Embed Size (px)
Citation preview

Body Sensor Networks:
An Application-Centric Approach
John LachJohn Lach
Charles L. Brown Department of Electrical & Computer Engineering
University of Virginia

Invasive
Under-S
ampled
Imprecise
Inaccurate
Qualita
tive
Expensive
In-Patient
Monitoring
Limitations of Healthcare Data Collection
• Physicians, nurses,
caretakers, and medical
researchers depend on high
quality data to monitor and
assess patients and study,
diagnose, and treat diseases
Project Motivation
Monitoring
Expert
Observation
Patient
Self-Reports
SignificantInsignificant
diagnose, and treat diseases
• But current data collection
mechanisms have limitations

Invasive
Under-S
ampled
Imprecise
Inaccurate
Qualita
tive
Expensive
In-Patient
Monitoring
Limitations of Healthcare Data Collection
• Physicians, nurses,
caretakers, and medical
researchers depend on high
quality data to monitor and
assess patients and study,
diagnose, and treat diseases
Project Motivation
Monitoring
Expert
Observation
Patient
Self-Reports
Body Sensor
Networks
SignificantInsignificant
diagnose, and treat diseases
• But current data collection
mechanisms have limitations
• Wireless body sensor
networks (BSNs) are
emerging as a promising
technological solution

Wireless Health Infrastructure
• HardwareCollecting the data and
getting it where it
needs to go
• SoftwareConverting data into
medically relevant medically relevant
information
• DatabaseEnabling access to
information for diverse
stakeholders
• Interfaces
between them
4

Big Wireless Health Questions
• What value does Wireless Health promise?– Improve patient care
– Enhance wellness
– Enable aging-in-place
– Lower healthcare costs
– …– …
• How can this value be demonstrated?– Need application domain expertise
• Collaborate, collaborate, collaborate
– Deploy platforms in real human subjects studies
– Convert data to medically relevant information
– Identify and use metrics appropriate for target application(s)
– Science-based research5

• “An interdisciplinary team of researchers focusing
on technology to improve healthcare…and
healthcare to improve technology”healthcare to improve technology”
• Co-directors: John Lach (ECE), Steve Patek (SIE),
Jack Stankovic (CS)
• Members from Neurology, Neurosurgery,
Neuropsychology, Nephrology, Biomechanics,
Orthopedic Surgery, Cardiology, Geriatric Nursing,
Psychiatry, etc.6

• Application-driven engineering research
– Embedded systems, circuits, and signal processing expertise
– Strong relationships with medical personnel and patients
– Real systems deployed in real clinical applications, including rapid prototyping
• Application focus is on movement disorders, requiring high precision motion capture and analysis tomotion capture and analysis to
– Study movement disorder etiology and progression
– Increase movement disorder diagnostic sensitivity
– Evaluate efficacy of therapeutic intervention
• Technology goal: maximize wearability and battery life of body sensor
networks (BSNs) while delivering required motion analysis fidelity
• Overall goal: improve healthcare and medical research to ultimately
improve patient outcomes and quality of life while reducing healthcare
costs
7

BSN Research Cycle
8

DBS-based Management of Tremor
• Tremor can impair quality of life for advanced Parkinson’s Disease (PD) and Essential Tremor (ET) patients
• Deep brain stimulation (DBS) offers tremor relief for recalcitrant, advanced tremorrecalcitrant, advanced tremor
• Drs. Jeffrey Elias and Robert Frysinger (UVA Neurosurgery Department) desired to study impact of different DBS settings on PD and ET with quantitative tremor analysis– Occurrence– Frequency– Magnitude– Classification
Image Credit: Wired Magazine 15.03, 20079

