Embed Size (px)
Citation preview

Blood-Gas and Hemodynamic Responses to Oxygen in AcuteMyocardial Infarction
By ROBERT M. DAVIDSON, M.D., BARRY W. RAMO, M.D., ANDREw G. WALLACE, M.D.,ROBERT E. WHALEN, M.D., AND C. FRANKLIN STARMER, PH.D.
SUMMARYBlood-gas (Pao2) and hemodynamic responses to the inhalation of oxygen were studied in 60
patients with acute myocardial infarction. Patients who were not in heart failure on admissionand did not develop signs of heart failure with n the next 5 days achieved the same Pa02 levelwhile breathing 100% oxygen as did patients without acute myocardial infarction. Patients withpulmonary edema or cardiogenic shock had a very poor Pa02 response to oxygen inhalation. Pa-tients in mild heart failure at the time of study and patients who developed heart failure subse-quent to the study had a Pao0 response intermeliate between the other two groups. This rise ofPa02 with oxygen correlated with the cardiac index and right atrial oxygen prior to inhalation ofoxygen. Uncomplicated patients responded to inhalation of oxygen with a decrease of heart rate,cardiac index, stroke index, and cardiac work, and an increase of peripheral resistance. Patientsin pulmonary edema or cardiogenic shock or with a low cardiac index or low Pa02 responded withonly a slight increase in peripheral resistance. The Pao0 achieved while breathing oxygen ap-
peared to determine the type of hemodynamic response to oxygen. Administration of oxygen topatients with acute myocardial infarction is useful in identifying latent heart failure and in pre-dicting the subsequent clinical course of these patients.
Additional Indexing Words:Heart failure Cardiac catheterization Cardiac output Coronary artery disease
T HE ADMINISTRATION of oxygen to pa-tients with acute myocardial infarction has
long been an accepted mode of therapy. Untilrecently, however, there were remarkably little dataconcerned with the physiologic effects of oxygen insuch patients, and several reports demonstrated avery wide range of changes in blood gases andhemodynamics in response to the inhalation ofoxygen.' 19 This variability among patients withacute myocardial infarction in their response tooxygen is in distinct contrast to normal subjects whoexhibit a consistent increase of arterial P02 (Pa02)and decrease of heart rate and cardiac output.5 20-23Several apparent phenomena might account for the
From Department of Medicine, Division of Cardiology,Duke University Medical Center, Durham, North Carolina.
Supported by grants from the U. S. Public Health Service,HE-05736 and HE-4807, and contract PH-43-67-1440. Dr.Wallace is the recipient of National Institutes of HealthResearch Career Development Award HE-19,949.
Address for reprints: Dr. Andrew G. Wallace, Departmentof Medicine, Duke University Medical Center, Durham,North Carolina 27710.
Received July 20, 1971; revision accepted for publicationNovember 13, 1972.
704
variable response to oxygen among patients withacute myocardial infarction or the differencebetween patients with acute infarction and normalsubjects (i.e. the presence of pulmonary edema, thelevel of arterial oxygen concentration, and theresponse of the myocardium to a change in oxygentension) .
This study was undertaken to examine the effectsof oxygen administration in a large group ofpatients with acute myocardial infarction and tofurther elucidate the factors which determine thehemodynamic and blood gas response. It was hopedthat this information might provide a basis forselecting patients in whom the potentially beneficialeffects of administration of oxygen could be tested.Furthermore, responses to the inhalation of oxygenwere analyzed to determine whether or not theobserved changes could be of value in predictingthe subsequent clinical course of patients with acutemyocardial infarction.
MethodsSixty patients with acute myocardial infarction were
studied within 1 hour of admission to the hospital andgenerally within 24 hours after the onset of symptoms.
Circulation, Volume XLVII, April 1973
by guest on June 6, 2018http://circ.ahajournals.org/
Dow
nloaded from

OXYGEN IN ACUTE MYOCARDIAL INFARCTION
There were 42 males and 18 females, ranging in agefrom 36 to 85 years. All patients who were included inthis study were considered to have had definite acutemyocardial infaretion on the basis of satisfying at leasttwo of the following three criteria: a typical clinicalhistory, electrocardiographic changes of transmuralinfarction (Q waves and S-T changes), and typicalserial changes of serum creatine phosphokinase andeither glutamic oxaloacetic transaminase or lactic aciddehydrogenase.The patients were assigned to one of four groups
according to their clinical status prior to the hemody-namic study. Class I included 28 patients who had no
clinical evidence of heart failure at the time ofadmission to the hospital. Clinical criteria for heartfailure included S3 gallop and/or wet rales and/orshock or pulmonary edema. Thirteen of these 28patients subsequently developed one or more of thephvsical findings of heart failure and will be referred toas class IB. The remaining 15 patients did not developcongestive heart failure and will be referred to as classIA. Class II consisted of 19 patients with findings on
admission of mild-to-moderate congestive heart failure(crepitant rales and/or an S3 gallop). Class IIIconsisted of nine patients with overt pulmonary edema,and class IV included four patients with cardiogenicshock (systolic blood pressure less than 90 mm Hg,urine output of less than 20 cc/hour, cold extremities,and disturbed sensorium). For the purpose of statisticalanalysis, patients in classes III and IV were consideredas one group (III/IV).
