol 2006 100
185ndash191
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336334
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1112
31 Kurman RJ amp Trimble CL The behavior of serous tumors of low malignant potential are they ever malignant Int J Gynecol
Pathol 1993 12 120ndash12732 Morice P Camatte S Rey A et al Prognostic factors for patients with advanced stage serous borderline tumours of the
ovary Ann Oncol 2003 14 592ndash59833 Bradley RF Stewart 4th JH Russell GB et al Pseudomyxoma peritonei of appendiceal origin a clinicopathologic analysis of
101 patients uniformly treated at a single institution with literature review Am J Surg Pathol 2006 30 551ndash559
34 Silva EG Gershenson DM Malpica A et al The recurrence and the overall survival rates of ovarian serous borderlineneoplasms with noninvasive implants is time dependent Am J Surg Pathol 2006 30 1367ndash137135 Seidman JD amp Kurman RJ Ovarian serous borderline tumors a critical review of the literature with emphasis on prognostic
indicators Hum Pathol 2000 31 539ndash55736 Chang SJ Ryu HS Chang KH et al Prognostic signi1047297cance of the micropapillary pattern in patients with serous borderline
ovarian tumors Acta Obstet Gynecol Scand 2008 87 476ndash48137 Fox H amp Wells M Surface epithelialstromal tumors of the ovary In Fox H amp Wells M (eds) Haines and Taylor Obstetrical and
Gynaecological Pathology 5th ed London Churchill Livingstone 2003 pp 713ndash74338 Ren J Peng Z amp Yang K A clinicopathologic multivariate analysis affecting recurrence of borderline ovarian tumors Gynecol
Oncol 2008 110 162ndash16739 Longacre TA McKenney JK Tazelaar HD et al Ovarian serous tumors of low malignant potential (borderline tumors)
outcome-based study of 276 patients with long-term (gt or frac145-year) follow-up Am J Surg Pathol 2005 29 707ndash72340 Cusidoacute M Balagueroacute L Hernandez G et al Results of the national survey of borderline ovarian tumors in Spain Gynecol
Oncol 2007 104 617ndash62241 Kaern J Tropeacute CG Kristensen GB et al DNA ploidy the most important prognostic factor in patients with borderline
tumors of the ovary Int J Gynecol Cancer 1993 3 349ndash35842 Meyer JS Gersell DJ amp Yim S Cell proliferation in ovarian carcinoma superior accuracy of S-phase fraction (SPF) by DNA
labeling index versus 1047298ow cytometric SPF lack of independent prognostic power for SPF and DNA ploidy and limitedeffect of SPF on tumor growth rate Gynecol Oncol 2001 81 466ndash476
43 Verbruggen MB van Diest PJ Baak JP et al The prognostic and clinical value of morphometry and DNA cytometry inborderline ovarian tumors a prospective study Int J Gynecol Pathol 2009 28 35ndash40
44 Yokoyama Y Moriya T Takano T et al Clinical outcome and risk factors for recurrence in borderline ovarian tumours Br J Cancer 2006 94 1586ndash1591
45 Leake JF Rader JS Woodruff JD et al Retroperitoneal lymphatic involvement with epithelial ovarian tumors of lowmalignant potential Gynecol Oncol 1991 42 124ndash130
46 Paulsen T Kaern J Kjaerheim K et al Symptoms and referral of women with epithelial ovarian tumors Int J Gynaecol Obstet 2005 88 31ndash37
47 Paulsen T Epithelial ovarian cancer A clinical epidemiological approach on diagnosis and treatment Dissertation Faculty of Medicine University of Oslo 2007
48 Tropeacute CG Kristensen G amp Makar A Surgery for borderline tumor of the ovary Semin Surg Oncol 2000 19 69ndash7549 Tempfer CB Polterauer S Bentz EK et al Accuracy of intraoperative frozen section analysis in borderline tumors of the
ovary a retrospective analysis of 96 cases and review of the literature Gynecol Oncol 2007 107 248ndash25250 Camatte S Morice P Thoury A et al Impact of surgical staging in patients with macroscopic lsquostage Irsquo ovarian borderline
tumours analysis of a continuous series of 101 cases Eur J Cancer 2004 40 1842ndash184951 Cadron I Leunen K Van Gorp T et al Management of borderline ovarian neoplasms J Clin Oncol 2007 25 2928ndash293752 Snider DD Stuart GC Nation JG et al Evaluation of surgical staging in stage I low malignant potential ovarian tumors
Gynecol Oncol 1991 40 129ndash13253 Ronnett BM Kurman RJ Zahn CM et al Pseudomyxoma peritonei in women a clinicopathologic analysis of 30 cases with
emphasis on site of origin prognosis and relationship to ovarian mucinous tumors of low malignant potential Hum Pathol
1995 26 509ndash52454 Seidman JD Elsayed AM Sobin LH et al Association of mucinous tumors of the ovary and appendix A clinicopathologic
study of 25 cases Am J Surg Pathol 1993 17 22ndash3455 Trimble EL amp Trimble LC Epithelial ovarian tumors of low malignant potential In Markman M amp Hoskins W (eds) Cancer
of the Ovary New York Raven Press 1993 pp 415ndash429
56 Zanetta G Rota S Chiari S et al Behavior of borderline tumors with particular interest to persistence recurrence andprogression to invasive carcinoma a prospective study J Clin Oncol 2001 19 2658ndash266457 Fauvet R Boccara J Dufournet C et al Restaging surgery for women with borderline ovarian tumors results of a French
multicenter study Cancer 2004 100 1145ndash115158 Zapardiel I Rosenberg P Peiretti M et al The role of restaging borderline ovarian tumors single institution experience and