BSN Research Cycle
Wearable Inertial
Sensor Nodes
Prototype
10
Joint Time-Frequency
Analysis of Motion
Continuous, Non-Invasive
Tremor Measurement
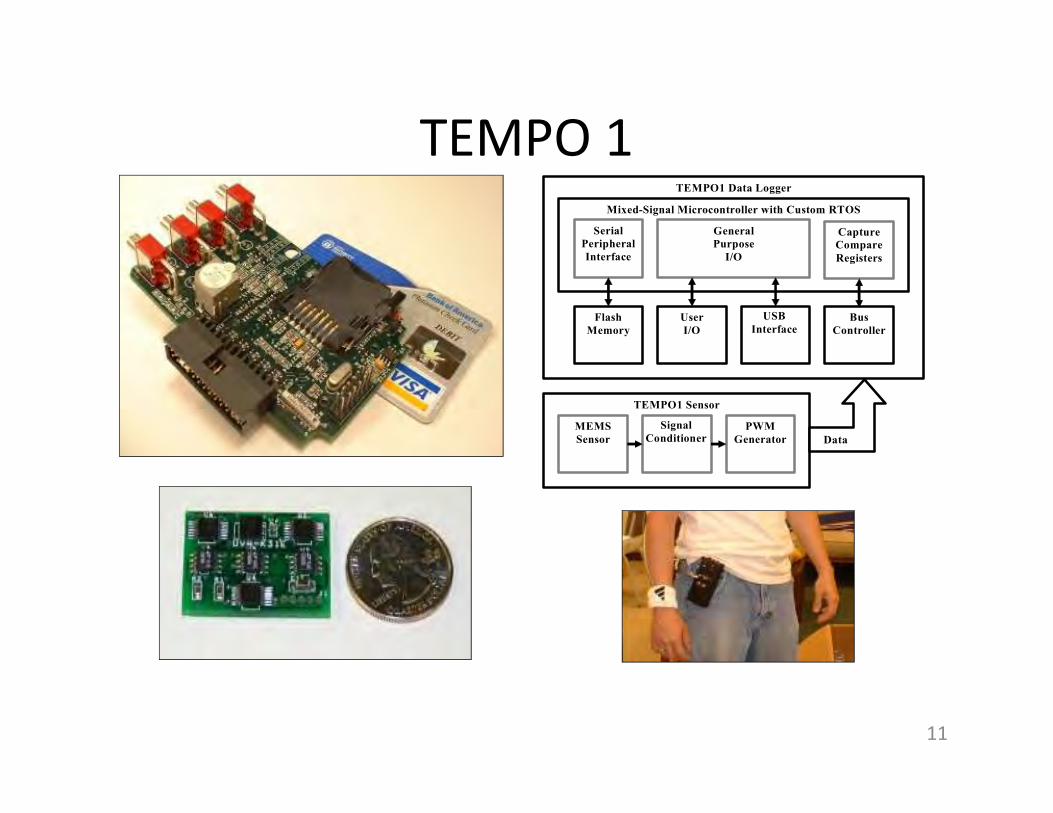
TEMPO 1
TEMPO1 Data Logger
Mixed-Signal Microcontroller with Custom RTOS
Capture
Compare
Registers
Flash
Memory
User
I/O
General
Purpose
I/O
Bus
Controller
USB
Interface
Serial
Peripheral
Interface
TEMPO1 Sensor TEMPO1 Sensor
MEMS
Sensor
PWM
Generator
Signal
Conditioner Data
11

TEMPO 3
12

TEMPOS, Aggregator, Explorer
13

• Complete power-aware, physically-aware re-
design of BSNs
• Low power CPU/transceiver
• Software stack takes advantage of new HW
Next Gen: Custom ICs for BSNs
• Software stack takes advantage of new HW
• 2+ orders of magnitude less energy
14
from Ben Calhoun

