Embed Size (px)
Citation preview

DOI: 10.1542/neo.11-4-e184 2010;11;e184-e193 NeoReviews
Maria Delivoria-Papadopoulos and Peter J. Marro Biochemical Basis of Hypoxic-Ischemic Encephalopathy
http://neoreviews.aappublications.org/cgi/content/full/neoreviews;11/4/e184located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Online ISSN: 1526-9906. Illinois, 60007. Copyright © 2010 by the American Academy of Pediatrics. All rights reserved. by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village,it has been published continuously since 2000. NeoReviews is owned, published, and trademarked NeoReviews is the official journal of the American Academy of Pediatrics. A monthly publication,
. Provided by USUHS LRC on July 18, 2010 http://neoreviews.aappublications.orgDownloaded from

Biochemical Basis of Hypoxic-IschemicEncephalopathyMaria Delivoria-
Papadopoulos, MD,*
Peter J. Marro, MD†
Author Disclosure
Drs Delivoria-
Papadopoulos and
Marro have disclosed
no financial
relationships relevant
to this article. This
commentary does not
contain a discussion
of an unapproved/
investigative use of a
commercial
product/device.
Objectives After completing this article, readers should be able to:
1. Describe the steps of posthypoxic brain injury.2. Explain the role of N-methyl-D-aspartate (NMDA) receptors in hypoxia.3. Delineate the contribution of free radicals to neuronal injury during hypoxia.4. Explain how hypoxia affects calcium influx and modification of apoptotic proteins.
AbstractDespite improved methods of intrapartum monitoring and advances in neonatal careand treatment, neonatal hypoxic-ischemic injury continues to produce significantmorbidity and mortality, often leading to long-term neurologic consequences. Hyp-oxia creates an imbalance in metabolic demand and cellular energy supply, resultingin the disruption of critical cellular functions and the activation of excitatory neuro-transmitters. In addition, the structure, function, and modification of cellular pro-cesses, such as the N-methyl-D-aspartate (NMDA) receptor and intracellular calciumregulation, are affected. Nuclear calcium signals control critical nuclear functions,including regulation of transcription factors and cell cycle, gene transcription, DNAreplication, and nuclear envelope breakdown. Nitric oxide synthase and the genera-tion of nitric oxide during hypoxia may contribute significantly to altered cellfunction, disruption in calcium homeostasis, and the activation of caspases, leading toprogrammed cell death. The biochemical mechanisms involved in hypoxic-ischemicneuronal injury and death are exceedingly complex and interdependent. This discus-sion focuses primarily on some of the major cellular and molecular mechanisms ofhypoxic neuronal injury in the newborn brain.
IntroductionPerinatal hypoxia-ischemia is the most common cause ofneurologic disease during the neonatal period. Hypoxic-ischemic encephalopathy (HIE) is associated with high mor-tality and morbidity rates, including cerebral palsy, intellec-tual disability, and seizures. The incidence of perinatalasphyxia is about 1.0% to 1.5% in most centers and usually isrelated to gestational age and birthweight. It occurs in 9.0%of infants younger than 36 weeks’ gestation and in 0.5% ofinfants older than 36 weeks’ gestation. (1) Perinatal HIEmay develop during the antepartum (20%), intrapartum(30%), antepartum and intrapartum (35%), or postpartum(10%) period. (2) HIE develops in the setting of perinatalasphyxia, which is a multiorgan system disease and includescircumstances affecting the cerebral blood flow in the fetusand newborn that compromise the supply of oxygen to thebrain. Assessment and management of these complications isan integral part of the treatment of perinatal asphyxia/HIE.(3)
A large amount of information has been collected on the
*Professor of Pediatrics and Physiology Emeritus, University of Pennsylvania School of Medicine, Philadelphia, Pa.†Division of Neonatology, Barbara Bush Children’s Hospital at Maine Medical Center, Portland, Me.
Abbreviations
Apaf-1: apoptotic protease activation factorATP: adenosine triphosphateCaM kinase: calcium/calmodulin kinaseCNS: central nervous systemCREB: cAMP response element bindingcyt c: cytochrome CHIE: hypoxic-ischemic encephalopathyICAD: inhibitor of caspase-activated DNaseIP3: inositol triphosphateNMDA: N-methyl-D-aspartateNNLA: Nw-nitro-l-argininenNOS: neuronal nitric oxide synthaseNO: nitric oxideNOS: nitric oxide synthasePARP: poly-ADP-ribose-polymerase
Article neurology
e184 NeoReviews Vol.11 No.4 April 2010. Provided by USUHS LRC on July 18, 2010 http://neoreviews.aappublications.orgDownloaded from

fetal cardiovascular and respiratory response to oxygenlimitations, giving rise to a better understanding andmanagement of neonatal deterioration induced by hyp-oxia. Besides these physiologic studies, cellular and bio-chemical mechanisms are being explored increasingly toinvestigate the complex and interrelated biochemicalalterations that result in hypoxic brain injury and braincell death in the fetus and newborn. (4)(5) It is importantto recognize the factors that may determine the sus-ceptibility of the developing brain to neonatal and peri-natal hypoxia. These determinants include the lipid com-position of the brain cell membrane, the rate of lipidperoxidation, the presence of antioxidant defenses, thedevelopment and modulation of the excitatory neuro-transmitter receptors such as the NMDA receptor, andthe intracellular calcium influx mechanisms. In additionto the developmental status of these cellular compo-nents, the response of the potential mechanisms to hyp-oxia determines the fate of the hypoxic brain cell in thedeveloping brain of the fetus and the newborn.