review of the literature Gynecol Oncol 2010 119 274ndash27759 Def 1047297eux X Morice P Camatte S et al Results after laparoscopic management of serous borderline tumor of the ovary with
peritoneal implants Gynecol Oncol 2005 97 84ndash8960 Fauvet R Boccara J Dufournet C et al Laparoscopic management of borderline ovarian tumors results of a French
multicenter study Ann Oncol 2005 16 403ndash41061 Vandenput I Amant F amp Vergote I Peritoneal recurrences might be less common in advanced stage serous borderline
ovarian tumors that were treated by laparotomy Gynecol Oncol 2005 98 52362 CadronI Amant F VanGorp Tet alThe management of borderline tumours of theovary Curr Opin Oncol 2006 18 488ndash49363 Vergote I De Brabanter J Fyles A et al Prognostic importance of degree of differentiation and cyst rupture in stage I
invasive epithelial ovarian carcinoma Lancet 2001 357 176ndash182
64 Gershenson DM amp Silva EG Serous ovarian tumors of low malignant potential with peritoneal implants Cancer 1990 65578ndash585
65 Gershenson DM Clinical management potential tumours of low malignancy Best Pract Res Clin Obstet Gynaecol 2002 16513ndash527
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 335
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1212
66 Heintz AP Odicino F Maisonneuve P et al Carcinoma of the ovary FIGO 26th Annual Report on the Results of Treatment inGynecological Cancer Int J Gynaecol Obstet 2006 95(Suppl 1) S161ndashS192
67 Bjoslashrge T Engeland A Hansen S et al Prognosis of patients with ovarian cancer and borderline tumours diagnosed inNorway between 1954 and 1993 Int J Cancer 1998 75 663ndash670
68 Seidman JD amp Kurman RJ Subclassi1047297cation of serous borderline tumors of the ovary into benign and malignant typesA clinicopathologic study of 65 advanced stage cases Am J Surg Pathol 1996 20 1331ndash1345
69 Sherman ME Berman J Birrer MJ et al Current challenges and opportunities for research on borderline ovarian tumorsHum Pathol 2004 35 961ndash97070 Leake JF Currie JL Rosenshein NB et al Long-term follow-up of serous ovarian tumors of low malignant potential Gynecol
Oncol 1992 47 150ndash15871 Lim-Tan SK Cajigas HE amp Scully RE Ovarian cystectomy for serous borderline tumors a follow-up study of 35 cases Obstet
Gynecol 1988 72 775ndash78172 Morice P Camatte S El Hassan J et al Clinical outcomes and fertility after conservative treatment of ovarian borderline
tumors Fertil Steril 2001 75 92ndash9673 Camatte S Morice P Pautier P et al Fertility results after conservative treatment of advanced stage serous borderline
tumour of the ovary BJOG 2002 109 376ndash38074 Crispens MA Bodurka D Deavers M et al Response and survival in patients with progressive or recurrent serous ovarian
tumors of low malignant potential Obstet Gynecol 2002 99 3ndash1075 Fauvet R Poncelet C Boccara J et al Fertility after conservative treatment for borderline ovarian tumors a French
multicenter study Fertil Steril 2005 83 284ndash29076 Morris RT Gershenson DM Silva EG et al Outcome and reproductive function after conservative surgery for borderline
ovarian tumors Obstet Gynecol 2000 95 541ndash54777 Gotlieb WH Flikker S Davidson B et al Borderline tumors of the ovary fertility treatment conservative management and
pregnancy outcome Cancer 1998 82 141ndash14678 Maltaris T Boehm D Dittrich R et al Reproduction beyond cancer a message of hope for young women Gynecol Oncol
2006 103 1109ndash112179 Beiner ME Gotlieb WH Davidson B et al Infertility treatment after conservative management of borderline ovarian
tumors Cancer 2001 92 320ndash32580 Fasouliotis SJ Davis O Schattman G et al Safety and ef 1047297cacy of infertility treatment after conservative management of
borderline ovarian tumors a preliminary report Fertil Steril 2004 82 568ndash57281 Kashyap S amp Davis OK Ovarian cancer and fertility medications a critical appraisal Semin Reprod Med 2003 21 65ndash7182 Morice P Camatte S Wicart-Poque F et al Results of conservative management of epithelial malignant and borderline
ovarian tumours Hum Reprod Update 2003 9 185ndash19283 Whittemore AS Harris R amp Itnyre J Characteristics relating to ovarian cancer risk collaborative analysis of 12 US case-
control studies II Invasive epithelial ovarian cancers in white women Collaborative Ovarian Cancer Group Am J Epi-demiol 1992 136 1184ndash1203
84 Fortin A Morice P Thoury A et al Impact of infertility drugs after treatment of borderline ovarian tumors results of a retrospective multicenter study Fertil Steril 2007 87 591ndash596
85 Burger CW van de Swaluw A Mooij TM et al Risk of borderline and invasive ovarian tumors after ovarian stimulation forin vitro fertilization in a large Dutch cohort after 15 years of follow-up Abstracts presented for the 40th Annual Meeting of the Society of Gynecologic Oncologists February 2009 (abstract no 6) Gynecol Oncol 2009 112(Suppl) S4
86 Donnez J Dolmans MM Demylle D et al Livebirth after orthotopic transplantation of cryopreserved ovarian tissue Lancet 2004 364 1405ndash1410
87 Lee DM Yeoman RR Battaglia DE et al Live birth after ovarian tissue transplant Nature 2004 428 137ndash138
