Embed Size (px)
Citation preview

BILLING, REIMBURSEMENT, AND COLLECTIONS
Chapter 9

Chapter 9 2
Billing, Reimbursement,and Collections Learning Objectives
Compute charges for medical services and create patient statements based on the patient encounter form and the physician's fee schedule.
Explain the process of completing and transmitting insurance claims.
Discuss the advantages of using electronic claims. Describe the different types of billing options
used by medical practices for billing patients. Discuss the procedures and options available for
collecting delinquent accounts.

Chapter 9 3
Key Terms Clearinghouse CMS-1500 claim form Collection agency Collection at the time
of service Cycle billing Dependent Electronic claims EOB ERA
Fee adjustment Fee schedule Guarantor Monthly billing Patient information
form Patient statement Terminated account Third-party liability Write-off

Chapter 9 4
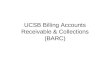
Patient Encounter Form Facilitates billing process Used to record details of each patient
encounter for billing and insurance Includes
Patient information Date Diagnosis for current visit Procedure information Financial information

Chapter 9 5
Patient Encounter Form (cont’d)
Usually preprinted with common diagnoses/procedures
New form attached to medical record for each visit
Physician fills in form as visit/procedures progress
Form is returned to administrative medical assistant for use in billing
AN
Y M
ED
ICA
L P
RA
CT
ICE
12
3 A
ny
Str
ee
t
An
yto
wn,
US
A
61
0-5
55
-12
12
Pa
tie
nt
Na
me
__
__
__
__
__
__
__
__
__
__
__
__
__
_D
OB
__
__
__
__
__
__
__
Da
te o
f S
er
vic
e _
__
__
__
__
__
__
__
__
__
_ L
ast
DO
S _
__
__
__
__
__
__
__
__
_
Tr
ea
tin
g P
hy
sic
ian
__
__
__
__
__
__
__
__
__
__
__
__
__
__
__
__
__
Re
fer
rin
g P
hy
sic
ian
__
__
__
__
__
__
__
__
__
__
__
__
__
__
__
__
_
De
scri
pti
on
De
scri
pti
on
Ne
w P
ati
en
tFE
E
Le
ve
l 1
/Fo
cu
sed
99
20
1_
__
_ G
00
01
La
b H
an
dli
ng
Fe
e –
Me
d.__
__
Le
ve
l 2
/Ex
pa
nd
ed
99
20
2_
__
_3
64
15
La
b H
an
dli
ng
Fe
e_
__
_
Le
ve
l 3
/De
tail
ed
99
20
3_
__
_8
50
22
CB
C w
/d
iff_
__
_
Le
ve
l 4
/Co
mp
.99
20
4_
__
_8
70
7C
&S
__
__
Le
ve
l 5
/Hig
h9
92
05__
__
80
54
CM
P_
__
_
82
46
5C
ho
lest
ero
l
Z
82
46
__
__
Est
ab
lish
ed P
ati
en
t87
08
6C
olo
ny
Co
un
t__
__
Le
ve
l 1
/Min
ima
l99
21
1_
__
_82
56
5C
rea
tin
ine
__
__
Le
ve
l 2
/Fo
cu
sed
99
21
2_
__
_80
16
2D
igo
xin__
__
Le
ve
l 3
/Ex
pa
nd
ed
99
21
3_
__
_9
30
00
EK
G-1
2 l
ea
d
W
93
10
__
__
Le
ve
l 4
/De
tail
ed
99
21
4_
__
_45
33
0F
ibe
rsig
mo
ido
sco
py
__
__
Le
ve
l 5
/Co
mp
.99
21
5_
__
_4
53
31
Fib
ers
igm
oid
osc
op
y w
/bx.
__
__
Po
st-o
p Vis
it9
90
24__
__G
01
04
Fib
ers
igm
oid
– C
A s
cre
en
__
__
82
94
7G
luc
ose__
__
Co
nsu
lta
tio
n8
83
04
Gro
ss &
Mic
ro_
__
_
Ne
w o
r Est
ab
lish
ed
83
03
6H
gb
A1
C_
__
_
Le
ve
l 1
/Fo
cu
sed
99
24
1_
__
_85
01
8H
gb
Z
85
58
__
__
Le
ve
l 2
/Ex
pa
nd
ed
99
24
2_
__
_8
37
18
HD
B C
ho
lest
ero
l__
__
Le
ve
l 3
/De
tail
ed
99
24
3_
__
_93
22
4H
olt
er
. E
KG
24
hr
am
b.__
__
Le
ve
l 4
/Co
mp
.99
24
4_
__
_9
32
27
Ho
lte
r –
Dr.
re
vie
w_
__
_
Le
ve
l 5
/Hig
h9
92
45__
__
87
21
0K
OH
/We
t P
rep
__
__