Steps of Posthypoxic Brain InjuryEnergy Breakdown
Under normal conditions, oxidative phosphorylationand the synthesis of high-energy phosphates such asadenosine triphosphate (ATP) requires adequate oxygensupply. Under anaerobic conditions, the metabolic costof ATP production is critically increased, leading to abreakdown of energy balance that depletes brain cells ofhigh-energy compounds necessary for energy-dependentmetabolic processes in neurons and glial cells.
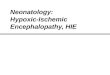
Excitotoxic Mechanisms (Fig. 1)The decrease in ATP concentrations leads to cell mem-brane depolarization and a disruption of voltage-dependent ion channels, which allows excessive amountsof calcium to enter the cytosol, initiating the release ofglutamate that activates NMDA receptors. The increasedexpression/activation of NMDA receptors further en-hances cellular calcium influx. The entire mechanism isaccelerated further by the dysfunction of the energy-dependent reuptake of glutamate both in neurons andin astrocytes in a vicious cycle. When calcium influx isunregulated, activation of phospholipases, proteases, andendonucleases can result in nuclear, organelle, and cellmembrane disruption.
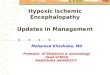
Cell Death (Fig. 2)Acute or long-term consequences of HIE are relatedeither to necrosis or to apoptosis of neuronal cells. Ne-crosis is characterized by passive cell swelling; rapid en-
ergy loss; generalized disruption of internal homeostasisleading to eventual lysis of the nucleus, organelles, andplasma cell membranes; and the release of intracellularcomponents that induce a local inflammatory response.The result is edema and injury to neighboring cells. Theinflammatory response triggers expression of the cyto-kines interleukin-1-beta and tumor necrosis factor-alpha,which stimulate release of oxygen free radicals fromneutrophils that activate microglial cells.
Necrosis is only one of the mechanisms of cell deathfollowing hypoxia or ischemia to the brain. Programmedcell death or apoptosis also appears to contribute to celldeath following hypoxia-ischemia, especially cell deaththat occurs days to weeks following the insult. (6)(7)Apoptosis is an active process that requires activation of agenetic program and specific endonucleolytic digestionof nuclear DNA. In contrast to necrosis, programmedcell death is characterized by cell shrinkage, coarse chro-
Figure 1. Effects of hypoxia leading to increased intranuclearcalcium. ATP�adenosine triphosphate, NMDA�N-methyl-D-aspartate
neurology hypoxic-ischemic encephalopathy
NeoReviews Vol.11 No.4 April 2010 e185. Provided by USUHS LRC on July 18, 2010 http://neoreviews.aappublications.orgDownloaded from

matin aggregation with extensive nuclear DNA fragmen-tation, nuclear pyknosis, and extrusion of membrane-bound cytoplasmic fragments or apoptotic bodies, but itis not associated with lysis of the plasma membrane.(8)(9) Studies in cell culture models have demonstratedthat hypoxia can trigger programmed cell death. (10)Programmed cell death, as assessed by the cleavage ofgenomic DNA, also has been shown to occur in the brainfollowing focal (6)(11)(12) and global ischemia. (7)(13)The mechanism by which hypoxia causes DNA fragmen-tation has been studied extensively but is not well under-stood.
NMDA ReceptorsGlutamate is the primary excitatory amino acid neuro-transmitter that contributes to a number of essentialdevelopmental processes such as synaptogenesis, synapticplasticity, long-term potentiation, learning, and memoryas well as neurodegeneration and hypoxia-induced in-jury. (14)(15) The physiologic and pathologic effects ofglutamate in the central nervous system (CNS) are me-
diated through its interaction with specific cell mem-brane receptors, of which the NMDA, kainate, andAMPA subtypes are the best characterized. (16)
The NMDA-type glutamate receptor is a predomi-nant mediator of excitotoxicity in the immature braincompared with the adult brain due to overexpression ofthe receptor in the developing immature CNS. (17)
Within the developmental period, NMDA receptor-mediated processes may depend not only on the ontog-eny of the NMDA receptor, but also potential modifica-tion by intracellular mechanisms.
Structure and Function of the NMDA ReceptorThe activity of the NMDA receptor-ion channel complexis regulated by a number of pharmacologically distinctbinding sites. The NMDA receptor possesses a neuro-transmitter binding site, or recognition site, that bindsglutamate or NMDA; a coactivator site that binds gly-cine; a channel site that binds MK-801; a voltage-dependent magnesium-binding site; a polyamine site; anifenprodil site; and an inhibitory divalent cation site thatbinds zinc. (17) Ligand binding studies indicate twodistinct binding sites or states associated with the gluta-mate recognition site, one that preferentially binds ago-nists and one that preferentially binds antagonists. (18)
The NMDA receptor is associated with a cation-selective ion channel that gates sodium, potassium, andcalcium ions. In the resting state, when blocked bymagnesium in a voltage-dependent manner, (19)(20)blockade of the ion channel complex by glutamate orNMDA is allowed, and agonist-dependent calcium in-flux occurs. The influx of calcium ions is believed toinitiate biochemical processes responsible for bothNMDA receptor-induced plasticity in the developingbrain and NMDA receptor-mediated excitotoxic celldeath. (15)(21)(22)
Each of the regulatory sites of the NMDA receptor-ion channel complex is modified during brain develop-ment, which may play a role in altering the response ofthe receptor during development and hypoxia.
