Embed Size (px)
Citation preview

7/28/2019 Bone Marrow Histology in Monoclonal B-Cell
http://slidepdf.com/reader/full/bone-marrow-histology-in-monoclonal-b-cell 1/6
390 Am J Clin Pathol 2013;139:390-395390 DOI: 10.1309/AJCPPHSUQM8XBJH7
© American Society for Clinical Pathology
Hematopathology / Bone Marrow Histology in MBL
/
Bone Marrow Histology in Monoclonal B-CellLymphocytosis Shows Various B-Cell Infiltration Patterns
Ulla Randen, MD,1,2 Anne M. Tierens, MD, PhD,1 Geir E. Tjønnfjord, MD, PhD,2,3
and Jan Delabie, MD, PhD1,2
Key Words: Monoclonal B-cell lymphocytosis; MBL; CLL; Bone marrow histology
DOI: 10.1309/AJCPPHSUQM8XBJH7
A b s t r a c t
Monoclonal B-cell lymphocytosis (MBL) is defined
as less than 5 × 109 /L monoclonal B cells in the blood of
otherwise healthy patients and is detected in 5% to 10%
of individuals older than 60 years. The bone marrow
findings in MBL have hitherto not been systematically
described. We have studied the histologic and
immunophenotypic findings in paired trephine biopsy
specimens and bone marrow aspirates of 26 patientswith MBL. Abnormal lymphoid infiltration was detected
in trephine biopsy specimens of 20 patients and was
demonstrated by flow cytometry of bone marrow
in all 26 patients. Three infiltration patterns were
discerned: focal interstitial lymphoid infiltration, focal
rounded and nonparatrabecular lymphoid aggregates,
and discrete diffuse lymphocytosis. Focal interstitial
lymphoid infiltration was seen only in patients with
chronic lymphocytic leukemia (CLL)–like or atypical
CLL-like MBL, whereas the other patterns were not
related to a particular MBL immunophenotype. Our results show that most patients with MBL also have
bone marrow lymphoid infiltration. The latter should
be distinguished from lymphoma infiltration by clinical
correlation.
Monoclonal B-cell lymphocytosis (MBL) was first rec-
ognized as an indolent variant of chronic lymphocytic leuke-
mia (CLL) in patients with Rai stage 0 disease. The patients
showed no disease progression, even after a period of more
than 24 years.1 A similar indolent form of CLL was later
described in otherwise healthy family members of patients
with CLL and in cohort studies of outpatients.2-5 The condi-
tion has since been called MBL, and its natural course and
genetics have been studied extensively.6 MBL is now definedas less than 5 × 109/L monoclonal B cells in the blood of
otherwise healthy patients. Large population-based screening
studies have revealed that the prevalence of MBL increases
with age, with a frequency of up to 14% at an age of more
than 62 years.7-9 Virtually all patients with clinically evident
CLL had a preceding MBL, whereas the risk for patients with
CLL-like MBL to develop leukemia is about 1% per year.7,8
MBL likely arises through chronic stimulation of a limited
B-cell repertoire in older individuals. Thus, it is a phenom-
enon associated with senescence of the lymphoid system.10
MBL shows genetic changes such as 13q14 deletion, trisomy12, and deletion of 17p and 11q, as also seen in CLL.7 CD38
and ZAP-70 expression, VH gene usage, and cytogenetic
abnormalities have not allowed prediction of the transition of
MBL to CLL, but B-cell counts, especially low-count MBL,
have been associated with a very low risk of progression to
CLL.11,12 In addition to the more frequent CLL-like immuno-
phenotype of MBL, characterized by CD5 and CD23 expres-
sion and weak expression of CD20 and immunoglobulins, an
atypical CLL-like phenotype with moderate or strong CD20
and immunoglobulin expression is also recognized. Further-
more, MBL with a non–CLL-like phenotype, characterized
Upon completion of this activity you will be able to:• recognizethebonemarrowtrephinehistologicfindingsinmonoclonal
B-cell lymphocytosis.•advisetheclinicianabouttheimplicationofdiagnosinglesionsin
bone marrow trephines that are consistent with monoclonal B-celllymphocytosis.