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336336

7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1012
Acknowledgement
We wish to thank Mrs Gry Seppola for technical assistance and gratefully acknowledge the1047297nancial
support from the Inger and John Fredriksen Foundation for Ovarian Cancer Research
References
1 Taylor HC Malignant and semi-malignant tumors of the ovary Surg Gynecol Obstet 1929 48 204ndash2302 Kottmeier HL Kolstad P McGarrity KA Annual report on results of treatment in gynaecologic cancer vol 17 Statements of
results obtained in 1969ndash1972 inclusive FIGO Stockholm Sweden Editorial of 1047297ce Radiumhemmet 19733 Serov SF Scully RE amp Sobin LH International histological classi 1047297cation of tumors no 9 Histoloigcal typing of ovarian tumours
Geneval World Health Organization 19734 Hart WR amp Norris HJ Borderline and malignant mucinous tumors of the ovary Histologic criteria and clinical behavior
Cancer 1973 31 1031ndash10455 Scully RE Tumors of the ovary and maldeveloped gonads Fascicle 16 In Atlas of tumor pathology Second series Wash-
ington DC Armed Forces Institute of Pathology 1979 pp 75ndash906 Lenhard MS Mitterer S Kuumlmper C et al Long-term follow-up after ovarian borderline tumor relapse and survival in
a large patient cohort Eur J Obstet Gynecol Reprod Biol 2009 145 189ndash194
7 Quirk JT amp Natarajan N Ovarian cancer incidence in the United States 1992ndash
1999 Gynecol Oncol 2005 97 519ndash
5238 Kaern J Tropeacute CG amp Abeler VM A retrospective study of 370 borderline tumors of the ovary treated at the NorwegianRadium Hospital from 1970 to 1982 A review of clinicopathologic features and treatment modalities Cancer 1993 711810ndash1820
9 Bjoslashrge T Engeland A Hansen S et al Trends in the incidence of ovarian cancer and borderline tumours in Norway1954ndash1993 Int J Cancer 1997 71 780ndash786
10 Skiacuternisdoacutettir I Garmo H Wilander E et al Borderline ovarian tumors in Sweden 1960ndash2005 trends in incidence and age atdiagnosis compared to ovarian cancer Int J Cancer 2008 123 1897ndash1901
11 Trillsch F Mahner S Ruetzel J et al Clinical management of borderline ovarian tumors Expert Rev Anticancer Ther 2010 101115ndash1124
12 Sherman ME Mink PJ Curtis R et al Survival among women with borderline ovarian tumors and ovarian carcinomaa population-based analysis Cancer 2004 100 1045ndash1052
13 Kramer JL Greene MH Epidemiology of ovarian fallopian tube and primary peritoneal cancer In Gershenson DMMcGuire WP Gore M et al eds Gynecologic cancer Controversies in management 1st ed Philadelphia Elsevier ChurchillLivingstone 2004 pp 327ndash340
14 Tropeacute C Davidson B Paulsen T et al Diagnosis and treatment of borderline ovarian neoplasms lsquothe state of the artrsquo Eur J Gynaecol Oncol 2009 30 471ndash482
15 Kurman RJ amp Shih IeM Pathogenesis of ovarian cancer lessons from morphology and molecular biology and their clinicalimplications Int J Gynecol Pathol 2008 27 151ndash160
16 Kurman RJ Visvanathan K Roden R et al Early detection and treatment of ovarian cancer shifting from early stage tominimal volume of disease based on a new model of carcinogenesis Am J Obstet Gynecol 2008 198 351ndash356
17 Shih IeM amp Kurman RJ Ovarian tumorigenesis a proposed model based on morphological and molecular genetic analysis Am J Pathol 2004 164 1511ndash1518
18 Levanon K Crum C amp Drapkin R New insights into the pathogenesis of serous ovarian cancer and its clinical impact J ClinOncol 2008 26 5284ndash5293
19 Meinhold-Heerlein I Bauerschlag D Hilpert F et al Molecular and prognostic distinction between serous ovarian carci-nomas of varying grade and malignant potential Oncogene 2005 24 1053ndash1065
20 Bonome T Lee JY Park DC et al Expression pro1047297ling of serous low malignant potential low-grade and high-grade tumorsof the ovary Cancer Res 2005 65 10602ndash10612
21 Mahner S Baasch C Schwarz J et al C-Fos expression is a molecular predictor of progression and survival in epithelialovarian carcinoma Br J Cancer 2008 99 1269ndash1275
22 Ortiz BH Ailawadi M Colitti C et al Second primary or recurrence Comparative patterns of p53 and K-ras mutationssuggest that serous borderline ovarian tumors and subsequent serous carcinomas are unrelated tumors Cancer Res 200161 7264ndash7267
23 Lee KR Tavassoli FA Prat J et al Tumours of the ovary and peritoneum In Tavassoli FA amp Devilee P (eds) Pathology and
genetics Tumours of the breast and female genital organs Lyon IARC Press 2003 pp 113ndash20224 Oedegaard E Ovarian carcinomas and borderline ovarian tumors - molecular markers and operative treatment Dissertation
Facutly of Medicine University of Oslo 200825 Mok SC Bell DA Knapp RC et al Mutation of K-ras protooncogene in human ovarian epithelial tumors of borderline
malignancy Cancer Res 1993 53 1489ndash149226 du Bois A Ewald-Riegler N du Bois O et al Borderline tumors of the ovary a systematic review [German] Geburtsh
Frauenheilk 2009 69 807ndash83327 Seidman JD Horkayne-Szakaly I Haiba M et al The histologic type and stage distribution of ovarian carcinomas of surface
epithelial origin Int J Gynecol Pathol 2004 23 41ndash44