Mechanism of NMDA Receptor ModificationDuring Hypoxia
Brain tissue hypoxia modifies the NMDA receptor rec-ognition, coactivator, and ion channel sites. A decrease inthe apparent number of NMDA receptors and an in-crease in receptor affinity for MK-801 were observed inhypoxic fetal guinea pig and newborn piglet brains.(23)(24) In these same studies, glutamate- and glycine-dependent activation of the NMDA receptor was de-creased and spermine-dependent and basal state receptor
Figure 2. Pathways of neuronal cell death following initialenergy failure. NMDA�N-methyl-D-aspartate. Reprintedwith permission from Marro PJ. The etiology and pharmaco-logic approach to hypoxic-ischemic encephalopathy in thenewborn. NeoReviews. 2002;3:e99.
neurology hypoxic-ischemic encephalopathy
e186 NeoReviews Vol.11 No.4 April 2010. Provided by USUHS LRC on July 18, 2010 http://neoreviews.aappublications.orgDownloaded from

activation were increased during hypoxia. Hypoxia-induced modification of the recognition, coactivator,and modulatory sites of the NMDA receptor-ion channelcomplex is likely through nitric oxide (NO)-mediatednitration. In neurons of the CNS, neuronal nitric oxidesynthase (nNOS) is colocalized with the NMDA recep-tor, (25)(26) thereby favoring nitration of the receptor.In addition, nNOS activity is decreased by phosphoryla-tion and increased by dephosphorylation, (27)(28) acondition likely present during hypoxia. Dephosphory-lation of the receptor also makes tyrosine sites availablefor nitration by peroxynitrite, which is produced by NOand superoxide radicals, both of which are producedduring hypoxia. Thus, dephosphorylation during hyp-oxia may facilitate peroxynitrite-mediated nitration oftyrosine-inhibiting phosphorylation of proteins and al-teration of the NMDA receptor-ion channel complex.(29)
In neurons of the CNS, nNOS is activated by calciuminflux through the NMDA receptor-ion channel, butnNOS is not efficiently stimulated by activation of non-NMDA receptors that also induce calcium influx. (30)The synaptic localization of nNOS in the brain may bemediated by the postsynaptic density protein PSD-95.Recently, it was demonstrated that nNOS, PSD-95, andNMDA receptor subunit NR2B from the brain coimmu-noprecipitate and that the PSD-95 is sufficient to assem-ble a tight tertiary complex with nNOS and the NR2Bsubunit of the NMDA receptor. (31)
In summary, results of these studies indicate that NOproduction in the brain is preferentially activated bycalcium influx through the NMDA receptor-ion channel,that there is a specific structural and functional linkbetween the NMDA receptor and nNOS, and that the
nitric oxide synthase (NOS) pathway plays a critical rolein the NO-mediated mechanism of hypoxia-inducedmodification of the NMDA receptor complex in thenewborn brain.
Free RadicalsFree radicals are molecular species that have unpairedelectrons in the outer orbit with a strong tendency toinitiate chain reactions that result in membrane peroxi-dation, protein oxidation, nucleic acid oxidation, and celldamage. Normally, more than 80% of the oxygen con-sumed by the cell is reduced completely by cytochromeoxidase to water without production of oxygen freeradicals. The remaining 10% to 20% undergoes otheroxidation reduction reactions in the cytoplasm and mi-tochondria that produce a superoxide anion radical.
Mechanisms of Free Radical Generation DuringHypoxia
There are a number of potential mechanisms of freeradical generation under hypoxic conditions. Duringhypoxia, the increased accumulation of intracellular cal-cium resulting from excessive activation of NMDA (32)and non-NMDA receptors is crucial in hypoxia-inducedexcitotoxicity. Increased intracellular calcium can initiatea number of biochemical events that could lead to freeradical generation and cell death (Table 1).
In addition to calcium mediation, other potentialmechanisms of free radical generation during hypoxiainclude: 1) reduction of electron transport chain com-ponents, including ubiquinone (a component that un-dergoes auto-oxidation to produce free radicals); 2) in-creased release of ferritin under the conditions ofdecreased cellular high-energy compounds; and 3) in-
Table 1. Deleterious Effects of Increased Intracellular CalciumAction Result
Activates phospholipases ● Phospholipid hydrolysis and cell membrane injury● Generation of free radicals
Activates proteases ● Cytoskeletal disruption of microtubules● Proteolysis of other cellular proteins
Activates nucleases ● Nuclear injuryActivates calcium-ATPase ● Further increase in cytosolic and nuclear calcium
● Consumes ATP at time of energy depletionEnters mitochondrion and uncouples oxidative phosphorylation ● Decreased ATP productionIncreases neurotransmitter release ● Activation of glutamate receptors and calcium influxActivates protein that transforms xanthine dehydrogenase
to xanthine oxide● Free radical formation
Activates nitric oxide synthase ● Generation of nitric oxide
ATP�adenosine triphosphate
neurology hypoxic-ischemic encephalopathy
NeoReviews Vol.11 No.4 April 2010 e187. Provided by USUHS LRC on July 18, 2010 http://neoreviews.aappublications.orgDownloaded from

creased degradation of ATP during hypoxia, increasingthe substrate for the xanthine oxidase reaction and lead-ing to increased free radical generation.
Increased free radical generation during hypoxia inthe cerebral cortex of newborn piglets has been docu-mented directly through spin trapping of free radicalsand measuring the resulting spin adduct signal withelectron spin resonance spectroscopy. The characteristicsof the spin adduct signal identify the free radical speciespresent in the hypoxic tissue as predominantly an alkoxylradical, indicating that free radical-mediated lipid peroxi-dation is an ongoing event during cerebral hypoxia, amechanism of hypoxic neuronal injury. These studies notonly demonstrate increased free radical generation dur-ing hypoxia in the cerebral cortex of the fetus and thenewborn but reduced hypoxia-induced production offree radical species due to inhibitors of pathways of freeradical generation.
