Embed Size (px)
Citation preview

Rasmus Sejersten Ripa G
ranulocyte‐Colony Stimulating Factor Therapy to Induce N
eovascularization in Ischemic Heart Disease
Granulocyte‐Colony Stimulating Factor Therapy to Induce Neovascularization
in Ischemic Heart Disease
Rasmus Sejersten Ripa
ISBN 978‐87‐994776‐0‐9
Cover: Phoenix depicted in the book Bilderbuch für Kinder by F.J. Bertuch (1747‐1822)

F A C U L T Y O F H E A L T H S C I E N C E S U N I V E R S I T Y O F C O P E N H A G E N
Granulocyte-Colony Stimulating Factor
Therapy to Induce Neovascularization in
Ischemic Heart Disease
Rasmus Sejersten Ripa
Forsvaret finder sted onsdag den 30. november 2011, kl. 14 præcis i Medicinsk Museion, Bredgade 62, København
Forsvarsleder: Professor, overlæge, dr.med. Torben V. Schroeder Formand for bedømmelsesudvalget: Professor, overlæge, dr.med. Niels Borregaard
Universitetets officielle opponenter: Professor, overlæge, dr.med. Erling Falk og Professor, overlæge, ph.d., dr.med. Hans Erik Bøtker

- 2 -
Denne afhandling er i forbindelse med anførte tidligere offentliggjorte artikler af Det Sundhedsvidenskabelige Fakultet ved Københavns Universitet antaget til offentligt at forsvares for den medicinske doktorgrad.
København, den 1. august 2011. Ulla Wewer, Dekan
This dissertation is based on the following original publications. These publications are referred to by their roman numerals:
(I) Ripa RS, Wang Y, Jørgensen E, Johnsen HE, Hesse B, Kastrup J. Intramyocardial Injection of Vascular Endothelial Growth Factor-A165 Plasmid Followed by Granulocyte-Colony Stimulating Factor to Induce Angiogenesis in Patients with Severe Chronic Ischemic Heart Disease. Eur Heart J 2006;27:1785-92.
(II) Ripa RS, Wang Y, Goetze JP, Jørgensen E, Johnsen HE, Tägil K, Hesse B, Kastrup J. Circulating Angiogenic Cytokines and Stem Cells in Patients with Severe Chronic Ischemic Heart Disease – Indicators of Myocardial Ischemic Burden? Int J Cardiol 2007;120:181-187.
(III) Ripa RS, Jørgensen E, Baldazzi F, Frikke-Schmidt R, Wang Y, Tybjærg-Hansen A, Kastrup J. The Influence of Genotype on Vascular Endothelial Growth Factor and Regulation of Myocardial Collateral Blood Flow in Patients with Acute and Chronic Coronary Heart Disease. Scand J Clin Lab Invest 2009;69:722-728.
(IV) Ripa RS, Jørgensen E, Wang Y, Thune JJ, Nilsson JC, Søndergaard L, Johnsen HE, Køber L, Grande P, Kastrup J. Stem Cell Mobilization Induced by Subcutaneous Granulocyte-Colony Stimulating Factor to Improve Cardiac Regeneration After Acute ST-Elevation Myocardial Infarction. Result of the Double-Blind Randomized Placebo Controlled STEMMI Trial. Circulation 2006;113:1983-1992.
(V) Ripa RS, Haack-Sørensen M, Wang Y, Jørgensen E, Mortensen S, Bindslev L, Friis T, Kastrup J. Bone Marrow-Derived Mesenchymal Cell Mobilization by Granulocyte-Colony Stimulating Factor after Acute Myocardial Infarction: Results from the Stem Cells in Myocardial Infarction (STEMMI) Trial. Circulation 2007;116(11 Suppl):I24-30.
(VI) Ripa RS, Nilsson JC, Wang Y, Søndergaard L, Jørgensen E, Kastrup J. Short- and Long-Term Changes in Myocardial Function, Morphology, Edema and Infarct Mass Following ST-Segment Elevation Myocardial Infarction Evaluated by Serial Magnetic Resonance Imaging. Am Heart J 2007;154:929-36.
(VII) Lyngbæk S, Ripa RS, Haack-Sørensen M, Cortsen A, Kragh L, Andersen CB, Jørgensen E, Kjær A, Kastrup J, Hesse B. Serial in vivo Imaging of the Porcine Heart After Percutaneous, Intramyocardially Injected 111Indium-Labeled Human Mesenchymal Stromal Cells. Int J Cardiovasc Imaging 2010; 26:273-84.
ISBN 978-87-994776-0-9

- 3 -
PREFACE
The thesis is based on research performed during my
time as research fellow at the Department of
Cardiology, Rigshospitalet, from 2003 to 2007.
I am indebted to Jens Kastrup, MD, DMSc who
introduced me to cardiac neovascularization therapy.
His continuous interest in my work and never failing
optimism despite negative results encouraged me to
move on. It has always been a pleasure working with
Jens. Erik Jørgensen, MD has provided brilliant ideas
and constructive criticism in all phases of our trials. His
clinical approach and broad view of things when I
tended to be lost into the details has improved the work
substantially.
The remaining members of the “Cardiac Stem Cell
Laboratory”, Wang Yongzhong, MD, PhD; Mandana
Haack-Sørensen, MSc; Lene Bindslev, MSc, PhD; Tina
Friis, MSc, PhD; Stig Lyngbæk, MD; Steen Mortensen,
Tech; and Sandra Miran, RN have provided an
innovative and enthusiastic atmosphere.
I was originally introduced to research during medical
school by Marie Luise Bisgaard, MD. The years of basic
laboratory work has been a steady foundation for my
continued interest in research. Later, I became involved
in clinical research during my stay as research fellow at
Duke University Medical Center, North Carolina, USA.
Galen S. Wagner, MD; Peter Clemmensen, MD, DMSc;
and Peer Grande, MD, DMSc were devoted mentors
(and pleasant travel companions) and have since been
following my work with great interest and inspiring
comments.
I wish to thank all my co-authors who contributed with
their expertise to complete the studies. A special
gratitude to Jens Christian Nilsson, MD, PhD and Lars
Søndergaard, MD, DMSc who taught me cardiovascular
MRI, and to Birger Hesse, MD, DMSc and Andreas Kjær,
MD, DMSc who introduced me to nuclear medicine.
Finally, I want to express my appreciation to all the
research fellows and study nurses at the 14th floor.
Space was limited, but we have had plenty of coffee,
fruitful discussions and exiting trips to conferences
around the world - it was never boring. A special thanks
to Jens Jakob Thune, MD, PhD who besides conducting
all the STEMMI echoes also was a daily source of
inspiration, and to Matias Lindholm, MD, PhD who
initiated the “kageklub” and explored Boston shopping
with me.
This work would not have been possible without the
generous donations by: The Danish Heart Foundation;
Danish Stem Cell Research Doctoral School; Faculty of
Health Sciences, Copenhagen University; Hjertecentrets
Forskningsfond, Rigshospitalet; The Danish Medical
Research Council; Lundbeck Fonden; Raimond og
Dagmar Ringgård-Bohn’s Fond; Aase og Ejnar
Danielsens Fond; Erik og Martha Scheibels Legat; Arvid
Nilssons Fond; Fonden af 17.12.1981; and Georg
Bestles Fond.
Rasmus Sejersten Ripa
February 2011
Til Maria,
Alvin og Josefine

- 4 -
CONTENTS
BACKGROUND AND AIM
Ischemic heart disease 7 Biological intervention in myocardial regenerative medicine 7 Protein therapy 7 Gene therapy 8 Stem cell therapy 8 Granulocyte-Colony Stimulating Factor 9 Pathogenesis of myocardial regeneration 11 Bone marrow-derived stem- and progenitor cells 13 Potential mechanisms of cell-based therapy 15 Aim and hypothesis 16 TRIAL DESIGN
Measures of efficacy 16 Myocardial volumes and function 16 Myocardial perfusion 17 Conclusion 18 Ethical considerations in trial design 18 G-CSF FOR CHRONIC ISCHEMIA
G-CSF and VEGF gene therapy 19 Safety of G-CSF to patients with chronic ischemia 21 Does G-CSF reduce myocardial ischemia? 21 Angiogenesis or arteriogenesis 21 Patient population 22 Homing of bone marrow-derived cells into ischemic myocardium 23
G-CSF FOR STEMI
Clinical trials 25 Safety of treatment with G-CSF after STEMI 26 Why does G-CSF not improve myocardial function following STEMI? 27 Time to G-CSF 27 The G-CSF dose 28 Differential mobilization of cells types 28 Homing of mobilized cells to the myocardium 29 Conclusion 30 MYOCARDIAL RECOVERY AFTER STEMI 31 FROM BED TO BENCH 32 GENERAL CONCLUSIONS AND FUTURE DIRECTIONS 34 SUMMARY IN DANISH – DANSK RESUMÉ 36 REFERENCES 37

- 5 -
Granulocyte-Colony Stimulating Factor Therapy to Induce Neovascularization in Ischemic Heart Disease Rasmus Sejersten Ripa ABSTRACT
Cell based therapy for ischemic heart disease has the
potential to reduce post infarct heart failure and chronic
ischemia.
Treatment with granulocyte-colony stimulating factor
(G-CSF) mobilizes cells from the bone marrow to the
peripheral blood. Some of these cells are putative stem
or progenitor cells. G-CSF is injected subcutaneously.
This therapy is intuitively attractive compared to other
cell based techniques since repeated catheterizations
and ex vivo cell purification and expansion are avoided.
Previous preclinical and early clinical trials have
indicated that treatment with G-CSF leads to improved
myocardial perfusion and function in acute or chronic
ischemic heart disease.
The hypothesis of this thesis is that patient with
ischemic heart disease will benefit from G-CSF therapy.
We examined this hypothesis in two clinical trials with
G-CSF treatment to patients with either acute
myocardial infarction or severe chronic ischemic heart
disease. In addition, we assed a number of factors that
could potentially affect the effect of cell based therapy.
Finally, we intended to develop a method for in vivo cell
tracking in the heart.
Our research showed that subcutaneous G-CSF along
with gene therapy do not improve myocardial function
in patients with chronic ischemia despite a large
increase in circulation bone marrow-derived cells. Also,
neither angina pectoris nor exercise capacity was
improved compared to placebo treatment. We could not
identify differences in angiogenic factors or bone
marrow-derived cells in the blood that could explain the
neutral effect of G-CSF.
Next, we examined G-CSF as adjunctive therapy
following ST segment elevation myocardial infarction.
We did not find any effect of G-CSF neither on the
primary endpoint - regional myocardial function - nor on
left ventricular ejection fraction (secondary endpoint)
compared to placebo treatment. In subsequent
analyses, we found significant differences in the types
of cells mobilized from the bone marrow by G-CSF. This
could explain why intracoronary injections of
unfractionated bone marrow-derived cells have more
effect that mobilization with G-CSF.
A number of other factors could explain the neutral
effect of G-CSF in our trial compared to previous
studies. These factors include timing of the treatment,
G-CSF dose, and study population. It is however,
remarkable that the changes in our G-CSF group are
comparable to the results of previous non-blinded
studies, whereas the major differences are in the
control/placebo groups. We found that ejection fraction,
wall motion, edema, perfusion, and infarct size all
improve significantly in the first month following ST-
segment myocardial infarction with standard guideline
treatment (including acute mechanical re-
vascularization), but without cell therapy. This is an
important factor to take into account when assessing
the results of non-controlled trials.
Finally, we found that ex vivo labeling of cells with
indium-111 for in vivo cell tracking after intramyocardial
injection is problematic. In our hand, a significant
amount of indium-111 remained in the myocardium
despite cell death. It is difficult to determine viability of
the cells after injection in human trials, and it is thus
complicated to determine if the activity in the
myocardium tracks viable cells.
Cell based therapy is still in the explorative phase, but
based on the intense research within this field it is our
hope that the clinical relevance of the therapy can be
determined in the foreseeable future. Ultimately, this
will require large randomized, double-blind and placebo-
controlled trials with “hard” clinical endpoints like
mortality and morbidity.

- 6 -

- 7 -
BACKGROUND AND AIM The concept of adult stem cells within the bone marrow
was introduced in 1960 by identification of cells capable
of reconstituting hematopoiesis in mice.1 Asahara et al2,3
extended this concept almost 40 years later by showing
that bone marrow-derived circulating endothelial
progenitor cells incorporated into sites of angiogenesis
in animal models of ischemia. In 2001, Orlic et al4
published a ground-breaking but also very
controversial5,6 trial challenging the paradigm of the
heart as a post-mitotic organ thereby igniting the notion
of cardiac regeneration. In the following decade an
increasing number of animal and small clinical studies
have indicated an effect of cell based therapies for
ischemic heart disease.
Ischemic heart disease
Ischemic heart disease is caused by a pathological
mismatch between the supply to and demand for
oxygen in the left ventricle. The pathology is most
commonly stenotic or obstructive atherosclerotic disease
of the epicardial coronary artery. The normal coronary
circulation supplies the heart with sufficient oxygen to
prevent underperfusion. This is accomplished by the
ability of the coronary vasculary bed to rapid adaptation
of the coronary blood flow by varying its resistance.
An atherosclerotic stenosis increases epicardial
resistance and thus limits appropriate increases in
perfusion when the demand for oxygen is augmented
(e.g. during exercise). In severe stenosis, small changes
in luminal diameter (e.g. by spasm or thrombi) can
produce significant hemodynamic effects and even
reduce myocardial perfusion at rest. Myocardial
ischemia can also occur with normal oxygen supply if
myocardial demands are markedly increased by left
ventricular hypertrophy or during exercise.
The symptoms of myocardial ischemia range from silent
ischemia to stable angina pectoris to unstable angina
pectoris to non-ST- and ST-segment elevation
myocardial infarction (STEMI).
Patients with STEMI or patients with moderate to severe
but stable angina pectoris (Canadian Cardiovascular
Society (CCS) angina class II-IV) have been included
into the majority of trials with gene- or cell-therapy. The
pathology in these two populations has many similarities
but also some important differences.
First, patients with STEMI (usually patients with
previous myocardial infarction are excluded) have a
single, or occasionally a few, severe ischemic events
caused by one coronary occlusion whereas the patients
with chronic ischemia suffer from intermittent
myocardial ischemia (often through years) usually
caused by stenotic lesions in several coronary arteries.
Second, patients with chronic ischemia typically have
reversible ischemia not leading to myocardial necrosis,
whereas patients with STEMI develop irreversible
myocardial damage. We thus have difference in the
therapeutic goals in the two patient populations.
Patients with STEMI need new myocytes and vascular
support for both new myocytes and for hibernating
myocytes within the necrotic area, whereas patients
with chronic ischemia primarily need improved perfusion
of the reversible ischemic area. This also affects the
endpoint assessment in the two populations. Patients
with chronic ischemia will be expected to have no
change or even a slow deterioration in heart function
with their current anti-ischemic treatment whereas
patients after STEMI are expected to have a recovery in
function due to recovery of hibernating myocardium
following balloon angioplasty and coronary stenting. A
significant placebo effect can be expected in both
populations underscoring the need for a proper control
group.
Many early phase clinical trials of new therapies for
patients with ischemic heart disease have safety as
primary endpoint and efficacy as secondary exploratory
endpoint. These early trials are often without control-
groups or with non-blinded, non-placebo treated
controls. This warrants for extreme caution in data
interpretation since both a significant placebo effect as
well as a significant change due to ‘the natural course’
must be accounted for.
Biological intervention in myocardial regenerative
medicine
Based on our pathogenetic understanding, previous
trials of biological intervention in myocardial
regeneration can roughly be divided into three main
groups, vascular growth factor proteins, genes encoding
vascular growth factors, and stem/progenitor cell
therapy. Only a few trials have combined these
modalities.
Protein therapy
The list of known vascular growth factors with

- 8 -
angiogenic potential is long and includes vascular
endothelial growth factor (VEGF) A,B,C,D,E; fibroblast
growth factor (FGF) 1,2,4,5; angiopoitin 1,2; hepatocyte
growth factor, monocyte chemotactic protein 1, platelet
derived growth factor BB, e-nitric-oxide synthase, i-
nitric-oxide synthase, and many more.7 So far, mainly
VEGF-A8-10 and FGF11-18 have been used in human trials
since these seem to be most important in adult vessel
growth.
The trials hypothesized that increased supply of vascular
growth factors increases neovascularization and thus
improve symptoms. The primary goals of the trials were
to develop an administration strategy that provided
optimal local tissue concentration for an optimal period
of time without high systemic concentrations.
The VIVA trial9 and the FIRST trial14 were the two
largest randomized trials using VEGF-A165 and FGF-2,
respectively. Despite encouraging earlier trials with
fewer patients and often without controls both the VIVA
trial and the FIRST trial were neutral without any
improvement beyond placebo. The explanations for
these disappointing results could be several, first VEGF-
A and FGF might not have any significant clinical effect,
second dose and route of administration may be
insufficient in achieving optimal concentration of the
growth factor within the heart. The second hypothesis is
supported by the short half-life of the administered
protein, but administration of a higher dose was not
possible due to dose-limiting toxicities resulting from
systemic exposure.
Trials with growth factor gene therapy were then
initiated to enhance myocardial expression for a
sustained period of time and to minimize systemic
effects.
Gene therapy
Gene therapy is introduction of genetic material into an
organism in order to obtain a therapeutic result by
production of proteins. The advantages over protein
therapy are primarily less systemic concentrations and
prolonged period of expression. Some of the pitfalls are
to achieve optimal tissue expression and to prevent
expression in other tissues. The gene needs a
transfection vector to get into the cells; this can be
viruses, liposome particles or naked plasmids.19 Naked
plasmid is the most simple to use, but also a method
with low transfection rate.
Several minor safety and efficacy trials using both the
VEGF-A and the FGF genes have been published.20-25
Naked plasmid, liposomes, and viruses have been used
as transfection vector, and both intracoronary and
intramyocardial (during thoracotomy or percutaneously)
administration has been used.
The REVASC Trial26 randomized 67 patients with severe
angina pectoris and coronary artery disease to
intramyocardial AdVEGF-A121 gene transfer (N=32) or
continued maximum medical therapy (N=35). The
treatment was open-label, and the control group did not
receive placebo treatment. The primary endpoint of
change in time to ST-segment depression on exercise
ECG after 12 weeks was not statistically significant
compared to controls. Several secondary endpoints
including exercise test at 26 weeks, and CCS angina
class did reach a statistical significant difference.26
Our group initiated a multicenter, randomized, double-
blind, and placebo controlled trial of plasmid VEGF-A165
gene therapy in patients with stable severe angina
pectoris (The Euroinject One Trial).27-29 Intramyocardial
injections of the plasmids or placebo were given via the
left ventricular cavity using a catheter-based guiding
and injection system (the NOGA-Myostar system).
Eighty patients with severe stable ischemic heart
disease and significant reversible perfusion defects
assessed by single photon emission tomography
(SPECT) were included. The prespecified primary end
point was improvement in myocardial perfusion defects
at the 3-months follow-up SPECT and patients were
followed with clinical examinations, SPECT, NOGA,
exercise test, angiography and echocardiography.
Disappointingly, the VEGF-A gene transfer did not
significantly improve the stress-induced myocardial
perfusion abnormalities compared with placebo.
However, local wall motion disturbances (secondary
endpoints) improved assessed both by NOGA (p = 0.04)
and contrast ventriculography (p = 0.03). Finally, no
gene-related adverse events were observed.27
The next step from protein/gene therapy to cell therapy
was promoted by these rather discouraging clinical
results with protein/gene treatment, and very positive
preclinical studies utilizing bone marrow-derived stem-
or progenitor cells.
Stem cell therapy
The rigorous definition of a stem cell requires that it
possesses self-renewal and unlimited potency. Potency
(differentiation potential) is divided into totipotent

- 9 -
(differentiate into embryonic and extraembryonic cell
types), pluripotent (differentiate into cells derived from
any of the three germ layers), multipotent (produce
only cells of a closely related family of cells), and
unipotent (can produce only one cell type); strictly only
totipotent and pluripotent cells are stem cells whereas
multipotent or unipotent cells with self-renewal capacity
should be referred to as progenitor cells. It is a matter
of ongoing and hectic debate whether committed
hematopoietic progenitor cells can undergo
transdifferentiation into cardiac myocytes or not.4-6,30
Human studies have indicated that mobilization of
progenitor and stem cells is a natural response to
myocardial injury31-33 correlating to endogenous
concentration of granulocyte-colony stimulating factor
(G-CSF).34 The degree of mobilization seems to predict
the occurrence of cardiovascular events and death.35
Animal studies showed that bone marrow-derived
endothelial precursor cells could induce new blood
vessel formation (vasculogenesis) and proliferation from
existing vessels (angiogenesis) after myocardial
infarction.4,36 After a quick translation from bench to
bedside, several small human safety trials have been
conducted in patients with both chronic myocardial
ischemia37-43 and acute myocardial infarction44-49. Five
larger trials with intracoronary infusion of bone marrow-
derived mononuclear cells after acute myocardial
infarction have been published with diverging results.50-
54 The Norwegian ASTAMI trial (n=100)51, the Polish
REGENT trial (n=200)53, and the Dutch HEBE trial
(n=200)54 were randomized, but without placebo
treatment in the control-arm, whereas the German
REPAIR-AMI (n=204)50 and a Belgian trial (n=67)52 were
both randomized, double-blind, and placebo-controlled.
Only REPAIR-AMI showed a significant improvement in
the primary endpoint ejection fraction in the active arm
(48.3±9.2% to 53.8±10.2%) compared to the control
arm (46.9±10.4% to 49.9±13.0%; p=0.02). The trial
was not designed to detect differences in cardiac events,
but the prespecified secondary combined endpoint of
death, recurrence of myocardial infarction, or
revascularization at one year follow-up was significantly
reduced in the cell group compared with the placebo
group (p=0.009).55 In addition, there was a trend
towards improvement of individual clinical endpoint such
as death, recurrence of myocardial infarction, and
rehospitalization for heart failure.55 The 2-year follow-up
of the REPAIR-AMI trial demonstrated a sustained
reduction in major cardiovascular events. In a subgroup
of 59 patients magnetic resonance imaging (MRI)
showed a higher regional left ventricular contractility
and a non-significant difference in ejection fraction.56 In
comparison, 18 months follow-up data from the
randomized BOOST trial indicate that a single dose of
intracoronary bone marrow cells does not provide long
term improvement in left ventricular function when
compared to controls.57 The REPAIR-AMI Doppler
Substudy (n=58) has provided insight into the
mechanism of intracoronary cells infusions by measuring
a substantial improvement in minimal vascular
resistance during adenosine infusion 4 months after
treatment indicating an improved microvascular
circulation.58
The hitherto largest published trial of intramyocardial
bone marrow-derived cell injection for chronic
myocardial ischemia included 50 patients into a double-
blind, placebo-controlled trial.59 The authors reported a
significant improvement in stress score by SPECT 3
months after treatment (treatment effect of -2.44
points, p<0.001).
The designs of the trials have so far often been driven
by pragmatic solutions, and while some questions have
been answered many more have been raised. This has
opened for a reverse translation from bedside to bench
in order to clarify some of the unknown factors such as
optimal cell type and number, optimal route of
administration, optimal time of therapy, optimal patient
selection, usefulness of repeated or combined
treatments etc.60
The use of pharmacological mobilization of stem and
progenitor cells from the bone marrow into the blood is
an attractive alternative to intracoronary or
intramyocardial injection because the treatment is
noninvasive and does not require ex-vivo purification of
the cells. G-CSF is an appealing candidate since it is well
known from clinical hematology and thus has an
established safety profile.61
Granulocyte-Colony Stimulating Factor
Endogenous G-CSF is a potent hematopoietic cytokine
which is produced and released by monocytes,
fibroblasts, and endothelial cells. G-CSF regulates the
production of neutrophils within the bone marrow and
stimulates neutrophil progenitor proliferation,
maturation, and functional activation. G-CSF binds to
the G-CSF cell surface receptor expressed on myeloid

- 10 -
progenitor cells, myeloid leukemia cells, leukemic cell
lines, mature neutrophils, platelets, monocytes, and
some lymphoid cell lines.62 Ligand binding induces
activation of a variety of intracellular signaling cascades
ultimately affecting gene transcription, cell survival and
differentiation.62,63
G-CSF is involved in mobilization of granulocytes, stem,
and progenitor cells from the bone marrow into the
blood circulation.64 The process of mobilization has
mainly been investigated for hematopoietic stem and
progenitor cells and is not fully understood, but seems
to be mediated through binding of G-CSF to the G-CSF
receptor, leading to a subsequent digestion of adhesion
molecules by enzyme release from myeloid cells, and
through trophic chemokines. Stem cell derived factor-1
(SDF-1, also named CXCL12) and its receptor CXCR4
seem to play a central role in regulation of
hematopoietic stem cell trafficking in the bone marrow
and in mobilization by G-CSF. SDF-1 is a potent chemo
attractant for hematopoietic stem cells produced in the
bone marrow by stromal cells65 and its receptor CXCR4
is expressed on the surface of hematopoietic stem
cells66.
SDF-1 protein concentrations in the bone marrow
decline sharply during G-CSF treatment.67 SDF-1 mRNA
expression decreases during G-CSF mobilization, and
the magnitude of the decline correlates well with the
magnitude of mobilization.68 Studies of CXCR4 deficient
mice have shown that this gene is necessary for
sufficient retention of myeloid precursors in the bone
marrow69 and neutralizing CXCR4 or SDF-1 antibodies
significantly reduced stem cell mobilization.67 In
addition, inhibition of SDF-1 binding to CXCR4 (by
AMD3100) leads to rapid mobilization of hematopoietic
cells (CD34+) from the bone marrow.70 The opposite
effects of AMD-3100 and neutralizing CXCR4 antibodies
are puzzling and could reflect differences in the binding
properties of the two molecules.
Several other adhesion molecules are known to regulate
hematopoietic stem cell trafficking, such as VCAM-1/β-1
integrin, hyaluronic acid/CD44, kit/kit ligand, and
several selectins.71 G-CSF induces through an unknown
mechanism, a proteolytic microenvironment in the bone
marrow by release of a number of proteases including
neutrophil elastase, cathepsin G, and matrix
metalloproteinase 9.72 These proteolytic enzymes are
capable of cleaving the key adhesion molecules within
the bone marrow, SDF-1, VCAM-1, and kit ligand.67,73,74
However, neutrophil elastase, cathepsin G or matrix
metalloproteinase 9 deficient mice have normal G-CSF
induced mobilization,75 and thus the precise mechanism
for G-CSF induced cell mobilization remains to be
determined.
It has recently been shown that the G-CSF receptor is
expressed in cardiomyocytes and that G-CSF activates
signaling molecules in cardiomyocytes and hydrogen
peroxide-induced apoptosis was significantly reduced by
pre-treatment of cardiomyocytes with G-CSF.76 These
results suggest that G-CSF has direct anti-apoptotic
effect in cardiomyocytes besides mobilization,
differentiation and proliferation of stem or progenitor
cells. The proposed molecular mechanisms of these G-
CSF induced cardioprotective effects in the subacute-
chronic phase are through the Janus kinase 2 / Signal
transducer and activator of transcription 3 (Jak2/STAT3)
pathway activated by the G-CSF receptor.76 STAT3 is a
transcriptional factor known to activate numerous
growth factors and cytokines and has been shown to
protect the heart during stress (e.g. in patients with
myocardial infarction and during treatment with
cytotoxics).77,78 The cardioprotective effects of G-CSF on
post-myocardial infarction hearts were abolished in mice
overexpressing dominant-negative mutant STAT3
protein in the cardiomyocytes.76
Also recently, G-CSF has been proposed to have an
acute “postconditioning-like” effect on the reperfusion
injury.79 G-CSF administration started at onset of
reperfusion in a Langendorff-perfused rat heart led to
myocardial activation of the Akt/endothelial nitric oxide
synthase pathway leading to increased nitric oxide
production and ultimately to reduction in infarct size.79
Finally, G-CSF has been reported to be an anti-
inflammatory immunomodulator by inhibition of main
inflammatory mediators such as interleukin-1, tumor
necrosis factor-alpha, and interferon gamma.80,81 Thus,
G-CSF could attenuate left ventricular remodeling
following acute myocardial infarction by a direct anti-
inflammatory effect.
It remains to be determined whether the beneficial
effect of G-CSF on cardiac function in animal studies is
primarily caused via cell recruitment82 or via a more
direct effect on the myocardium.76
Filgrastim is a recombinant methionyl human
granulocyte colony-stimulating factor (r-metHuG-CSF)
of 175 amino acids. Neupogen® is the Amgen Inc.
trademark for filgrastim produced by Escherichia coli (E

- 11 -
coli) bacteria. The protein has an amino acid sequence
identical to the natural sequence, but the product is
nonglycosylated because Neupogen® is produced in E
coli, and thus differs from G-CSF isolated from human
cells.
Filgrastim has been used to mobilize hematopoietic
stem cells from the bone marrow to the peripheral
circulation for the treatment of patients with
hematologic diseases for several years, thus Filgrastim
treatment has been proven safe and effective in both
hematological patients and healthy donors.83,84 Mild side
effects are very frequent (typically bone pain, myalgia,
artralgia or headache) but they almost never leads to
discontinuation of treatment. Rare side effects (0.01-
0.1%) are interstitial pneumonitis, respiratory distress
syndrome, thrombocytopenia and reversible elevations
in uric acid. Very rare side effects (<0.01%) are spleen
rupture and allergic reactions.
The current clinical indications of Filgrastim in Denmark
are to (1) reduce the duration of neutropenia in patients
with nonmyeloid malignancies undergoing myeloablative
chemotherapy followed by marrow transplantation, (2)
reduce time to neutrophil recovery following
chemotherapy, (3) mobilize stem cells to the peripheral
blood, (4) for chronic administration to reduce the
incidence and duration of sequelae of severe
neutropenia.
Pathogenesis of myocardial regeneration
This section gives a short review of the mechanisms and
variables of importance for clinical biological
intervention. It is focused on vascular regeneration and
the impact of cellular components, growth factor and
cytokines.
Embryonic development and subsequent postnatal
adaptation of the vascular system to chances in
functional needs occur by three different processes: (1)
vasculogenesis, (2) angiogenesis, or (3) arteriogenesis
(review in 85). This nomenclature is not always strictly
followed, and some even uses the term ‘angiogenesis’ to
summarize all types of vascular formation. All tree
processes involves a cascade of different cell types,
numerous soluble and cell-bound factors, transcription
factors, and cell receptor expression in a complex
coordinated interaction that is still not completely
described. The below description is an overview of the
processes and some of the most important steps
involved. The mechanism of how bone marrow-derived
cells influence neovascularization remains debated
(page 15): Do the cells incorporate into the tissue (e.g.
as endothelial or smooth muscle cells) or do they
primarily act through paracrine signaling to support the
vessel growth and/or maturation?
Vasculogenesis is the first process in embryonic vascular
development and denotes an in situ differentiation of
endothelial precursor cells (hemangioblasts86) into blood
vessels. The mesoderm-derived angioblasts migrate into
clusters (blood islands) and mature into endothelial cells
that assemble into a primitive vascular network in both
the yolk sac and the embryo (review in 87) The process
is regulated by a cascade of growth and transcriptional
factors, proteases and receptor expressions. The
initiating signal for vasculogenesis in embryology is
probably tissue ischemia due to rapid tissue growth.
CXCR4 and SDF-1 are expressed during embryonic
development88 and a role in angioblasts migration to
ischemic areas could be assumed. FGF-2 and VEGF-A
appear paramount in subsequent blood island formation,
cell differentiation and vascular maturation.89-91
Tissue ischemia and exogenous granulocyte
macrophage-colony stimulating factor (GM-CSF) or
VEGF-A has been shown, in animal studies, to stimulate
postnatal vasculogenesis by mobilization and
differentiation of endothelial precursor cells.92,93 Like
angiogenesis, the process of postnatal vasculogenesis
within ischemic tissue is driven by hypoxia-induced
production of cytokines and growth factors like VEGF-A94
and SDF-195. Postnatal vasculogenesis requires
extravasation and migration of the progenitor cells as
described on page 23.
Angiogenesis is the capillary growth (sprouting) from
existing vessels. The term also involves division of
existing vessels by transendothelial cell bridges or pillars
of periendothelial cells. Angiogenesis is initiated by
hypoxic stabilization of the transcription factor hypoxia-
inducible factor (HIF)-1α.96 This leads to a local
upregulation in expression of VEGF-A and a number of
other angiogenic factors.97 The new sprouting vessel is
initiated in one endothelial cell lining the native vessel
(the ‘tip cell’). The endothelial cell exposed to the
highest VEGF-A concentration is selected as the
endothelial tip cell.98,99 Furthermore, this tip cell seems
to gain competitive advantage over neighboring
endothelial cells by VEGF-A induced upregulation of

- 12 -
‘delta-like 4’. Delta-like 4 activates Notch receptors on
the neighboring cells leading to a down-regulation of
delta-like 4 expression in these cells.100 VEGF-A exerts
its effect in angiogenesis primarily through binding to
the VEGFR2.99 The tip cell becomes a polarized non- or
low-proliferative cell with filopodia extending towards
and ‘sensing’ the angiogenic stimuli and environment.
The sprout elongates by migration of the tip cell and
proliferation of endothelial ‘stalk cell’ trailing behind the
tip cell.98,99 The stalk cells form junctions from the tip
cell to the native vessel and form a lumen in the new
sprout. The migration of the tip cell is an invasive
process requiring proteolytic degradation of the
extracellular matrix, especially the ‘membrane type-1
matrix metalloproteinase’ appears paramount for the
invasion.101 Eventually the sprout connects with another
sprout by tip cell fusion.102 The new tubular structure is
stabilized into a mature vessel by tightening of cellular
junctions, recruitment of pericytes and deposition of
extracellular matrix. Normoxia of the tissue once the
new vessel is perfused lowers the local VEGF-A
concentration leading to quiescent of the endothelial
cells (named ‘phalanx cells’) and vascular homeostasis.
Arteriogenesis denotes the formation of muscular
arterioles from preexisting capillaries or small arterioles.
Postnatal arteriogenesis is widely studied in collateral
vessel circulation following arterial occlusion. The
temporal sequence of arteriogenesis is divided into the
initiation phase, the growth phase, and the maturation
phase.
In contrast to angiogenesis, arteriogenesis seems
initiated by physical forces experienced by the cell
independent of ischemia. A pre-existing network of
small caliber collateral anastomoses exists in humans.
Arterial occlusion (e.g. by atherosclerotic plaque) result
in a drop in pressure distal to the occlusion. This new
pressure gradient across the occlusion drives the flow
along the smaller pre-existing bridging arteries to
circumvent the occlusion. Increased flow in the collateral
arteries creates a shear stress and circumferential
tension at the wall sensed by the smooth muscle cells
and endothelial cells. The physical stimuli in the smooth
muscle cells seem to increase expression of the
proarteriogenic molecule, ‘monocyte chemotactic
protein-1’ via the mechanosensitive transcription factor
‘activator protein-1’.103 The mechanical stimuli of
endothelial cells modulates endothelial gene
expression104 and gene expression analysis following
hindlimb ischemia in mice have identified differential
expression of more than 700 genes.105 Very fast surface
expression of adhesion molecules on the endothelial
cells106 as well as expression of inflammatory
cytokines105 leads to recruitment of bone marrow-
derived cells and differentiation of collateral artery
smooth muscle cells to a synthetic phenotype.106 The
next ‘growth’ phase of arteriogenesis result in luminal
expansion. This is accomplished by a degradation of the
basal membrane,106,107 and outward migration and
proliferation of the vascular cells triggered by a number
of signaling pathways involving both growth factors108
and paracrine signaling from recruited bone marrow-
derived cells.109 As luminal diameter increases, shear
stress decreases, and expression of inflammatory
cytokines decreases.105 In this ‘maturation’ phase,
collateral vessels can either mature and stabilize or
undergo neointimal hyperplasia and regression. The fate
of the vessel is probably determined by the
hemodynamic forces, that is, the largest and most
developed vessels will stabilize and the smaller and less
developed vessels will regress.110
A number of cell populations from the bone marrow play
a role in arteriogenesis. These participate in a
temporally coordinated process in the different phases
of arteriogenesis. Neutrophil leukocytes are the first
cells to infiltrate the vessel during the initial phase
(within a few hours) through binding to the adhesion
molecules expressed by the endothelial cells, but the
neutrophils are only present in the first few days of the
process.111 The neutrophils seem to recruite
inflammatory monocytes to the growing vessel112
perhaps mediated by VEGF-A release. The monocyte has
a paramount role in arteriogenesis113 and accumulates in
the vessel shortly after the neutrophil recruitment106
that is, in the growth phase of arteriogenesis. Depletion
of macrophages seems to eliminate flow-induced
remodeling of the vessel in mice.114 The origin of the
inflammatory cells involved in arteriogenesis remains
controversial. An experiment in rats could indicate that
inflammatory leukocytes and monocytes/macrophages
at least in the first days of the process comes from
proliferation of tissue resident cells rather than from the
circulation.115

- 13 -
Bone marrow-derived stem- and progenitor cells
This paragraph aims to give a brief overview of the bone
marrow-derived cells potentially involved in cardiac cell-
based therapy. Three cell populations from the bone
marrow are typically described in cardiac cell based
therapies: the hematopoietic stem/progenitor cells, the
endothelial progenitor cells (EPC), and the multipotent
mesenchymal stromal cells (MSC). Irrespective of the
cell type, several potential mechanisms of cell based
therapies can be hypothesized. These mechanisms can
be both direct by incorporation and differentiation of the
cells into cardiac or/and vascular cells, or indirect by
secretion of paracrine factors, cytoprotection, or
immunomodulatory effects (page 15). The main source
of progenitor cells is thought to be the bone marrow,
but cells from other tissues like fat most likely also
contribute.116,117 A number of resident cardiac
stem/progenitor cell has been identified and also appear
involved in cardiac myogenesis (review in 118). These
cells will not be described further in this overview.
Hematopoietic stem/progenitor cells is multipotent cells
that can differentiate into all the blood cell types, both
in the myeloid and the lymphoid cell lineage and has
unlimited capacity of self-renewal. Numerous studies of
bone marrow transplantation in hematological patients
have documented the possibility of restoration of bone
marrow and hematopoietic function119; however the
precise phenotype and characteristic of the
hematopoietic stem cells remain debated.
Hematopoietic stem cells have been isolated from bone
marrow and peripheral blood as cells expressing CD34
and/or CD133. The number of cells expressing CD34
predicts hematopoietic recovery after blood stem cell
transplantation120 and are thus used to assess the
numbers of peripheral blood hematopoietic
progenitor/stem cells in the clinic.
The interest in myocyte-differentiation potential of the
hematopoietic stem cells was motivated by the still
controversial publication in Nature by P. Anversas
group.4 The authors found that transplantation of
hematopoietic stem cells into infarcted mice hearts led
to myocardial regeneration apparently through
transdifferentiation of hematopoietic stem cells to
functional myocytes. These results were later
reproduced by the same group30,121, whereas other
groups could not.5,6,122
Endothelial progenitor cells are found in the bone
marrow and in peripheral blood. There has been and is a
continued debate over the phenotype and functional
characteristics of EPC.
The term EPC has typically been cells in the blood or the
bone marrow co-expressing a hematopoietic (CD34,
CD133) and endothelial markers (e.g. VEGFR, CD31,
Tie-2). However, this phenotype is not exclusive to EPC.
Another approach to EPC isolation is to plate peripheral
blood mononuclear cells to give rise to colonies. This
result in two cell populations: the ‘early outgrowth EPC’
(also called proangiogenic haematopoietic cells) and the
extremely rare ‘late outgrowth EPC’ (also called
endothelial colony-forming cells).123 The late outgrowth
cells have rapid proliferation and seem to include true
stem/progenitor cells. They are reported to have a
CD34+CD45- phenotype and express VEGFR2 but not
CD133 or CD14.124 The majority of published studies of
EPC have used early outgrowth EPC.
The number of circulating EPC following acute
myocardial ischemia increases31,125 whereas patients
with 3-vessel disease undergoing diagnostic cardiac
catheterization have low numbers of circulating EPC.126
Several drugs used in patients with myocardial ischemia
increases the concentration of EPC in the blood e.g.
ACE-inhibitors and statins.127,128
Circulating putative EPC were first isolated by Asahara
et al. 3 who cultured cells expressing CD34 or VEGFR2.
The cells differentiated into a endothelial-like phenotype
and incorporated into areas with vasculogenesis/
angiogenesis where the cells appeared integrated into
the capillary wall.3 Shi et al. found in a similar study
that a subset of CD34+ cells could differentiate into
endothelial cells in vitro in the presence of FGF, insulin-
like growth factor 1, and VEGF-A.129
The mechanism of EPC contribution to adult
angiogenesis and arteriogenesis is not clarified but the
prevailing belief is a paracrine rather than a direct
incorporation and differentiation of the cells (page 15).
This is supported by their capability of releasing
angiogenic growth factors including VEGF-A, SDF-1, and
insulin-like growth factor 1.130
Transdifferentiation of EPC into cardiomyocytes has
been reported by the group of S. Dimmeler,131,132
however, like in the case of hematopoietic stem cells
these results have been difficult to reproduce by
others.133

- 14 -
Multipotent Mesenchymal stromal cells: Nearly 40 years
ago Friedenstien et al. described that fibroblast-like
(stromal) cells from the bone marrow were capable of
reconstituting the hematopoietic microenvironment at
ectopic sites.134 Later, research identified the
multipotent bone marrow stromal cells (MSC) that can
differentiate into mesodermal cell lines. The group of
Verfaillie has even described a pluripotent cell-type
(termed multipotent adult progenitor cells (MAPC))
purified from the bone marrow.135,136 Noteworthy
though, evidence for pluripotency of MAPC has been
difficult to reproduce by others.
MSC is often isolated from the bone marrow, but has
been identified in a number of tissues, including fetal
and umbilical blood, lung, liver, kidney and adipose
tissue.137 It has recently been shown that pericytes138
(cells surrounding epithelial cells in capillaries and
microvessels) and cells residing in the tunica
adventitia139 share antigenic markers and behave
similarly to MSC in culture. It has thus been proposed
that the natural MSC niche is perivascular both within
bone marrow and other tissues.139
Both the defining characteristics and the isolation
procedure of MSC differ among investigators due to a
lack of simple sensitive and specific markers. MSC is
often isolated by plastic adherence and a fibroblastic
appearance. Flow cytometry is an easy approach for cell
phenotyping based on cell-surface antigens.
Unfortunately, no sensitive and specific marker-set of
MSC has been found – in contrary a huge list of markers
expressed or not-expressed by MSC isolated by different
groups from different tissues exist140 making
comparisons of published results difficult. In addition,
often MSC phenotypes are described after in vitro
culture and little is known about the in vivo phenotype.
To complex matters more, the nomenclature is
ambiguous. Terms like colony forming units fibroblasts,
mesenchymal stem cells, marrow stromal cells,
mesenchymal progenitor cells, mesodermal progenitor
cells, skeletal stem cells, multipotent mononuclear stem
cell, non-hematopoietic stem cell, and multipotent adult
progenitor cell probably name the same cell population
(at least to some extent).
The International Society for Cellular Therapy
recommended in 2005/2006 ‘multipotent mesenchymal
stromal cell’ (MSC) as the designation for plastic-
adherent cells isolated from bone marrow and other
tissues. The following three minimal criteria for defining
MSC were suggested: (1) plastic-adherent when
maintained in standard culture conditions, (2) Specific
surface phenotype (must express CD105, CD73, CD90
and must lack expression of CD45, CD34, CD14 or
CD11b, CD79α or CD19, HLA-DR), and (3) In vitro
differentiation into osteoblasts, adipocytes and
chondroblasts.141,142
MSC has been shown to differentiate into both
endothelial cells143,144, vascular smooth muscle cells145
and cardiomyocytes146,147. However, another study
indicate that MSC cannot acquire a mature
cardiomyocyte phenotype.148 MSC has been shown to
express anti-apoptotic, angio- and arteriogenic factors
like interleukin 6, VEGF-A, leukemia inhibitory factor,
and matrix metalloproteinase 2.149 Enzyme-linked
immunosorbent assay of MSC medium contained
secreted VEGF-A, insulin-like growth factor 1,
hepatocyte growth factor, adrenomedullin, placental
growth factor and interleukin 6.149,150 These
characteristics of MSC could indicate both a potential
direct (by cell engraftment and differentiation) and
indirect (by paracrine) effect.
MSC are reported to express a number of functional
chemokine receptors151 allowing for their migration in
response to chemokine gradients in damaged tissue.
However, some controversy exist e.g. over the
expression of the CXCR4 receptor.152 Myokardial
infarctions, bone fractures, and renal injury are
examples where transplanted MSC has been shown to
home to the damages area.153-155 Passage of the
endothelial barrier is essential for tissue homing of
circulating cells. MSCs has been shown in vitro to
interact by P-selectin and VCAM-1/β1-integrin with
endothelial cells under shear flow, thus allowing egress
from the bloodstream.156 The SDF-1/CXCR4 signaling
axis is a strong candidate for MSC migration155,157,158
although one recent study could not show an effect of
CXCR4 inhibition on MSC migration to ischemic tissue159
and another study indicate that ‘monocyte chemotactic
protein 3’ is an important MSC homing factor.160
Numerous studies have described a positive effect of
MSC therapy on ischemic tissue (e.g. increased capillary
density in infracted area161 or reduce scar formation
after myocardial infarction.162-164). The majority of
engraftment studies show, that only a small fraction of
intravenous MSC engraft, and of these, only a small
fraction differentiates.165 A growing number of studies
support the hypothesis that the benefit of MSC

- 15 -
transplantation comes from release of paracrine
molecules.109,166 These effects could potentially be
angiogenic, anti-apoptotic, anti-inflammatory or perhaps
through a paracrine effect on resident cardiac stem
cells.
Peripheral blood multipotent mesenchymal stromal cell
(PBMSC): The existence of MSC in the peripheral blood
under homeostatic conditions remains controversial. It
is also unclear where PBMSC originates and where they
go. As with bone marrow-derived MSC, terminology and
isolation procedures differ among investigators (review
in 167), this may contribute to the mixed results
regarding PBMSC. PBMSC are often isolated as
adherent, clonogenic, and fibroblast-like and thus also
termed colony-forming units-fibroblastic (CFU-F). CFU-F
from peripheral blood (typically following G-CSF
treatment) has been claimed identified by several
groups.168-170 The frequency of CFU-F from peripheral
blood varies widely among studies but is low (or even
absent171,172) compared to the frequency in bone
marrow-derived mononuclear cells.167 A trial by Kassis
et al. comparing isolation of PBMSC by plastic adherence
with fibrin microbeads-based isolation could indicate
that a suboptimal isolation procedure enhances the low
yield of PBMSC in many trials.173
The immunophenotype of CFU-F from peripheral blood
share many similarities with bone marrow-derived-MSC
but also some differences. They lack CD34, CD45, and
HLA-DR and express CD90 and CD106 as bone marrow-
derived MSC do. In contrary to marrow-derived MSC,
CD133 has been reported expressed169, and CD105 are
not always expressed168. These differences open the
question if PBMSC are bone marrow-derived MSC
mobilized to the blood or a distinct cell population.
Potential mechanisms of cell-based therapy
Improved myocardial function after cell based therapies
was initially ascribed vascular and/or myocardial
regeneration by a direct action of transplanted cells
through myogenesis and/or vasculogenesis. Different
lines of stem- and progenitor cells were repeatedly
demonstrated to differentiate into endothelial cells,
vascular smooth muscle cells and myocytes.4,145,174,175
However, an increasing number of studies have shown a
remarkable lack of sustained engraftment and
differentiation of the transplanted cells.165 Another
observation is the absent correlation between the
number of transplanted cells and functional
improvement. These observations have led to the
hypothesis that the improved function after cell therapy
may – at least in part – be caused by secretion of
paracrine factors rather than differentiation. Potential
paracrine effects could be neovascularization
(potentially vasculogenesis, angiogenesis and
arteriogenesis), improved remodeling and contractility
as well as myocardial protection and/or cardiac
regeneration by resident cells. The importance of
neovascularization was confirmed by Yoon et al who
demonstrated in a very elegant design that vascular
differentiation (endothelial and smooth muscle lineage
commitment) of bone marrow-derived mononuclear cells
is critical in left ventricular recovery following acute
myocardial infarction.176 Elimination of cardiac-
committed cells in the same study did not affect ejection
fraction.
A growing body of evidence for the paracrine hypothesis
exist (review in 177). Some of the most notably studies
have shown that conditioned medium from
stem/progenitor cells can reproduce the functional
results observed after cell transplantation.178-181 Shabbir
et al.182 found in an unusual setup, that injection of MSC
into skeletal muscle improved cardiac function although
the transplanted cell appeared to be trapped in the
skeletal muscle. The authors found evidence that MSC-
derived interleukin 6 activated skeletal muscle-cell
Jak/STAT3 pathway. Skeletal muscle then increased
expression of VEGF-A and hepatocyte growth factor that
supposedly had a positive effect on heart failure. This
study could indicate a very complex cascade from
transplanted cell to target organ involving several cell-
types and trophic factors.
The paracrine mechanism opens the opportunity for
protein-based rather than cell-based therapy once the
paracrine factors are identified. However, the temporal
and spatiel co-operation between several beneficial
factors could be so complex that a cell-based strategy
would still be most optimal.