Chapter 9 6
Fee Schedule Lists the usual procedures
performed in the office and corresponding charges There may be more than one fee schedule,
depending on insurance plan participation Administrative medical assistant
must be familiar with office policy regarding financial arrangements for payment

Chapter 9 7
Patient Statements All transaction data stored in patient
ledger Statement shows
Services rendered Charges Payments made Balance owed
Statement is sent to patient or guarantor

Chapter 9 8
Computerized Billing Used to print patient statements and
blank patient encounter forms Also used to produce reports such
as Day sheets Monthly reports Aging reports Departmental income Physician income Procedure code usage

Chapter 9 9
Insurance Claims Most practices complete the
insurance form for the patient Form captures both clinical and
financial information Transmitted to patient’s insurance carrier Partial or full reimbursement

Chapter 9 10
The CMS-1500 Claim Form
Most common paper claim form Prepared by medical insurance
specialist Data is collected from
Patient information form Patient encounter form
Transmitted via mail

Chapter 9 11
The HIPAA Claim Form
Standard format for electronic claims Accepted by government and private
carriers Prepared on computer by medical
insurance specialist Transmitted via a modem to insurance
company Faster and easier to track

Chapter 9 12
Third-Party Payers Insurance carriers
Review claim for accuracy and completeness Evaluate treatment received Decide what benefits are due to the insured
Carrier may Pay the claim Deny the claim Pay less than the full amount

Chapter 9 13
ERA/EOB ERA is electronic EOB is paper Explains reimbursement decision
Amount of benefit Benefits paid to Paid on behalf of How determined
May include check or record of EFT

Chapter 9 14
ERA/EOB (cont’d)
Administrative medical assistant checks report against original claim
Files with patient’s financial records Updates patient’s ledger Deposits check or records EFT

Chapter 9 15
Patient Billing After insurance claim process has
been completed Patient may be billed for amounts not
fully reimbursed by the carrier Administrative medical assistant acts
as go-between for carrier and patient

Chapter 9 16
Completing the Claim Form
Verify insurance information Use phone, fax, or Web to verify coverage
Accuracy of data Contract numbers Patient’s identification information Insured’s information Secondary carriers, if any Illness or injury related to work or accident Diagnosis codes Procedure codes and charges Provider information

Chapter 9 17
Using Computers to Create Claims
Computerized billing and claims Most practices use software programs, such as
NDCMediSoft, to store information about patients and insurance plans
Claims created by billing programs may be printed or submitted electronically
The stored information is called a database

Chapter 9 18
Electronic vs. Paper Claims
Electronic claims Transmitted via
modem Receive immediate
feedback Faster
reimbursement Greater accuracy Less expensive
Paper claims Sent through mail Must be keyed or
scanned by insurance company into its computer system
Possibility of errors

Chapter 9 19
Clearinghouses Service bureau
Acts as an intermediary between provider and payer
Reformats data from provider to a form accepted by the payer

Chapter 9 20
Follow-up ERA/EOB checked
Procedures listed on ERA/EOB match claim
Unpaid charges explained Codes on ERA/EOB match claim Payment listed for each procedure is
correct