Nitric Oxide Free Radicals and Neuronal InjuryThree major isoforms of NOS have been identified:constitutive neuronal, constitutive endothelial, and in-ducible macrophage isoforms. Following ischemia, NOproduced from neuronal NOS has toxic effects, but NOproduced from endothelial NOS has protective effects inthe brain. (33) Hypoxic brain injury is associated withthe formation of NO. (34)(35) Although NO physiolog-ically mediates cerebral vasodilation under normal con-ditions, (36) recent studies suggest that NO, a gaseousfree radical, may react with superoxide anion to formperoxynitrite and cause neurotoxicity. (37)(38)(39)
NO is reported to cause neuronal damage throughvarious mechanisms. Studies using the NOS inhibitorNw-nitro-l-arginine (NNLA) demonstrated that freeradicals, corresponding to alkoxyl radicals, were inducedby hypoxia but were inhibited by pretreatment withNNLA. NNLA also inhibited hypoxia-induced genera-tion of conjugated dienes (products of lipid peroxida-tion) and preserved Na�, K�-ATPase activity (an indexof cellular membrane function). These data demon-strated that NOS generates free radicals during hypoxiavia peroxynitrite production, presumably causing lipidperoxidation and membrane dysfunction. The produc-tion of secondarily formed lipid free radicals providesstrong evidence of peroxidative injury. This is particularlytrue for alkoxyl radicals, which are generated from lipidperoxide by either iron or copper ions and can abstracthydrogen atoms from polyunsaturated fatty acids, lead-ing to further lipid peroxidation. This suggests that NOhas an in vivo role in the generation of alkoxyl radicals,leading to free radical-mediated lipid peroxidation.
The exact molecular mechanism of hypoxic mem-brane damage is not clear. However, it has been shownthat peroxynitrite (formed by the reaction between su-peroxide anions and NO) can cause lipid peroxidation invitro. (40) Therefore, high concentrations of NO duringhypoxia may result in increased production of peroxyni-trite, causing lipid peroxidation.
Neuronal Nuclear Calcium InfluxA number of critical nuclear functions, including regula-tion of transcription factors, cell cycle regulation tran-scription, DNA replication, and nuclear envelope break-down, are controlled by intracellular calcium (Table 2).(41) Furthermore, nuclear calcium signals potentiallycontrol a number of events leading to hypoxia-inducedprogrammed cell death. Nuclear and cytosolic calciumsignals are regulated differently, and the extranuclearcalcium concentration determines the mode of calciumentry into the nucleus. Increased intracellular calciumhas been shown to be a primary mediator of activity-dependent gene transcription under a number of exper-imental conditions. (42)(43)(44) Several factors may beinvolved in calcium-regulated gene expression and tran-scription, including the site of calcium entry, the ampli-tude and the spatial properties of the calcium signals, andthe duration of the calcium signal. (45)(46)
Studies have shown that cerebral hypoxia results inincreased nuclear calcium influx in neuronal nuclei of thecerebral cortex of newborn guinea pigs. (47) The nuclearcalcium influx increased as a function of increased cere-bral tissue hypoxia. Cerebral hypoxia resulted in in-creased calcium/calmodulin kinase (CaM kinase) IV ac-tivity, cAMP response element binding (CREB) proteinphosphorylation, activity of high-affinity Ca��-ATPase,and inositol triphosphate (IP3)-dependent calcium in-flux in neuronal nuclei of newborn piglets. In addition,NO donors increased neuronal nuclear calcium influx,(42) and hypoxia resulted in generation of NO freeradicals and increased high-affinity Ca��-ATPase activ-ity.
During hypoxia, NO-mediated modification of the
Table 2. Role of Calcium Insidethe Nucleus● Transcription of genes● Regulation of the cell cycle● Replication of DNA● Breakdown of the nuclear envelope
neurology hypoxic-ischemic encephalopathy
e188 NeoReviews Vol.11 No.4 April 2010. Provided by USUHS LRC on July 18, 2010 http://neoreviews.aappublications.orgDownloaded from

nuclear membrane high-affinity Ca��-ATPase and IP3receptor is a potential mechanism of increased intranu-clear calcium that leads to activation of calcium-dependent nuclear mechanisms and activates cascades ofhypoxic programmed cell death.
Expression and PosttranslationalModification of Apoptotic Proteins
The Bcl-2 ProteinsThe Bcl-2 family of proteins (including Bax and Bcl-2) control cell proliferation, differentiation, and pro-grammed cell death during normal brain development.(48)(49) Bax and Bcl-2 are inducible genes found in thedeveloping and adult central and peripheral nervoussystems. (50)(51) The antiapoptotic protein Bcl-2 pre-vents apoptosis by forming a heterodimer with the pro-apoptotic protein Bax and protects cells from pro-grammed cell death following hypoxia. (48)(49)
Cerebral hypoxia results in increased expression ofBax protein in neuronal nuclei of the cerebral cortex ofnewborn piglets. (52) Increased Bax protein in the mi-tochondrial, cytosolic, and neuronal nuclear fractionsindicates increased expression of the protein rather thanits translocation from mitochondria to cytosol duringhypoxia. The expression of antiapoptotic protein Bcl-2did not increase during hypoxia. Therefore, the ratio ofproapoptotic protein Bax to antiapoptotic protein Bcl-2increases in all compartments of the cell during hypoxia,which may lead to activation of the hypoxia-inducedcascade of neuronal death. NOS inhibition prevented thehypoxia-induced increased expression of proapoptoticprotein Bax, indicating that the hypoxia-induced in-creased expression of Bax is mediated by NO. (53)
Caspases-3, -8, and -9Caspases are a unique family of cysteinyl-aspartate pro-teases that play an important role in the initiation andexecution of apoptosis. (54) They are divided into twoprimary classes: Class I caspases have long prodomainand Class II caspases have short prodomain.