- 16 -
Aim and hypothesis
With this background it has been the aim of this
translational programme to establish and evaluate cell
based therapies using G-CSF as a treatment modality
for patients with ischemic heart disease. It has been our
hypothesis that clinical effective cardiac regeneration
requires cellular components and exogeneous/
endogeneous modulating molecules in symphoni.
Therefore, we
• Evaluated safety and effects of combined treatment
with G-CSF and VEGF-A-gene therapy in patients
with chronic ischemic heart disease.I
• Investigated if inherent differences in patients could
serve as markers for selecting patients for gene- or
cell-therapy.II,III
• Evaluated the clinical effect and safety of treatment
with G-CSF following STEMIIV and reasons for failed
effect of G-CSF.V
• Determined the recovery in left ventricular function
and morphology after current guideline treatment of
STEMI.VI
• Evaluated a method for intramyocardial in vivo cell
tracking.VII
This review will aim at presenting the implications and
conclusions of our studies in relation to other
investigations.
TRIAL DESIGN Measures of efficacy
The optimal and conclusive efficacy endpoint in a
cardiovascular trial is allcause mortality or perhaps
morbidity. However, this would require a huge patient
population which is neither ethically nor economically
justifiable for neovascularization trials at present. One
key issue in our trial designs has thus been to find the
best surrogate endpoint available.
For patients with stable chronic ischemia, one approach
is the patient’s subjective assessment of symptoms and
wellbeing since we would expect only minor changes in
the disease without new intervention. For some patients
with chronic disease this endpoint may be more
important than prolongation of life.183 However, this
evaluation of ‘quality of life’ will require a strict control
for the substantial placebo-effect instituted by our
invasive treatment and by the close follow-up of our
tendering study nurses.
To diminish the significance of influence from the
placebo effect, a number of more objective measures of
cardiac function and perfusion can be considered.
Myocardial volumes and function
Myocardial function and left ventricular volumes are
traditionally assessed using echocardiography, but also
ventriculography, SPECT, positron emission tomography
(PET), computed tomography (CT), and MRI can be
used.184 Most often, myocardial function is assessed at
rest, but it can be visualized during pharmacological or
even physiological stress. Change in left ventricular
ejection fraction is often used as primary endpoint. This
seems reasonable since ejection fraction has been
shown to predict mortality.185 However, ejection fraction
at rest can be preserved despite large infarctions due to
hypercontractility of non-infarcted myocardium.186
Regional function may be more informative and the wall
motion score index has been found to be superior to
ejection fraction in predicting prognosis following
myocardial infarction.187
2D echocardiography is widely used in clinical practice
and research because it is fast, easily accessible, and
contains no radiation exposure but is also dependent on
the operator and the acoustic window. In addition,
quantification of left ventricular volumes rely on some
geometric assumptions that are not always met
especially in ischemic cardiomyopathy.188 These
limitations result in an only moderate accuracy (median
limits of agreement from ±16 to ±19%) when compared
to radionuclide or contrast ventriculography.189
ECG gated SPECT allows assessment of left ventricular
volumes190 using an automated 3-D reconstruction of
the ventricle and the method has a good
reproducibility.191 The primary drawbacks are the use of
ionizing tracers, the long acquisition time and the low
temporal resolution. In addition, low spatial resolution
limits the assessment of regional wall motion.
At present, most investigators consider MRI as the gold
standard for assessing global and regional left
ventricular function due to high accuracy and
reproducibility combined with high spatial resolution.
The advantages of MRI for functional evaluation
compared to other imaging techniques are its non-
invasiveness, the use of non-ionizing radiation,
independence of geometrical assumptions and acoustical
windows, and no need of contrast media. The primary
drawbacks are low (but improving) temporal resolution,
and low accessibility. The examination of patients with

- 17 -
tachycardia, especially irregular, (e.g. atrial fibrillation)
or implanted ferromagnetic devices such as implantable
cardioverter-defibrillator and pacemaker is problematic
or impossible. Furthermore, MRI scanners may cause
claustrophobia in many patients. The STEMMI trialIV
included 78 patients and MRI was not feasible in 20
patients (25%) primarily due to claustrophobia. This is
more than usually expected, but the patients were
psychologically fragile due to the very recent STEMI.
Another recent MRI trial early after acute myocardial
infarction showed an even higher drop-out rate.53
The cinematographic MRI technique used for the
measurements of cardiac volumes also poses problems.
Image information for each frame in a given position is
sampled over a number of consecutive heart cycles (15
in our trials) within a set time-window (50 ms in our
trials); the process is termed segmented k-space
sampling. This temporal resolution can 1) cause
problems in defining the frame with endsystolic phase,
2) cause blurring of the endo- and epicardial borders
since the myocardium is contracting in the 50 ms time
window, and 3) the required breath-hold during the 15
heart cycles can be difficult for the patients.
Furthermore, only one short axis slice could be obtained
within a single breath-hold (in end-expiration) with our
equipment. Thus, if the point of end-expiration varies
from slice to slice, this affects the position of the
diaphragm, resulting in non-consecutive slices.
Partial volume effect can be a problem near the base
and apex, since each slice has a thickness (8 mm in our
trials). This may result in imprecise border definitions.
Despite these problems several studies have reported
high accuracy192-194 and reproducibility195,196 in
determining left ventricular volumes and thus function.
Still, echocardiography will fulfill the clinician’s needs in
the vast majority of cases, whereas MRI is a
sophisticated alternative primarily indicated for research
purposes.
Myocardial perfusion
Regional myocardial perfusion is another important
endpoint in trials of cardiac neovascularization since
these therapies are hypothesized to induce capillaries
and small arterioles not visible by coronary angiography.
Gamma camera imaging and PET have been used for
perfusion assessment for more than a decade and more
recently CT, contrast echocardiography and MRI197 have
advanced within this field. Perfusion can be visualized
during both rest and stress (pharmacological or
physical).
SPECT is probably the most available clinical method for
perfusion assessment. The myocardial uptake of the
radioactive tracers’ thallium 201 and technetium 99m
labeled sestamibi/tetrofosmin is proportional to the
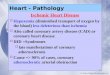
Figure 1. Example of MRI perfusion scan in one patient with infero-lateral ischemia treated with VEGF-A165 gene transfer followed by G-CSF. A: Time versus signal intensity curves showing the fast initial contrast input into the cavity of the left ventricle and subsequent contrast enhancement in the myocardium. B: Baseline and follow-up examination. Images from 20 sec after contrast infusion, demonstrating poor perfusion with no contrast enhancement in the lateral wall (black arrows), moderate perfusion with attenuated enhancement (white arrows) in the inferior wall, and normal perfusion in the anterior wall (transparent arrows). (Adapted from Ripa et al. Eur Heart J 2006 by permission of Oxford University Press)

- 18 -
blood flow. The method is limited by high ionizing
radiation, low spatial resolution (aprox. 10 mm with our
equipment) and frequent image artifacts. In comparison
PET has better spatial resolution (6-10 mm) but is still
insufficient to detect minor subendocardial defects. With
PET absolute perfusion can be quantified by dynamic
imaging of radioactive isotopes as they pass through the
cardiovascular system. PET is less prone to attenuation
artifacts than SPECT since accurate attenuation
correction can be done. However, PET is expensive and
has low accessibility.
CT and contrast echocardiography is emerging as
modalities for perfusion assessments. The great
advantage is the high spatial resolution (<1 mm) but
more validation and optimization of the methods
remains.
MRI can quantify the myocardial perfusion by dynamic
imaging of the first pass of a paramagnetic (non-
ionizing) contrast agent through the heart (Figure 1).197-
200 The modality has an acceptable spatial (2-3 mm) and
temporal (0.5-1.0 s) resolution, but is not widely
validated and it is cumbersome to assess the absolute
perfusion using this method. The method is further
limited by recent accumulating evidence that MRI
contrast media containing gadolinium (especially
gadodiamide) can cause irreversible nephrogenic
systemic fibrosis in patients with renal insufficiency.201
To date, nephrogenic systemic fibrosis has only been
reported in patients with severe renal impairment.
Conclusion
There are several surrogate endpoints and methods with
clinical relevance for neovascularization trials. PET offers
accurate measure of perfusion and left ventricular
volume during stress and rest with higher spatial
resolution than SPECT. Echocardiography is very
accessible and has excellent temporal resolution for
volume assessment. The MRI technology offers a range
of high-quality endpoints with very high spatial
resolution within a single examination without a need for
radiation. In the design of each trial it remains
important to choose the primary endpoint with most
clinical relevance.
Ethical considerations in trial design
Treatment with gene or cell therapy is a new area of
research warranting for caution in study design. The
primary concern is and must be the safety of the
treatment and the secondary concern is the efficacy of
the treatment. This is not different from traditional
drug-trials, but this being a new treatment modality
should probably demand for an even higher bar of
safety than usually required. The real question is how to
gain this knowledge or assumption of safety? Ultimately,
we need large double-blinded and randomized patient
groups followed for a long period of time. Obviously, this
is not possible or even ethical with a new treatment
modality where we need to base our initial safety
assumption in theoretical knowledge of the treatment
(what side effects do we expect knowing the potential
effect of the treatment?), early animal trials, early
phase clinical trials with few (perhaps healthy)
individuals, and the gradual increase in patient number
if the treatment still seems safe and effective. In the
ethical consideration, it is also important to account for
the morbidity of the patients before inclusion. Very ill
patients with poor prognosis and without any treatment
options will probably accept higher risk than patients
with a more benign disease.
The trials included in this thesis have primarily focused
on treatment with one pharmacon (G-CSF) in patients
with either severe chronic myocardial ischemiaI or
following acute myocardial infarctionIV. G-CSF is a
registered drug (page 10) used for years in healthy
donors and patients with hematological diseases. The
drug is generally well tolerated with few and mild side
effects. However, the drug was not formally tested in
patients with ischemic heart disease. At the time of the
trial design there was increasing evidence from animal
and small clinical trials that autologous bone-marrow
derived cells (mononuclear cells) led to improved
myocardial function via neovascularization and perhaps
myogenesis.2,4,36,42,46,202-204 It was believed that
hematopoietic stem or progenitor cells were the ‘active
substance’.174,205,206 Mobilization of cells from the bone
marrow seemed like an attractive alternative to
intracoronary or intramyocardial injection that would not
require bone marrow aspiration or cardiac
catheterization. G-CSF was known to mobilize
hematopoietic cells from the bone marrow into the
circulation (page 10). Animal studies had shown that
circulating stem and progenitor cells are attracted to
ischemic myocardium and incorporates into the
formation of new blood vessels.36,92 On this background
Orlic et al207 injected mice with recombinant rat stem
cell factor and recombinant human G-CSF to mobilize

- 19 -
stem cells for 5 days, then ligated the coronary artery,
and continued the treatment with stem cell factor and
G-CSF for 3 days. Afterwards, the ejection fraction
progressively improved as a consequence of the
formation of new myocytes with arterioles and
capillaries.207
Our initial studies with G-CSF included patients with
severe chronic ischemic heart disease208,I since we found
more evidence that bone marrow derived cells would
promote neovascularization, than neogeneration of
myocytes. We thus hypothesized that patients with
severe chronic ischemia would potentially benefit more
from the treatment compared to patients with acute
myocardial infarction or heart failure. In addition, the
clinical experience with G-CSF to patients with ischemic
heart disease was at that time limited. Despite good
long term safety results from hematology, we initially
included patients only with severe morbidity without any
options for further conventional treatment. All patients
included went through a strict screening procedure
including a renewed evaluation by independent
cardiologists and thoracic surgeons to ensure that no
conventional treatment was possible.
Later, accumulating evidence31,37,44,45,209,210 of both
safety and efficacy of G-CSF lead us to initiate a trial
with G-CSF to patients with STEMI.IV,211
G-CSF FOR CHRONIC ISCHEMIA Hill et al212 and our group208 have treated patients with
chronic myocardial ischemia due to stable severe
occlusive coronary artery disease with G-CSF to induce
myocardial vasculogenesis and angiogenesis. Both trials
were small, non-randomized safety trials with few
patients (n=16 and n=13). Three other trials have
included patients with intractable angina to treatment
with G-CSF and subsequent leukopheresis and
intracoronary cell infusion.213-215
Hill et al212 showed no change in left ventricular ejection
fraction, in resting or dobutamine stressed left
ventricular wall motion or perfusion measured by MRI,
nor in treadmill exercise test despite a huge increase in
hematopoietic progenitor cells (CD34+ and
CD34+/CD133+ cells).
We showed a similar increase in CD34+ cells in the blood
following G-CSF treatment.208 The perfusion defects at
rest and stress assessed with SPECT demonstrated
unchanged number of segments from baseline to 2
months follow-up. This was confirmed with MRI where
myocardial perfusion during pharmacological stress was
unchanged in the ischemic myocardium from baseline to
follow-up. Left ventricular ejection fraction decreased
from baseline to follow-up measured with MRI (from
57±12 to 52±11, p=0.01), and the trend was the same
with SPECT (from 48±10 to 44±12, p=0.09), whereas
the ejection fraction was unchanged by
echocardiographic evaluation. This finding could indicate
an adverse effect of G-CSF on the myocardium, maybe
by an inflammatory response in the microcirculation by
the mobilized leucocytes and subsequent development
of myocardial fibrosis.
The change in subjective clinical outcomes were more
positive, CCS class improved from 2.7±0.6 to 1.7±0.6
(p=0.01), nitroglycerin consumption from 1.5±2.1 to
0.5±1.2 per day (p<0.05), and number of angina
pectoris attacks per day from 1.7±1.7 to 1.0±1.6
(p<0.05).208 The interpretation of these subjective
measures is not easy. On one hand this endpoint is
most important for the patient (who does not care about
improvement in SPECT); on the other hand this is a
non-randomized study with only historical controls
making placebo effect a potential confounder. However,
the clinical improvement seems restricted to patients
with a pronounced mobilization into the peripheral
circulating of CD34+ stem suggesting a causal
relationship.208 It can be speculated if the treatment
with G-CSF led to deterioration of perfusion and thus
infarction of previously ischemic myocardium, this might
explain the deterioration in ejection fraction and the
diminished symptoms of ischemia.
G-CSF and VEGF-A gene therapy
G-CSF therapy increased the vascular supply of bone
marrow-derived cells to the myocardium but did not
improve myocardial perfusion and function.208,212 We
hypothesized that this could be caused by a lack of
signals from the myocardium to engraft the cells into
the ischemic myocardium. VEGF-A165 has been
demonstrated to be of importance for the differentiation
of stem cells into endothelial cells participating in the
vasculogenesis93 and is also important in the homing of
cells to ischemic areas (page 23). Animal studies further
suggest that a combination of treatment with VEGF-A
gene transfer followed by G-CSF mobilization of stem
cells might be superior to either of the therapies.216,217

- 20 -
Figure 4. Changes in angina pectoris in patients treated with placebo, plasmid VEGF-A165 or plasmid VEGF-A165 and G-CSF. I
On this background, we performed a clinical study to
evaluate the safety and clinical effect of VEGF-A165 gene
transfer followed by bone marrow stimulation with G-
CSF in patients with severe occlusive coronary artery
disease.I Sixteen patients were treated with direct
intramyocardial injections of the VEGF-A165 plasmid
followed 1 week later by subcutaneous injection of G-
CSF for 6 days. Two historic control groups from the
Euroinject trial27 were included in the study: 16 patients
treated with VEGF-A gene transfer alone and 16 patients
treated with blinded placebo gene injections. The
treatment was well tolerated and seemed safe with no
serious adverse events during the combined VEGF-A165
gene and G-CSF treatment or in the follow-up period.I
Also we had no serious procedural events during
intramyocardial injection of the VEGF-A165 gene in these
16 patients. However, it is known that NOGA mapping
and injection is not a risk free procedure. Five patients
(6%) in the Euroinject One Trial had serious procedure-
related complications, two of these were at our
institution.27 Similar events following the NOGA
procedure has been reported by others.59 It is our
impression that most of these events can be avoided
with increased experience by the staff. Approximately
100 NOGA procedures have been performed at our
institution without any serious events since the two
described events (J. Kastrup, personal communication).
We have also detected significant (but usually only
minor) release of cardiac markers (CKMB and troponin
T) following the NOGA procedure.218
The treatments lead to a significant increase in
circulating CD34+ cells as expected after the G-CSF
treatment (Figure 2).219,220 The prespecified primary
efficacy endpoint of change in perfusion defects at
stress SPECT came out neutral after 3 months follow-up
(Figure 3), this result was confirmed with MRI
measurement of myocardial perfusion during adenosine
stress (baseline 62%±32 to 74%±32 at follow-up,
p=0.16).I In addition, there was no significant difference
in changes in CCS classification, angina pectoris attacks,
nitroglycerin consumption, or exercise time between the
three groups (Figure 4). In opposition to the trial with
G-CSF as monotherapy208, there was no deterioration in
resting left ventricular ejection fraction after G-CSF
treatment neither with MRI nor with SPECT.I This trial
has several limitations, and primarily it must be
considered if this trial was underpowered to detect a
difference especially since we included few patients with
short follow-up period into an open-label design with
only historical controls. Furthermore, we were unable to
Figure 2. Circulating CD34+ cells from baseline to day 28 after different treatment strategies. (Adapted from Wang et al. Scand Cardiovasc J 2007 with permission from Taylor & Francis)
Figure 3. Myocardial perfusion at rest and stress measured by SPECT after treatment with VEGF gene therapy and subsequent bone marrow cell mobilization with G-CSF.(I)

- 21 -
analyze all patients for all endpoints due to technical
difficulties and in some instances poor image quality. In
favour of our results are the facts that multiple
endpoints using different methods consistently have
shown virtually identical results from baseline to follow-
up. In conclusion, we found no indication of clinical
effects or improved myocardial function following
combined treatment with VEGF-A165 gene transfer and
G-CSF.
Of interest, a trial (clinicaltrials.gov, NCT NCT00747708)
is currently being conducted in patients with congestive
heart failure secondary to ischemic heart disease. The
investigators aim to include 165 patients into several
treatment arms to investigate G-CSF alone or in
combination with intracoronary/intramyocardial cell
injections.
Safety of G-CSF to patients with chronic ischemia
Our group has treated a total of 29 patients with severe
chronic myocardial ischemia with G-CSF without any
serious vascular adverse events. Serious vascular
adverse events have been reported in two patients
(13%) by Hill et al212 and one patient (20%) by Boyle et
al213. In a rigorous trial by Kovacic et al214 4 patients
(20%) had episodes of cardiac ischemia with elevated
troponin I and either ECG changes or elevated CKMB, in
addition troponins were elevated in 17 other occasions
but without ECG changes or elevated CKMB after G-CSF.
The patients described the episodes as typical for their
usual angina pattern. The authors speculate if these
troponin elevations reflect the natural history of
refractory angina, or the G-CSF treatment, since the
trial was not placebo controlled.213
Patients with multi-vessel chronic ischemic heart disease
are potentially susceptible to the G-CSF-induced
increase in leukocyte numbers and inflammation via
plaque destabilization or growth. However, a study of
cholesterol fed swine suggests that the administration of
G-CSF causes neither exacerbation nor modification of
atherosclerotic lesions.221
The few and small trials do not permit us to draw any
meaningful conclusions regarding the safety of G-CSF
treatment to chronic ischemic heart disease.
Clarification of safety needs studies of more patients
with longer follow-up, and preferably the inclusion of a
control group.
Does G-CSF reduce myocardial ischemia?
No convincing effect of G-CSF has been described in
patient with chronic ischemia.208,212,I There have been
indications of improved subjective measures of efficacy
in several trials but objective measures of myocardial
perfusion and ischemia were unchanged. We cannot
exclude the possibility that the trials have been
underpowered and/or endpoint assessment to poor to
find a statistical significant difference. The GAIN II trial
included 18 patients with chronic ischemic heart disease
into a randomized placebo-controlled double-blinded
crossover trial of G-CSF using a more accurate primary
endpoint (myocardial perfusion by MRI) than SPECT.
The trial was presented at ACC 2010222, but remains
unpublished. The authors found no effect of G-CSF on
the primary endpoint.
Several explanations to the apparent lack of effect of G-
CSF in this clinical setting can be suggested.
Angiogenesis or arteriogenesis
Our pretrial hypothesis was that G-CSF and VEGF-A
gene therapy would increase angiogenesis in reversible
ischemic myocardium by engraftment and differentiation
of bone marrow-derived cells. We chose G-CSF since it
was a known mobilizer of progenitor/stem cells from the
bone marrow, and VEGF-A because it was a major
contributor in cell homing (page 23) and angiogenesis
(page 11). Further, we included patients with at least
one open epicardial artery to the ischemic area since
angiogenesis without epicardial blood supply will
probably be of little effect. Retrospectively, it is plausible
that increasing the number of circulating cells and the
tissue expression of VEGF-A is simply ‘to easy’ despite
earlier encouraging results. Both vasculogenesis and
angiogenesis involve a complex cascade of several cells
types and numerous soluble factors – VEGF-A being just
one important player.
It should also be considered if arteriogenesis rather that
angiogenesis should be the primary aim of
neovascularization. Despite an open epicardial artery,
blood flow to the capillaries may still be compromised
and arteriogenesis would result in large caliber
conductance arteries that could more effectively restore
blood flow to ischemic myocardium. Recent evidence
from a clinical trial of patients with chronic stable
coronary artery disease suggest that G-CSF has the
capacity to promote coronary collateral growth.223 Fifty-
two patients were randomized to a two week period with

- 22 -
G-CSF or placebo every other day. Both ECG signs of
ischemia and collateral flow index in a stenotic coronary
artery during balloon occlusion improved after G-CSF
indicating an improved collateral function.
Patient population
It can be speculated whether angiogenic mechanisms to
improve blood supply to the ischemic heart are already
activated in patients with severe chronic myocardial
ischemia, leaving little therapeutic effect for exogenous
angiogenic therapy.
We investigated the plasma concentration of factors
known to influence angiogenesis, cell mobilization and
homing as well as putative stem/progenitor cells in 54
patients with severe chronic ischemia and 15 healthy
controls.II Surprisingly, we found that, in general,
circulating stem/progenitor cells and plasma
concentrations of angiogenic related cytokines were not
significantly different from the control group (Table 1).
This result could be influenced by the fact that plasma
concentrations of the cytokines are perhaps a poor
indicator of the concentrations within the myocardium. A
more precise measurement would require cardiac
catheterizations of the patients, which is not clinically
applicable for patient stratification, and furthermore the
procedure could potentially influence the cytokine
concentrations as has been shown for pro-b-type
natriuretic peptide.224 In addition, measuring plasma
VEGF-A is potentially influenced by release from the
platelets during collection and processing of the blood.
We have standardized the procedures to diminish this
source of error but cannot exclude that this could
explain some of the large inter-patient variations
observed. However, our results are supported by our
finding of unaffected VEGF-A mRNA contents in chronic
ischemic myocardial tissue compared to normally
perfused myocardium.225
We assessed the number of peripheral blood MSC in
patients and control subjects using flowcytometry
identification of circulating mononuclear cells negative
for both the endothelial marker CD34 and the pan-
leukocyte marker CD45.II This identification procedure
has low specificity for MSC since we did not include any
positive marker (like CD105, CD73 and CD90), thus our
nomenclature in the paper was imprecise since the
whole population of CD45-/CD34- cells should not be
referred to as putative stem cells (Page 15). Our
reasons for focusing on the population of CD45-/CD34-
circulating cells were several. First, at the time of
analyses of the blood no consensus on which surface
markers that determined MSC existed. In contrary,
different surface markers on MSC where described in an
increasing number of publications (Page 15). Second,
very few had published results regarding surface
markers identifying PBMSC168. And third, we had
identified cells within a population of CD45-/CD34- cells
with a mesenchymal-like phenotype after culture.32 We
decided on this basis to focus our attention on the CD45-
/CD34- cells knowing that this would result in an
unspecific identification of MSC. We feared that
including positive surface markers in the identification
process would exclude some of the MSC, since we could
find only little consistency regarding surface markers of
PBMSC in the literature. We did include a number of
surface-markers in the sub classification of the CD45-
/CD34- cells. These were chosen from the literature to
include both markers often reported to be expressed by
bone marrow-derived MSC (CD105, CD73, CD166),140,226
markers found on endothelial cells (CD31, CD144,
VEGFR2)140 and a marker expressed by hematopoietic
progenitor cells that has also been found on PBMSC, but
not in bone marrow-derived MSC (CD133)140,169. We
Table 1. Circulating cell and cytokine concentrations in patients with chronic myocardial ischemia and control subjects.
Patients (n=54) Control subjects (n=15) p-value
VEGF-A (10-12*g/ml) 35.0 (18.6-51.4) 91.7 (8.2-175.1) 0.4 FGF-2 (10-12*g/ml) 9.0 (6.2-11.7) 11.3 (2.2-20.3) 0.7 SDF-1 (10-10*g/ml) 22.48
(21.24-23.72) 20.14
(17.50-22.79) 0.2
CD34+ (103/ml) 2.8 (2.4-3.3) 3.0 (2.1-3.9) 0.6 CD45-/CD34- (104/ml) 20.8 (17.0-24.6) 21.9 (13.0-31.0) 0.8 Values are mean (95% confidence interval)

- 23 -
observed that the fraction of CD45-/CD34- cells co-
expressing surface markers expressed by bone marrow-
derived MSC (CD 105 and CD 166) and endothelial cell
markers (CD31, CD144, VEGFR) were higher in ischemic
patients compared to controls (Figure 5)II indicating that
ischemia mobilizes both endothelial committed cells and
more undifferentiated cell. We found some evidence for
a relation between the severity of the ischemia and
VEGF-A and FGF-2 concentrations in the patient group.
Due to large inter-individual variations of these
angiogenic factors as reflected by the inability of the
markers to separate healthy from sick, they do not
appear to be suitable as markers for selecting individual
patients for gene or cell therapy.II
We performed another trial to test the hypothesis that
germline DNA variations in the VEGF-A promoter and 5´
untranslated region were associated with the plasma
concentration of VEGF-A, and that these DNA variations
as well as the VEGF-A plasma concentration influence
the ability to open coronary collateral arteries in patients
with acute and chronic obstructive coronary heart
disease.III The plasma concentration of VEGF-A was
significantly increased in patients with acute coronary
heart disease compared to patients with chronic
coronary heart disease, but the inter-patient variations
were large.III This is in concordance with results showing
that VEGF-A plasma concentration seems to increase
shortly after acute myocardial infarctionIV and that
VEGF-A mRNA expression is low in chronic ischemic
myocardium but increased in acute ischemia and
reperfused myocardium.225 A model combining four
polymorphic loci (including two in Hardy-Weinberg
disequilibrium) in the VEGF-A gene promoter and 5´
untranslated region seemed to explain about 30% of the
variation in plasma concentration of VEGF-A, but this
model was identified in a stepwise analysis including
many loci and should thus be interpreted with caution.III
Coronary collaterals can be assessed by several
methods. We could not perform invasive measurements
in these patients and chose to assess collateral flow and
function indirectly using two previously described
angiographic methods. The Rentrop classification
assesses collateral filling of the epicardial artery227
whereas the Werner classification assesses the size of
recruitable collaterals following occlusion of an epicardial
artery. The Werner classification has been shown to
closely reflect both invasively determined collateral
resistance and the collateral functional capacity to
preserve ventricular function.228 We identified an inverse
association between the VEGF-A plasma concentration
and the size of the collaterals as classified by the
Werner classification228 in patients with chronic
myocardial ischemia.III The present results could
suggest that patients with lower concentration of
circulating VEGF-A have decreased coronary collateral
function. This is in concordance with other trials showing
that polymorphism in the VEGF-A promoter is associated
with impaired prognosis in heart failure229 and affects
diseases such as proliferative diabetic retinopathy230 and
end-stage renal disease.231 It can be speculated if the
neutral results of larger clinical trials with VEGF-A
treatment9,27 are affected by differences in the VEGF-A
gene leading to a very heterogeneous patient population
regarding VEGF-A plasma concentration. It would be of
conceptual interest to include analysis of size of
coronary collaterals or even hypoxic regulation of VEGF-
A by in-vitro assay in future trials of neovascularization
for cardiovascular disease.
Homing of bone marrow-derived cells into ischemic
myocardium
All studies have demonstrated high concentrations of
putative hematopoietic stem or progenitor cells in the
blood after treatment with G-CSF (Figure 2).I,208,212 It
can be speculated if these cells home into the chronic
ischemic myocardium.
Homing is the process where circulating cells migrate
into the target tissue by traversing the endothelial
barrier. The general consensus that cell-based therapies
primarily derive from paracrine actions requires homing
of the cells (regardless of type) to the ischemic area
Figure 5. Subclassification of circulating CD45-/CD34- cells in patients with ischemic heart disease compared to healthy controls. (Reproduced from Ripa et al. Int J Cardiol 2007 with permission from Elsevier)

- 24 -
since the secreted factors are limited to a local area with
high concentration. Cell homing is in many aspects a
mirror process of bone marrow cell mobilization.
Most of the knowledge regarding cell homing and
migration comes from studies on hematopoietic stem
cells and EPC but it is natural to assume related
mechanisms for other cell populations. Local tissue
ischemia induces fast increased expression of
chemokines, where SDF-1 and VEGF-A in particular has
attracted much attention.232,233 Homing of cells is a
multistep procedure involving interaction with the host
endothelium, transmigration through the endothelial
barrier and migration into the host tissue. Human CD34+
cells initiate the low affinity rolling phase on E- and P-
selectin.234 A high affinity adhesion results from β2- and
β1-integrin interaction with their counter ligands
expressed on the endothelial cells (ICAM-1 and VCAM-
1). SDF-1 expressed on the endothelia appear crucial in
this process of integrin adhesion.234,235 The next step of
extravasation involves SDF-1 induced cell polarization236
and degradation of the basal membrane probably by
matrix-degrading enzymes, β2-integrin appear
important in this process.237 The next step of migration
towards the ischemic area guided by chemokine
gradient also involve proteolytic activity e.g. by
cathepsin L.238
The main proposed mechanism of G-CSF therapy to
ischemic heart disease is mobilization and subsequent
homing of progenitor cells to the ischemic area. The
myocardial homing of G-CSF mobilized cells in patients
with ischemic cardiomyopathy may be impaired by a
number of factors: (1) microarray analysis and real-time
PCR could not demonstrate any significant difference in
SDF-1 expression between chronic ischemic myocardium
and normally perfused myocardium.225 A study of gene-
expression in human limbs following amputation
similarly showed a low expression of VEGF-A, SDF-1,
and CXCR4 in chronic ischemic tissue compared to non-
ischemic tissue.239 This impaired chemokine respons
could potentially reduce cell homing substantially. (2)
The angiogenic potency of bone marrow cells have been
shown reduced in patients with chronic ischemic heart
disease as well as a number of conditions related to
ischemic heart disease, such as high cholesterol, high c-
reactive protein, aging, renal failure, anemia etc.240,241
The angiogenic potential of bone marrow-derived MSC
does not seem impaired in patients with chronic
ischemic heart disease.242 (3) Endothelial dysfunction
seems to impair neoangiogenesis by reducing tissue
nitric oxide synthase expression.243-245 (4) The Jak/STAT
pathway is a downstream target from CXCR4 on EPC
that modulates cell migration. It was recently shown
that Jak-2 phosphorylation in response to SDF-1 was
reduced in patients with ischemic heart disease
indicating a functional impairment of the cells.246 (5) G-
CSF in itself may also affect the bone marrow-derived
cells, as impaired migratory capacity following G-CSF
has been found.247,248 Another study showed that G-CSF
mobilized bone marrow-derived mononuclear cells do
not engraft in chronic ischemic myocardium.
Engraftment was only observed after transplantation of
SDF-1 expressing fibroblasts.232 Finally, G-CSF was
shown to reduce expression of adhesion molecules
involved in the homing process (CXCR4, β2- and β1-
integrin) on circulating CD133+ cells in the RIVIVAL-2
trial.249
Animal studies have shown that VEGF-A gene transfer
combined with G-CSF therapy leads to incorporation of
bone marrow-derived cells into ischemic myocardium.216
However, in animal studies, chronic ischemia will include
components of acute and subacute ischemia as well.
Most animal studies induce chronic myocardial ischemia,
using an ameroid constrictor around the circumflex or
anterior descendent artery. Four to five weeks later the
myocardium is often called chronic ischemic
myocardium. However, the intracellular milieu is
probably in many respects not similar to patients’
myocardium suffering from repetitive chronic ischemia
for several years.
Imaging studies (page 32) are warranted to elucidate
the issue regarding homing and engraftment of
injected/infused cells in vivo.

- 25 -
G-CSF FOR STEMI Clinical trials
Encouraging animal and laboratory results led to a quick
translation from the bench to patients suffering an acute
myocardial infarction and numerous small sample safety
and efficacy trials have been conducted and
published.250-255
Kuethe et al251 included 14 patients to subcutaneous G-
CSF 2 days after primary percutaneous coronary
intervention (PCI) and nine patients who refused G-CSF
treatment were included as control group. The authors
found a non-significantly larger increase in ejection
fraction in the G-CSF treated patients when compared
with the control group (7.8 vs. 3.2%). A single-blinded,
placebo-controlled study with G-CSF treatment 1.5 days
after STEMI (n=20) found almost identical results with a
non-significant trend towards improvement in ejection
fraction252. Leone et al253 randomized 41 patients 1:2 to
unblinded G-CSF or conventional treatment. All patients
had anterior STEMI and ejection fraction<50 at
inclusion. After 5 months there were a significant
improvement in left ventricular ejection fraction
(p=0.02) and absence of left ventricular dilatation
(p=0.04) when compared to conventional treatment.
Remarkably, patients receiving conventional treatment
had no change in ejection fraction in the follow-up
period (from 38±6% to 38±8%).253 The larger
FIRSTLINE-AMI256 trial (n=50) was a phase 1
randomized, open-label trial of G-CSF treatment
initiated within 90 min after primary PCI treated STEMI.
The control group did not receive placebo injections. The
G-CSF-treated patients had a significant improvement in
left ventricular function with enhanced systolic wall
thickening in the infarct zone (from 0.3±0.2mm to
1.1±0.3mm) and an improvement in ejection fraction
(from 48±4% to 54±8%). In contrast, the control group
had less systolic wall thickening (from 0.3±0.3% to
0.6±0.3%) and a decrease in ejection fraction (from
47±5% to 43±5%) measured with echocardiography.256
The finding that patients in the control group did not
experience any improvement in left ventricular ejection
fraction is remarkable and not consistent with other
clinical studies (page 31) and daily clinical experience.
Four randomized, double-blinded, placebo-controlled G-
CSF trials have been published and all reached similar
conclusions despite some differences in study
design.IV,257-259 The REVIVAL-2258 and the STEMMIIV trials
included patients with STEMI treated with PCI within 12
hours after symptom onset (Figure 6). Patients in the
STEMMI trial (N=78) received the first G-CSF or placebo
injection 10 to 65 hours (with 85% initiated <48 hours
after PCI), and five days after the PCI in the REVIVAL-2
trial (N=114). The primary endpoint in the STEMMI trial
was change in regional systolic function (systolic wall
thickening) and this did not differ significantly between
the placebo and G-CSF groups (17±32 versus 17±22
percentage points, Figure 7).IV Left ventricular ejection
fraction improved similarly in the two groups measured
by both MRI (8.5 versus 8.0; P=0.9) and
echocardiography (5.7 versus 3.7; P=0.7). The infarct
sizes were unchanged in the 2 groups from baseline to
the 6-month follow-up.IV This was probably due to the
small sample size, since pooling of all the patients in the
STEMMI trial suggested a significant decrease in infarct
mass during the first monthVI – a result similar to other
Figure 7. Primary endpoint of regional systolic wall thickening efter G-CSF or placebo treatment. (Adapted from Ripa et al. Circulation 2006 with permission from Wolters Kluwer Health)
Figure 6. STEMMI trial design.

- 26 -
MRI studies.260 The STEMMI trial has some inherent
limitations that increase the risk of a false negative
result. First, we included 78 patients, and 54 (69%)
were available for paired analysis of the primary
endpoint – this is a small population even though the
pretrial analysis indicated a 90% power to detect a
significant change. Second, the trial was designed to
include a homogeneous population where early MRI was
possible (mean ejection fraction 53% and infarct size
13g); this probably led to exclusion of high-risk patients
who would potentially benefit most from the
treatment.50 We intended to increase statistical power
by using a paired design with an accurate method
(MRI). The primary endpoint of the REVIVAL-2 trial was
reduction of left ventricular infarct size according to
technetium 99m sestamibi scintigraphy. Between base-
line and follow-up, left ventricular infarct size was
reduced by a mean (SD) of 6.2% (9.1%) in the G-CSF
group and 4.9% (8.9%) in the placebo group (P=0.56).
Ejection fraction was improved by 0.5% (3.8%) in the
G-CSF group and 2.0% (4.9%) in the placebo group
(P=0.14).
Engelmann et al259 included patients (N=44) undergoing
late revascularization (6-168 hours) after subacute
STEMI. G-CSF was initiated approximately 1½ day after
the PCI. Global myocardial function from baseline (1
week after PCI) to 3 months improved in both groups,
but G-CSF was not superior to placebo (∆ejection
fraction 6.2±9.0 vs. 5.3±9.8%, p = 0.77). Ellis et al257
included few patients (N=18) into a pilot dose-escalation
randomized trial and found no effect of G-CSF on left
ventricular ejection fraction.
In a recent meta-analysis we aimed to evaluate the
effect of cell mobilization by G-CSF on myocardial
regeneration after acute myocardial infarction.261 Ten
randomized trials, including 445 patients, were included.
Compared with placebo, stem cell mobilization by G-CSF
did not enhance the improvement of left ventricular
ejection fraction at follow-up (Figure 8, mean difference
1.32% [95% confidence interval -1.52 to 4.16; p =
0.36]) or reduction of infarct size (mean difference -
0.15 [95% confidence interval -0.38 to 0.07, p =
0.17]).261
Safety of treatment with G-CSF after STEMI
A major issue to consider is the possibility that the
neutral outcome of the G-CSF trials is the result of
undetected adverse outcomes balancing any benefits of
the G-CSF treatment.
In all reported trials G-CSF was generally well tolerated.
Only a few patients experienced minor musculoskeletal
pain, a well known side-effect of G-CSF.
Safety data from more than 200 patients treated with
G-CSF early after STEMI have been published. Four of
these severely ill patients died in the follow-up
period251,255,258,259, one patient had a spleen rupture250
and three patients had a sub-acute in-stent thrombosis
or re-infarction.IV,211,257,259 We recently performed a 5-
year clinical follow up of the patients included in STEMMI
(presented as abstract262). The clinical events were
combined into 4 prespecified endpoints: Time to first (1)
hospital admittance (all cause), (2) cardiovascular
related hospital admittance, (3) major cardiovascular
event, (4) Death. Survival analyses in this small cohort
showed no differences in the occurrence of any of the 4
prespecified composit endpoints between the two groups
(p=0.6; 0.5; 0.8; 0.3). This result must be interpreted
with extreme caution due to the low number of both
patients and events.
Trials by Kang et al263 and Steinwender et al264 have
indicated that G-CSF treatment increase the progression
of atherosclerosis and in-stent restenosis if initiated a
few days prior to stent implantation, maybe by
increased inflammation or blood viscosity. However,
both trials have several potentially inflicting issues. In
the trial by Steinwender et al264 at the time of cell
injection into the infarct related artery, one vessel was
occluded, four patients needed additional stents to
restore normal antegrade flow, one patient had a guide
Figure 8. The effect of G-CSF treatment on recovery of ejection fraction – a meta-analysis. (Reprinted from Zohlnhöfer et al. JACC 2008 with permission from Elsevier)

- 27 -
wire-induced dissection of the vessel, and only four
patients were treated with drug-eluting stents.
Therefore, it is more likely that the very high restenosis
rate (40%) was procedure and stent-related and not
related to the G-CSF treatment. The trial by Kang et al
included only few patients, into a clinically irrelevant
design with a very late stent revascularization.263 The
trial by Kang et al was published in Lancet in the middle
of the inclusion period of the STEMMI trial. This
obviously gave us severe concern regarding the
continued inclusion of patients into the trial despite the
differences in study design. We chose to do a non-
prespecified interim analysis of baseline data, 1-week
blood tests, and data from the 5 months invasive follow-
up (including intravascular ultrasound) from all patient
included at that time (n=41) to evaluate whether it was
safe to continue inclusion in the STEMMI trial.265 The
analyses of the intravascular ultrasound and angiograms
were performed in a blinded fashion by an independent
core laboratory (Bio-Imaging Technologies B.V., Leiden,
The Netherlands). In conclusion, we found identical re-
stenosis rates in G-CSF-treated and control groups by
quantitative coronary angiography and by intravascular
ultrasound and which legitimized continued inclusion.265
We found it most likely that the differences compared to
the trial by Kang et al was caused by significant
differences in the timing of G-CSF administration in
relation to PCI. Later, our preliminary results were
confirmed in the total STEMMI populationIV,266, the
FIRSTLINE-AMI trial256, the G-CSF-STEMI trial259, the
REVIVAL-2 trial258, and in a meta-analysis267. In
addition, a recent new report with more patients and
longer follow-up from Kang et al do not support their
initial conclusions.254
Treatment with G-CSF leads to a slight increase in
inflammatory markers as determined by C-reactive
protein and erythrocyte sedimentation rates.IV This
inflammatory response combined with the increase in
neutrofil granulocytesIV could potentially lead to plaque
destabilization and progression of atherosclerosis. An
experiment with high cholesterol-fed pigs showed no
effect of G-CSF on the atherosclerotic lesions or on
neutrophil infiltration in the lesions.221 In contrast, a
preclinical study in apolipoprotein E-deficient mice,
demonstrated an exacerbation of the atherosclerotic
lesions after treatment with G-CSF for 8 weeks.268 This
effect was only evident in mice maintained on high fat
diet.
There has been some evidence that intramyocardial
transplantation of skeletal myoblasts induce ventricular
tachyarrhythmia in patients.269,270 None of the clinical
trials with G-CSF treatment to ischemic heart disease
has indicated a pro-arrhythmic effect and an experiment
in mice has even indicated a reduced inducibility of
ventricular arrhythmias after G-CSF treatment when
compared with controls.271
In conclusion, the treatment with G-CSF following
STEMI and PCI seems to be safe. Still, it cannot be
totally excluded that G-CSF may have contributed to the
serious adverse events reported from the trials leading
to an offset of the positive effects observed in animal
studies.
Why does G-CSF not improve myocardial function
following STEMI?
It is remarkable that early phase clinical trials and in
particular the randomized FIRSTLINE-AMI trial including
50 patients suggested a positive effect of G-CSF,
whereas all randomized and double-blinded trials using
G-CSF for STEMI were neutral in effect. The major
differences between the FIRSTLINE-AMI and the later
double blinded trials are the lack of placebo treatment in
the FIRSTLINE-AMI and thus lack of blinding; and the
time of G-CSF administration.
Time to G-CSF
G-CSF was administered as early as 89 min (SD 35 min)
after reperfusion in the FIRSTLINE-AMI study, which is
somewhat earlier than the remaining trials (Figure 9).
This could explain some of the differences since
Figure 9. Recovery of ejection fraction in human trials of G-CSF after STEMI in relation to time to G-CSF. (Adapted from Ripa et al. Exp Hematol 2008 with permission from Elsevier)

- 28 -
experimental evidence in mice suggest a time-sensitive,
direct, cardioprotective effect of G-CSF rather than a
cell-mediated effect. The study indicated that the anti-
apoptotic effect was significantly reduced if treatment
was delayed to only 3 days post-myocardial infarction.76
It is however important to notice that the G-CSF dose
used in the mouse study was 10 to 20 times higher than
the dosages used in human trials (up to 100 μg/kg).
The REPAIR-AMI trial revealed a significant interaction
between the absolute changes in left ventricular ejection
fraction at 4 months and the time from reperfusion
therapy to direct intracoronary infusion of bone marrow
cell solution or placebo medium, in fact beneficial effect
was confined to patients treated later than 4 days after
reperfusion.50 This corresponds well with results from
the STEMMI trial where the peak concentration of CD34+
and CD45-/CD34- mononuclear cells, was measured in
peripheral blood 4 to 7 days after the initiation of G-CSF
treatment.V Some evidence could even suggest a very
late time-point of cell therapy as optimal since homing
factors involved in myocardial engraftment of mobilized
or infused cells (SDF-1) and vascular growth factors
(VEGF-A and FGF) only increase slowly during the first
weeks after acute myocardial infarction and reach
maximum concentrations after 3 weeks.32 We have
performed a post hoc analysis of the STEMMI trial to
address the issue regarding time to treatment in relation
to outcome.272 There were no indications in this study
that the timing of G-CSF treatment in STEMI patients
plays a role in the recovery of left ventricular ejection
fraction (Figure 10). This result is comparable to a post-
hoc analysis of the G-CSF–STEMI trial273 concluding that
G-CSF after myocardial infarction does not improve
myocardial function if the cytokine is given early. The G-
CSF–STEMI trial however, did not include STEMI
patients treated with acute primary PCI, but patients
with subacute STEMI and late revascularization (mean
32 hours after symptom onset), making a direct
comparison to our data difficult.
The G-CSF dose
The optimal dose of G-CSF remains unknown. Most
clinical trials so far have pragmatically used 10 μg G-
CSF/kg per day known from clinical hematology. Only a
single clinical trial of patients with myocardial ischemia
has addressed this issue. Ellis et al257 randomized 18
patients with STEMI into double blind treatment with
placebo (N=6), G-CSF 5 μg/kg per day (N=6), or G-CSF
10 μg/kg per day (N=6). G-CSF treatment led to a 5- to
7-fold increase in CD34+ and CD117+ cells with no
apparent difference in mobilization between the 2 doses
of G-CSF.257 In contrast, we have found evidence of a
dose-dependent cell mobilization in patients with stable
ischemic heart disease.219 One trial found dose-
dependent improvement in regional myocardial function
after intracoronary infusion of bone marrow
mononuclear cells.274 The direct cardioprotective effect
of G-CSF seen in mice76 could requires an even higher
dose of G-CSF since this study used up to 100 μg/kg per
day.
Differential mobilization of cell types
Another aspect of G-CSF treatment versus direct
intracoronary cell infusion is the type of cells used. It
remains puzzling that in vivo mobilization of bone
marrow–derived cells by G-CSF to the circulation does
not result in myocardial recovery comparable to that
apparently achieved by ex vivo purification and
subsequent intracoronary infusion of bone marrow–
derived cells in the REPAIR-AMI trial.50 Animal
experiments indicate that MSC may be good candidates
for cardiac repair163,164,275, whereas the hematopoietic
progenitor cells are less likely to improve cardiac
function.6 One hypothesis could thus be that G-CSF does
not mobilize effective cell types (such as MSC) whereas
bone marrow aspiration and purification yields these
cells. We analyzed peripheral blood cells from the
STEMMI trial to investigate this hypothesis.V G-CSF is
known to mobilize endothelial and hemotopoietic cells
from the bone marrow to the peripheral blood (page
9).220,247 The mobilization of MSC by G-CSF is more
debated. In a much cited paper Pitchford et al. showed
that treatment with G-CSF did not increase PBMSC276
Figure 10. Association between time to treatment and recovery of left ventricular ejection fraction in the STEMMI trial. (Adapted from Overgaard et al. Int J Cardiol 2010 with permision from Elsevier)

- 29 -
and others have found similar results.172,277 However,
several other trials have found indications that G-CSF do
increase the number of PBMCS.173,278-282 Indirect
evidence of bone marrow mobilization and myocardial
engraftment of MSC comes from studies of mice
receiving bone marrow transplantation with MSC
expressing enhanced green fluorescent protein.
Following acute myocardial infarction and G-CSF
treatment, cells expressing enhanced green fluorescent
protein and actinin were identified in the myocardium.278
More direct evidence come from trials identifying PBMSC
(typically CFU-F) in both healthy donors (humans or
animals)173,279,280 or following myocardial ischemia281,282.
Myocardial ischemia without any mobilizing treatment
also seem to increase the number of PBMSC.282 The
mechanism of G-CSF induced increase in PBMSC is
unknown but the observed differences in the temporal
concentrations of MSC, EPC and hematopoietic stem
cells in the blood following G-CSF treatment of normal
mice could indicate diverse mechanisms.279 We assessed
the number of PBMSC by identification of circulating
mononuclear cells negative for both the endothelial
marker CD34 and the pan-leukocyte marker CD45 for
reasons discussed on page 22. This identification
procedure has low specificity for MSC, and to designate
the whole population of circulating CD45-/CD34- cells as
putative MSC in the paper is retrospectively and
according to the minimal criteria by The International
Society for Cellular Therapy141 inexact.
Figure 11 shows the number of CD34+ cells (panel A)
and CD45-/CD34- cells (panel B) relative to the
leukocytes following treatment with G-CSF in the
STEMMI trial.V The fraction of CD34+ cells increased
during G-CSF treatment, whereas the fraction of CD45-
/CD34- cells decreased during the treatment. Also,
treatment with G-CSF compared to placebo caused a
shift in the subtypes of CD45-/CD34- in the peripheral
blood with a minor fraction of cells expressing CD73 (a
marker expressed by MSC) and CD31 (an endothelial
marker), and a larger fraction expressing the VEGF-R
(an endothelial marker) and CD133 (a hematopoitic
marker).V However, expression of several of the marker
known to be expressed by both MSC and endothelial
cells are not affected by G-CSF (CD105, CD166, CXCR4,
CD144). This heterogenous change in subtypes of CD45-
/CD34- is difficult to interpret and is probably caused by
the low sensitivity and specificity of the included
markers.
It can be hypothesized, that the identified differential G-
CSF mobilization of circulating CD34+ and CD45-/CD34-
cells might in part explain the observed difference in
therapeutic effect of G-CSF vs. intracoronary infusion of
bone marrow cells (in the STEMMI vs. in the REPAIR-
AMI trial). However, the results should be interpreted
with caution due to the low number of patients, the
exploratory nature of the design, and the low sensitivity
and specificity of the surface markers for identifying
discrete cell populations.
Homing of mobilized cells to the myocardium
Homing of the circulating cells into the ischemic
myocardium is a prerequisite for both a paracrine
mechanism and a direct incorporation and differentiation
of progenitor/stem cells. Patients with ischemic heart
disease seem to have impaired homing capacity and
additionally G-CSF seems to impair the migratory
capacity of the mobilized cells (page 23). We have
roughly estimated the number of cells supplied to the
ischemic myocardium (and thus available for homing)
during the first week after G-CSF/placebo treatment.
The purpose of this estimate was to compare our
mobilizing approach with the number of cells infused in
studies using an intracoronary infusion of bone marrow-
derive mononuclear cells, and also to compare the
number of cells mobilized in the STEMMI and the
FIRSTLINE-AMI trials. For the estimate, we used cell
concentrations measured at day 1, day 4, and day 7.
The blood flow to ischemic myocardium was
approximated at 80 ml/min in all patients based on the
method used by Ince et al in the FIRSTLINE-AMI
trial.256,283 Previously, one trial found a mean flow rate of
approximately 60 ml/min through the stented segment
following primary PCI284 and another trial found a mean
Figure 11. Ratio of (A) CD34+ cells/1000 leucocytes, and (B) CD45−/CD34− cells/1000 leucocytes in the blood during 30 days after myocardial infarction. Full line is G-CSF treatment and bracket line is placebo treatment. (Reproduced from Ripa et al. Circulation 2007 with permission from Wolters Kluwer Health)

- 30 -
flow of 140/118/144 ml/min in the proximal
LAD/LCx/RCA and 55/51/64 ml/min in the distal
segments of the same arteries.285 More recently, Erbs et
al measured a basal coronary blood flow just below 80
ml/min in the stented infarct related artery 4 days after
STEMI in the REPAIR-AMI trial.58 The estimate has the
obvious limitations that differences in volume of
ischemic tissue, vascular dilatation, and presence of
microvascular obstruction will cause inter-patient
differences in the true blood volume supplied to the
ischemic area. Compared to FIRSTLINE-AMI we found
almost identical numbers of CD34+ cells (2.5x1010 vs
2.8x1010). Thus, our G-CSF approach seemed to expose
the myocardium to more than 100 times the number of
CD34+ cells infused in the REPAIR-AMI trial50. We found
no association between the estimated total number of
CD34+ cells supplied to the postischemic myocardium
after myocardial infarction and the subsequent change
in left ventricular ejection fraction.V An inverse
association was found between the estimated number of
CD45-/CD34- cells supplied to the postischemic
myocardium and the change in left ventricular ejection
fraction (95% CI of regression coefficient -11.4 to -2.2,
P=0.004).V We found similar results when using the day
7 concentration of CD34+ or CD45-/CD34- cells rather
that the estimated total number of cells to predict
recovery of ejection fraction (Figure 12). The association
was not reproduced when using systolic wall thickening
as dependent variable. This could indicate a statistical
type I error.
A causality of the association cannot be determined in
an observational study, but the results may suggest that
a low concentration of the CD45-/CD34- cells in the
blood is due to engraftment of the cells into the
myocardium. Thus, patients with a high inert potential
for myocardial homing after STEMI will have the highest
degree of systolic recovery due to the engrafted cells. Of
note, we found a similar inverse association between
ejection fraction and CD45−/CD34− cells in patients with
chronic myocardial ischemia.II
It could alternatively be speculated that CD45−/CD34−
cells are not homing, but potentially reduce the recovery
of the myocardial function explaining the inverse
association between circulating CD45-/CD34- cells and
changes in global ventricular function.V A study in dogs
has indicated that intra-coronary infusion of MSC could
cause micro-infarctions, probably due to microvascular
obstruction by the cells.286 However, there was no
biochemical or electrocardiographic evidence of
myocardial ischemia during the G-CSF treatment in the
STEMMI trial. In addition, circulating mononuclear cells
collected after G-CSF treatment and then injected into
the infarct related coronary artery in patients with
STEMI did not result in any signs of myocardial
damage.287
Conclusion
There is no convincing evidence that monotheraphy with
G-CSF early after STEMI improves recovery of left
ventricular function, despite the discrepancy in results
when compared with previous animal and uncontrolled
or unblinded clinical G-CSF trials. We still cannot
exclude the possibility that the trials have been
underpowered to detect a small difference but the
recent meta-analysis makes this unlikely.261 As for
patients with chronic ischemia, it must be speculated if
arteriogenesis rather that angiogenesis should be the
goal of the therapy. The complex interaction between
stem cell mobilization/engraftment and cytokines
remains poorly understood, and the results do not
exclude the possibility that G-CSF could be part of a
treatment strategy combing several cytokines and/or
local stem cell delivery in future trials.288 The MAGIC
Cell-5-Combicytokine Trial (clinicaltrial.org,
NCT00501917) that was initiated March 2007 to
evaluate the efficacy of combination therapy with
erythropoietin and intracoronary infusion of G-CSF
mobilized peripheral blood stem cells. The SITAGRAMI-
Trial initiated in March 2008 aim to test a dual strategy
of G-CSF in combination with an inhibition of SDF-1
degradation.289
Figure 12. Association between changes in left ventricular ejection fraction during 6 months and concentration of (A) CD34+, and (B) CD45−/CD34− cells on day 7 after treatment with G-CSF or placebo. Regression line with 95% confidence interval. *Abscissa in logarithmic scale.

- 31 -
MYOCARDIAL RECOVERY AFTER STEMI Cardiac MRI is an attractive method for efficacy
assessment in early phase clinical trials since the high
accuracy and precision allows for inclusion of a
minimum of patients (page 16). However, in using MRI-
derived endpoints it is important to acknowledge
(especially in early trials without randomized control
groups) the limited knowledge of the natural course of
myocardial recovery following a reperfused acute
myocardial infarction with modern guideline treatment.
One example is the use of G-CSF for acute myocardial
infarction where early non-controlled trials postulated an
effect. However, the later randomized trials showed a
similar improvement in the placebo treated groups. We
therefore performed a study aiming at the investigation
of the short-term and long-term effects of current
guideline treatment of STEMI, including successful
primary PCI, in terms of left ventricular function,
morphology, edema, and perfusion using cardiac MRI.VI
Overall, we observed a substantial recovery of all
investigated variables primarily within the first month
after the reperfusion. Left ventricular ejection fraction
increased with more that 8 percentage points (Figure
13), the systolic wall thickening in the infarct area
almost doubled (Figure 14), and the perfusion of the
infarcted myocardium increased with approximately
50%.VI These results are potentially biased by the low
number of patients with a potential selection bias
(n=54) and the post hoc design, but the variance of the
means were still acceptable (e.g. 95% CI of the mean
ejection fraction change from 4 to 9 percentage points).
Furthermore, these patients were all included in a trialIV
and we cannot exclude the possibility that the post AMI
care were more careful than daily clinical practice.
The results found are comparable to those of a smaller
MRI study (N=22) by Baks et al290 who found an
increase in ejection fraction of 7 percentage points.
Trials assessing the change in ejection fraction from
angiography show minor but still substantial increases
(3-6 percentage points)291-293
In contrast, one trial including 51 patients with
myocardial infarction found no change in ejection
fraction.294 Study design and population can potentially
explain some of the differences; first and perhaps most
important, the baseline MRI was not performed until 5
days after the infarction, second, only 16 of the patients
were treated with angioplasty, 21 with trombolysis and
14 with aspirin alone owing to late admission or
diagnosis, and third, the left ventricular volumes were
assessed from two long axis cine loops using the
modified biplane Simpson’s method,294 whereas we
assessed the volumes from short-axis cine loops
(usually 10) covering the entire left ventricle.VI The
improvement in wall thickening confirmed a previous
trial of 17 patients showing a increase from 22 to 38%
in the infarcted area.295
Figure 13. Change in ejection fraction. Bold line indicates mean±SE. (Reproduced from Ripa et al. Am Heart J 2007 with permission from Elsevier)
Figure 14. Mean change in systolic wall thickening efter STEMI in 3 myocardial areas. (Adapted from Ripa et al. Am Heart J 2007 with permission from Elsevier)

- 32 -
A limitation of our study design is the 30-day time span
between the initial and first follow-up examination,
which does not allow firm conclusions about the precise
timing of the changes observed. However, results from
others suggest that the recovery of left ventricular
ejection fraction primarily happens within the first week
following reperfusion,258,296,297 since these trials with a
later baseline MRI observe less recovery of ejection
fraction. This spontaneous recovery is probably primarily
due to early myocardial stunning following the ischemic
event.298
The infarct mass was reduced by almost 30% from
baseline to 6 months follow-up,VI a result very similar to
the results of others.260,299,300 This is consistent with
animal data showing that healing of a myocardial infarct
is an ongoing process:301 After four days central
necrosis, hemorrhage and inflammation can be
observed. This is followed by infarct resorption, scar
formation by tissue composed of fibroblasts in a dense
collagen matrix and wall thinning after six weeks.301
There has been some suggestions that infarct size
assessed by MRI in the first days after the infarction
overestimates the true infarct size302-304 perhaps due to
myocardial edema in the adjacent myocardium.
However, two methodologically strong studies in dogs
by the group of Kim and Judd305,306 showed a very close
correlation between in vivo and ex vivo infarct size
measured with MRI and infarcted regions defined by
triphenyltetrazolium chloride staining from 4 hours to 8
weeks after coronary artery occlusion (both with and
without reperfusion).
The results of our MRI studyVI underscores the
importance of a proper control group in trials including
patients after acute myocardial infarction due to the
substantial change in all measured parameters during
the first month, or at the very least a good knowledge of
the natural course of the disease. In addition, it appears
of crucial importance that baseline examinations are
performed within a narrow time window after the STEMI
when comparing several populations.
FROM BED TO BENCH To date most clinical trials of cells therapy have had a
pragmatic design with intracoronary infusion of
autologeous bone marrow-derived mononuclear cells.307
Bone marrow-derived mononuclear cells are isolated
using density gradient centrifugation following bone
marrow aspiration. The bone marrow-derived
mononuclear cell suspension primarily comprises
nonprogenitor cells and only about 3% hematopoietic
stem/progenitor cells or EPC.42 Cells positive for the
hematopoietic surface marker CD34 can also be
obtained from the peripheral blood, but an experimental
rat study has suggested that bone marrow-derived
mononuclear cells may provide an advantage when
compared to peripheral blood-derived mononuclear
cells.215,308 The modest improvement in ejection fraction
seen in most clinical trials (3% in a meta-analysis307)
has shifted the focus towards the use of more specific
stem or progenitor cell lines to improve outcomes. One
potentially useful cell line is the MSC, which can be
isolated from the bone marrow and expanded in
culture.309-311 Allogeneic MSC has been infused
intravenous in a clinical trial in patients after myocardial
infarction.312 It was primarily a safety trial, but the
results indicated a positive impact of MSC on ejection
fraction by MRI and by echocardiography in anterior wall
infarction only. A number of other secondary endpoints
(wall thickness, wall motion score index, and 6-min walk
test) were unaffected by MSC.
The optimal route of delivery of cells to the heart and
the potential mechanism by which cell-based therapy
works also remains to be determined. Imaging based
cell-tracking can potentially elucidate important
mechanistic issues by determining homing, engraftment
and growth of cells following transplantation.
Furthermore identification of redistribution to other
organs where the transplanted cells might lead to side
effects is of vital importance.
The ideal imaging technique should allow for serial
tracking in humans for a prolonged period of time with
high spatial resolution and with the capability of tracking
a few cells without affecting the cells or the organ. It is
important that the marker remains in the viable cell but
is quickly cleared from the tissue upon cell death.
Several in vivo imaging techniques are available and
currently direct labeling with radionuclides for gamma
camera imaging or PET310,311,313 or labeling with iron
particles for MRI314 appear suitable.
Imaging of leukocyte distribution using 111Indium (111In)
is a safe clinical routine procedure.315 In-111 is
commercially available with a half-life of 2.8 days
making in vivo tracking up to 2 weeks possible.
Experiments by Jin et al316 and Gholamrezanezhad et
al317 might suggest that the radioactivity from 111In

- 33 -
could be toxic to stromal cells, however, we found no
indication of radiotoxic effects on viability and/or
function after labeling of human MSC with 111In-
tropolone.318 Perhaps differences in culture or labeling
procedures could explain these differences in results.
Previously, several studies have used indium labeling of
both MSC and EPC and subsequent in vivo tracking of
the radioactivity as a surrogate measure of cell
engraftment and migration. These trials have been
conducted assuming that radioactivity assesses living
and active cells.319-322 In one trial 111In labeled
progenitor cells were infused into the coronary artery in
patients after acute myocardial infarction (N=20).319
One hour after infusion of progenitor cells, a mean of
6.9±4.7% (range, 1% to 19%; n=17) of total
radioactivity was detected in the heart. Radioactivity
remained in the heart after 3 to 4 days, indicating
homing of progenitor cells to the myocardium.319
Several of the experimental trials have confirmed the
presence of labeled cells by histology following
euthanasia of the animals.323-326
We designed a pilot trial to investigate whether the
biodistribution and retention of ex-vivo cultured MSC
can be determined after direct percutaneous
intramyocardial transplantation in a large animal model
by 111In-tropolone radiolabeling of human MSC.VII
Labeled MSC were first transplanted into four pigs by
trans-endocardial percutaneous injections. The 111In
activity in the heart was 35% (±11%) of the total
activity in the pig one hour after injection of viable 111In
labeled MSC,VII compared to only 6.9±4.7% after
intracoronary infusion319 and from 11.3±3%327 to
20.7±2.3%324 after trans-epicardiel injection. SPECT
imaging identified the 111In within the myocardium
corresponding to the locations of the intramyocardial
injections (Figure 15). Whole body scintigraphy revealed
focal indium accumulations in the cardiac region up to 6
days after injection.VII Myocardium with high
radioactivity was analyzed by fluorescence in situ
hybridization (FISH) and microscopy after euthanization
of the animals. No human MSCs were identified with
FISH, and microscopy identified widespread necrosis
and acute inflammation. Two new pigs were then
treated with immunosuppressive therapy to diminish the
host-versus-graft reaction observed in the first 4 pigs,
but injection of MSC still lead to a similar pattern with
focal indium accumulation, and inflammation but no
human MSCs could be identified. Two additional pigs
were injected with 111In-tropolone (without cells) to test
the tissue response to the gamma radiation from 111In.
In these two pigs radioactive tissue samples, identified
using a gamma detection probe, showed normal
myocardium without inflammation.VII This indicates that
neither the gamma radiation nor the intramyocardial
injection causes the inflammation and tissue-damage,
which is in concordance with our previous experience
from intramyocardial injections.218 A last pig was
injected with dead 111In labeled cells. The clearance of
Figure 15. A, Endocardial NOGA mapping of a pig heart. The dots indicate the injection sites. B, Dual isotope SPECT images of the left ventricle in the short axis showing a hot spot of 111In activity in the anterior wall, corresponding to the injection sites in the NOGA map. (Reproduced from Ripa et al. Int J Cardiovasc Imaging 2010 with permission from the Editor)
Figure 16. Relative retention of radioactivity after correction for decay. (Reproduced from Ripa et al. Int J Cardiovasc Imaging 2010 with permission from the Editor)

- 34 -
radioactivity of injected dead cells and of 111In alone
appeared faster initially compared to that of viable cells,
but retention after injection of viable cells, dead cells
and 111In followed a very similar pattern (Figure 16).
The results of this trial were potentially biased by
several factors. We only included few animals in a
prospective design making this a hypothesis generating
trial. However, we did consistently in 6 animals observe
intense radioactivity despite disappearance of the cells.
In our opinion, a very high specificity (close to 100%)
should be demanded of this labeling method, and our
results are in conflict with this. Another limitation is the
FISH method; we have not quantitatively determined
the sensitivity of the method in our setup and thus
cannot exclude the possibility that a few of the cells
were present despite the negative FISH result. However,
based on the radioactivity in the tissue-sample excised
for FISH analysis, we would expect >105 human cells
per gram tissue (assessed using our initial mean activity
of 1.4 Bq/cell).
In conclusion, the pilot study generates two important
hypotheses.VII First, as radioactivity from 111In-labeled
cells stays in the myocardium for a long time despite the
disappearance of transplanted cells, clinical use of 111In-
labeled cells for monitoring of MSC in the human heart
seems problematic unless viability can be determined by
another method. Second, xenografting of human MSC
into a pig leads to an inflammatory response and fast
degradation of the cells even under pharmacologic
immunosuppression.VII
Our results indicate that an alternative imaging modality
is warranted. Iron-oxide labeling for MRI tracking of
injected cells has appeared as a suitable alternative to
indium labeling, with the possibility of even longer
follow-up. However, recent results very similar to ours
using iron labeling were reported.328,329 After 3-4 weeks
no transplanted cells were detected. Instead a continued
enhanced magnetic resonance signal was found from
cardiac macrophages that engulfed the labeling particles
suggesting that iron-oxide labeling is also an unreliable
marker for monitoring cell survival and migration.328,329
Reporter gene imaging using clinical PET is another
promising modality.330 The reporter gene is expected to
be lost after cell death providing a more specific signal,
but the technology still needs further work.
GENERAL CONCLUSIONS AND FUTURE DIRECTIONS The objective of our investigations was to evaluate G-
CSF as a cell-based therapy for ischemic heart disase.
We found no effects of combined treatment with G-CSF
and VEGF-A-gene therapy in patients with chronic
ischemic heart disease in a small scale clinical trial.
Concordantly, we must conclude that if G-CSF and
VEGF-A have an effect on these patients, the effect is
most likely very small. We could not identify any
inherent factors in the blood or genetic variations in the
VEGF-A gene that could select optimal patients for cell-
based therapies.
When randomizing patients with STEMI to G-CSF or
placebo we found no clinical effect of G-CSF, but we did
observe a substantial recovery of myocardial function
following current guideline-based therapy of STEMI. This
´natural´ effect could potentially explain the apperant
effect of G-CSF previously reported in non-controlled
trials. Thus, our results did not support our pretrial
hypothesis that cell mobilization alone or in combination
with modulating molecules would result in clinical
effective cardiac regeneration.
Several clinical trials of G-CSF for ischemic heart disease
were published and planned prior to the presentation of
the STEMMI and the RIVIVAL-2 results. The group
behind the FIRSTLINE-AMI trial even planned a large-
scale multicenter clinical trial of G-CSF after acute
myocardial infarction based on their positive results in a
non-blinded trial. Our trials brought science past G-CSF
as monotherapy for ischemic heart disease despite the
negative results.
The heart is a complex organ composed of muscle and
non-muscle cells integrated into a three-dimensional
structure. Cardiac regeneration will probably require
more than simply supplying the right cell to the right
tissue, at the right time. So far, clinical trials have had a
pragmatic design using the cell types that are readily
available. This probably leads to extensive cell death
and inadequate integration in a hostile immunoreactive,
ischemic or necrotic environment explaining the neutral
or small effects observed in clinical trials.
Defining the factors present in the hostile
microenvironment of injured myocardium that limit the
homing, functional engraftment and survival of
transplanted cells will be essential for guiding the
development of stem-cell-based therapies.