In addition to these 60 patients, nine others were
included in our study to serve as controls. Thesepatients were suspected of having acute mvocardialinfarction at the time of admission but were subse-quently found to lack objective evidence for thisdiagnosis. Six had arteriosclerotic heart disease, andthree were not thought to have heart disease. None ofthe control patients had heart failure; their mean age
was 49 years. No patient was included in this study ifhe had evidence of parenchymal or obstructive lungdisease, an oral temperature greater than 38°C, or a
hematocrit of less than 35%. No patient receivedmedication within 30 min prior to study. Informedconsent was obtained from each patient or from hisfamily.The patients were studied in the catheterization
laboratorv on the Myocardial Infarcton Research Unit.A no. 7 Zucker catheter (U. S. Catheter and InstrumentCorporation, Glens Falls, New York) was passedthrough a basilic or femoral vein under local anesthes;aand positioned in the high right atrium underfluoroscopic control. A no. 16 Teflon needle (Longwell,Becton-Dickson Company, Rutherford, New Jersey)was placed in the radial or femoral artery. Arterial andright atrial pressures were measured using as zero
reference a point 10 cm above the surface of thecatheterization table. Pressures were measured withHewlett-Packard transducers (no. 1280C) and re-
corded on a Hewlett-Packard data acquisition system.Cardiac output was estimated by the dye dilutiontechnic. Indocyanine green dye was injected into theright atrium, and blood was withdrawn continuouslyCirculation, Volume XLVII, April 1973
from the radial or femoral artery through a Watersdensitometer (XP-302). Dye curves were calibratedusing the patient's blood to which a known amount ofdye was added; and cardiac output was calculated bythe method of Thompson et al.24,25 Samples of arterialand right atrial blood were placed in ice immediatelyafter being drawn, and blood gases were measuredwithin 30 min. Arterial PO,, was measured withan Instrumentation Laboratories Blood Gas Sys-tem (113S2). Oxygen saturation was measured on areflection oximeter (American Optical Company model1824). The oximeter was calibrated using standardssupplied with the machine and by the method of VanSlyke and McNeal.26 The oximeter was linear when theoxygen saturation was between 37 and 100%. A linearregression equation derived from the correlationbetween the oximeter and Van Slyke values wasdeveloped to correct the oximeter reading. Theequiation was: oxygen saturation =-13.692 + 1.137(oximeter reading) (r = 0.997; SEE 1.7%).Each patient was studied while breathing room air
and after 10 min of breathing 100% oxygen. Oxygenwas delivered through a rebreathing-type plastic facemask at a flow rate of 8-10 liters/min. This method ofadministering oxygen was chosen because of itscommon use in the clinical setting. The quantitativeresults of our study cannot, however, be extrapolated tosituations where other methods of administering oxygenare employed. Each patient was studied in therecumbent or near-recumbent position. Total peripheralresistance (TPR, in units) was calculated according tothe formula:
TPR_--mean aortic pressure - right atrial pressurecardiac output
Cardiac work (in kg-m/min) was calculated accordingto the formula:
Work mean arterial pressure x cardiac output x 13.61000
(where pressures are in mm Hg, and cardiac output isin liters/min). Analysis of variance was used to test thedifference of a selected variable across patient classes.The paired t test was used to test differences within apatient class while breathing room air or oxygen. Thescheffe contrast was used to indicate pairs of patientclasses which were different.
ResultsThe mean arterial P02 (Pa02) while breathing
room air was found to correlate with the clinicalclass of the patient at the time of admission to thehospital. Highest values were observed in controlpatients, and progressively lower values wereobserved in patients with acute infarction and withincreasing severity of heart failure (table 1). Therewas considerable overlap, however, between thePa02 values of individual patients in differentclasses; the difference between mean Pa02 inadjacent classes was not statistically significant.