Class I caspases such as 8, 9, and 10 can autocatalyzetheir own activation and are activated in the early phaseof apoptosis. These are termed the initiator caspases.Class II caspases, such as 3, 6, and 7, require cleavageby another protease and are responsible for the break-down of cells. These are termed the effector or theexecutioner caspases. Upstream caspase activation dur-ing apoptosis leads to the activation of downstreamcaspases in a self-amplifying cascade.
Two pathways of caspase activation have been inves-tigated: the cell surface death receptor-mediated path-
way and the mitochondria-initiated pathway. The re-cruitment and cleavage of procaspase-8 to produce theactive form of caspase-8 is a critical biochemical event inthe death receptor-mediated apoptosis. Following itsactivation, caspase-8 can activate downstream caspasesby direct cleavage or by indirectly cleaving the proapop-totic protein and inducing cytochrome c (cyt c) releasefrom the mitochondria. In the mitochondria-initiatedpathway, caspase activation is triggered by formationof an oligomeric apoptotic protease activation factor(Apaf-1)/cyt c complex. The resulting complex formedby the combination of Apaf-1, cyt c, Bax/Bcl-2, andprocaspase-9 is referred to as the apoptosome, whichleads to recruiting and activating procaspase-9, an up-stream caspase. Other, less-defined pathways of apopto-tic caspase activation that also are active in neurons actpredominantly through the caspases-8 or -9. Followinghypoxia in the cerebral cortex of newborn piglets, there isan increase in protein expression and activity of caspase-8 and caspase-9 (initiator caspases) as well as the expres-sion and activity of caspase-3 (executioner caspase).
Nuclear Calcium Influx and Caspase-9 andCaspase-3 Activation
Increased activity of casapse-9 and caspase-3 duringhypoxia is mediated by nuclear calcium influx. Studiesinvestigating the role of nuclear calcium influx in caspaseactivation during hypoxia were performed in newbornpiglets. (55)(56) The calcium-ATPase inhibitor (cloni-dine) was administered to block nuclear calcium influx.Cerebral tissue hypoxia resulted in increased caspase-9activity, and pretreatment with clonidine prevented thishypoxia-induced increase in caspase-9 activity. In addi-tion, hypoxia resulted in increased caspase-3 activity, aconsequence of caspase-9 activation, and pretreatmentwith clonidine prevented this increase in caspase-3 activ-ity. These results demonstrate that hypoxia-induced in-crease in caspase-3 activity is mediated by nuclear calciuminflux.
NO and Caspase-9 and Caspase-3 ActivationTo delineate caspase activation during hypoxia further,the role of NO derived from neuronal NOS was studiedin newborn piglets, using a relatively selective inhibitorof nNOS, 7-NINA salt. (44) Following cerebral tissuehypoxia, an increase in caspase-9 activity was seen, butpretreatment with the nNOS inhibitor prevented thehypoxia-induced increase in caspase-9 activity. Cerebraltissue hypoxia again resulted in increased caspase-3 activ-ity, a consequence of caspase-9 activation, and pre-treatment with the nNOS inhibitor prevented this
neurology hypoxic-ischemic encephalopathy
NeoReviews Vol.11 No.4 April 2010 e189. Provided by USUHS LRC on July 18, 2010 http://neoreviews.aappublications.orgDownloaded from

hypoxia-induced increase in caspase-3 activity. Theseresults demonstrate that the hypoxia-induced increase incaspase-9 is mediated by nNOS-derived NO.
Caspase-9 can be activated during hypoxia by multi-ple mechanisms that are dependent on generation ofnNOS-derived NO and neuronal nuclear calcium influx.NO increases calcium influx in synaptosomes as well asneuronal nuclei. By increasing nuclear calcium influx,NO can increase expression of caspase-9 as well as pro-apoptotic proteins. NO-mediated protein modificationalso may alter its activation. Caspase-9 plays a significantrole in the hypoxia-induced programmed cell death inthe newborn brain, and caspase activation during hyp-oxia in the newborn brain is mediated by bothtranscription-dependent and -independent mechanisms.(57)
DNA FragmentationIt has been proposed that the cleavage of DNA at itsintranucleosomal linkage region is produced by specificendonucleases that are dependent on calcium. (58)(59)Caspase-3, acting as cysteine protease, cleaves and inac-tivates nuclear enzymes, including poly-ADP-ribose-polymerase (PARP), a DNA repair enzyme, and inhibitorof caspase-activated DNase (ICAD). The caspase-activated DNase then enters the nucleus and cleavesgenomic chromosomal DNA. (60)(61) This nucleargenomic DNA fragmentation correlates exponentiallywith the degree of cerebral tissue hypoxia in newbornpiglets (62) and is characteristic of cellular apoptosis.
Temporal Biochemical ChangesThe steps of posthypoxic neuronal injury evolve withinhours (the necrotic process) and days (the apoptoticprocess). Temporal biochemical changes and associatednuclear fragmentation have been assessed in the cerebralcortex of newborn guinea pigs following hypoxia. Initialcellular injury may be followed by a failure of cellularrepair mechanisms, leading to further delayed brain in-jury. Neuronal nuclear calcium influx increases immedi-ately following hypoxia and remains elevated through7 days of age. Similarly, nuclear Bax protein expressionincreases immediately following hypoxia and remainselevated through 7 days, but Bcl-2 protein remains sim-ilar to control during hypoxia. These biphasic temporalchanges may reflect not only the primary hypoxic insultbut also a secondary cellular damage due to recurrent(continuing) free radical release during the reperfusion–reoxygenation phase.