TheASCPisaccreditedbytheAccreditationCouncilforContinuingMedicalEducationtoprovidecontinuingmedicaleducationforphysicians.TheASCPdesignatesthisjournal-basedCMEactivityforamaximumof1AMA PRA Category 1 Credit ™perarticle.Physiciansshouldclaimonlythecreditcommensuratewiththeextentoftheirparticipationintheactivity.ThisactivityqualifiesasanAmericanBoardofPathologyMaintenanceofCertificationPartIISelf-AssessmentModule.
Theauthorsofthisarticleandtheplanningcommitteemembersandstaff
havenorelevantfinancialrelationshipswithcommercialintereststodisclose.Questionsappearonp399.Examislocatedatwww.ascp.org/ajcpcme.

7/28/2019 Bone Marrow Histology in Monoclonal B-Cell
http://slidepdf.com/reader/full/bone-marrow-histology-in-monoclonal-b-cell 2/6
Am J Clin Pathol 2013;139:390-395 391391 DOI: 10.1309/AJCPPHSUQM8XBJH7 391
© American Society for Clinical Pathology
Hematopathology / Original Article
by the absence of CD5 expression, has also been described.5,6
In view of the frequency of MBL in the general population,
MBL is often seen in combination with other diseases, includ-
ing those for which a trephine biopsy regularly is performed
as part of the diagnostic workup. Trephine biopsy is part of
the panel of tests performed for a large number of diseases,
including primary nonmalignant as well as malignant hema-
tologic diseases, nonhematologic malignancies, and certain
infectious diseases. Hitherto, there have been no systematic
studies of bone marrow infiltration, including bone marrow
histologic findings, in patients with MBL despite its high fre-
quency in the population. We therefore investigated whether
MBL involved the bone marrow and, if so, what its histology
was like and whether it could be differentiated from bone mar-
row involvement by lymphoma. We studied the bone marrow
histology in 26 patients with well-documented MBL.
Materials and Methods
Patient Selection
Patients were selected from the database of the Depart-
ment of Pathology, Oslo University Hospital, Oslo, Norway.
Only patients with an established MBL diagnosed between
2008 and 2011 and from whom a trephine biopsy was
procured at the time of MBL diagnosis were selected for
this study. All patients with non-Hodgkin lymphoma were
excluded from the study, with the exception of 2 cases in
which lymphoma involvement was easy to distinguish fromMBL by morphology and immunohistochemistry. In total,
26 patients were retrieved from the database, including 18
men and 8 women with a mean age 70 years (range, 50-94
years). The patients underwent bone marrow examination as
part of the clinical workup of their initial symptoms or pri-
mary disease. In 17 patients who presented with nonspecific
symptoms such as fatigue, weight loss, or fever, no disease
was eventually diagnosed. Chronic myeloproliferative disease
was diagnosed in 4 patients and myelodysplastic syndrome
in 1 patient. Three patients had a plasma cell neoplasia, 1
had a primary cutaneous follicular lymphoma, and 1 had ahepatosplenic T-cell lymphoma. One patient had renal cell
carcinoma. A bone marrow aspirate had also been procured
in all 26 patients.
Flow Cytometry
Flow cytometry analyses were performed on blood and
bone marrow samples from all 26 patients. Samples were
anticoagulated with heparin. Between 0.5 and 1 × 106 cells
were stained for surface antigens. For samples analyzed before
2011, a 4-color analysis13 was performed with the following
antibody combinations labeled with fluorescein isothiocyanate
(FITC)/phycoerythrin (Pe)/peridinin-chlorophyll cyanine 5.5
(PercPCY5.5)/allophycocyanin (APC): (1) CD20/CD5/CD19/
CD43, (2) FMC7/CD23/CD19/CD5, (3) Igk/Igl/CD20/CD19,
(4) CD22/CD24/CD19/CD34, and (5) cyBcl2/CD10/CD19/
CD38. From 2011, an 8-color flow cytometry analysis14 was
used with the following antibody combinations labeled with
Pacific Blue/e450 (PB/e450), Krome Orange (KO), FITC/
Pe/PercPCy5.5/phycoerythrin cyanine 7(PeCy7)/APC/APC
Hilite7, or APC/cyanine 7 (APCH7/cy7): (1) CD20+CD4/
CD45/CD8+Igl/CD56+Igk/CD5/CD19+TCRγδ/CD38 and
(2) CD20/CD45/CD23/CD10/CD79b/CD19/CD200/CD43.