705
by guest on June 6, 2018http://circ.ahajournals.org/
Dow
nloaded from

DAVIDSON ET AL.
Table 1
Change of Pao0 in Response to Oxygen
Pao2 (mean +E SE, mm Hg)Patient group No. of patients Room air 02 02-air diff
Conitrols 9 84 - 4 306 - 27 223 - 27Actute myocardial infarction:
Class I 28 72 2 268 11 196 13Class IA 15 76 - 3 307 - 15 231 - 13ClaKssIB 13 67=3 21a18 1.5)1=218Class II 16 65 -=5 243 -24 178 -22Class III/IV 13 50 3 111 - 14 61l- 12
Cardiac index (liters/minm/M2)> 2.5 18 66 4 261- 21 195- 20< 2.5 1 -5 a 8 4 185 27 127 24
Right atrial °2 sat(, ):> 60 2.3) 70 - 3 262 16 192 14<60 22 58- 4 182 24 124=215
During inhalation of oxygen the differencebetween classes became much more apparent thanduring inhalation of room air, as shown in figure 1.The response of the arterial Po2 to inhalation ofoxygen was virtually identical in control andclass IA patients and differed markedly from theresponses observed in classes IB and II patients.Patients who were either class III or IV had an
350
300-
IA*CONTROL
2E50
£200 i.xEE
0a 150
Figure 1
Each hatched area represents the mean and SE of Pa02values for each group of patients while breathing room air(left) and 100% oxygen (right). The responses of the threegroups (IA and control, IB and II, and IIl/IV) were dis-tinctly different.
even greater reduction of the Pa02 response toinhalation of oxygen. The difference between thesethree groups (control and IA, IB and II, andIII!IV) with respect to the change of Pa02produced by oxygen was highly significant(P<0.01).The individual Pa02 values of each class I patient
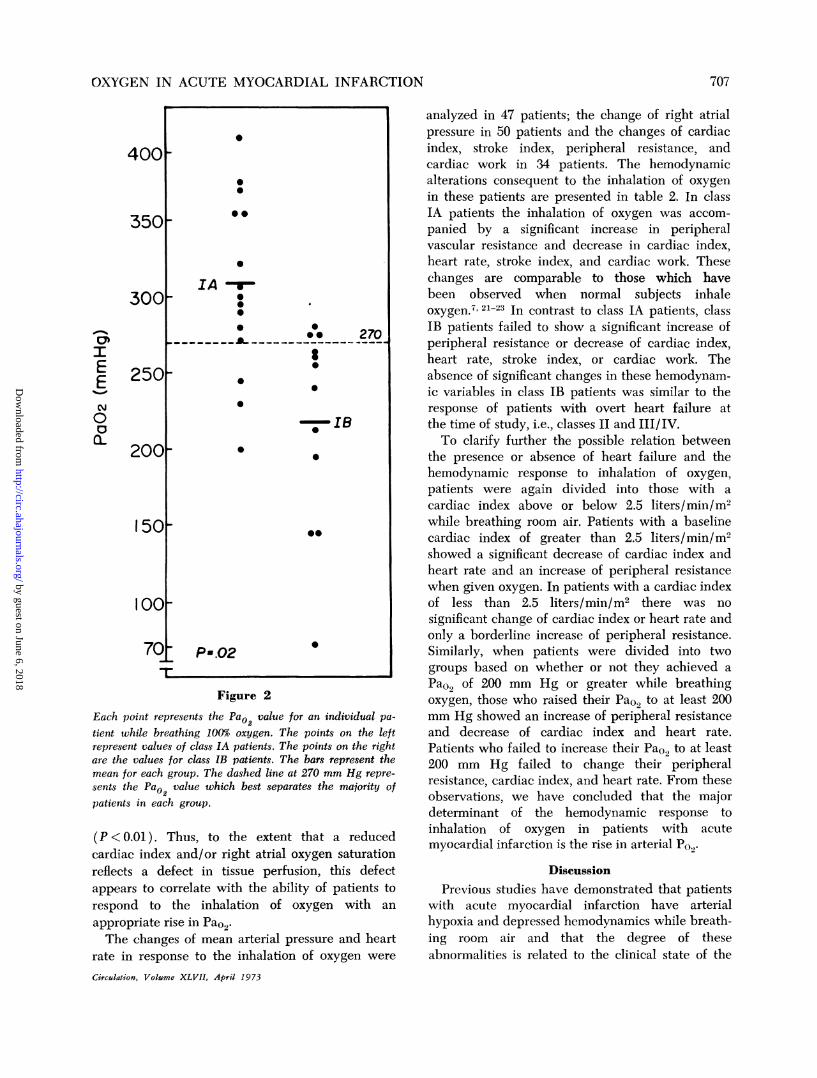
are shown in figure 2 (while breathing oxygen).The mean Pao0 of class IA patients was significantlyhigher than class IB patients (P < 0.025). Althoughthere was overlap of values in the range from 200 to300 mm Hg, only three of the class IA patients hada PaO2 of less than 270 mm Hg and only three of theclass IB patients had a Pao2 of greater than 270 mmHg. From these observations, we have concludedthat the Pa0, while breathing oxygen correlatesbetter with clinical class, and with the subsequentdevelopment of heart failure, than does the Pa02while breathing room air.To elucidate further the possible relation between
Pa0., and the degree of heart failure, correlationsbetween Pa02 and either cardiac index or rightatrial oxygen saturation were examined. In thegroup of patients with a cardiac index of less than2.5 liters/min/m2 the Pa02 while breathing oxygenwas 185 ±27 mm Hg, while in the group with acardiac index of 2.5 liters/min/m2 or greater thePaO, was 261 + 21 mm Hg (P < 0.05). A similardifference was noted when patients were separatedon the basis of their right atrial oxygen saturationwhile breathing room air. In the group with a rightatrial oxygen saturation of less than 60%, the Pa02while breathing oxygen was 182 ± 24 mm Hg,while in those with a right atrial oxygen saturationof 60% or greater the Pa02 was 263 ± 16 mm Hg
Circulation, Volume XLVII, April 1973
70)6
by guest on June 6, 2018http://circ.ahajournals.org/
Dow
nloaded from