Clinical ImplicationsUnderstanding the very complex and interrelated mech-anisms of cell death after a hypoxic-ischemic result mayserve as background for critical care of the newborn.Hypoxia at the cellular level results from failure in oxygentransport from the lung alveolar space to the mitochon-dria. To prevent neuronal cell death, any insufficiency orfailure in the respiratory and circulatory systems must berestored in a matter of minutes. Among the hazards inrestoring oxygen supply is medically induced hyperoxia(high FiO2), which may worsen the neuronal insult byproducing additional oxygen free radicals. An under-standing of the temporal evolution of the posthypoxicbiochemical disturbances during and following hypoxic-ischemic insult may offer the opportunity for pharmaco-logic interventions at key steps of the biochemical events.
References1. Hill A, Volpe J. Hypoxic-ischemic cerebral injury in the new-born. In: Swaiman KF, Ashwal S, eds. Pediatric Neurology: Princi-ples and Practice. St. Louis, Mo: Mosby; 1999:191–2042. Raichle ME. The pathophysiology of brain ischemia. Ann Neu-rol. 1983;13:2–103. Piazza AJ. Postasphyxial management of the newborn. ClinPerinatol. 1983;26:749–7654. Vannucci RC. Experimental biology of cerebral hypoxia-isch-emia: relation to perinatal brain damage. Pediatr Res. 1990;27:317–3265. Legido A, Katsetos CD, Mishra OP, et al. Perinatal hypoxia-ischemia encephalopathy: current and future treatments. Int Pedi-atr. 2001;15:143–1516. Linnik MD, Zobirst RH, Hatfield MD. Evidence supporting arole for programmed cell death in focal cerebral ischemia in rats.Strokes. 1993;24:2002–20087. Ferrer I, Tortosa A, Macaya A, et al. Evidence of nuclear DNAfragmentation following hypoxia-ischemia in the infant rat brain,and transient forebrain ischemia in the adult gerbil. Brain Pathol.1994;4:115–1228. Wylie AH, Kerr JFR, Currie AR. Cell death, the significance ofapoptosis. Int Rev Cytol. 1980;68:251–3069. Columbano A. Cell death: current difficulties in discriminatingapoptosis and necrosis in the context of pathological processes invivo. J Cell Biochem. 1995;58:181–19010. Rosenbaum DM, Michaelson M, Batter DK, et al. Evidence forhypoxia induced programmed cell death of cultured neurons. AnnNeurol. 1994;25:19–33
American Board of Pediatrics Neonatal-PerinatalMedicine Content Specification• Know the incidence, causes and
pathophysiology, including cellularabnormalities, of acute perinatal asphyxia.
neurology hypoxic-ischemic encephalopathy
e190 NeoReviews Vol.11 No.4 April 2010. Provided by USUHS LRC on July 18, 2010 http://neoreviews.aappublications.orgDownloaded from

11. Dragunow M, Beiharz E, Sirimanne E, etal. Immediately earlygene protein expression in neurons undergoing delayed death, butnot necrosis following hypoxic-ischemic injury to the young ratbrain. Brain Res Mol Brain Res. 1994;25:193312. Gillardon F, Lenz C, Waschle KF. Altered expression of Bcl-2,Bcl-X, Bax and c-Fos colocalizes with DNA fragmentation andischemic cell damage following middle cerebral artery occlusion inrats. Brain Res Mol Brain Res. 1996;40:254–26013. Nitatori T, Sato N, Waguri S, et al. Delayed neuronal death inthe CA1 pyramidal layer of the gerbil hippocampus followingtransient ischemia in apoptsis. J Neurosci. 1995;15:1001–101114. Choi DW. Cerebral hypoxia: some new approaches and unan-swered questions. J Neurosci. 1990;10:2493–250115. Rothman SM, Olney JW. Glutamate and the pathophysiologyof hypoxic-ischemic brain damage. Anne Neurol. 1986;19:105–11116. Monaghan DT, Bridges RJ, Cotman CW. The excitatoryamino acid receptors: their classes, pharmacology, and distinctproperties in the function of the central nervous system. Annu RevPharmacol Toxicol. 1989;29:365–40217. Johnston MV. Neurotransmitters and vulnerability of the de-veloping brain. Brain Dev. 1995;17:301–30618. Monaghan DT, Olvenman HJ, Nguyen L, et al. Two classes ofN-methyl-D-aspartate recognition sites: differential distributionand differential regulation by glycine. Proc Natl Acad Sci USA.1988;85:9836–984019. Nowak L, Bregetovski P, Ascher P, et al. Magnesium gatesglutamate-activated channels in mouse central neurons. Nature.1984;307:462–46520. Mayer ML, Westbrook GL, Guthrie PB. Voltage-dependentblock by Mg�� of NMDA responses in spinal cord neurons. Na-ture. 1984;309:261–26321. Collingridge G. Synaptic plasticity. The role of NMDA recep-tors in learning and memory. Nature. 1987;330:604–60522. Tang YP, Shimizu E, Dube GR, et al. Genetic enhancement oflearning and memory in mice. Nature. 