- 35 -
Unfortunately, no good method for long-term in vivo
imaging of transplanted cells exists. To complicate
matters even more, the results in clinical trials are
potentially biased by a significant change in both
morphology, function, and perfusion following PCI
treated acute myocardial infarction without cell therapy.
Tissue engineering331,332 combining cells with artificial or
natural scaffolds, or intramyocardial injection of
combinations of cell types and/or cytokines may be
more effective than a single intracoronary injection of
single-cell suspensions. Alternatively, long-time
engraftment and survival of transplanted cells may not
be necessary if paracrine effects are the main
mechanism of cell-based therapies. In that case,
identification and administration of the secreted active
components could be more appropriate than cell
transplantation. As the many remaining questions
regarding cardiac regeneration are elucidated,
meticulously designed clinical trials should proceed with
caution and with a paramount concern for patient
safety. Ultimately larger trials are needed to answer the
key question if improvement in surrogate endpoints
translates into improvement in clinical endpoints such as
mortality and morbidity. The publication of both positive
and negative trial results provides the research
community the important opportunity to progress.
Hopefully, the next decade will make the intuitively
attractive concept of regenerating the broken heart a
reality.

- 36 -
SUMMARY IN DANISH – DANSK RESUMÉ Celle baseret terapi til iskæmisk hjertesygdom er en
behandlingsform med potentiale til at kunne mindske
post infarkt-hjerteinsufficiens og kronisk iskæmi.
Behandling med granulocytkolonistimulerende faktor (G-
CSF) fører til en mobilisering af celler fra knoglemarven
til det perifere blod. En del af disse celler formodes at
være stamceller eller lavt differentieret celler. G-CSF
gives som subkutan injektion og er intuitivt attraktiv
sammenlignet med andre cellebaserede teknikker, da
patienten undgår gentagne hjertekateriseringer, og da
der ikke ex vivo skal foretages oprensning/dyrkning af
cellerne.
Prækliniske og tidlige kliniske forsøg tydede på, at
behandling med G-CSF kunne forbedre myokardie-
perfusionen og myokardiefunktionen ved akut eller
kronisk iskæmi. Hypotesen i denne afhandling er, at G-
CSF gavner patienter med myokardieiskæmi. Vi
undersøgte denne hypotese i to kliniske forsøg med G-
CSF til henholdsvis patienter med akut myokardieinfarkt
eller svær kronisk iskæmi. Desuden har vi undersøgt en
række faktorer, som kunne påvirke effekten af
cellebaseret terapi. Endelig har vi forsøgt at udvikle en
metode til at følge celler i hjertet in vivo.
Vores forsøg viste, at subkutan G-CSF sammen med
genterapi ikke forbedrer myokardieperfusionen hos
patienter med kronisk iskæmi trods en stor stigning i
cirkulerende knoglemarvsderiverede celler. Ligeledes
fandt vi ingen forbedring i angina pectoris eller
gangdistance i sammenligning med placebo-behandlede
patienter. Vi kunne ikke påvise ændringer i
plasmakoncentrationen af hverken angiogene faktorer
eller knoglemarvsderiverede celler, som kunne forklare
den neutrale effekt af G-CSF.
Derefter undersøgte vi G-CSF behandling som
adjuverende terapi umiddelbart efter ST elevations-
myokardieinfarkt. Vi fandt ingen effekt hverken på det
primære effektmål regional myokardiefunktion eller på
venstre ventrikel uddrivningsfraktion (sekundært
endepunkt) i sammenligning med placebobehandling. I
efterfølgende analyser fandt vi forskel på hvilke
celletyper, der blev mobiliseret af G-CSF, hvilket kan
være en del af forklaring på, hvorfor intrakoronar
injektion af knoglemarvs deriverede celler
tilsyneladende har bedre effekt end mobilisering med G-
CSF.
En række andre forhold kan tænkes at forklare den
neutrale effekt af G-CSF i vores studie sammenlignet
med tidligere G-CSF studier såsom tidspunkt for
behandling, G-CSF dosis og population. Det er imidlertid
påfaldende, at forskellen i forbedring sammenlignet med
tidligere ikke-blindede studier af G-CSF ligger i kontrol-
gruppen og ikke i den aktivt behandlede gruppe. Vi
fandt, at uddrivningsfraktion, lokal vægbevægelse,
ødem, perfusion og infarktstørrelse blev signifikant
forbedret i især den første måned efter et ST elevations-
myokardieinfarkt efter standard guideline behandling
(inklusiv akut mekanisk revaskularisering), men uden
celle terapi. Dette er en faktor, der er vigtig at tage
højde for, når ikke-kontrollerede interventions forsøg
skal vurderes.
Endelig fandt vi, at ex vivo mærkning af celler med
indium-111 med henblik på in vivo visualisering efter
myokardiel injektion er problematisk. En stor del af
mærkningen forblev i hjertet selvom cellerne i vores
studie var døde. I humane studier er det vanskeligt at
afgøre, om cellerne forbliver levende efter injektion, og
det vil derfor være vanskeligt at afgøre, om vedvarende
indium aktivitet i myokardiet stammer fra viable celler
eller ej.
Celle baseret terapi er fortsat i den eksplorative fase,
men på baggrund af det store arbejde, der i øjeblikket
bliver lagt inden for dette felt, er det forhåbningen, at
terapiens kliniske relevans inden for en overskuelig
fremtid kan vurderes. I sidste ende vil dette kræve
gennemførelse af store randomiserede, dobbeltblindede,
placebokontrollerede studier med »hårde« kliniske
endepunkter som mortalitet og morbiditet.

- 37 -
REFERENCES
1. McCulloch EA, Till JE. The Radiation Sensitivity of Normal
Mouse Bone Marrow Cells, Determined by Quantitative
Marrow Transplantation into Irradiated Mice. Radiat Res
1960;13:115-25.
2. Asahara T, Masuda H, Takahashi T, Kalka C, Pastore C,
Silver M, Kearne M, Magner M, Isner JM. Bone Marrow
Origin of Endothelial Progenitor Cells Responsible for
Postnatal Vasculogenesis in Physiological and Pathological
Neovascularization. Circ Res 1999;85:221-8.
3. Asahara T, Murohara T, Sullivan A, Silver M, van der ZR, Li
T, Witzenbichler B, Schatteman G, Isner JM. Isolation of
Putative Progenitor Endothelial Cells for Angiogenesis.
Science 1997;275:964-7.
4. Orlic D, Kajstura J, Chimenti S, Jakoniuk I, Anderson SM, Li
B, Pickel J, McKay R, Nadal-Ginard B, Bodine DM, Leri A,
Anversa P. Bone Marrow Cells Regenerate Infarcted
Myocardium. Nature 2001;410:701-5.
5. Nygren JM, Jovinge S, Breitbach M, Sawen P, Roll W,
Hescheler J, Taneera J, Fleischmann BK, Jacobsen SE. Bone
Marrow-Derived Hematopoietic Cells Generate
Cardiomyocytes at a Low Frequency Through Cell Fusion,
but Not Transdifferentiation. Nat Med 2004;10:494-501.
6. Murry CE, Soonpaa MH, Reinecke H, Nakajima H, Nakajima
HO, Rubart M, Pasumarthi KB, Virag JI, Bartelmez SH,
Poppa V, Bradford G, Dowell JD, Williams DA, Field LJ.
Haematopoietic Stem Cells Do Not Transdifferentiate into
Cardiac Myocytes in Myocardial Infarcts. Nature
2004;428:664-8.
7. Kastrup J, Jørgensen E, Drvota V. Vascular Growth Factor
and Gene Therapy to Induce New Vessels in the Ischemic
Myocardium. Therapeutic Angiogenesis. Scand Cardiovasc J
2001;35:291-6.
8. Hendel RC, Henry TD, Rocha-Singh K, Isner JM, Kereiakes
DJ, Giordano FJ, Simons M, Bonow RO. Effect of
Intracoronary Recombinant Human Vascular Endothelial
Growth Factor on Myocardial Perfusion: Evidence for a
Dose-Dependent Effect. Circulation 2000;101:118-21.
9. Henry TD, Annex BH, McKendall GR, Azrin MA, Lopez JJ,
Giordano FJ, Shah PK, Willerson JT, Benza RL, Berman DS,
Gibson CM, Bajamonde A, Rundle AC, Fine J, McCluskey ER.
The VIVA Trial: Vascular Endothelial Growth Factor in
Ischemia for Vascular Angiogenesis. Circulation
2003;107:1359-65.
10. Henry TD, Rocha-Singh K, Isner JM, Kereiakes DJ, Giordano
FJ, Simons M, Losordo DW, Hendel RC, Bonow RO, Eppler
SM, Zioncheck TF, Holmgren EB, McCluskey ER.
Intracoronary Administration of Recombinant Human
Vascular Endothelial Growth Factor to Patients With
Coronary Artery Disease. Am Heart J 2001;142:872-80.
11. Schumacher B, Pecher P, von Specht BU, Stegmann T.
Induction of Neoangiogenesis in Ischemic Myocardium by
Human Growth Factors: First Clinical Results of a New
Treatment of Coronary Heart Disease. Circulation
1998;97:645-50.
12. Laham RJ, Chronos NA, Pike M, Leimbach ME, Udelson JE,
Pearlman JD, Pettigrew RI, Whitehouse MJ, Yoshizawa C,
Simons M. Intracoronary Basic Fibroblast Growth Factor
(FGF-2) in Patients With Severe Ischemic Heart Disease:
Results of a Phase I Open-Label Dose Escalation Study. J
Am Coll Cardiol 2000;36:2132-9.
13. Laham RJ, Sellke FW, Edelman ER, Pearlman JD, Ware JA,
Brown DL, Gold JP, Simons M. Local Perivascular Delivery of
Basic Fibroblast Growth Factor in Patients Undergoing
Coronary Bypass Surgery: Results of a Phase I
Randomized, Double-Blind, Placebo-Controlled Trial.
Circulation 1999;100:1865-71.
14. Simons M, Annex BH, Laham RJ, Kleiman N, Henry T,
Dauerman H, Udelson JE, Gervino EV, Pike M, Whitehouse
MJ, Moon T, Chronos NA. Pharmacological Treatment of
Coronary Artery Disease With Recombinant Fibroblast
Growth Factor-2: Double-Blind, Randomized, Controlled
Clinical Trial. Circulation 2002;105:788-93.
15. Sellke FW, Laham RJ, Edelman ER, Pearlman JD, Simons M.
Therapeutic Angiogenesis With Basic Fibroblast Growth
Factor: Technique and Early Results. Ann Thorac Surg
1998;65:1540-4.
16. Unger EF, Goncalves L, Epstein SE, Chew EY, Trapnell CB,
Cannon RO, III, Quyyumi AA. Effects of a Single
Intracoronary Injection of Basic Fibroblast Growth Factor in
Stable Angina Pectoris. Am J Cardiol 2000;85:1414-9.
17. Ruel M, Laham RJ, Parker JA, Post MJ, Ware JA, Simons M,
Sellke FW. Long-Term Effects of Surgical Angiogenic
Therapy With Fibroblast Growth Factor 2 Protein. J Thorac
Cardiovasc Surg 2002;124:28-34.
18. Udelson JE, Dilsizian V, Laham RJ, Chronos N, Vansant J,
Blais M, Galt JR, Pike M, Yoshizawa C, Simons M.
Therapeutic Angiogenesis With Recombinant Fibroblast
Growth Factor-2 Improves Stress and Rest Myocardial
Perfusion Abnormalities in Patients With Severe
Symptomatic Chronic Coronary Artery Disease. Circulation
2000;102:1605-10.
19. Yla-Herttuala S, Alitalo K. Gene Transfer As a Tool to
Induce Therapeutic Vascular Growth. Nat Med 2003;9:694-
701.
20. Symes JF, Losordo DW, Vale PR, Lathi KG, Esakof DD,
Mayskiy M, Isner JM. Gene Therapy With Vascular
Endothelial Growth Factor for Inoperable Coronary Artery
Disease. Ann Thorac Surg 1999;68:830-6.
21. Rosengart TK, Lee LY, Patel SR, Sanborn TA, Parikh M,
Bergman GW, Hachamovitch R, Szulc M, Kligfield PD, Okin

- 38 -
PM, Hahn RT, Devereux RB, Post MR, Hackett NR, Foster T,
Grasso TM, Lesser ML, Isom OW, Crystal RG. Angiogenesis
Gene Therapy: Phase I Assessment of Direct
Intramyocardial Administration of an Adenovirus Vector
Expressing VEGF121 CDNA to Individuals With Clinically
Significant Severe Coronary Artery Disease. Circulation
1999;100:468-74.
22. Grines CL, Watkins MW, Helmer G, Penny W, Brinker J,
Marmur JD, West A, Rade JJ, Marrott P, Hammond HK,
Engler RL. Angiogenic Gene Therapy (AGENT) Trial in
Patients With Stable Angina Pectoris. Circulation
2002;105:1291-7.
23. Losordo DW, Vale PR, Hendel RC, Milliken CE, Fortuin FD,
Cummings N, Schatz RA, Asahara T, Isner JM, Kuntz RE.
Phase 1/2 Placebo-Controlled, Double-Blind, Dose-
Escalating Trial of Myocardial Vascular Endothelial Growth
Factor 2 Gene Transfer by Catheter Delivery in Patients
With Chronic Myocardial Ischemia. Circulation
2002;105:2012-8.
24. Sylvén C, Sarkar N, Ruck A, Drvota V, Hassan SY, Lind B,
Nygren A, Kallner Q, Blomberg P, van der LJ, Lindblom D,
Brodin LA, Islam KB. Myocardial Doppler Tissue Velocity
Improves Following Myocardial Gene Therapy With VEGF-
A165 Plasmid in Patients With Inoperable Angina Pectoris.
Coron Artery Dis 2001;12:239-43.
25. Vale PR, Losordo DW, Milliken CE, McDonald MC, Gravelin
LM, Curry CM, Esakof DD, Maysky M, Symes JF, Isner JM.
Randomized, Single-Blind, Placebo-Controlled Pilot Study of
Catheter-Based Myocardial Gene Transfer for Therapeutic
Angiogenesis Using Left Ventricular Electromechanical
Mapping in Patients With Chronic Myocardial Ischemia.
Circulation 2001;103:2138-43.
26. Stewart DJ, Hilton JD, Arnold JM, Gregoire J, Rivard A,
Archer SL, Charbonneau F, Cohen E, Curtis M, Buller CE,
Mendelsohn FO, Dib N, Page P, Ducas J, Plante S, Sullivan
J, Macko J, Rasmussen C, Kessler PD, Rasmussen HS.
Angiogenic Gene Therapy in Patients With
Nonrevascularizable Ischemic Heart Disease: a Phase 2
Randomized, Controlled Trial of AdVEGF(121) (AdVEGF121)
Versus Maximum Medical Treatment. Gene Ther
2006;13:1503-11.
27. Kastrup J, Jørgensen E, Ruck A, Tägil K, Glogar D, Ruzyllo
W, Bøtker HE, Dudek D, Drvota V, Hesse B, Thuesen L,
Blomberg P, Gyöngyösi M, Sylvén C. Direct Intramyocardial
Plasmid Vascular Endothelial Growth Factor-A165 Gene
Therapy in Patients With Stable Severe Angina Pectoris A
Randomized Double-Blind Placebo-Controlled Study: the
Euroinject One Trial. J Am Coll Cardiol 2005;45:982-8.
28. Kastrup J, Jørgensen E, Drvota V, Thuesen L, Bøtker HE,
Gyöngyösi M, Glogar D, Rück A, Bin Islam K, Sylvén C.
Intramyocardial Injection of Genes With a Novel
Percutaneous Technique: Initial Safety Data of the
Euroinject One Study. Heart Drug 2001;1:299-304.
29. Gyöngyösi M, Khorsand A, Zamini S, Sperker W, Strehblow
C, Kastrup J, Jørgensen E, Hesse B, Tägil K, Bøtker HE,
Ruzyllo W, Teresinska A, Dudek D, Hubalewska A, Ruck A,
Nielsen SS, Graf S, Mundigler G, Novak J, Sochor H, Maurer
G, Glogar D, Sylvén C. NOGA-Guided Analysis of Regional
Myocardial Perfusion Abnormalities Treated With
Intramyocardial Injections of Plasmid Encoding Vascular
Endothelial Growth Factor A-165 in Patients With Chronic
Myocardial Ischemia: Subanalysis of the EUROINJECT-ONE
Multicenter Double-Blind Randomized Study. Circulation
2005;112:I157-I165.
30. Kajstura J, Rota M, Whang B, Cascapera S, Hosoda T,
Bearzi C, Nurzynska D, Kasahara H, Zias E, Bonafe M,
Nadal-Ginard B, Torella D, Nascimbene A, Quaini F,
Urbanek K, Leri A, Anversa P. Bone Marrow Cells
Differentiate in Cardiac Cell Lineages After Infarction
Independently of Cell Fusion. Circ Res 2005;96:127-37.
31. Shintani S, Murohara T, Ikeda H, Ueno T, Honma T, Katoh
A, Sasaki K, Shimada T, Oike Y, Imaizumi T. Mobilization of
Endothelial Progenitor Cells in Patients With Acute
Myocardial Infarction. Circulation 2001;103:2776-9.
32. Wang Y, Johnsen HE, Mortensen S, Bindslev L, Ripa RS,
Haack-Sørensen M, Jørgensen E, Fang W, Kastrup J.
Changes in Circulating Mesenchymal Stem Cells, Stem Cell
Homing Factor, and Vascular Growth Factors in Patients
With Acute ST Elevation Myocardial Infarction Treated With
Primary Percutaneous Coronary Intervention. Heart
2006;92:768-74.
33. Wojakowski W, Tendera M, Michalowska A, Majka M, Kucia
M, Maslankiewicz K, Wyderka R, Ochala A, Ratajczak MZ.
Mobilization of CD34/CXCR4+, CD34/CD117+, C-Met+
Stem Cells, and Mononuclear Cells Expressing Early
Cardiac, Muscle, and Endothelial Markers into Peripheral
Blood in Patients With Acute Myocardial Infarction.
Circulation 2004;110:3213-20.
34. Leone AM, Rutella S, Bonanno G, Contemi AM, de Ritis DG,
Giannico MB, Rebuzzi AG, Leone G, Crea F. Endogenous G-
CSF and CD34+ Cell Mobilization After Acute Myocardial
Infarction. Int J Cardiol 2006;111:202-8.
35. Werner N, Kosiol S, Schiegl T, Ahlers P, Walenta K, Link A,
Bohm M, Nickenig G. Circulating Endothelial Progenitor
Cells and Cardiovascular Outcomes. N Engl J Med
2005;353:999-1007.
36. Kocher AA, Schuster MD, Szabolcs MJ, Takuma S, Burkhoff
D, Wang J, Homma S, Edwards NM, Itescu S.
Neovascularization of Ischemic Myocardium by Human
Bone-Marrow-Derived Angioblasts Prevents Cardiomyocyte
Apoptosis, Reduces Remodeling and Improves Cardiac
Function. Nat Med 2001;7:430-6.
37. Tse HF, Kwong YL, Chan JK, Lo G, Ho CL, Lau CP.
Angiogenesis in Ischaemic Myocardium by Intramyocardial
Autologous Bone Marrow Mononuclear Cell Implantation.
Lancet 2003;361:47-9.

- 39 -
38. Dohmann HF, Perin EC, Takiya CM, Silva GV, Silva SA,
Sousa AL, Mesquita CT, Rossi MI, Pascarelli BM, Assis IM,
Dutra HS, Assad JA, Castello-Branco RV, Drummond C,
Dohmann HJ, Willerson JT, Borojevic R. Transendocardial
Autologous Bone Marrow Mononuclear Cell Injection in
Ischemic Heart Failure: Postmortem Anatomicopathologic
and Immunohistochemical Findings. Circulation
2005;112:521-6.
39. Strauer BE, Brehm M, Zeus T, Bartsch T, Schannwell C,
Antke C, Sorg RV, Kogler G, Wernet P, Muller HW,
Kostering M. Regeneration of Human Infarcted Heart
Muscle by Intracoronary Autologous Bone Marrow Cell
Transplantation in Chronic Coronary Artery Disease: the
IACT Study. J Am Coll Cardiol 2005;46:1651-8.
40. Fuchs S, Kornowski R, Weisz G, Satler LF, Smits PC,
Okubagzi P, Baffour R, Aggarwal A, Weissman NJ,
Cerqueira M, Waksman R, Serrruys P, Battler A, Moses JW,
Leon MB, Epstein SE. Safety and Feasibility of
Transendocardial Autologous Bone Marrow Cell
Transplantation in Patients With Advanced Heart Disease.
Am J Cardiol 2006;97:823-9.
41. Fuchs S, Satler LF, Kornowski R, Okubagzi P, Weisz G,
Baffour R, Waksman R, Weissman NJ, Cerqueira M, Leon
MB, Epstein SE. Catheter-Based Autologous Bone Marrow
Myocardial Injection in No-Option Patients With Advanced
Coronary Artery Disease: a Feasibility Study. J Am Coll
Cardiol 2003;41:1721-4.
42. Perin EC, Dohmann HF, Borojevic R, Silva SA, Sousa AL,
Mesquita CT, Rossi MI, Carvalho AC, Dutra HS, Dohmann
HJ, Silva GV, Belem L, Vivacqua R, Rangel FO, Esporcatte
R, Geng YJ, Vaughn WK, Assad JA, Mesquita ET, Willerson
JT. Transendocardial, Autologous Bone Marrow Cell
Transplantation for Severe, Chronic Ischemic Heart Failure.
Circulation 2003;107:2294-302.
43. Perin EC, Dohmann HF, Borojevic R, Silva SA, Sousa AL,
Silva GV, Mesquita CT, Belem L, Vaughn WK, Rangel FO,
Assad JA, Carvalho AC, Branco RV, Rossi MI, Dohmann HJ,
Willerson JT. Improved Exercise Capacity and Ischemia 6
and 12 Months After Transendocardial Injection of
Autologous Bone Marrow Mononuclear Cells for Ischemic
Cardiomyopathy. Circulation 2004;110:II213-II218.
44. Strauer BE, Brehm M, Zeus T, Kostering M, Hernandez A,
Sorg RV, Kogler G, Wernet P. Repair of Infarcted
Myocardium by Autologous Intracoronary Mononuclear
Bone Marrow Cell Transplantation in Humans. Circulation
2002;106:1913-8.
45. Stamm C, Westphal B, Kleine HD, Petzsch M, Kittner C,
Klinge H, Schumichen C, Nienaber CA, Freund M, Steinhoff
G. Autologous Bone-Marrow Stem-Cell Transplantation for
Myocardial Regeneration. Lancet 2003;361:45-6.
46. Assmus B, Schächinger V, Teupe C, Britten M, Lehmann R,
Dobert N, Grunwald F, Aicher A, Urbich C, Martin H, Hoelzer
D, Dimmeler S, Zeiher AM. Transplantation of Progenitor
Cells and Regeneration Enhancement in Acute Myocardial
Infarction (TOPCARE-AMI). Circulation 2002;106:3009-17.
47. Schächinger V, Assmus B, Britten MB, Honold J, Lehmann
R, Teupe C, Abolmaali ND, Vogl TJ, Hofmann WK, Martin H,
Dimmeler S, Zeiher AM. Transplantation of Progenitor Cells
and Regeneration Enhancement in Acute Myocardial
Infarction: Final One-Year Results of the TOPCARE-AMI
Trial. J Am Coll Cardiol 2004;44:1690-9.
48. Wollert KC, Meyer GP, Lotz J, Ringes-Lichtenberg S, Lippolt
P, Breidenbach C, Fichtner S, Korte T, Hornig B, Messinger
D, Arseniev L, Hertenstein B, Ganser A, Drexler H.
Intracoronary Autologous Bone-Marrow Cell Transfer After
Myocardial Infarction: the BOOST Randomised Controlled
Clinical Trial. Lancet 2004;364:141-8.
49. Fernandez-Aviles F, San Roman JA, Garcia-Frade J,
Fernandez ME, Penarrubia MJ, de la FL, Gomez-Bueno M,
Cantalapiedra A, Fernandez J, Gutierrez O, Sanchez PL,
Hernandez C, Sanz R, Garcia-Sancho J, Sanchez A.
Experimental and Clinical Regenerative Capability of Human
Bone Marrow Cells After Myocardial Infarction. Circ Res
2004;95:742-8.
50. Schächinger V, Erbs S, Elsasser A, Haberbosch W,
Hambrecht R, Holschermann H, Yu J, Corti R, Mathey DG,
Hamm CW, Suselbeck T, Assmus B, Tonn T, Dimmeler S,
Zeiher AM. Intracoronary Bone Marrow-Derived Progenitor
Cells in Acute Myocardial Infarction. N Engl J Med
2006;355:1210-21.
51. Lunde K, Solheim S, Aakhus S, Arnesen H, Abdelnoor M,
Egeland T, Endresen K, Ilebekk A, Mangschau A, Fjeld JG,
Smith HJ, Taraldsrud E, Grogaard HK, Bjornerheim R,
Brekke M, Muller C, Hopp E, Ragnarsson A, Brinchmann JE,
Forfang K. Intracoronary Injection of Mononuclear Bone
Marrow Cells in Acute Myocardial Infarction. N Engl J Med
2006;355:1199-209.
52. Janssens S, Dubois C, Bogaert J, Theunissen K, Deroose C,
Desmet W, Kalantzi M, Herbots L, Sinnaeve P, Dens J,
Maertens J, Rademakers F, Dymarkowski S, Gheysens O,
Van Cleemput J, Bormans G, Nuyts J, Belmans A,
Mortelmans L, Boogaerts M, Van de WF. Autologous Bone
Marrow-Derived Stem-Cell Transfer in Patients With ST-
Segment Elevation Myocardial Infarction: Double-Blind,
Randomised Controlled Trial. Lancet 2006;367:113-21.
53. Tendera M, Wojakowski W, Ruzyllo W, Chojnowska L,
Kepka C, Tracz W, Musialek P, Piwowarska W, Nessler J,
Buszman P, Grajek S, Breborowicz P, Majka M, Ratajczak
MZ. Intracoronary Infusion of Bone Marrow-Derived
Selected CD34+CXCR4+ Cells and Non-Selected
Mononuclear Cells in Patients With Acute STEMI and
Reduced Left Ventricular Ejection Fraction: Results of
Randomized, Multicentre Myocardial Regeneration by
Intracoronary Infusion of Selected Population of Stem Cells
in Acute Myocardial Infarction (REGENT) Trial. Eur Heart J
2009;30:1313-21.

- 40 -
54. Hirsch A, Nijveldt R, van d, V, Tijssen JG, van der Giessen
WJ, Tio RA, Waltenberger J, Ten Berg JM, Doevendans PA,
Aengevaeren WR, Zwaginga JJ, Biemond BJ, van Rossum
AC, Piek JJ, Zijlstra F. Intracoronary Infusion of
Mononuclear Cells From Bone Marrow or Peripheral Blood
Compared With Standard Therapy in Patients After Acute
Myocardial Infarction Treated by Primary Percutaneous
Coronary Intervention: Results of the Randomized
Controlled HEBE Trial. Eur Heart J 2010 Dec 10. [Epub
ahead of print]
55. Schächinger V, Erbs S, Elsasser A, Haberbosch W,
Hambrecht R, Holschermann H, Yu J, Corti R, Mathey DG,
Hamm CW, Suselbeck T, Werner N, Haase J, Neuzner J,
Germing A, Mark B, Assmus B, Tonn T, Dimmeler S, Zeiher
AM. Improved Clinical Outcome After Intracoronary
Administration of Bone-Marrow-Derived Progenitor Cells in
Acute Myocardial Infarction: Final 1-Year Results of the
REPAIR-AMI Trial. Eur Heart J 2006;27:2775-83.
56. Assmus B, Rolf A, Erbs S, Elsasser A, Haberbosch W,
Hambrecht R, Tillmanns H, Yu J, Corti R, Mathey DG,
Hamm CW, Suselbeck T, Tonn T, Dimmeler S, Dill T, Zeiher
AM, Schachinger V. Clinical Outcome 2 Years After
Intracoronary Administration of Bone Marrow-Derived
Progenitor Cells in Acute Myocardial Infarction. Circ Heart
Fail 2010;3:89-96.
57. Meyer GP, Wollert KC, Lotz J, Steffens J, Lippolt P, Fichtner
S, Hecker H, Schaefer A, Arseniev L, Hertenstein B, Ganser
A, Drexler H. Intracoronary Bone Marrow Cell Transfer After
Myocardial Infarction: Eighteen Months' Follow-Up Data
From the Randomized, Controlled BOOST (BOne MarrOw
Transfer to Enhance ST-Elevation Infarct Regeneration)
Trial. Circulation 2006;113:1287-94.
58. Erbs S, Linke A, Schachinger V, Assmus B, Thiele H,
Diederich KW, Hoffmann C, Dimmeler S, Tonn T,
Hambrecht R, Zeiher AM, Schuler G. Restoration of
Microvascular Function in the Infarct-Related Artery by
Intracoronary Transplantation of Bone Marrow Progenitor
Cells in Patients With Acute Myocardial Infarction: the
Doppler Substudy of the Reinfusion of Enriched Progenitor
Cells and Infarct Remodeling in Acute Myocardial Infarction
(REPAIR-AMI) Trial. Circulation 2007;116:366-74.
59. van Ramshorst J., Bax JJ, Beeres SL, bbets-Schneider P,
Roes SD, Stokkel MP, de RA, Fibbe WE, Zwaginga JJ,
Boersma E, Schalij MJ, Atsma DE. Intramyocardial Bone
Marrow Cell Injection for Chronic Myocardial Ischemia: a
Randomized Controlled Trial. JAMA 2009;301:1997-2004.
60. Ripa RS, Wang Y, Jørgensen E, Kastrup J. [Therapy With
Stem Cells for Acute Ischemic Heart Disease: Myocardial
Regeneration?]. Ugeskr Laeger 2007;169:119-22.
61. Johnsen HE. Clinical Practice and Future Needs in
Recombinant Human Granulocyte Colony-Stimulating Factor
Treatment: a Review of Randomized Trials in Clinical
Haemato-Oncology. J Int Med Res 2001;29:87-99.
62. Avalos BR. Molecular Analysis of the Granulocyte Colony-
Stimulating Factor Receptor. Blood 1996;88:761-77.
63. Dong F, Larner AC. Activation of Akt Kinase by Granulocyte
Colony-Stimulating Factor (G-CSF): Evidence for the Role of
a Tyrosine Kinase Activity Distinct From the Janus Kinases.
Blood 2000;95:1656-62.
64. Anderlini P, Donato M, Chan KW, Huh YO, Gee AP, Lauppe
MJ, Champlin RE, Korbling M. Allogeneic Blood Progenitor
Cell Collection in Normal Donors After Mobilization With
Filgrastim: the M.D. Anderson Cancer Center Experience.
Transfusion 1999;39:555-60.
65. Nagasawa T, Kikutani H, Kishimoto T. Molecular Cloning
and Structure of a Pre-B-Cell Growth-Stimulating Factor.
Proc Natl Acad Sci U S A 1994;91:2305-9.
66. Deichmann M, Kronenwett R, Haas R. Expression of the
Human Immunodeficiency Virus Type-1 Coreceptors CXCR-
4 (Fusin, LESTR) and CKR-5 in CD34+ Hematopoietic
Progenitor Cells. Blood 1997;89:3522-8.
67. Petit I, Szyper-Kravitz M, Nagler A, Lahav M, Peled A,
Habler L, Ponomaryov T, Taichman RS, renzana-Seisdedos
F, Fujii N, Sandbank J, Zipori D, Lapidot T. G-CSF Induces
Stem Cell Mobilization by Decreasing Bone Marrow SDF-1
and Up-Regulating CXCR4. Nat Immunol 2002;3:687-94.
68. Semerad CL, Christopher MJ, Liu F, Short B, Simmons PJ,
Winkler I, Levesque JP, Chappel J, Ross FP, Link DC. G-CSF
Potently Inhibits Osteoblast Activity and CXCL12 MRNA
Expression in the Bone Marrow. Blood 2005;106:3020-7.
69. Kawabata K, Ujikawa M, Egawa T, Kawamoto H, Tachibana
K, Iizasa H, Katsura Y, Kishimoto T, Nagasawa T. A Cell-
Autonomous Requirement for CXCR4 in Long-Term
Lymphoid and Myeloid Reconstitution. Proc Natl Acad Sci U
S A 1999;96:5663-7.
70. Flomenberg N, DiPersio J, Calandra G. Role of CXCR4
Chemokine Receptor Blockade Using AMD3100 for
Mobilization of Autologous Hematopoietic Progenitor Cells.
Acta Haematol 2005;114:198-205.
71. Nervi B, Link DC, DiPersio JF. Cytokines and Hematopoietic
Stem Cell Mobilization. J Cell Biochem 2006;99:690-705.
72. Levesque JP, Hendy J, Takamatsu Y, Williams B, Winkler
IG, Simmons PJ. Mobilization by Either Cyclophosphamide
or Granulocyte Colony-Stimulating Factor Transforms the
Bone Marrow into a Highly Proteolytic Environment. Exp
Hematol 2002;30:440-9.
73. Levesque JP, Takamatsu Y, Nilsson SK, Haylock DN,
Simmons PJ. Vascular Cell Adhesion Molecule-1 (CD106) Is
Cleaved by Neutrophil Proteases in the Bone Marrow
Following Hematopoietic Progenitor Cell Mobilization by
Granulocyte Colony-Stimulating Factor. Blood
2001;98:1289-97.
74. Heissig B, Hattori K, Dias S, Friedrich M, Ferris B, Hackett
NR, Crystal RG, Besmer P, Lyden D, Moore MA, Werb Z,

- 41 -
Rafii S. Recruitment of Stem and Progenitor Cells From the
Bone Marrow Niche Requires MMP-9 Mediated Release of
Kit-Ligand. Cell 2002;109:625-37.
75. Levesque JP, Liu F, Simmons PJ, Betsuyaku T, Senior RM,
Pham C, Link DC. Characterization of Hematopoietic
Progenitor Mobilization in Protease-Deficient Mice. Blood
2004;104:65-72.
76. Harada M, Qin Y, Takano H, Minamino T, Zou Y, Toko H,
Ohtsuka M, Matsuura K, Sano M, Nishi J, Iwanaga K,
Akazawa H, Kunieda T, Zhu W, Hasegawa H, Kunisada K,
Nagai T, Nakaya H, Yamauchi-Takihara K, Komuro I. G-CSF
Prevents Cardiac Remodeling After Myocardial Infarction by
Activating the Jak-Stat Pathway in Cardiomyocytes. Nat
Med 2005;11:305-11.
77. Hilfiker-Kleiner D, Hilfiker A, Fuchs M, Kaminski K, Schaefer
A, Schieffer B, Hillmer A, Schmiedl A, Ding Z, Podewski E,
Podewski E, Poli V, Schneider MD, Schulz R, Park JK,
Wollert KC, Drexler H. Signal Transducer and Activator of
Transcription 3 Is Required for Myocardial Capillary Growth,
Control of Interstitial Matrix Deposition, and Heart
Protection From Ischemic Injury. Circ Res 2004;95:187-95.
78. Yamauchi-Takihara K, Kishimoto T. A Novel Role for STAT3
in Cardiac Remodeling. Trends Cardiovasc Med
2000;10:298-303.
79. Ueda K, Takano H, Hasegawa H, Niitsuma Y, Qin Y, Ohtsuka
M, Komuro I. Granulocyte Colony Stimulating Factor
Directly Inhibits Myocardial Ischemia-Reperfusion Injury
Through Akt-Endothelial NO Synthase Pathway. Arterioscler
Thromb Vasc Biol 2006;26:e108-e113.
80. Boneberg EM, Hareng L, Gantner F, Wendel A, Hartung T.
Human Monocytes Express Functional Receptors for
Granulocyte Colony-Stimulating Factor That Mediate
Suppression of Monokines and Interferon-Gamma. Blood
2000;95:270-6.
81. Hartung T. Anti-Inflammatory Effects of Granulocyte
Colony-Stimulating Factor. Curr Opin Hematol 1998;5:221-
5.
82. Misao Y, Takemura G, Arai M, Ohno T, Onogi H, Takahashi
T, Minatoguchi S, Fujiwara T, Fujiwara H. Importance of
Recruitment of Bone Marrow-Derived CXCR4+ Cells in Post-
Infarct Cardiac Repair Mediated by G-CSF. Cardiovasc Res
2006;71:455-65.
83. Anderlini P, Przepiorka D, Seong D, Miller P, Sundberg J,
Lichtiger B, Norfleet F, Chan KW, Champlin R, Korbling M.
Clinical Toxicity and Laboratory Effects of Granulocyte-
Colony-Stimulating Factor (Filgrastim) Mobilization and
Blood Stem Cell Apheresis From Normal Donors, and
Analysis of Charges for the Procedures. Transfusion
1996;36:590-5.
84. Cavallaro AM, Lilleby K, Majolino I, Storb R, Appelbaum FR,
Rowley SD, Bensinger WI. Three to Six Year Follow-Up of
Normal Donors Who Received Recombinant Human
Granulocyte Colony-Stimulating Factor. Bone Marrow
Transplant 2000;25:85-9.
85. Carmeliet P. Mechanisms of Angiogenesis and
Arteriogenesis. Nat Med 2000;6:389-95.
86. Lancrin C, Sroczynska P, Stephenson C, Allen T, Kouskoff V,
Lacaud G. The Haemangioblast Generates Haematopoietic
Cells Through a Haemogenic Endothelium Stage. Nature
2009;457:892-5.
87. Ferguson JE, III, Kelley RW, Patterson C. Mechanisms of
Endothelial Differentiation in Embryonic Vasculogenesis.
Arterioscler Thromb Vasc Biol 2005;25:2246-54.
88. McGrath KE, Koniski AD, Maltby KM, McGann JK, Palis J.
Embryonic Expression and Function of the Chemokine SDF-
1 and Its Receptor, CXCR4. Dev Biol 1999;213:442-56.
89. Cox CM, Poole TJ. Angioblast Differentiation Is Influenced
by the Local Environment: FGF-2 Induces Angioblasts and
Patterns Vessel Formation in the Quail Embryo. Dev Dyn
2000;218:371-82.
90. Carmeliet P, Ferreira V, Breier G, Pollefeyt S, Kieckens L,
Gertsenstein M, Fahrig M, Vandenhoeck A, Harpal K,
Eberhardt C, Declercq C, Pawling J, Moons L, Collen D,
Risau W, Nagy A. Abnormal Blood Vessel Development and
Lethality in Embryos Lacking a Single VEGF Allele. Nature
1996;380:435-9.
91. Tomanek RJ, Christensen LP, Simons M, Murakami M,
Zheng W, Schatteman GC. Embryonic Coronary
Vasculogenesis and Angiogenesis Are Regulated by
Interactions Between Multiple FGFs and VEGF and Are
Influenced by Mesenchymal Stem Cells. Dev Dyn
2010;239:3182-91.
92. Takahashi T, Kalka C, Masuda H, Chen D, Silver M, Kearney
M, Magner M, Isner JM, Asahara T. Ischemia- and Cytokine-
Induced Mobilization of Bone Marrow-Derived Endothelial
Progenitor Cells for Neovascularization. Nat Med
1999;5:434-8.
93. Asahara T, Takahashi T, Masuda H, Kalka C, Chen D,
Iwaguro H, Inai Y, Silver M, Isner JM. VEGF Contributes to
Postnatal Neovascularization by Mobilizing Bone Marrow-
Derived Endothelial Progenitor Cells. EMBO J
1999;18:3964-72.
94. Hattori K, Dias S, Heissig B, Hackett NR, Lyden D, Tateno
M, Hicklin DJ, Zhu Z, Witte L, Crystal RG, Moore MA, Rafii
S. Vascular Endothelial Growth Factor and Angiopoietin-1
Stimulate Postnatal Hematopoiesis by Recruitment of
Vasculogenic and Hematopoietic Stem Cells. J Exp Med
2001;193:1005-14.
95. Ceradini DJ, Kulkarni AR, Callaghan MJ, Tepper OM,
Bastidas N, Kleinman ME, Capla JM, Galiano RD, Levine JP,
Gurtner GC. Progenitor Cell Trafficking Is Regulated by
Hypoxic Gradients Through HIF-1 Induction of SDF-1. Nat
Med 2004;10:858-64.

- 42 -
96. Kaelin WG, Jr., Ratcliffe PJ. Oxygen Sensing by Metazoans:
the Central Role of the HIF Hydroxylase Pathway. Mol Cell
2008;30:393-402.
97. Kelly BD, Hackett SF, Hirota K, Oshima Y, Cai Z, Berg-
Dixon S, Rowan A, Yan Z, Campochiaro PA, Semenza GL.
Cell Type-Specific Regulation of Angiogenic Growth Factor
Gene Expression and Induction of Angiogenesis in
Nonischemic Tissue by a Constitutively Active Form of
Hypoxia-Inducible Factor 1. Circ Res 2003;93:1074-81.
98. Ruhrberg C, Gerhardt H, Golding M, Watson R, Ioannidou
S, Fujisawa H, Betsholtz C, Shima DT. Spatially Restricted
Patterning Cues Provided by Heparin-Binding VEGF-A
Control Blood Vessel Branching Morphogenesis. Genes Dev
2002;16:2684-98.
99. Gerhardt H, Golding M, Fruttiger M, Ruhrberg C, Lundkvist
A, Abramsson A, Jeltsch M, Mitchell C, Alitalo K, Shima D,
Betsholtz C. VEGF Guides Angiogenic Sprouting Utilizing
Endothelial Tip Cell Filopodia. J Cell Biol 2003;161:1163-77.
100. Hellstrom M, Phng LK, Hofmann JJ, Wallgard E, Coultas L,
Lindblom P, Alva J, Nilsson AK, Karlsson L, Gaiano N, Yoon
K, Rossant J, Iruela-Arispe ML, Kalen M, Gerhardt H,
Betsholtz C. Dll4 Signalling Through Notch1 Regulates
Formation of Tip Cells During Angiogenesis. Nature
2007;445:776-80.
101. Yana I, Sagara H, Takaki S, Takatsu K, Nakamura K, Nakao
K, Katsuki M, Taniguchi S, Aoki T, Sato H, Weiss SJ, Seiki
M. Crosstalk Between Neovessels and Mural Cells Directs
the Site-Specific Expression of MT1-MMP to Endothelial Tip
Cells. J Cell Sci 2007;120:1607-14.
102. Fantin A, Vieira JM, Gestri G, Denti L, Schwarz Q,
Prykhozhij S, Peri F, Wilson SW, Ruhrberg C. Tissue
Macrophages Act As Cellular Chaperones for Vascular
Anastomosis Downstream of VEGF-Mediated Endothelial Tip
Cell Induction. Blood 2010;116:829-40.
103. Demicheva E, Hecker M, Korff T. Stretch-Induced Activation
of the Transcription Factor Activator Protein-1 Controls
Monocyte Chemoattractant Protein-1 Expression During
Arteriogenesis. Circ Res 2008;103:477-84.
104. Garcia-Cardena G, Comander J, Anderson KR, Blackman
BR, Gimbrone MA, Jr. Biomechanical Activation of Vascular
Endothelium As a Determinant of Its Functional Phenotype.
Proc Natl Acad Sci U S A 2001;98:4478-85.
105. Lee CW, Stabile E, Kinnaird T, Shou M, Devaney JM,
Epstein SE, Burnett MS. Temporal Patterns of Gene
Expression After Acute Hindlimb Ischemia in Mice: Insights
into the Genomic Program for Collateral Vessel
Development. J Am Coll Cardiol 2004;43:474-82.
106. Scholz D, Ito W, Fleming I, Deindl E, Sauer A, Wiesnet M,
Busse R, Schaper J, Schaper W. Ultrastructure and
Molecular Histology of Rabbit Hind-Limb Collateral Artery
Growth (Arteriogenesis). Virchows Arch 2000;436:257-70.
107. Cai W, Vosschulte R, fsah-Hedjri A, Koltai S, Kocsis E,
Scholz D, Kostin S, Schaper W, Schaper J. Altered Balance
Between Extracellular Proteolysis and Antiproteolysis Is
Associated With Adaptive Coronary Arteriogenesis. J Mol
Cell Cardiol 2000;32:997-1011.
108. Wu S, Wu X, Zhu W, Cai WJ, Schaper J, Schaper W.
Immunohistochemical Study of the Growth Factors, AFGF,
BFGF, PDGF-AB, VEGF-A and Its Receptor (Flk-1) During
Arteriogenesis. Mol Cell Biochem 2010;343:223-9.
109. Kinnaird T, Stabile E, Burnett MS, Lee CW, Barr S, Fuchs S,
Epstein SE. Marrow-Derived Stromal Cells Express Genes
Encoding a Broad Spectrum of Arteriogenic Cytokines and
Promote in Vitro and in Vivo Arteriogenesis Through
Paracrine Mechanisms. Circ Res 2004;94:678-85.
110. Hoefer IE, van RN, Buschmann IR, Piek JJ, Schaper W.
Time Course of Arteriogenesis Following Femoral Artery
Occlusion in the Rabbit. Cardiovasc Res 2001;49:609-17.
111. Behm CZ, Kaufmann BA, Carr C, Lankford M, Sanders JM,
Rose CE, Kaul S, Lindner JR. Molecular Imaging of
Endothelial Vascular Cell Adhesion Molecule-1 Expression
and Inflammatory Cell Recruitment During Vasculogenesis
and Ischemia-Mediated Arteriogenesis. Circulation
2008;117:2902-11.
112. Soehnlein O, Zernecke A, Eriksson EE, Rothfuchs AG, Pham
CT, Herwald H, Bidzhekov K, Rottenberg ME, Weber C,
Lindbom L. Neutrophil Secretion Products Pave the Way for
Inflammatory Monocytes. Blood 2008;112:1461-71.
113. Bergmann CE, Hoefer IE, Meder B, Roth H, van RN, Breit
SM, Jost MM, Aharinejad S, Hartmann S, Buschmann IR.
Arteriogenesis Depends on Circulating Monocytes and
Macrophage Accumulation and Is Severely Depressed in
Op/Op Mice. J Leukoc Biol 2006;80:59-65.
114. Bakker EN, Matlung HL, Bonta P, de Vries CJ, van RN,
Vanbavel E. Blood Flow-Dependent Arterial Remodelling Is
Facilitated by Inflammation but Directed by Vascular Tone.
Cardiovasc Res 2008;78:341-8.
115. Khmelewski E, Becker A, Meinertz T, Ito WD. Tissue
Resident Cells Play a Dominant Role in Arteriogenesis and
Concomitant Macrophage Accumulation. Circ Res
2004;95:E56-E64.
116. Aicher A, Rentsch M, Sasaki K, Ellwart JW, Fandrich F,
Siebert R, Cooke JP, Dimmeler S, Heeschen C. Nonbone
Marrow-Derived Circulating Progenitor Cells Contribute to
Postnatal Neovascularization Following Tissue Ischemia.
Circ Res 2007;100:581-9.
117. Tepper OM, Capla JM, Galiano RD, Ceradini DJ, Callaghan
MJ, Kleinman ME, Gurtner GC. Adult Vasculogenesis Occurs
Through in Situ Recruitment, Proliferation, and Tubulization
of Circulating Bone Marrow-Derived Cells. Blood
2005;105:1068-77.
118. Reinecke H, Minami E, Zhu WZ, Laflamme MA. Cardiogenic