OXYGEN IN ACUTE MYOCARDIAL INFARCTION
400[
3501
3001
I
E
N
0c-
250[
2001
150[
100[
T~~~~~~~~~~~~~~Figure 2
Each point represents the Pa02 value for an individual pa-tient while breathing 100% oxygen. The points on the leftrepresent values of class IA patients. The points on the rightare the values for class IB patients. The bars represent themean for each group. The dashed line at 270 mm Hg repre-sents the Pa02 value which best separates the majority ofpatients in each group.
(P < 0.01). Thus, to the extent that a reducedcardiac index and/or right atrial oxygen saturationreflects a defect in tissue perfusion, this defectappears to correlate with the ability of patients torespond to the inhalation of oxygen with anappropriate rise in Pa02.The changes of mean arterial pressure and heart
rate in response to the inhalation of oxygen were
Ciuculation, Volume XLVII, April 1973
analyzed in 47 patients; the change of right atrialpressure in 50 patients and the changes of cardiacindex, stroke index, peripheral resistance, andcardiac work in 34 patients. The hemodynamicalterations consequent to the inhalation of oxygenin these patients are presented in table 2. In classIA patients the inhalation of oxygen was accom-panied by a significant increase in peripheralvascular resistance and decrease in cardiac index,heart rate, stroke index, and cardiac work. Thesechanges are comparable to those which havebeen observed when normal subjects inhaleoxygen.7' 21-23 In contrast to class IA patients, classIB patients failed to show a significant increase ofperipheral resistance or decrease of cardiac index,heart rate, stroke index, or cardiac work. Theabsence of significant changes in these hemodynam-ic variables in class IB patients was similar to theresponse of patients with overt heart failure atthe time of study, i.e., classes II and III/IV.To clarify further the possible relation between
the presence or absence of heart failure and thehemodynamic response to inhalation of oxygen,patients were again divided into those with acardiac index above or below 2.5 liters/min/m2while breathing room air. Patients with a baselinecardiac index of greater than 2.5 liters/min/m2showed a significant decrease of cardiac index andheart rate and an increase of peripheral resistancewhen given oxygen. In patients with a cardiac indexof less than 2.5 liters/min/m2 there was nosignificant change of cardiac index or heart rate andonly a borderline increase of peripheral resistance.Similarly, when patients were divided into twogroups based on whether or not they achieved aPa02 of 200 mm Hg or greater while breathingoxygen, those who raised their Pa02 to at least 200mm Hg showed an increase of peripheral resistanceand decrease of cardiac index and heart rate.Patients who failed to increase their Pa02 to at least200 mm Hg failed to change their peripheralresistance, cardiac index, and heart rate. From theseobservations, we have concluded that the majordeterminant of the hemodynamic response toinhalation of oxygen in patients with acutemyocardial infarction is the rise in arterial PO2.