All antibodies for the 4-color panels were purchased from
Becton-Dickinson (San Jose, CA) except anti-FMC7, CD22,
CD23, and anti-Bcl2, which were purchased from DAKO
(Glostrup, Denmark). For the 8-color panels, CD56, CD5,
CD3, and 79b were purchased from Becton-Dickinson; CD23
from DAKO; CD200 from eBioscience (San Diego, CA);
CD8, k, and l from Cytognos (Salamanca, Spain); and the rest
from Beckman Coulter (Brea, CA). Flow cytometry analysis
was performed on a FACSCalibur or LSRII instrument (Bec-
ton-Dickinson) using CellQuest Pro and FACSDiva software
(Becton-Dickinson), respectively.
Immunohistochemistry
The primary antibodies used for immunophenotypic
analysis of the lymphoid infiltrates were anti-CD45, anti-
CD20, anti-Bcl6, anti-Mum1, anti-IgA, anti-IgD, anti-IgG,
anti-IgM, and anti-Ki67 (all from DAKO); anti-CD10, anti-
Bcl2, anti-CD21, anti-CD23, anti-CD5, anti-CD43, and anti–
cyclin D1 (all from Novocastra Laboratories, Newcastle uponTyne, UK); anti-PAX5 (Becton-Dickinson); and anti-CD3
(Thermo Fisher Scientific, Fremont, CA). For all antibodies,
heat-induced epitope retrieval was performed in a microwave
oven by heating the slides for 5 minutes at 750 W and sub-
sequently for 15 minutes at 500 W in retrieval buffer. The
detection system EnVision (DAKO) was used for all antibod-
ies. The stain was developed with 3,3'-diaminobenzidine and
H2O
2, and the slides were counterstained with hematoxylin.
The immunostaining was performed in a DAKO Autostainer
(DAKO) according to the instructions of the manufacturer.
Results
Flow cytometry analysis revealed a CLL-, an atypical
CLL-, or a non–CLL-like immunophenotype MBL in 11, 5,
and 10 patients, respectively ❚Table 1❚. Monoclonal B cells
were also detected in the bone marrow samples of all 26
patients. The immunophenotypes of the cells in the bone mar-
row were identical to those of the respective blood samples.
The trephine biopsy specimens showed no evidence of
abnormal lymphoid infiltration in 6 of 26 patients. Infiltration

7/28/2019 Bone Marrow Histology in Monoclonal B-Cell
http://slidepdf.com/reader/full/bone-marrow-histology-in-monoclonal-b-cell 3/6
392 Am J Clin Pathol 2013;139:390-395392 DOI: 10.1309/AJCPPHSUQM8XBJH7
© American Society for Clinical Pathology
Randen et al / Bone Marrow Histology in MBL
of the bone marrow by small B cells was found in 20 patients.
Three infiltration patterns were discerned: 7 patients showed
small interstitial foci, varying from 1 to 5, with monotonous
small lymphoid cells with a rounded nucleus. At the periphery
of these foci, cells infiltrated between fat cells in small rows
❚Image 1A-D❚. Eight patients showed more rounded lym-
phoid foci, varying from 1 to 9, without interstitial infiltration
between fat cells at the periphery. These lymphoid foci con-
sisted of small lymphoid cells with a slightly more irregular
nuclear contour, as well as a few scattered immunoblasts and
histiocytic cells ❚Image 1E-H❚. Centrally located tiny germinalcenters could occasionally be observed (Image 1H). The latter
were highlighted by CD21 staining. Finally, 5 patients showed
a discrete diffuse lymphocytosis that was only discerned upon
immunohistochemical staining for CD20. Diffuse B-cell lym-
phocytosis in patients with MBL could be distinguished from
the presence of hematogones by the homogeneous small size
of B cells in the former and by the variable small to medium-
large size in the latter. In addition, hematogones showed a
variable CD20 expression in contrast to the homogeneous
CD20 expression seen with MBL. Intrasinusoidal infiltration
was not seen in any of the cases.
Of interest, there was a correlation between the infiltra-
tion pattern and the immunophenotype of MBL (Table 1). The
interstitial pattern was exclusively seen in patients with MBL
with a CLL-like or an atypical CLL-like immunophenotype.