- 43 -
Differentiation and Transdifferentiation of Progenitor Cells.
Circ Res 2008;103:1058-71.
119. Copelan EA. Hematopoietic Stem-Cell Transplantation. N
Engl J Med 2006;354:1813-26.
120. Shpall EJ, Champlin R, Glaspy JA. Effect of CD34+
Peripheral Blood Progenitor Cell Dose on Hematopoietic
Recovery. Biol Blood Marrow Transplant 1998;4:84-92.
121. Rota M, Kajstura J, Hosoda T, Bearzi C, Vitale S, Esposito
G, Iaffaldano G, Padin-Iruegas ME, Gonzalez A, Rizzi R,
Small N, Muraski J, Alvarez R, Chen X, Urbanek K, Bolli R,
Houser SR, Leri A, Sussman MA, Anversa P. Bone Marrow
Cells Adopt the Cardiomyogenic Fate in Vivo. Proc Natl Acad
Sci U S A 2007;104:17783-8.
122. Balsam LB, Wagers AJ, Christensen JL, Kofidis T, Weissman
IL, Robbins RC. Haematopoietic Stem Cells Adopt Mature
Haematopoietic Fates in Ischaemic Myocardium. Nature
2004;428:668-73.
123. Richardson MR, Yoder MC. Endothelial Progenitor Cells: Quo
Vadis? J Mol Cell Cardiol 2011;50:266-72.
124. Timmermans F, Van HF, De SM, Raedt R, Plasschaert F, De
Buyzere ML, Gillebert TC, Plum J, Vandekerckhove B.
Endothelial Outgrowth Cells Are Not Derived From CD133+
Cells or CD45+ Hematopoietic Precursors. Arterioscler
Thromb Vasc Biol 2007;27:1572-9.
125. Massa M, Rosti V, Ferrario M, Campanelli R, Ramajoli I,
Rosso R, De Ferrari GM, Ferlini M, Goffredo L, Bertoletti A,
Klersy C, Pecci A, Moratti R, Tavazzi L. Increased
Circulating Hematopoietic and Endothelial Progenitor Cells
in the Early Phase of Acute Myocardial Infarction. Blood
2005;105:199-206.
126. Kunz GA, Liang G, Cuculi F, Gregg D, Vata KC, Shaw LK,
Goldschmidt-Clermont PJ, Dong C, Taylor DA, Peterson ED.
Circulating Endothelial Progenitor Cells Predict Coronary
Artery Disease Severity. Am Heart J 2006;152:190-5.
127. Wang CH, Verma S, Hsieh IC, Chen YJ, Kuo LT, Yang NI,
Wang SY, Wu MY, Hsu CM, Cheng CW, Cherng WJ. Enalapril
Increases Ischemia-Induced Endothelial Progenitor Cell
Mobilization Through Manipulation of the CD26 System. J
Mol Cell Cardiol 2006;41:34-43.
128. Vasa M, Fichtlscherer S, Adler K, Aicher A, Martin H, Zeiher
AM, Dimmeler S. Increase in Circulating Endothelial
Progenitor Cells by Statin Therapy in Patients With Stable
Coronary Artery Disease. Circulation 2001;103:2885-90.
129. Shi Q, Rafii S, Wu MH, Wijelath ES, Yu C, Ishida A, Fujita Y,
Kothari S, Mohle R, Sauvage LR, Moore MA, Storb RF,
Hammond WP. Evidence for Circulating Bone Marrow-
Derived Endothelial Cells. Blood 1998;92:362-7.
130. Urbich C, Aicher A, Heeschen C, Dernbach E, Hofmann WK,
Zeiher AM, Dimmeler S. Soluble Factors Released by
Endothelial Progenitor Cells Promote Migration of
Endothelial Cells and Cardiac Resident Progenitor Cells. J
Mol Cell Cardiol 2005;39:733-42.
131. Badorff C, Brandes RP, Popp R, Rupp S, Urbich C, Aicher A,
Fleming I, Busse R, Zeiher AM, Dimmeler S.
Transdifferentiation of Blood-Derived Human Adult
Endothelial Progenitor Cells into Functionally Active
Cardiomyocytes. Circulation 2003;107:1024-32.
132. Koyanagi M, Urbich C, Chavakis E, Hoffmann J, Rupp S,
Badorff C, Zeiher AM, Starzinski-Powitz A, Haendeler J,
Dimmeler S. Differentiation of Circulating Endothelial
Progenitor Cells to a Cardiomyogenic Phenotype Depends
on E-Cadherin. FEBS Lett 2005;579:6060-6.
133. Gruh I, Beilner J, Blomer U, Schmiedl A, Schmidt-Richter I,
Kruse ML, Haverich A, Martin U. No Evidence of
Transdifferentiation of Human Endothelial Progenitor Cells
into Cardiomyocytes After Coculture With Neonatal Rat
Cardiomyocytes. Circulation 2006;113:1326-34.
134. Friedenstein AJ, Chailakhyan RK, Latsinik NV, Panasyuk AF,
Keiliss-Borok IV. Stromal Cells Responsible for Transferring
the Microenvironment of the Hemopoietic Tissues. Cloning
in Vitro and Retransplantation in Vivo. Transplantation
1974;17:331-40.
135. Jiang Y, Jahagirdar BN, Reinhardt RL, Schwartz RE, Keene
CD, Ortiz-Gonzalez XR, Reyes M, Lenvik T, Lund T,
Blackstad M, Du J, Aldrich S, Lisberg A, Low WC,
Largaespada DA, Verfaillie CM. Pluripotency of
Mesenchymal Stem Cells Derived From Adult Marrow.
Nature 2002;418:41-9.
136. Reyes M, Verfaillie CM. Characterization of Multipotent Adult
Progenitor Cells, a Subpopulation of Mesenchymal Stem
Cells. Ann N Y Acad Sci 2001;938:231-3.
137. Porada CD, meida-Porada G. Mesenchymal Stem Cells As
Therapeutics and Vehicles for Gene and Drug Delivery. Adv
Drug Deliv Rev 2010;62:1156-66.
138. Crisan M, Yap S, Casteilla L, Chen CW, Corselli M, Park TS,
Andriolo G, Sun B, Zheng B, Zhang L, Norotte C, Teng PN,
Traas J, Schugar R, Deasy BM, Badylak S, Buhring HJ,
Giacobino JP, Lazzari L, Huard J, Peault B. A Perivascular
Origin for Mesenchymal Stem Cells in Multiple Human
Organs. Cell Stem Cell 2008;3:301-13.
139. Corselli M, Chen CW, Crisan M, Lazzari L, Peault B.
Perivascular Ancestors of Adult Multipotent Stem Cells.
Arterioscler Thromb Vasc Biol 2010;30:1104-9.
140. Rojewski M, Weber B, Schrezenmeier H. Phenotypic
Characterization of Mesenchymal Stem Cells From Various
Tissues. Transfus Med Hemother 2008;35:168-84.
141. Dominici M, Le BK, Mueller I, Slaper-Cortenbach I, Marini F,
Krause D, Deans R, Keating A, Prockop D, Horwitz E.
Minimal Criteria for Defining Multipotent Mesenchymal
Stromal Cells. The International Society for Cellular
Therapy Position Statement. Cytotherapy 2006;8:315-7.
142. Horwitz EM, Le BK, Dominici M, Mueller I, Slaper-

- 44 -
Cortenbach I, Marini FC, Deans RJ, Krause DS, Keating A.
Clarification of the Nomenclature for MSC: The
International Society for Cellular Therapy Position
Statement. Cytotherapy 2005;7:393-5.
143. Wu X, Huang L, Zhou Q, Song Y, Li A, Jin J, Cui B.
Mesenchymal Stem Cells Participating in Ex Vivo
Endothelium Repair and Its Effect on Vascular Smooth
Muscle Cells Growth. Int J Cardiol 2005;105:274-82.
144. Oswald J, Boxberger S, Jorgensen B, Feldmann S, Ehninger
G, Bornhauser M, Werner C. Mesenchymal Stem Cells Can
Be Differentiated into Endothelial Cells in Vitro. Stem Cells
2004;22:377-84.
145. Ball SG, Shuttleworth AC, Kielty CM. Direct Cell Contact
Influences Bone Marrow Mesenchymal Stem Cell Fate. Int J
Biochem Cell Biol 2004;36:714-27.
146. Toma C, Pittenger MF, Cahill KS, Byrne BJ, Kessler PD.
Human Mesenchymal Stem Cells Differentiate to a
Cardiomyocyte Phenotype in the Adult Murine Heart.
Circulation 2002;105:93-8.
147. Tokcaer-Keskin Z, Akar AR, yaloglu-Butun F, Terzioglu-Kara
E, Durdu S, Ozyurda U, Ugur M, Akcali KC. Timing of
Induction of Cardiomyocyte Differentiation for in Vitro
Cultured Mesenchymal Stem Cells: a Perspective for
Emergencies. Can J Physiol Pharmacol 2009;87:143-50.
148. Dai W, Hale SL, Martin BJ, Kuang JQ, Dow JS, Wold LE,
Kloner RA. Allogeneic Mesenchymal Stem Cell
Transplantation in Postinfarcted Rat Myocardium: Short-
and Long-Term Effects. Circulation 2005;112:214-23.
149. Iso Y, Spees JL, Serrano C, Bakondi B, Pochampally R,
Song YH, Sobel BE, Delafontaine P, Prockop DJ. Multipotent
Human Stromal Cells Improve Cardiac Function After
Myocardial Infarction in Mice Without Long-Term
Engraftment. Biochem Biophys Res Commun
2007;354:700-6.
150. Sadat S, Gehmert S, Song YH, Yen Y, Bai X, Gaiser S, Klein
H, Alt E. The Cardioprotective Effect of Mesenchymal Stem
Cells Is Mediated by IGF-I and VEGF. Biochem Biophys Res
Commun 2007;363:674-9.
151. Honczarenko M, Le Y, Swierkowski M, Ghiran I, Glodek AM,
Silberstein LE. Human Bone Marrow Stromal Cells Express a
Distinct Set of Biologically Functional Chemokine Receptors.
Stem Cells 2006;24:1030-41.
152. Von L, I, Notohamiprodjo M, Wechselberger A, Peters C,
Henger A, Seliger C, Djafarzadeh R, Huss R, Nelson PJ.
Human Adult CD34- Progenitor Cells Functionally Express
the Chemokine Receptors CCR1, CCR4, CCR7, CXCR5, and
CCR10 but Not CXCR4. Stem Cells Dev 2005;14:329-36.
153. Barbash IM, Chouraqui P, Baron J, Feinberg MS, Etzion S,
Tessone A, Miller L, Guetta E, Zipori D, Kedes LH, Kloner
RA, Leor J. Systemic Delivery of Bone Marrow-Derived
Mesenchymal Stem Cells to the Infarcted Myocardium:
Feasibility, Cell Migration, and Body Distribution. Circulation
2003;108:863-8.
154. Morigi M, Imberti B, Zoja C, Corna D, Tomasoni S, Abbate
M, Rottoli D, Angioletti S, Benigni A, Perico N, Alison M,
Remuzzi G. Mesenchymal Stem Cells Are Renotropic,
Helping to Repair the Kidney and Improve Function in Acute
Renal Failure. J Am Soc Nephrol 2004;15:1794-804.
155. Granero-Molto F, Weis JA, Miga MI, Landis B, Myers TJ,
O'Rear L, Longobardi L, Jansen ED, Mortlock DP, Spagnoli
A. Regenerative Effects of Transplanted Mesenchymal Stem
Cells in Fracture Healing. Stem Cells 2009;27:1887-98.
156. Ruster B, Gottig S, Ludwig RJ, Bistrian R, Muller S, Seifried
E, Gille J, Henschler R. Mesenchymal Stem Cells Display
Coordinated Rolling and Adhesion Behavior on Endothelial
Cells. Blood 2006;108:3938-44.
157. Cheng Z, Ou L, Zhou X, Li F, Jia X, Zhang Y, Liu X, Li Y,
Ward CA, Melo LG, Kong D. Targeted Migration of
Mesenchymal Stem Cells Modified With CXCR4 Gene to
Infarcted Myocardium Improves Cardiac Performance. Mol
Ther 2008;16:571-9.
158. Cho HH, Kyoung KM, Seo MJ, Kim YJ, Bae YC, Jung JS.
Overexpression of CXCR4 Increases Migration and
Proliferation of Human Adipose Tissue Stromal Cells. Stem
Cells Dev 2006;15:853-64.
159. Ip JE, Wu Y, Huang J, Zhang L, Pratt RE, Dzau VJ.
Mesenchymal Stem Cells Use Integrin Beta1 Not CXC
Chemokine Receptor 4 for Myocardial Migration and
Engraftment. Mol Biol Cell 2007;18:2873-82.
160. Schenk S, Mal N, Finan A, Zhang M, Kiedrowski M, Popovic
Z, McCarthy PM, Penn MS. Monocyte Chemotactic Protein-3
Is a Myocardial Mesenchymal Stem Cell Homing Factor.
Stem Cells 2007;25:245-51.
161. Silva GV, Litovsky S, Assad JA, Sousa AL, Martin BJ, Vela D,
Coulter SC, Lin J, Ober J, Vaughn WK, Branco RV, Oliveira
EM, He R, Geng YJ, Willerson JT, Perin EC. Mesenchymal
Stem Cells Differentiate into an Endothelial Phenotype,
Enhance Vascular Density, and Improve Heart Function in a
Canine Chronic Ischemia Model. Circulation 2005;111:150-
6.
162. Shake JG, Gruber PJ, Baumgartner WA, Senechal G, Meyers
J, Redmond JM, Pittenger MF, Martin BJ. Mesenchymal
Stem Cell Implantation in a Swine Myocardial Infarct Model:
Engraftment and Functional Effects. Ann Thorac Surg
2002;73:1919-25.
163. Amado LC, Saliaris AP, Schuleri KH, St JM, Xie JS, Cattaneo
S, Durand DJ, Fitton T, Kuang JQ, Stewart G, Lehrke S,
Baumgartner WW, Martin BJ, Heldman AW, Hare JM.
Cardiac Repair With Intramyocardial Injection of Allogeneic
Mesenchymal Stem Cells After Myocardial Infarction. Proc
Natl Acad Sci U S A 2005;102:11474-9.
164. Miyahara Y, Nagaya N, Kataoka M, Yanagawa B, Tanaka K,

- 45 -
Hao H, Ishino K, Ishida H, Shimizu T, Kangawa K, Sano S,
Okano T, Kitamura S, Mori H. Monolayered Mesenchymal
Stem Cells Repair Scarred Myocardium After Myocardial
Infarction. Nat Med 2006;12:459-65.
165. Ziegelhoeffer T, Fernandez B, Kostin S, Heil M, Voswinckel
R, Helisch A, Schaper W. Bone Marrow-Derived Cells Do Not
Incorporate into the Adult Growing Vasculature. Circ Res
2004;94:230-8.
166. Lee RH, Pulin AA, Seo MJ, Kota DJ, Ylostalo J, Larson BL,
Semprun-Prieto L, Delafontaine P, Prockop DJ. Intravenous
HMSCs Improve Myocardial Infarction in Mice Because Cells
Embolized in Lung Are Activated to Secrete the Anti-
Inflammatory Protein TSG-6. Cell Stem Cell 2009;5:54-63.
167. He Q, Wan C, Li G. Concise Review: Multipotent
Mesenchymal Stromal Cells in Blood. Stem Cells
2007;25:69-77.
168. Kuznetsov SA, Mankani MH, Gronthos S, Satomura K,
Bianco P, Robey PG. Circulating Skeletal Stem Cells. J Cell
Biol 2001;153:1133-40.
169. Tondreau T, Meuleman N, Delforge A, Dejeneffe M, Leroy R,
Massy M, Mortier C, Bron D, Lagneaux L. Mesenchymal
Stem Cells Derived From CD133-Positive Cells in Mobilized
Peripheral Blood and Cord Blood: Proliferation, Oct4
Expression, and Plasticity. Stem Cells 2005;23:1105-12.
170. Fernandez M, Simon V, Herrera G, Cao C, Del FH, Minguell
JJ. Detection of Stromal Cells in Peripheral Blood Progenitor
Cell Collections From Breast Cancer Patients. Bone Marrow
Transplant 1997;20:265-71.
171. Wexler SA, Donaldson C, ning-Kendall P, Rice C, Bradley B,
Hows JM. Adult Bone Marrow Is a Rich Source of Human
Mesenchymal /`Stem/' Cells but Umbilical Cord and
Mobilized Adult Blood Are Not. Br J Haematol
2003;121:368-74.
172. Lazarus HM, Haynesworth SE, Gerson SL, Caplan AI.
Human Bone Marrow-Derived Mesenchymal Stromal
(Progenitor Cells MPCs) Cannot Be Recovered From
Peripheral Blood Progenitor Cell Collections. J Hematother
1997;6:447-55.
173. Kassis I, Zangi L, Rivkin R, Levdansky L, Samuel S, Marx G,
Gorodetsky R. Isolation of Mesenchymal Stem Cells From
G-CSF-Mobilized Human Peripheral Blood Using Fibrin
Microbeads. Bone Marrow Transplant 2006;37:967-76.
174. Kawamoto A, Gwon HC, Iwaguro H, Yamaguchi JI, Uchida
S, Masuda H, Silver M, Ma H, Kearney M, Isner JM, Asahara
T. Therapeutic Potential of Ex Vivo Expanded Endothelial
Progenitor Cells for Myocardial Ischemia. Circulation
2001;103:634-7.
175. Oswald J, Boxberger S, Jorgensen B, Feldmann S, Ehninger
G, Bornhauser M, Werner C. Mesenchymal Stem Cells Can
Be Differentiated into Endothelial Cells in Vitro. Stem Cells
2004;22:377-84.
176. Yoon CH, Koyanagi M, Iekushi K, Seeger F, Urbich C, Zeiher
AM, Dimmeler S. Mechanism of Improved Cardiac Function
After Bone Marrow Mononuclear Cell Therapy: Role of
Cardiovascular Lineage Commitment. Circulation
2010;121:2001-11.
177. Gnecchi M, Zhang Z, Ni A, Dzau VJ. Paracrine Mechanisms
in Adult Stem Cell Signaling and Therapy. Circ Res
2008;103:1204-19.
178. Gnecchi M, He H, Liang OD, Melo LG, Morello F, Mu H,
Noiseux N, Zhang L, Pratt RE, Ingwall JS, Dzau VJ.
Paracrine Action Accounts for Marked Protection of Ischemic
Heart by Akt-Modified Mesenchymal Stem Cells. Nat Med
2005;11:367-8.
179. Takahashi M, Li TS, Suzuki R, Kobayashi T, Ito H, Ikeda Y,
Matsuzaki M, Hamano K. Cytokines Produced by Bone
Marrow Cells Can Contribute to Functional Improvement of
the Infarcted Heart by Protecting Cardiomyocytes From
Ischemic Injury. Am J Physiol Heart Circ Physiol
2006;291:H886-H893.
180. Maxeiner H, Krehbiehl N, Muller A, Woitasky N, Akinturk H,
Muller M, Weigand MA, Abdallah Y, Kasseckert S,
Schreckenberg R, Schluter KD, Wenzel S. New Insights into
Paracrine Mechanisms of Human Cardiac Progenitor Cells.
Eur J Heart Fail 2010;12:730-7.
181. Kinnaird T, Stabile E, Burnett MS, Shou M, Lee CW, Barr S,
Fuchs S, Epstein SE. Local Delivery of Marrow-Derived
Stromal Cells Augments Collateral Perfusion Through
Paracrine Mechanisms. Circulation 2004;109:1543-9.
182. Shabbir A, Zisa D, Lin H, Mastri M, Roloff G, Suzuki G, Lee
T. Activation of Host Tissue Trophic Factors Through JAK-
STAT3 Signaling: a Mechanism of Mesenchymal Stem Cell-
Mediated Cardiac Repair. Am J Physiol Heart Circ Physiol
2010;299:H1428-H1438.
183. Lewis EF, Johnson PA, Johnson W, Collins C, Griffin L,
Stevenson LW. Preferences for Quality of Life or Survival
Expressed by Patients With Heart Failure. J Heart Lung
Transplant 2001;20:1016-24.
184. Sugeng L, Mor-Avi V, Weinert L, Niel J, Ebner C, Steringer-
Mascherbauer R, Schmidt F, Galuschky C, Schummers G,
Lang RM, Nesser HJ. Quantitative Assessment of Left
Ventricular Size and Function: Side-by-Side Comparison of
Real-Time Three-Dimensional Echocardiography and
Computed Tomography With Magnetic Resonance
Reference. Circulation 2006;114:654-61.
185. St John SM, Pfeffer MA, Plappert T, Rouleau JL, Moye LA,
Dagenais GR, Lamas GA, Klein M, Sussex B, Goldman S, .
Quantitative Two-Dimensional Echocardiographic
Measurements Are Major Predictors of Adverse
Cardiovascular Events After Acute Myocardial Infarction.
The Protective Effects of Captopril. Circulation 1994;89:68-
75.
186. Kjoller E, Kober L, Jorgensen S, Torp-Pedersen C. Long-

- 46 -
Term Prognostic Importance of Hyperkinesia Following
Acute Myocardial Infarction. TRACE Study Group.
TRAndolapril Cardiac Evaluation. Am J Cardiol
1999;83:655-9.
187. Moller JE, Hillis GS, Oh JK, Reeder GS, Gersh BJ, Pellikka
PA. Wall Motion Score Index and Ejection Fraction for Risk
Stratification After Acute Myocardial Infarction. Am Heart J
2006;151:419-25.
188. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E,
Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise JS,
Solomon SD, Spencer KT, Sutton MS, Stewart WJ.
Recommendations for Chamber Quantification: a Report
From the American Society of Echocardiography's
Guidelines and Standards Committee and the Chamber
Quantification Writing Group, Developed in Conjunction
With the European Association of Echocardiography, a
Branch of the European Society of Cardiology. J Am Soc
Echocardiogr 2005;18:1440-63.
189. McGowan JH, Cleland JG. Reliability of Reporting Left
Ventricular Systolic Function by Echocardiography: a
Systematic Review of 3 Methods. Am Heart J
2003;146:388-97.
190. Faber TL, Cooke CD, Folks RD, Vansant JP, Nichols KJ,
DePuey EG, Pettigrew RI, Garcia EV. Left Ventricular
Function and Perfusion From Gated SPECT Perfusion
Images: an Integrated Method. J Nucl Med 1999;40:650-9.
191. Nakajima K, Nishimura T. Inter-Institution Preference-
Based Variability of Ejection Fraction and Volumes Using
Quantitative Gated SPECT With 99mTc-Tetrofosmin: a
Multicentre Study Involving 106 Hospitals. Eur J Nucl Med
Mol Imaging 2006;33:127-33.
192. Koch JA, Poll LW, Godehardt E, Korbmacher B, Modder U.
Right and Left Ventricular Volume Measurements in an
Animal Heart Model in Vitro: First Experiences With Cardiac
MRI at 1.0 T. Eur Radiol 2000;10:455-8.
193. Møgelvang J, Stokholm KH, Saunamaki K, Reimer A,
Stubgaard M, Thomsen C, Fritz-Hansen P, Henriksen O.
Assessment of Left Ventricular Volumes by Magnetic
Resonance in Comparison With Radionuclide Angiography,
Contrast Angiography and Echocardiography. Eur Heart J
1992;13:1677-83.
194. Florentine MS, Grosskreutz CL, Chang W, Hartnett JA, Dunn
VD, Ehrhardt JC, Fleagle SR, Collins SM, Marcus ML,
Skorton DJ. Measurement of Left Ventricular Mass in Vivo
Using Gated Nuclear Magnetic Resonance Imaging. J Am
Coll Cardiol 1986;8:107-12.
195. Mogelvang J, Lindvig K, Sondergaard L, Saunamaki K,
Henriksen O. Reproducibility of Cardiac Volume
Measurements Including Left Ventricular Mass Determined
by MRI. Clin Physiol 1993;13:587-97.
196. Semelka RC, Tomei E, Wagner S, Mayo J, Caputo G,
O'Sullivan M, Parmley WW, Chatterjee K, Wolfe C, Higgins
CB. Interstudy Reproducibility of Dimensional and
Functional Measurements Between Cine Magnetic
Resonance Studies in the Morphologically Abnormal Left
Ventricle. Am Heart J 1990;119:1367-73.
197. Schwitter J, Nanz D, Kneifel S, Bertschinger K, Buchi M,
Knusel PR, Marincek B, Luscher TF, von Schulthess GK.
Assessment of Myocardial Perfusion in Coronary Artery
Disease by Magnetic Resonance: a Comparison With
Positron Emission Tomography and Coronary Angiography.
Circulation 2001;103:2230-5.
198. Ibrahim T, Nekolla SG, Schreiber K, Odaka K, Volz S, Mehilli
J, Guthlin M, Delius W, Schwaiger M. Assessment of
Coronary Flow Reserve: Comparison Between Contrast-
Enhanced Magnetic Resonance Imaging and Positron
Emission Tomography. J Am Coll Cardiol 2002;39:864-70.
199. Nagel E, Klein C, Paetsch I, Hettwer S, Schnackenburg B,
Wegscheider K, Fleck E. Magnetic Resonance Perfusion
Measurements for the Noninvasive Detection of Coronary
Artery Disease. Circulation 2003;108:432-7.
200. Sakuma H, Suzawa N, Ichikawa Y, Makino K, Hirano T,
Kitagawa K, Takeda K. Diagnostic Accuracy of Stress First-
Pass Contrast-Enhanced Myocardial Perfusion MRI
Compared With Stress Myocardial Perfusion Scintigraphy.
AJR Am J Roentgenol 2005;185:95-102.
201. Marckmann P. An Epidemic Outbreak of Nephrogenic
Systemic Fibrosis in a Danish Hospital. Eur J Radiol
2008;66:187-90.
202. Kalka C, Masuda H, Takahashi T, Gordon R, Tepper O,
Gravereaux E, Pieczek A, Iwaguro H, Hayashi SI, Isner JM,
Asahara T. Vascular Endothelial Growth Factor(165) Gene
Transfer Augments Circulating Endothelial Progenitor Cells
in Human Subjects. Circ Res 2000;86:1198-202.
203. Tomita S, Li RK, Weisel RD, Mickle DA, Kim EJ, Sakai T, Jia
ZQ. Autologous Transplantation of Bone Marrow Cells
Improves Damaged Heart Function. Circulation
1999;100:II247-II256.
204. Sesti C, Hale SL, Lutzko C, Kloner RA. Granulocyte Colony-
Stimulating Factor and Stem Cell Factor Improve
Contractile Reserve of the Infarcted Left Ventricle
Independent of Restoring Muscle Mass. J Am Coll Cardiol
2005;46:1662-9.
205. Kalka C, Masuda H, Takahashi T, Kalka-Moll WM, Silver M,
Kearney M, Li T, Isner JM, Asahara T. Transplantation of Ex
Vivo Expanded Endothelial Progenitor Cells for Therapeutic
Neovascularization. Proc Natl Acad Sci U S A
2000;97:3422-7.
206. Uemura R, Xu M, Ahmad N, Ashraf M. Bone Marrow Stem
Cells Prevent Left Ventricular Remodeling of Ischemic Heart
Through Paracrine Signaling. Circ Res 2006;98:1414-21.
207. Orlic D, Kajstura J, Chimenti S, Limana F, Jakoniuk I,
Quaini F, Nadal-Ginard B, Bodine DM, Leri A, Anversa P.

- 47 -
Mobilized Bone Marrow Cells Repair the Infarcted Heart,
Improving Function and Survival. Proc Natl Acad Sci U S A
2001;98:10344-9.
208. Wang Y, Tägil K, Ripa RS, Nilsson JC, Carstensen S,
Jørgensen E, Søndergaard L, Hesse B, Johnsen HE, Kastrup
J. Effect of Mobilization of Bone Marrow Stem Cells by
Granulocyte Colony Stimulating Factor on Clinical
Symptoms, Left Ventricular Perfusion and Function in
Patients With Severe Chronic Ischemic Heart Disease. Int J
Cardiol 2005;100:477-83.
209. Seiler C, Pohl T, Wustmann K, Hutter D, Nicolet PA,
Windecker S, Eberli FR, Meier B. Promotion of Collateral
Growth by Granulocyte-Macrophage Colony-Stimulating
Factor in Patients With Coronary Artery Disease: a
Randomized, Double-Blind, Placebo-Controlled Study.
Circulation 2001;104:2012-7.
210. Tateishi-Yuyama E, Matsubara H, Murohara T, Ikeda U,
Shintani S, Masaki H, Amano K, Kishimoto Y, Yoshimoto K,
Akashi H, Shimada K, Iwasaka T, Imaizumi T. Therapeutic
Angiogenesis for Patients With Limb Ischaemia by
Autologous Transplantation of Bone-Marrow Cells: a Pilot
Study and a Randomised Controlled Trial. Lancet
2002;360:427-35.
211. Ripa RS, Wang Y, Jørgensen E, Johnsen HE, Grande P,
Kastrup J. Safety of Bone-Marrow Stem Cell Mobilisation
Induced by Granulocyte-Colony Stimulating Factor: Clinical
30 Days Blinded Results From the Stem Cells in Myocardial
Infarction (STEMMI) Trial. Heart Drug 2005;5:177-82.
212. Hill JM, Syed MA, Arai AE, Powell TM, Paul JD, Zalos G,
Read EJ, Khuu HM, Leitman SF, Horne M, Csako G, Dunbar
CE, Waclawiw MA, Cannon RO, III. Outcomes and Risks of
Granulocyte Colony-Stimulating Factor in Patients With
Coronary Artery Disease. J Am Coll Cardiol 2005;46:1643-
8.
213. Boyle AJ, Whitbourn R, Schlicht S, Krum H, Kocher A,
Nandurkar H, Bergmann S, Daniell M, O'Day J, Skerrett D,
Haylock D, Gilbert RE, Itescu S. Intra-Coronary High-Dose
CD34+ Stem Cells in Patients With Chronic Ischemic Heart
Disease: a 12-Month Follow-Up. Int J Cardiol 2006;109:21-
7.
214. Kovacic JC, Macdonald P, Feneley MP, Muller DWM, Freund
J, Dodds A, Milliken S, Tao H, Itescu S, Moore J, Ma D,
Graham RM. Safety and Efficacy of Consecutive Cycles of
Granulocyte-Colony Stimulating Factor, and an
Intracoronary CD133+ Cell Infusion in Patients With
Chronic Refractory Ischemic Heart Disease: The G-CSF in
Angina Patients With IHD to Stimulate Neovascularization
(GAIN I) Trial. Am Heart J 2008;156:954-63.
215. Losordo DW, Schatz RA, White CJ, Udelson JE,
Veereshwarayya V, Durgin M, Poh KK, Weinstein R,
Kearney M, Chaudhry M, Burg A, Eaton L, Heyd L, Thorne
T, Shturman L, Hoffmeister P, Story K, Zak V, Dowling D,
Traverse JH, Olson RE, Flanagan J, Sodano D, Murayama T,
Kawamoto A, Kusano KF, Wollins J, Welt F, Shah P, Soukas
P, Asahara T, Henry TD. Intramyocardial Transplantation of
Autologous CD34+ Stem Cells for Intractable Angina: a
Phase I/IIa Double-Blind, Randomized Controlled Trial.
Circulation 2007;115:3165-72.
216. Kawamoto A, Murayama T, Kusano K, Ii M, Tkebuchava T,
Shintani S, Iwakura A, Johnson I, von Samson P, Hanley A,
Gavin M, Curry C, Silver M, Ma H, Kearney M, Losordo DW.
Synergistic Effect of Bone Marrow Mobilization and Vascular
Endothelial Growth Factor-2 Gene Therapy in Myocardial
Ischemia. Circulation 2004;110:1398-405.
217. Shintani S, Kusano K, Ii M, Iwakura A, Heyd L, Curry C,
Wecker A, Gavin M, Ma H, Kearney M, Silver M, Thorne T,
Murohara T, Losordo DW. Synergistic Effect of Combined
Intramyocardial CD34+ Cells and VEGF2 Gene Therapy
After MI. Nat Clin Pract Cardiovasc Med 2006;3 Suppl
1:S123-S128.
218. Baldazzi F, Jørgensen E, Ripa RS, Kastrup J. Release of
Biomarkers of Myocardial Damage After Direct
Intramyocardial Injection of Genes and Stem Cells Via the
Percutaneous Transluminal Route. Eur Heart J
2008;29:1819-26.
219. Wang Y, Ripa RS, Jørgensen E, Hesse B, Mortensen S,
Kastrup J. Mobilization of Haematopoietic and Non-
Haematopoietic Cells by Granulocyte-Colony Stimulating
Factor and Vascular Endothelial Growth Factor Gene
Therapy in Patients With Stable Severe Coronary Artery
Disease. Scand Cardiovasc J 2007;41:397-404.
220. Powell TM, Paul JD, Hill JM, Thompson M, Benjamin M,
Rodrigo M, McCoy JP, Read EJ, Khuu HM, Leitman SF,
Finkel T, Cannon RO, III. Granulocyte Colony-Stimulating
Factor Mobilizes Functional Endothelial Progenitor Cells in
Patients With Coronary Artery Disease. Arterioscler Thromb
Vasc Biol 2005;25:296-301.
221. Takai H, Miyoshi A, Yamazaki M, Adachi K, Katagiri K,
Arakawa H, Katsuyama K, Ito T, Fujii E, Hayashi S, Kato A,
Suzuki M. Granulocyte Colony-Stimulating Factor Has No
Adverse Effects on Atherosclerotic Lesions in High
Cholesterol-Fed Miniature Swine. J Vet Med Sci
2008;70:943-50.
222. Chih, Sharon S., Macdonald, Peter, McCrohon, Jane A., Ma,
David, John, Moore, Law, Matthew, Feneley, Michael P.,
Herbert, Andrea, Kovacic, Jason C., and Graham, Robert M.
Granulocyte-Colony Stimulating Factor in Angina Patients
With Ischaemic Heart Diesase to Stimulate
Neovascularisation (GAIN II Trial). J Am Coll Cardiol
2010;55:A126.E1184 [Abstract]
223. Meier P, Gloekler S, de Marchi SF, Indermuehle A, Rutz T,
Traupe T, Steck H, Vogel R, Seiler C. Myocardial Salvage
Through Coronary Collateral Growth by Granulocyte
Colony-Stimulating Factor in Chronic Coronary Artery
Disease: a Controlled Randomized Trial. Circulation
2009;120:1355-63.

- 48 -
224. Goetze JP, Yongzhong W, Rehfeld JF, Jørgensen E, Kastrup
J. Coronary Angiography Transiently Increases Plasma Pro-
B-Type Natriuretic Peptide. Eur Heart J 2004;25:759-64.
225. Wang Y, Gabrielsen A, Lawler PR, Paulsson-Berne G,
Steinbruchel DA, Hansson GK, Kastrup J. Myocardial Gene
Expression of Angiogenic Factors in Human Chronic
Ischemic Myocardium: Influence of Acute
Ischemia/Cardioplegia and Reperfusion. Microcirculation
2006;13:187-97.
226. Wynn RF, Hart CA, Corradi-Perini C, O'Neill L, Evans CA,
Wraith JE, Fairbairn LJ, Bellantuono I. A Small Proportion of
Mesenchymal Stem Cells Strongly Expresses Functionally
Active CXCR4 Receptor Capable of Promoting Migration to
Bone Marrow. Blood 2004;104:2643-5.
227. Rentrop KP, Cohen M, Blanke H, Phillips RA. Changes in
Collateral Channel Filling Immediately After Controlled
Coronary Artery Occlusion by an Angioplasty Balloon in
Human Subjects. J Am Coll Cardiol 1985;5:587-92.
228. Werner GS, Ferrari M, Heinke S, Kuethe F, Surber R,
Richartz BM, Figulla HR. Angiographic Assessment of
Collateral Connections in Comparison With Invasively
Determined Collateral Function in Chronic Coronary
Occlusions. Circulation 2003;107:1972-7.
229. van der MP, De Boer RA, White HL, van der SG, Hall AS,
Voors AA, van Veldhuisen DJ. The VEGF +405 CC Promoter
Polymorphism Is Associated With an Impaired Prognosis in
Patients With Chronic Heart Failure: a MERIT-HF Substudy.
J Card Fail 2005;11:279-84.
230. Ray D, Mishra M, Ralph S, Read I, Davies R, Brenchley P.
Association of the VEGF Gene With Proliferative Diabetic
Retinopathy but Not Proteinuria in Diabetes. Diabetes
2004;53:861-4.
231. Doi K, Noiri E, Nakao A, Fujita T, Kobayashi S, Tokunaga K.
Functional Polymorphisms in the Vascular Endothelial
Growth Factor Gene Are Associated With Development of
End-Stage Renal Disease in Males. J Am Soc Nephrol
2006;17:823-30.
232. Askari AT, Unzek S, Popovic ZB, Goldman CK, Forudi F,
Kiedrowski M, Rovner A, Ellis SG, Thomas JD, DiCorleto PE,
Topol EJ, Penn MS. Effect of Stromal-Cell-Derived Factor 1
on Stem-Cell Homing and Tissue Regeneration in Ischaemic
Cardiomyopathy. Lancet 2003;362:697-703.
233. Grunewald M, Avraham I, Dor Y, Bachar-Lustig E, Itin A,
Jung S, Chimenti S, Landsman L, Abramovitch R, Keshet E.
VEGF-Induced Adult Neovascularization: Recruitment,
Retention, and Role of Accessory Cells. Cell 2006;124:175-
89.
234. Peled A, Grabovsky V, Habler L, Sandbank J, renzana-
Seisdedos F, Petit I, Ben-Hur H, Lapidot T, Alon R. The
Chemokine SDF-1 Stimulates Integrin-Mediated Arrest of
CD34(+) Cells on Vascular Endothelium Under Shear Flow.
J Clin Invest 1999;104:1199-211.
235. De FE, Porcelli D, Torella AR, Straino S, Iachininoto MG,
Orlandi A, Truffa S, Biglioli P, Napolitano M, Capogrossi MC,
Pesce M. SDF-1 Involvement in Endothelial Phenotype and
Ischemia-Induced Recruitment of Bone Marrow Progenitor
Cells. Blood 2004;104:3472-82.
236. Peled A, Kollet O, Ponomaryov T, Petit I, Franitza S,
Grabovsky V, Slav MM, Nagler A, Lider O, Alon R, Zipori D,
Lapidot T. The Chemokine SDF-1 Activates the Integrins
LFA-1, VLA-4, and VLA-5 on Immature Human CD34(+)
Cells: Role in Transendothelial/Stromal Migration and
Engraftment of NOD/SCID Mice. Blood 2000;95:3289-96.
237. Chavakis E, Aicher A, Heeschen C, Sasaki K, Kaiser R, El
MN, Urbich C, Peters T, Scharffetter-Kochanek K, Zeiher
AM, Chavakis T, Dimmeler S. Role of Beta2-Integrins for
Homing and Neovascularization Capacity of Endothelial
Progenitor Cells. J Exp Med 2005;201:63-72.
238. Urbich C, Heeschen C, Aicher A, Sasaki K, Bruhl T, Farhadi
MR, Vajkoczy P, Hofmann WK, Peters C, Pennacchio LA,
Abolmaali ND, Chavakis E, Reinheckel T, Zeiher AM,
Dimmeler S. Cathepsin L Is Required for Endothelial
Progenitor Cell-Induced Neovascularization. Nat Med
2005;11:206-13.
239. van Weel V, Seghers L, de Vries MR, Kuiper EJ,
Schlingemann RO, Bajema IM, Lindeman JH, is-van Diemen
PM, van H, V, van Bockel JH, Quax PH. Expression of
Vascular Endothelial Growth Factor, Stromal Cell-Derived
Factor-1, and CXCR4 in Human Limb Muscle With Acute and
Chronic Ischemia. Arterioscler Thromb Vasc Biol
2007;27:1426-32.
240. Heeschen C, Lehmann R, Honold J, Assmus B, Aicher A,
Walter DH, Martin H, Zeiher AM, Dimmeler S. Profoundly
Reduced Neovascularization Capacity of Bone Marrow
Mononuclear Cells Derived From Patients With Chronic
Ischemic Heart Disease. Circulation 2004;109:1615-22.
241. Li TS, Kubo M, Ueda K, Murakami M, Ohshima M, Kobayashi
T, Tanaka T, Shirasawa B, Mikamo A, Hamano K.
Identification of Risk Factors Related to Poor Angiogenic
Potency of Bone Marrow Cells From Different Patients.
Circulation 2009;120:S255-S261.
242. Friis T, Haack-Sorensen M, Hansen SK, Hansen L, Bindslev
L, Kastrup J. Comparison of Mesenchymal Stromal Cells
From Young Healthy Donors and Patients With Severe
Chronic Coronary Artery Disease. Scand J Clin Lab Invest
2011 Jan 11. [Epub ahead of print]
243. Suuronen EJ, Hazra S, Zhang P, Vincent R, Kumarathasan
P, Zhang Y, Price J, Chan V, Sellke FW, Mesana TG, Veinot
JP, Ruel M. Impairment of Human Cell-Based
Vasculogenesis in Rats by Hypercholesterolemia-Induced
Endothelial Dysfunction and Rescue With L-Arginine
Supplementation. J Thorac Cardiovasc Surg 2010;139:209-
16.
244. Murohara T, Asahara T, Silver M, Bauters C, Masuda H,

- 49 -
Kalka C, Kearney M, Chen D, Symes JF, Fishman MC,
Huang PL, Isner JM. Nitric Oxide Synthase Modulates
Angiogenesis in Response to Tissue Ischemia. J Clin Invest
1998;101:2567-78.
245. Matsunaga T, Weihrauch DW, Moniz MC, Tessmer J,
Warltier DC, Chilian WM. Angiostatin Inhibits Coronary
Angiogenesis During Impaired Production of Nitric Oxide.
Circulation 2002;105:2185-91.
246. Walter DH, Haendeler J, Reinhold J, Rochwalsky U, Seeger
F, Honold J, Hoffmann J, Urbich C, Lehmann R, renzana-
Seisdesdos F, Aicher A, Heeschen C, Fichtlscherer S, Zeiher
AM, Dimmeler S. Impaired CXCR4 Signaling Contributes to
the Reduced Neovascularization Capacity of Endothelial
Progenitor Cells From Patients With Coronary Artery
Disease. Circ Res 2005;97:1142-51.
247. Honold J, Lehmann R, Heeschen C, Walter DH, Assmus B,
Sasaki K, Martin H, Haendeler J, Zeiher AM, Dimmeler S.
Effects of Granulocyte Colony Stimulating Factor on
Functional Activities of Endothelial Progenitor Cells in
Patients With Chronic Ischemic Heart Disease. Arterioscler
Thromb Vasc Biol 2006;26:2238-43.
248. Brunner S, Huber BC, Fischer R, Groebner M, Hacker M,
David R, Zaruba MM, Vallaster M, Rischpler C, Wilke A,
Gerbitz A, Franz WM. G-CSF Treatment After Myocardial
Infarction: Impact on Bone Marrow-Derived Vs Cardiac
Progenitor Cells. Exp Hematol 2008;36:695-702.
249. Stein A, Zohlnhofer D, Pogatsa-Murray G, von WJ, Steppich
BA, Schomig A, Kastrati A, Ott I. Expression of CXCR4,
VLA-1, LFA-3 and Transducer of ERB in G-CSF-Mobilised
Progenitor Cells in Acute Myocardial Infarction. Thromb
Haemost 2010;103:638-43.
250. Suarez de LJ, Torres A, Herrera I, Pan M, Romero M,
Pavlovic D, Segura J, Ojeda S, Sanchez J, Lopez RF, Medina
A. [Effects of Stem-Cell Mobilization With Recombinant
Human Granulocyte Colony Stimulating Factor in Patients
With Percutaneously Revascularized Acute Anterior
Myocardial Infarction]. Rev Esp Cardiol 2005;58:253-61.
251. Kuethe F, Figulla HR, Herzau M, Voth M, Fritzenwanger M,
Opfermann T, Pachmann K, Krack A, Sayer HG, Gottschild
D, Werner GS. Treatment With Granulocyte Colony-
Stimulating Factor for Mobilization of Bone Marrow Cells in
Patients With Acute Myocardial Infarction. Am Heart J
2005;150:115.
252. Valgimigli M, Rigolin GM, Cittanti C, Malagutti P, Curello S,
Percoco G, Bugli AM, Della PM, Bragotti LZ, Ansani L, Mauro
E, Lanfranchi A, Giganti M, Feggi L, Castoldi G, Ferrari R.
Use of Granulocyte-Colony Stimulating Factor During Acute
Myocardial Infarction to Enhance Bone Marrow Stem Cell
Mobilization in Humans: Clinical and Angiographic Safety
Profile. Eur Heart J 2005;26:1838-45.
253. Leone AM, Galiuto L, Garramone B, Rutella S, Giannico MB,
Brugaletta S, Perfetti M, Liuzzo G, Porto I, Burzotta F,
Niccoli G, Biasucci LM, Leone G, Rebuzzi AG, Crea F.
Usefulness of Granulocyte Colony-Stimulating Factor in
Patients With a Large Anterior Wall Acute Myocardial
Infarction to Prevent Left Ventricular Remodeling (the
Rigenera Study). Am J Cardiol 2007;100:397-403.
254. Kang HJ, Kim HS, Koo BK, Kim YJ, Lee D, Sohn DW, Oh BH,
Park YB. Intracoronary Infusion of the Mobilized Peripheral
Blood Stem Cell by G-CSF Is Better Than Mobilization Alone
by G-CSF for Improvement of Cardiac Function and
Remodeling: 2-Year Follow-Up Results of the Myocardial
Regeneration and Angiogenesis in Myocardial Infarction
With G-CSF and Intra-Coronary Stem Cell Infusion (MAGIC
Cell) 1 Trial. Am Heart J 2007;153:237-8.
255. Takano H, Hasegawa H, Kuwabara Y, Nakayama T, Matsuno
K, Miyazaki Y, Yamamoto M, Fujimoto Y, Okada H, Okubo
S, Fujita M, Shindo S, Kobayashi Y, Komiyama N, Takekoshi
N, Imai K, Himi T, Ishibashi I, Komuro I. Feasibility and
Safety of Granulocyte Colony-Stimulating Factor Treatment
in Patients With Acute Myocardial Infarction. Int J Cardiol
2007;122:41-7.
256. Ince H, Petzsch M, Kleine HD, Schmidt H, Rehders T,
Korber T, Schumichen C, Freund M, Nienaber CA.
Preservation From Left Ventricular Remodeling by Front-
Integrated Revascularization and Stem Cell Liberation in
Evolving Acute Myocardial Infarction by Use of Granulocyte-
Colony-Stimulating Factor (FIRSTLINE-AMI). Circulation
2005;112:3097-106.
257. Ellis SG, Penn MS, Bolwell B, Garcia M, Chacko M, Wang T,
Brezina KJ, McConnell G, Topol EJ. Granulocyte Colony
Stimulating Factor in Patients With Large Acute Myocardial
Infarction: Results of a Pilot Dose-Escalation Randomized
Trial. Am Heart J 2006;152:1051-14.
258. Zohlnhöfer D, Ott I, Mehilli J, Schomig K, Michalk F,
Ibrahim T, Meisetschlager G, von Wedel J, Bollwein H,
Seyfarth M, Dirschinger J, Schmitt C, Schwaiger M, Kastrati
A, Schomig A. Stem Cell Mobilization by Granulocyte
Colony-Stimulating Factor in Patients With Acute Myocardial
Infarction: a Randomized Controlled Trial. JAMA
2006;295:1003-10.
259. Engelmann MG, Theiss HD, Hennig-Theiss C, Huber A,
Wintersperger BJ, Werle-Ruedinger AE, Schoenberg SO,
Steinbeck G, Franz WM. Autologous Bone Marrow Stem Cell
Mobilization Induced by Granulocyte Colony-Stimulating
Factor After Subacute ST-Segment Elevation Myocardial
Infarction Undergoing Late Revascularization: Final Results
From the G-CSF-STEMI (Granulocyte Colony-Stimulating
Factor ST-Segment Elevation Myocardial Infarction) Trial. J
Am Coll Cardiol 2006;48:1712-21.
260. Baks T, van Geuns RJ, Biagini E, Wielopolski P, Mollet NR,
Cademartiri F, van der Giessen WJ, Krestin GP, Serruys PW,
Duncker DJ, de Feyter PJ. Effects of Primary Angioplasty for
Acute Myocardial Infarction on Early and Late Infarct Size
and Left Ventricular Wall Characteristics. J Am Coll Cardiol

- 50 -
2006;47:40-4.
261. Zohlnhöfer D, Dibra A, Koppara T, de WA, Ripa RS, Kastrup
J, Valgimigli M, Schomig A, Kastrati A. Stem Cell
Mobilization by Granulocyte Colony-Stimulating Factor for
Myocardial Recovery After Acute Myocardial Infarction: a
Meta-Analysis. J Am Coll Cardiol 2008;51:1429-37.
262. Ripa, R. S., Jørgensen, E., and Kastrup, J. Risk of Adverse
Events at 5-Years Follow-Up After Cell Mobilization With
Granulocyte-Colony Stimulating Factor After Acute ST-
Elevation Myocardial Infarction. Circulation
2010;122:A15055 [Abstract]
263. Kang HJ, Kim HS, Zhang SY, Park KW, Cho HJ, Koo BK, Kim
YJ, Soo LD, Sohn DW, Han KS, Oh BH, Lee MM, Park YB.
Effects of Intracoronary Infusion of Peripheral Blood Stem-
Cells Mobilised With Granulocyte-Colony Stimulating Factor
on Left Ventricular Systolic Function and Restenosis After
Coronary Stenting in Myocardial Infarction: the MAGIC Cell
Randomised Clinical Trial. Lancet 2004;363:751-6.
264. Steinwender C, Hofmann R, Kammler J, Kypta A, Pichler R,
Maschek W, Schuster G, Gabriel C, Leisch F. Effects of
Peripheral Blood Stem Cell Mobilization With Granulocyte-
Colony Stimulating Factor and Their Transcoronary
Transplantation After Primary Stent Implantation for Acute
Myocardial Infarction. Am Heart J 2006;151:1296-13.
265. Jørgensen E, Ripa RS, Helqvist S, Wang Y, Johnsen HE,
Grande P, Kastrup J. In-Stent Neo-Intimal Hyperplasia After
Stem Cell Mobilization by Granulocyte-Colony Stimulating
Factor Preliminary Intracoronary Ultrasound Results From a
Double-Blind Randomized Placebo-Controlled Study of
Patients Treated With Percutaneous Coronary Intervention
for ST-Elevation Myocardial Infarction (STEMMI Trial). Int J
Cardiol 2006;111:174-7.
266. Jørgensen E, Baldazzi F, Ripa RS, Friis T, Wang Y, Helqvist
S, Kastrup J. Instent Neointimal Hyperplasia After
Percutaneous Intervention for ST-Elevation Myocardial
Infarction and Treatment With Granulocyte-Colony
Stimulating Factor. Results From the Stem Cells in
Myocardial Infarction (STEMMI) Trial. Int J Cardiol
2010;139:269-75.
267. Ince H, Valgimigli M, Petzsch M, de Lezo JS, Kuethe F,
Dunkelmann S, Biondi-Zoccai G, Nienaber CA.
Cardiovascular Events and Re-Stenosis Following
Administration of G-CSF in Acute Myocardial Infarction:
Systematic Review and Meta-Analysis. Heart 2008;94:610-
6.
268. Haghighat A, Weiss D, Whalin MK, Cowan DP, Taylor WR.
Granulocyte Colony-Stimulating Factor and Granulocyte
Macrophage Colony-Stimulating Factor Exacerbate
Atherosclerosis in Apolipoprotein E-Deficient Mice.
Circulation 2007;115:2049-54.
269. Menasche P, Hagege AA, Vilquin JT, Desnos M, Abergel E,
Pouzet B, Bel A, Sarateanu S, Scorsin M, Schwartz K,
Bruneval P, Benbunan M, Marolleau JP, Duboc D.
Autologous Skeletal Myoblast Transplantation for Severe
Postinfarction Left Ventricular Dysfunction. J Am Coll
Cardiol 2003;41:1078-83.
270. Menasche P, Alfieri O, Janssens S, McKenna W,
Reichenspurner H, Trinquart L, Vilquin JT, Marolleau JP,
Seymour B, Larghero J, Lake S, Chatellier G, Solomon S,
Desnos M, Hagege AA. The Myoblast Autologous Grafting in
Ischemic Cardiomyopathy (MAGIC) Trial: First Randomized
Placebo-Controlled Study of Myoblast Transplantation.
Circulation 2008;117:1189-200.
271. Kuhlmann MT, Kirchhof P, Klocke R, Hasib L, Stypmann J,
Fabritz L, Stelljes M, Tian W, Zwiener M, Mueller M, Kienast
J, Breithardt G, Nikol S. G-CSF/SCF Reduces Inducible
Arrhythmias in the Infarcted Heart Potentially Via Increased
Connexin43 Expression and Arteriogenesis. J Exp Med
2006;203:87-97.
272. Overgaard M, Ripa RS, Wang Y, Jørgensen E, Kastrup J.
Timing of Granulocyte-Colony Stimulating Factor Treatment
After Acute Myocardial Infarction and Recovery of Left
Ventricular Function: Results From the STEMMI Trial. Int J
Cardiol 2010;140:351-5.
273. Engelmann MG, Theiss HD, Theiss C, Huber A,
Wintersperger BJ, Werle-Ruedinger AE, Schoenberg SO,
Steinbeck G, Franz WM. G-CSF in Patients Suffering From
Late Revascularized ST Elevation Myocardial Infarction:
Analysis on the Timing of G-CSF Administration. Exp
Hematol 2008;36:703-9.
274. Meluzin J, Mayer J, Groch L, Janousek S, Hornacek I,
Hlinomaz O, Kala P, Panovsky R, Prasek J, Kaminek M,
Stanicek J, Klabusay M, Koristek Z, Navratil M, Dusek L,
Vinklarkova J. Autologous Transplantation of Mononuclear
Bone Marrow Cells in Patients With Acute Myocardial
Infarction: the Effect of the Dose of Transplanted Cells on
Myocardial Function. Am Heart J 2006;152:975-15.
275. Iwase T, Nagaya N, Fujii T, Itoh T, Murakami S, Matsumoto
T, Kangawa K, Kitamura S. Comparison of Angiogenic
Potency Between Mesenchymal Stem Cells and
Mononuclear Cells in a Rat Model of Hindlimb Ischemia.
Cardiovasc Res 2005;66:543-51.
276. Pitchford SC, Furze RC, Jones CP, Wengner AM, Rankin SM.
Differential Mobilization of Subsets of Progenitor Cells From
the Bone Marrow. Cell Stem Cell 2009;4:62-72.
277. Brouard N, Driessen R, Short B, Simmons PJ. G-CSF
Increases Mesenchymal Precursor Cell Numbers in the Bone
Marrow Via an Indirect Mechanism Involving Osteoclast-
Mediated Bone Resorption. Stem Cell Res 2010;5:65-75.
278. Kawada H, Fujita J, Kinjo K, Matsuzaki Y, Tsuma M,
Miyatake H, Muguruma Y, Tsuboi K, Itabashi Y, Ikeda Y,
Ogawa S, Okano H, Hotta T, Ando K, Fukuda K.
Nonhematopoietic Mesenchymal Stem Cells Can Be
Mobilized and Differentiate into Cardiomyocytes After

- 51 -
Myocardial Infarction. Blood 2004;104:3581-7.
279. Delgaudine M, Lambermont B, Lancellotti P, Roelants V,
Walrand S, Vanoverschelde JL, Pierard L, Gothot A, Beguin
Y. Effects of Granulocyte-Colony-Stimulating Factor on
Progenitor Cell Mobilization and Heart Perfusion and
Function in Normal Mice. Cytotherapy 2011;13:237-47.
280. Cesselli D, Beltrami AP, Rigo S, Bergamin N, D'Aurizio F,
Verardo R, Piazza S, Klaric E, Fanin R, Toffoletto B,
Marzinotto S, Mariuzzi L, Finato N, Pandolfi M, Leri A,
Schneider C, Beltrami CA, Anversa P. Multipotent Progenitor
Cells Are Present in Human Peripheral Blood. Circ Res
2009;104:1225-34.
281. Tatsumi K, Otani H, Sato D, Enoki C, Iwasaka T, Imamura
H, Taniuchi S, Kaneko K, Adachi Y, Ikehara S. Granulocyte-
Colony Stimulating Factor Increases Donor Mesenchymal
Stem Cells in Bone Marrow and Their Mobilization into
Peripheral Circulation but Does Not Repair Dystrophic Heart
After Bone Marrow Transplantation. Circ J 2008;72:1351-8.
282. Delgaudine M, Gothot A, Beguin Y. Spontaneous and
Granulocyte-Colony-Stimulating Factor-Enhanced Marrow
Response and Progenitor Cell Mobilization in Mice After
Myocardial Infarction. Cytotherapy 2010;12:909-18.
283. Ince H, Petzsch M, Kleine HD, Eckard H, Rehders T, Burska
D, Kische S, Freund M, Nienaber CA. Prevention of Left
Ventricular Remodeling With Granulocyte Colony-
Stimulating Factor After Acute Myocardial Infarction: Final
1-Year Results of the Front-Integrated Revascularization
and Stem Cell Liberation in Evolving Acute Myocardial
Infarction by Granulocyte Colony-Stimulating Factor
(FIRSTLINE-AMI) Trial. Circulation 2005;112:I73-I80.
284. Neumann FJ, Blasini R, Schmitt C, Alt E, Dirschinger J,
Gawaz M, Kastrati A, Schomig A. Effect of Glycoprotein
IIb/IIIa Receptor Blockade on Recovery of Coronary Flow
and Left Ventricular Function After the Placement of
Coronary-Artery Stents in Acute Myocardial Infarction.
Circulation 1998;98:2695-701.
285. Ofili EO, Kern MJ, St Vrain JA, Donohue TJ, Bach R, al-
Joundi B, Aguirre FV, Castello R, Labovitz AJ. Differential
Characterization of Blood Flow, Velocity, and Vascular
Resistance Between Proximal and Distal Normal Epicardial
Human Coronary Arteries: Analysis by Intracoronary
Doppler Spectral Flow Velocity. Am Heart J 1995;130:37-
46.
286. Vulliet PR, Greeley M, Halloran SM, MacDonald KA, Kittleson
MD. Intra-Coronary Arterial Injection of Mesenchymal
Stromal Cells and Microinfarction in Dogs. Lancet
2004;363:783-4.
287. Kang HJ, Lee HY, Na SH, Chang SA, Park KW, Kim HK, Kim
SY, Chang HJ, Lee W, Kang WJ, Koo BK, Kim YJ, Lee DS,
Sohn DW, Han KS, Oh BH, Park YB, Kim HS. Differential
Effect of Intracoronary Infusion of Mobilized Peripheral
Blood Stem Cells by Granulocyte Colony-Stimulating Factor
on Left Ventricular Function and Remodeling in Patients
With Acute Myocardial Infarction Versus Old Myocardial
Infarction: the MAGIC Cell-3-DES Randomized, Controlled
Trial. Circulation 2006;114:I145-I151.
288. Lutz M, Rosenberg M, Kiessling F, Eckstein V, Heger T,
Krebs J, Ho AD, Katus HA, Frey N. Local Injection of Stem
Cell Factor (SCF) Improves Myocardial Homing of
Systemically Delivered C-Kit + Bone Marrow-Derived Stem
Cells. Cardiovasc Res 2008;77:143-50.
289. Theiss HD, Brenner C, Engelmann MG, Zaruba MM, Huber
B, Henschel V, Mansmann U, Wintersperger B, Reiser M,
Steinbeck G, Franz WM. Safety and Efficacy of SITAgliptin
Plus GRanulocyte-Colony-Stimulating Factor in Patients
Suffering From Acute Myocardial Infarction (SITAGRAMI-
Trial)--Rationale, Design and First Interim Analysis. Int J
Cardiol 2010;145:282-4.
290. Baks T, van Geuns RJ, Biagini E, Wielopolski P, Mollet NR,
Cademartiri F, Boersma E, van der Giessen WJ, Krestin GP,
Duncker DJ, Serruys PW, de Feyter PJ. Recovery of Left
Ventricular Function After Primary Angioplasty for Acute
Myocardial Infarction. Eur Heart J 2005;26:1070-7.
291. Brodie BR, Stuckey TD, Kissling G, Hansen CJ, Weintraub
RA, Kelly TA. Importance of Infarct-Related Artery Patency
for Recovery of Left Ventricular Function and Late Survival
After Primary Angioplasty for Acute Myocardial Infarction. J
Am Coll Cardiol 1996;28:319-25.
292. Stone GW, Grines CL, Cox DA, Garcia E, Tcheng JE, Griffin
JJ, Guagliumi G, Stuckey T, Turco M, Carroll JD, Rutherford
BD, Lansky AJ. Comparison of Angioplasty With Stenting,
With or Without Abciximab, in Acute Myocardial Infarction.
N Engl J Med 2002;346:957-66.
293. Jørgensen E, Madsen T, Kastrup J. Comparison of the Left
Ventricular Electromechanical Map Before Percutaneous
Coronary Stent Revascularization and at One-Month Follow-
Up in Patients With a Recent ST Elevation Infarction.
Catheter Cardiovasc Interv 2005;64:153-9.
294. Schroeder AP, Houlind K, Pedersen EM, Nielsen TT, Egeblad
H. Serial Magnetic Resonance Imaging of Global and
Regional Left Ventricular Remodeling During 1 Year After
Acute Myocardial Infarction. Cardiology 2001;96:106-14.
295. Petersen SE, Voigtlander T, Kreitner KF, Horstick G, Ziegler
S, Wittlinger T, Abegunewardene N, Schmitt M, Schreiber
WG, Kalden P, Mohrs OK, Lippold R, Thelen M, Meyer J.
Late Improvement of Regional Wall Motion After the
Subacute Phase of Myocardial Infarction Treated by Acute
PTCA in a 6-Month Follow-Up. J Cardiovasc Magn Reson
2003;5:487-95.
296. Nijveldt R, Beek AM, Hirsch A, Stoel MG, Hofman MB,
Umans VA, Algra PR, Twisk JW, van Rossum AC. Functional
Recovery After Acute Myocardial Infarction: Comparison
Between Angiography, Electrocardiography, and
Cardiovascular Magnetic Resonance Measures of