DiscussionPrevious studies have demonstrated that patients
with acute myocardial infarction have arterialhypoxia and depressed hemodynamics while breath-ing room air and that the degree of theseabnormalities is related to the clinical state of the
0
00
0@
IA -r-0
* 00*o 270a
. IS0
0
0~~~~~~~~
*-1
_ =02 s
P-.02 070
707
by guest on June 6, 2018http://circ.ahajournals.org/
Dow
nloaded from

DAVIDSON ET AL.
Table 2
Hemnodynamic Responses to Oxygen (Mean ± SE)
AP (mm HIg) HR (heats/min) CI (litersmin/rn') SI (ml/beat/M2) TPR (units)Patient group Air 02 Air 02 Air 0e Air 02 Air 02
Class IA 104 4 105 4 78 4 73 4 3.4 0.4 2.9 0.4 44-5 38- 4 19 3 23 4% change +1 -6 - 15 -14 +21P value NS <0.01 <0.001 <00005 <0.00.3
Class IB 98 A 102=8 85 5 83 - 5 2.8 0.2 2.7 - 0.2 34 4 33 ff4 18+ 1 19='1% chanige +4 -2 -3 -3 +-P value NS NS NS NS NS
Class II 98 4 97 4 89 5 85 - 5 2.7 0.2 2.6 -0.3 33 3 32 3 21 2 23 -3' change -1 -4 -4 -3 +6P value xs <0.02 NS NS NS
Class III/IV 87 7 93 i9 101 5 101 4 2.0 0.2 1.9 0.2 20 1 20 1 27 2 30 i2%change +7 0 0 0 +12P value <0.01 NS NS .S <0.02
CI (liters `mi/m2):>2.51 101 4 103 4 84 4 79 5 3.4 0.2 3.1 0.1 42 3 39 3 17 1 19 1/C change +1 -6 -9 -7 +12P value NS <0.001 <0.02 <0.03) <0.()1<2.5 96 - 6 101 7 90 - 5 88 4 2.0 - 0.1 2.0 - 0.1 24 1 23 - 1 27 2 30 2ac chanige +5 2 0 -4 +11P value <0.01 NS NS NS <0.05
Pao2 (mm Hg):>200 101 3 102 3 84 - 3 79 - 3 3.1 0.2 2.8 - 0.2 37 3 34 3 19 2 22 2% change +1 -6 -10 -8 +15P value Ns <0.001 <0.005 <0.005 < 0.005<200 91 .5 97 6 94 5 94 - 5 2.3 0.2 2.3 0.2 28 4 28 - 4 24 2 26 2/0 chanige +7 0 0 0 +6P value <0.001 NS NS NS NS
Abbreviations: AP = arterial pressure; HR = heart rate; CIresistance; NS = not significant.
patients.2, 3, 7, 5, 10-12, 15, 18, 19, 27-33 Several studieshave also suggested that the changes of arterial Po2and cardiac output which result from the adminis-tration of oxygen are abnormal.4' 7, 5, 10, 11, 16, 19, 32The present study provides additional data whichare in general agreement with those observations.Furthermore, our data suggest that examiningblood-gas and hemodynamic responses to oxygencan be of value in predicting the subsequentdevelopment of clinical heart failure in patientswho do not have obvious signs of heart failure atthe time of admission to the hospital.
Arterial Po2 values correlated with clinical classas well as with cardiac index and right atrial oxygensaturation. Differences of mean values of Pao2 weresmall between clinical classes while breathing roomair, but these differences were magnified during theinhalation of oxygen. While breathing 100%, oxygen,patients could be clearly separated into threegroups. Maximal Pa02 was noted in the controland class IA patients, and the lowest Pao2 valueswere observed in class JII/IV patients. The
cardiac index; SI = stroke iadex; TPR = total peripheral
classes IB and II patients had an intermediateresponse. Regardless of clinical class, patients witha low cardiac index or a low right atrial oxygensaturation had a much smaller increase of Pao0when given oxygen than patients with a higherbaseline cardiac index and right atrial oxygensaturation. These observations suggest that patientswith acute myocardial infarction, but with minimalor no reduction of cardiac output, resemble normalsubjects in their response to inhalation of oxygen.However, patients with acute myocardial infarctionand objective evidence of reduced ventricularperformance show a reduced ability to oxygenatetheir arterial blood when they are given oxygen. Thefact that the response of arterial P02 to inhalation ofoxygen correlates better with hemodynamic mea-surements than it does with clinical class, and thatclass IB patients show a significantly differentresponse than class IA patients, supports thisview.