The 2 other patterns were most commonly seen in non–CLL-
like MBL, although these patterns were also observed in 3
patients with a CLL-like or an atypical CLL-like MBL.
Discussion
With the extensive use of highly sensitive multiparameter
flow cytometry analyses of blood and bone marrow samples,
MBL is increasingly being detected.9,15 The etiology of MBL
is not clear, but it is hypothesized that it results from chronic
and persistent antigen stimulation.10,16 CLL-like and atypical
CLL-like MBL shows genetic changes such as chromosome
13q deletion, trisomy 12, and even chromosome 17p deletions
as well as stereotyped immunoglobulin receptors as seen in
CLL, adding to the argument that MBL is a precursor state of
CLL.7,12 Less is known about non–CLL-like MBL, although
genetic changes are also seen, albeit different from those
❚Table 1❚Infiltration Pattern and Immunophenotype of Bone Marrow B-Cell Infiltration in Patients With MBL
Infiltration No. of DiscretePatient No. Sex/Age, y Pattern Infiltrations Concurrent Disease
CLL-phenotype casesa
1 F/73 0 0 CMPD2 M/74 1 1 Primary cutaneous FL
4 M/67 0 0 ND12 M/80 1 2 MDS13 F/58 2 1 ND14 F/50 1/3 4 ND20 F/72 1 3 ND24 M/76 0 0 ND25 M/89 2 1 Plasma cell neoplasia22 M/69 0 0 ND23 M/82 1 2 ND
Atypical CLL-phenotype casesb 6 M/64 0 0 ND7 M/70 1 3 ND8 M/56 3 0 CMPD15 M/60 2 7 ND26 M/55 1 5 ND
Non–CLL-phenotype casesc 3 F/74 0 0 CMPD5 F/63 3 0 ND9 M/82 3 0 Renal cell carcinoma10 M/88 2 1 CMPD11 F/79 3 0 Plasma cell neoplasia16 F/75 2 2 ND17 M/67 2 1 Plasma cell neoplasia18 M/94 2 9 ND19 F/81 2 1 Hepatosplenic T-cell lymphoma21 M/69 3 0 ND
Infiltration patterns: 0, no infiltration; 1, interstitial infiltration; 2, circumscribed intraparenchymatous lymphoid aggregates; 3, diffuse infiltration. CLL, chronic lymphocyticleukemia; CMPD, chronic myeloproliferative disease; FL, follicular lymphoma; MBL, monoclonal B-cell lymphocytosis; MDS, myelodysplastic syndrome; ND, no disease.
a CD20dim+, CD5+, CD23+, Ig light chain dim+. b CD20+, CD5+, CD23+, Ig light chain+.c CD20+, CD5–, CD23–, Ig light chain+.

7/28/2019 Bone Marrow Histology in Monoclonal B-Cell
http://slidepdf.com/reader/full/bone-marrow-histology-in-monoclonal-b-cell 4/6
Am J Clin Pathol 2013;139:390-395 393393 DOI: 10.1309/AJCPPHSUQM8XBJH7 393
© American Society for Clinical Pathology
Hematopathology / Original Article
demonstrated in CLL-like MBL.17 Whether non–CLL-like
MBL is a precursor state for non-Hodgkin lymphoma—in
particular, marginal zone lymphoma or lymphoplasmacytic
lymphoma and perhaps also diffuse large B-cell lymphoma,
as the immunophenotype and genetic changes seem to indi-
cate—remains to be demonstrated.18 Whether and how MBL
affects the bone marrow was hitherto poorly described except
for 1 study published as an abstract.19 However, knowledge
about bone marrow infiltration in MBL is of potential inter-
est to avoid diagnosis of marrow infiltration with lymphoma.
We therefore studied trephine biopsy specimens by histology
and immunohistochemistry in 26 individuals with established
MBL. We reviewed the flow cytometry findings in peripheral
blood and bone marrow in all patients.
