Embed Size (px)
Citation preview

Biostatistics Case Studies 2006
Peter D. Christenson
Biostatistician
http://gcrc.LAbiomed.org/Biostat
Session 4:
An Alternative to Last-Observation-Carried-Forward:
Last-Rank-Carried-Forward

Motivation for Session Topic
• Setting: Baseline, intermediate, and final visits.• Primary outcome: change from baseline to final visit.• Not all subjects are measured at final visit.
• Analysis of completers is not ITT.• Popular alternative: carry forward values at last intermediate visit to the final visit (LOCF).
• If progressive disease: LOCF under-estimates placebo group.• If progressive treatment effect: LOCF under-estimates treated group.

Today’s Method: LRCF Idealized
Change from Baseline
Baseline Final VisitIntermediate Visit
0
Change from Baseline
Intermediate Visit
Final VisitBaseline
0
LOCF:
Ignore Presumed
Progression
LRCF:
Maintain Expected Relative
Progression
Individual Subjects

Basic Issues
• Reasons for missing data:• Administrative choice: long-term study ends; early termination; interim analyses.• Related to treatment; subject choice. Unknown.
• Time-specific or global differences between treatments:• Time course or Specific times or Only at end?• Do groups differ in the following Kaplan-Meier curves?
“Well, in the long run, we’re all
dead.”
Milton Freidman, Economist0.
000.
250.
500.
751.
00
0 2 4 6 8Year
group = 1 group = 2
Kaplan Meier Survival

Some Typical Summaries
1. Use all available data: • only in graphs, not analysis.• in analysis with mixed models• in analysis with imputation from modeling.
2. Use only completers:• Sometimes only require final visit.• Sometimes require all visits.
3. Last-observation-carried-forward (LOCF):• Project last value to all subsequent visits• Sometimes interpolate for intermediate missing visits.
Last session: Cumulative change is an alternative method that is better than (2) or (3).

Last Week’s Method: Use Successive ΔsFigure 2: Carvedilol
Week
0 2 4 6 8 10
DB
P
88
90
92
94
96
98
100
102
104
106
N=100 N=100 N=94 N=87 N=83
Mean +/- SE
0
12
-10.2
-8.3
Valid est of Δ24 from N=94
Cumulative Change
Valid est of Δ02 from N=100
Δ46 from N=87 -11.8
Δ6-12 from N=83

Today’s Method
• Used when only interest is in baseline to final visit change.
• Need data at one or more intermediate visits.
• Less bias than LOCF.
• More power than Completer analysis.
• More intuitive than mixed models for repeated measures (MMRM).
• Less robust than MMRM if dropout is related to subject choice.
• O’Brien(2005) Stat in Med; 24:341-358.

Case Study
Henry K., et al, for the AIDS Clinical Trial Group 193A Study Team:
A randomized, controlled, double-blind study comparing the survival benefit of four different reverse transcriptase inhibitor therapies for the treatment of advanced AIDS.
J AIDS 1998;19:339-349.

ACTG Study 193A Outline
1313 AIDS subjects with CD4 ≤ 50 cells/mm3
Randomized to one of 4 regimens (combinations of HIV RT inhibitors, all with ZDV).
Clinical visits every 8 weeks; lab samples every 16 weeks up to 48 weeks; mortality status at study end.
Primary outcome is survival time. We will ignore.
A secondary outcome is CD4 count over time.• We will analyze several ways.• Table 3 – top half.

Comments on Study
Only 25% of subjects completed the study or died.
Most subjects discontinued due to toxicity, too ill, changing to other therapies.
Intention-to-treat analysis was used.
Paper only reports statistical comparisons for baseline to week 16 CD4 cell count changes.