Several mechanisms have been postulated toexplain the arterial hypoxia which is observed inmany patients with acute myocardial infarction.
Circulation, Volume XLVII, April 1973
708
by guest on June 6, 2018http://circ.ahajournals.org/
Dow
nloaded from
OXYGEN IN ACUTE MYOCARDIAL INFARCTION
These include ventilation-perfusion abnormal-ities, anatomic right-to-left shunting, reducedcardiac output, atelectasis, and diffusionabnormalities.8 10-13.15-19,32.34-38 The existence ofventilation-perfusion abnormalities in patients withmyocardial infarction has recently been demon-strated by Kazemi and co-workers.35 Their datasuggest that decreased perfusion of the lung basesmay result, at least in part, from an elevatedpulmonary venous pressure and interstitial edema.Improvement of Pa09 after the administration of adiuretic" supports this thesis. Pulmonary arterialpressure was not measured in the present series ofpatients, but recent studies have shown thatpatients with acute myocardial infarction andelevated pulmonary artery diastolic or wedgepressures are more hypoxemic than patients withnormal pressures.39' 40
It also has been suggested that a reduced cardiacoutput per se may contribute to arterial hypoxia anda decrease in the oxygen saturation of mixed venousblood.18 The association of a low cardiac output anda low right oxygen saturation with a poor Pao2response to oxygen was demonstrated in the presentstudy. The cardiac output and/or the right atrialoxygen saturation may be important in determiningthe Pao2 response to inhalation of oxygen, but acausal relation between these variables is difficult toprove.The hemodynamic responses to oxygen also can
be related to clinical class, to cardiac index, and toarterial oxygen saturation. In previous studies,patients who appeared clinically and hemodynam-ically to be uncomplicated responded to theinhalation of oxygen with a decrease of heart rateand cardiac output. Patients in cardiogenic shock orthose with a very low cardiac output or markedhypoxemia responded to oxygen with only a slightincrease in cardiac output and in arterial pres-sure.7' 8, 10 In the present study, uncomplicatedpatients demonstrated a decrease in heart rate,cardiac index, and cardiac work, and an increase inperipheral resistance. Patients in acute pulmonaryedema or cardiogenic shock or those with a lowcardiac index or moderate to severe hypoxemiashowed only a slight increase of peripheralresistance with inhalation of oxygen and no othersignificant hemodynamic changes. The ability toachieve a Pao0, of 200 mm Hg or greater duringinhalation of oxygen appeared to be the mostimportant factor determining the type of hemody-namic response.Circulation, Volume XLVII, April 1973
Patients with acute myocardial infarction andnormal subjects appear to differ in the mechanismof the reduction of cardiac output during theinhalation of oxygen. In normal subjects, thereduction of output is due entirely to a decrease inheart rate, since there is no accompanying reductionin stroke volume.22 23 This is apparently a reflexmechanism since it can be prevented with atro-pine.22 In subjects with uncomplicated myocardialinfarction there is a decrease in stroke volume aswell as cardiac output.1 4 13 At the present timethere is no evidence in man that arterial PO2 valuesin the range observed in this study exert a directinotropic action on the heart. The possibility of anegative inotropic action of oxygen should beconsidered, however, because at least two reportshave shown that oxygen at hyperbaric pressuresexerts a direct suppressive action on myocardialcontractility in experimental animals.41 42The finding of most immediate clinical interest in
this study was that patients who appeared uncom-plicated at the time of admission, but who laterdeveloped clinical evidence of heart failure (classIB) had a distinct difference in their arterial PO,,response to oxygen when compared to patients whoremained free of heart failure (class IA). Our datawould suggest that it is possible to identify patientswho are in subclinical heart failure by measuringtheir Pa0.) after breathing oxygen for 10 min. Theearly identification of such patients using this testmay be a convenient and reliable way to predictheart failure, and thus to identify a group in whomthe efficacy of therapeutic interventions includingoxygen could be evaluated.
