-
8/14/2019 Blood Glucose Oki Aziz894180
1/77
Oral glucose Tolerance TestOral glucose Tolerance Testand
Factors Influencing Bloodand Factors Influencing Blood
Glucose Level.Glucose Level. one By bdulaziz Massoud Alfaydi
-
8/14/2019 Blood Glucose Oki Aziz894180
2/77
-
8/14/2019 Blood Glucose Oki Aziz894180
3/77
-
8/14/2019 Blood Glucose Oki Aziz894180
4/77
DefinitionDefinition. The glucose tolerance test (GTT)
Consists of drinking (75 to 100 )gramsof glucose solution
..Measuring the blood glucose values
every hour toget a cerve ..A 2 hour GTT is used to diagnosis
diabetes , but a 6 hour test might alsodiagnosis diabetes plus
hypoglycemia..Symptoms of hypoglycemia occur after
the 5 th hour..In healthy individual the insuline
-
8/14/2019 Blood Glucose Oki Aziz894180
5/77
-
8/14/2019 Blood Glucose Oki Aziz894180
6/77
Referance valuesReferance values
Normal /FPG:Adults: 110mg/dl or 6.1 mmol/L.30-minute
Adults 110-170 mg/dl or 6.1-9.4mmol/L.60- minute PG after
glucose load :
Adults
-
8/14/2019 Blood Glucose Oki Aziz894180
7/77
.3- hours PG afterglucose load:
Adults b70-120
mg/dl or 3.9-6.7mmol/L.All four blood
values must bewithin normallimits to beconsidered normal.
-
8/14/2019 Blood Glucose Oki Aziz894180
8/77
ProcedureProcedure
This is timed test for glucosetolerance . A-2 hourplasma glucose
test is done
after glucose load to detectdiabetes in individuals otherthan
pregnant women .
The 3- hour test is done forpregnant women .The 4- hourtest
evaluates possiblehypoglycemia.
1- Have patiant eat a diet with
-
8/14/2019 Blood Glucose Oki Aziz894180
9/77
Ensure that the following drugsare discontinued 3 dayes
beforethe test because they mayinfluence test results:
a) Hormones , oralcontraceptives , steroids.
b)Salicylates, anti inflammatory
drugs.C)Diuretic agentsd) Hypoglycemic agents.
.e)Antihypertensive drugs
-
8/14/2019 Blood Glucose Oki Aziz894180
10/77
F)Anti convulsants .3-Insuline and oral hypoglycemics
should be with held until the testcompleted .
4- Record the patient s weighta)Pediatric doses of glucose
are
based on body weight. Calculated
as 1.75g/kg not to exceed a totalof 75g.b)Pregnant women 100g
glucose.C) Non pregnant adults 75g
glucose.
-
8/14/2019 Blood Glucose Oki Aziz894180
11/77
5-A 5ml sample of venous blood isdrawn. The patient should fast
12to 16 hours before testing .
6-Bbood samples are obtained 30menutes , 1 hr, 2hrs, 3hrs
afterglucose ingestion.
7- Specimens taken 4 hrs afteringestion are significants
fordetecting hypoglycemia .
8-Tolerance tests can also be
performed for pentose ,lactose-
-
8/14/2019 Blood Glucose Oki Aziz894180
12/77
a) Persistent fastinghyperglycemia >140mg/dl
or>7.8mmol/l.
b) persistent fasting normalplasma glucose .
c)Patient with overt diabetes
mellitus.d)Persistent 2-hour plasmaglucose >200mg/dl
or>11.1mmol/l.
-
8/14/2019 Blood Glucose Oki Aziz894180
13/77
Interfering factorsInterfering factors
1- Smoking increases glucoselevels.
2-Altered diets (weight reduction)
before testing can diminishcarbohydrate tolerance andsuggest
,false diabetes.
Glucose levels normally tend toincrease with aging.3-Prolonged
oral contraceptive
use causes significantly higherlucose levels in the second
-
8/14/2019 Blood Glucose Oki Aziz894180
14/77
5-Infections disease illnesses andoperative procedures
affectglucose tolerance.