- 52 -
Microvascular Injury. J Am Coll Cardiol 2008;52:181-9.
297. Dill T, Schachinger V, Rolf A, Mollmann S, Thiele H,
Tillmanns H, Assmus B, Dimmeler S, Zeiher AM, Hamm C.
Intracoronary Administration of Bone Marrow-Derived
Progenitor Cells Improves Left Ventricular Function in
Patients at Risk for Adverse Remodeling After Acute ST-
Segment Elevation Myocardial Infarction: Results of the
Reinfusion of Enriched Progenitor Cells And Infarct
Remodeling in Acute Myocardial Infarction Study (REPAIR-
AMI) Cardiac Magnetic Resonance Imaging Substudy. Am
Heart J 2009;157:541-7.
298. Gerber BL, Wijns W, Vanoverschelde JL, Heyndrickx GR, De
BB, Bartunek J, Melin JA. Myocardial Perfusion and Oxygen
Consumption in Reperfused Noninfarcted Dysfunctional
Myocardium After Unstable Angina: Direct Evidence for
Myocardial Stunning in Humans. J Am Coll Cardiol
1999;34:1939-46.
299. Hombach V, Grebe O, Merkle N, Waldenmaier S, Hoher M,
Kochs M, Wohrle J, Kestler HA. Sequelae of Acute
Myocardial Infarction Regarding Cardiac Structure and
Function and Their Prognostic Significance As Assessed by
Magnetic Resonance Imaging. Eur Heart J 2005;26:549-57.
300. Fieno DS, Hillenbrand HB, Rehwald WG, Harris KR, Decker
RS, Parker MA, Klocke FJ, Kim RJ, Judd RM. Infarct
Resorption, Compensatory Hypertrophy, and Differing
Patterns of Ventricular Remodeling Following Myocardial
Infarctions of Varying Size. J Am Coll Cardiol
2004;43:2124-31.
301. Richard V, Murry CE, Reimer KA. Healing of Myocardial
Infarcts in Dogs. Effects of Late Reperfusion. Circulation
1995;92:1891-901.
302. Rogers WJ, Jr., Kramer CM, Geskin G, Hu YL, Theobald TM,
Vido DA, Petruolo S, Reichek N. Early Contrast-Enhanced
MRI Predicts Late Functional Recovery After Reperfused
Myocardial Infarction. Circulation 1999;99:744-50.
303. Saeed M, Lund G, Wendland MF, Bremerich J, Weinmann H,
Higgins CB. Magnetic Resonance Characterization of the
Peri-Infarction Zone of Reperfused Myocardial Infarction
With Necrosis-Specific and Extracellular Nonspecific
Contrast Media. Circulation 2001;103:871-6.
304. Oshinski JN, Yang Z, Jones JR, Mata JF, French BA. Imaging
Time After Gd-DTPA Injection Is Critical in Using Delayed
Enhancement to Determine Infarct Size Accurately With
Magnetic Resonance Imaging. Circulation 2001;104:2838-
42.
305. Kim RJ, Fieno DS, Parrish TB, Harris K, Chen EL, Simonetti
O, Bundy J, Finn JP, Klocke FJ, Judd RM. Relationship of
MRI Delayed Contrast Enhancement to Irreversible Injury,
Infarct Age, and Contractile Function. Circulation
1999;100:1992-2002.
306. Fieno DS, Kim RJ, Chen EL, Lomasney JW, Klocke FJ, Judd
RM. Contrast-Enhanced Magnetic Resonance Imaging of
Myocardium at Risk: Distinction Between Reversible and
Irreversible Injury Throughout Infarct Healing. J Am Coll
Cardiol 2000;36:1985-91.
307. Lipinski MJ, Biondi-Zoccai GG, Abbate A, Khianey R,
Sheiban I, Bartunek J, Vanderheyden M, Kim HS, Kang HJ,
Strauer BE, Vetrovec GW. Impact of Intracoronary Cell
Therapy on Left Ventricular Function in the Setting of Acute
Myocardial Infarction: a Collaborative Systematic Review
and Meta-Analysis of Controlled Clinical Trials. J Am Coll
Cardiol 2007;50:1761-7.
308. Kawamoto A, Iwasaki H, Kusano K, Murayama T, Oyamada
A, Silver M, Hulbert C, Gavin M, Hanley A, Ma H, Kearney
M, Zak V, Asahara T, Losordo DW. CD34-Positive Cells
Exhibit Increased Potency and Safety for Therapeutic
Neovascularization After Myocardial Infarction Compared
With Total Mononuclear Cells. Circulation 2006;114:2163-9.
309. Pittenger MF, Mackay AM, Beck SC, Jaiswal RK, Douglas R,
Mosca JD, Moorman MA, Simonetti DW, Craig S, Marshak
DR. Multilineage Potential of Adult Human Mesenchymal
Stem Cells. Science 1999;284:143-7.
310. Haack-Sørensen M, Friis T, Bindslev L, Mortensen S,
Johnsen HE, Kastrup J. Comparison of Different Culture
Conditions for Human Mesenchymal Stromal Cells for
Clinical Stem Cell Therapy. Scand J Clin Lab Invest
2008;68:192-203.
311. Haack-Sørensen M, Friis T, Kastrup J. Mesenchymal
Stromal Cell and Mononuclear Cell Therapy in Heart
Disease. Future Cardiology 2008;4:481-94.
312. Hare JM, Traverse JH, Henry TD, Dib N, Strumpf RK,
Schulman SP, Gerstenblith G, DeMaria AN, Denktas AE,
Gammon RS, Hermiller JB, Jr., Reisman MA, Schaer GL,
Sherman W. A Randomized, Double-Blind, Placebo-
Controlled, Dose-Escalation Study of Intravenous Adult
Human Mesenchymal Stem Cells (Prochymal) After Acute
Myocardial Infarction. J Am Coll Cardiol 2009;54:2277-86.
313. Hofmann M, Wollert KC, Meyer GP, Menke A, Arseniev L,
Hertenstein B, Ganser A, Knapp WH, Drexler H. Monitoring
of Bone Marrow Cell Homing into the Infarcted Human
Myocardium. Circulation 2005;111:2198-202.
314. He G, Zhang H, Wei H, Wang Y, Zhang X, Tang Y, Wei Y,
Hu S. In Vivo Imaging of Bone Marrow Mesenchymal Stem
Cells Transplanted into Myocardium Using Magnetic
Resonance Imaging: a Novel Method to Trace the
Transplanted Cells. Int J Cardiol 2007;114:4-10.
315. Kjær A, Lebech AM. [Leukocyte Scintigraphy: Indications
and Diagnostic Value]. Ugeskr Laeger 2001;163:4380-4.
316. Jin Y, Kong H, Stodilka RZ, Wells RG, Zabel P, Merrifield PA,
Sykes J, Prato FS. Determining the Minimum Number of
Detectable Cardiac-Transplanted 111In-Tropolone-Labelled
Bone-Marrow-Derived Mesenchymal Stem Cells by SPECT.
Phys Med Biol 2005;50:4445-55.

- 53 -
317. Gholamrezanezhad A, Mirpour S, Ardekani JM, Bagheri M,
Alimoghadam K, Yarmand S, Malekzadeh R. Cytotoxicity of
111In-Oxine on Mesenchymal Stem Cells: a Time-
Dependent Adverse Effect. Nucl Med Commun
2009;30:210-6.
318. Bindslev L, Haack-Sørensen M, Bisgaard K, Kragh L,
Mortensen S, Hesse B, Kjaer A, Kastrup J. Labelling of
Human Mesenchymal Stem Cells With Indium-111 for
SPECT Imaging: Effect on Cell Proliferation and
Differentiation. Eur J Nucl Med Mol Imaging 2006;33:1171-
7.
319. Schächinger V, Aicher A, Dobert N, Rover R, Diener J,
Fichtlscherer S, Assmus B, Seeger FH, Menzel C, Brenner
W, Dimmeler S, Zeiher AM. Pilot Trial on Determinants of
Progenitor Cell Recruitment to the Infarcted Human
Myocardium. Circulation 2008;118:1425-32.
320. Goussetis E, Manginas A, Koutelou M, Peristeri I,
Theodosaki M, Kollaros N, Leontiadis E, Theodorakos A,
Paterakis G, Karatasakis G, Cokkinos DV, Graphakos S.
Intracoronary Infusion of CD133+ and CD133-CD34+
Selected Autologous Bone Marrow Progenitor Cells in
Patients With Chronic Ischemic Cardiomyopathy: Cell
Isolation, Adherence to the Infarcted Area, and Body
Distribution. Stem Cells 2006;24:2279-83.
321. Caveliers V, De KG, Everaert H, Van R, I, Van CG, Verheye
S, Roland J, Schoors D, Franken PR, Schots R. In Vivo
Visualization of 111In Labeled CD133+ Peripheral Blood
Stem Cells After Intracoronary Administration in Patients
With Chronic Ischemic Heart Disease. Q J Nucl Med Mol
Imaging 2007;51:61-6.
322. Kurpisz M, Czepczynski R, Grygielska B, Majewski M, Fiszer
D, Jerzykowska O, Sowinski J, Siminiak T. Bone Marrow
Stem Cell Imaging After Intracoronary Administration. Int J
Cardiol 2007;121:194-5.
323. Zhou R, Thomas DH, Qiao H, Bal HS, Choi SR, Alavi A,
Ferrari VA, Kung HF, Acton PD. In Vivo Detection of Stem
Cells Grafted in Infarcted Rat Myocardium. J Nucl Med
2005;46:816-22.
324. Tossios P, Krausgrill B, Schmidt M, Fischer T, Halbach M,
Fries JW, Fahnenstich S, Frommolt P, Heppelmann I,
Schmidt A, Schomacker K, Fischer JH, Bloch W, Mehlhorn
U, Schwinger RH, Muller-Ehmsen J. Role of Balloon
Occlusion for Mononuclear Bone Marrow Cell Deposition
After Intracoronary Injection in Pigs With Reperfused
Myocardial Infarction. Eur Heart J 2008;29:1911-21.
325. Aicher A, Brenner W, Zuhayra M, Badorff C, Massoudi S,
Assmus B, Eckey T, Henze E, Zeiher AM, Dimmeler S.
Assessment of the Tissue Distribution of Transplanted
Human Endothelial Progenitor Cells by Radioactive Labeling.
Circulation 2003;107:2134-9.
326. Brenner W, Aicher A, Eckey T, Massoudi S, Zuhayra M,
Koehl U, Heeschen C, Kampen WU, Zeiher AM, Dimmeler S,
Henze E. 111In-Labeled CD34+ Hematopoietic Progenitor
Cells in a Rat Myocardial Infarction Model. J Nucl Med
2004;45:512-8.
327. Hou D, Youssef EA, Brinton TJ, Zhang P, Rogers P, Price ET,
Yeung AC, Johnstone BH, Yock PG, March KL. Radiolabeled
Cell Distribution After Intramyocardial, Intracoronary, and
Interstitial Retrograde Coronary Venous Delivery:
Implications for Current Clinical Trials. Circulation
2005;112:I150-I156.
328. Amsalem Y, Mardor Y, Feinberg MS, Landa N, Miller L,
Daniels D, Ocherashvilli A, Holbova R, Yosef O, Barbash IM,
Leor J. Iron-Oxide Labeling and Outcome of Transplanted
Mesenchymal Stem Cells in the Infarcted Myocardium.
Circulation 2007;116:I38-I45.
329. Terrovitis J, Stuber M, Youssef A, Preece S, Leppo M,
Kizana E, Schar M, Gerstenblith G, Weiss RG, Marban E,
Abraham MR. Magnetic Resonance Imaging Overestimates
Ferumoxide-Labeled Stem Cell Survival After
Transplantation in the Heart. Circulation 2008;117:1555-
62.
330. Gyongyosi M, Blanco J, Marian T, Tron L, Petnehazy O,
Petrasi Z, Hemetsberger R, Rodriguez J, Font G, Pavo IJ,
Kertesz I, Balkay L, Pavo N, Posa A, Emri M, Galuska L,
Kraitchman DL, Wojta J, Huber K, Glogar D. Serial
Noninvasive In Vivo Positron Emission Tomographic
Tracking of Percutaneously Intramyocardially Injected
Autologous Porcine Mesenchymal Stem Cells Modified for
Transgene Reporter Gene Expression. Circ Cardiovasc
Imaging 2008;1:94-103.
331. Zimmermann WH, Melnychenko I, Wasmeier G, Didie M,
Naito H, Nixdorff U, Hess A, Budinsky L, Brune K, Michaelis
B, Dhein S, Schwoerer A, Ehmke H, Eschenhagen T.
Engineered Heart Tissue Grafts Improve Systolic and
Diastolic Function in Infarcted Rat Hearts. Nat Med
2006;12:452-8.
332. Feinberg AW, Feigel A, Shevkoplyas SS, Sheehy S,
Whitesides GM, Parker KK. Muscular Thin Films for Building
Actuators and Powering Devices. Science 2007;317:1366-
70.


Clinical researchCoronary heart disease
Intramyocardial injection of vascular endothelial growthfactor-A165 plasmid followed by granulocyte-colonystimulating factor to induce angiogenesis in patientswith severe chronic ischaemic heart disease
Rasmus Sejersten Ripa1,2, Yongzhong Wang1, Erik Jørgensen1, Hans Erik Johnsen3, Birger Hesse4,and Jens Kastrup1*
1Medical Department B, Cardiac Catheterization Laboratory 2014, The Heart Centre, University Hospital Rigshospitalet,DK-2100 Copenhagen Ø, Denmark; 2Department of Radiology, University Hospital Rigshospitalet, Copenhagen, Denmark;3Department of Haematology, Aalborg University Hospital, Aalborg, Denmark; and 4Department of Clinical Physiology,University Hospital Rigshospitalet, Copenhagen, Denmark
Received 11 December 2005; revised 22 May 2006; accepted 2 June 2006; online publish-ahead-of-print 6 July 2006
Aims To assess the safety and effects of combined treatment with vascular endothelial growthfactor-A165 plasmid (VEGF-A165) and granulocyte- colony stimulating factor (G-CSF) mobilization ofbone marrow stem cells in patients with severe chronic ischaemic heart disease (IHD).Methods and results Sixteen patients with severe chronic IHD were treated with intramyocardial injec-tions of VEGF-A165 plasmid followed 1 week later by G-CSF (10 mg/kg/day for 6 days). Two control groupsincluded (i) sixteen patients treated with intramyocardial injections of VEGF-A165 plasmid and (ii)sixteen patients treated with intramyocardial injections of placebo. In the G-CSF group, circulatingCD34þ stem cells increased almost 10-fold compared with the control groups (P , 0.0001). After3 months, there was no improvement in myocardial perfusion at single photon emission computerizedtomography in the VEGF-A165 and G-CSF treated group, and clinical symptoms were unchanged.There were no side effects to the gene and G-CSF therapy.Conclusion Intramyocardial VEGF-A165 gene transfer followed by bone marrow stem cell mobilizationwith G-CSF seemed safe. However, a significant increase in circulating stem cells did not lead toimproved myocardial perfusion or clinical effects suggesting a neutral effect of the treatment. Toimprove homing of stem cells, higher doses of VEGF-A165 and/or use of SDF-1 transfer might beconsidered.
KEYWORDSCardiovascular diseases;
Gene therapy;
Stem cell;
Angiogenesis;
G-CSF
Introduction
Several vascular growth factors have the potential toinduce angiogenesis in ischaemic tissue.1–3 However, onlyvascular endothelial growth factor (VEGF) and fibroblastgrowth factor (FGF) have been tested in clinical studiesof patients with occlusive coronary artery disease(CAD).4–10 Small and unblinded gene therapy studies ofintramyocardial delivered genes encoding VEGF-A165 orVEGF-A121 have been performed in patients with severeCAD and results have been encouraging, demonstratingboth clinical improvement and evidence of angiogen-esis.5,8–10 However, in the first large double-blind random-ized placebo-controlled study, we could not demonstratesignificant improvement in myocardial perfusion, whencompared with placebo.4
Haematopoietic stem cells from the bone marrow havethe potential to induce vasculogenesis in animals with anacute myocardial infarction.11,12 Recent human studiesindicate that mononuclear cell solutions aspirated fromthe bone marrow can induce vasculogenesis both inacute and chronic myocardial ischaemia.13–19 However, itremains unknown, whether the vasculogenesis is inducedby the few (2–3%) stem cells within the mononuclear cellssuspension17 or by cytokines released from the leucocytes.It has been demonstrated that treatment with granulocyte-colony stimulating factor (G-CSF), in order to mobilize stemcells from the bone marrow, does not induce vasculogenesisin patients with chronic myocardial ischaemia20,21 or follow-ing acute myocardial infarction.22 Animal studies suggestthat a combination of treatment with VEGF-A gene transferfollowed by G-CSF mobilization of stem cells might besuperior to either of the therapies.23
The aim of the present study was, in a clinical phase Isafety and efficacy study, to evaluate the safety and clinical
& The European Society of Cardiology 2006. All rights reserved. For Permissions, please e-mail: [email protected]
* Corresponding author. Tel: þ45 3545 2817; fax: þ45 3545 2805.E-mail address: [email protected]
European Heart Journal (2006) 27, 1785–1792doi:10.1093/eurheartj/ehl117

effect of VEGF-A165 gene transfer followed by bone marrowstimulation with G-CSF to induce myocardial vasculogenesisin patients with severe occlusive CAD.
Methods
Population
Patients were eligible in the study if they had (i) significant revers-ible myocardial ischaemia on an adenosine stress single photonemission computerized tomography (SPECT) as judged by an experi-enced nuclear physician blinded to all other patient data, (ii) atleast one remaining large coronary vessel from which new collat-erals/vessels could be supplied, (iii) age between 18 and 75 years,(iv) stable angina pectoris and Canadian Cardiovascular Society(CCS) class �3. Excluded were patients with (i) unstable angina pec-toris, (ii) acute myocardial infarction within the last 3 months, (iii)diabetes mellitus with proliferative retinopathy, (iv) diagnosedor suspected cancer, (v) chronic inflammatory disease, and(vi) fertile women.All patients received oral and written information, and signed a
written informed consent. The study followed the recommendationsof the Helsinki II Declaration and was approved by the EthicsCommittee of Copenhagen (KF 01-130/01) and the Danish DrugAgency (2612-1490). The study has been registered in clinicaltrial.gov (NCT00135850).
Study design
We prospectively treated 16 patients with severe chronic CAD andno option for revascularization with open-label VEGF-A165 genetransfer followed by G-CSF bone marrow stem cell mobilization(15 men, 1 woman, mean age 62 years, Table 1). Patients weretreated with direct intramyocardial injections of the VEGF-A165plasmid followed one week later by in-hospital daily subcutaneousinjection of 10 mg/kg body weight G-CSF (Neupogenw) for 6 days.We (Rigshospitalet, Copenhagen) have previously randomized atotal of 32 patients (16 active and 16 placebo) in the double-blindEuroinject One multicentre trial.4 These patients were used as con-trols: (i) sixteen patients treated with VEGF gene transfer alone (15men, 1 woman, mean age 61 years) and (ii) sixteen patients treatedwith placebo gene injections (14 men, 2 women, mean age 62years). Inclusion criteria in Euroinject One and the present trialwere identical.Before inclusion, patients had a screening of blood tests, urinary
tests, stools for occult blood � 3, and chest X-ray. Patients with dia-betes mellitus had an opthalmoscopy, and a mammography was per-formed in all women. All patients were scheduled to undergoclinical examination, exercise test, stress SPECT, coronary angiogra-phy, and cardiac magnetic resonance imaging (MRI) before the genetransfer and 3 months after. In addition, a clinical examination wasperformed after 1 month. Peripheral circulating stem cells (CD34þcells) and biochemistry controls were measured before and on day7, 14, 21, and 30 after treatment. Circulating CD34þ progenitorcells were determined by flow cytometry and plasma VEGF-A165and SDF-1 by ELISA.A total of 73 patients were screened for inclusion; 50 of these
were eligible for inclusion but two refused consent resulting in apatient population of 48 (16 in each group). All patients in allthree groups (except one patient in the placebo group who died)went through the 3 months follow-up as planned.
Safety assessment
Each patient was carefully examined and interviewed about possibleside-effects to the treatment by a physician the day after the gene/placebo injection, after the G-CSF treatment, and at the 1 and 3month visits. All adverse and serious adverse events (SAEs) withinthe 3-month follow-up period were recorded in all groups. SAEs
are defined as any adverse events that result in any of the followingoutcomes: death, life-threatening conditions, hospitalization orprolongation of existing hospitalization, persistent or significantdisability/incapacity, medically significant event (includes seriouslaboratory abnormalities), and any new cancer.
Efficacy assessment
The pre-specified efficacy endpoint was changes in perfusion defectsat stress SPECT from baseline to 3 months follow-up. Secondaryexploratory endpoints were change in (i) CCS angina class,(ii) Seattle Angina Pectoris Questionnaire (SEQ) scores, (iii) frequencyof angina attacks, (iv) nitroglycerine consumption, (v) exercisecapacity, and (vi) left ventricular volumes measured by SPECTand MRI.
Single photon emission computerized tomography
SPECT studies were performed as a 2-day protocol (500–700 MBq99mTc-sestamibi at each study) with adenosine infusion over4–6 min (0.14 mg/kg/min by infusion pump), combined with a sub-maximal exercise test except in patients with left bundle branchblock.24,25 Care was taken to perform the stress tests at theinclusion and at the follow-up studies with identical cumulative ade-nosine doses and identical sub-maximal exercise loads. Gated (eightframes) imaging was performed with a two-headed Millennium GEgamma camera, with a Gadolinium interleaved attenuation-scattercorrection. A disk with investigations of nine patients belonging toVEGF-A165 and 10 patients to the placebo group was accidentallydestroyed and was technically unreadable. Therefore, these dataare missing in the comparison analyses.
An independent core laboratory (Bio-Imaging Technologies B.V.,Leiden, The Netherlands) performed blinded readings of theSPECT investigations.
NOGAw—electromechanical mapping of leftventricle
Electromechanical evaluation of the left ventricle was performedwith the NOGAw system (Biosense Webster A/S, Cordis, Johnson &Johnson) as previously described.4,26,27 The diagnostic NOGAw
catheter was introduced percutaneously via the groin into the leftventricle. A sensor at the tip of the catheter in contact withthe endocardial surface registered the local myocardial unipolarvoltage and regional wall motion/contraction (local shortening)within the left ventricle, and created a three-dimensional colourimage of the left ventricle as described previously.4
Intramyocardial injections
The intramyocardial injections were done with the 8-french-sizedMyostarw mapping-injection catheter (Biosense Webster A/S,Cordis, Johnson & Johnson) inserted into the left ventricle via thegroin.4 Ten 0.3 mL injections were given around and within thearea with reversible ischaemia with a total dose of 0.5 mgVEGF-A165 or placebo plasmid. The injections were performedslowly (30–40 s) and only to areas with unipolar voltage above5 mV and with a thickness of the ventricle wall on echocardiographyexceeding 6 mm.
Quality control of the injections included (i) the catheter’s tipperpendicular (+308) to the left ventricular wall in two planes,(i) the loop stability at the same level as during the mapping pro-cedure, if possible ,2 mm, and (iii) one or more ectopic extraven-tricular beats should appear in the exact moment of the protrusionof the injection needle into the myocardium.
Plasmid VEGF-A165 and placebo plasmid
The plasmid contained a cytomegalovirus promotor/enhancer todrive VEGF-A165 expression. The placebo plasmid was identical to
1786 R.S. Ripa et al.

the plasmid VEGF-A165 except for the VEGF-A165 gene that had beencut out, as previously described.4
Magnetic resonance imaging
MRI was only performed in the VEGF-A165þ G-CSF group and was notfeasible in six patients due to claustrophobia or obesity. Myocardialfunction and perfusion were examined by MRI before and 3 monthsafter VEGF-A165 and G-CSF treatment. The examinations wereperformed with 1.5 T (Siemens Vision Magnetom, Siemens AG,Erlangen, Germany) using a standard phased-array chest coil. Leftventricular volumes and systolic function were derived from succes-sive short axis slices. Volumes were determined by planimetry andmyocardial mass was determined by applying a density factor of1.05 g/cm3.
Perfusion estimates were obtained from images acquired in asingle position in the true short axis of the left ventricle startingimmediately after intravenous injection of gadopentetate dimeglu-mine (Magnevistw, Schering AG) (0.1 mmol/kg) during intravenousinfusion of adenosine (0.14 mg/kg/min), which was allowed toreach steady-state concentration during 2 min initial infusion.Myocardial perfusion was assessed as the change in MR signal inten-sity as a function of time during the first pass (initial slope).28
The investigations were analysed blinded to all patient-data,using the CMRtools software.
Statistical analysis
The sample size of 16 patients in the combined VEGF-A165 gene andG-CSF group was calculated to yield an expected power of 0.8 todetect a difference of 30% from baseline to 3 months follow-up inperfusion defects at stress SPECT, with a two-sided significancelevel of 0.05 and an assumed standard deviation (of the differences)of 4, on the basis of previous results.4
Baseline characteristics were compared using Fischer’s exact testfor categorical or one-way ANOVA for continuous variables.
For comparisons between baseline and follow-up data within thegroups, we used Wilcoxon signed-ranks test, whereas betweengroup comparisons were done using one-way ANOVA. All data wereanalysed using SPSS statistical analysis program (SPSS version
12.0, SPSS Inc., Chicago, Il, USA). To account for multiple testing,a difference was only considered statistically significant if two-sidedP, 0.01.
Results
The baseline characteristics of the patients are depictedin Table 1. All patients had severe stable chronic anginapectoris and limited exercise capacity. They were all onmaximal tolerable anti-angina therapy with short- and long-lasting nitroglycerin, calcium antagonists, beta-blockers,and ACE-inhibitors. All had previously been treated with atleast one coronary artery bypass surgery or percutaneouscoronary intervention (PCI).
Safety data
There were no major side effects during the combinedVEGF-A165 gene and G-CSF treatment or in the follow-upperiod. During G-CSF treatment, two patients had slightmuscular discomfort, which disappeared after NSAID treat-ment. One patient with a previous history of a gall bladderstone abdominal pains developed acute abdominal painsand increase in plasma liver parameters. Symptoms andliver test normalized immediately after cessation of G-CSFtreatment. No change was seen in liver function tests inthe remaining patients.Five patients in the placebo group had SAEs: one
ST-elevation myocardial infarction (STEMI) with third-degree AV-blockade, the patient progressed into cardiogenicshock despite implantation of a pacemaker and sub-sequently died 2 months after the placebo treatment; twouncomplicated STEMI; one non-STEMI; and one newly devel-oped coronary in-stent stenosis, which needed treatmentwith PCI. In the plasmid VEGF-A165 group, three patientsdeveloped new coronary artery in-stent stenoses with symp-toms of unstable angina.
Table 1 Demographic data for patients treated with placebo, plasmid VEGF-A165, or plasmid VEGF-A165 andG-CSF at baseline
Placebo(n ¼ 16)
VEGF-A165(n ¼ 16)
VEGF-A165þ G-CSF(n ¼ 16)
P-value
Age (years) 62+ 9 61+ 7 62+ 9 0.9Gender (m/f) (14/2) (15/1) (14/2) 0.8Body mass index (kg/m2) 29+ 5 28+ 3 29+ 4 0.7Current smoker, n (%) 1 (6) 4 (25) 2 (13) 0.5Diabetes mellitus, n (%) 1 (6) 4 (25) 7 (44) 0.06Hypertension, n (%) 6 (38) 9 (56) 7 (44) 0.7Hypercholesterolaemia, n (%) 16 (100) 16 (100) 16 (100) 1.0Previous CABG, n (%) 14 (88) 16 (100) 16 (100) 0.3Previous PCI, n (%) 10 (63) 11 (69) 9 (56) 0.8Previous STEMI, n (%) 11 (69) 7 (44) 6 (38) 0.3LVEF (%) 53+ 11 57+ 9 57+ 10 0.4CCS 3.0+ 0.0 3.1+ 0.3 3.0+ 0.0 0.4Number of patients with two
or three-vessels disease, n2/14 3/13 4/12 0.9
Occluded vessel segments(LM/LAD/LCX/RCA), n
4/12/13/14 2/13/13/12 2/14/13/12 1.0
LVEF, left ventricular ejection fraction measured by ventriculography; CABG, coronary artery bypass grafting; CCS, CanadianCardiovascular Society angina classification; LM, left main artery; LAD, left anterior descending artery; LCX, left circumflexartery; RCA, right coronary artery.Values are expressed as mean+ SD or n (%).
VEGF gene and stem cell therapy in IHD 1787

Single photon emission computerized tomography
The combined VEGF-A165 and G-CSF treated group had nochanges in myocardial perfusion at rest and stress betweenbaseline and follow-up, and they had identical summeddifference perfusion scores (Table 2). Left ventricular end-diastolic (EDV) and end-systolic volumes (ESV), and ejectionfraction showed no significant difference in any of the threegroups from baseline to follow-up, and there were no differ-ences between changes in these parameters between groups(Table 3). In addition, regional wall thickening and motionwere unchanged from baseline to follow-up in the grouptreated with VEGF-A165 and G-CSF (Table 4).
Clinical outcome
There was no significant difference in changes in CCS classifi-cation, angina pectoris attacks, NTG consumption, or exer-cise time between the three groups (Table 5). This patternwas unchanged, also after classifying patients in theVEGF-Aþ G-CSF group into CD34þ stem cell responders andnon-responders. The SEQ scores demonstrated improvementin physical limitation, angina stability, and angina frequencyin all groups, and improvement in treatment satisfactionand disease perception in the VEGF gene transfer group only.
Magnetic resonance imaging
Both EDV and ESV increased, and the change in ESV from 40to 46 mL was statistically significant (P ¼ 0.009, Table 6).However, the increase in ESV did not change the left ventri-cular ejection fraction significantly, and there was no differ-ence in left ventricular mass. There was no significantincrease in perfusion in the region treated with gene injec-tions (Table 6). Representative images of the myocardialperfusion are shown in Figure 1.
Plasma VEGF-A165, SDF-1, and CD341progenitor cells
Circulating CD34þ stem cells from the bone marrowincreased significantly during the G-CSF treatment, with
Table 3 Left ventricular ejection fraction and volumes at restmeasured by SPECT in patients treated with placebo, plasmidVEGF-A165, or the combined plasmid VEGF-A165–G-CSF
Baseline Follow-up P-value
Placebo (n ¼ 6)EDV (mL) 139+ 48 147+ 47 0.4ESV (mL) 83+ 36 85+ 46 1.0Ejectionfraction (%)
42+ 6 45+ 11 0.3
VEGF treated (n ¼ 7)EDV (mL) 137+ 43 132+ 44 0.3ESV (mL) 71+ 34 69+ 38 0.5Ejectionfraction (%)
50+ 9 50+ 11 0.6
VEGFþ G-CSFtreated (n ¼ 11)EDV (mL) 131+ 50 125+ 47 0.4ESV (mL) 68+ 38 66+ 39 0.7Ejection fraction (%) 51+ 10 51+ 11 0.3
Mean+ SD.
Table
2Myo
cardialperfusion
atrest
andstress
mea
suredbySP
ECTin
allpatients
Place
bo(n
¼5)
VEG
F-A165(n
¼6)
VEG
F-A165þG-CSF
(n¼
14)
Differenc
efrom
baselineto
follow
-up
Baseline
Follow
-up
P-va
lue
Baseline
Follow
-up
P-va
lue
Baseline
Follow
-up
P-va
lue
Place
boVEG
F-A165
VEG
F-A165þ
G-CSF
P-va
lue
Summed
stress
scorea
17.8
+8.2
14.0
+9.5
0.06
13.0
+7.4
10.8
+6.8
0.2
12.7
+7.1
12.1
+8.5
0.6
23.8+
1.6
22.2+
3.3
20.6+
3.4
0.1
Summed
rest
scorea
5.0+
7.0
5.3+
4.6
0.7
2.6+
4.3
4.1+
5.1
0.3
3.6+
4.7
3.4+
5.3
0.8
0.3+
3.6
1.6+
3.2
20.2+
1.7
0.3
Summed
differenc
escore
11.6
+6.6
8.2+
7.4
0.2
9.5+
4.8
5.2+
4.2
0.1
8.6+
5.3
8.5+
7.1
0.7
23.4+
4.6
24.3+
5.4
20.1+
3.9
0.1
Mea
n+
SD.
aBased
onperfusion
score(ran
ging
from
0to
4)forall20
segm
ents.
1788 R.S. Ripa et al.

normalization after 1 week (Figure 2A). At all other timepoints, the CD34þ levels were identical between the threegroups. However, four patients were ‘poor mobilizers’ tothe G-CSF treatment (max CD34þ cells ,15.000/mLblood) with a maximal increase in CD34þ cells to 8.000+2.050/mL blood (mean+ SD) compared with 60.182+11.024/mL blood in ‘mobilizers’ (max CD34þ � 12.000/mLblood). This phenomenon is well known from clinicalhaematology.At baseline SDF-1 was lower in the control group com-
pared with the two active treated groups (Figure 2B).SDF-1 decreased non-significantly during G-CSF treatmentand then increased and tended to be higher after theG-CSF treatment (P ¼ 0.06, Figure 2B).The baseline level of plasma VEGF-A165 varied within the
groups, but there was no difference between baselinelevels. Plasma VEGF-A165 increased in the two VEGF-A165
Table 5 Changes in angina attack and exercise time in patientstreated with placebo, plasmid VEGF-A165, or plasmid VEGF-A165
and G-CSF
Placebo(n ¼ 16)
VEGF-A165(n ¼ 16)
VEGF-A165þG-CSF(n ¼ 16)
P-value
CCSanginaclassifi-cation
20.9+ 0.8 20.5+ 0.8 21.0+ 0.9 0.2
Frequencyof nitro-glycerineconsump-tion perday
0.3+ 2.2 21.3+ 2.3 21.0+ 1.6 0.1
Frequencyof anginalattacks perday
0.5+ 2.1 21.2+ 2.9 20.4+ 1.2 0.2
Exercisetime (s)
27+ 157 248+ 91 5+ 93 0.2
Mean+ SD.
Table 6 Left ventricular volumes, mass, ejection fraction, andperfusion measured by MRI in gene-injected area in patientstreated with VEGF-A165 and G-CSF
Baseline(n ¼ 10)
Follow-up(n ¼ 10)
P-value
EDV (mL) 102+ 32 109+ 33 0.12ESV (mL) 40+ 20 46+ 23 0.01Left ventricular
mass190+ 66 194+ 62 0.40
Left ventricularejectionfraction (%)
62+ 10 60+ 10 0.14
Perfusion ininjection-areain % of normal-area
62+ 32 74+ 32 0.16
Mean+ SD.
Table
4Re
gion
alwallthicke
ning
andmotionat
rest
mea
suredbySP
ECT
Place
bo(n
¼6)
VEG
F-A165(n
¼7)
VEG
F-A165þ
G-CSF
(n¼
11)
Differenc
efrom
baselineto
follow
-up
Baseline
Follow
-up
P-va
lue
Baseline
Follow
-up
P-va
lue
Baseline
Follow
-up
P-va
lue
Place
bo
VEG
F-A165
VEG
F-A165þ
G-CSF
P-va
lue
Region
alwallthicke
ning
in%from
end-diastoleto
end-systole
Apex
(%)
37+
1244
+18
0.2
41+
1144
+14
0.3
44+
1444
+17
0.7
7+
103+
70+
50.2
Lateralwall(%)
20+
821
+9
0.7
26+
828
+11
0.2
30+
1029
+10
0.7
1+
53+
40+
50.4
Intrav
entricular
septum
(%)
22+
325
+8
0.3
29+
630
+8
0.9
28+
930
+10
0.1
3+
61+
52+
40.8
Inferior
wall(%)
16+
417
+8
0.8
25+
625
+10
0.8
26+
824
+8
0.4
2+
80+
621+
60.7
Anteriorwall(%)
26+
329
+6
0.3
29+
731
+7
0.2
30+
832
+10
0.2
3+
42+
52+
40.9
Region
alinne
rwallmotion(0–1
0mm
rang
e)Apex
(mm)
5.1+
1.1
5.9+
1.7
0.1
4.8+
1.8
5.3+
2.3
0.4
5.6+
1.9
5.5+
2.4
0.6
0.7+
1.0
0.5+
0.9
20.1+
0.9
0.2
Lateralwall(m
m)
7.5+
1.6
7.8+
1.4
0.5
9.6+
0.9
9.5+
1.3
0.8
9.3+
1.8
9.4+
1.6
1.0
0.4+
1.2
20.1+
0.9
0.1+
1.0
0.8
Septalwall(m
m)
1.9+
1.0
2.4+
1.4
0.3
2.1+
2.0
2.2+
2.3
1.0
2.5+
1.9
2.4+
1.9
0.5
0.5+
0.9
0.1+
1.1
20.1+
0.4
0.4
Inferior
wall(m
m)
3.6+
0.7
4.2+
2.0
0.5
5.6+
1.9
5.5+
2.2
0.8
5.2+
1.8
5.0+
1.3
0.7
0.6+
2.0
20.1+
1.5
20.3+
1.3
0.5
Anteriorwall(m
m)
7.5+
1.0
7.9+
0.7
0.2
8.3+
1.0
8.6+
1.1
0.6
8.2+
1.2
8.3+
1.6
0.5
0.3+
0.7
0.3+
1.0
0.1+
0.8
0.8
Mea
n+
SD.
VEGF gene and stem cell therapy in IHD 1789

treated groups and in the placebo group 1 week after theintramyocardial injections (Figure 2C).
Discussion
We present the first, single-centre, clinical safety and effi-cacy trial, in which patients with chronic reversible myocar-dial ischaemia have been treated with intramyocardialinjections of the gene encoding VEGF-A165, followed bytreatment for 6 days with G-CSF stem cell mobilizationfrom the bone marrow. This treatment was well toleratedwith no increase in adverse events, when compared withgene transfer or placebo or G-CSF treatment alone.4,20,21
Several small and uncontrolled clinical studies have indi-cated that growth factor gene transfer might be safe andhave the potential to improve myocardial perfusion.5,8–10
In the first large double-blind placebo-controlled study, wecould not demonstrate improved myocardial perfusionafter VEGF-A165 gene transfer compared with placebo inpatients with severe CAD.4 However, the study may havebeen underpowered since we found a significant improve-ment within the VEGF-A165 group. Also, in a comparablegroup of patients, we found that G-CSF mobilization ofstem cells from the bone marrow did not improve myocar-dial perfusion or symptoms.20 Animal studies have suggestedthat the combination of gene transfer for VEGF-A165 andG-CSF mobilization of stem cells from the bone marrowinduce angiogenesis more effectively than gene therapyalone.23
In the present study, we could not demonstrate a signifi-cant improvement in myocardial perfusion or symptoms inpatients with chronic reversible myocardial ischaemiaafter the combined therapy with gene transfer of VEGFand subsequent bone marrow stimulation with G-CSF. Thediscrepancy between animal research and studies in
patients, as the present one, might be related to the defi-nition of chronic ischaemia. In animal studies, chronicischaemia will include components of acute and subacuteischaemia as well. Most animal studies induce chronic myo-cardial ischaemia, using an ameroid constrictor around thecircumflex or anterior descendent artery. Four to fiveweeks later the myocardium is often called chronic ischae-mic myocardium. However, the intracellular milieu is prob-ably not equivalent to patients’ myocardium suffering fromchronic ischaemia for several years. In patients with acutemyocardial infarction, plasma concentrations of the vascu-lar growth factors VEGF and b-FGF, and the stem cellhoming factor SDF-1 increase gradually above controllevels with maximum �3 weeks after the infarction. Thiscould indicate that it takes some time to initiate the tran-scription of the genes for the cytokine production.29
Furthermore, transfection of cells with the VEGF geneafter intramyocardial injection is probably similar inchronic human or pig ischaemic myocardium. However, thetranscription of the transferred VEGF gene and thusthe induced VEGF production might be different within thehuman cells after prolonged ischaemia and in animal cellsafter short-term experimental ischaemia.
Recently, it has been speculated if the VEGF production isalready increased within chronic ischaemic human myocar-dium, thus attempts to further stimulate angiogenesis viaan additional VEGF gene stimulation would potentially bewithout effect. However, we recently studied biopsiesfrom human chronic ischaemic myocardium and found iden-tical quantities of VEGF mRNA in chronic ischaemic myo-cardium compared with non-ischaemic normal perfusedmyocardium in the same patient.30 Thus, it seems thatVEGF-A165 gene therapy can potentially increase the localproduction of the growth factor stimulating the growth ofnew blood vessels. For safety reasons, however, we chose
Figure 1 MRI perfusion scan at baseline and follow-up in one patient treated with VEGF-A165 gene transfer followed by G-CSF. The recordings were performed20 s after contrast infusion, demonstrating poor perfusion with no contrast enhancement in the lateral wall (black arrows), moderate perfusion with attenuatedenhancement (white arrows) in the inferior wall, and normal perfusion in the anterior wall (transparent arrows).
1790 R.S. Ripa et al.

a low VEGF-A165 plasmid dose. A higher dose should be con-sidered for further studies.We could not confirm the hypothesis, that the combi-
nation therapy would increase local production of VEGFand the number of circulation endothelial progenitor cellshoming into the ischaemic myocardium, suggested by experi-mental animal studies,11 in this clinical study of patientssuffering from severe, chronic CAD.SDF-1 has been found essential for stem cell mobilization/
homing after arterial injury. In a recent study, it has beendemonstrated that SDF-1 gene transfer increased the
homing of bone-marrow-derived stem cells in infarcted myo-cardium but not in normally perfused myocardium, andinduced both vasculogenesis and angiogenesis.31,32
Moreover, blockade of VEGF prevented all such SDF-1effects.32 We have found that there is no differencebetween the SDF-1 mRNA levels in normally perfused andchronic ischaemic human myocardium.30 Therefore, themissing effect of combined gene therapy and stem cellmobilization might be due to a low SDF-1 level in thechronic ischaemic tissue resulting in poor engraftment ofstem cells despite an increased number of circulating stemcells as seen during G-CSF treatment.The efficacy results of the combined treatment have a
potential limitation, as (i) it was not the primary endpointand (ii) missing data potentially introduced a selection bias.However, the patients with missing data were random (dueto a disc error) thus minimizing the risk of selection bias.Still, these results should be interpreted with caution.In conclusion, combined VEGF-A165 gene transfer and bone
marrow stem cell mobilization with G-CSF in patients withchronic myocardial ischaemia is safe but, despite a signifi-cant increase in circulating stem cells, there were no signsof clinical effects or improved myocardial perfusion of theischaemic area. Evaluation of homing of circulating stemcells in the clinical setting needs further studies. HigherVEGF-A165 gene doses and the addition of SDF-1 gene trans-fer might be considered.
Acknowledgements
The study was supported by grants from The Danish HeartFoundation (No. 0442B18-A1322141), Research Foundation atRigshospitalet, and the Danish Medical Research Council. We arevery thankful to Professor Christer Sylven, MD, Department ofCardiology and the Gene Therapy Centre, Huddinge UniversityHospital, Karolinska Institute, Stockholm, Sweden for the deliveryof the genes.
Conflict of interest: none declared.
References
1. Kastrup J. Therapeutic angiogenesis in ischaemic heart disease: gene orrecombinant vascular growth factor protein therapy? Curr Gene Ther2003;3:197–206.
2. Isner JM. Myocardial gene therapy. Nature 2002;415:234–239.3. Lewis BS, Flugelman MY, Weisz A, Keren-Tal I, Schaper W. Angiogenesis by
gene therapy: a new horizon for myocardial revascularization? CardiovascRes 1997;35:490–497.
4. Kastrup J, Jørgensen E, Ruck A, Tagil K, Glogar D, Ruzyllo W, Bøtker HE,Dudek D, Drvota V, Hesse B, Thuesen L, Blomberg P, Gyongyosi M,Sylven C. Direct intramyocardial plasmid vascular endothelial growthfactor-A165 gene therapy in patients with stable severe angina pectoris.A randomized double-blind placebo-controlled study: the Euroinject Onetrial. J Am Coll Cardiol 2005;45:982–988.
5. Hedman M, Hartikainen J, Syvanne M, Stjernvall J, Hedman A, Kivela A,Vanninen E, Mussalo H, Kauppila E, Simula S, Narvanen O, Rantala A,Peuhkurinen K, Nieminen MS, Laakso M, Yla-Herttuala S. Safety and feasi-bility of catheter-based local intracoronary vascular endothelial growthfactor gene transfer in the prevention of postangioplasty and in-stentrestenosis and in the treatment of chronic myocardial ischaemia: phaseII results of the Kuopio Angiogenesis Trial (KAT). Circulation 2003;107:2677–2683.
6. Eppler SM, Combs DL, Henry TD, Lopez JJ, Ellis SG, Yi JH, Annex BH,McCluskey ER, Zioncheck TF. A target-mediated model to describe thepharmacokinetics and hemodynamic effects of recombinant humanvascular endothelial growth factor in humans. Clin Pharmacol Ther2002;72:20–32.
Figure 2 (A) CD34þ cells, (B) Plasma stromal-derived factor-1 (SDF-1), and(C) VEGF-A165 in patients treated with VEGF-A165 gene transfer followed byG-CSF, VEGF-A165 gene transfer, or placebo gene transfer the first monthafter treatment. * indicates P , 0.05 compared with baseline, ** indicatesP, 0.01 compared with baseline, and *** indicates P , 0.005 comparedwith baseline.
VEGF gene and stem cell therapy in IHD 1791

7. Simons M, Annex BH, Laham RJ, Kleiman N, Henry T, Dauerman H,Udelson JE, Gervino EV, Pike M, Whitehouse MJ, Moon T, Chronos NA.Pharmacological treatment of coronary artery disease with recombinantfibroblast growth factor-2: double-blind, randomized, controlled clinicaltrial. Circulation 2002;105:788–793.
8. Losordo DW, Vale PR, Hendel RC, Milliken CE, Fortuin FD, Cummings N,Schatz RA, Asahara T, Isner JM, Kuntz RE. Phase 1/2 placebo-controlled,double-blind, dose-escalating trial of myocardial vascular endothelialgrowth factor 2 gene transfer by catheter delivery in patients withchronic myocardial ischemia. Circulation 2002;105:2012–2018.
9. Sylven C, Sarkar N, Ruck A, Drvota V, Hassan SY, Lind B, Nygren A,Kallner Q, Blomberg P, van der LJ, Lindblom D, Brodin LA, Islam KB.Myocardial Doppler tissue velocity improves following myocardialgene therapy with VEGF-A165 plasmid in patients with inoperableangina pectoris. Coron Artery Dis 2001;12:239–243.
10. Rosengart TK, Lee LY, Patel SR, Sanborn TA, Parikh M, Bergman GW,Hachamovitch R, Szulc M, Kligfield PD, Okin PM, Hahn RT, Devereux RB,Post MR, Hackett NR, Foster T, Grasso TM, Lesser ML, Isom OW,Crystal RG. Angiogenesis gene therapy: phase I assessment of directintramyocardial administration of an adenovirus vector expressingVEGF121 cDNA to individuals with clinically significant severe coronaryartery disease. Circulation 1999;100:468–474.
11. Kawamoto A, Gwon HC, Iwaguro H, Yamaguchi JI, Uchida S, Masuda H,Silver M, Ma H, Kearney M, Isner JM, Asahara T. Therapeutic potentialof ex vivo expanded endothelial progenitor cells for myocardial ischemia.Circulation 2001;103:634–637.
12. Orlic D, Kajstura J, Chimenti S, Limana F, Jakoniuk I, Quaini F, Nadal-Ginard B, Bodine DM, Leri A, Anversa P. Mobilized bone marrow cellsrepair the infarcted heart, improving function and survival. Proc NatlAcad Sci USA 2001;98:10344–10349.
13. Wollert KC, Meyer GP, Lotz J, Ringes-Lichtenberg S, Lippolt P,Breidenbach C, Fichtner S, Korte T, Hornig B, Messinger D, Arseniev L,Hertenstein B, Ganser A, Drexler H. Intracoronary autologous bone-marrow cell transfer after myocardial infarction: the BOOST randomisedcontrolled clinical trial. Lancet 2004;364:141–148.
14. Schachinger V, Assmus B, Britten MB, Honold J, Lehmann R, Teupe C,Abolmaali ND, Vogl TJ, Hofmann WK, Martin H, Dimmeler S, Zeiher AM.Transplantation of progenitor cells and regeneration enhancement inacute myocardial infarction: final 1 year results of the TOPCARE-AMITrial. J Am Coll Cardiol 2004;44:1690–1699.
15. Kuethe F, Richartz BM, Sayer HG, Kasper C, Werner GS, Hoffken K,Figulla HR. Lack of regeneration of myocardium by autologous intracor-onary mononuclear bone marrow cell transplantation in humans withlarge anterior myocardial infarctions. Int J Cardiol 2004;97:123–127.
16. Stamm C, Westphal B, Kleine HD, Petzsch M, Kittner C, Klinge H,Schumichen C, Nienaber CA, Freund M, Steinhoff G. Autologous bone-marrow stem-cell transplantation for myocardial regeneration. Lancet2003;361:45–46.
17. Perin EC, Dohmann HF, Borojevic R, Silva SA, Sousa AL, Mesquita CT,Rossi MI, Carvalho AC, Dutra HS, Dohmann HJ, Silva GV, Belem L,Vivacqua R, Rangel FO, Esporcatte R, Geng YJ, Vaughn WK, Assad JA,Mesquita ET, Willerson JT. Transendocardial, autologous bone marrowcell transplantation for severe, chronic ischaemic heart failure.Circulation 2003;107:2294–2302.
18. Fuchs S, Satler LF, Kornowski R, Okubagzi P, Weisz G, Baffour R,Waksman R, Weissman NJ, Cerqueira M, Leon MB, Epstein SE.Catheter-based autologous bone marrow myocardial injection inno-option patients with advanced coronary artery disease: a feasibilitystudy. J Am Coll Cardiol 2003;41:1721–1724.
19. Strauer BE, Brehm M, Zeus T, Kostering M, Hernandez A, Sorg RV,Kogler G, Wernet P. Repair of infarcted myocardium by autologous intra-coronary mononuclear bone marrow cell transplantation in humans.Circulation 2002;106:1913–1918.
20. Wang Y, Tagil K, Ripa RS, Nilsson JC, Carstensen S, Jørgensen E,Sondergaard L, Hesse B, Johnsen HE, Kastrup J. Effect of mobilizationof bone marrow stem cells by granulocyte colony stimulating factor onclinical symptoms, left ventricular perfusion and function in patientswith severe chronic ischaemic heart disease. Int J Cardiol2005;100:477–483.
21. Hill JM, Syed MA, Arai AE, Powell TM, Paul JD, Zalos G, Read EJ, Khuu HM,Leitman SF, Horne M, Csako G, Dunbar CE, Waclawiw MA, Cannon RO III.Outcomes and risks of granulocyte colony-stimulating factor inpatients with coronary artery disease. J Am Coll Cardiol 2005;46:1643–1648.
22. Ripa RS, Jørgensen E, Wang Y, Thune JJ, Nilsson JC, Søndergaard L,Johnsen HE, Køber L, Grande P, Kastrup J. Stem cell mobilizationinduced by subcutaneous granulocyte-colony stimulating factor toimprove cardiac regeneration after acute ST-elevation myocardial infarc-tion. Result of the double-blind, randomized, placebo-controlled stemcells in myocardial infarction (STEMMI) trial. Circulation 2006;113:1983–1992.
23. Kawamoto A, Murayama T, Kusano K, Ii M, Tkebuchava T, Shintani S,Iwakura A, Johnson I, von Samson P, Hanley A, Gavin M, Curry C,Silver M, Ma H, Kearney M, Losordo DW. Synergistic effect ofbone marrow mobilization and vascular endothelial growthfactor-2 gene therapy in myocardial ischemia. Circulation 2004;110:1398–1405.
24. Kjær A, Cortsen A, Rahbek B, Hasseldam H, Hesse B. Attenuation andscatter correction in myocardial SPET: improved diagnostic accuracy inpatients with suspected coronary artery disease. Eur J Nucl Med MolImaging 2002;29:1438–1442.
25. Cerqueira MD, Weissman NJ, Dilsizian V, Jacobs AK, Kaul S, Laskey WK,Pennell DJ, Rumberger JA, Ryan T, Verani MS. Standardized myocardialsegmentation and nomenclature for tomographic imaging of the heart:a statement for healthcare professionals from the Cardiac ImagingCommittee of the Council on Clinical Cardiology of the American HeartAssociation. Circulation 2002;105:539–542.
26. Jørgensen E, Madsen T, Kastrup J. Comparison of the left ventricularelectromechanical map before percutaneous coronary stent revasculari-zation and at one-month follow-up in patients with a recent ST elevationinfarction. Catheter Cardiovasc Interv 2005;64:153–159.
27. Gyongyosi M, Khorsand A, Zamini S, Sperker W, Strehblow C, Kastrup J,Jørgensen E, Hesse B, Tagil K, Bøtker HE, Ruzyllo W, Teresinska A,Dudek D, Hubalewska A, Ruck A, Nielsen SS, Graf S, Mundigler G,Novak J, Sochor H, Maurer G, Glogar D, Sylven C. NOGA-guided analysisof regional myocardial perfusion abnormalities treated with intramyocar-dial injections of plasmid encoding vascular endothelial growth factorA-165 in patients with chronic myocardial ischemia: subanalysis of theEUROINJECT-ONE multicenter double-blind randomized study.Circulation 2005;112:I157–I165.
28. Epstein FH, London JF, Peters DC, Goncalves LM, Agyeman K, Taylor J,Balaban RS, Arai AE. Multislice first-pass cardiac perfusion MRI:validation in a model of myocardial infarction. Magn Reson Med 2002;47:482–491.
29. Wang Y, Johnsen HE, Mortensen S, Bindslev L, Ripa RS, Haack-Sørensen M,Jørgensen E, Fang W, Kastrup J. Changes in circulating mesenchymalstem cells, stem cell homing factor, and vascular growth factorsin patients with acute ST-elevation myocardial infarction treatedwith primary percutaneous coronary intervention. Heart 2005;92:768–774.
30. Wang Y, Gabrielsen A, Lawler PR, Paulsson-Berne G, Steinbruchel DA,Hansson GK, Kastrup J. Myocardial gene expression of angiogenicfactors in human chronic ischaemic myocardium: influence of acuteischemia/cardioplegia and reperfusion. Microcirculation 2006;13:187–197.
31. Abbott JD, Huang Y, Liu D, Hickey R, Krause DS, Giordano FJ.Stromal cell-derived factor-1alpha plays a critical role in stem cellrecruitment to the heart after myocardial infarction but is not sufficientto induce homing in the absence of injury. Circulation 2004;110:3300–3305.
32. Hiasa K, Ishibashi M, Ohtani K, Inoue S, Zhao Q, Kitamoto S, Sata M,Ichiki T, Takeshita A, Egashira K. Gene transfer of stromal cell-derivedfactor-1alpha enhances ischaemic vasculogenesis and angiogenesisvia vascular endothelial growth factor/endothelial nitric oxidesynthase-related pathway: next-generation chemokine therapy for thera-peutic neovascularization. Circulation 2004;109:2454–2461.
1792 R.S. Ripa et al.