References1. THOMAS M, MALMCRONA R, SHILLINGFORD T: Haemo-
dynamic effects of oxygen in patients with acutemyocardial infarction. Brit Heart J 27: 401, 1965
2. SHILLINGFORD T, THOMAS M: Hemodynamic effects ofacute myocardial infarction in man. Progr CardiovascDis 9: 571, 1967
3. SHILLINGFORD TP, THOMAS M: Cardiovascular andpulmonary changes in patients with myocardialinfarction treated in an intensive care and researchunit. Amer J Cardiol 20: 484, 1967
4. KENMURE ACF, MURDOCH WR, BEATTIE AD,MARSHALL PCB, CAMERON AJV: Circulatory andmetabolic effects of oxygen in myocardial infarction.Brit Med J 4: 360, 1968
5. PAIN MCF, STANNARD M, SLOMAN G: Disturbances ofpulmonary function after acute myocardial infarction.Brit Med J 2: 591, 1967
6. EDITORIAL: Oxygen in acute myocardial infarction.Lancet 2: 525, 1969
709
by guest on June 6, 2018http://circ.ahajournals.org/
Dow
nloaded from

DAVIDSON ET AL.
7. FOSTER GL, CASTEN GC, REEVES TJ: The effects ofoxygen breathing in patients with acute myocardialinfarction. Cardiovasc Res 3: 179, 1969
8. SUKUMALCHANTRA Y, LEVY S, DANZIG R, RUBENS S.ALPERN H, SWAN HJC: Correcting arterial hypox-emia by oxygen therapy in patients with acutemyocardial infaretion. Amer J Cardiol 24: 838,1969
9. FRIEDBERG CK: General treatment of acute myocardialinfarction. Circulation 40 (suppl IV): IV-252, 1969
10. MACKENZIE CJ, TAYLOR SH, FLENLEY DC, MCDONALDAH, STAUNTON HP, DONALD KW: Circulatory andrespiratory studies in myocardial infarction andshock. Lancet 2: 825, 1964
11. McNICOL WM, KTRBY BJ, BHOOLA KD, EVERST ME,PRICE HV, FREEDM\.AN SF: Pulmonary function inacute myocardial infarction. Brit Med J 2: 1270,1965
12. VALENTINE PA, FLUCK DC, MOUNSEY JPD, REID D,SHILLINGFORD JP, STEINER RE: Blood-gas changesafter acute myocardial infarction. Lancet 2: 837,1966
13. CAMERON AJV, HUTrON I, KENMURE ACF, MURDOCHWR: Haemodynamic and metabolic effects ofhyperbaric oxygen in myocardial infarction. Lancet2: 833, 1966
14. HuTTON I, KENMURE ACF, MURDOCH WR, CAMERONAJV: Haemodynamic, respiratory, and metabolicchanges following acute myocardial infarction, withspecial reference to effects of hyperbaric oxygen. BritHeart J 28: 852, 1966
15. HIGGs BE: Factors influencing pulmonary gas exchangeduring the acute stages of myocardial infarction. ClinSci 35: 115, 1968
16. STORSTEIN 0, RASMUSSEN K: The cause of arterialhypoxemia in acute myocardial infarction. Acta MedScand 183: 193, 1968
17. CHERRNIACK RM, CUDDY TE: Respiratory insufficiencyin acute myocardial infarction. Canad Med Ass J101: 84, 1969
18. SUKUMALCHANTRA Y, DANZIG R, LEVY SE, SWAN HJC:The mechanism of arterial hypoxemia in acutemyocardial infarction. Circulation 41: 641, 1970
19. FILLMIORE SJ, SHAPIRO M, KILLIP T: Arterial oxygentension in acute myocardial infarction: Serial analysisof clinical state and blood gas changes. Amer Heart J79: 620, 1970
20. BARRATT-BOYES BG, WOOD EH: The oxygen saturationof blood in the vena cavae, right heart chambers andpulmonary vessels of healthy subject. J Lab Clin Med50: 93, 1957
21. BARRATT-BOYES BG, WOOD EH: Cardiac output andrelated measurements and pressure values in the rightheart and associated vessels, together with an analysisof the hemodynamic response to the inhalation ofhigh oxygen mixtures in healthy subjects. J Lab ClinMed 51: 72, 1958
22. DALY WJ, BONDURANT S: Effects of oxygen breathingon the heart rate, blood pressure, and cardiac indexof normal men: Resting, with reactive hyperemia,and after atropine. J Clin Invest 41: 126, 1962
23. WHALEN RE, SALTZMAN HA, HOLLOWAY DH JR,MCINTOSH HD, SEIKER HO, BROWN IW: Cardiovas-cular and blood gas responses to hyperbaric oxygen.Amer J Cardiol 15: 638, 1965
24. THOMPSON HK, STARMER CF, WHALEN RE, MCINTOSHHD: Indicator transit time considered as a gammavariate. Circ Res 14: 502, 1964