6- Certain drugs impair glucosetolerance levels .a) Insulin .b)
Oral hypoglycemics.c)Large doses of salicylates , anti-
inflammatoriesd) Thiazide diuretics.e) Oral contraceptives.
-
8/14/2019 Blood Glucose Oki Aziz894180
15/77
1a. Normal Minimum curve1a. Normal Minimum curveaccording to
Seale Harrisaccording to Seale Harris
Time [hours] 0 0.5 1 2 3 4 5 6
Blood glucose [mg/dl] 80 90 105 90 80 80 80 80
-
8/14/2019 Blood Glucose Oki Aziz894180
16/77
1b. Normal Maximum1b. Normal Maximumcurvecurve
Time [hours] 0 0.5 1 2 3 4 5 6
Blood glucose [mg/dl] 120 135 160 130 110 100 110 105
-
8/14/2019 Blood Glucose Oki Aziz894180
17/77
..diabetesdiabetesTime [hours] 0 0.5 1 2 3 4 5 6
Blood glucose[mg/dl] 115 145 180 160 120 130 130 130
h3 C i h
-
8/14/2019 Blood Glucose Oki Aziz894180
18/77
3. Curve with severe3. Curve with severediabetesdiabetesTime
[hours] 0 0.5 1 2 3 4 5 6
Blood glucose[mg/dl] 200 235 265 280 300 295 280 270
b d4 Di b d
-
8/14/2019 Blood Glucose Oki Aziz894180
19/77
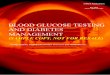
4. Diabetes and4. Diabetes andhypoglycemiahypoglycemia
Time [hours] 0 0.5 1 2 3 4 5 6
Blood glucose[mg/dl] 100 160 220 160 85 60 50 85
-
8/14/2019 Blood Glucose Oki Aziz894180
20/77
5. Continuous low values5. Continuous low values Time [hours] 0
0.5 1 2 3 4 5 6
Blood glucose[mg/dl] 60 80 100 60 60 60 60 55
-
8/14/2019 Blood Glucose Oki Aziz894180
21/77
6. Pre-hypoglycemia6. Pre-hypoglycemia Time [hours] 0 0.5 1 2 3
4 5 6
Blood glucose [mg/dl] 90 115 140 100 85 80 70 75
-
8/14/2019 Blood Glucose Oki Aziz894180
22/77
7. Mild hypoglycemia7. Mild hypoglycemiaTime [hours] 0 0.5 1 2 3
4 5 6
Blood glucose [mg/dl] 80 120 80 60 80 75 80 80
-
8/14/2019 Blood Glucose Oki Aziz894180
23/77
8. Severe hypoglycemia I8. Severe hypoglycemia ITime [hours] 0
0.5 1 2 3 4 5 6
Blood glucose[mg/dl] 95 110 120 105 100 60 40 60
-
8/14/2019 Blood Glucose Oki Aziz894180
24/77
-
8/14/2019 Blood Glucose Oki Aziz894180
25/77
10. Flat curve10. Flat curve Time [hours] 0 0.5 1 2 3 4 5 6
Blood glucose [mg/dl] 90 90 90 100 90 100 80 90
-
8/14/2019 Blood Glucose Oki Aziz894180
26/77
f) Corticosteroids.g) Estrogens.h) Heparin.
i) Nicotinic acid . j) Phenothiazines.k) Lithium .l)
Metryrapone(metopirone).
