Embed Size (px)
Citation preview

S
Bw
A
S
a
A
R
A
A
K
B
C
E
P
D
d
N
E
E
2
a r c h s o c e s p o f t a l m o l . 2 0 1 2;8 7(1 0):333–336
ARCHIVOS DE LA SOCIEDADESPAÑOLA DE OFTALMOLOGÍA
www .e lsev ier .es /o f ta lmologia
hort communication
est’s vitelliform macular dystrophy associatedith choroidal neovascularization�
. Céspedes, M. Pérez-De-Arcelus ∗, J. García-Arumí
ervicio de Oftalmología, Hospital Vall d’Hebron, Barcelona, Spain
r t i c l e i n f o
rticle history:
eceived 1 September 2011
ccepted 27 November 2011
vailable online 30 November 2012
eywords:
est’s vitelliform macular dystrophy
horoidal neovascularization
lectrooculogram
a b s t r a c t
Case report: We report the case of a child with a sudden loss of vision of the left eye. Oph-
thalmoscopic examination revealed vitelliform lesions in both foveal centers, as well as an
adjacent hemorrhage in his left eye. Fluorescein angiography confirmed the presence of
a neovascular membrane in his left eye. The electrooculogram showed disease. According
to complementary studies the patient was diagnosed with Best’s disease associated with
choroidal neovascularization.
Discussion: The diagnosis of Best’s vitelliform macular dystrophy is often a casual finding
as visual acuity tends to remain stable for long periods of time. A sudden deterioration in
vision may suggest complications, such as choroidal neovascularization.
© 2011 Sociedad Española de Oftalmología. Published by Elsevier España, S.L. All rights
reserved.
Distrofia macular viteliforme de Best asociada a neovascularizacióncoroidea
alabras clave:
istrofia macular viteliforme
e Best
eovascularización coroidea
lectrooculograma
r e s u m e n
Caso clínico: Se presenta el caso de un nino con pérdida súbita de visión en ojo izquierdo.
El examen funduscópico revela una lesión foveal viteliforme bilateral, y una hemorragia
adyacente en ojo izquierdo. La angiografía con fluoresceína confirma la presencia de una
membrana neovascular en ojo izquierdo. El electrooculograma resulta patológico. Tras com-
pletar el estudio, es diagnosticado de enfermedad de Best asociada a neovascularización
coroidea.
Discusión: El diagnóstico de enfermedad de Best puede ser casual dado que la agudeza visual
suele permanecer estable. Una pérdida súbita de visión ha de sugerirnos la aparición de
complicaciones tales como neovascularización coroidea.
spañ
© 2011 Sociedad E� Please cite this article as: Céspedes A, et al. Distrofia macular vitelsp Oftalmol. 2012;87:333–6.∗ Corresponding author.
E-mail address: [email protected] (M. Pérez-De-Arcelus).
173-5794/$ – see front matter © 2011 Sociedad Española de Oftalmolog
ola de Oftalmología. Publicado por Elsevier España, S.L. Todos los
derechos reservados.
iforme de Best asociada a neovascularización coroidea. Arch Soc
ía. Published by Elsevier España, S.L. All rights reserved.