TEMPO 1,
TEMPO 2,
TEMPO 3
BSN Research Cycle
15

• Parkinson’s disease – study efficacy of deep brain stimulation– Jeffrey Elias, Robert Frysinger (UVA Neurosurgery)
• Parkinson’s disease – study impact of cognitive stress– Scott Wylie (UVA Neurology)
• Normal pressure hydrocephalus – improve diagnosis– Jeffrey Barth, Donna Broshek, Jason Freeman (UVA Neuropsychology)
• Geriatrics – enable fall risk assessment in naturalistic settings
TEMPO in Human Subject Studies
– Thurmon Lockhart (Virginia Tech Locomotion Laboratory)
– Mark Williams (UVA Geriatric Medicine)
– Amy Papadopoulos, Cindy Crump (AFrame Digital)
• Dialysis – study cause of higher fall rates– Emaad Abdel-Rahman (UVA Nephrology)
• Cerebral palsy – study efficacy of orthopedics for children– Brad Bennett (Kluge Children’s Rehabilitation Center)
• Dementia – assess physical agitation– Azziza Bankole, Martha Anderson, Aubrey Knight (Carilion Center for Healthy Aging)
• Multiple sclerosis – gait analysis for early diagnosis– Myla Goldman (UVA Neurology)
16

Tremor AssessmentRaw 3-axis Tremor Acceleration Waveforms
Teager Tremor Waveform
17

Tremor Assessment
18
Head
Right Hand
Left Hand
DBS Best Setting DBS Off

TEMPO 1,
TEMPO 2,
TEMPO 3
BSN Research Cycle
Teager & STFT Energy,
ANN, SVM, KNN,
Real-time variance,
Haar DWT
Tremor, Gait Disorders, Fall
Risk, Agitation, …
19

• To make health assessment of human
movement a reality, platforms will need:
– Smaller form factor (invisible to the user) for
unobtrusive, naturalistic use
BSN Requirements
unobtrusive, naturalistic use
– Longer battery life (from hours now to days and
weeks in the near future) for continuous,
longitudinal monitoring
– Higher application fidelity (data that reliably yields
clinically-meaningful, non-obvious information) for
delivering value
20
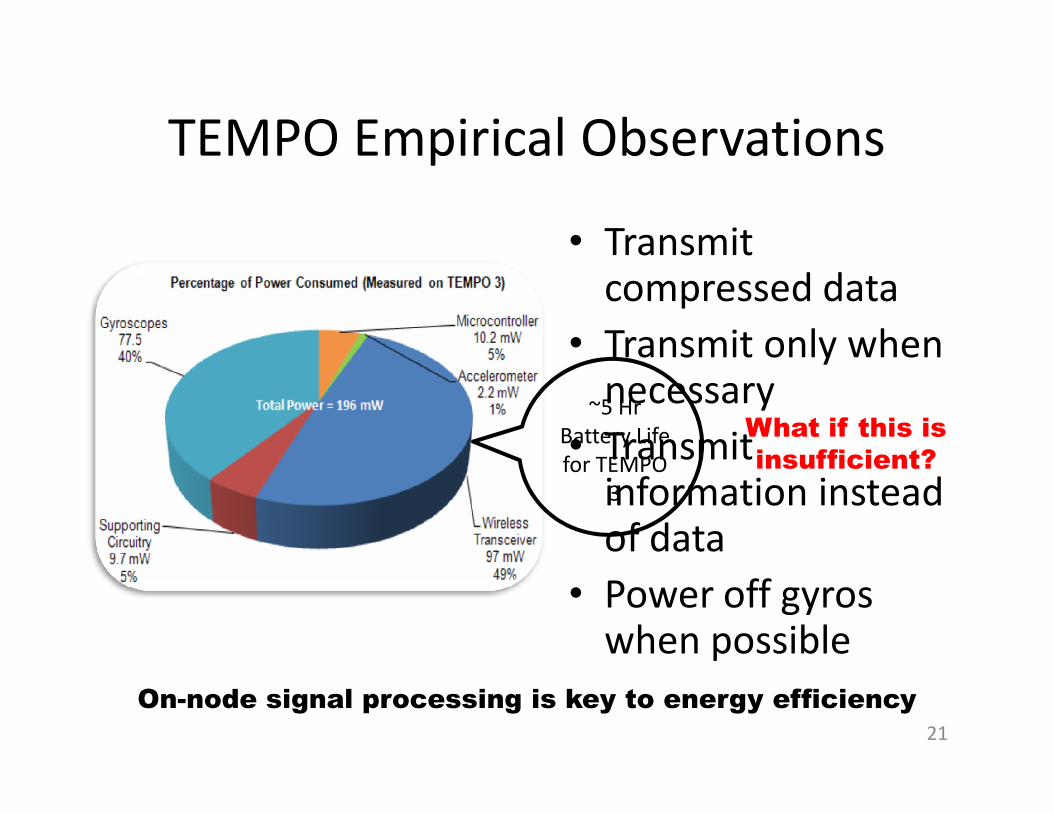
TEMPO Empirical Observations
~5 Hr
• Transmit compressed data
• Transmit only when necessary
~5 Hr
Battery Life
for TEMPO
3
necessary
• Transmit information instead of data
• Power off gyros when possible
On-node signal processing is key to energy efficiency
21
What if this is
insufficient?