Histology and immunohistochemistry highlighted abnor-
mal lymphoid infiltration in the bone marrow of 20 patients,
displaying patterns that were indistinguishable from limited
infiltration by CLL or marginal zone lymphoma. CLL or
small lymphocytic lymphoma shows nodular or diffuse
non-paratrabecular interstitial infiltration with monotonous
small lymphoid cells variably admixed with paraimmuno-
blasts.20 Occasionally, more limited focal patchy interstitial
A B
C D
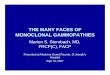
❚Image 1❚ A-D, Bone marrow lymphoid infiltration in chronic lymphocytic leukemia (CLL)–type monoclonal B-cell lymphocytosis
(MBL). Focal interstitial infiltration by small lymphoid cells with rounded nuclei is shown (A, H&E, ×400, patient 12; B, H&E,
×400, patient 14). Immunohistochemical staining for CD20 highlights the focal interstitial infiltration pattern (C, ×200, patient 23)
and cell-poor diffuse infiltration pattern that can be seen in MBL (D, ×200, patient 13).

7/28/2019 Bone Marrow Histology in Monoclonal B-Cell
http://slidepdf.com/reader/full/bone-marrow-histology-in-monoclonal-b-cell 5/6
394 Am J Clin Pathol 2013;139:390-395394 DOI: 10.1309/AJCPPHSUQM8XBJH7
© American Society for Clinical Pathology
Randen et al / Bone Marrow Histology in MBL
infiltrates are seen in CLL, indistinguishable from the pat-
tern of infiltration reported here for MBL with a CLL-like
or an atypical CLL-like immunophenotype.20 Marginal
zone lymphoma in the bone marrow most frequently shows
focal, more rounded nonparatrabecular infiltrates with small
lymphoid cells often admixed with some immunoblasts and
histiocytic cells as well as follicular dendritic cells.20,21
This is also one of the patterns seen in MBL with a non–
CLL-like immunophenotype, although this pattern could
occasionally be observed in MBL with a CLL-like and an
atypical CLL-like immunophenotype. Of interest, diffuse
but limited B-cell infiltration was almost exclusively seen
in MBL with a non–CLL-like immunophenotype. This
infiltration pattern is distinct from the diffuse but intrasinu-
soidal infiltration pattern often seen in splenic marginal
zone lymphoma.20 Intrasinusoidal infiltration was not seen
in any of the MBL cases.
There was perfect agreement between the immunophe-
notype of MBL in peripheral blood and the monoclonal B
cells in the bone marrow. In addition, immunohistochemical
findings were also in agreement with the immunopheno-
types detected by flow cytometry. This supports the finding
❚Image 1❚ (cont) E and F, Lymphoid infiltration seen in non–CLL-type MBL (E, H&E, ×400, patient 16; F, anti-CD20, ×400,
patient 15); there is focal but more clustered infiltration in contrast to the typical CLL-type MBL. There are small lymphoid cells
with nuclei with slightly irregular contours admixed with the same few immunoblasts (E). G, Lymphoid infiltration in a case of
atypical CLL-type MBL (H&E, ×400, patient 16). In this case, small lymphoid cells are admixed with epithelioid histiocytic cells.
H, Focal cluster of B cells in a patient with atypical CLL-type MBL (anti-CD20, ×200, patient 7) displaying a small network of
follicular dendritic cells in the background of the lymphoid focus as highlighted by CD21 expression (not illustrated).
E F
G H

7/28/2019 Bone Marrow Histology in Monoclonal B-Cell
http://slidepdf.com/reader/full/bone-marrow-histology-in-monoclonal-b-cell 6/6
Am J Clin Pathol 2013;139:390-395 395395 DOI: 10.1309/AJCPPHSUQM8XBJH7 395
© American Society for Clinical Pathology
Hematopathology / Original Article
that lymphoid infiltration seen in bone marrow is the tissue
counterpart of MBL.
The frequent involvement of bone marrow in patients
with MBL displaying an infiltration pattern and immunophe-
notype that is indistinguishable from that of limited infiltration
with lymphoma, especially CLL or marginal zone lymphoma,
is of diagnostic importance. Our results indicate that a final
diagnosis of lymphoma in the bone marrow should not be
made in the absence of an established lymphoma diagnosis or
in the absence of adequate clinical information. Whether the
patient with limited lymphoid infiltration in the bone marrow,
originally taken as part of the investigation for other diseases,
should be screened for lymphoma and how extensive this
screening should be is a matter of discussion. Noninvasive
investigations with abdominal ultrasound and chest x-ray
in addition to a complete blood cell count, whenever these
have not been performed as part of the investigations for the
patient’s primary disease, are most likely indicated, as recom-
mended for MBL.10,22
Whether the extent of bone marrow infiltration with
MBL correlates with increased progression toward overt
clinical disease is of interest but still needs to be studied. This
question may be answered by studying a larger cohort of
patients with a longer follow-up time.