25. STARMER CF, CLARK DO: Computer computations ofcardiac output using the gamma function. J ApplPhysiol 28: 219, 1970
26. VAN SLYKE DD, MCNEIL JM: The determination ofgases in blood and other solutions by vacuumextraction and monometric measurements. J BiolChem 61: 523, 1924
27. FRIES ED, SCHAPNER HW, JOHNSON RL, SCHREINERGE: Hemodynamic alterations in acute myocardialinfarction: I. Cardiac output, mean arterial pressure,total peripheral resistance, "central" and total bloodvolumes, venous pressure and average circulationtime. J Clin Invest 31: 131, 1952
28. SMITH WW, WIKLER NS, Fox AC: Hemodynamicstudies of patients with myocardial infarction.Circulation 9: 847, 1954
29. GILBERT RP, GOLDBERG M, GRIFFIN J: Circulatorychanges in acute myocardial infarction. Circulation9: 847, 1954
30. LJUNGSTRO\I B, JOHANSSON BW, SIEVERS J: ArterialP02, pH and standard bicarbonate in patients with anacute myocardial infarction. Cardiologia 51: 138,1967
31. GOLDMAN RH, BRANIFF B, HARRISON DC, SPIVAC AP:The use of central venous oxygen saturationmeasurements in a coronary care unit. Ann InternMed 68: 1280, 1968
32. VALENCIA A, BURGESS JH: Arterial hypoxemia follow-ing acute myocardial infarction. Circulation 40: 641,1969
33. RAMO BW, MYERS N, WALLACE AG, STARMER F,CLARK DO, WHALEN RE: Hemodynamic findings in123 patients with acute myocardial infarction onadmission. Circulation 42: 567, 1970
34. HARDY W, AYRES S, KEYLOUN V, GRACE W: Causes ofhypoxemia and alkalemia in acute myocardialinfarction. (Abstr) Circulation 38 (suppl VI): VI-94,1968
35. KAZEMI H, PARSONS EF, VALENCA LM, STRIEDER DJ:Distribution of pulmonary blood flow after myocar-dial ischemia and infarction. Circulation 41: 1025,1970
36. EVANS CT, SCHEINMAN M: Relationships betweenptulmonary artery pressures, flow, and right to leftshunts in acute myocardial infarction. (Abstr)Circulation 42 (suppl III): III-152, 1970
37. EVANS CT, HOWAR R, SCHEINMAN MM: Mechanism ofright to left intrapulmonary shunts in acutemyocardial infarction. (Abstr) Amer J Cardiol 26:632, 1970
38. AYRES SM, MUELLER H, GIANNELLI S JR, FLEMING P,GRACE WJ: The lung in shock: Alveolar-capillary gasexchange in the shock syndrome. Amer J Cardiol 26:588, 1970
Circulation Volume XLVII, April 1973
710
by guest on June 6, 2018http://circ.ahajournals.org/
Dow
nloaded from

OXYGEN IN ACUTE MYOCARDIAL INFARCTION
39. LASSERS BW, GEORGE M, ANDERTON JL, HIGGINS MR,PHILP T: Left ventricular failure in acute myocardialinfarction. Amer J Cardiol 25: 511, 1970
40. SJOGREN A: Left heart failure in acute myocardialinfarction. Acta Med Scand (suppl 510): 1, 1970
41. KIoscHos JM, BEHAR VS, SALTZMAN HA, THOMPSON
HK, MYERS NE, SMITH WW, MCINTOSH HD: Effectof hyperbaric oxygenation on left ventricular func-tion. Amer J Physiol 216: 161, 1969
42. MAUNEY FM JR, WAXMAN MB, MoRms JJ, ROTMANME: Cardiac oxygen toxicity. Curr Top Surg Res 2:359, 1970
.Circulation, Volume XLVII, April 1973
711
by guest on June 6, 2018http://circ.ahajournals.org/
Dow
nloaded from

and C. FRANKLIN STARMERROBERT M. DAVIDSON, BARRY W. RAMO, ANDREW G. WALLACE, ROBERT E. WHALEN
Blood-Gas and Hemodynamic Responses to Oxygen in Acute Myocardial Infarction
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1973 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.47.4.704
1973;47:704-711Circulation.
http://circ.ahajournals.org/content/47/4/704Wide Web at:
The online version of this article, along with updated information and services, is located on the World
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer in the
Permissions in the middle column of the Web page under Services. Further information about this process is availableOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Circulation Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 6, 2018http://circ.ahajournals.org/
Dow
nloaded from





