28 Prat J amp De Nictolis M Serous borderline tumors of the ovary a long-term follow-up study of 137 cases including 18 witha micropapillary pattern and 20 with microinvasion Am J Surg Pathol 2002 26 1111ndash1128
29 Bell DA Weinstock MA amp Scully RE Peritoneal implants of ovarian serous borderline tumors Histologic features andprognosis Cancer 1988 62 2212ndash2222
30 Tinelli R Tinelli A Tinelli FG et al Conservative surgery for borderline ovarian tumors a review Gynecol Oncol 2006 100
185ndash191
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336334
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1112
31 Kurman RJ amp Trimble CL The behavior of serous tumors of low malignant potential are they ever malignant Int J Gynecol
Pathol 1993 12 120ndash12732 Morice P Camatte S Rey A et al Prognostic factors for patients with advanced stage serous borderline tumours of the
ovary Ann Oncol 2003 14 592ndash59833 Bradley RF Stewart 4th JH Russell GB et al Pseudomyxoma peritonei of appendiceal origin a clinicopathologic analysis of
101 patients uniformly treated at a single institution with literature review Am J Surg Pathol 2006 30 551ndash559
34 Silva EG Gershenson DM Malpica A et al The recurrence and the overall survival rates of ovarian serous borderlineneoplasms with noninvasive implants is time dependent Am J Surg Pathol 2006 30 1367ndash137135 Seidman JD amp Kurman RJ Ovarian serous borderline tumors a critical review of the literature with emphasis on prognostic
indicators Hum Pathol 2000 31 539ndash55736 Chang SJ Ryu HS Chang KH et al Prognostic signi1047297cance of the micropapillary pattern in patients with serous borderline
ovarian tumors Acta Obstet Gynecol Scand 2008 87 476ndash48137 Fox H amp Wells M Surface epithelialstromal tumors of the ovary In Fox H amp Wells M (eds) Haines and Taylor Obstetrical and
Gynaecological Pathology 5th ed London Churchill Livingstone 2003 pp 713ndash74338 Ren J Peng Z amp Yang K A clinicopathologic multivariate analysis affecting recurrence of borderline ovarian tumors Gynecol
Oncol 2008 110 162ndash16739 Longacre TA McKenney JK Tazelaar HD et al Ovarian serous tumors of low malignant potential (borderline tumors)
outcome-based study of 276 patients with long-term (gt or frac145-year) follow-up Am J Surg Pathol 2005 29 707ndash72340 Cusidoacute M Balagueroacute L Hernandez G et al Results of the national survey of borderline ovarian tumors in Spain Gynecol
Oncol 2007 104 617ndash62241 Kaern J Tropeacute CG Kristensen GB et al DNA ploidy the most important prognostic factor in patients with borderline
tumors of the ovary Int J Gynecol Cancer 1993 3 349ndash35842 Meyer JS Gersell DJ amp Yim S Cell proliferation in ovarian carcinoma superior accuracy of S-phase fraction (SPF) by DNA
labeling index versus 1047298ow cytometric SPF lack of independent prognostic power for SPF and DNA ploidy and limitedeffect of SPF on tumor growth rate Gynecol Oncol 2001 81 466ndash476
43 Verbruggen MB van Diest PJ Baak JP et al The prognostic and clinical value of morphometry and DNA cytometry inborderline ovarian tumors a prospective study Int J Gynecol Pathol 2009 28 35ndash40
44 Yokoyama Y Moriya T Takano T et al Clinical outcome and risk factors for recurrence in borderline ovarian tumours Br J Cancer 2006 94 1586ndash1591
45 Leake JF Rader JS Woodruff JD et al Retroperitoneal lymphatic involvement with epithelial ovarian tumors of lowmalignant potential Gynecol Oncol 1991 42 124ndash130
46 Paulsen T Kaern J Kjaerheim K et al Symptoms and referral of women with epithelial ovarian tumors Int J Gynaecol Obstet 2005 88 31ndash37
47 Paulsen T Epithelial ovarian cancer A clinical epidemiological approach on diagnosis and treatment Dissertation Faculty of Medicine University of Oslo 2007
48 Tropeacute CG Kristensen G amp Makar A Surgery for borderline tumor of the ovary Semin Surg Oncol 2000 19 69ndash7549 Tempfer CB Polterauer S Bentz EK et al Accuracy of intraoperative frozen section analysis in borderline tumors of the
ovary a retrospective analysis of 96 cases and review of the literature Gynecol Oncol 2007 107 248ndash25250 Camatte S Morice P Thoury A et al Impact of surgical staging in patients with macroscopic lsquostage Irsquo ovarian borderline
tumours analysis of a continuous series of 101 cases Eur J Cancer 2004 40 1842ndash184951 Cadron I Leunen K Van Gorp T et al Management of borderline ovarian neoplasms J Clin Oncol 2007 25 2928ndash293752 Snider DD Stuart GC Nation JG et al Evaluation of surgical staging in stage I low malignant potential ovarian tumors
Gynecol Oncol 1991 40 129ndash13253 Ronnett BM Kurman RJ Zahn CM et al Pseudomyxoma peritonei in women a clinicopathologic analysis of 30 cases with
emphasis on site of origin prognosis and relationship to ovarian mucinous tumors of low malignant potential Hum Pathol
1995 26 509ndash52454 Seidman JD Elsayed AM Sobin LH et al Association of mucinous tumors of the ovary and appendix A clinicopathologic
study of 25 cases Am J Surg Pathol 1993 17 22ndash3455 Trimble EL amp Trimble LC Epithelial ovarian tumors of low malignant potential In Markman M amp Hoskins W (eds) Cancer
of the Ovary New York Raven Press 1993 pp 415ndash429