From the 1 Department of Pathology and the 3 Department of
Hematology, Oslo University Hospital, Oslo, Norway; and 2 Institute of Clinical Medicine, University of Oslo, Oslo, Norway.
This study was supported by a grant from the Norwegian
Cancer Society.
Address reprint requests to Dr Randen: Dept. of Pathology,
Oslo University Hospital, Ullernchausséen 70, 0310 Oslo,
Norway; e-mail: [email protected].
References
1. H T, Oz H, Gv M, . B mB- mph— b v f CLL: ,mmu, php d ud 20p. Blood. 1984;64:244-252.
2. M GE, Fu GB, S C, . Evu f ukmh f hum B- mph b dh p. Curr Top Microbiol Immunol. 1992;182:303-
311.3. R AC, Yu MR, Fu J, . Ihd
pdp CLL db ub mB-mph xp. Blood. 2002;100:2289-2290.
4. R AC, G MJ, Kuzmk A, . M Bmph h h h f “d” hmph ukm p 3.5% f du hm bd u. Blood. 2002;100:635-639.
5. Gh P, P G, Sz C, . M CD5+d CD5– B-mph xp fqu hpph bd f h d. Blood. 2004;103:2337-2342.
6. M GE, R AC, Gh P, ; Th IFm CLL Cum. D f mB- mph. Br J Haematol. 2005;130:325-332.
7. R AC, B FL, O’C SJ, . MB-mph d h mph ukm. N Engl
J Med. 2008;359:575-583.
8. Ld O, Ab M, M W, . B- mk f h mph ukm. N Engl J Med. 2009;360:659-667.
9. N WG, Amd J, Rm A, , f Pm HhC Gup f Sm f h Sud f MBL. Id
fqu (12%) f u h mphukm-k B- hh ubj u hh v mu f m pph.Blood. 2009;114:33-37.
10. Gh P, C-Cpp F. M B-mph: h k d h? Blood. 2012;119:4358-4362.
11. R AC, Shf T, L MC, . Dffb d um d h buumb f B- m B- mph(MBL). Cytometry B Clin Cytom. 2010;78(upp 1):S19-S23.
12. Fz C, Sfò L, P L, . G ppu-u CLL-k MBL p v m hu p, huh h m
bm f CLL. Blood. 2011;118:6618-6625.13. Sáhz ML, Amd J, Vd B, . Id f
php b f 467 p h Bh mphpfv dd: b f h d f pf fu- b ud f mm dud v. Leukemia. 2002;16:1460-1469.
14. v D JJ, Lhm L, Böh S, . EuFbd p f ddzd -dm fm mmuphp f m, v dm uk. Leukemia. 2012;26:1908-1975.
15. Amd J, N WG, Td C, , f Pm HhC Gup f Sm f h Sud f MBL. CLL-kB-mph m p v umb pph bd f hh du. Leukemia. 2011;25:718-
722.16. Sfò L, Dk A, Sz C, . CLL-k m
B- mph: bud hv ? SeminCancer Biol. 2010;20:384-390.
17. N WG, Td C, Lópz A, , f PmHh C Gup f Sm f h Sud f MBL.
N–CLL-k m B- mph h ppu: pv d php/h. Cytometry B Clin Cytom. 2010;78(upp1):S24-S34.
18. T AM, H H, Wm A, . L v f m m B h b m f p hdffu B- mphm f vd B- p bu f m B- p. Haematologica. 2010;95:1334-
1341.19. Hk JL, Shf TD, K NE, . M B-
mph (MBL): b m ud f dfm f h mph ukm (CLL). Mod Pathol. 2008;21:256A.
20. Zh QY, Fu K. B m vvm b Hdkd -Hdk mphm. Hematol Oncol Clin North
Am. 2009;23:873-902.
21. Sd SH, Cmp E, H NL, , d. WHOClassification of Tumours of Haematopoietic and LymphoidTissues. L, F: IARC; 2008.
22. R AC, Hm P. C d dmp f m B- mph.Best PractRes Clin Haematol. 2010;23:61-69.