Our Goal
Suppose outcome of interest is CD4 change from baseline to 32 weeks.
We have CD4 data between 0 and 40 weeks: N=1299 at baseline; 973 at week 16; 759 at week 32.
We compare three methods: • Use only the 759 week 32 “completers”.• Use last-observation-carried-forward to assign
week 16 changes to week 32 for subjects not measured at 32 weeks.• Apply new method: carry forward ranks at week
16 to week 32.
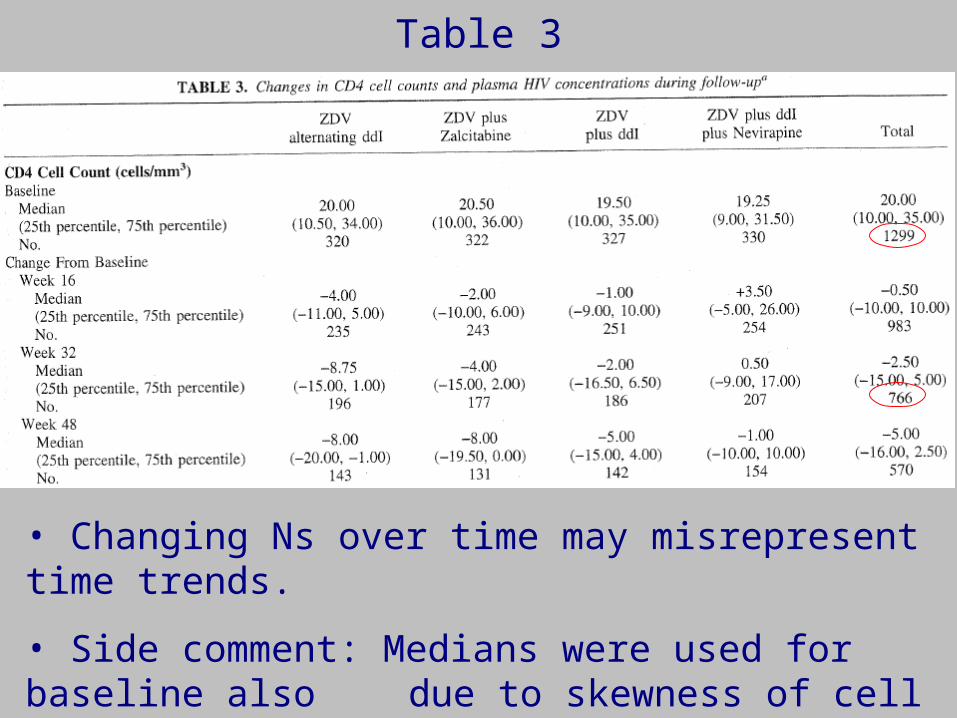
Table 3
• Changing Ns over time may misrepresent time trends.
• Side comment: Medians were used for baseline also due to skewness of cell count distributions; see next slide.

Table 3: Baseline CD4 Distribution
0 24 48 72 96 120 144 168
0
5
10
15
20
25
30
35
Percent
cd4
0 0. 6 1. 2 1. 8 2. 4 3 3. 6 4. 2 4. 8
0
2. 5
5. 0
7. 5
10. 0
12. 5
15. 0
Percent
l ogCD4
Actual counts Log(count+1)
Mean +/- 2SD
Median w/ 95% limits
-18

Subjects with Measured Changes
Number of Subjects with Data
Week 32:
Yes
Week 32:
No Total
Week 16: Yes 701 272 973
Week 16: No 58 * 58
Total 759 272 1031
• Thus, 1031 subjects with info on at least 1 change.
• Paper: 983, not 973; 766, not 759. (? Mistiming, +/- 4 weeks.)
*268
Baseline 1299

Goal: Replace Median Counts using a Common N:
• The published method requires at least one post-baseline value.
• We will thus use N=1031. Applying to N=1299 would probably be preferable to LOCF on 1299.
1031?
1299 or 1031

LRCF: Algorithm
1. Rank subjects at visit 1 according to change from baseline to visit 1. [All subgroup groups pooled.]
2. Rank subjects at visit 2 according to change from baseline to visit 2.
3. Subjects unranked at visit 2 are assigned their rank from visit 1, if available.
4. Some of the other subjects at visit 2 (who have actual ranks then) have their ranks shifted upward to accommodate the non-completers who are using visit 1 rank.
5. If necessary, make adjustment for tied ranks. See O’Brien.
6. Repeat at visit 3 using visit 2 assigned ranks; loop to end.

LRCF: ExampleID T0 T1 T2 T3
1 31 21 18 12
2 40 28 . .
3 34 20 17 16
4 35 19 16 .
5 37 19 19 15
ID Δ1 R1 Δ2 S2 R2 Δ3 S3 R3 LOCF
1 10 1 13 1 1 19 2 3 19
2 12 2 . . 2 . . 2 12
3 14 3 17 2 3 18 1 1 18
4 16 4 19 4 5 . . 5 19
5 18 5 18 3 4 22 3 4 22
N=5 subjects
T0 = baseline
N=2 missing final visit T3
Δ=Change R=Rank S=Temp Rank