Circulating angiogenic cytokines and stem cells in patients with severechronic ischemic heart disease — Indicators of
myocardial ischemic burden?
Rasmus Sejersten Ripa a,⁎, Yongzhong Wang a, Jens Peter Goetze a,b, Erik Jørgensen a,Hans E. Johnsen d, Kristina Tägil e, Birger Hesse c, Jens Kastrup a
a Cardiac Catheterization Laboratory, University Hospital Rigshospitalet, Copenhagen, Denmarkb Department of Clinical Biochemistry, University Hospital Rigshospitalet, Copenhagen, Denmark
c Clinic of Nuclear Medicine, University Hospital Rigshospitalet, Copenhagen, Denmarkd Department of Haematology, Aalborg University Hospital, Aalborg, Denmark
e Department of Clinical Physiology, Malmø, Sweden
Received 24 February 2006; received in revised form 11 September 2006; accepted 20 September 2006Available online 6 December 2006
Abstract
Background: Angiogenic growth factors and stem cell therapies have demonstrated varying results in patients with chronic coronary arterydisease. A reason could be that these mechanisms are already up-regulated due to reduced blood supply to the myocardium. The objective ofthis study was to examine if plasma concentrations of circulating stem cells and angiogenic cytokines in patients with severe stable chroniccoronary artery disease were correlated to the clinical severity of the disease.Methods: Fifty-four patients with severe coronary artery disease and reversible ischemia at stress myocardial perfusion scintigraphy wereprospectively included. The severity of the disease was quantified by an exercise tolerance test, Canadian Cardiovascular Society anginaclassification, and Seattle Angina Pectoris Questionnaire. Fifteen persons without coronary artery disease served as control subjects.Results: Plasma concentration of VEGF-A, FGF-2, SDF-1, and circulating CD34+ and CD34−/CD45−cells were similar in the two groups,but early stem cell markers (CD105, CD73, CD166) and endothelial markers (CD31, CD144, VEGFR2) were significantly different betweenpatients and control subjects (pb0.005−0.001). Diabetic patients had higher concentration of SDF-1 (2528 vs. 2150 pg/ml, p=0.004). Wefound significant correlations between both VEGF-A, FGF-2, and CD34+ to disease severity, including degree of reversible ischemia, anginastability score, and exertional dyspnoea.Conclusions: Plasma concentrations of circulating stem cells and angiogenic cytokines have large inter-individual variations, which probablyexclude them from being useful as indicators of myocardial ischemic burden.© 2006 Elsevier Ireland Ltd. All rights reserved.
Keywords: Ischemic heart disease; Angiogenesis; Endothelial progenitor cell; Mesenchymal stem cell; Diabetes
1. Introduction
Acute and chronic coronary artery diseases are the leadingcauses of morbidity and mortality in cardiology. Numerouspatients cannot be treated sufficiently with current therapies,and have a poor quality of life. This has lead to an extensivesearch for new treatment modalities, including stem cell andgrowth factor therapies to induce growth of new bloodvessels in the ischemic myocardium. So far, therapies withangiogenic vascular endothelial growth factors and bone
International Journal of Cardiology 120 (2007) 181–187www.elsevier.com/locate/ijcard
Grant support: The study was supported by grants from The DanishHeart Foundation (No. 02-2-5-75-22036) and Research Foundation atRigshospitalet, Copenhagen, Denmark.⁎ Corresponding author. Cardiac Catheterization Laboratory 2014,
Rigshospitalet, Copenhagen University Hospital, Blegdamsvej 9, DK-2100 Copenhagen Ø, Denmark. Tel.: +45 35 45 85 96; fax: +45 35 45 25 13.
E-mail address: [email protected] (R.S. Ripa).
0167-5273/$ - see front matter © 2006 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.ijcard.2006.09.011

marrow suspension of cells have demonstrated bothencouraging and more questionable results in phase I–IIstudies in patients with acute myocardial infarction orchronic coronary artery disease [1–14]. These discrepanciescould be due to prior activation of angiogenic mechanisms toimprove blood supply to the ischemic heart. Therefore, it isimportant to know the basic conditions for these factors inthe subset of patients intended for treatment, in order tooptimize type and timing of the treatment with growthfactors and/or stem cells. Currently, there is a very limitedinformation about the natural occurrence of angiogenicfactors, known to be of importance in the development andgrowth of new blood vessels in patients with severe chroniccoronary artery disease [15], and no information regardingthe correlation to the clinical severity of the disease.
The aim of the present study was to determine concentra-tions of circulating stem cells and angiogenic related cyto-kines in patients with stable severe chronic coronary artery
disease, and evaluate whether concentrations were correlatedwith the clinical severity of the disease.
2. Materials and methods
2.1. Patients
We prospectively included 54 patients with stable severeocclusive coronary artery disease with evidence of andreversible ischemia as determined by adenosine stress singlephoton emission computerized tomography (SPECT).Inclusion criteria were: age 20–80 years; CanadianCardiovascular Society angina classification (CCS) ≥3despite optimal medical treatment; left ventricular ejectionfraction ≥40%; and coronary angiography with significantcoronary artery disease ineligible for revascularization.Exclusion criteria were patients with: unstable anginapectoris, acute myocardial infarction within the last3 months, diagnosed or suspected malignant disease,chronic inflammatory disease and fertile women. Fifteen
Table 1Baseline characteristics
Controls (n=15) Patients (n=54)
Mean±s.d. Mean±s.d.
Age, years 54.9±9.3 61.4±8.4Males, % 73 87Weight, kg 79.9±10.5 83.4±12.7Diabetes mellitus, % 6.7 27.8ProBNP 5.9±3.8 32.8±25.1CCS II/III/IV, % N/A 9.3/87.0/3.7LVEF by angiography, % N/A 53.4±11.1SPECT SDS N/A 8.8±5.8History of myocardial infarction, % N/A 53Exercise time, sec N/A 507.1±173.4Exercise METS N/A 5.1±1.3Nitroglycerin tablets/day N/A 2.0±2.4Angina attacks/day N/A 1.7±2.4Physical limitation ⁎ N/A 44.4±16.2Angina stability ⁎ N/A 46.1±16.9Angina frequency ⁎ N/A 35.2±26.7Treatment satisfaction ⁎ N/A 86.6±11.6Disease perception quality of life ⁎ N/A 50.5±25.1
CCS=Canadian Cardiovascular Society angina classification, SPECTSDS=single photon emission computerized tomography summed differencestress score, METS=metabolic equivalents, LVEF=left ventricular ejectionfraction.⁎ By Seattle Angina Pectoris Questionnaire.
Table 2Circulating cell and cytokine concentrations in patients with chronicmyocardial ischemia and control subjects
Patients(n=54)
Control subjects(n=15)
p-value
VEGF-A (10−12 g/ml) 35.0 (18.6–51.4) 91.7 (8.2–175.1) 0.38FGF-2 (10−12 g/ml) 9.0 (6.2–11.7) 11.3 (2.2–20.3) 0.67SDF-1 (10−10 g/ml) 22.48 (21.24–23.72) 20.14 (17.50–22.79) 0.15CD34+ (103/ml) 2.8 (2.4–3.3) 3.0 (2.1–3.9) 0.64CD45−/CD34−(104/ml) 20.8 (17.0–24.6) 21.9 (13.0–31.0) 0.79
Values are mean (95% confidence interval).
Fig. 1. Subclassification of CD45−/CD34−cells.
Fig. 2. Mean concentrations of cells and cytokines with 95% confidenceinterval in patients with or without diabetes.
182 R.S. Ripa et al. / International Journal of Cardiology 120 (2007) 181–187

healthy subjects with a similar age and gender distributionserved as a control group. Venous blood samples for stemcell and cytokine analyses were obtained after 15 min inresting supine position. All patients received oral andwritten information, and provided written consent. Thestudy was approved by the Ethical Committee of Copenha-gen (KF02-078/00).
2.2. Clinical and SPECT data
All patients underwent a maximal bicycle exercisetolerance test. Angina pectoris was described using theCCS classification, Seattle Angina Pectoris Questionnaire(SAQ), frequency of angina attacks and nitroglycerineconsumption per week. Dyspnoea was graded as moderateto severe if present during light exercise or at rest.
SPECT studies were performed as a 2-day protocol(500–700 MBq 99 mTc-sestamibi at each study) withadenosine infusion over 4–6 min (0.14 mg/kg/min byinfusion pump), combined with a sub-maximal exercisetest, except in patients with left bundle branch block [16].Gated (8 frames) imaging was performed with a two-headed Millennium GE gamma camera, with a Gadoliniuminterleaved attenuation-scatter correction. Blinded, visualanalysis according to a 17 segment model of the SPECTimages (myocardial slices in three planes) was performedas consensus readings by 2 experienced nuclear medicinespecialists, using an eNTEGRA working station (GEMedical). Summed stress scores were calculated by theECTool Box software program.
2.3. Quantification and characterization of stem cells
The concentration of circulating CD34 positive (CD34+)cells and circulating putative mesenchymal stem cells(MSC) in the blood, quantified as CD45 and CD34 negative(CD45−/CD34−) cells, was measured by multiparametricflow cytometry as previously described [17].
A panel of monoclonal and polyclonal antibodies wereused to further characterize MSCs, including anti-CD45(HI30 clone, IgG1; Becton Dickinson (BD)) and anti-CD34(8G12 clone, IgG1; BD), as well as anti-CD105 (Endoglin,NI-3A1, clone, IgG1; Ancell), anti-CD31 (PECAM-1, plate-let endothelial cell adhesion molecule, WM59 clone, IgG1;BD), anti-CD133 (haematopoietic stem cell antigen, AC133clone, IgG1; Miltenyi Biotec), anti-CD73 (PI-linked; AD2clone, IgG1; BD), anti-CD166 (ALCAM, activated leuko-cyte adhesion molecule, 3A6 clone, IgG1; BD), anti-VEGFR2 (KDR; R&D Systems), and anti-CD144 (VE-cadherin;BMS158FI polyclonale; BenderMed).
2.4. Quantification of plasma cytokines
Plasma concentrations of vascular endothelial growthfactor A (VEGF-A), fibroblast growth factor 2 (FGF-2),and stromal derived factor 1 (SDF-1) were measured induplicate by enzyme-linked immunosorbent assays(ELISA) (R&D Systems, Minneapolis, Minnesota, USA).The lower limits of detection by ELISA were 10 pg/ml for
Table 3Linear regressions between cells and cytokines for patients and controlsubjects
VEGF-A FGF-2 SDF-1 CD34+
β p β p β p β p
FGF-2 1.94 0.04SDF-1 4.23 0.07 0.54 0.07CD34+ −0.20 0.97 0.29 0.73 −47.39 0.15CD45−/CD34− −0.01 0.87 −0.01 0.47 −0.02 0.97 0.00 0.32
β=regression coefficient.
Table 4Correlations between cells, cytokines and clinical characteristics for patients (n=54)
VEGF FGF-2 SDF-1 CD34+ CD45−/CD34−
r p r p r p r p r p
Left ventricular ejection fraction 0.03 0.79 −0.04 0.79 −0.02 0.88 0.01 0.92 −0.29 0.04SPECT summed difference score 0.22 0.24 0.40 0.03 0.03 0.87 0.43 0.02 0.05 0.80METS −0.09 0.51 −0.03 0.81 −0.13 0.34 −0.06 0.67 −0.18 0.19Nitroglycerin/day −0.13 0.37 −0.26 0.07 0.11 0.46 0.18 0.22 0.04 0.79Angina attacks/day 0.07 0.64 −0.08 0.58 0.17 0.25 0.07 0.65 −0.05 0.73Physical limitation ⁎ −0.13 0.36 0.02 0.91 −0.05 0.72 −0.09 0.51 −0.13 0.36Angina stability ⁎ −0.13 0.37 0.20 0.15 −0.13 0.37 0.31 0.03 0.27 0.06Treatment satisfaction ⁎ 0.03 0.84 −0.17 0.22 0.02 0.90 −0.22 0.11 0.04 0.78Disease perception quality of life ⁎ 0.02 0.91 0.04 0.79 −0.25 0.07 −0.10 0.47 −0.06 0.65
Statistical significant results are marked in bold.⁎ By Seattle Angina Pectoris Questionnaire.
Table 5Circulating cell and cytokine concentrations in patients with mild or severeexertional dyspnoea (n=54)
No or milddyspnoea (n=36)
Moderate to severedyspnoea (n=18)
p-value
VEGF-A (10−12 g/ml) 32.8 (11.8–53.8) 39.3 (11.2–67.5) 0.71FGF-2 (10−12 g/ml) 7.0 (5.3–8.6) 12.8 (5.2–20.5) 0.04SDF-1 (10−10 g/ml) 22.33 (20.88–23.79) 22.76 (20.20–25.32) 0.75CD34+(103/ml) 2.8 (2.2–3.4) 2.9 (2.0–3.9) 0.74CD45−/CD34−
(104/ml)19.7 (14.8–24.5) 23.1 (17.1–29.1) 0.41
Values are mean (95% confidence interval).
183R.S. Ripa et al. / International Journal of Cardiology 120 (2007) 181–187

VEGF-A and FGF-2, and 18 pg/ml for SDF-1. PlasmaproBNP concentrations were measured using an in-houseradioimmunoassay [18].
2.5. Statistical analysis
Categorical variables were compared using the Chi-square test. Means were compared using the student t-test(or Mann–Whitney U-test when the distribution wasskewed) or the ANOVA test for linearity. Associationbetween continuous variables was tested using the Pearsonr analysis or linear regression. Independent predictors ofplasma concentrations were identified using stepwise back-ward linear regression. All data were analyzed using SPSSstatistical analysis program (SPSS version 13.0, SPSSINC., Chicago, Il.). Statistical significance was determinedby pb0.05.
3. Results
The demographic and clinical characteristics of theincluded patients are outlined in Table 1. All patients wereon stable unchanged anti-angina therapy 2 months prior toinclusion in the study, and had previously undergonecoronary artery by-pass surgery or percutaneous coronaryintervention. All patients had severe angina pectoris withlimited exercise capacity, and reversible myocardialischemia identified by a stress SPECT. The patients had asignificantly higher plasma proBNP concentration com-pared to the control group, despite a near normal leftventricular ejection fraction.
The plasma concentration of VEGF-A showed a non-significant trend towards lower values in the patients comparedto the control subjects, but with very large inter-individualvariations (Table 2). Comparable concentrations of theangiogenic factor FGF-2, the CD34+ and CD45−/CD34−stem cell populations, and the stem cell homing factor SDF-1were seen in the two groups (Table 2). However, the CD45−/CD34− cell (MSC) population is heterogeneous and sub-
characterizing by co-expression of early stem cell markers(CD105, CD73, CD166) and endothelial markers (CD31,CD144, VEGFR2) revealed highly significant differencesbetween patients and control subjects (Fig. 1). Patients withchronic ischemic heart disease had significantly higher levels ofMSCs with both early stem cell markers (CD105 and CD166),and endothelial progenitor cell markers (CD144 and VEGFR2);whereas cells with the haematopoietic marker CD133 weresignificantly lower in patients compared to control subjects,suggesting an important functional difference.
In a subgroup analysis of patients with diabetes, we foundsignificantly higher plasma concentrations of SDF-1 com-pared to non-diabetic patients (Fig. 2).
The relationships between the angiogenic factors for allsubjects are shown in Table 3. The positive correlation be-tween VEGF-A and FGF-2 appears to be explained by amarked association within the patient group.
The bivariate correlation between clinical severity of thedisease and the angiogenic factors are shown in Tables 4 and 5.Plasma FGF-2, circulating CD34+, and CD45−/CD34− werefound to correlate with the clinical severity of the ischemicheart disease. The independent, clinical predictors forcirculating angiogenic factors analyzed by multivariate linearregression are outlined in Table 6.
4. Discussion
To evaluate if angiogenic factors within the myocardiumare activated in patients with stable chronic myocardialischemia and whether such activation is reflected by alteredconcentrations in the circulation, we examined a patientpopulation with severe clinical chronic myocardial ischemiaand stress induced myocardial perfusion defects documen-ted by SPECT. We found that, in general, circulating stemcells and plasma concentrations of angiogenic relatedcytokines were not significantly different from the controlgroup. Nevertheless, some association between differentmeasures of the severity of the disease was demonstrated,but a large inter-individual variation will probably limit theclinical applicability of these measures.
Since we expected a substantial difference between theplasma concentration of stem cells and angiogenic factorsafter a short-term acute ischemic period compared tosustained or repeated periods of ischemia in our population,this study did not include patients with acute myocardialinfarction. We have recently found that angiogenic factors(VEGF-A, FGF-2 and SDF-1) in the month following anacute myocardial infarction increase substantially above theconcentrations found in the present study. Conversely, CD34positive and mesenchymal stem cells were in the same rangeas in the present study [19]. These variations in concentra-tions of angiogenic factors and stem cells are important sincepatients with acute myocardial infarction are included inseveral angiogenic trials, however, whether these differencesare of clinical importance, remains to be elucidated. Onecould speculate that therapy with exogenous angiogenic
Table 6Linear regression analysis in cardiac patients (n=54)
Dependent variable Independent predictors β p-value
VEGF-A Dyspnoea −66.2 0.003Angina stability according to SAQ −1.0 0.04
FGF-2 Dyspnoea 5.9 0.04SDF-1 Diabetes mellitus 388.4 0.004CD34+ SPECT summed difference score 0.14 0.01CD45−/CD34− Left ventricular ejection fraction −3.6 0.04
Independent predictors included in the analysis: gender, age, weight, historyof myocardial infarction, diabetes mellitus, left ventricular ejection fraction,dyspnoea, CCS class, METS, mean number of short acting nitroglycerine,mean number of angina attacks, physical limitation according to SeattleAngina Pectoris Questionnaire (SAQ), angina stability according to SAQ,treatment satisfaction according to SAQ, disease perception quality of lifeaccording to SAQ, SPECT summed difference score.
184 R.S. Ripa et al. / International Journal of Cardiology 120 (2007) 181–187

factors may have more therapeutic effects in patients withchronic ischemic heart disease since they have the lowestinert concentrations.
4.1. VEGF-A
VEGF-A is a major mediator of neovascularization inphysiological and pathophysiological conditions, with akey role in regulation of hypoxia-induced tissue angiogen-esis. In patients with acute myocardial ischemia andinfarction, elevated contents of VEGF-A mRNA in myo-cardial tissues have been reported, suggesting VEGF-A tobe an important local response to oxygen deprivation [20].We found a trend towards lower concentrations in patientsas compared to control subjects, but with very large inter-individual variations in both groups. In addition, we foundan inverse relation to CCS class and to anginal stability(Table 6). These observations are surprising, since weexpected that the patient population with documentedfrequent myocardial ischemia during stress, would have aninduction of VEGF production as previously found in 20patients with stable angina pectoris [15]. However, thefinding may be in accordance with our recent finding ofunaffected VEGF mRNA contents in chronic ischemicmyocardial tissue compared to normally perfused myocar-dium, in patients undergoing coronary artery by-passsurgery [21].
The association with CCS class should be evaluatedwith extreme caution due to the small numbers of patientsin classes II and IV. However, one might speculate thatpatients with innate low level of VEGF-A will form fewercoronary collaterals and thus will be more prone tosymptomatic myocardial ischemia. This hypothesis issupported by the work of Schultz et al. [22], showingthat monocytes from patients with ischemic heart diseaseand few collaterals have reduced hypoxic induction ofVEGF-A. In addition, a recent work by Lambiase et al.[23] showed a non-significant trend towards the sameresults.
4.2. FGF-2
FGF-2 is a potent stimulant of angiogenesis like VEGF-A [24], and we established an anticipated associationbetween those two factors. Moreover, we detected anincrease in plasma FGF-2 in association with increasingdegree of reported dyspnoea in both univariate andmultivariate analysis (Tables 5 and 6). To our knowledge,this has not been reported previously.
It should be noted that patients with heart failure werenot intentionally included in our trial and all had ejectionfraction above 40%. Hence, it appears likely that thedifferences in dyspnoea reflect an angina equivalent ratherthan the degree of heart failure. This hypothesis is furtherstrengthened by the correlation between FGF-2 and stressinduced ischemia shown by SPECT (Table 4).
4.3. SDF-1
SDF-1 is a chemokine ligand involved in numerousbiological processes including vasculogenesis, cardiogen-esis, and haematopoiesis. SDF-1 mediates its functionthrough the CXCR4 transmembrane receptor [25]. SDF-1has been suggested to augment recruitment of endothelialprogenitor cells into ischemic tissue and thus enhanceischemic neovascularization [26].
We found similar concentrations of plasma SDF-1 inpatients and healthy controls. This is in contrast to a recentstudy by Damås et al. [27] who reported a significantly higherconcentrations in control subjects compared to patients withstable angina. In a previous in vitro study, SDF-1 inducedsecretion of VEGF from lymphohaematopoietic cells. This isin concordance with our finding of a trend towards an as-sociation between the plasma concentration of SDF-1 andVEGF-A ( p=0.07).
Interestingly, we found a highly significant, positivecorrelation between circulating SDF-1 and presence ofdiabetes by both univariate and multivariate analyses. To ourknowledge, this has never been described before. However,the result is supported by a very recent reporting that theconcentration of circulating SDF-1 is correlated to theseverity of diabetic retinopathy in patients [28].
SDF-1 is produced in almost all organs, but mostabundantly in the pancreas [29]. The association betweenhigh concentrations of plasma SDF-1 and diabetes couldthus be due to a high endocrine drive on the diabetic pancreasleading to an excess production of SDF-1. Recent experi-ments in mice suggest that intravitreal SDF-1 is a keymediator of diabetic proliferative retinopathy [30] and it canbe speculated if the increased concentrations of SDF-1 in theblood is instrumental to pathological formation of new bloodvessels in other vascular beds in diabetes. Since this was asubgroup analysis and not the primary objective of our trial,it would be interesting to determine if our finding can bereproduced in diabetic patients without concomitant ische-mic heart disease.
4.4. CD34 positive cells
Endothelial progenitor cells have been isolated fromcirculating CD34+ mononuclear cells and are thought toparticipate in vasculogenesis. The number of circulatingCD34+ cells have been found both to increase and to beunchanged in the period after an acute myocardial infarctiontreated with primary percutaneous coronary interventionand stenting [19,31]. Valgimigli et al. [32] recently showedthat CD34+ cells and EPC mobilization occurs in heartfailure and displays a biphasic response with elevation anddepression in the early and advanced phases, respectively. Itthus seems plausible that CD34+ cells are also related to theseverity of ischemic heart disease. We detected a weekassociation to self-reported angina stability and to theamount of reversible ischemia determined by SPECT. These
185R.S. Ripa et al. / International Journal of Cardiology 120 (2007) 181–187

results could indicate that patients with a large myocardialarea with reversible ischemia have an augmented mobiliza-tion of CD34+ cells into the circulation. However, the cellconcentrations are close to the detection limit of the methodused, and thus the results should be evaluated with caution.
Recently, Eizawa et al. [33] found that patients with stableangina and diabetes had decreased CD34+ cells compared tocontrol subjects. These results were not confirmed in ourstudy. This may be due to differences in patient selection; ourtrial appears to have included a population with more severemyocardial ischemia.
4.5. CD45−/CD34− mesenchymal stem cells
The MSC can differentiate into endothelia, bone, cartilageand even myoblasts if appropriately stimulated. MSC arecharacterized by the non-expression of haematopoieticmarkers CD34 and CD45. Several trials using MSC therapyfor ischemic heart disease are currently being planned, and itis therefore important to determine the baseline concentrationof circulating MSCs, but this has never previously beeninvestigated.
We found the same concentrations of CD45−/CD34− cellsin the patients and control subjects. However, when weexamined the CD45−/CD34− cells with early stem cell andendothelial markers (Fig. 2), several important subpopula-tions differed: cells with mesenchymal stem cell markers(CD105, CD166) and cells with endothelial markers (CD144,CD31, VEGF-receptor) were increased, whereas anothermesenchymal stem cell marker (CD73) was unaffected. Incontrast, the fraction of cells with the haematopoietic marker(CD133) was decreased. These results could indicate thatboth early and endothelial differentiated mesenchymal stemcells are mobilized and are potentially involved in vasculo-genesis in ischemic heart disease. Furthermore, we observeda significant negative association between CD45−/CD34−cells and left ventricular ejection fraction. This could indicatethat mobilization of CD45−/CD34− cells is more affected byleft ventricular dysfunction than ischemia, and it would beinteresting to examine this relationship in patients withejection fraction below 40%.
5. Conclusion
The plasma concentrations of VEGF-A, FGF-2, circulatingCD34+ and mesenchymal stem cells were not different fromcontrols. However, they seemed related to the severity of thedisease in patients with severe stable chronic coronary arterydisease, but with a very large inter-individual variation.Mesenchymal stem cells with early stem cell and endothelialcell markers were more pronounced in cardiac patients. Theplasma concentration of SDF-1 was increased in diabeticpatients, whichmight influence the progression of the vasculardisease. Due to the large inter-individual variations of theseangiogenic factors, they do not appear to be suitable for use asclinical indicators of myocardial ischemic burden.
Acknowledgments
We appreciate the skilful and enthusiastic laboratoryassistance of Steen Mortensen. We are grateful to Dr. C.Burton for help with the preparation of the manuscript.
References
[1] Grines CL, Watkins MW, Helmer G, et al. Angiogenic Gene Therapy(AGENT) trial in patients with stable angina pectoris. Circulation2002;105:1291–7.
[2] Henry TD, Annex BH, McKendall GR, et al. The VIVA trial: vascularendothelial growth factor in ischemia for vascular angiogenesis.Circulation 2003;107:1359–65.
[3] Kastrup J, Jørgensen E, Drvota V, et al. Intramyocardial injection ofgenes with a novel percutaneous technique: initial safety data of theEuroinject One Study. Heart Drug 2001;1:299–304.
[4] Kastrup J, Jørgensen E, Drvota V. Vascular growth factor and gene therapyto induce new vessels in the ischemic myocardium. Therapeuticangiogenesis. Scand Cardiovasc J 2001;35:291–6.
[5] Kastrup J. Therapeutic angiogenesis in ischemic heart disease: gene orrecombinant vascular growth factor protein therapy? Curr Gene Ther2003;3:197–206.
[6] Kastrup J, Jørgensen E, Ruck A, et al. Direct intramyocardial plasmidvascular endothelial growth factor-A165 gene therapy in patients withstable severe angina pectoris A randomized double-blind placebo-controlled study: the Euroinject One trial. J Am Coll Cardiol 2005;45:982–8.
[7] Losordo DW, Vale PR, Hendel RC, et al. Phase 1/2 placebo-controlled,double-blind, dose-escalating trial of myocardial vascular endothelialgrowth factor 2 gene transfer by catheter delivery in patients withchronic myocardial ischemia. Circulation 2002;105:2012–8.
[8] Ripa RS, Wang Y, Jørgensen E, Johnsen HE, Grande P, Kastrup J.Safety of bone-marrow stem cell mobilisation induced by granulocyte-colony stimulating factor: clinical 30 days blinded results from thestem cells in myocardial infarction (STEMMI) trial. Heart Drug2005;5:177–82.
[9] Ripa RS, Jørgensen E, Wang Y, et al. Stem cell mobilization inducedby subcutaneous granulocyte-colony stimulating factor to improvecardiac regeneration after acute ST-elevation myocardial infarction:result of the double-blind, randomized, placebo-controlled stem cells inmyocardial infarction (STEMMI) trial. Circulation 2006;113:1983–92.
[10] Schachinger V, Assmus B, Britten MB, et al. Transplantation ofprogenitor cells and regeneration enhancement in acute myocardialinfarction: final one-year results of the TOPCARE-AMI Trial. J AmColl Cardiol 2004;44:1690–9.
[11] Simons M, Annex BH, Laham RJ, et al. Pharmacological treatment ofcoronary artery diseasewith recombinant fibroblast growth factor-2: double-blind, randomized, controlled clinical trial. Circulation 2002;105:788–93.
[12] Vale PR, Losordo DW, Milliken CE, et al. Randomized, single-blind,placebo-controlled pilot study of catheter-based myocardial genetransfer for therapeutic angiogenesis using left ventricular electrome-chanical mapping in patients with chronic myocardial ischemia.Circulation 2001;103:2138–43.
[13] Wang Y, Tägil K, Ripa RS, et al. Effect of mobilization of bone marrowstem cells by granulocyte colony stimulating factor on clinical symp-toms, left ventricular perfusion and function in patients with severechronic ischemic heart disease. Int J Cardiol 2005;100:477–83.
[14] Wollert KC, Meyer GP, Lotz J, et al. Intracoronary autologous bone-marrow cell transfer after myocardial infarction: the BOOST ran-domised controlled clinical trial. Lancet 2004;364:141–8.
[15] Soeki T, Tamura Y, Shinohara H, Tanaka H, Bando K, Fukuda N. Roleof circulating vascular endothelial growth factor and hepatocytegrowth factor in patients with coronary artery disease. Heart Vessels2000;15:105–11.
186 R.S. Ripa et al. / International Journal of Cardiology 120 (2007) 181–187

[16] Hesse B, Tagil K, Cuocolo A, et al. EANM/ESC procedural guidelinesfor myocardial perfusion imaging in nuclear cardiology. Eur J NuclMed Mol Imaging 2005;32:855–97.
[17] Mancuso P, Burlini A, Pruneri G, Goldhirsch A, Martinelli G, BertoliniF. Resting and activated endothelial cells are increased in the peripheralblood of cancer patients. Blood 2001;97:3658–61.
[18] Goetze JP, Kastrup J, Pedersen F, Rehfeld JF. Quantification of pro-B-typenatriuretic peptide and its products in human plasma by use of an analysisindependent of precursor processing. Clin Chem 2002;48:1035–42.
[19] Wang Y, Johnsen HE, Mortensen S, et al. Changes in circulatingmesenchymal stem cells, stem cell homing factor, and vascular growthfactors in patients with acute ST elevation myocardial infarction treatedwith primary percutaneous coronary intervention. Heart 2006;92:768–74.
[20] Lee SH, Wolf PL, Escudero R, Deutsch R, Jamieson SW, ThistlethwaitePA. Early expression of angiogenesis factors in acute myocardialischemia and infarction. N Engl J Med 2000;342:626–33.
[21] Wang Y, Gabrielsen A, Lawler PR, et al. Myocardial gene expressionof angiogenic factors in human chronic ischemic myocardium:influence of acute ischemia/cardioplegia and reperfusion. Microcircu-lation 2006;13:187–97.
[22] Schultz A, Lavie L, Hochberg I, et al. Interindividual heterogeneity in thehypoxic regulation of VEGF: significance for the development of thecoronary artery collateral circulation. Circulation 1999;100:547–52.
[23] Lambiase PD, Edwards RJ, Anthopoulos P, et al. Circulating humoralfactors and endothelial progenitor cells in patients with differingcoronary collateral support. Circulation 2004;109:2986–92.
[24] Yongzhong W, Johnsen HE, Jørgensen E, Kastrup J. The clinicalimpact of vascular growth factors and endothelial progenitor cells inthe acute coronary syndrome. Scand Cardiovasc J 2003;37:18–22.
[25] Juarez J, Bendall L, Bradstock K. Chemokines and their receptors astherapeutic targets: the role of the SDF-1/CXCR4 axis. Curr PharmDes 2004;10:1245–59.
[26] Yamaguchi J, Kusano KF, Masuo O, et al. Stromal cell-derived factor-1effects on ex vivo expanded endothelial progenitor cell recruitment forischemic neovascularization. Circulation 2003;107:1322–8.
[27] Damas JK, Waehre T, Yndestad A, et al. Stromal cell-derived factor-1alpha in unstable angina: potential antiinflammatory and matrix-stabilizing effects. Circulation 2002;106:36–42.
[28] Meleth AD, Agron E, Chan CC, et al. Serum inflammatory markers indiabetic retinopathy. Invest Ophthalmol Vis Sci 2005;46:4295–301.
[29] Shirozu M, Nakano T, Inazawa J, et al. Structure and chromosomallocalization of the human stromal cell-derived factor 1 (SDF1) gene.Genomics 1995;28:495–500.
[30] Butler JM,Guthrie SM,KocM, et al. SDF-1 is bothnecessary and sufficientto promote proliferative retinopathy. J Clin Invest 2005;115:86–93.
[31] MassaM, Rosti V, FerrarioM, et al. Increased circulating hematopoieticand endothelial progenitor cells in the early phase of acute myocardialinfarction. Blood 2005;105:199–206.
[32] Valgimigli M, Rigolin GM, Fucili A, et al. CD34+ and endothelialprogenitor cells in patients with various degrees of congestive heartfailure. Circulation 2004;110:1209–12.
[33] Eizawa T, Ikeda U, Murakami Y, et al. Decrease in circulatingendothelial progenitor cells in patients with stable coronary arterydisease. Heart 2004;90:685–6.
187R.S. Ripa et al. / International Journal of Cardiology 120 (2007) 181–187

Scandinavian Journal of Clinical & Laboratory Investigation Vol. 69, No. 6, October 2009, 722–728
ISSN 0036-5513 print/ISSN 1502-7686 online © 2009 Informa UK Ltd. (Informa Healthcare, Taylor & Francis AS)DOI: 10.1080/00365510903078803
Correspondence: Rasmus S. Ripa, MD, Department of Clinical Physiology, Frederiksberg Hospital, Norde Fasanvej 57, DK-2000 Frederiksberg, Denmark. Tel: 45 3816 4771. Fax: 45 3816 4779. E-mail: [email protected]
(Received 3 March 2009; accepted 25 May 2009)
ORIGINAL ARTICLE
The influence of genotype on vascular endothelial growth factor and regulation of myocardial collateral blood flow in patients with acute and chronic coronary heart disease
RASMUS SEJERSTEN RIPA1, ERIK JØRGENSEN1, FEDERICA BALDAZZI1,RUTH FRIKKE-SCHMIDT2, YONGZHONG WANG1, ANNE TYBJÆRG-HANSEN2 & JENS KASTRUP1
1Department of Cardiology, The Heart Centre, Rigshospitalet, Copenhagen University Hospital, and University of Copenhagen, Faculty of Health Sciences, Denmark, and 2Department of Clinical Biochemistry, Rigshospitalet, Copenhagen University Hospital, and University of Copenhagen, Faculty of Health Sciences, Denmark
AbstractObjective: To test the hypothesis that mutations in the vascular endothelial growth factor (VEGF) gene are associated with plasma concentration of VEGF and subsequently the ability to influence coronary collateral arteries in patients with coronary heart disease (CHD). Methods: Blood samples from patients with chronic ischemic heart disease (n 53) and acute coronary syndrome (n 61) were analysed. Coronary collaterals were scored from diagnostic biplane coronary angiograms. Results: The plasma concentration of VEGF was increased in patients with acute compared to chronic CHD (p 0.01). The genotype frequencies differed significantly from Hardy-Weinberg equilibrium in three of 15 examined loci. Four new mutations in addition to the already described were identified. The VEGF haplotype did not seem to predict plasma VEGFconcentration (p 0.5). There was an association between the genotype in locus VEGF-1154 and coronary collateral size (p 0.03) and a significant association between the VEGF plasma concentration and the collateral size (p 0.03). Conclusion: VEGF plasma concentration seems related to coronary collateral function in patients with CHD. The results did not support the hypothesis that polymorphisms in the untranslated region of the VEGF gene were associated with the concentration of circulating VEGF. Increased understanding of VEGF in the regulation of myocardial collateral flow may lead to new therapies in CHD.
Key Words: Coronary collaterals, geno-phenotype, ischemic heart disease, VEGF
Introduction
The opening and growth of preexistent collateral coronary arterioles are innate mechanisms in res-ponse to acute and chronic coronary heart disease (CHD) [1,2]. Within minutes to hours after symptom onset, in patients with ST-elevation infarction, col-laterals have been shown in angiograms. On the other hand, it is known that collateral arteries may take up to 3 months to become fully developed [3,4]. The development of collaterals is a complex process involving growth modulators (promoters and inhibi-tors), growth factor receptors, different cell types, and proteolytic enzymes [1]. Recently, it was shown that monocyte transcription profile influence coronary collateral vessel growth [5]. Vascular endothelial growth factor (VEGF) as collateral growth promoter
has received much attention [6–9] and evidence sug-gests that the genotype of the VEGF promoter and 5 untranslated region can influence the induction of VEGF [10–14].
The angiogenic cytokines VEGF and fibroblast growth factor (FGF) have been tested in clinical studies of patients with mainly chronic occlusive coronary artery disease [15–20]. However, in the first larger double-blind randomized placebo-controlled VEGF gene therapy study we could not demonstrate significant improvement in collateral flow and myocardial perfusion, when compared to placebo [15].
The aim of the present study was to test the hypothesis that germline DNA variations in the VEGF promoter and 5 untranslated region was associated with the plasma concentration of VEGF,

VEGF and collaterals in heart disease 723
Minneapolis, Minn). The lower limits of detection were 9 pg/mL for VEGF-A. To account for day-to-day variation in the concentration of VEGF-A, a mean concentration of two samples was used for analysis. The first VEGF sample was drawn 24–48 hours after the angiogram and the next sample 30 days later.
Grading of coronary collaterals
Angiograms were assessed by two experienced inva-sive cardiologists blinded to all patient data. The final collateral grading was a consensus agreement bet-ween the two readers. Coronary collateral filling was graded according to the method described by Rentrop et al. [23]: 0 no filling of any collateral vessels, 1 filling of side branches of the artery by collateral vessels without visualization of the epicardial segment, 2 partial filling of the epicardial artery by collateral vessel, 3 complete filling of the epicardial artery by collateral vessels.
In addition, the visible diameter of the collateral con-nection was graded as described by Werner et al. [24] CC0 no continuous visible connection between donor and recipient branch, CC1 continuousthreadlike connection, or CC2 continuous small sidebranch–like connection. Patients with thrombol-ysis in myocardial infarction (TIMI) flow 3 in the culprit artery were excluded from scoring of collater-als. If multiple coronary collaterals were present, then the most prominent was used for grading.
Statistical analysis
Analyses were performed using SPSS (version 12.0, SPSS Inc, Chicago, Ill). The level of statistical sig-nificance was set at p 0.05. Continuous variables in the disease groups were compared using the Mann-Whitney U test and correlation coefficients were tested using Spearman’s Rank Correlation. Univari-ate geno-phenotype associations were analysed using Mann-Whitney U test. Association between the VEGF haplotypes and VEGF plasma concentrations were tested using the non-parametric Kruskal-Wallis test. Stepwise ANCOVA with genotype as indepen-dent factors and VEGF plasma concentration as out-come, type of ischemic disease and age was included as covariate was employed to identify a model associ-ated with plasma VEGF concentration. Association between genotype and coronary collaterals were tested using Fisher’s exact test, whereas VEGFplasma concentration and coronary collaterals were tested using multinominal logistic regression with collateral score as outcome.
Results
Patients included in the two disease groups (acute and chronic CHD) had typical cardiac risk factors as
and that these DNA variations as well as the VEGFplasma concentration influences the ability to open coronary collateral arteries in patients with acute and chronic obstructive CHD.
Material and methods
We included patients with acute CHD (n 61) or sta-ble chronic CHD (n 53). Patients with acute CHD had either ST elevation myocardial infarction [21] or non-ST elevation myocardial infarction [22]. Patients with chronic CHD had: (i) Canadian Cardiac Soci-ety (CCS) class 3 angina and significant reversible myocardial ischemia on an adenosine stress single photon emission computed tomography (SPECT), (ii) at least one remaining larger coronary vessel from which new collaterals/vessels could be supplied, (iii) preserved left ventricular ejection fraction ( 40), and (iv) been without unstable angina or acute infarction within the last three months.
Demographic and clinical data were recorded and blood samples for plasma VEGF analysis were obtained. All patients underwent diagnostic coronary angiography (ST-elevation myocardial infarction patients immediately before the primary PCI). All patients received oral and written information about the study and signed an informed consent before inclusion in the study. The study followed the recom-mendations of the Helsinki II Declaration and was approved by the Ethics Committee of Copenhagen.
VEGF SNP genotyping
DNA was extracted from peripheral blood. A total of 15 previously published SNPs in the VEGF pro-moter or 5 untranslated region were genotyped in all patients using an ABI PRISM 7900HT Sequence Detection System (Applied Biosystems, Foster City, CA) using the Assay-by-Design Service from Applied Biosystems (VEGF-7, -634, 1001, -1455, -1498, -1952, -2155, -2488) or direct sequencing using an ABI 310 Sequencer (a single fragment covering VEGF-1075, -1154, -1179, -1190, -1198, -1203, -1210). Seque-nces of all polymerase chain reaction primers and reporter probes are available from the authors. The human DNA reference sequence AL136131.15, GI:10045276 was used.
Collection and analysis of peripheral blood
Blood samples were collected from the antecubital vein in vacutainer tubes containing EDTA as an anti-coagulant. Samples were kept on ice until procession 15 to 30 minutes after collection. Plasma was obtained by 10-minute centrifugation at 3000g. The plasma clos-est to the cells was not used. Plasma for VEGF analysis were immediately frozen and stored at 80°C.
Plasma concentrations of VEGF-A were mea-sured by a colorimetric ELISA kit (R&D Systems,

724 R. S. Ripa et al.
We found no mutations in two examined loci (VEGF-1001, -1210), and very rarely mutations in four other loci (VEGF-1198, -1203, -1952, -2155). Mutations in VEGF-1498 very often segregated with mutations in VEGF-2488. In addition to the already described mutations and polymorphisms we identified four new mutations within the fragment analyzed by direct sequencing. Four patients were heterozygote for an identical 2bp deletion (VEGF-1283 to -1284delAG). Three single base mutations (VEGF-1111G A,-1142C T, -1277G A) were identified in 3 other patients. The identified mutations resulted in 27 dif-ferent haplotypes in the included patients, 13 of these haplotypes were identified in only one individual per haplotype and three haplotypes were identified in only two individuals per haplotype.
Geno- pheno-type association
The association between VEGF plasma concentra-tion and genotype is shown in Table III. Only one marker (VEGF-1154) showed a significant differ-ence in VEGF concentration by univariate analysis. We found no indication of an effect of the VEGFhaplotype on the VEGF plasma concentration (p 0.5using the Kruskal-Wallis test and only including 11 haplotypes identified in three or more individuals). Stepwise analysis of the loci identified a model combin-ing VEGF-7, -1075, -1154, and -1498 with plasma VEGF concentration as outcome with a r2 of 0.30. The relation was not affected when including type of ischemic disease and/or age into the model.
Coronary angiography
An analysable coronary angiogram was available in 97 (85%) of the patients. As expected, coronary col-laterals were mainly distinct in patients with chronic CHD (Table I). The correlation between the collat-eral filling (Rentrop grade) and collateral size (Werner classification) was highly significant in both patients with chronic CHD (r 0.4, p 0.003) and acute CHD (r 0.7, p 0.001).
shown in Table I. The plasma concentration of VEGFwas significantly increased in patients with acute CHD (median concentration and 95% confidence interval of the median: 56 (33–92)) compared to patients with chronic CHD (18 (13–32)), p 0.01using the Mann-Whitney U test, but the inter-patient variations within the groups were large (Figure 1).
Genotyping
The genotype frequencies are shown in Table II. Genotype frequencies differed significantly from those predicted by the Hardy-Weinberg equilibrium in three loci (VEGF-1154, -1498, -2488, p 0.02; 0.04; 0.04), and one locus tended to differ from the predicted (VEGF-1190, p 0.07) in the patients with CHD. All the identified disequilibrium’s were caused by a lower frequency of heterozygote’s than expected.
Table I. Cardiac risk factors and angiographic characteristics.
Chronic CHD (n 53) Acute CHD (n 61) p
Age (years) 62 9 56 11 0.01Gender (m/f) (46/7) (48/13) 0.3Body mass index kg/m2 28 4 28 5 0.3Current or previous smoker, n (%) 40 (75) 41 (67) 0.4Diabetes mellitus, n (%) 13 (25) 6 (9) 0.2Known hypertension, n (%) 26 (49) 20 (33) 0.1Family history of CHD, n (%) 24 (51) 18 (33) 0.07Previous PCI, n (%) 32 (62) 3 (4) 0.01Rentrop score (23) [0 /1/2/3], % 0/2/17/81 32/18/22/28 0.01Werner score (24) [0/1/2], % 6/40/53 48/38/14 0.01
CHD, Coronary heart disease; PCI, Percutaneous coronary intervention.
Figure 1. Plasma concentration of VEGF-A in two groups of patients with ischemic heart disease. Horizontal lines indicate median value. Ordinate in logarithmic scale.

VEGF and collaterals in heart disease 725
There was an association between the genotype in locus VEGF-7 and coronary collaterals graded by the Werner score (p 0.03), but no association with the Rentrop grading (p 0.3). All remaining genotypes tested did not predict the coronary collaterals.
There was a significant association between the VEGF plasma concentration and the collateral size as classified by the Werner classification (p 0.03)when controlling for type of disease (acute or chronic CHD) (Figure 2). From Figure 2 it is apparent that patients with chronic CHD are primarily in CC1 or CC2 with an inverse relation to plasma VEGFplasma concentration, whereas collateral size in patients with acute CHD is directly related to the VEGF plasma concentration Excluding the three cases with chronic CHD and CC0 and the seven cases with acute CHD and CC2 from analysis do not change the results significantly. The interaction between type of disease and VEGF concentration in
predicting Werner classification is not statistically sig-nificant (p 0.6).
Discussion
Patients with CHD have large variations in plasma VEGF concentrations. The VEGF phenotype was found to be related to the size of the coronary collaterals.
It is well known that the size and number of cor-onary collaterals is a major determinant of symptoms in patients with CHD. It would thus be of clinical significance to identify patients with inert potential for development of coronary collaterals. Previously, VEGF polymorphisms have been reported to affect several diseases such as proliferative diabetic retin-opathy [25] and end-stage renal disease [26]. The genotype of the VEGF promoter and 5 untranslated region has been shown to influence the induction of
Table II. Genotype frequencies in patients with coronary heart disease.
LocusWildtypebasepair
Mutation basepair
Homo-zygotewildtype Hetero-zygote
Homo-zygotemutation
Test for HWE p
-7 cc tt 80 (71) 30 (27) 3 (3) 0.93-634 cc gg 47 (41) 54 (47) 13 (11) 0.67-1001 gg 113 (100) 0 (0) 0 (0)-1075 cc aa 107 (96) 4 (4) 0 (0) 0.85-1154 gg aa 55 (50) 38 (34) 18 (16) 0.02-1179 aa cc 102 (92) 9 (8) 0 (0) 0.66-1190 gg aa 35 (32) 46 (41) 30 (27) 0.07-1198 cc aa 112 (99) 1 (1) 0 (0) 0.96-1203 cc tt 112 (99) 1 (1) 0 (0) 0.96-1210 cc 113 (100) 0 (0) 0 (0)-1455 tt cc 103 (90) 11 (10) 0 (0) 0.59-1498 cc tt 33 (29) 45 (40) 34 (30) 0.04-1952 cc aa 114 (100) 0 (0) 0 (0)-2155 cc aa 114 (100) 0 (0) 0 (0)-2488 tt cc 33 (29) 45 (40) 34 (30) 0.04
Data are n (%).HWE, Hardy-Weinberg equilibrium.
Table III. Association between genotype and plasma concentration of VEGF.
VEGF plasma concentration
Locus Homozygote wildtype Heterozygote Homozygote mutation
-7 34 (13–112) 32 (9–130) 20 (17–95)-634 47 (12–136) 28 (10–99) 33 (12–61)-1075 33 (11–105) 79 (9–845) –-1154 27 (10–68) 53 (17–136) 43 (11–144)-1179 33 (11–113) 28 (11–88) –-1190 29 (10–70) 33 (11–120) 56 (12–157)-1198 33 (11–109) 20 –-1203 33 (11–109) 9 –-1455 35 (11–112) 28 (15–42) –-1498 59 (11–159) 38 (12–124) 28 (11–66)-2488 59 (11–159) 38 (12–124) 28 (11–66)
Median (interquartile range).p 0.01.

726 R. S. Ripa et al.
tion seem to increase shortly after acute myocardial infarction [30], and that mRNA expression is low in chronic ischemic myocardium but increased in acute ischemia and reperfused myocardium [31].
The relation between plasma concentration of VEGF and coronary collateral size (Werner classifi-cation, Figure 2), which we present in the present paper, is to our knowledge the first analysis of plasma VEGF versus coronary collaterals. A potential expla-nation for the differences in acute versus chronic ischemia could be that the duration of ischemia is important, and that VEGF concentration is back-regulated by large collaterals size in the patient with chronic CHD, whereas size of collaterals might be influenced by the VEGF concentration in patients with acute ischemia.
We could identify four new loci with mutations. These results supports previous trials in showing the VEGF promoter and 5 untranslated region to be very polymorph, it is not surprising if these polymor-phisms affects the plasma concentration of VEGFprobably through changed affinity for transcriptional factors.
The genotype results are potentially limited by the sample size that could lead to Hardy-Weinberg disequilibrium, type II errors due to the many hap-lotypes, and type I errors due to the multiple poly-morphic loci included in the stepwise analysis. Measuring plasma VEGF is potentially influenced by release from the platelets during collection and pro-cessing of the blood. We have standardized the pro-cedures to diminish this source of error but cannot totally exclude that this could explain some of the large inter-patient variation observed.
Recent larger clinical trials with VEGF treatment in chronic CHD have been disappointing [15,18], and it can be speculated if these neutral results are – at least in part – caused by a very heterogenous patient-population regarding VEGF plasma concen-tration. It would be of conceptual interest to include analysis of coronary collateral size or even hypoxic regulation of VEGF by in-vitro assay in future trials of neovascularization for cardiovascular disease.
We did not find results in support of the hypoth-esis that the VEGF genotype was associated with the concentration of plasma VEGF. The results could suggest that patients with lower concentration of cir-culating VEGF have decreased coronary collateral function. This is of potential interest to future clinical trials for induction of neovascularization.
Acknowledgements
We thank Jesper Schou and Steen Mortensen for skilful technical assistance. The study was supported by grants from the Danish Heart Foundation (No. 0442B18-A1322141); Danish Stem Cell Research Doctoral School; Faculty of Health Sciences,
VEGF [10–14,27]. In addition, Schultz et al. [28] have shown that the development of coronary collat-eral circulation is strongly associated with the ability to induce VEGF in response to hypoxia.
Our trial complements the previous observations in several aspects, first, we have analysed more poly-morphisms, second, we have used plasma concentra-tion of VEGF rather than in vitro induction of VEGFsince this is a more clinical applicable parameter, third, we have assessed both coronary collateral fill-ing (Rentrop) and size (Werner) since we find it likely that VEGF could influence these dissimilar, fourth, we included patients with both acute and chronic CHD, and fifth, we were the first to analyse both genotype, VEGF concentration, and coronary collaterals in the same patients.
After genotyping point-mutations in the VEGFpromoter and 5 untranslated region we could iden-tify 27 different haplotypes where more that half were infrequent ( 2 individuals per haplotype). We found no indication of an effect of the total haplotype on the VEGF plasma concentration. We did identify a cluster of four loci that seemed to explain about 30% of the variation in plasma concentration of VEGF. However, this was found in a stepwise analy-sis including many loci and should thus be inter-preted with great caution and needs validating in an unrelated population. Two of these four loci were in Hardy-Weinberg disequilibrium. The variation in plasma concentration of VEGF is known to be large in both patients with CHD (Figure 1) and in healthy controls [29]. It would be of interest to correlate the four identified polymorphic loci with hypoxic induc-tion of VEGF in a future trial. The plasma concen-tration of VEGF differed between patients with acute versus chronic CHD, and this is in concordance with recent results showing that VEGF plasma concentra-
Figure 2. Association between the VEGF plasma concentration and coronary collateral size according to the Werner classification showing median and interquartile range. Abscissa; Werner Classification: 0 no continuous visible connection between donor and recipient branch, 1 continuous threadlike connection, 2 continuous small sidebranch-like connection. Ordinate in logarithmic scale.