56 Zanetta G Rota S Chiari S et al Behavior of borderline tumors with particular interest to persistence recurrence andprogression to invasive carcinoma a prospective study J Clin Oncol 2001 19 2658ndash266457 Fauvet R Boccara J Dufournet C et al Restaging surgery for women with borderline ovarian tumors results of a French
multicenter study Cancer 2004 100 1145ndash115158 Zapardiel I Rosenberg P Peiretti M et al The role of restaging borderline ovarian tumors single institution experience and
review of the literature Gynecol Oncol 2010 119 274ndash27759 Def 1047297eux X Morice P Camatte S et al Results after laparoscopic management of serous borderline tumor of the ovary with
peritoneal implants Gynecol Oncol 2005 97 84ndash8960 Fauvet R Boccara J Dufournet C et al Laparoscopic management of borderline ovarian tumors results of a French
multicenter study Ann Oncol 2005 16 403ndash41061 Vandenput I Amant F amp Vergote I Peritoneal recurrences might be less common in advanced stage serous borderline
ovarian tumors that were treated by laparotomy Gynecol Oncol 2005 98 52362 CadronI Amant F VanGorp Tet alThe management of borderline tumours of theovary Curr Opin Oncol 2006 18 488ndash49363 Vergote I De Brabanter J Fyles A et al Prognostic importance of degree of differentiation and cyst rupture in stage I
invasive epithelial ovarian carcinoma Lancet 2001 357 176ndash182
64 Gershenson DM amp Silva EG Serous ovarian tumors of low malignant potential with peritoneal implants Cancer 1990 65578ndash585
65 Gershenson DM Clinical management potential tumours of low malignancy Best Pract Res Clin Obstet Gynaecol 2002 16513ndash527
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 335
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1212
66 Heintz AP Odicino F Maisonneuve P et al Carcinoma of the ovary FIGO 26th Annual Report on the Results of Treatment inGynecological Cancer Int J Gynaecol Obstet 2006 95(Suppl 1) S161ndashS192
67 Bjoslashrge T Engeland A Hansen S et al Prognosis of patients with ovarian cancer and borderline tumours diagnosed inNorway between 1954 and 1993 Int J Cancer 1998 75 663ndash670
68 Seidman JD amp Kurman RJ Subclassi1047297cation of serous borderline tumors of the ovary into benign and malignant typesA clinicopathologic study of 65 advanced stage cases Am J Surg Pathol 1996 20 1331ndash1345
69 Sherman ME Berman J Birrer MJ et al Current challenges and opportunities for research on borderline ovarian tumorsHum Pathol 2004 35 961ndash97070 Leake JF Currie JL Rosenshein NB et al Long-term follow-up of serous ovarian tumors of low malignant potential Gynecol
Oncol 1992 47 150ndash15871 Lim-Tan SK Cajigas HE amp Scully RE Ovarian cystectomy for serous borderline tumors a follow-up study of 35 cases Obstet
Gynecol 1988 72 775ndash78172 Morice P Camatte S El Hassan J et al Clinical outcomes and fertility after conservative treatment of ovarian borderline
tumors Fertil Steril 2001 75 92ndash9673 Camatte S Morice P Pautier P et al Fertility results after conservative treatment of advanced stage serous borderline
tumour of the ovary BJOG 2002 109 376ndash38074 Crispens MA Bodurka D Deavers M et al Response and survival in patients with progressive or recurrent serous ovarian
tumors of low malignant potential Obstet Gynecol 2002 99 3ndash1075 Fauvet R Poncelet C Boccara J et al Fertility after conservative treatment for borderline ovarian tumors a French
multicenter study Fertil Steril 2005 83 284ndash29076 Morris RT Gershenson DM Silva EG et al Outcome and reproductive function after conservative surgery for borderline
ovarian tumors Obstet Gynecol 2000 95 541ndash54777 Gotlieb WH Flikker S Davidson B et al Borderline tumors of the ovary fertility treatment conservative management and
pregnancy outcome Cancer 1998 82 141ndash14678 Maltaris T Boehm D Dittrich R et al Reproduction beyond cancer a message of hope for young women Gynecol Oncol
2006 103 1109ndash112179 Beiner ME Gotlieb WH Davidson B et al Infertility treatment after conservative management of borderline ovarian
tumors Cancer 2001 92 320ndash32580 Fasouliotis SJ Davis O Schattman G et al Safety and ef 1047297cacy of infertility treatment after conservative management of
borderline ovarian tumors a preliminary report Fertil Steril 2004 82 568ndash57281 Kashyap S amp Davis OK Ovarian cancer and fertility medications a critical appraisal Semin Reprod Med 2003 21 65ndash7182 Morice P Camatte S Wicart-Poque F et al Results of conservative management of epithelial malignant and borderline
ovarian tumours Hum Reprod Update 2003 9 185ndash19283 Whittemore AS Harris R amp Itnyre J Characteristics relating to ovarian cancer risk collaborative analysis of 12 US case-
control studies II Invasive epithelial ovarian cancers in white women Collaborative Ovarian Cancer Group Am J Epi-demiol 1992 136 1184ndash1203
84 Fortin A Morice P Thoury A et al Impact of infertility drugs after treatment of borderline ovarian tumors results of a retrospective multicenter study Fertil Steril 2007 87 591ndash596
85 Burger CW van de Swaluw A Mooij TM et al Risk of borderline and invasive ovarian tumors after ovarian stimulation forin vitro fertilization in a large Dutch cohort after 15 years of follow-up Abstracts presented for the 40th Annual Meeting of the Society of Gynecologic Oncologists February 2009 (abstract no 6) Gynecol Oncol 2009 112(Suppl) S4