m o l . 2 0 1 2;8 7(1 0):333–336
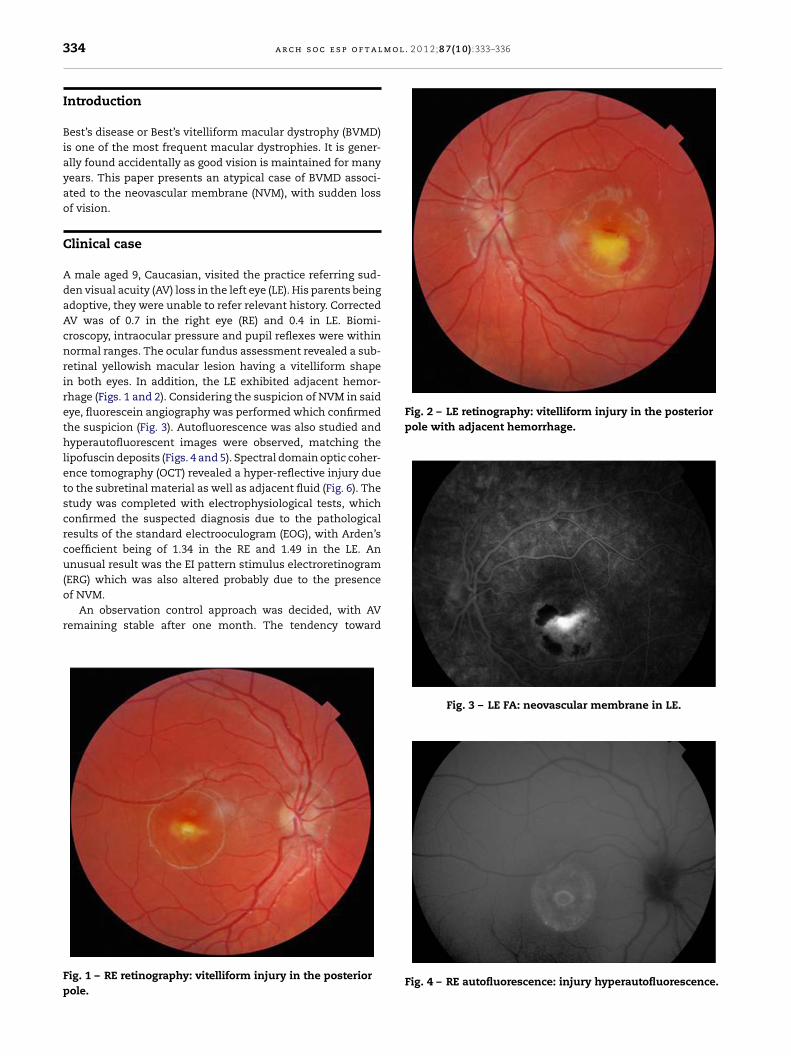
Fig. 2 – LE retinography: vitelliform injury in the posteriorpole with adjacent hemorrhage.
334 a r c h s o c e s p o f t a l
Introduction
Best’s disease or Best’s vitelliform macular dystrophy (BVMD)is one of the most frequent macular dystrophies. It is gener-ally found accidentally as good vision is maintained for manyyears. This paper presents an atypical case of BVMD associ-ated to the neovascular membrane (NVM), with sudden lossof vision.
Clinical case
A male aged 9, Caucasian, visited the practice referring sud-den visual acuity (AV) loss in the left eye (LE). His parents beingadoptive, they were unable to refer relevant history. CorrectedAV was of 0.7 in the right eye (RE) and 0.4 in LE. Biomi-croscopy, intraocular pressure and pupil reflexes were withinnormal ranges. The ocular fundus assessment revealed a sub-retinal yellowish macular lesion having a vitelliform shapein both eyes. In addition, the LE exhibited adjacent hemor-rhage (Figs. 1 and 2). Considering the suspicion of NVM in saideye, fluorescein angiography was performed which confirmedthe suspicion (Fig. 3). Autofluorescence was also studied andhyperautofluorescent images were observed, matching thelipofuscin deposits (Figs. 4 and 5). Spectral domain optic coher-ence tomography (OCT) revealed a hyper-reflective injury dueto the subretinal material as well as adjacent fluid (Fig. 6). Thestudy was completed with electrophysiological tests, whichconfirmed the suspected diagnosis due to the pathologicalresults of the standard electrooculogram (EOG), with Arden’scoefficient being of 1.34 in the RE and 1.49 in the LE. Anunusual result was the EI pattern stimulus electroretinogram(ERG) which was also altered probably due to the presence
of NVM.An observation control approach was decided, with AVremaining stable after one month. The tendency toward
Fig. 1 – RE retinography: vitelliform injury in the posteriorpole.
Fig. 3 – LE FA: neovascular membrane in LE.
Fig. 4 – RE autofluorescence: injury hyperautofluorescence.