VEGF and collaterals in heart disease 727
Kastrup J, Jørgensen E, Ruck A, Tägil K, Glogar D, [15]Ruzyllo W, Bøtker HE, Dudek D, Drvota V, Hesse B, Thuesen L, Blomberg P, Gyongyosi M, Sylvén C. Direct intramyocardial plasmid vascular endothelial growth factor-A165 gene therapy in patients with stable severe angina pectoris A randomized double-blind placebo-controlled study: the Euroinject One trial. J Am Coll Cardiol. 2005;45:982–8.Ripa RS, Wang Y, Jørgensen E, Johnsen HE, Hesse B, Kastrup J. [16]Intramyocardial injection of vascular endothelial growth factor-A165 plasmid followed by granulocyte-colony stimulating factor to induce angiogenesis in patients with severe chronic ischaemic heart disease. Eur Heart J. 2006;27:1785–92.Hedman M, Hartikainen J, Syvanne M, Stjernvall J, Hedman [17]A, Kivela A, Vanninen E, Mussalo H, Kauppila E, Simula S, Narvanen O, Rantala A, Peuhkurinen K, Nieminen MS, Laakso M, Yla-Herttuala S. Safety and feasibility of catheter-based local intracoronary vascular endothelial growth factor gene transfer in the prevention of postangioplasty and in-stent restenosis and in the treatment of chronic myocardial ischemia: phase II results of the Kuopio Angiogenesis Trial (KAT). Circulation. 2003;107:2677–83.Henry TD, Annex BH, McKendall GR, Azrin MA, Lopez JJ, [18]Giordano FJ, Shah PK, Willerson JT, Benza RL, Berman DS, Gibson CM, Bajamonde A, Rundle AC, Fine J, McCluskey ER. The VIVA trial: Vascular endothelial growth factor in Ischemia for Vascular Angiogenesis. Circulation. 2003;107:1359–65.Simons M, Annex BH, Laham RJ, Kleiman N, Henry T, [19]Dauerman H, Udelson JE, Gervino EV, Pike M, Whitehouse MJ, Moon T, Chronos NA. Pharmacological treatment of coronary artery disease with recombinant fibroblast growth factor-2: double-blind, randomized, controlled clinical trial. Circulation. 2002;105:788–93.Losordo DW, Vale PR, Hendel RC, Milliken CE, [20]Fortuin FD, Cummings N, Schatz RA, Asahara T, Isner JM, Kuntz RE. Phase 1/2 placebo-controlled, double-blind, dose-escalating trial of myocardial vascular endothelial growth factor 2 gene transfer by catheter delivery in patients with chronic myocardial ischemia. Circulation. 2002;105:2012–8.Van de WF, Ardissino D, Betriu A, Cokkinos DV, Falk E, [21]Fox KA, Julian D, Lengyel M, Neumann FJ, Ruzyllo W, Thygesen C, Underwood SR, Vahanian A, Verheugt FW, Wijns W. Management of acute myocardial infarction in patients presenting with ST-segment elevation. The Task Force on the Management of Acute Myocardial Infarction of the European Society of Cardiology. Eur Heart J. 2003;24:28–66.Bertrand ME, Simoonsml, Fox KA, Wallentin LC, [22]Hamm CW, McFadden E, de Feyter PJ, Specchia G, Ruzyllo W. Management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2002;23:1809–40.Rentrop KP, Cohen M, Blanke H, Phillips RA. Changes in [23]collateral channel filling immediately after controlled coro-nary artery occlusion by an angioplasty balloon in human subjects. J Am Coll Cardiol. 1985;5:587–92.Werner GS, Ferrari M, Heinke S, Kuethe F, Surber R, [24]Richartz BM, Figulla HR. Angiographic assessment of collateral connections in comparison with invasively deter-mined collateral function in chronic coronary occlusions. Circulation. 2003;107:1972–7.Ray D, Mishra M, Ralph S, Read I, Davies R, Brenchley P. [25]Association of the VEGF gene with proliferative diabetic retinopathy but not proteinuria in diabetes. Diabetes. 2004;53:861–4.Doi K, Noiri E, Nakao A, Fujita T, Kobayashi S, Tokunaga K. [26]Functional polymorphisms in the vascular endothelial growth factor gene are associated with development of end-stage renal disease in males. J Am Soc Nephrol. 2006;17:823–30.Renner W, Kotschan S, Hoffmann C, Obermayer-Pietsch B, [27]Pilger E. A common 936 C/T mutation in the gene for
Copenhagen University. The study was supported by grants from the Danish Heart Foundation (No. 0442B18-A1322141); Danish Stem Cell Research Doctoral School; and the Faculty of Health Sciences, Copenhagen University.
Declaration of interest: The authors report no con-flicts of interest. The authors alone are responsible for the content and writing of the paper.
References
Schaper W, Scholz D. Factors regulating arteriogenesis. [1]Arterioscler Thromb Vasc Biol. 2003;23:1143–51.Carmeliet P. Mechanisms of angiogenesis and arteriogenesis. [2]Nat Med. 2000;6:389–95.Elsman P, van[3] ,t Hof AW, de Boer MJ, Hoorntje JC, Suryapranata H, Dambrink JH, Zijlstra F. Role of collateral circulation in the acute phase of ST-segment-elevation myocardial infarction treated with primary coronary inter-vention. Eur Heart J. 2004;25:854–8.Werner GS, Ferrari M, Betge S, Gastmann O, Richartz BM, [4]Figulla HR. Collateral function in chronic total coronary occlusions is related to regional myocardial function and duration of occlusion. Circulation. 2001;104:2784–90.Chittenden TW, Sherman JA, Xiong F, Hall AE, Lanahan [5]AA, Taylor JM, Duan H, Pearlman JD, Moore JH, Schwartz SM, Simons M. Transcriptional profiling in coronary artery disease: indications for novel markers of coronary collater-alization. Circulation. 2006;114:1811–20.Clayton JA, Chalothorn D, Faber JE. Vascular endothelial [6]growth factor-A specifies formation of native collaterals and regulates collateral growth in ischemia. Circ Res. 2008;103:1027–36.Deindl E, Buschmann I, Hoefer IE, Podzuweit T, Boengler [7]K, Vogel S, van RN, Fernandez B, Schaper W. Role of ischemia and of hypoxia-inducible genes in arteriogenesis after femoral artery occlusion in the rabbit. Circ Res. 2001;89:779–86.Toyota E, Warltier DC, Brock T, Ritman E, Kolz C, [8]O’Malley P, Rocic P, Focardi M, Chilian WM. Vascular endothelial growth factor is required for coronary collateral growth in the rat. Circulation. 2005;112:2108–13.Pipp F, Heil M, Issbrucker K, Ziegelhoeffer T, Martin S, [9]van den HJ, Weich H, Fernandez B, Golomb G, Carmeliet P, Schaper W, Clauss M. VEGFR-1-selective VEGF homologue PlGF is arteriogenic: evidence for a monocyte-mediated mechanism. Circ Res. 2003;92:378–85.Howell WM, Ali S, Rose-Zerilli MJ, Ye S. VEGF poly-[10]morphisms and severity of atherosclerosis. J Med Genet. 2005;42:485–90.Brogan IJ, Khan N, Isaac K, Hutchinson JA, Pravica V, [11]Hutchinson IV. Novel polymorphisms in the promoter and 5 UTR regions of the human vascular endothelial growth factor gene. Hum Immunol. 1999;60:1245–9.Watson CJ, Webb NJ, Bottomley MJ, Brenchley PE. Identi-[12]fication of polymorphisms within the vascular endothelial growth factor (VEGF) gene: correlation with variation in VEGF protein production. Cytokine. 2000;12:1232–5.Shahbazi M, Fryer AA, Pravica V, Brogan IJ, Ramsay HM, [13]Hutchinson IV, Harden PN. Vascular endothelial growth factor gene polymorphisms are associated with acute renal allograft rejection. J Am Soc Nephrol. 2002;13:260–4.Awata T, Inoue K, Kurihara S, Ohkubo T, Watanabe M, [14]Inukai K, Inoue I, Katayama S. A common polymorphism in the 5 -untranslated region of the VEGF gene is associated with diabetic retinopathy in type 2 diabetes. Diabetes. 2002;51:1635–9.

728 R. S. Ripa et al.
Ripa RS, Jørgensen E, Wang Y, Thune JJ, Nilsson JC, [30]Søndergaard L, Johnsen HE, Køber L, Grande P, Kastrup J. Stem cell mobilization induced by subcutaneous granulocyte-colony stimulating factor to improve cardiac regeneration after acute ST-elevation myocardial infarction: result of the double-blind, randomized, placebo-controlled stem cells in myocardial infarction (STEMMI) trial. Circulation. 2006;113:1983–92.Wang Y, Gabrielsen A, Lawler PR, Paulsson-Berne G, [31]Steinbruchel DA, Hansson GK, Kastrup J. Myocardial gene expression of angiogenic factors in human chronic ischemic myocardium: influence of acute ischemia/cardioplegia and reperfusion. Microcirculation. 2006;13:187–97.
vascular endothelial growth factor is associated with vascular endothelial growth factor plasma levels. J Vasc Res. 2000;37:443–8.Schultz A, Lavie L, Hochberg I, Beyar R, Stone T, Skorecki [28]K, Lavie P, Roguin A, Levy AP. Interindividual heterogeneity in the hypoxic regulation of VEGF: significance for the development of the coronary artery collateral circulation. Circulation. 1999;100:547–52.Ripa RS, Wang Y, Goetze JP, Jørgensen E, Johnsen HE, [29]Tägil K, Hesse B, Kastrup J. Circulating angiogenic cytokines and stem cells in patients with severe chronic ischemic heart disease – indicators of myocardial ischemic burden? Int JCardiol. 2007;120:181–7.

Stem Cell Mobilization Induced by SubcutaneousGranulocyte-Colony Stimulating Factor to
Improve Cardiac Regeneration After Acute ST-ElevationMyocardial Infarction
Result of the Double-Blind, Randomized, Placebo-Controlled Stem Cells inMyocardial Infarction (STEMMI) Trial
Rasmus Sejersten Ripa, MD; Erik Jørgensen, MD; Yongzhong Wang, MD; Jens Jakob Thune, MD;Jens Christian Nilsson, MD; Lars Søndergaard, MD; Hans Erik Johnsen, MD; Lars Køber, MD;
Peer Grande, MD; Jens Kastrup, MD
Background—Phase 1 clinical trials of granulocyte-colony stimulating factor (G-CSF) treatment after myocardialinfarction have indicated that G-CSF treatment is safe and may improve left ventricular function. This randomized,double-blind, placebo-controlled trial aimed to assess the efficacy of subcutaneous G-CSF injections on left ventricularfunction in patients with ST-elevation myocardial infarction.
Methods and Results—Seventy-eight patients (62 men; average age, 56 years) with ST-elevation myocardial infarction wereincluded after successful primary percutaneous coronary stent intervention �12 hours after symptom onset. Patients wererandomized to double-blind treatment with G-CSF (10 �g/kg of body weight) or placebo for 6 days. The primary end pointwas change in systolic wall thickening from baseline to 6 months determined by cardiac magnetic resonance imaging (MRI).An independent core laboratory analyzed all MRI examinations. Systolic wall thickening improved 17% in the infarct areain the G-CSF group and 17% in the placebo group (P�1.0). Comparable results were found in infarct border and noninfarctedmyocardium. Left ventricular ejection fraction improved similarly in the 2 groups measured by both MRI (8.5 versus 8.0;P�0.9) and echocardiography (5.7 versus 3.7; P�0.7). The risk of severe clinical adverse events was not increased by G-CSF.In addition, in-stent late lumen loss and target vessel revascularization rate in the follow-up period were similar in the 2 groups.
Conclusions—Bone marrow stem cell mobilization with subcutaneous G-CSF is safe but did not lead to furtherimprovement in ventricular function after acute myocardial infarction compared with the recovery observed in theplacebo group. (Circulation. 2006;113:1983-1992.)
Key Words: angiogenesis � heart failure � magnetic resonance imaging � myocardial infarction � stem cells
In patients with acute ST-elevation myocardial infarction(STEMI), treatment with acute percutaneous coronary
stent intervention (PCI) is the method of choice to reestablishcoronary blood flow. Although normal epicardial blood flowis reestablished within a few hours after symptom onset,myocardial damage is usually unavoidable and may result inheart failure caused by adverse left ventricular remodeling.1
Editorial p 1926Clinical Perspective p 1992
Animal studies indicate that treatment with bone mar-row– derived adult stem cells after STEMI may regenerate
myocardium by inducing myogenesis and vasculogenesisand improve left ventricular function.2 Most clinical stud-ies have used intracoronary infusion of bone marrowmononuclear cells during cardiac catheterization afteracute STEMI.3–5 However, the results are not conclusive,and the optimal route of stem cell administration remainsto be determined.
Prolonged pharmacological mobilization of bone marrowstem cells with granulocyte colony stimulating factor (G-CSF) is an attractive alternative because the treatment isnoninvasive and well known from clinical hematology.6
Phase 1 clinical trials after myocardial infarction have indi-
Received January 13, 2006; revision received February 23, 2006; accepted February 27, 2006.From the Department of Cardiology, The Heart Centre, University Hospital Rigshospitalet, Copenhagen (R.S.R., E.J., Y.W., J.J.T., L.S., L.K., P.G.,
J.K.); Department of Radiology, University Hospital Rigshospitalet, Copenhagen (R.S.R.); Danish Research Centre for Magnetic Resonance, UniversityHospital Hvidovre, Hvidovre (J.C.N.); and Department of Haematology, Aalborg University Hospital, Aalborg (H.E.J.), Denmark.
The online-only Data Supplement can be found at http://circ.ahajournals.org/cgi/content/full/CIRCULATIONAHA.105.610469/DC1.The study has been registered in clinicaltrial.gov (NCT00135928).Correspondence to Jens Kastrup, MD, DMSc, Medical Department B, Cardiac Catheterization Laboratory 2014, The Heart Centre, University Hospital
Rigshospitalet, DK-2100 Copenhagen Ø, Denmark. E-mail:[email protected]© 2006 American Heart Association, Inc.
Circulation is available at http://www.circulationaha.org DOI: 10.1161/CIRCULATIONAHA.105.610469
1983
Vascular Medicine

cated that G-CSF treatment is safe and may improve leftventricular function.7–10 However, none of these were double-blinded and placebo-controlled trials; thus, the effect ofG-CSF–induced mobilization of bone marrow–derived stemcells on left ventricular function remains unknown.11
The aim of the present Stem Cells in Myocardial Infarction(STEMMI) trial was to asses, in a prospective, double-blind,randomized, placebo-controlled study, the efficacy of subcu-taneous G-CSF injections on the regional and global leftventricular myocardial function in patients with STEMI andsuccessful primary PCI.
MethodsStudy PopulationSeventy-eight patients with STEMI (62 men, 16 women; age, 56�8years, mean�SD) who had been treated successfully with primaryPCI within 12 hours after the onset of symptoms were included in thestudy. STEMI was diagnosed from typical chest pain at rest lasting�30 minutes, the presence of cumulative ST-elevations �0.4 mV in�2 contiguous leads on a standard 12-lead ECG, and a significantrise in serum markers of myocardial infarction. Only patients whowere between 20 and 70 years of age with a culprit lesion located inthe proximal section of a large coronary artery branch, plasmacreatine kinase-MB �100 �g/L, or development of significant Qwaves in the ECG were included. Exclusion criteria were priormyocardial infarction, significant stenosis in a nonculprit coronaryvessel, ventricular arrhythmia after PCI requiring treatment, preg-nancy, unprotected left main stem lesion, diagnosed or suspectedcancer, New York Heart Association class 3 to 4 heart failuresymptoms, or known severe claustrophobia.
The study was approved by the local ethical committee (KF01–239/02) and the Danish Medicines Agency (2612–2225). Allpatients received oral and written information about the study andsigned an informed consent before inclusion in the study.
Study DesignThe STEMMI trial was a prospective, double-blind, randomized,placebo-controlled study allocating patients with acute STEMI in a1:1 ratio after the primary PCI to G-CSF or placebo as a supplementto treatment according to guidelines. Randomization was done inblocks of 4 patients through the use of sequentially numbered, sealedenvelopes. Patients received double-blinded treatment with eitherG-CSF (Neupogen, Amgen Europe BV, Breda, The Netherlands; 10�g/kg body weight) or a similar volume of placebo (isotonicsodium-chloride) as a subcutaneous injection once daily for 6 days.
The treatment was initiated from 1 to 2 days after the STEMI, and 78patients were included from June 2003 to January 2005, as illustratedin Figure 1. Four patients withdrew consent before completion ofG-CSF/placebo treatment as a result of severe claustrophobia duringthe baseline magnetic resonance imaging (MRI). MRI was notfeasible in another 16 patients because of claustrophobia or obesity;these patients remained in the trial and were followed up per protocolwith echocardiography and clinical and invasive examinations.Three patients refused follow-up examinations.
The authors had full access to the data and take full responsibilityfor its integrity. All authors have read and agree to the manuscript aswritten.
End PointsThe prespecified primary end point was change in regional systolicwall thickening from day 1 to 6 months evaluated with cardiac MRI.Secondary end points were (1) change in ejection fraction, end-sys-tolic and end-diastolic volumes, and infarct size by MRI and (2)change in ejection fraction and end-systolic and end-diastolic vol-umes by echocardiography. Safety end points were (1) death of anycause, reinfarction, and new revascularization; (2) other adverseevents; (3) in-stent restenosis; and (4) changes in inflammatoryparameters (C-reactive protein and erythrocyte sedimentation rate).The 30-day clinical safety data have been published previously.12
Cardiac MRIMRI was performed before and 1 and 6 months after inclusion. Adetailed description of the method is available in the online supple-ment 1. In short, cine images and late contrast-enhanced images wereobtained with a 1.5-T clinical scanner (Siemens Vision Magnetom,Siemens AG, Erlangen, Germany).
The independent core laboratory (Bio-Imaging Technologies BV,Leiden, the Netherlands) analyzed all examinations using the MRI-MASS version 6.1 (MEDIS Medical Imaging Systems, Leiden, theNetherlands). The core laboratory was blinded to all patient data andto the order of the follow-up examinations. The analyses of cardiacMRI have a low interobserver variability (3% to 6%); to reduce thisvariability even more, each analysis was quality controlled by asecond MRI technician before final approval. Regional left ventric-ular function was assessed by systolic wall thickening in the infarctregion, the border region, and normal myocardium. Relative systolicwall thickening was calculated as the difference between diastolicand systolic divided by the diastolic wall thickness.
Left ventricular end-diastolic volumes, end-systolic volumes, andmyocardial mass were automatically calculated by the software.Infarct mass was quantified by selecting the signal intensity thresh-old of the hyperenhanced area.
Figure 1. STEMMI trial flowchart.
1984 Circulation April 25, 2006

EchocardiographyTwo-dimensional echocardiography was performed in 55 patients atbaseline and after 6 months of follow-up. All patients were examinedin the left recumbent position with a Vivid7 scanner (GE MedicalSystems, Horten, Norway). Left ventricular volumes at end systoleand end diastole were assessed by Simpson’s biplane method. Leftventricular ejection fraction was assessed in multiples of 5% byvisual assessment by 1 experienced echocardiogram reader blindedto all patient data.
Quantitative Coronary AngiographyAll patients were scheduled to undergo coronary angiography and, ifrequired, repeated PCI before the 6-month MRI follow-up. Allcoronary angiograms for quantitative coronary angiography (QCA)analysis were acquired after intracoronary injection of 0.2 mgglyceryl nitrate according to guidelines. The independent corelaboratory (Bio-Imaging Technologies BV) performed the QCAanalysis using the QCA-CMS version 5.3 software (MEDIS MedicalImaging Systems). Before analysis, the core laboratory conducted
TABLE 1. Baseline Characteristics
Placebo (n�39) G-CSF (n�39)
Age, y 54.7�8.1 57.4�8.6
Male gender, n (%) 34 (87) 28 (72)
Body mass index, kg/m2 28.1�3.9 27.4�4.4
Current smoker, n (%) 31 (80) 22 (56)
Diabetes mellitus, n (%) 4 (10) 3 (8)
Known hypertension, n (%) 10 (26) 13 (33)
Family history of ischemic heart disease, n (%) 14 (37) 15 (40)
Median time from symptom debut to primary PCI(quartiles), h
4:23 (3:32–6:44) 3:47 (2:43–5:25)
Index infarct-related artery, n (%)
LAD 13 (33) 21 (54)
LCx 7 (18) 5 (13)
RCA 19 (49) 13 (33)
TIMI flow grade 0 or 1 before primary PCI 34 (87) 33 (85)
TIMI flow grade 3 after primary PCI 39 (100) 36 (92)
Type of stent, n (%)
No stent 2 (5) 1 (3)
Bare metal 26 (67) 25 (64)
Drug eluting 11 (28) 13 (33)
Platelet glycoprotein IIb/IIIa inhibitors, n (%) 18 (46) 14 (36)
PCI of second vessel during acute procedure, n (%) 4 (10) 9 (23)
Median maximum serum CK-MB concentration(quartiles),* �g/L
274 (141–441) 320 (194–412)
Median time from PCI to G-CSF/placebo(quartiles), h
27:50 (22:34–36:16) 29:37 (25:21–44:15)
Discharge medication,† n (%)
Aspirin 38 (100) 39 (100)
Clopidogrel 37 (97) 39 (100)
�-Blocker 33 (87) 33 (85)
Statin 38 (100) 39 (100)
ACE inhibitor 15 (40) 20 (51)
Medication at 6-mo‡ follow-up
Aspirin 33 (97) 37 (100)
Clopidogrel 33 (97) 37 (100)
�-Blocker 27 (79) 31 (84)
Statin 34 (100) 37 (97)
ACE inhibitor 21 (62) 24 (65)
LAD indicates left anterior descending artery; LCx, left circumflex artery; RCA, right coronary artery;and CK-MB, creatine kinase myocardial band. Data are mean�SD when appropriate.
*Normal upper limit�5.†One in-hospital death in the placebo group.‡Five and 2 patients lost to follow-up, respectively.
Ripa et al Stem Cells in Myocardial Infarction 1985

the standardized frame selection on the angiograms according to theworst view. The selected frames were end diastolic, showed minimalforeshortening, had no overlap, and had good contrast. All frameselections and QCA analyses were conducted according to estab-lished standard operating procedures. After each analysis, a secondQCA technician performed the quality control before final approval.The QCA technicians were fully blinded to all patient data.
Analyses of Peripheral BloodSamples of venous blood were obtained before the G-CSF/placebotreatment (baseline), at days 4 and 7, and at 1 month. The concen-trations of CD34� cells, CD45�/CD34�, and subpopulations in theperipheral blood were measured by flow cytometry as previouslydescribed.13 Plasma concentrations of vascular endothelial growthfactor A (VEGF-A) and stromal cell-derived factor 1 (SDF-1)concentrations were measured in duplicate by a colorimetric ELISAkit (R&D Systems, Minneapolis, Minn). The lower limits of detec-tion were 10 pg/mL for VEGF-A and 18 pg/mL for SDF-1.
Statistical AnalysisThe pretrial power calculation showed that a sample size of 50 wouldyield an expected power of �90% to detect a difference of 15percentage points between the treated and the placebo groups, witha 2-sided significance level of 0.05, and an assumed standarddeviation of 15 percentage points for the systolic wall thickeningchange from baseline to 6 months in both groups. To allow for 33%dropout and claustrophobia or difficulties with breathholding duringthe very early baseline MRI, we decided on a sample size of 78patients.
Analyzes were performed on an intention to treat basis. Theeffects of the G-CSF treatment were analyzed in a 2-factor ANOVAwith repeated measures as a within-subject factor and treatmentgroup as a between-subjects factor or Student’s t test comparingchanges from baseline to 6 months follow-up in the G-CSF andplacebo groups.
Subgroup analyses were not prespecified but based on recentresults from the Reinfusion of Enriched Progenitor cells And Infarct
Figure 2. Changes during the first month after STEMI of (A) white blood cell count and concentration of CD34� cells and plasma con-centration of (B) SDF-1 and (C) VEGF-A. Bars indicate mean�SE.
1986 Circulation April 25, 2006

Remodeling in Acute Myocardial Infarction (REPAIR-AMI) trial.3Analyses were performed with SPSS (version 12.0, SPSS Inc,Chicago, Ill). The level of statistical significance was set at P�0.05,except for the subgroup analyses (see online-only Data SupplementTable), for which significance was set at P�0.01 to account formultiple testing.
ResultsThe clinical and angiographic characteristics of the studypopulation are shown in Table 1. The groups were homoge-neous with a trend toward more smokers and slightly longertime from symptom onset to primary PCI in the placebogroup. All patients received optimal medical treatment in thefollow-up period (Table 1). Subcutaneous G-CSF or placebowas initiated 10 to 65 hours (with 85% initiated �48 hours)after the primary PCI, resulting in a rapid parallel mobiliza-tion of leukocytes and CD34� cells into the peripheralcirculation in the G-CSF group (Figure 2A), whereas the cellsremained unchanged or decreased slightly in the placebogroup. In addition, treatment with G-CSF resulted in mobili-zation of a mesenchymal stem cell line CD45�/CD34� cellsexpressing the SDF-1 receptor CXCR-4 and the VEGFreceptor 2 (Table 2).
The plasma concentration of SDF-1 increased rapidly andsignificantly within the first days after the STEMI in theplacebo group and remained elevated in the first month(Figure 2B). In contrast, SDF-1 was unchanged duringG-CSF treatment and increased significantly at the 1-monthfollow-up. VEGF-A fluctuated nonsignificantly without dif-ferences between the placebo and G-CSF groups (Figure 2C).
Treatment Effect of G-CSF on LeftVentricular FunctionChange in systolic wall thickening in the infarct area frombaseline to the 6-month follow-up did not differ significantlybetween the placebo and G-CSF groups (17�32 versus17�22 percentage points; Figure 3A and 3D). The corre-sponding changes in systolic wall thickening in the infarctborder zone (Figure 3B and 3D) and in noninfarcted normalmyocardium (Figure 3C and 3D) tended to be lower in theG-CSF group (8�23 and �2�30 percentage points) com-
pared with the placebo group (23�23 and 19�38 percentagepoints). However, these differences can be attributed todifferences in the baseline values because the values weresimilar in the 2 groups at the 6-month follow-up.
No significant differences were identified between the 2groups in terms of end-diastolic volume, end-systolic volume,left ventricular mass, and left ventricular ejection fractionderived from the MRI examinations (Figure 4). These resultsare further confirmed by similar changes in the placebo andG-CSF groups measured with echocardiography (Figure 5).In addition, baseline measures of global left ventricularmorphology and function were very similar in the 2 groups(Table 3). The homogeneity of left ventricular ejectionfraction changes measured with MRI between the placeboand G-CSF groups was consistent in a number of subgroupsanalyzed (Data Supplement Table).
The initial infarct size measured by late contrast enhance-ment MRI was similar in the G-CSF (median, 8 g; range, 1 to31 g) and placebo (median, 9 g; range, 1 to 37 g) groups. Theinfarct sizes were unchanged in the 2 groups from baseline tothe 6-month follow-up (Figure 6A). Similar results werefound for infarct size in percent of left ventricular mass(Figure 6B).
Safety of Treatment With G-CSF SoonAfter STEMIG-CSF treatment was well tolerated, with a trend towardmore patients in the G-CSF group reporting mild to moderatemusculoskeletal pain (Table 4) during the treatment. Nopatients withdrew consent because of this side effect.C-reactive protein and erythrocyte sedimentation rates wereanalyzed as markers of inflammation. C-reactive protein waselevated similarly at baseline in the 2 groups (median, 17 and19 mg/L) and subsequently normalized in the placebo group,whereas the concentration increased slightly during G-CSFtreatment (median at day 4, 34 mg/L; at day 7, 22 mg/L) buthad normalized at the 1-month follow-up (G-CSF treatmenteffect, P�0.07). Blood sedimentation rates showed a similarpattern in the G-CSF and placebo groups (P�0.2).
TABLE 2. G-CSF–Induced Cell Mobilization
Placebo(n�33)
G-CSF(n�37) P
CD45�/CD34�, per 1 �L
Baseline 246�164 253�205 0.7
Day 7 260�202 1015�1114 �0.001
Day 28 183�134 169�137 0.5
CD45�/CD34�/CXCR4�, per 1 �L
Baseline 14�12 22�48 0.6
Day 7 15�15 42�45 �0.001
Day 28 6�7 9�12 0.5
CD45�/CD34�/VEGFR-2�, per 1 �L
Baseline 4�3 5�6 1.0
Day 7 3�3 30�47 �0.001
Day 28 2�2 3�3 0.8
Data are mean�SD.
Ripa et al Stem Cells in Myocardial Infarction 1987

As previously reported,12 there were 2 in-hospital majoradverse cardiac events (Table 4). One patient in the placebogroup progressed into cardiogenic shock after the primaryPCI and died 2.5 days later, despite aggressive treatment(intra-aortic balloon pump, dialysis, and ventilator therapy).At the time of death, the patient had received a total of 2injections of placebo.
One patient in the G-CSF group had subacute stentthrombosis 2 days after the primary PCI. The patient initiallyhad a thrombotic total occlusion of the distal right coronaryartery, which was treated with a bare metal stent (18�4 mm),resulting in TIMI grade 3 flow. Forty-eight hours later, thepatient had recurrent chest pain and reelevation of theST-segment on the ECG but no recurrent increase in bio-chemical markers. An acute angiogram showed thromboticocclusion at the proximal edge of the stent. This occlusionwas treated with a new stent implantation. TIMI grade 3 flowwas restored, and there was complete ST resolution. Thesubacute stent thrombosis occurred 6 hours after the firstsubcutaneous injection of G-CSF.
No sustained ventricular arrhythmias were detected duringin-hospital telemetric monitoring. No additional death, rein-farction, or stent thrombosis occurred in the follow-up period(Table 4). However, 2 patients in the placebo group werereferred for heart surgery. One patient had mitral valve repair,and 1 patient underwent coronary artery bypass surgery as aresult of progressive symptoms of coronary artery disease.
Coronary angiograms were obtained in 31 placebo (80%)and 35 G-CSF (90%) patients on average 5 months after theinitial PCI. Target vessel revascularization was performed in8 patients (12%) in relation to the angiographic follow-up (4patients in the placebo group, 4 in the G-CSF group; P�1.0),whereas non–target vessel revascularization was performedin 4 (13%) patients in the placebo group and 2 (6%) in theG-CSF group (P�0.4) (Table 4). The results of the quanti-tative coronary angiography are shown in Table 5; 5 angio-grams were not analyzable for technical reasons. There wereno differences between groups at baseline and at follow-up.
Figure 3. Regional systolic wall thickening measured with MRIat baseline and 1- and 6-month follow-up. Bars indicatemean�SE.
Figure 4. Change in global left ventricular volumes and massfrom baseline to 6-month follow-up measured with MRI. Barsindicate mean�SE.
1988 Circulation April 25, 2006

DiscussionThis first double-blind, randomized, placebo-controlled trialdemonstrated that subcutaneous G-CSF mobilization of bonemarrow stem cells had no effect on left ventricular myocar-dial function or infarct size after STEMI treated with primaryPCI. However, treatment with G-CSF seemed safe and welltolerated.
G-CSF is a potent hematopoietic cytokine that increasesthe production of granulocytes and is involved in mobiliza-tion of granulocytes and stem and progenitor cells from thebone marrow into the blood circulation.14 The mobilizationprocess is not fully understood but is mediated throughenzyme release, leading to digestion of adhesion molecules,and through trophic chemokines; SDF-1 and its receptorCXCR-4 seem of paramount importance.15 Animal studiesand phase 1 clinical trials have suggested a beneficial effectof G-CSF on left ventricular function after myocardial infarc-tion. Orlic et al2 reported favorable results after stem cellmobilization with G-CSF and stem cell factor in mice withacute myocardial infarction. A recent experiment with G-CSFafter reperfused myocardial infarction in rabbits showed animprovement in left ventricular ejection fraction and reducedremodeling.16
Kuethe et al8 compared 14 patients treated with G-CSF 2days after STEMI with 9 patients who refused G-CSFtreatment. The treated group had a nonsignificantly higherincrease in ejection fraction compared with the control group.
Similar results were found in a single-blinded, placebo-controlled study including 20 patients 1.5 days after STEMI.7
The Front-Integrated Revascularization and Stem Cell Liber-ation in Evolving Acute Myocardial Infarction by Granulo-cyte Colony Stimulating Factor (FIRSTLINE-AMI) trial wasa phase 1 randomized, open-label trial of 50 patients. G-CSFtreatment was initiated 1.5 hours after STEMI. The controlgroup did not receive placebo. The trial suggested improve-ment in left ventricular function with enhanced wall thicken-ing, improvement in ejection fraction, and no change inend-diastolic diameter. The control group had less systolicwall thickening, decreased ejection fraction, and increasedend-diastolic diameter.9 Thus, several studies support theefficacy of G-CSF treatment after STEMI, suggesting an
Figure 5. Change in global left ventricular volumesfrom baseline to 6-month follow-up measured withechocardiography. Bars indicate mean�SE.
TABLE 3. Baseline Left Ventricular Morphology and FunctionMeasured by MRI and Echocardiography
Placebo G-CSF P
MRI, n 29 28
Ejection fraction,% 55.7�9.8 51.2�15.4 0.2
End-diastolic volume, mL 127.4�28.3 125.5�36.5 0.8
End-systolic volume, mL 57.5�22.5 64.0�36.5 0.4
Left ventricular mass, g 186.2�39.0 181.8�46.8 0.7
Echocardiography, n 26 29
Ejection fraction,% 48.9�10.6 49.9�10.8 0.7
End-diastolic volume, mL 100.1�28.8 90.3�26.8 0.2
End-systolic volume, mL 49.7�17.9 45.4�18.9 0.4
Data are mean�SD.
Figure 6. Infarct size in (A) grams and (B) percent of left ventric-ular mass measured with MRI. Bars indicate mean�SE. LV indi-cates left ventricular; AMI, acute myocardial infarction.
Ripa et al Stem Cells in Myocardial Infarction 1989

improvement in ejection fraction of 6% to 8%, improvedsystolic wall thickening in the infarct zone, and unchangedend-diastolic volume. When our results, analyzed by ablinded, independent core laboratory, are reviewed, it isremarkable that the changes in our G-CSF group are compa-rable to the results of previous nonblinded phase 1 studies,whereas there are major differences in the control/placebogroups. The changes in global left ventricular function in theplacebo group we report are comparable to those of the MRIstudy by Baks et al,17 who found an increase in ejectionfraction of 7%, an unchanged end-systolic volume, and asmall increase in end-diastolic volume following primarystent PCI after STEMI. Thus, an important finding of our trialis the prominent effect of primary stent PCI on left ventricularfunction in the treatment of STEMI. These findings empha-size the need for caution in the interpretation of positiveresults of phase 1 G-CSF trials.
Possible explanations for the absence of an additionalimprovement in left ventricular function, despite a verysignificant G-CSF mobilization of CD34� and CD45�/CD34� mononuclear cells with the potential for homing tothe necrotic areas, are lack of homing signals from themyocardium, too low a dose of G-CSF, wrong timing of thetreatment, mobilization of inactive subsets of stem cellpopulations, and use of inappropriate end points.
Plasma concentration of stromal cell–derived factor-1(SDF-1) is known to increase rapidly during the first weekafter a myocardial infarction and to reach a maximumconcentration after 3 weeks,18 which is in concordance withour findings in the placebo group. The SDF-1 expression isthought to play a crucial role in induction of stem cellengraftment to ischemic tissue.19 However, we found anunchanged concentration of SDF-1 during the G-CSF treat-ment. This could be due to an inhibition of production ofhoming signals from the myocardium or to the consumptionof SDF-1 by cells that engrafted to the infarcted myocardium.In addition, the quantity of membrane-bound SDF-1, whichmay be the key mediator of homing, was unknown.
Our trial was not designed to investigate either the optimaldose or the optimal time point for G-CSF treatment. Thetreatment regimen resulted in a maximum concentration ofCD34� mononuclear cells 4 to 7 days after the STEMI,which corresponds well to the recent results from theREPAIR-AMI trial that indicated that the optimal time forintracoronary infusion of bone marrow mononuclear cells isday 5 to 6 after the infarction.3 However, considering thatplasma SDF-1 and VEGF-A reach a maximum 3 weeks afterthe infarction, one can speculate whether G-CSF treatmentshould have been postponed until this period. In contrast, arecent study in mice has indicated that G-CSF inhibitsapoptosis of cardiomyocytes by directly affecting the cellsrather than through mobilization of bone marrow cells.20 Thestudy further indicated that the antiapoptotic effect of G-CSFwas significantly reduced if treatment was delayed to 3 daysafter the infarction.20 This concept is interesting because theFIRSTLINE-AMI treated patients 1.5 hours after the STEMIand found an improvement in left ventricular function.9,10 Wecan only speculate if the difference in time to G-CSF canaccount for some of the difference in outcome.
TABLE 4. Cumulative Clinical Events in the 6-MonthFollow-Up Period
Placebo(n�39), n
G-CSF(n�39), n
In-hospital events
Death 1 0
Reinfarction 0 0
Stent thrombosis 0 1
Documented ventricular arrhythmia 0 0
Musculoskeletal discomfort* 3 8
6-Month follow-up (cumulative)
Death 1 0
Reinfarction 0 0
Stent thrombosis 0 1
Thoracic surgery 2 0
Target vessel revascularization 4 4
Non–target vessel revascularization 4 2
Documented ventricular arrhythmia 0 0
Cumulative death or reinfarction 1 0
Cumulative death, reinfarction, or targetvessel revascularization
5 4
*P�0.2
TABLE 5. Angiographic Core Laboratory Results
In-Lesion Zone In-Stent Zone
G-CSF(n�32)
Placebo(n�30) P
G-CSF(n�32)
Placebo(n�30) P
Reference vessel diameter, mm 3.04�0.60 2.99�0.55 0.7 3.06�0.55 2.98�0.56 0.6
Minimal lumen diameter, mm
After primary procedure 2.66�0.57 2.68�0.54 0.9 2.78�0.49 2.71�0.52 0.6
Follow-up 2.14�0.72 2.00�0.71 0.5 2.26�0.71 2.10�0.74 0.4
Diameter stenosis, %
After primary procedure 12.4�14.1 11.1�9.9 0.7 8.4�11.5 9.0�7.9 0.8
Follow-up 28.0�22.2 31.4�19.0 0.5 23.42�22.6 28.1�20.0 0.4
Late lumen loss, mm 0.43�0.59 0.69�0.64 0.1 0.45�0.50 0.63�0.64 0.3
Binary (�50%) restenosis, n (%) 3 (10) 4 (13) 0.7 3 (10) 3 (10) 1.0
Data are mean�SD when appropriate.
1990 Circulation April 25, 2006

We studied a homogeneous patient population withoutnumerous factors that would tend to confound the results, butthis has probably also led to exclusion of high-risk patientswho would potentially benefit most from the treatment. Onlypatients with a significant rise in biochemical markers or anECG indicating a large myocardial infarction were included.In addition, we had an upper age limit of 70 years becauseseveral previous trials have indicated that the mobilization ofCD34� cells decreases with increasing age.21 To furtherincrease the power of our study, we chose regional myocar-dial function rather than global myocardial function as aprimary end point. Thus, we consider the present findingsvery “robust” despite the discrepancy in results when com-pared with previous uncontrolled or unblinded phase 1G-CSF trials, but we cannot exclude the possibility that thetrial has been underpowered to detect a very small difference.The complex interaction between stem cell mobilization andcytokines remains poorly understood, and the results do notexclude the possibility that G-CSF could be part of atreatment strategy combing several cytokines and/or localstem cell delivery in future trials.
SafetyThe trial indicates good short-term safety with G-CSF treat-ment. The subcutaneous injections were well tolerated, withfew patients experiencing mild musculoskeletal pain. Therewere no indications of excessively increased progression ofatherosclerosis in the G-CSF group by angiography and nodeaths or myocardial infarctions in patients treated withG-CSF. We found no indications of clinical significantchange in blood viscosity caused by the increase in whiteblood cell count. This is in concordance with the unalteredviscosity measured in the FIRSTLINE-AMI trial.9 Notewor-thy, as in recent trials7,9 we found no evidence of clinicallyimportant worsening of myocardial inflammation despiteincreases in inflammatory markers in patients treated withG-CSF. This is in agreement with our findings for G-CSFtreatment in patients with chronic myocardial ischemia.22 Wecannot exclude the possibility that G-CSF may have contrib-uted to the 1 case of subacute stent thrombosis observed;however, we find this possibility very unlikely because of theshort time period between the first subcutaneous injection ofG-CSF and the occurrence of the stent thrombosis.
Target vessel revascularization as a result of restenosis andlate lumen loss in the G-CSF and placebo groups was low andwithin the expected range, considering the low proportion ofdiabetics in the patient cohort, typical for a Scandinaviancohort.23,24 Thus, the present coronary angiographic dataanalyzed by an independent core laboratory, combined withsimilar recent trials,7–9,25 argue strongly against speculationsthat G-CSF might enhance the restenosis process, as previ-ously suggested.26 Further examination of safety shouldinclude treatment of more patients and a longer follow-up.
In conclusion, subcutaneous injections of G-CSF soon afterSTEMI treated with primary PCI was well tolerated andseemed safe. However, there was no additional G-CSFtreatment effect on the prespecified primary end points,addressing regional myocardial function, compared with thesubstantial recovery found in the placebo group. In addition,
secondary end points of global left ventricular function andinfarct size were unaffected by the G-CSF treatment. Thediscrepancy in results between previous open-label and thisdouble-blind, placebo-controlled study seems to underscorethe need for blinding and for placebo controls in the evalua-tion of new, potentially angiogenic, stem cell therapies.
AcknowledgmentsThe STEMMI trial has been funded with grants from the DanishHeart Foundation (No. 0442B18-A1322141); Danish Stem CellResearch Doctoral School; Faculty of Health Science, CopenhagenUniversity; Research Foundation of Rigshospitalet; Raimond ogDagmar Ringgård-Bohn’s Foundation; Aase og Ejnar DanielsensFoundation; Erik og Martha Scheibels Legat; and Arvid NilssonsFoundation.
DisclosuresNone.
References1. Pfeffer MA, Braunwald E. Ventricular remodeling after myocardial
infarction: experimental observations and clinical implications. Circu-lation. 1990;81:1161–1172.
2. Orlic D, Kajstura J, Chimenti S, Limana F, Jakoniuk I, Quaini F, Nadal-Ginard B, Bodine DM, Leri A, Anversa P. Mobilized bone marrow cellsrepair the infarcted heart, improving function and survival. Proc NatlAcad Sci U S A. 2001;98:10344–10349.
3. Schächinger V, Erbs S, Elsässer A, Haberbosch W, Hambrecht R,Hölschermann H, Yu J, Corti R, Mathey D, Hamm C, Süselbeck T,Assmus B, Tonn T, Dimmeler S, Zeiher AM. Intracoronary infusion ofbone marrow-derived progenitor cells in acute myocardial infarction: arandomized, double-blind, placebo-controlled multicenter trial(REPAIR-AMI). Circulation. 2005;112:3362. Abstract.
4. Strauer BE, Brehm M, Zeus T, Kostering M, Hernandez A, Sorg RV,Kogler G, Wernet P. Repair of infarcted myocardium by autologousintracoronary mononuclear bone marrow cell transplantation in humans.Circulation. 2002;106:1913–1918.
5. Wollert KC, Meyer GP, Lotz J, Ringes-Lichtenberg S, Lippolt P,Breidenbach C, Fichtner S, Korte T, Hornig B, Messinger D, Arseniev L,Hertenstein B, Ganser A, Drexler H. Intracoronary autologous bone-marrow cell transfer after myocardial infarction: the BOOST randomisedcontrolled clinical trial. Lancet. 2004;364:141–148.
6. Johnsen HE. Clinical practice and future needs in recombinant humangranulocyte colony-stimulating factor treatment: a review of randomizedtrials in clinical haemato-oncology. J Int Med Res. 2001;29:87–99.
7. Valgimigli M, Rigolin GM, Cittanti C, Malagutti P, Curello S, Percoco G,Bugli AM, Della PM, Bragotti LZ, Ansani L, Mauro E, Lanfranchi A,Giganti M, Feggi L, Castoldi G, Ferrari R. Use of granulocyte-colonystimulating factor during acute myocardial infarction to enhance bonemarrow stem cell mobilization in humans: clinical and angiographicsafety profile. Eur Heart J. 2005;26:1838–1845.
8. Kuethe F, Figulla HR, Herzau M, Voth M, Fritzenwanger M, OpfermannT, Pachmann K, Krack A, Sayer HG, Gottschild D, Werner GS.Treatment with granulocyte colony-stimulating factor for mobilization ofbone marrow cells in patients with acute myocardial infarction. AmHeart J. 2005;150:115.
9. Ince H, Petzsch M, Kleine HD, Schmidt H, Rehders T, Korber T,Schumichen C, Freund M, Nienaber CA. Preservation from left ventric-ular remodeling by front-integrated revascularization and stem cell lib-eration in evolving acute myocardial infarction by use of granulocyte-colony-stimulating factor (FIRSTLINE-AMI). Circulation. 2005;112:3097–3106.
10. Ince H, Petzsch M, Kleine HD, Eckard H, Rehders T, Burska D, KischeS, Freund M, Nienaber CA. Prevention of left ventricular remodeling withgranulocyte colony-stimulating factor after acute myocardial infarction:final 1-year results of the Front-Integrated Revascularization and StemCell Liberation in Evolving Acute Myocardial Infarction by GranulocyteColony-Stimulating Factor (FIRSTLINE-AMI) Trial. Circulation. 2005;112(suppl I):I-73–I-80.
Ripa et al Stem Cells in Myocardial Infarction 1991

11. de Muinck ED, Simons M. Calling on reserves: granulocyte colonystimulating growth factor in cardiac repair. Circulation. 2005;112:3033–3035.
12. Ripa RS, Wang Y, Jørgensen E, Johnsen HE, Grande P, Kastrup J. Safetyof bone-marrow stem cell mobilisation induced by granulocyte-colonystimulating factor: clinical 30 days blinded results from the Stem Cells inMyocardial Infarction (STEMMI) trial. Heart Drug. 2005;5:177–182.
13. Mancuso P, Burlini A, Pruneri G, Goldhirsch A, Martinelli G, BertoliniF. Resting and activated endothelial cells are increased in the peripheralblood of cancer patients. Blood. 2001;97:3658–3661.
14. Anderlini P, Donato M, Chan KW, Huh YO, Gee AP, Lauppe MJ,Champlin RE, Korbling M. Allogeneic blood progenitor cell collection innormal donors after mobilization with filgrastim: the M.D. AndersonCancer Center experience. Transfusion. 1999;39:555–560.
15. Flomenberg N, DiPersio J, Calandra G. Role of CXCR4 chemokinereceptor blockade using AMD3100 for mobilization of autologous hema-topoietic progenitor cells. Acta Haematol. 2005;114:198–205.
16. Minatoguchi S, Takemura G, Chen XH, Wang N, Uno Y, Koda M, AraiM, Misao Y, Lu C, Suzuki K, Goto K, Komada A, Takahashi T, Kosai K,Fujiwara T, Fujiwara H. Acceleration of the healing process and myo-cardial regeneration may be important as a mechanism of improvement ofcardiac function and remodeling by postinfarction granulocyte colony-stimulating factor treatment. Circulation. 2004;109:2572–2580.
17. Baks T, van Geuns RJ, Biagini E, Wielopolski P, Mollet NR, CademartiriF, Boersma E, van der Giessen WJ, Krestin GP, Duncker DJ, Serruys PW,de Feyter PJ. Recovery of left ventricular function after primary angio-plasty for acute myocardial infarction. Eur Heart J. 2005;26:1070–1077.
18. Wang Y, Johnsen HE, Mortensen S, Bindslev L, Ripa RS, Haack-Sorensen M, Jørgensen E, Fang W, Kastrup J. Changes in circulatingmesenchymal stem cells, stem cell homing factor, and vascular growthfactors in patients with acute ST-elevation myocardial infarction treatedwith primary percutaneous coronary intervention. Heart. October 26,2005. DOI: 10.1136/hrt.2005.069799. Available at: http://heart.bmjjour-nals.com/. Accessed 2006.
19. Askari AT, Unzek S, Popovic ZB, Goldman CK, Forudi F, KiedrowskiM, Rovner A, Ellis SG, Thomas JD, DiCorleto PE, Topol EJ, Penn MS.Effect of stromal-cell-derived factor 1 on stem-cell homing and tissueregeneration in ischaemic cardiomyopathy. Lancet. 2003;362:697–703.
20. Harada M, Qin Y, Takano H, Minamino T, Zou Y, Toko H, Ohtsuka M,Matsuura K, Sano M, Nishi J, Iwanaga K, Akazawa H, Kunieda T, Zhu
W, Hasegawa H, Kunisada K, Nagai T, Nakaya H, Yamauchi-TakiharaK, Komuro I. G-CSF prevents cardiac remodeling after myocardialinfarction by activating the Jak-Stat pathway in cardiomyocytes. NatMed. 2005;11:305–311.
21. de la Rubia J, Arbona C., de Arriba F, del Canizo C, Brunet S, ZamoraC, Diaz MA, Bargay J, Petit J, de la SJ, Insunza A, Arrieta R, Pascual MJ,Serrano D, Sanjuan I, Espigado I, Alegre A, Martinez D, Verdeguer A,Martinez C, Benlloch L, Sanz MA. Analysis of factors associated withlow peripheral blood progenitor cell collection in normal donors. Trans-fusion. 2002;42:4–9.
22. Wang Y, Tägil K, Ripa RS, Nilsson JC, Carstensen S, Jørgensen E,Sondergaard L, Hesse B, Johnsen HE, Kastrup J. Effect of mobilizationof bone marrow stem cells by granulocyte colony stimulating factor onclinical symptoms, left ventricular perfusion and function in patients withsevere chronic ischemic heart disease. Int J Cardiol. 2005;100:477–483.
23. Jørgensen E, Kelbæk H, Helqvist S, Jensen GV, Saunamaki K, Kastrup J,Havndrup O, Bundgaard H, Kyst MJ, Christiansen M, Andersen PS,Reiber JH. Predictors of coronary in-stent restenosis: importance of an-giotensin-converting enzyme gene polymorphism and treatment with an-giotensin-converting enzyme inhibitors. J Am Coll Cardiol. 2001;38:1434–1439.
24. Kelbæk H, Thuesen L, Helqvist S, Kløvgaard L, Jørgensen E, AljabbariS, Saunamaki K, Krussell LR, Jensen GVH, Bøtker HE, Lassen JF,Andersen HR, Thayssen P, Galløe A, van Weert AW. The StentingCoronary Arteries in Non-Stress/Benestent Disease (SCANDSTENT)Trial. J Am Coll Cardiol. 2006;47:449–455.
25. Jørgensen E, Ripa RS, Helqvist S, Wang Y, Johnsen HE, Grande P,Kastrup J. In-stent neo-intimal hyperplasia after stem cell mobilization bygranulocyte-colony stimulating factor: preliminary intracoronaryultrasound results from a double-blind randomized placebo-controlledstudy of patients treated with percutaneous coronary intervention forST-elevation myocardial infarction (STEMMI Trial). Int J Cardiol. July28, 2005. DOI: 10.1016/j.ijcard.2005.06.045. Available at: http://www.sciencedirect.com/science/journal/01675273. Accessed 2006.
26. Kang HJ, Kim HS, Zhang SY, Park KW, Cho HJ, Koo BK, Kim YJ, SooLD, Sohn DW, Han KS, Oh BH, Lee MM, Park YB. Effects of intra-coronary infusion of peripheral blood stem-cells mobilised withgranulocyte-colony stimulating factor on left ventricular systolic functionand restenosis after coronary stenting in myocardial infarction: theMAGIC cell randomised clinical trial. Lancet. 2004;363:751–756.
CLINICAL PERSPECTIVEPrevious research indicated that mobilization of bone marrow–derived stem cells with granulocyte-colony stimulatingfactor (G-CSF) could help regenerate cardiac cells after acute myocardial infarction by increased vascularization,regeneration of cardiomyocytes, and/or a direct antiapoptotic effect. Accordingly, we performed a randomized,placebo-controlled, double-blind trial to test whether patients with an ST-segment elevation myocardial infarction treatedwith primary percutaneous coronary stent intervention (PCI) derive therapeutic benefit from addition of G-CSF to modernconventional therapy. Disappointingly, there was no evidence of additional benefit of G-CSF after 6 months follow-up.Systolic wall thickening in the infarct area had increased 17% in the G-CSF group and 17% in the placebo group. Leftventricular ejection fraction increased at nearly identical rates in the 2 groups measured by both magnetic resonanceimaging and echocardiography. Rates of death or myocardial infarction, new revascularization, and restenosis 6 monthsafter the acute myocardial infarction were also similar in the G-CSF and placebo groups. Thus, subcutaneous G-CSF afterPCI for ST-elevation infarction was safe, but did not lead to further improvements of left ventricular function whencompared to placebo. It remains to be determined if G-CSF treatment could be an effective part of a treatment strategycombining several cytokines and/or local stem cell delivery. However, this trial underscores the need for blinding andplacebo controls in the evaluation.
1992 Circulation April 25, 2006

Circulation. 2006;113:1983-1992
ONLINE SUPPLEMENT 1 Cardiac MRI Myocardial function and infarct size was examined by MRI before, 1 and 6 months after the G-CSF or placebo treatment. All MRI images were obtained with a 1.5-T clinical scanner (Siemens Vision Magnetom, Siemens AG, Erlangen, Germany) using a phased array chest coil. Patients were examined in the supine position with care taken to ensure identical position in the scanner at all three exams. All images were acquired using ECG gating and breath-hold technique. Cine images were acquired with a fast low angle shot (FLASH) cinematographic pulse sequence. The entire left ventricle was covered with a stack of short axis images. Slice thickness was 8 mm with 2 mm inter-slice gaps. A bolus of gadopentetate dimeglumine (Magnevist, Schering), 0.15 mmol per kilogram of bodyweight was injected intravenously. After a 15 minutes break with the patient positioned in the scanner, the inversion time was set to null normal myocardium, using a segmented inverse recovery turbo-FLASH sequence.1 Using this optimized inversion time the total infarct area was covered with consecutive short axis slices with slice thickness of 8 mm and 2 mm inter-slice gaps. All MRI exams were analyzed by an independent core laboratory (Bio-Imaging Technologies B.V., Leiden, The
Netherlands) using the MRI-MASS® version 6.1 software (MEDIS Medical Imaging Systems, Leiden, The Netherlands). The core laboratory was blinded to all patient-data and to the order of the two follow-up exams. All analyses were conducted according to established standard operating procedures. Endocardial and epicardial borders were manually traced in all end-diastolic and end-systolic short-axis slices by one technician using the automated contour detection as starting point. The analyses of cardiac MRI have a low interobserver variability (3-6%). After each analysis a second MRI technician performed a quality control before final approval to diminish the variability even more. Regional left-ventricular function was assessed by determining systolic wall thickening in the infarct region, the border region, and normal myocardium. The systolic and diastolic thicknesses were measured along 100 chords on each slice that
were equally distributed along the circumference of the LV. To correct for rotational transformation during systole, we used the internal posterior junction of the right ventricular wall with the interventricular septum as landmark for cord number 1. The mean thickness in each region was determined by averaging the measurements of the chords within the regions. Relative systolic wall thickening was calculated as the difference between diastolic and systolic wall thickness divided by the diastolic wall thickness. The position of the three regions was determined using the baseline contrast enhanced images, where areas adjacent to the region with delayed contrast enhancement were defined as the border regions. Left ventricular end-diastolic volumes and left-ventricular end-systolic volumes were automatically calculated by the software using the planimetrically measured areas of the cavities multiplied by slice thickness plus inter-slice gap. The left-ventricular myocardial mass generated by the software is a direct multiplication of the myocardial volume (ml) times a density factor of 1.05 g/ml, including the papillary muscles as part of the myocardium. For assessment of infarct volumes, late contrast enhancement was quantified. Infarct size on each of the short-axis images was assessed by selecting the signal intensity threshold of the hyperenhanced area (i.e. the pixels between the endo- and epi-cardial borders considered to be late enhanced). The infarct size in each patient was calculated as total infarct area multiplied by the section thickness. After determining the total mass of enhanced tissue, the percentages of enhanced tissue for total LV myocardium was calculated by dividing with the total mass of LV myocardium and multiply with 100. References
1. Simonetti OP, Kim RJ, Fieno DS, Hillenbrand HB,
Wu E, Bundy JM, Finn JP, Judd RM. An improved MR imaging technique for the visualization of myocardial infarction. Radiology. 2001;218:215-223.