-
8/14/2019 Blood Glucose Oki Aziz894180
27/77
27
HOMEOSTASIS NORMALHOMEOSTASIS NORMAL
3 Mechanisms:
1.Metabolic2.Hormonal3.Renal
-
8/14/2019 Blood Glucose Oki Aziz894180
28/77
28
MetabolicMetabolic.Dietary-Primary
source of all bodycomponents
Glycogen-Initial-liver(92%), later-
muscle(8%),sufficient for 18 hrsGluconeogenesis:Non-cabohydrates
Glucogenic amino acids all except ,lys,
leu TG Glycerol DHAP Odd chain FA-PropionicAcid
Succinyl CoA Lactate Pyruvate
-
8/14/2019 Blood Glucose Oki Aziz894180
29/77
-
8/14/2019 Blood Glucose Oki Aziz894180
30/77
30
HormonalHormonal
Insulin- cell of Langerhans favoursuptake into cell
Glucagon,
epinephrine,glucocorticoids,GH,thyroxin-antagonists to
insulin,favoursexcessive glycogenolysis andrelease of more glucose
in blood
Cooperative action of both types of hormones help maintaining
theblood glucose
-
8/14/2019 Blood Glucose Oki Aziz894180
31/77
31
RenalRenal
Rates of Glomerularfiltration and Tubular absorption maintain
bloodglucose
Kidney threshold for glucose-180 mg%, more than this spillover
in urine glycosuria
TMG-375 mg/min,more accurate indexthan kidney threshold
-
8/14/2019 Blood Glucose Oki Aziz894180
32/77
10/18/09 32
ABNORMALABNORMAL
HYPERGLYCEMIAHYPOGLYCEMIA
-
8/14/2019 Blood Glucose Oki Aziz894180
33/77
33
HYPERGLYCEMIA:HYPERGLYCEMIA:
DIABETES:10 % population worldwide affected, 2
%>50 y
-
8/14/2019 Blood Glucose Oki Aziz894180
34/77
34
:: Iry (Known causes)Iry (Known causes)
I.IDDM- Insulin deficiencyI.IDDM- Insulin deficiencyAutoimmune
-Immunity mediated(Antibodies to
insulin 50%,antibodies to islet cell cytoplasmicproteins 80%),
idiopathic( damage of cell of islet of Langerhans or viral
infection)
II.NIDDM- Normal insulin but
unavailable(insulinresistance)-Obese(60%),non-obese(40%)(antibodies),MODY
(maturity onset diebetes of young)(Glucokinase ,gene mutated-KT
insulin )
III.Prone -i)Gestation-occurs 15%nondiabetes diabetes, Childrisk
mortality ,BWt ,ii)IFG, iii)IGT
-
8/14/2019 Blood Glucose Oki Aziz894180
35/77
35
IIry (Unknown causes)IIry (Unknown causes)
Pancreatic diseases-pancreatitis,cystic fibrosis
Endocrinopathies-cushing
syndrome,thyrotoxicosis,acromegalyDrug induced-steroids,
blockers
-
8/14/2019 Blood Glucose Oki Aziz894180
36/77
10/18/09 36
GLYCOSURIAGLYCOSURIA
GFR-NC,KT & TMG A. HYPERGLYCEMIC:
Alimentary-IFG
Emotional-sympathetic and splanicnerve excitation
Endocrinal
Experimental-alloxan
-
8/14/2019 Blood Glucose Oki Aziz894180
37/77
37
GLYCOSURIAGLYCOSURIA
B.RENAL:HereditaryAcquired
Threshold ( 180 mg%) Tubular reabsorption
Experimental-phloridzine
-
8/14/2019 Blood Glucose Oki Aziz894180
38/77
10/18/09 38
II.HYPOGLYCEMIAII.HYPOGLYCEMIA
Risk-50 mg%,fatal < 30 mg%Insulin
Thyroid Liver diseasesSevere exerciseGlycogen storage
diseasesAlcohol ingestion.