1999;401:63–6923. Mishra OP, Delivoria-Papadopoulos M. NMDA receptormodification of the fetal guinea pig brain during hypoxia. Neuro-chem Res. 1992;17:1211–121624. Hoffman DJ, DiGiacomo JE, Marro PJ, et al. Hypoxia-induced modification of the N-methyl-D-aspartate (NMDA) recep-tor in the brain of newborn piglets. Neurosci Lett. 1994;167:156–16025. Bhat GK, Mahesh VB, Lamar CA, et al. Histochemical local-ization of nitric oxide neurons in the hypothalamus: associationwith gonadotropin-releasing hormone neurons and co-localizationwith N-methyl-D-aspartate receptors. Neuroendocrinol Lett. 1997;62:187–19726. Aoki C, Rhee J, Lubin, M, et al. NMDA-R1 subunit of thecerebral cortex co-localizes with neuronal nitric oxide synthase atpre and postsynaptic sites and in spines. Brain Res. 1997;750:25–4027. Bredt DS, Ferris CD, Snyder SH. Nitric oxide synthase regu-latory sites. Phosphorylation by cyclic AMP-dependent proteinkinase, protein kinase C, and calcium/calmodulin protein kinase,identification of flavin and calmodulin sites. J Biol Chem. 1992;267:10976–1098128. Dawson TM, Steiner JP, Dawson VL, et al. Immunosuppres-sant FK506 enhances phosphorylation of nitric oxide synthase andprotects against glutamate neurotoxicity. Proc Natl Acad Sci USA.1993;90:9808–981229. Gow AJ, Duran D, Malcom S, et al. Effect of peroxynitrite-
induced protein modification on tyrosine phosphorylation and deg-radation. FEBS Lett. 1996;385:63–6630. Kiedrowski I, Costa E, Wroblewski JT. Glutamate receptoragonist stimulate nitric oxide synthase in primary cultures of cere-bellar granule cells. J Neuroch. 1992;58:335–34131. Christopherson KS, Hillier BJ, Lim WAS, et al. PSD-95 assem-bles a ternary complex with the N-methyl-D-aspartic acid receptorand bivalent neuronal NO synthase PDX domain. J Biol Chem.1999;274:27467–2747332. Zanelli SA. NMDA receptor-mediated calcium influx in cere-bral cortical synaptosomes of the hypoxic guinea pig fetus. Neuro-chem Res. 1999;24:434–44633. Huang Z. Effects of cerebral ischemia in mice deficient inneuronal nitric oxide. Science. 1994;265:1883–188534. Beckman JS. The double-edged role of nitric oxide in brainfunction and superoxide-mediated injury. J Dev Physiol. 1991;15:53–5935. Cazevielle C. Superoxide and nitric oxide cooperation inhypoxia/reoxygenation-induced neuron injury. Free Radic BiolMed. 1993;14:359–39536. Faraci FM. Role of endothelium-derived relaxing factor incerebral circulation: large arteries vs. microcirculation. Am J Physiol.1991;261:H1038–H104237. Beckman JS. Apparent hydroxyl radical production by per-oxynitrite: implications for endothelial injury from nitric oxide andsuperoxide. Proc Natl Acad Sci USA. 1990;87:1620–162438. Dawson VL. Nitric oxide mediates glutamate neurotoxicity inprimary cortical cultures. Proc Natl Acad Sci USA. 1991;88:6368–637139. Hamada Y. Inhibitors of nitric oxide synthesis reduce hypoxic-ischemic brain damage in the neonatal rat. Pediatr Res. 1994;35:10–1440. Radi R. Peroxynitrite-induced membrane lipid peroxidation:the cytotoxic potential of superoxide and nitric oxide. Arch BiochemBiophys. 1991;288:481–48741. Delivoria-Papadopoulos M, Akhter W, Mishra OP. Hypoxia-induced Ca�� -influx in cerebral cortical neuronal nuclei of new-born piglets. Neurosci Lett. 2003;342:11942. Ghosh A, Greenberg ME. Calcium signaling in neurons: mo-lecular and cellular consequences. Science. 1995;268:239–24743. Hardigham GE, Bading H. Nuclear calcium: a key regulator ofgene expression. Biometals. 1998;11:34544. Chawla S, Bading H. CREB/CBP and SRE-interacting tran-scriptional regulators are fast on-off switches: duration of calciumtransients specifies the magnitude of transcriptional responses.J Neurochem. 2001;79:849–85845. Handigham GE, Chawla S, Cruzaleguie S, et al. Control ofrecruitment and transcription-activating function of CBP deter-mines gene regulation by NMDA receptors and L-type calciumchannels. Neuron. 1999;22:78946. Dometsch RE, Pajvani U, Fife R, et al. Signaling to the nucleusby an L-type calcium channel-calmodulin complex through theMAP kinase pathway. Science. 2001;294:33347. Mishra OP, Delivoria-Papadopoulos M. Hypoxia-inducedgeneration of nitric oxide free radicals in the cerebral cortex ofnewborn guinea pigs. Neurochem Res. 2000;25:155948. Farlie PG, Dringen R, Rees SM, et al. Bcl-2 transgene expres-sion can protect neurons against developmental and induced celldeath. Proc Natl Acad Sci USA. 1995;92:439749. Oltavi ZN, Milliman CM, Korsmeyer SJ. Bcl-2 heterodimer-
neurology hypoxic-ischemic encephalopathy
NeoReviews Vol.11 No.4 April 2010 e191. Provided by USUHS LRC on July 18, 2010 http://neoreviews.aappublications.orgDownloaded from