LRCF: This study: CD4 Changes at Week 32
Method Alt’g w/ ddI + Zalcitabine + ddI + ddI + Nev All
Compl.
N=759
-8.8
-15.0 to 1.0
-4.0
-16.0 to 2.0
-2.5
-17.0 to 5.5
0.5
-9.0 to 17.0
-3.0
-15.0 to 5.0
LOCF
N=1031
-7.5
-15.0 to 1.0
-4.5
-15.0 to 2.0
-3.0
-15.0 to 5.0
0.5
-9.0 to 17.0
-3.0
-13.5 to 5.0
LRCF
N=1031
-10.0
-19.3 to 1.0
-5.0
-19.0 to 0.5
-5.5
-18.0 to 2.5
-0.25
-10.5 t 11.5
-4.0
-16.0 to 3.0
• All methods give same overall conclusions; p-values similar.
• Completer and LOCF tend to attenuate change estimates, relative to LRCF.
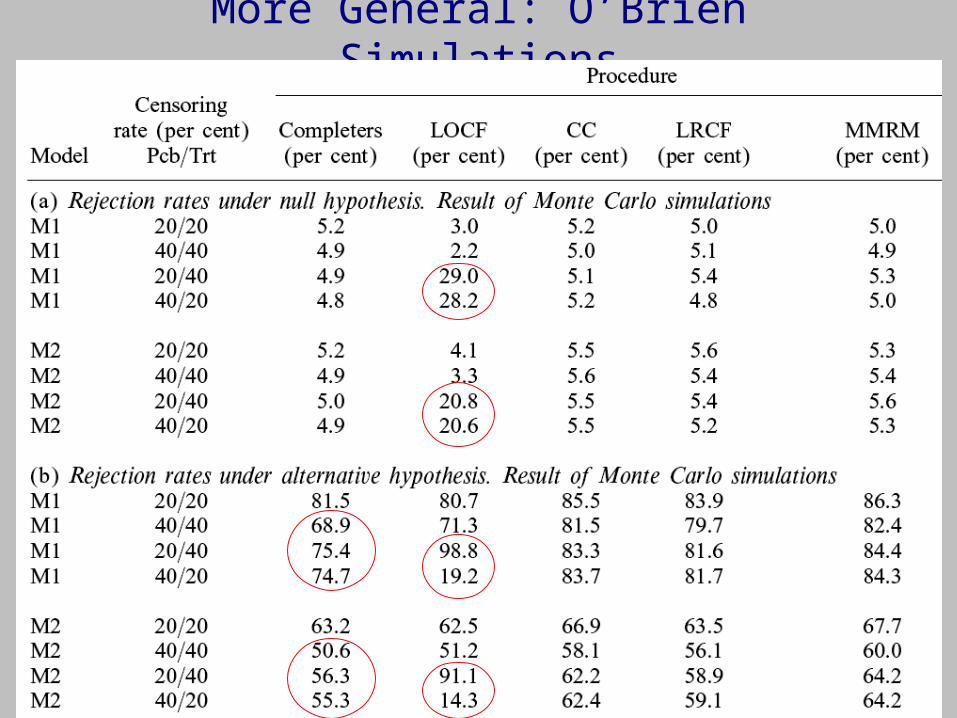
More General: O’Brien Simulations

Summary for LRCF Method
• More powerful than completer method and less biased than LOCF. Similar to cumulative change from last week.
• Use standard non-parametric tests (Wilcoxon, Kruskal -Wallis) on final visit ranks of changes.
• Identical to standard test (Wilcoxon, K-W) if no dropout.
• Developer O’Brien suggests use of %iles rather than ranks, if computational simplicity is desired.
• More intuitive than mixed model repeated measures (MMRM – see Case Studies 2004 Session 3).
• More potential for bias than MMRM if subjects choose to drop out.
• Same lack of bias as MMRM if administratively censored.

Self Quiz
For all questions, consider a study with 2 treatment groups that has scheduled visits at baseline and at study end. Primary outcome is change from baseline to study end, but not all subjects are measured at study end.
1. If a subject dropped out due to side effects, is he “administratively censored”? Why does it matter?
2. What additional information is necessary in order to use the method we discussed today?

Self Quiz
Now, suppose we also have intermediate visits with measurements for some subjects, for the remaining questions.
3. Criticize the use of only completing subjects in the analysis.
4. Criticize the use last-observation-carried-forward.
5. Criticize the use of imputation methods.
6. Criticize the use of mixed models.
7. Criticize the use of today’s method of extrapolating ranks.





