86 Donnez J Dolmans MM Demylle D et al Livebirth after orthotopic transplantation of cryopreserved ovarian tissue Lancet 2004 364 1405ndash1410
87 Lee DM Yeoman RR Battaglia DE et al Live birth after ovarian tissue transplant Nature 2004 428 137ndash138
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336336

7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1112
31 Kurman RJ amp Trimble CL The behavior of serous tumors of low malignant potential are they ever malignant Int J Gynecol
Pathol 1993 12 120ndash12732 Morice P Camatte S Rey A et al Prognostic factors for patients with advanced stage serous borderline tumours of the
ovary Ann Oncol 2003 14 592ndash59833 Bradley RF Stewart 4th JH Russell GB et al Pseudomyxoma peritonei of appendiceal origin a clinicopathologic analysis of
101 patients uniformly treated at a single institution with literature review Am J Surg Pathol 2006 30 551ndash559
34 Silva EG Gershenson DM Malpica A et al The recurrence and the overall survival rates of ovarian serous borderlineneoplasms with noninvasive implants is time dependent Am J Surg Pathol 2006 30 1367ndash137135 Seidman JD amp Kurman RJ Ovarian serous borderline tumors a critical review of the literature with emphasis on prognostic
indicators Hum Pathol 2000 31 539ndash55736 Chang SJ Ryu HS Chang KH et al Prognostic signi1047297cance of the micropapillary pattern in patients with serous borderline
ovarian tumors Acta Obstet Gynecol Scand 2008 87 476ndash48137 Fox H amp Wells M Surface epithelialstromal tumors of the ovary In Fox H amp Wells M (eds) Haines and Taylor Obstetrical and
Gynaecological Pathology 5th ed London Churchill Livingstone 2003 pp 713ndash74338 Ren J Peng Z amp Yang K A clinicopathologic multivariate analysis affecting recurrence of borderline ovarian tumors Gynecol
Oncol 2008 110 162ndash16739 Longacre TA McKenney JK Tazelaar HD et al Ovarian serous tumors of low malignant potential (borderline tumors)
outcome-based study of 276 patients with long-term (gt or frac145-year) follow-up Am J Surg Pathol 2005 29 707ndash72340 Cusidoacute M Balagueroacute L Hernandez G et al Results of the national survey of borderline ovarian tumors in Spain Gynecol
Oncol 2007 104 617ndash62241 Kaern J Tropeacute CG Kristensen GB et al DNA ploidy the most important prognostic factor in patients with borderline
tumors of the ovary Int J Gynecol Cancer 1993 3 349ndash35842 Meyer JS Gersell DJ amp Yim S Cell proliferation in ovarian carcinoma superior accuracy of S-phase fraction (SPF) by DNA
labeling index versus 1047298ow cytometric SPF lack of independent prognostic power for SPF and DNA ploidy and limitedeffect of SPF on tumor growth rate Gynecol Oncol 2001 81 466ndash476
43 Verbruggen MB van Diest PJ Baak JP et al The prognostic and clinical value of morphometry and DNA cytometry inborderline ovarian tumors a prospective study Int J Gynecol Pathol 2009 28 35ndash40
44 Yokoyama Y Moriya T Takano T et al Clinical outcome and risk factors for recurrence in borderline ovarian tumours Br J Cancer 2006 94 1586ndash1591
45 Leake JF Rader JS Woodruff JD et al Retroperitoneal lymphatic involvement with epithelial ovarian tumors of lowmalignant potential Gynecol Oncol 1991 42 124ndash130
46 Paulsen T Kaern J Kjaerheim K et al Symptoms and referral of women with epithelial ovarian tumors Int J Gynaecol Obstet 2005 88 31ndash37
47 Paulsen T Epithelial ovarian cancer A clinical epidemiological approach on diagnosis and treatment Dissertation Faculty of Medicine University of Oslo 2007
48 Tropeacute CG Kristensen G amp Makar A Surgery for borderline tumor of the ovary Semin Surg Oncol 2000 19 69ndash7549 Tempfer CB Polterauer S Bentz EK et al Accuracy of intraoperative frozen section analysis in borderline tumors of the
ovary a retrospective analysis of 96 cases and review of the literature Gynecol Oncol 2007 107 248ndash25250 Camatte S Morice P Thoury A et al Impact of surgical staging in patients with macroscopic lsquostage Irsquo ovarian borderline
tumours analysis of a continuous series of 101 cases Eur J Cancer 2004 40 1842ndash184951 Cadron I Leunen K Van Gorp T et al Management of borderline ovarian neoplasms J Clin Oncol 2007 25 2928ndash293752 Snider DD Stuart GC Nation JG et al Evaluation of surgical staging in stage I low malignant potential ovarian tumors
Gynecol Oncol 1991 40 129ndash13253 Ronnett BM Kurman RJ Zahn CM et al Pseudomyxoma peritonei in women a clinicopathologic analysis of 30 cases with
emphasis on site of origin prognosis and relationship to ovarian mucinous tumors of low malignant potential Hum Pathol
1995 26 509ndash52454 Seidman JD Elsayed AM Sobin LH et al Association of mucinous tumors of the ovary and appendix A clinicopathologic
study of 25 cases Am J Surg Pathol 1993 17 22ndash3455 Trimble EL amp Trimble LC Epithelial ovarian tumors of low malignant potential In Markman M amp Hoskins W (eds) Cancer
of the Ovary New York Raven Press 1993 pp 415ndash429