-
8/14/2019 Blood Glucose Oki Aziz894180
39/77
39
DIEBETES STATUSDIEBETES STATUS
MONITORINGA.Conventional:
Glucose-Blood (GOD-POD)-Urine
Benedict reagent
G Y O R0.5% 1% 1.5% 2->2%
GTT: 1.Lab-Oral GTT (OGTT)
2.Clinic-Post-prandial (meal)
-
8/14/2019 Blood Glucose Oki Aziz894180
40/77
40
B. Modern investigationsB. Modern investigations
1.Glycated Hb(HbA1c) (Normal 4-8%)-1%30% risk (life span
120D)
2.Glycated albumin-fructosamine(life span 20D)
3.Lipid profile4.Microalbuminuria- >300 mg%/D
excretion5.Ketone bodies (Bl.0-2 mg % 125 mg
%,urine 20-60 mg% 5000 mg% /D )
-
8/14/2019 Blood Glucose Oki Aziz894180
41/77
41
Factors affecting GTTFactors affecting GTT
Concerned with the blood glucoseregulation
1.Metabolic-diet-thiamine
-starvation-excretion-liver diseases, infection
2.Hormones-insulin-antagonists
epinephrine,glucagon,glucocorticoids,
GH,thyroxin.
-
8/14/2019 Blood Glucose Oki Aziz894180
42/77
10/18/09 42
GTTGTT
-
8/14/2019 Blood Glucose Oki Aziz894180
43/77
-
8/14/2019 Blood Glucose Oki Aziz894180
44/77
10/18/09 44
MANAGEMENT OFMANAGEMENT OFDIEBETESDIEBETES
Organs involved-side
effects-complications,acute,chronic-multipleorgans.
-
8/14/2019 Blood Glucose Oki Aziz894180
45/77
10/18/09 45
CLINICAL PRESENTATION INCLINICAL PRESENTATION INDMDM
Cardinal Symptoms:Complications1.Poly-urea-Urine (wt.loss)
-dypsea-thirst-water intake -phagia-Food intake
2.Chronic skin infection-Boils-Celluloitis-Absesses
3.Plaques-CVD:CHD+CADMyocardial
infarction4.Retinopathy5.Nephropathy6.Fatty liver
-
8/14/2019 Blood Glucose Oki Aziz894180
46/77
10/18/09 46
7.Ketone bodies8.altered lipid profile
-
8/14/2019 Blood Glucose Oki Aziz894180
47/77
-
8/14/2019 Blood Glucose Oki Aziz894180
48/77
-
8/14/2019 Blood Glucose Oki Aziz894180
49/77
-
8/14/2019 Blood Glucose Oki Aziz894180
50/77
-
8/14/2019 Blood Glucose Oki Aziz894180
51/77
-
8/14/2019 Blood Glucose Oki Aziz894180
52/77
-
8/14/2019 Blood Glucose Oki Aziz894180
53/77
-
8/14/2019 Blood Glucose Oki Aziz894180
54/77
-
8/14/2019 Blood Glucose Oki Aziz894180
55/77
-
8/14/2019 Blood Glucose Oki Aziz894180
56/77
-
8/14/2019 Blood Glucose Oki Aziz894180
57/77
-
8/14/2019 Blood Glucose Oki Aziz894180
58/77
-
8/14/2019 Blood Glucose Oki Aziz894180
59/77
-
8/14/2019 Blood Glucose Oki Aziz894180
60/77
-
8/14/2019 Blood Glucose Oki Aziz894180
61/77
-
8/14/2019 Blood Glucose Oki Aziz894180
62/77
-
8/14/2019 Blood Glucose Oki Aziz894180
63/77
-
8/14/2019 Blood Glucose Oki Aziz894180
64/77
Drug therapy for DKADrug therapy for DKAInsulin therapy: lower
BG by 75-
150mg/dl/hr1. Regular insulin IV bolus dose of .1u/kg
followed by IV drip of .1u/kg/hr.2. SQ insulin when client can
eat and ketosis
has ended.Electrolyte replacement
1. Potassium2. Bicarbonate
-
8/14/2019 Blood Glucose Oki Aziz894180
65/77
Treatment for DKATreatment for DKA
Frequent assessment of client: LOC,V/S, blood glucose levels,
fluid andelectrolyte status