Chapter 9 21
Follow-up (cont’d)
Tracer Contains basic billing information and
asks carrier about status Paper or electronic Some providers automatically rebill after
30 days

Chapter 9 22
Follow-up (cont’d)
Denied or late claims Unclear denial or incorrect payment should
be followed up to determine cause Carrier asks for more information to process
claim Claims investigated for preexisting
conditions

Chapter 9 23
Follow-up (cont’d)
Provider resubmits claims on own Mistake in billing Claim overlooked
Insurance carrier asks for resubmission Incorrect codes have been submitted Information is incomplete or missing Charges do not total properly
Appeal process

Chapter 9 24
Patient Payments
Cash flow Payment methods
Collection at the time of service Monthly billing Fixed weekly or monthly payments Bill health insurance carriers Cash-only basis

Chapter 9 25
Cash Payments Each payment is entered in
Patient’s ledger Daily record
Payments given to assistant, not physician
Receipt must be given Safeguard money
Endorse checks for deposit only Daily bank deposits

Chapter 9 26
Patient Statements Monthly billing
Bills sent once a month Timed near end of month to coincide with
patient’s other bills Cycle billing
Avoids once-a-month billing workload Stabilizes cash flow Accounts divided into equal groups Each group billed on a different date

Chapter 9 27
Payment Plansand Adjustments
Payment plans Patients unable to pay bill in one lump sum Agreement in writing
Fee adjustment Write-offs—PAR provider not permitted to
bill for difference between amount charged and amount reimbursed
Physician may choose to reduce or cancel a bill
Written evidence; don’t delete transactions

Chapter 9 28
Health Insurance Provides payment for a portion of
medical expenses Participating (PAR) providers usually file
claims for patients Patients responsible for copayments
Non-participating (nonPAR) providers expect payment at time of service
Receipt given to patient for payment Patient may file claim

Chapter 9 29
Third-Party Liability Person other than patient is
responsible for charges Assistant must obtain verification from third
party Must be in writing; can not be oral
Guarantor Person who is the policyholder for the
patient Dependent children

Chapter 9 30
Collections Effective communication with
patients is first step in collections process Notify patient in advance of probable costs
not covered by insurance plans Have patient agree in writing to pay for
noncovered services Advance Notice for Noncovered Services
Make payment arrangements before services are performed

Chapter 9 31
Collections (cont’d)
Collection ratio At least 1/3 of the outstanding accounts
should be collected each day Aging accounts
Status: 30, 60, or 90 days past due Laws regulating collections
Fair Debt Collection Practices Act of 1977 Telephone Consumer Protection Act of 1991

Chapter 9 32
Collections (cont’d)
Collection methods Office policies Federal laws and state laws
Telephone Letter Terminated accounts
Physician may terminate the relationship due to lack of payment
Collection agencies

Chapter 9 33
Collections (cont’d)
Statute of Limitations Set by each state
Truth in Lending Act of 1960 For payment plans over 4 payments in
length, with finance charges Regulation Z requires a disclosure form to
be completed and signed by practice manager and patient

Chapter 9 34
Collections (cont’d)
Uncollectable accounts All collection attempts have been exhausted Would cost more to continue collection
attempts than the amount due Written off as bad debt

Chapter 9 35
Quiz
False, collections are begun after the bill is more than 30 days overdue.
False, the insurance carrier uses ERA/EOB to inform the patient/provider of the status of claims.
The ERA/EOB is submitted to the insurance carrier as part of the claim. (T/F)
An appeal is a formal method of asking for reconsideration of a denied claim. (T/F)
Collections are made on current bills. (T/F)
True, the appeal is done in writing.

Chapter 9 36
Critical Thinking List some advantages of electronic
claims.
Advantages of electronic claims: lower costs, reduced rejection, greater accuracy, faster payment, access to status reports.