• Reducing energy use (and increasing battery life) is
easy. We simply need to reduce the amount of
transmitted data for a given BSN application.
– BUT…reduction of data may decrease application fidelity
• So move processing to the periphery of the network
Research Direction
• So move processing to the periphery of the network
and reduce transmission energy
– BUT…processing consumes power and resources are
limited (lack of FPU, memory, clock speed, etc.)
A framework is needed to both understand and
manipulate the energy-fidelity tradeoff for healthcare
BSN applications
22

Effects of Lossy Compression• Assume an application accepts
a maximum MSE distortion of
100 (from raw 12-bit ADC
acceleration)
• For fixed compression ratio:
– Distortion above this
threshold violates the
23
For a given data rate, distortion will change over time,
so dynamic management of data rate is desirable
threshold violates the
requirement, so data rate
must increase
– Operating well below the
threshold is energy inefficient
since data-rate can be further
reduced

Energy-Fidelity FrameworkBSN Hardware
Measured
Time
Energy-Fidelity
Tradeoff Space
Epb
Energy Model
LabVIEW
Source
C Source
Data Rate
Reduction
Techniques
BSN Tremor DataFidelity Measurer
Raw Data
CR MSE
24

Dynamic Energy-Fidelity Management
25
What is the right measure of “fidelity”?
Almost certainly NOT MSE!!!

• A data controller and a destination controller
• Runtime optimization of tradeoffs between power consumption, computational complexity, and signal fidelity
• Adjust to system dynamics– Data characteristics
– Wireless channel characteristics
– Application priorities
BSN Control Architecture
26

• DVFS promotes power savings when
timing and/or processing
requirements are relaxed
– Takes advantage of the relationship
of supply voltage and operating
frequency in CMOS circuits
• DVFS is found in higher powered
Dynamic Voltage-Frequency Scaling for BSNs
using COTS Components
Tremor Inertial Accelerometer Data
No activity -
”lightweight
calculations”
Active Tremor
α⋅⋅⋅ FVC=P DDp
2
• DVFS is found in higher powered
consumer mobile electronics and
cutting edge, low-power circuit
research
• Common BSN microcontrollers can
operate over a range of voltages and
frequencies
– On-chip oscillators for clock
generation
• MSP430 maximum operating
frequency equation:
Tremor Inertial Accelerometer Data
Teager “Energy” Calculation
No Teager
computation
requiredGreater
Processing
Load
( ) 6100.667.6)( ×−⋅ DDDCO V=HzF
27

TEMPO 1,
TEMPO 2,
TEMPO 3
Energy-Fidelity Scalability,
Application Profiling, DVFS,
BCC
BSN Research Cycle
Teager & STFT Energy,
ANN, SVM, KNN,
Real-time variance,
Haar DWT
Tremor, Gait Disorders, Fall
Risk, Agitation, …
28

• Parkinson’s disease – study efficacy of deep brain stimulation– Jeffrey Elias, Robert Frysinger (UVA Neurosurgery)
• Parkinson’s disease – study impact of cognitive stress– Scott Wylie (UVA Neurology)
• Normal pressure hydrocephalus – improve diagnosis– Jeffrey Barth, Donna Broshek, Jason Freeman (UVA Neuropsychology)
• Geriatrics – enable fall risk assessment in naturalistic settings
TEMPO in Human Subject Studies
– Thurmon Lockhart (Virginia Tech Locomotion Laboratory)
– Mark Williams (UVA Geriatric Medicine)
– Amy Papadopoulos, Cindy Crump (AFrame Digital)
• Dialysis – study cause of higher fall rates– Emaad Abdel-Rahman (UVA Nephrology)
• Cerebral palsy – study efficacy of orthopedics for children– Brad Bennett (Kluge Children’s Rehabilitation Center)
• Dementia – assess physical agitation– Azziza Bankole, Martha Anderson, Aubrey Knight (Carilion Center for Healthy Aging)
• Multiple sclerosis – gait analysis for early diagnosis– Myla Goldman (UVA Neurology)
29