56 Zanetta G Rota S Chiari S et al Behavior of borderline tumors with particular interest to persistence recurrence andprogression to invasive carcinoma a prospective study J Clin Oncol 2001 19 2658ndash266457 Fauvet R Boccara J Dufournet C et al Restaging surgery for women with borderline ovarian tumors results of a French
multicenter study Cancer 2004 100 1145ndash115158 Zapardiel I Rosenberg P Peiretti M et al The role of restaging borderline ovarian tumors single institution experience and
review of the literature Gynecol Oncol 2010 119 274ndash27759 Def 1047297eux X Morice P Camatte S et al Results after laparoscopic management of serous borderline tumor of the ovary with
peritoneal implants Gynecol Oncol 2005 97 84ndash8960 Fauvet R Boccara J Dufournet C et al Laparoscopic management of borderline ovarian tumors results of a French
multicenter study Ann Oncol 2005 16 403ndash41061 Vandenput I Amant F amp Vergote I Peritoneal recurrences might be less common in advanced stage serous borderline
ovarian tumors that were treated by laparotomy Gynecol Oncol 2005 98 52362 CadronI Amant F VanGorp Tet alThe management of borderline tumours of theovary Curr Opin Oncol 2006 18 488ndash49363 Vergote I De Brabanter J Fyles A et al Prognostic importance of degree of differentiation and cyst rupture in stage I
invasive epithelial ovarian carcinoma Lancet 2001 357 176ndash182
64 Gershenson DM amp Silva EG Serous ovarian tumors of low malignant potential with peritoneal implants Cancer 1990 65578ndash585
65 Gershenson DM Clinical management potential tumours of low malignancy Best Pract Res Clin Obstet Gynaecol 2002 16513ndash527
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336 335
7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1212
66 Heintz AP Odicino F Maisonneuve P et al Carcinoma of the ovary FIGO 26th Annual Report on the Results of Treatment inGynecological Cancer Int J Gynaecol Obstet 2006 95(Suppl 1) S161ndashS192
67 Bjoslashrge T Engeland A Hansen S et al Prognosis of patients with ovarian cancer and borderline tumours diagnosed inNorway between 1954 and 1993 Int J Cancer 1998 75 663ndash670
68 Seidman JD amp Kurman RJ Subclassi1047297cation of serous borderline tumors of the ovary into benign and malignant typesA clinicopathologic study of 65 advanced stage cases Am J Surg Pathol 1996 20 1331ndash1345
69 Sherman ME Berman J Birrer MJ et al Current challenges and opportunities for research on borderline ovarian tumorsHum Pathol 2004 35 961ndash97070 Leake JF Currie JL Rosenshein NB et al Long-term follow-up of serous ovarian tumors of low malignant potential Gynecol
Oncol 1992 47 150ndash15871 Lim-Tan SK Cajigas HE amp Scully RE Ovarian cystectomy for serous borderline tumors a follow-up study of 35 cases Obstet
Gynecol 1988 72 775ndash78172 Morice P Camatte S El Hassan J et al Clinical outcomes and fertility after conservative treatment of ovarian borderline
tumors Fertil Steril 2001 75 92ndash9673 Camatte S Morice P Pautier P et al Fertility results after conservative treatment of advanced stage serous borderline
tumour of the ovary BJOG 2002 109 376ndash38074 Crispens MA Bodurka D Deavers M et al Response and survival in patients with progressive or recurrent serous ovarian
tumors of low malignant potential Obstet Gynecol 2002 99 3ndash1075 Fauvet R Poncelet C Boccara J et al Fertility after conservative treatment for borderline ovarian tumors a French
multicenter study Fertil Steril 2005 83 284ndash29076 Morris RT Gershenson DM Silva EG et al Outcome and reproductive function after conservative surgery for borderline
ovarian tumors Obstet Gynecol 2000 95 541ndash54777 Gotlieb WH Flikker S Davidson B et al Borderline tumors of the ovary fertility treatment conservative management and
pregnancy outcome Cancer 1998 82 141ndash14678 Maltaris T Boehm D Dittrich R et al Reproduction beyond cancer a message of hope for young women Gynecol Oncol
2006 103 1109ndash112179 Beiner ME Gotlieb WH Davidson B et al Infertility treatment after conservative management of borderline ovarian
tumors Cancer 2001 92 320ndash32580 Fasouliotis SJ Davis O Schattman G et al Safety and ef 1047297cacy of infertility treatment after conservative management of
borderline ovarian tumors a preliminary report Fertil Steril 2004 82 568ndash57281 Kashyap S amp Davis OK Ovarian cancer and fertility medications a critical appraisal Semin Reprod Med 2003 21 65ndash7182 Morice P Camatte S Wicart-Poque F et al Results of conservative management of epithelial malignant and borderline
ovarian tumours Hum Reprod Update 2003 9 185ndash19283 Whittemore AS Harris R amp Itnyre J Characteristics relating to ovarian cancer risk collaborative analysis of 12 US case-
control studies II Invasive epithelial ovarian cancers in white women Collaborative Ovarian Cancer Group Am J Epi-demiol 1992 136 1184ndash1203
84 Fortin A Morice P Thoury A et al Impact of infertility drugs after treatment of borderline ovarian tumors results of a retrospective multicenter study Fertil Steril 2007 87 591ndash596
85 Burger CW van de Swaluw A Mooij TM et al Risk of borderline and invasive ovarian tumors after ovarian stimulation forin vitro fertilization in a large Dutch cohort after 15 years of follow-up Abstracts presented for the 40th Annual Meeting of the Society of Gynecologic Oncologists February 2009 (abstract no 6) Gynecol Oncol 2009 112(Suppl) S4