Correct fluid volume deficit1. 1 liter of hypertonic solution
(D51/2NS)
over 8 to 12 hrs.2. 1 liter of isotonic saline over 1 hour3. 1
liter of hypotonic saline over 6 to 8 hrs
-
8/14/2019 Blood Glucose Oki Aziz894180
66/77
Management ofManag
ement of
-
8/14/2019 Blood Glucose Oki Aziz894180
67/77
Management of Manag ement of HypoglycemiaHypoglycemia
Hypoglycemic protocol1. Mild hypoglycemia (BG < 60 and
symptomatic)- 10 to 15g of carbohydrate- Recheck BG in
15minutes
2.Moderate (BG < 40 and symptomatic)-15 to 30g of rapidly
absorbed CHO
3. Severe (BG < 20 and unable to swallow)- 1mg of glucagon
IM/SQ or
amp of D50 IVP
HbAHbA Predicts CHD in TypePredicts CHD in Type
-
8/14/2019 Blood Glucose Oki Aziz894180
68/77
0
5
10
1520
25
0
5
10
1520
25
HD mortali ty(%) .ncidence in 3 5
years
l l CHD events(%) .ncidence in 3 5
years
HbA1c HbA1c
Low< %
Middle- . %7 9
High> .9
%
Low< %
Middle- . %7 9
High> .9
%
HbAHbA 1c1c Predicts CHD in TypePredicts CHD in Type22
-
8/14/2019 Blood Glucose Oki Aziz894180
69/77
ADA Treatment GoalsADA Treatment Goals
Hgb A1C maintained at 7% or below. Premeal blood glucose level
70 to
110mg/dl
Blood glucose at bedtime 100-140mg/Dl
-
8/14/2019 Blood Glucose Oki Aziz894180
70/77
Values for HbAValues for HbA 1c1c
Non-diabetic
-
8/14/2019 Blood Glucose Oki Aziz894180
71/77
Hemoglobin AHemoglobin A 1c1c
A blood testthat showsglucose levelsfor the past 3months
No preparationneeded i.e.fasting, etc.
H b A 1 cH b A 1 c
-
8/14/2019 Blood Glucose Oki Aziz894180
72/77
Checking Blood GlucoseChecking Blood Glucose
CBGs
AccuChecksGlucometerGlucoscan
-
8/14/2019 Blood Glucose Oki Aziz894180
73/77
Lab Assessment for AllLab Assessment for All
Diabetic ClientsDiabetic ClientsBlood tests
1. Fasting Blood GlucoseTest (Cavenaugh pg. 105)
2. Blood GlucoseMonitor Systems2. Oral Glucose
Tolerance Test(Cavenaugh pg. 109)
3. Glycosylated Hemoglobin
Assays (Cavenaugh pg. 112)4. Glycosylated Serum
Proteins and Albumin(Cavenaugh pg. 114)
-
8/14/2019 Blood Glucose Oki Aziz894180
74/77
Type 2 DiabetesTyp e 2 Diabetes
80% are obese10% non-obese10% unstable:may look morelike a Type
1Diabetic
Type 2 DiabetesType 2 Diabetes
-
8/14/2019 Blood Glucose Oki Aziz894180
75/77
Type 2 Diabetes Type 2 DiabetesSigns and SymptomsSig ns and
Symptoms
HyperglycemiaPolyuriaPolydipsiaBlurred
visionFatigueParesthesiasSkin infections
-
8/14/2019 Blood Glucose Oki Aziz894180
76/77
Type 2 DiabetesType 2 DiabetesEtiologyEtiology
There isabnormallyhigh level of glucose
Pancreas does produce insulin
Body resists theinsulinseffects
-
8/14/2019 Blood Glucose Oki Aziz894180
77/77
DIABETES COMPARISONDIABETES COMPARISONTYPE 1TYPE 1 TYPE 2TYPE
2
AutoimmuneProcess: Betacellsdestroyed Insulin deficiency
Has no insulin
IdiopathicGeneticpredisposition
< Age 30
Insulinresistance hassome insulin
Obesity is risk factorPhysical inactivityGenetic
predispositionAdult onset