a r c h s o c e s p o f t a l m o l . 2
Fig. 5 – LE autofluorescence.
tdtoidgm
D
Btm(mcwapl
he self-limitation of choroidal NVM in young patients wasescribed by Ho and Glaser, probably due to the hyper func-ion of the retina pigment epithelium (RPE) in the areaf the injury and to the production of neovascularization
nhibitors.1,2 On the other hand, prospective studies withefinitive results on the possible adverse effects of antian-iogenic injection in young patients have not yet beenade.
iscussion
VMD is an autosomic dominant inheritance maculopa-hy with variable expressiveness and penetration, related to
utations of the bestrophin gene located in chromosome 1111q131). The product of said gene is bestrophin-1, a trans-
embrane protein the expression of which is associated tohlorine channels in the EPR cells.3 The ionic flow alteration
ould explain both the electrophysiological findings and theccumulation of lipofuscin. Accordingly, a reduced luminouseak of EOG is typical. It seems that this peak reflects the depo-arization of the basal RPE membrane due to an increase in
Fig. 6 – OCT of both eyes: hyper-reflective injury wi
0 1 2;8 7(1 0):333–336 335
the conductivity of chlorine,3 so that a poor function of thesechannels would give rise to an Arden quotient below 1.5. EOGcan be useful to detect patients who exhibit said mutationwithout funduscopic involvement. The detection of carriersis important because they can transmit the disease to thefollowing generations.
BVMD is typically bilateral and appears in childhood.Patients frequently exhibit yellowish lesions due to accumu-lation of lipofuscin which deposits excessively due to theinability of RPE to digest the external segments of photore-ceptors in the context of an ionic imbalance.
Classically, it has been classified in 6 phenotypic stages4:
1. Pre-vitelliform stage: altered EOG can be detected althoughthe funduscopy appears normal.
2. Vitelliform stage: a subretinal yellowish lesion can be seen,similar to the yolk of an egg.
3. Pseudohypopion: the material deposits forming a level withrespect to the LSR situated in the upper area.
4. Vitelliruptive stage: the lesion becomes more uneven andthe alteration of the RPE becomes more evident.
5. Atrophy: the pigment disappears leaving a central atrophyarea in the RPE with ensuing visual loss.
6. Subretinal neovascularization: on some occasions NVMcan develop causing a sudden AV reduction. Said complica-tion is infrequent and can appear in late stages, in contrastwith the instant case.
In what concerns supplementary tests, a marked hyper-autofluorescence of the vitelliform material is characteristicalthough in advanced stages hypoautofluorescence predomi-nates due to RPE atrophy. OCT allows the identification of thedeposit site and the existence of subretinal fluid or RPE atro-phy. FA is not routinely performed unless NVM is suspected.
Despite the typical and striking macular alterations inBVMD patients, its diagnosis is accidental as they maintaingood vision.5 For this reason, any AV reduction should sug-gest the appearance of complications, such as NVM, fibrosis or
macular atrophy. However, as stated above, said injuries gen-erally appear in late stages, presentation at the onset beingatypical.th accumulation of adjacent subretinal liquid.

m o l
r
1
2
3
336 a r c h s o c e s p o f t a l
Conflict of interests
No conflict of interest has been declared by the authors.
e f e r e n c e s
. Glaser BM, Campochiaro PA, Davis Jr JL, Jerdan JA. Retinalpigment epithelial cells release inhibitors ofneovascularization. Ophthalmology. 1987;94:780–4.
4
5
. 2 0 1 2;8 7(1 0):333–336
. Ho AC, Yannuzzi LA, Pisicano K, DeRosa J. The natural historyof idiopathic subfoveal choroidal neovascularization.Ophthalmology. 1995;102:782–9.
. Hartzell C, Qu Z, Putzier I, Artinian L, Chien LT, Cui Y. Lookingchloride channels straight in the eye: besthropins,lipofucsinosis and retinal degeneration. Physiology (Bethesda).2005;20:292–302.
. Blodi CF, Stone EM. Best’s vitelliform dystrophy. OphthalmicPaediatr Genet. 1990;11:49–59.
. Mohler CW, Fine SL. Long-term evaluation of patients withBest’s vitelliform dystrophy. Ophthalmology. 1981;88:688–91.





