86 Donnez J Dolmans MM Demylle D et al Livebirth after orthotopic transplantation of cryopreserved ovarian tissue Lancet 2004 364 1405ndash1410
87 Lee DM Yeoman RR Battaglia DE et al Live birth after ovarian tissue transplant Nature 2004 428 137ndash138
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336336

7262019 borderline ovarian tumour
httpslidepdfcomreaderfullborderline-ovarian-tumour 1212
66 Heintz AP Odicino F Maisonneuve P et al Carcinoma of the ovary FIGO 26th Annual Report on the Results of Treatment inGynecological Cancer Int J Gynaecol Obstet 2006 95(Suppl 1) S161ndashS192
67 Bjoslashrge T Engeland A Hansen S et al Prognosis of patients with ovarian cancer and borderline tumours diagnosed inNorway between 1954 and 1993 Int J Cancer 1998 75 663ndash670
68 Seidman JD amp Kurman RJ Subclassi1047297cation of serous borderline tumors of the ovary into benign and malignant typesA clinicopathologic study of 65 advanced stage cases Am J Surg Pathol 1996 20 1331ndash1345
69 Sherman ME Berman J Birrer MJ et al Current challenges and opportunities for research on borderline ovarian tumorsHum Pathol 2004 35 961ndash97070 Leake JF Currie JL Rosenshein NB et al Long-term follow-up of serous ovarian tumors of low malignant potential Gynecol
Oncol 1992 47 150ndash15871 Lim-Tan SK Cajigas HE amp Scully RE Ovarian cystectomy for serous borderline tumors a follow-up study of 35 cases Obstet
Gynecol 1988 72 775ndash78172 Morice P Camatte S El Hassan J et al Clinical outcomes and fertility after conservative treatment of ovarian borderline
tumors Fertil Steril 2001 75 92ndash9673 Camatte S Morice P Pautier P et al Fertility results after conservative treatment of advanced stage serous borderline
tumour of the ovary BJOG 2002 109 376ndash38074 Crispens MA Bodurka D Deavers M et al Response and survival in patients with progressive or recurrent serous ovarian
tumors of low malignant potential Obstet Gynecol 2002 99 3ndash1075 Fauvet R Poncelet C Boccara J et al Fertility after conservative treatment for borderline ovarian tumors a French
multicenter study Fertil Steril 2005 83 284ndash29076 Morris RT Gershenson DM Silva EG et al Outcome and reproductive function after conservative surgery for borderline
ovarian tumors Obstet Gynecol 2000 95 541ndash54777 Gotlieb WH Flikker S Davidson B et al Borderline tumors of the ovary fertility treatment conservative management and
pregnancy outcome Cancer 1998 82 141ndash14678 Maltaris T Boehm D Dittrich R et al Reproduction beyond cancer a message of hope for young women Gynecol Oncol
2006 103 1109ndash112179 Beiner ME Gotlieb WH Davidson B et al Infertility treatment after conservative management of borderline ovarian
tumors Cancer 2001 92 320ndash32580 Fasouliotis SJ Davis O Schattman G et al Safety and ef 1047297cacy of infertility treatment after conservative management of
borderline ovarian tumors a preliminary report Fertil Steril 2004 82 568ndash57281 Kashyap S amp Davis OK Ovarian cancer and fertility medications a critical appraisal Semin Reprod Med 2003 21 65ndash7182 Morice P Camatte S Wicart-Poque F et al Results of conservative management of epithelial malignant and borderline
ovarian tumours Hum Reprod Update 2003 9 185ndash19283 Whittemore AS Harris R amp Itnyre J Characteristics relating to ovarian cancer risk collaborative analysis of 12 US case-
control studies II Invasive epithelial ovarian cancers in white women Collaborative Ovarian Cancer Group Am J Epi-demiol 1992 136 1184ndash1203
84 Fortin A Morice P Thoury A et al Impact of infertility drugs after treatment of borderline ovarian tumors results of a retrospective multicenter study Fertil Steril 2007 87 591ndash596
85 Burger CW van de Swaluw A Mooij TM et al Risk of borderline and invasive ovarian tumors after ovarian stimulation forin vitro fertilization in a large Dutch cohort after 15 years of follow-up Abstracts presented for the 40th Annual Meeting of the Society of Gynecologic Oncologists February 2009 (abstract no 6) Gynecol Oncol 2009 112(Suppl) S4
86 Donnez J Dolmans MM Demylle D et al Livebirth after orthotopic transplantation of cryopreserved ovarian tissue Lancet 2004 364 1405ndash1410
87 Lee DM Yeoman RR Battaglia DE et al Live birth after ovarian tissue transplant Nature 2004 428 137ndash138
CG Tropeacute et al Best Practice amp Research Clinical Obstetrics and Gynaecology 26 (2012) 325ndash 336336
![Borderline Epithelial Tumors of the Ovary · Borderline ovarian tumors represent 10-20% of epithelial ovarian neoplasm’s [5] with an incidence of 1.8-4.8 out of 100.000 women per](https://img.dokumen.tips/doc/110x75/5ebc0423c96cad7a96616a43/borderline-epithelial-tumors-of-the-ovary-borderline-ovarian-tumors-represent-10-20.jpg)
















![Epithelial borderline ovarian tumor: Diagnosis and ...€¦ · Borderline ovarian tumor (BOT) was first described in 1929 by Taylor [1], as the tumor having a pathological and clinical](https://img.dokumen.tips/doc/110x75/5f07430e7e708231d41c1cf4/epithelial-borderline-ovarian-tumor-diagnosis-and-borderline-ovarian-tumor.jpg)