Portable, Non-Invasive Fall Risk Assessment
in End Stage Renal Disease Patients on HemodialysisThurmon E. Lockhart, Emaad Abdel-Rahman, John Lach
30

Major Findings:•Get-up & Go Time:
•Post-HD > pre-HD
� after HD session: less mobility
•PLM Simultaneous Index:
Pilot Results
•PLM Simultaneous Index:
•Post-HD < pre-HD
� after HD session: less mobility
•Strength:
•Post-HD < pre-HD
� after HD session: less strength
•Gait parameters and stability:
•No significant difference
�ESRD patients’ fall problem is unique
Pending R21 proposal (NIA) for further exploration and out of clinic monitoring
31

• Parkinson’s disease – study efficacy of deep brain stimulation– Jeffrey Elias, Robert Frysinger (UVA Neurosurgery)
• Parkinson’s disease – study impact of cognitive stress– Scott Wylie (UVA Neurology)
• Normal pressure hydrocephalus – improve diagnosis– Jeffrey Barth, Donna Broshek, Jason Freeman (UVA Neuropsychology)
• Geriatrics – enable fall risk assessment in naturalistic settings
TEMPO in Human Subject Studies
– Thurmon Lockhart (Virginia Tech Locomotion Laboratory)
– Mark Williams (UVA Geriatric Medicine)
– Amy Papadopoulos, Cindy Crump (AFrame Digital)
• Dialysis – study cause of higher fall rates– Emaad Abdel-Rahman (UVA Nephrology)
• Cerebral palsy – study efficacy of orthopedics for children– Brad Bennett (Kluge Children’s Rehabilitation Center)
• Dementia – assess physical agitation– Azziza Bankole, Martha Anderson, Aubrey Knight (Carilion Center for Healthy Aging)
• Multiple sclerosis – gait analysis for early diagnosis– Myla Goldman (UVA Neurology)
32

Enabling Longitudinal Assessment of
Ankle-Foot Orthosis Efficacy for Children with Cerebral Palsy
Bradford C. Bennett, John Lach
• AFO goals
– Facilitate walking by controlling the position of the ankle and providing
a base of support
– Prevent contractures by putting muscles in a lengthened position and
providing variable ranges of motion
– Prevent deformity by controlling the position of the foot/ankle
Ankle-foot orthosis (AFO) Children with equinus pattern gait (A)
and crouch pattern gait (B) deformity
– Prevent deformity by controlling the position of the foot/ankle
• Joint angles, gait moments, and gait velocity assessments in
VICON laboratories
33

AFO-Embedded Inertial Sensing• Validation against VICON
• 4 CP children to date
• Preparation for in-field data collection
• Working with prosthetics manufacturers
Ankle Joint Angle Shank Angular Velocity34

• Parkinson’s disease – study efficacy of deep brain stimulation– Jeffrey Elias, Robert Frysinger (UVA Neurosurgery)
• Parkinson’s disease – study impact of cognitive stress– Scott Wylie (UVA Neurology)
• Normal pressure hydrocephalus – improve diagnosis– Jeffrey Barth, Donna Broshek, Jason Freeman (UVA Neuropsychology)
• Geriatrics – enable fall risk assessment in naturalistic settings
TEMPO in Human Subject Studies
– Thurmon Lockhart (Virginia Tech Locomotion Laboratory)
– Mark Williams (UVA Geriatric Medicine)
– Amy Papadopoulos, Cindy Crump (AFrame Digital)
• Dialysis – study cause of higher fall rates– Emaad Abdel-Rahman (UVA Nephrology)
• Cerebral palsy – study efficacy of orthopedics for children– Brad Bennett (Kluge Children’s Rehabilitation Center)
• Dementia – assess physical agitation– Azziza Bankole, Martha Anderson, Aubrey Knight (Carilion Center for Healthy Aging)
• Multiple sclerosis – gait analysis for early diagnosis– Myla Goldman (UVA Neurology)
35