izes in vivo with a conserved homolog, Bax, that accelerates pro-grammed cell death. Cell. 1993;74:60950. Merry DE, Veis DJ, Hickey WF, et al. Bcl-2 protein expressionis widespread in the developing nervous system and retained in theadult PNS. Development. 1994;120:30151. Reed JC. Mechanisms of Bcl-2 family protein function anddysfunction in health and disease. Behring Inst Mitt. 1996;97:7252. Ravishankar S, Ashraf QM, Mishra OP, et al. Expression of Baxand Bcl-2 proteins during hypoxia in the cerebral cortical neuronalnuclei of newborn piglets: effect of administration of magnesiumsulfate. Brain Res. 2001;901:2353. Zanelli SA, Ashraf QM, Mishra OP. Nitration is a mechanismof regulation of the NMDA receptor function during hypoxia.Neurosci. 2002;11286954. Nicholson DW, Thornberry NA. Caspase killer proteases.Trends Biochem Sci. 1997;22:299–30655. Delivoria-Papadopoulos M, Ashraf QM, Mishra OP. Effect ofhypoxia on expression of apoptotic proteins in nuclear, mitochon-drial and cytosolic fractions of the cerebral cortex of newbornpiglets: the role of nuclear Ca�� -influx. Neurochem Res. 2008;33:1196–120456. Hornick K, Chang E, Zubrow AB, Mishra OP, Delivoria-Papadopoulos M. Mechanism of Ca(2�)/calmodulin-dependent
protein kinase IV activation and of cyclic AMP response elementbinding protein phosphorylation during hypoxia in the cerebralcortex of newborn piglets. Brain Res. 2007;1150:40–4557. Mishra OP, Delivoria-Papadopoulos M. Effect of neuronalnitric oxide synthase inhibition on caspase-9 activity during hypoxiain the cerebral cortex of newborn piglets. Neurosci Lett. 2006;401:81–8558. Cohen JJ, Duke RC. Glucocorticoid activation of a calcium-dependent endonuclease in thymocyte nuclei leads to cell death.J Immunol. 1984;32:38–4259. Ishida R, Akiyoshi H, Takahashi T. Isolation and purificationof calcium and magnesium dependent endonuclease from rat livernuclei. Biochem Biophys Res Commun. 1974;56:703–71060. Hameed A, Olsen KJ, Lee MK, et al. Cytolysis by Ca-permeable transmembrane channels: pore formation causes exten-sive DNA degradation and cell lysis. J Exp Med. 1989;169:765–77761. Tominaga T, Kagure S, Narisawa K, et al. Endonuclease acti-vation following focal ischemic injury in the rat brain. Brain Res.1993;608:21–2662. Waseem W, Ashraf QM, Zanelli SA, et al. Effect of gradedhypoxia on cerebral cortical genomic DNA fragmentation in new-born piglet. Biol Neonate. 2001;79:187–193
neurology hypoxic-ischemic encephalopathy
e192 NeoReviews Vol.11 No.4 April 2010. Provided by USUHS LRC on July 18, 2010 http://neoreviews.aappublications.orgDownloaded from

NeoReviews Quiz
1. Under anaerobic conditions, the production of high-energy phosphates decreases, which leads to cellmembrane depolarization and intracellular calcium influx. Increased intracellular calcium has severaldeleterious effects on cell structure and function. Of the following, cytoskeletal disruption of microtubulesis most likely the result of calcium-mediated activation of:
A. Nitric oxide synthase.B. Nuclease.C. Phospholipase.D. Protease.E. Xanthine oxidase.
2. The two mechanisms of cell death following hypoxia-ischemia of the brain are necrosis and apoptosis.Whereas necrosis is more immediate in onset after the hypoxic-ischemic injury, apoptosis occurs days toweeks following the insult. Of the following, the most distinguishing feature of apoptosis is:
A. Cell swelling.B. Chromatin aggregation.C. Local cytokine release.D. Oxygen free radical formation.E. Plasma membrane lysis.
3. N-methyl-D-aspartate (NMDA) cell membrane receptor is a predominant mediator of excitotoxicity in theimmature developing brain. This receptor has a number of pharmacologically distinct binding sites. Of thefollowing, the coactivator site of the NMDA receptor is most likely to bind to:
A. Glutamine.B. Glycine.C. Magnesium.D. Mk-801.E. Zinc.
4. Caspases are a family of cysteinyl-aspartate proteases that play an important role in the initiation andexecution of apoptosis. Caspases are of two classes: class I caspases initiate apoptosis and class II caspasesexecute apoptosis. Caspase activation occurs through two pathways: the cell surface death receptor-mediated pathway and mitochondria-initiated pathway. Of the following, the critical caspase in cell surfacedeath receptor-mediated apoptosis is:
A. Caspase-3.B. Caspase-6.C. Caspase-7.D. Caspase-8.E. Caspase-10.
neurology hypoxic-ischemic encephalopathy
NeoReviews Vol.11 No.4 April 2010 e193. Provided by USUHS LRC on July 18, 2010 http://neoreviews.aappublications.orgDownloaded from

DOI: 10.1542/neo.11-4-e184 2010;11;e184-e193 NeoReviews
Maria Delivoria-Papadopoulos and Peter J. Marro Biochemical Basis of Hypoxic-Ischemic Encephalopathy
& ServicesUpdated Information
s;11/4/e184http://neoreviews.aappublications.org/cgi/content/full/neoreviewincluding high-resolution figures, can be found at:
Permissions & Licensing
http://neoreviews.aappublications.org/misc/Permissions.shtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://neoreviews.aappublications.org/misc/reprints.shtml
Information about ordering reprints can be found online:
. Provided by USUHS LRC on July 18, 2010 http://neoreviews.aappublications.orgDownloaded from