Continuous, Non-Invasive Assessment of Agitation in
Dementia Using Inertial Body SensorsAzziza Bankole, Martha Anderson, Aubrey Knight, Tonya Smith-Jackson, John Lach
• Agitation is common in dementia patients
– Major caregiver burden
– Changes over time and in response to stimuli
• Approaches to mitigate agitation require evaluation• Approaches to mitigate agitation require evaluation
• Cohen-Mansfield Agitation Inventory (CMAI) requires
sampled expert observation
• Need for continuous, longitudinal monitoring
36

• Explored use of inertial BSNs for
physical agitation assessment
• Jerky, repetitive movements
correlate with physical agitation– Requires joint time-frequency analysis
• Pilot study: six dementia subjects
Inertial BSNs for Agitation Assessment
• Pilot study: six dementia subjects
in long term care facility– Three 3-hour sessions over six weeks
(different times of day)
– Three TEMPO nods (dominant wrist,
waist, and opposite leg) with triaxial
accelerometers
– Suggested Teager energy a good measure
of physical agitation
37

• Epilepsy – detect seizures
• Parkinson’s disease – study fall risk
• Traumatic brain injury – measure head forces
• Dementia – study relationship between agitation & incontinence
• Posture – provide real-time feedback to users
Planned Human Subject Studies
• Posture – provide real-time feedback to users
• Autism – improve diagnosis using motor skill assessment
• Prosthetics – develop smarter controls
• Stroke – track stroke rehabilitation progress via telemedicine
38

Acknowledgments
• This work is funded in part by
– National Science Foundation and National Institutes
of Health
– The UVA Biomedical Innovation Fund and the UVA – The UVA Biomedical Innovation Fund and the UVA
Institute on Aging
– Philips, Carilion Health Systems, and the MITRE
Corporation
39

40
41

ASSIST Platform Evolution
Gen 2: Add
Gen 1:� EKG� NOx
� pH� Skin Resistance� Temperature� Battery Assist
Gen 2: Add � Pulse Oxymetry
� CO, Ozone, H2S
� Skin Resistance
� Stress Response
� Lung Sounds
Gen 3: Add� Ultra-miniature� Particulate Matter� Breath NOx, pH� Self-powered� ~0.1 mJ/sample with
Advanced Computation
42

ASSIST’s Strategic Leadership
43

• Ongoing human subjects studies with clinician and medical researcher collaborators
– Tremor assessment for Parkinson’s Disease study, diagnosis, treatment
– Gait analysis for movement disorder diagnosis and fall risk assessment
– Agitation in dementia patients– Many others… TEMPO sensor node provides 6 degrees of freedom motion
We are using a vertically integrated approach to develop miniature on-body wireless sensor
nodes for continuous, long-term, non-invasive collection of accurate, precise, quantitative data
for a variety of healthcare and medical research applications.
Summary
– Many others…
• Key system metrics– Wearable (small, light, easy to use)– Low power (long lifetime with small battery)– Configurable (adaptable for specific applications)– High fidelity (achieve application requirements)
• Key engineering research thrusts– Embedded, low-power system design– Adaptive wireless communication systems– Resource-constrained DSP algorithms– Sensor fusion– Biomedical analysis and feature detection
• Project goal: Improve quality of medical data and ultimately patients’ health and quality of life while reducing healthcare costs
TEMPO sensor node provides 6 degrees of freedom motion
capture (3 axes of both linear acceleration and rotational rate)
in the form factor of a wristwatch
Gait cycle data collected from an ankle-worn TEMPO node
44

Body Sensor Networks:
An Application-Centric Approach
John LachJohn Lach
Charles L. Brown Department of Electrical & Computer Engineering
University of Virginia





