Circulation. 2006;113:1983-1992
ONLINE SUPPLEMENT 2 Online Supplemental Table 1. G-CSF treatment effect on left ventricular ejection fraction changes from baseline to 6
months follow-up by MRI in different subgroups.
G-CSF treatment effect* P-value ‡
Males (n=43) 1.6 (-5.1 to 8.2) 0.6
Females (n=11) -3.9 (-17.9 to 10.0) 0.5
Age < 58 years (n=25)† -5.4 (-11.8 to 1.0) 0.1
Age ≥ 58 years (n=29)† 4.5 (-5.3 to 14.3) 0.4
Time from symptom onset to G-CSF
<34:30 hours (n=24) †
3.5 (-2.9 to 9.9) 0.3
Time from symptom onset to G-CSF
≥34:30 hours (n=30) †
-1.8 (-11.2 to 7.6) 0.7
Baseline ejection fraction <56 (n=26) † 6.5 (-2.9 to 15.8) 0.2
Baseline ejection fraction ≥56 (n=28) † -6.2 (-11.8 to -0.6) 0.03
Infarct size <8.5% (n=26) † -4.1 (-12.0 to 3.9) 0.3
Infarct size ≥8.5% (n=26) † 2.6 (-5.8 to 11) 0.5
* Mean difference (95% confidence intervals) between placebo and G-CSF group in percentage points; positive numbers indicates G-CSF better than placebo. † Median values of the total study population are used as cut-off. ‡ Significance level set at p<0.01 to ac

Bone Marrow–Derived Mesenchymal Cell Mobilization byGranulocyte-Colony Stimulating Factor After Acute
Myocardial InfarctionResults From the Stem Cells in Myocardial Infarction (STEMMI) Trial
Rasmus Sejersten Ripa, MD; Mandana Haack-Sørensen, MSc; Yongzhong Wang, MD, PhD;Erik Jørgensen, MD; Steen Mortensen, Tech; Lene Bindslev, MSc, PhD;
Tina Friis, MSc, PhD; Jens Kastrup, MD, DMSc
Background—Granulocyte-colony stimulating factor (G-CSF) after myocardial infarction does not affect systolic functionwhen compared with placebo. In contrast, intracoronary infusion of bone marrow cells appears to improve ejectionfraction. We aimed to evaluate the G-CSF mobilization of subsets of stem cells.
Methods and Results—We included 78 patients (62 men; 56�8 years) with ST-elevation myocardial infarction treatedwith primary percutaneous intervention �12 hours after symptom onset. Patients were randomized to double-blindG-CSF (10 �g/kg/d) or placebo. Over 7 days, the myocardium was exposed to 25�109 G-CSF mobilized CD34� cells,compared with 3�109 cells in placebo patients (P�0.001); and to 4.9�1011 mesenchymal stem cells, compared with2.0�1011 in the placebo group (P�0.001). The fraction of CD34� cells/leukocyte increased during G-CSF treatment(from 0.3�0.2 to 1.1�0.9 �10�3, P�0.001 when compared with placebo), whereas the fraction of putativemesenchymal stem cells/leukocyte decreased (from 22�17 to 14�11 �10�3, P�0.01 when compared with placebo).An inverse association between number of circulating mesenchymal stem cells and change in ejection fraction was found(regression coefficient �6.8, P�0.004), however none of the mesenchymal cell subtypes analyzed, were independentpredictors of systolic recovery.
Conclusions—The dissociated pattern for circulating CD34� and mesenchymal stem cells could be attributable to reducedmesenchymal stem cell mobilization from the bone marrow by G-CSF, or increased homing of mesenchymal stem cellsto the infarcted myocardium. The inverse association between circulating mesenchymal stem cells and systolic recoverymay be of clinical importance and should be explored further. (Circulation. 2007;116[suppl I]:I-24–I-30.)
Key Words: stem cells � angiogenesis � heart failure � magnetic resonance imaging � myocardial infarction
Granulocyte-colony stimulating factor (G-CSF) therapy,with the mobilization of bone marrow stem cells soon
after ST-elevation acute myocardial infarction in the StemCells in Myocardial Infarction (STEMMI) trial, did notimprove left ventricular systolic function when comparedwith placebo.1,2 These results have been confirmed by theREVIVAL-2 trial3 and the G-CSF-STEMI trial.4 G-CSF washypothesized to have beneficial effects on the myocardiumboth indirectly through the mobilization of bone-marrowstem cells into the peripheral circulation, and also perhapsdirectly by inhibiting myocardial apoptosis.5 Direct infusionof bone marrow mononuclear cells into the coronary arteriesafter an acute myocardial infarction has been investigated inseveral medium sized clinical trials,6–8 but only 29,10 arerandomized, double-blind, and placebo-controlled. TheREPAIR-AMI trial suggested a significant improvement of
left ventricular ejection fraction,9 whereas only regionalsystolic function appeared to improve after intracoronaryinfusion of bone marrow mononuclear cells in the trial byJanssens et al.10 The apparently contradictory results of directintracoronary infusion of bone marrow–aspirated cells versuspharmacological mobilization of bone marrow–derived stemcells are puzzling. G-CSF is known to mobilize cells from thehematopoietic cell line,11 and recent evidence suggests thatbone marrow–derived mesenchymal stem cells, in particular,have cardiac reparative properties.12
The primary end point of the published STEMMI trial waschange in regional systolic wall thickening from day 1 to 6 monthsas evaluated by cardiac magnetic resonance imaging (MRI).Changes in ejection fraction by MRI were a secondary end point.1
The objective of this substudy was to describe (1) the cellsmobilized by G-CSF with special emphasis on mesenchymal
From the Department of Cardiology, The Heart Centre, University Hospital Rigshospitalet, Copenhagen, Denmark.Presented at the American Heart Association Scientific Sessions, Chicago, Ill, November 12–15, 2006.Correspondence to Jens Kastrup MD, DMSc, Medical Department B, Cardiac Catheterization Laboratory 2014, The Heart Centre, University Hospital
Rigshospitalet, DK-2100 Copenhagen Ø, Denmark. E-mail [email protected]© 2007 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.106.678649
I-24
Cell Transplantation and Tissue Regeneration

stem cells, and (2) the association between the plasmaconcentration of the cells and subsequent changes in leftventricular systolic function.
MethodsStudy DesignAll 78 patients from the STEMMI trial were included for analyses.Details of the study design and inclusion criteria have been publishedpreviously.1 Briefly, patients were included if they had a first timeST-elevation myocardial infarction (STEMI) successfully treatedwith primary percutaneous coronary intervention within 12 hoursafter the onset of symptoms. Patients were randomized to double-blind treatment with subcutaneous G-CSF (Neupogen, Amgen Eu-rope BV, Breda, The Netherlands; 10 �g/kg body weight) or asimilar volume of placebo (isotonic sodium-chloride) once daily for6 days. The study was approved by the local ethical committee (KF01 to 239/02), the Danish Medicines Agency (2612–2225), and wasregistered in clinicaltrials.gov (NCT00135928). All patients receivedverbal and written information about the study, and gave their signedconsent before inclusion.
Quantification and Characterization of Stem CellsThe concentration of circulating CD34-positive (CD34�) cells andcirculating putative mesenchymal stem cells in the blood quantifiedas CD45 and CD34 double-negative (CD45�/CD34�) cells wasmeasured by multiparametric flow cytometry using anti-CD45 (Bec-ton Dickinson) and anti-CD34 (BD), as previously described.13,14
A panel of monoclonal and polyclonal antibodies was used tofurther characterize mesenchymal stem cells, including anti-CD105(Endoglin; Ancell), anti-CD31 (platelet endothelial cell adhesionmolecule; BD), anti-CD133 (hematopoietic stem cell antigen; Milte-nyi Biotec), anti-CD73 (BD), anti-CD166 (activated leukocyte ad-hesion molecule; BD), anti-CXC chemokine receptor 4; R&DSystems), anti-VEGF R2 (R&D Systems), and anti-CD144 (VE-cadherin; BenderMed). Analytic gates were used to enumerate thetotal number and subsets of circulating CD45�/CD34� cells. Cellsuspensions were evaluated by a FACS Calibur (BD). At least100 000 cells per sample were acquired. Analyses were consideredinformative when adequate numbers of CD45�/CD34�events (300–400) were collected in the analytic gate.
The mean number of both CD34� cells and CD45�/CD34� cellssupplied to the postischemic myocardium by the blood during thefirst week after the treatment was approximated. First, we calculatedthe mean plasma concentration of cells during the first week:[(concentration day 1)�(concentration day 4)�(concentration day7)]/3 (assuming a near linear increase in concentration). Next, weestimated the blood flow through the infarct related artery during oneweek (4800 mL/hr�24 hour�7 days). Finally, to get a roughestimate of the number of cells passing through the infarct relatedartery during 1 week, we multiplied the blood flow with the “meanplasma cell concentration” in each patient.
Plasma CytokinesPlasma concentrations of vascular endothelial growth factor A(VEGF-A) and stromal cell-derived factor 1 (SDF-1) concentrationswere measured in duplicate by a colorimetric ELISA kit (R&DSystems). The lower limits of detection were 10 pg/mL for VEGF-Aand 18 pg/mL for SDF-1, respectively.
Cardiac MRIMRI was performed at baseline and 6 months after inclusion aspreviously described in details.1 In short, cine and late contrast-enhancement images were obtained with a 1.5-T scanner (SiemensVision Magnetom, Siemens AG). The examinations were analyzedby an independent core laboratory (Bio-Imaging Technologies B.V.)using the MRI-MASS v6.1 (MEDIS Medical Imaging Systems). Thecore laboratory was blinded to all patient-data. MRI was feasible in28 and 31 patients in the placebo and the G-CSF group, respectively.
Statistical AnalysesData were analyzed using SPSS 13.0. The numbers of cells in the 2treatment groups were compared using Mann-Whitney U test. Theeffects of the G-CSF treatment on cell, SDF-1, and VEGF-Aconcentrations were analyzed in a 2-factor ANOVA with repeatedmeasures as a within-subject factor and treatment group as abetween-subjects factor after logarithmic transformation to assumenormal distribution if appropriate. Associations between number ofcell supplied to the postischemic myocardium and change in leftventricular systolic function were determined using linear regressionmodels with type of treatment included as covariate in all analyses.All data are expressed as mean�SD unless otherwise stated. All testswere 2-sided, and statistical level of significance was set at P�0.05.
The authors had full access to the data and take responsibility forits integrity. All authors have read and agree to the manuscript aswritten.
ResultsPatientsMain baseline characteristics are shown in Table 1, a detaileddescription has been published previously.1 We included 39patients in each group. In the placebo group, 3 patientswithdrew consent and 1 patient died, and 1 patient in theG-CSF group withdrew consent before completion of thestudy treatment. Thus, cell data pertaining to the placebo andG-CSF were available from 35 and 38 patients, respectively.
Mobilized CellsThe G-CSF treatment led to a substantial increase in theplasma concentration of leukocytes (from 8.3�2.2 to51.2�18.0 �106/mL) and CD34� cells (supplemental TableI, available online at http://circ.ahajournals.org), with a peak
TABLE 1. Baseline Characteristics
Placebo (n�39) G-CSF (n�39)
Age, y 54.7�8.1 57.4�8.6
Male, n (%) 34 (87) 28 (72)
Body mass index, kg/m2 28.1�3.9 27.4�4.4
Diabetes mellitus, n (%) 4 (10) 3 (8)
Known hypertension, n (%) 10 (26) 13 (33)
Current smoker, n (%) 31 (80) 22 (56)
Median maximum serum CK-MB concentration(quartiles),�g/L
274 (141–441) 320 (194–412)
Median time from symptom debut to primarypercutaneous coronary intervention. (quartiles), h
4:23 (3:32–6:44) 3:47 (2:43–5:25)
Ripa et al Stem Cells in Myocardial Infarction I-25

value 7 days after initiation of G-CSF therapy and normal-ization after 30 days. Thus, over 7 days, the postischemicmyocardium was exposed to approximately 25�20 �109
circulating CD34� cells, compared with approximately3.2�1.4 �109 cells in the patients receiving placebo(P�0.001).
The number of circulating putative mesenchymal stemcells (CD45�/CD34�) increased approximately 4-fold (sup-plemental Table I) during G-CSF treatment, resulting inmyocardial exposure to 5.0�3.7 �1011 cells after G-CSFtreatment compared with 2.0�1.2 �1011 in the placebo group(P�0.001).
Figure 1 shows the number of CD34� cells (panel A) andCD45�/CD34� (panel B) relative to the leukocytes. Thefraction of CD34� cells increased during G-CSF treatment,whereas the fraction of CD45�/CD34� cells surprisinglydecreased during the treatment. The fraction of mononuclearcells in the blood without the CD45 marker but with theCD34 marker (CD45�/CD34�) was unaffected by the G-CSFtreatment (P�0.1: 0.14�0.09 versus 0.19�0.14 per 1000leukocytes at day 7 in the placebo and G-CSF groups,respectively).
The CD45�/CD34� mesenchymal stem cells were subchar-acterized by early stem cell markers (CD105, CD73, CD166,CXCR4), endothelial markers (CD31, CD144, VEGFR2), ora hematopoietic marker (CD133). Figure 2 shows the relative
change from baseline to day 7 in both the placebo and theG-CSF groups. Most of the mesenchymal stem cells subfrac-tions were increased (had a value above 1) in the placebogroup and reflect the natural course after a myocardialinfarction. However, the fraction of CD45�/CD34� cells withthe early stem cell marker CD73 had a significantly lowerincrease in the G-CSF group compared with the increase inthe placebo group; and the fraction with endothelial markerCD31 was significantly decreased in the G-CSF treatedgroup. As expected, cells with the hematopoietic markerCD133 increased significantly more in the G-CSF group thanin the placebo group. Furthermore, it is apparent from Figure3 that most of the sub-cell fractions tended to decrease duringG-CSF treatment.
Change in Left Ventricular Systolic Function andStem Cell MobilizationThere was no association between the total number of CD34�
cells supplied to the postischemic myocardium after myocar-dial infarction and the subsequent change in left ventricularejection fraction (Figure 4A; 95% CI of regression coefficient�8.5 to 1.5, P�0.2).
An inverse association was found between the number ofCD45�/CD34� cells supplied to the postischemic myocardi-um and the change in left ventricular ejection fraction (Figure4B) (95% CI of regression coefficient �11.4 to �2.2,
Figure 1. Ratio of (A) CD34� cells/1000 leukocytes, (B) CD45�/CD34� cells/1000 leukocytes, and (C) CD45�/CD34� cells/CD34� cell inthe blood during 30 days after myocardial infarction, divided into treatment groups. Compared using repeated measures ANOVA.
Figure 2. Subtypes of CD45�/CD34� cells. Theconcentration ratios on day 7 in relation to base-line concentrations are shown. A value above 1indicates an increase in concentration.
I-26 Circulation September 11, 2007

P�0.004). This association remained significant when con-trolling for infarct size, plasma concentration of SDF-1,plasma concentration of VEGF, and leukocyte concentration.The association was not reproduced when using systolic wall
thickening in the infarct area (regression coefficient �0.08,P�0.2), the infarct border area (regression coefficient �0.08,P�0.1), or infarct size (regression coefficient 2.04, P�0.3) asoutcome. There was no significant interaction between typeof treatment and number of CD45�/CD34� cells indicatingthat the association was not significantly affected by theG-CSF treatment.
Next, we examined the association between the subtypes ofCD45�/CD34� cells and changes in left ventricular ejectionfraction (Table 2). None of the subtypes were independentpredictors when controlling for treatment type and the totalnumber of CD45�/CD34� cells. Only cells with the hemato-poietic marker CD133 tended to have a positive associationwith the systolic improvement (P�0.07).
Change in SDF-1 and VEGF-APlasma ConcentrationsThe individual time course of homing factor SDF-1 and thevascular growth factor VEGF-A plasma concentrations areshown in supplemental Figure I. As previously shown,1 theSDF-1 time course differed significantly between the G-CSFand placebo groups (P�0.001), whereas the VEGF-A timecourse were similar (P�0.4). Classic cardiovascular riskfactors (diabetes mellitus, smoking, age, and gender) as wellas time to reperfusion and infarct size did not relate to theplasma concentration of SDF-1 by linear regression analysis,but high VEGF concentration at day 4 and 7 were signifi-
Figure 3. Subtypes of CD45�/CD34� cells during 30 days after myo-cardial infarction. Compared using repeated measures ANOVA.
Figure 4. Association between changes in left ven-tricular ejection fraction during 6 months and (A)CD34� and (B) CD45�/CD34� cells. Regression linewith 95% confidence interval. *Abscissa in loga-rithmic scale.
TABLE 2. Association Between Subtypes of CD45�/CD34� andRecovery of Left Ventricular Ejection Fraction
Cells in 109 per ml Regression Coefficient* 95% CI
CD45�/34�/105� �0.15 �0.38 to 0.38
CD45�/34�/73� �1.13 �3.45 to 1.18
CD45�/34�/166� 0.50 �0.30 to 1.29
CD45�/34�/CXCR4� �0.09 �0.25 to 0.8
CD45�/34�/31� 0.01 �0.04 to 0.07
CD45�/34�/144� �0.03 �0.20 to 0.14
CD45�/34�/VEGF-R� 0.21 �0.22 to 0.63
CD45�/34�/133� 1.23 �0.10 to 2.57
*Type of treatment and total number of CD45�/CD34� are included ascovariates in all models.
Ripa et al Stem Cells in Myocardial Infarction I-27

cantly related to long time to reperfusion (regression coeffi-cient 43.2, P�0.002).
There were no apparent association between either CD45�/CD34� or CD34� and VEGF-A (supplemental Table II),whereas both cell types were negatively associated withSDF-1 on all 3 days in the G-CSF group. Only CD34�
seemed to be negatively associated with SDF-1 in the placebogroup, whereas CD45�/CD34� was not.
Neither SDF-1 nor VEGF-A concentrations in the weekafter the STEMI predicted the recovery of ejection fraction(Figure 5). In addition, there was no demonstrable associationbetween leukocyte concentration and recovery of ejectionfraction (P�0.4).
DiscussionThis trial demonstrated that G-CSF treatment induced adissociated pattern in circulating CD34� mononuclear cellsand CD45�/CD34� mononuclear cells (mesenchymal) withhigher concentration per leukocyte of CD34�, compared withCD45�/CD34� cells. In addition, treatment with G-CSFcauses a shift in the subtypes of mesenchymal stem cells inthe peripheral blood. Finally, the numbers of circulatingmesenchymal stem cells appeared to predict the change in leftventricular ejection fraction after STEMI.
The initial optimism regarding the application of stem celltherapy to ischemic heart disease after the preclinical andearly clinical studies has been dampened recently by largerclinical trials designed to investigate efficacy. Intracoronaryinfusion of ex vivo purified bone marrow mononuclear cellsmight have effects on left ventricular recovery after STEMI,even though results are still scattered.9,10 G-CSF therapy tomobilize bone marrow stem cells, however, has failed toimprove left ventricular restoration in 3 double-blindplacebo-controlled trials using several end points.1,3,4
It seems paradoxical that in vivo mobilization of bonemarrow–derived cells to the circulation does not result inmyocardial recovery comparable to that achieved by ex vivopurification and subsequent intracoronary infusion of bonemarrow–derived cells. There may be several reasons for this.For example, G-CSF may not mobilize effective cell types.This hypothesis would be difficult to test in humans, how-ever, because (1) the cells infused intracoronary are veryheterogeneous15 and the cell(s) with potential for cardiac
repair have not been established; and (2) G-CSF mobilizationis difficult to asses because the measured concentration ofcirculating stem cells is dependent on both the mobilizationand the homing of cells to the infarcted myocardium. Recentanimal experiments indicate that mesenchymal stem cellsmay be good candidates for cardiac repair,12,16 whereas thehematopoietic cells (CD34�) are less likely to improvecardiac function.17 The information presented here supports adissociated G-CSF mobilization of CD34� cells comparedwith mesenchymal stem cells which may indicate a differenttherapeutic potential of G-CSF stem cell mobilization versusintracoronary purified cell infusions.
Furthermore, if cells are not directly responsible for thetreatment effect after intracoronary infusion of bone marrowsolution, but rather it is substances such as paracrine factorssecreted by the cells,18,19 this might also explain some of thedifferences when compared with G-CSF treatment. Also,recent evidence suggests that G-CSF treatment impairs themigratory response to SDF-1 of endothelial progenitor cells.20
It is thus of importance to include measures of functionalcapacities in future cell trials.
The hypothesis of the STEMMI trial was that G-CSFmobilized CD34� or CD45�/CD34� would home to andengraft into infarcted myocardium and participate in neovas-cularization and perhaps cardiomyocyte regeneration. Thisstudy demonstrated that there was no statistical significantassociation with the calculated total number of CD34� cells,and an inverse association with the calculated CD45�/CD34�
cells delivered to the myocardial perfusion during G-CSFtreatment and the subsequent improvement in left ventricularejection fraction. These results may indicate that a lowconcentration of the mesenchymal stem cells in the blood isattributable to engraftment of the cells into the myocardium.Thus, patients with a high inert potential for myocardialhoming of the mesenchymal stem cells after STEMI will havethe highest degree of systolic recovery attributable to theengrafted stem cells. We measured the plasma concentrationof cytokines SDF-1 and VEGF as indicators of inert homingpotential. Neither of these cytokines appeared to influence therecovery of ejection fraction, but a high concentration ofSDF-1 was associated with a low concentration of cellsindicating that SDF-1 may increase homing of the cells.However, plasma concentrations of the cytokines are proba-
Figure 5. Association between changes in left ven-tricular ejection fraction during 6 months and (A)stromal derived factor-1 and (B) vascular endothe-lial growth factor. Regression line with 95% confi-dence interval. *Abscissa in logarithmic scale.
I-28 Circulation September 11, 2007

bly poor indicators of the concentrations within the myocar-dium, but a more precise measurement would require re-peated catheterizations of the patients. Recent evidencesuggest that acute myocardial ischemia does not upregulateSDF-1 gene expression in human heart shortly after ischemiaand reperfusion, whereas VEGF-A gene expression seemedupregulated after reperfusion.21 It would be very interesting tolabel mesenchymal stem cells within the bone marrow, andthen follow their potential engraftment within the myocardi-um during G-CSF treatment.
If mobilization of CD34� cells does not contribute tomyocardial recovery after STEMI, and if circulating CD45�/CD34� cells are not homing but potentially reduce therecovery of the myocardial function, this may also explain theinverse association between circulating mesenchymal stemcells and changes in ventricular function. However, the resultcould also be a random finding, because we could notdemonstrate any correlation to changes in regional systolicfunction, and the calculated total amount of cells duringG-CSF treatment is an estimate of cardiac exposure to stemcells based on several assumptions.
Previously, a study in dogs has indicated that intracoronaryinfusion of mesenchymal stem cells could cause microinfarc-tions, probably attributable to microvascular obstruction bythe cells.22 However, circulating mononuclear cells collectedafter G-CSF treatment and then injected into the infarctrelated coronary artery in patients with STEMI did not resultin any signs of myocardial damage.23 In addition, there wasno biochemical or electrocardiographic evidence of myocar-dial ischemia during the G-CSF treatment in the present trial(data not shown). These issues are of importance consideringseveral ongoing trials with intravenous delivery of mesenchy-mal stem cells in the treatment of STEMI, such as theProvacel Clinical trial (ClinicalTrials.gov: NCT00114452).One study previously observed higher rates of restenosis inpatients treated with G-CSF when injected before primarypercutaneous coronary intervention.24 In contrast, severalrecent clinical trials report occurrences of restenosis withinthe expected range1,3,4,25 and intravascular ultrasound demon-strated no increased neointima formation after G-CSFtreatment.26
A potential limitation of this study is the exploratory natureof the analyses, which warrants for caution in the interpreta-tion. Especially the lack of statistical significant associationbetween CD34� cells and systolic recovery could be attrib-utable to low power. Also, it is important to recognize thatdifferences in patient characteristics (eg, age, level of inflam-mation, infarct mass, and success of revascularization) be-tween patients included in G-CSF trial and patients includedin trials with intracoronary infusion could contribute to thedifferences in results.
Nevertheless, human data regarding stem cell treatment ofischemic heart disease are sparse and potentially clinicallyimportant aspects should be identified for further human orlaboratory exploration. In addition, detailed descriptions ofthe cells used for therapy should be supplied in publishedtrials to promote interstudy comparisons.
The identified dissociated G-CSF mobilization pattern forcirculating CD34� and mesenchymal stem cells might explain
the neutral clinical effect of G-CSF treatment soon after aSTEMI. The inverse association between circulating putativemesenchymal stem cells and subsequent recovery of leftventricular ejection fraction is of potential importance forongoing and future trials with mesenchymal stem cells andshould be investigated further.
Sources of FundingThe STEMMI trial has been funded with grants from the DanishHeart Foundation (No. 0442B18-A1322141); Danish Stem CellResearch Doctoral School; Faculty of Health Sciences, CopenhagenUniversity; Lundbeck Foundation, Raimond og Dagmar Ringgård-Bohn’s Fond; Aase og Ejnar Danielsens Fond; Erik og MarthaScheibels Legat; Fonden af 17.12.1981; and Arvid Nilssons Fond.
DisclosuresNone.
References1. Ripa RS, Jørgensen E, Wang Y, Thune JJ, Nilsson JC, Søndergaard L,
Johnsen HE, Køber L, Grande P, Kastrup J. Stem cell mobilizationinduced by subcutaneous granulocyte-colony stimulating factor toimprove cardiac regeneration after acute ST-elevation myocardialinfarction: result of the double-blind, randomized, placebo-controlledstem cells in myocardial infarction (STEMMI) trial. Circulation. 2006;113:1983–1992.
2. Ripa RS, Wang Y, Jørgensen E, Johnsen HE, Grande P, Kastrup J. Safetyof bone-marrow stem cell mobilisation induced by granulocyte-colonystimulating factor: Clinical 30 days blinded results from the stem cells inmyocardial infarction (STEMMI) trial. Heart Drug. 2005;5:177–182.
3. Zohlnhofer D, Ott I, Mehilli J, Schomig K, Michalk F, Ibrahim T,Meisetschlager G, von Wedel J, Bollwein H, Seyfarth M, Dirschinger J,Schmitt C, Schwaiger M, Kastrati A, Schomig A. Stem cell mobilizationby granulocyte colony-stimulating factor in patients with acute myo-cardial infarction: a randomized controlled trial. JAMA. 2006;295:1003–1010.
4. Engelmann MG, Theiss HD, Hennig-Theiss C, Huber A, WinterspergerBJ, Werle-Ruedinger AE, Schoenberg SO, Steinbeck G, Franz WM.Autologous bone marrow stem cell mobilization induced by granulocytecolony-stimulating factor after subacute ST-segment elevation myo-cardial infarction undergoing late revascularization: final results from theG-CSF-STEMI (Granulocyte Colony-Stimulating Factor ST-SegmentElevation Myocardial Infarction) trial. J Am Coll Cardiol. 2006;48:1712–1721.
5. Harada M, Qin Y, Takano H, Minamino T, Zou Y, Toko H, Ohtsuka M,Matsuura K, Sano M, Nishi J, Iwanaga K, Akazawa H, Kunieda T, ZhuW, Hasegawa H, Kunisada K, Nagai T, Nakaya H, Yamauchi-TakiharaK, Komuro I. G-CSF prevents cardiac remodeling after myocardialinfarction by activating the Jak-Stat pathway in cardiomyocytes. NatMed. 2005;11:305–311.
6. Strauer BE, Brehm M, Zeus T, Kostering M, Hernandez A, Sorg RV,Kogler G, Wernet P. Repair of infarcted myocardium by autologousintracoronary mononuclear bone marrow cell transplantation in humans.Circulation. 2002;106:1913–1918.
7. Wollert KC, Meyer GP, Lotz J, Ringes-Lichtenberg S, Lippolt P, Bre-idenbach C, Fichtner S, Korte T, Hornig B, Messinger D, Arseniev L,Hertenstein B, Ganser A, Drexler H. Intracoronary autologous bone-marrow cell transfer after myocardial infarction: the BOOST randomisedcontrolled clinical trial. Lancet. 2004;364:141–148.
8. Lunde K, Solheim S, Aakhus S, Arnesen H, Abdelnoor M, Egeland T,Endresen K, Ilebekk A, Mangschau A, Fjeld JG, Smith HJ, Taraldsrud E,Grogaard HK, Bjornerheim R, Brekke M, Muller C, Hopp E, RagnarssonA, Brinchmann JE, Forfang K. Intracoronary injection of mononuclearbone marrow cells in acute myocardial infarction. N Engl J Med. 2006;355:1199–1209.
9. Schachinger V, Erbs S, Elsasser A, Haberbosch W, Hambrecht R, Hol-schermann H, Yu J, Corti R, Mathey DG, Hamm CW, Suselbeck T,Assmus B, Tonn T, Dimmeler S, Zeiher AM. Intracoronary bone marrow-derived progenitor cells in acute myocardial infarction. N Engl J Med.2006;355:1210–1221.
Ripa et al Stem Cells in Myocardial Infarction I-29

10. Janssens S, Dubois C, Bogaert J, Theunissen K, Deroose C, Desmet W,Kalantzi M, Herbots L, Sinnaeve P, Dens J, Maertens J, Rademakers F,Dymarkowski S, Gheysens O, Van Cleemput J, Bormans G, Nuyts J,Belmans A, Mortelmans L, Boogaerts M, Van de WF. Autologous bonemarrow-derived stem-cell transfer in patients with ST-segment elevationmyocardial infarction: double-blind, randomised controlled trial. Lancet.2006;367:113–121.
11. Anderlini P, Donato M, Chan KW, Huh YO, Gee AP, Lauppe MJ,Champlin RE, Korbling M. Allogeneic blood progenitor cell collection innormal donors after mobilization with filgrastim: the M.D. AndersonCancer Center experience. Transfusion. 1999;39:555–560.
12. Amado LC, Saliaris AP, Schuleri KH, St JM, Xie JS, Cattaneo S, DurandDJ, Fitton T, Kuang JQ, Stewart G, Lehrke S, Baumgartner WW, MartinBJ, Heldman AW, Hare JM. Cardiac repair with intramyocardial injectionof allogeneic mesenchymal stem cells after myocardial infarction. ProcNatl Acad Sci U S A. 2005;102:11474–11479.
13. Mancuso P, Burlini A, Pruneri G, Goldhirsch A, Martinelli G, BertoliniF. Resting and activated endothelial cells are increased in the peripheralblood of cancer patients. Blood. 2001;97:3658–3661.
14. Wang Y, Johnsen HE, Mortensen S, Bindslev L, Ripa RS, Haack-Sørensen M, Jørgensen E, Fang W, Kastrup J. Changes in circulatingmesenchymal stem cells, stem cell homing factor, and vascular growthfactors in patients with acute ST elevation myocardial infarction treatedwith primary percutaneous coronary intervention. Heart. 2006;92:768–774.
15. Perin EC, Dohmann HF, Borojevic R, Silva SA, Sousa AL, Mesquita CT,Rossi MI, Carvalho AC, Dutra HS, Dohmann HJ, Silva GV, Belem L,Vivacqua R, Rangel FO, Esporcatte R, Geng YJ, Vaughn WK, Assad JA,Mesquita ET, Willerson JT. Transendocardial, autologous bone marrowcell transplantation for severe, chronic ischemic heart failure. Circulation.2003;107:2294–2302.
16. Miyahara Y, Nagaya N, Kataoka M, Yanagawa B, Tanaka K, Hao H,Ishino K, Ishida H, Shimizu T, Kangawa K, Sano S, Okano T, KitamuraS, Mori H. Monolayered mesenchymal stem cells repair scarred myocar-dium after myocardial infarction. Nat Med. 2006;12:459–465.
17. Murry CE, Soonpaa MH, Reinecke H, Nakajima H, Nakajima HO, RubartM, Pasumarthi KB, Virag JI, Bartelmez SH, Poppa V, Bradford G,Dowell JD, Williams DA, Field LJ. Haematopoietic stem cells do nottransdifferentiate into cardiac myocytes in myocardial infarcts. Nature.2004;428:664–668.
18. Dimmeler S, Zeiher AM, Schneider MD. Unchain my heart: the scientificfoundations of cardiac repair. J Clin Invest. 2005;115:572–583.
19. Kinnaird T, Stabile E, Burnett MS, Shou M, Lee CW, Barr S, Fuchs S,Epstein SE. Local delivery of marrow-derived stromal cells augmentscollateral perfusion through paracrine mechanisms. Circulation. 2004;109:1543–1549.
20. Honold J, Lehmann R, Heeschen C, Walter DH, Assmus B, Sasaki K,Martin H, Haendeler J, Zeiher AM, Dimmeler S. Effects of granulocytecolony simulating factor on functional activities of endothelial progenitorcells in patients with chronic ischemic heart disease. Arterioscler ThrombVasc Biol. 2006;26:2238–2243.
21. Wang Y, Gabrielsen A, Lawler PR, Paulsson-Berne G, Steinbruchel DA,Hansson GK, Kastrup J. Myocardial gene expression of angiogenicfactors in human chronic ischemic myocardium: influence of acute is-chemia/cardioplegia and reperfusion. Microcirculation. 2006;13:187–197.
22. Vulliet PR, Greeley M, Halloran SM, MacDonald KA, Kittleson MD.Intra-coronary arterial injection of mesenchymal stromal cells and micro-infarction in dogs. Lancet. 2004;363:783–784.
23. Kang HJ, Lee HY, Na SH, Chang SA, Park KW, Kim HK, Kim SY,Chang HJ, Lee W, Kang WJ, Koo BK, Kim YJ, Lee DS, Sohn DW, HanKS, Oh BH, Park YB, Kim HS. Differential effect of intracoronaryinfusion of mobilized peripheral blood stem cells by granulocyte colony-stimulating factor on left ventricular function and remodeling in patientswith acute myocardial infarction versus old myocardial infarction: theMAGIC Cell-3-DES randomized, controlled trial. Circulation. 2006;114:I145–I151.
24. Kang HJ, Kim HS, Zhang SY, Park KW, Cho HJ, Koo BK, Kim YJ, SooLD, Sohn DW, Han KS, Oh BH, Lee MM, Park YB. Effects of intra-coronary infusion of peripheral blood stem-cells mobilised withgranulocyte-colony stimulating factor on left ventricular systolic functionand restenosis after coronary stenting in myocardial infarction: theMAGIC cell randomised clinical trial. Lancet. 2004;363:751–756.
25. Ince H, Petzsch M, Kleine HD, Schmidt H, Rehders T, Korber T,Schumichen C, Freund M, Nienaber CA. Preservation from left ventric-ular remodeling by front-integrated revascularization and stem cell lib-eration in evolving acute myocardial infarction by use of granulocyte-colony-stimulating factor (FIRSTLINE-AMI). Circulation. 2005;112:3097–3106.
26. Jørgensen E, Ripa RS, Helqvist S, Wang Y, Johnsen HE, Grande P,Kastrup J. In-stent neo-intimal hyperplasia after stem cell mobilization bygranulocyte-colony stimulating factor Preliminary intracoronaryultrasound results from a double-blind randomized placebo-controlledstudy of patients treated with percutaneous coronary intervention forST-elevation myocardial infarction (STEMMI Trial). Int J Cardiol. 2006;111:174–177.
I-30 Circulation September 11, 2007

Circulation. 2007;116[suppl I]:I-24-I-30
Data Supplement Figure
Legend: Individual time course of SDF-1 (upper panel) and VEGF-A (lower panel). Bold line indicate mean and standard deviation. Ordinate in logarithmic scale. Data Supplement Table 1. G-CSF induced cell mobilization* Placebo
(N=33) G-CSF (N=37)
P
CD34+, /µl Baseline 3.9±1.7 [1-9] 3.6±2.1 [0-9] Day 4 4.0±2.1 [2-12] 34.2±23.7 [4-105] Day 7 3.7±1.6 [2-8] 55.1±53.3 [6-259] Day 28 3.1±1.9 [0-8] 2.5±1.4 [0-7]
<0.001
CD45-/CD34-, /µl Baseline 246±164 [28-963] 253±205 [28-963] Day 4 229±174 [49-828] 587±480 [150-2196] Day 7 260±202 [58-770] 1015±1114 [68-4805] Day 28 183±134 [43-601] 169±137 [20-620]
<0.001
Data are mean values±SD [range], statistical comparison by repeated measures ANOVA after logarithmic transformation. *Data are previously published in Ripa et al. Circulation 2006;113:1983-1992 Data Supplement Table 2. Linear regression between cell cytokine concentrations. CD34+ CD45-/CD34-
Regression coefficient (95% CI) Regression coefficient (95% CI) VEGF-A Baseline 83 (47 to 120)* 0.1 (-0.1 to 0.4) Day 4 0.9 (-2.6 to 4.4) 1.0 (0.5 to 1.5)* Day 7 0.05 (-1.4 to 1.5) 0.02 (-0.05 to 0.09) SDF-1 Baseline -81 (-134 to -29) -0.7 (-1.3 to -0.2) Day 4 -6 (-12 to -0.4) 0.8 (-0.09 to 1.6)* Day 7 -4 (-7 to -1) 0.8 (0 to 1.6)* * Significant interaction with treatment group, indicating a statistical significant difference in association between cells and cytokines in the two groups.

Short- and long-term changes in myocardial function,morphology, edema, and infarct mass afterST-segment elevation myocardial infarction evaluatedby serial magnetic resonance imagingRasmus Sejersten Ripa, MD,a, b Jens Christian Nilsson, MD, PhD,c Yongzhong Wang, MD, PhD,a
Lars Søndergaard, MD, DMSc,a Erik Jørgensen, MD, FESC,a and Jens Kastrup, MD, DMSc, FESCa
Copenhagen and Hvidovre, Denmark
Background Knowledge of the natural course after an ST-elevation myocardial infarction (STEMI) treated according toguidelines is limited because comprehensive serial magnetic resonance imaging (MRI) of systolic left ventricular function,edema, perfusion, and infarct size after STEMI has not been undertaken. The aim of this study was to evaluate effects of therapyfor STEMI on left ventricular function and perfusion and to test the hypothesis that myocardial perfusion by MRI predictsrecovery of left ventricular function.
Methods Cine MRI, edema, first-pass perfusion, and late enhancement imaging were performed in 58 patients at day2 and at 1 and 6 months after successful primary percutaneous coronary stent intervention for STEMI.
Results Ejection fraction increased 6.3% during the first month (P b .001) and 1.9% from 1 to 6 months (P b .06),indicating a maximal recovery very early after the infarction. The systolic wall thickening in the infarct area almost doubled(P b .001), the perfusion of infarcted myocardium increased approximately 50% (P = .02), and perfusion improved in 72% ofpatients. Edema decreased with a mean of 2 segments (P b .001) during the first month and another 2.5 segments from1 to 6 months (P b .001). Infarct size decreased to 1 month (P = .01) and was unchanged from 1 to 6 months (P = .5). Baselineperfusion did not predict improvement in ejection fraction (r = 0.2, P = .2) but did predict regional systolic function (P = .03).
Conclusions Left ventricular function, perfusion, and infarct mass recovered substantially after STEMI, with the main partof the change within the first month. First-pass perfusion at rest appeared to predict regional ventricular recovery. (Am Heart J2007;154:929-36.)
Acute percutaneous coronary stent intervention (PCI)is the method of choice to treat patients with acuteST-elevation myocardial infarction (STEMI). However,although normal epicardial blood flow is reestablishedwithin hours after onset of symptoms, transient and
permanent myocardial damage is usually unavoidable andmay result in impaired cardiac function and eventuallyheart failure due to adverse left ventricular remodeling.Several authors 1-6 have shown that cardiac magnetic
resonance imaging (MRI) allows for analysis of leftventricular recovery, but information using different MRIimaging modalities at several time points is very limited.Magnetic resonance imaging measures are often used asend points in clinical trials of ischemic heart disease dueto high accuracy and precision and low risk, allowing forinclusion of a minimum of patients. 7 However, severalearly human trials after STEMI have used MRI results asend points without including a control or placebo group.This constitutes a potential bias because a comprehen-sive analysis of systolic left ventricular function, edema,perfusion, and infarct mass after STEMI using serial MRIhas not been undertaken and the knowledge of thenatural course of these variables after a STEMI treatedaccording to guidelines is thus limited. In addition, inmost previous studies, baseline MRI is performed around
From the Departments of aCardiology, The Heart Centre, and bRadiology, UniversityHospital Rigshospitalet, Copenhagen, Denmark, and cDanish Research Centre forMagnetic Resonance, University Hospital Hvidovre, Hvidovre, Denmark.The STEMMI trial has been funded with grants from the Danish Heart Foundation (no.0442B18-A1322141); Danish Stem Cell Research Doctoral School; Faculty of HealthSciences, Copenhagen University; Lundbeck Foundation; Raimond og Dagmar Ringgård-Bohn's Fond; Aase og Ejnar Danielsens Fond; Erik og Martha Scheibels Legat; Fonden af17.12.1981; and Arvid Nilssons Fond.Submitted March 29, 2007; accepted June 27, 2007.Reprint requests: Jens Kastrup MD, DMSc, Department of Cardiology 2014, The HeartCentre, University Hospital Rigshospitalet, DK-2100 Copenhagen Ø, Denmark.E-mail: [email protected]/$ - see front matter© 2007, Mosby, Inc. All rights reserved.doi:10.1016/j.ahj.2007.06.038

a week after the acute event 1-6 and thereby potentiallyintroducing important bias due to recovery of hibernat-ing myocardium.The objective of this study was (1) to investigate the
short-term and long-term effects of current guidelinetreatment of STEMI, including successful primary PCI interms of left ventricular function, morphology, edema,and perfusion using cardiac MRI and (2) to test thehypothesis that measures of myocardial perfusion byMRI shortly after STEMI predicts recovery of leftventricular function.
MethodsPatient populationWe included all patients from the Stem Cells in Myocardial
Infarction (STEMMI) trial, 8 with a baseline and at least 1 follow-up MRI examination. Detailed inclusion criteria of the STEMMItrial have been published previously 8; briefly, patients with agesbetween 20 and 70, who had been treated successfully withprimary PCI within 12 hours after the onset of symptoms, wereincluded in the study. The culprit lesion was located in theproximal section of a large coronary artery branch, and plasmacreatine kinase myocardial band was greater than 100 μg/L. Theexclusion criteria included prior myocardial infarction, signifi-cant stenosis in a nonculprit coronary vessel, ventriculararrhythmia after PCI requiring treatment, pregnancy, unpro-tected left main stem lesion, diagnosed or suspected cancer,New York Heart Association functional class 3-4 heart failuresymptoms, or known severe claustrophobia.The study was approved by the local ethical committee (KF
01-239/02) and the Danish Medicines Agency (2612-2225). Thestudy has been registered in clinicaltrials.gov (NCT00135928).All patients received oral and written information about thestudy and signed the consent before inclusion in the study.
Study designThe main STEMMI trial was a prospective, double-blind,
randomized, placebo-controlled study allocating patients withacute STEMI in a 1:1 ratio after the primary PCI to medicaltreatment with granulocyte colony-stimulating factor (G-CSF) orplacebo as a supplement to treatment according to guidelines. 9
However, G-CSF did not affect any of the end points examined inthe STEMMI trial, a result confirmed by other very similarstudies. 10,11 The present observational MRI study investigatesthe course of cardiac volumes and function up to 6 months afteran acute STEMI successfully reperfused with primary PCI. Acoronary angiogram was performed 1 month before the6-month follow-up examination, and significant restenoses weretreated with intracoronary stenting to achieve optimal epicardialflow during the MRI examinations.
Cardiac MRI protocolMagnetic resonance imaging was performed as soon as
possible after inclusion and 1 and 6 months after inclusion.Patients were examined, with care taken to ensure identical coilposition at all 3 examinations. All images were acquired usingelectrocardiographic gating and breath-hold technique with a1.5-T clinical scanner (Siemens Vision Magnetom, Siemens AG,Erlangen, Germany) and a standard phased array chest coil. The
imaging protocol was identical at all 3 time points and consistedof 4 parts:
1. For myocardial volumes, cine true short axis imagesencompassing the entire left ventricle were acquired usinga cinematographic gradient echo pulse sequence with atemporal resolution of 50 milliseconds. Slice thickness was8 mm with 2-mm interslice gaps.
2. Images for visualizing myocardial edema covered theentire left ventricle using the same views as those usedfor cine MRI. The images were acquired in the diastoleusing a T2-weighted short-inversion-time, inversion-recovery (STIR) breath-hold MRI pulse sequence withsegmented data acquisition.
3. One short axis view was chosen for perfusion imagingbecause 1 slice would cover infarcted, noninfarcted, andborder zone myocardium. The location of the slice wasin the middle of the infarct area as defined by cine andSTIR MRI. The identical anatomical position was used atthe follow-up examinations. A bolus of gadopentetatedimeglumine (Magnevist, Schering), 0.1 mmol/kg ofbodyweight, was injected over 5 seconds and flushedwith normal saline for 10 seconds using an automatedsyringe. Forty images were acquired with 1 image perheartbeat using an inversion-recovery turbo fast low-angle shot pulse sequence.
4. Another bolus of 0.05 mmol/kg gadopentetate dimeglu-mine was injected immediately after the perfusion scan(without scanning), adding up to a total of 0.15 mmol/kggadopentetate dimeglumine for late enhancement ima-ging. After 15 minutes, the inversion time was again set tonull normal myocardium using a segmented inversion-recovery turbo fast low-angle shot pulse sequence. Usingthis inversion time, the total infarct area was covered withconsecutive short axis slices.
Magnetic resonance imaging analysesThe independent core laboratory (Bio-Imaging Technologies
B.V., Leiden, The Netherlands) analyzed all examinations, exceptthe STIR images, using the MRI-MASS v6.1 (MEDIS MedicalImaging Systems, Leiden, The Netherlands). The core laboratorywas blinded to all patients' data and to the order of the follow-upexaminations. The analyses of cardiac MRI have a lowinterobserver variability (3%-6%); to reduce this variability evenmore, each analysis was quality-controlled by a second blindedMRI technician before final approval. Left ventricular end-diastolic volumes, end-systolic volumes, and myocardial masswere automatically calculated by the software. Regional leftventricular function was assessed by systolic wall thickening(SWT) in the infarct region, the border region, and normalmyocardium by the centerline method. The position of the3 regions was determined using the baseline contrast-enhancedimages, where areas adjacent to the region with delayedcontrast enhancement were defined as the border regions.Relative SWTwas calculated as the difference between diastolicand systolic divided by the diastolic wall thickness.Myocardial perfusion was assessed in the middle of the infarct
and in the border area of the infarct as the change in MRI signalintensity as a function of time during the first pass (initialslope). 12 The assessments were normalized by the initial slopein normal noninfarcted myocardium.
930 Ripa et alAmerican Heart Journal
November 2007

Infarct mass was quantified planimetrically by outlining thelate enhanced area and using a density factor of 1.05 g/cm3.The average value of the signal intensity of the left ventricleblood pool in all slices was used as starting point for thethreshold, the next step involved the fine-tuning of thethreshold by manually adapting it (max. 10% below or abovethe calculated threshold) until the outlined region matchedthe late enhanced area as identified by visual assessment. Ablack area in the center of the enhanced region at the baselineimaging was defined as microvascular obstruction.Myocardial edema was assessed independently by 2 investi-
gators (R.S.R., J.C.N.) blinded to all patient data and timesequence of the examinations using the 17-segment model ofthe left ventricle. Each segment was semiquantitatively assigneda score of 0 (total absence of edema) or 1 (presence of edema).The segment scores for the entire left ventricle were finallysummated. Interobserver disagreement in the score of a singlesegment in an examination was adjudicated by taking the meanof the 2 final scores. All other interobserver disagreements weresolved by adjudication after review of the examination. The2 observers reached exact agreement in 89% of the segmentswith a κ of 0.78 (good strength of agreement).
StatisticsAll data regardless of treatment with G-CSF or placebo were
pooled because we8 and others 10,11 have found no effect ofG-CSF on the tested variables. However, the treatment group(G-CSF or placebo) was entered as covariate in all regression andanalysis of variance models to account for any minor differencebetween the groups. This covariate was not significantly relatedto any of the outcomes.Data are given as mean ± SD unless otherwise stated. The
effects of time were analyzed in a repeated measures analysis ofvariance model. Post hoc analyses of change from baseline to1 month and from 1 month to 6 months were performed usingpaired sample t test without correction for 2 comparisons.Associations between functional data were described usinglinear regression analysis and Pearson correlation coefficient. Allavailable results were included in analyses (eg, if a patientrefused MRI at 6 months, then only baseline and 1 month resultswere included in analyses).Analyses were performed with SPSS (version 12.0,
SPSS Inc, Chicago, IL). The level of statistical significancewas set at P b .05.
ResultsFifty-eight patients went through a baseline and at least
1 follow-up MRI examination and were included in this
study, 55 (95%) of these patients had all 3 examinations(3 patients refused MRI follow-up at 6 months). Therewere 5% to 15% of the data points missing (except forinfarct mass at baseline) (Table I). Approximately 50% ofthese were rejected by the core laboratory due to poorquality (eg, massive breathing artifacts or wrong electro-cardiographic triggering), and a part of the MRI exam-ination was not performed in the remaining cases (eg, dueto severe patient discomfort or technical problems duringthe scanning). The perfusion part of the scanning requiredlonger breath-hold and was performed late in theexamination, thus more perfusion examinations wererejected or not performed (Table I). A substantial part ofthe baseline infarct mass results were missing (Table I).The first 6 patients included did not have baseline infarctmass results because they by mistake were scanned usinga nonsegmented scanner pulse sequence, and the next 10patients were rejected for analysis by the core laboratory
Table I. Magnetic resonance imaging results included inanalyses
Volumes(cine) Edema
Infarctmass Perfusion
Results frombaseline
57 (98) 54 (93) 38 (66) 51 (88)
Results from 1 mo 54 (93) 53 (91) 49 (84) 50 (86)Results from 6 mo 55 (95) 51 (88) 50 (86) 49 (84)
Data are n (% of included patients [N = 58]).
Table II. Patient characteristics
N = 58
Age (y) 56.3 ± 8.7Male sex 47 (81)Body mass index (kg/m2) 27.6 ± 3.7Current smoker 39 (67)Diabetes mellitus 6 (10)Known hypertension 17 (29)Family history of ischemic heart disease 25 (43)Median time (h) from symptomdebut to primary PCI (quartiles)
4:19 (3:23-6:25)
Index infarct-related arteryLAD 25 (43)LCX 7 (12)RCA 26 (45)
TIMI flow grade 0 or 1 before primary PCI 50 (86)TIMI flow grade 3 after primary PCI 56 (97)Type of stentNo stent 2 (3)Bare metal 38 (66)Drug eluting 18 (31)
Platelet glycoprotein IIb/IIIa inhibitors 24 (41)Median maximum serum CKMBconcentration (μg/L) (quartiles)*
284 (159-426)
Treated with G-CSF 29 (50)Discharge medicationAspirin 58 (100)Clopidogrel 57 (98)β-Blocker 49 (85)Statin 58 (100)Angiotensin-converting enzyme inhibitor 29 (50)
Medication at 6 monthsy follow-upAspirin 56 (98)Clopidogrel 56 (98)β-Blocker 47 (83)Statin 56 (98)Angiotensin-converting enzyme inhibitor 38 (67)
Data are mean values ± SD or n (%) unless otherwise stated. CKMB, Creatine kinasemyocardial band; LAD, left anterior descending artery; LCX, left circumflex artery;RCA, right coronary artery.*Normal upper limit = 5.yOne patient died before follow-up.
Ripa et al 931American Heart JournalVolume 154, Number 5

due to poor image quality. The baseline MRI examinationwas performed early at a median of 51 hours (interquartilerange, 26-58) after the primary PCI.The clinical and angiographic characteristics of the
study population are shown in Table II. Patientsreceived medical treatment in accordance with guide-lines in the follow-up period. 13 Angiotensin-convertingenzyme inhibitors were administered if the patient hadejection fraction below 0.40 on an echocardiogram,clinical symptoms of heart failure, or high risk of newischemic event (eg, diabetes, hypertension, and per-ipheral artery disease).
Global volumesThe individual time courses of left ventricular ejection
fraction are shown in Figure 1. We found a highlysignificant increase in ejection fraction during the 6monthsafter an acutely reperfused STEMI (P b .001). This covers amean increase of 6.3 percentage points during the firstmonth (95% confidence interval [CI] 3.4-9.2,P b .001) and atrend toward a small increase of 1.9 percentage points from1 to 6 months (95% CI −0.1 to 3.9, P b .06), indicating amaximal recovery very early after the infarction. Therecovery was not statistically significantly affected by theuse of angiotensin-converting enzyme inhibitor (P = .7).The mean values of end-diastolic volume, end-systolicvolume, and mass are shown in Table III. It is evident thatthe primary change occurs within the first month after theinfarction and that the observed increase in ejectionfraction is caused by both an increase in end-diastolicvolume and a decrease in the end-systolic volume.
Regional left ventricular functionThe SWT was measured in the center of the infarct, in
the border zone of the infarct, and in the noninfarcted(normal) myocardium. Mean data are shown in Table IV,and again it is apparent that the main change occurswithin the first month and primarily in the infarcted area,whereas the increase in the noninfarcted myocardiumonly barely reaches statistical significance.
Myocardial edemaAll patients had at least 3 segments with myocardial
edema at baseline MRI (mean 9.3 ± 2.6 segments), andonly 3 patients (6%) were without any edema 6 monthsafter the infarction. The amount of edema decreasedsignificantly over time (Figure 2) (P b .001) with a meandecrease of 2 segments (95% CI of difference 1.1-2.8, P b.001) during the first month and another 2.5 segmentsfrom 1 to 6 months (95% CI of difference 1.6-3.4, P b.001). There was no association between the initialamount of myocardial edema and the subsequentincrease in ejection fraction.
Infarct massInfarct mass was assessed by late enhancement
imaging. Central microvascular obstruction on lateenhancement images was present at the baselineexamination in 16 (42%) patients. We observed asignificant decrease in infarct mass from baseline (13.2 ±10.9 g) to 1 month (95% CI of difference −0.8 to −6.0 g,P = .01) and unchanged mass from 1 month (11.4 ± 9.4 g)to 6 months (95% CI of difference 2.1 to −1.0 g, P = .5).We found a very close correlation (r = 0.9) between the
logarithmic transformed initial and final infarct mass, withan approximately 30% reduction in infarct mass from
Figure 1
Change in ejection fraction. Bold line indicates mean ± SE.
Table III. Change over time in left ventricular morphology,function, and left ventricular mass1
Baseline,mean(SD)
1 mo,mean(SD)
6 mo,mean(SD) P*
Changefrom
baselineto 6 mo,mean (SE)
Enddiastolicvolume(mL)
128 (35) 142 (38) 140 (35) b.001 11.1 (3.5)
Endsystolicvolume(mL)
63 (34) 60 (33) 57 (30) .03 −6.7 (3.1)
LV mass(g)
184 (43) 173 (39) 173 (40) .002 −12.6 (3.2)
Ejectionfraction(%)
52.9 (13.4) 59.4 (12.7) 61.0 (11.9) b.001 8.3 (1.4)
LV, Left ventricle.*Repeated measures analysis of variance.
932 Ripa et alAmerican Heart Journal
November 2007

baseline to 6 months follow-up (Figure 3). In addition, theinitial infarct mass predicted the ejection fraction after6 months (r = 0.67, P b .001).
Myocardial perfusionThe perfusion improved from baseline to 6 months
follow-up in 72% of the patients. We found a meanincrease of 28 percentage points (95% CI 15-41, P b .001)in the infarcted area and of 18 percentage points (95% CI8-28, P = .001) in the border zone of the infarct. Theobserved increase in perfusion occurred primarily in thefirst month (Table IV).Surprisingly, we found no correlation (P = .3) between
the baseline perfusion measured with first-pass perfusionand the amount of initial central microvascular obstruc-tion as determined with late enhancement MRI. Inaddition, baseline perfusion in the infarct area did notpredict the improvement in ejection fraction (r = 0.2,P = .2). However, there was a trend toward improvedrecovery of SWT in patients without baseline micro-vascular obstruction as determined with late enhance-ment MRI compared with patients with microvascularobstruction (19.8 ± 28.3 vs 8.1 ± 21.3, P = .2). This waseven more evident when comparing the baseline perfu-sion of the infarcted area with the recovery of SWT(Figure 4, A). This association was primarily driven by avery low recovery of SWT in patients in the quartile withthe poorest baseline perfusion (Figure 4, B).
DiscussionThe results of this trial represent a comprehensive MRI
description of the “natural course” of left ventricularmyocardial recovery after a STEMI reperfused by primaryPCI within 12 hours using 4 MRI imaging modalities at3 time points with a very early baseline measurement.The following are the main findings: (1) substantialrecovery of all investigated variables; (2) the main part ofthe changes occurs within the first month after thereperfusion; and (3) impaired perfusion very early after
the STEMI seems to predict subsequent low improvementin regional myocardial function.The population in this trial is homogenous but with
some differences that could potentially influence theresult (eg, culprit artery, thrombosis in myocardialinfarction flow grade before PCI, and time to PCI). Thistrial do not have statistical power to properly control forthese factors; however, they were tried to be minimizedby only including patients with proximal coronary lesionsand enzyme rise indicative of larger infarctions.The MRI modality is especially appealing for repeated
measurements because of lack of radiation exposure to thepatient. In addition, the high spatial resolutions allow for
Table IV. Change over time in systolic wall thickening and perfusion
Baseline,mean (SD)
1 mo,mean (SD)
6 mo,mean (SD) P*
Change frombaseline to
6 mo, mean (SE)
SWTyInfarcted myocardium 19.5 (16.1) 35.4 (30.8) 35.1 (27.8) b.001 16.8 (3.7)Border myocardium 24.8 (17.5) 37.3 (24.6) 39.8 (26.4) b.001 15.8 (3.3)Normal myocardium 47.2 (32.9) 58.2 (36.9) 56.3 (42.1) .04 9.0 (4.9)PerfusionzInfarcted myocardium 53.4 (39.5) 82.7 (46.2) 79.6 (44.4) .02 27.8 (6.5)Border myocardium 74.6 (32.1) 90.5 (35.3) 91.8 (33.9) .04 18.0 (5.6)
*Repeated measures analysis of variance.yIn percentage of the diastolic wall thickness.zIn percentage of perfusion in noninfarcted myocardium.
Figure 2
Change in segments with myocardial edema. Bold line indicatesmean ± SE.
Ripa et al 933American Heart JournalVolume 154, Number 5

precise and accurate measurement of regional morphol-ogy, function, and perfusion compared with other imagingmodalities such as echocardiography and nuclear imaging.The drawbacks are primarily the low temporal resolutionas well as low accessibility in many countries. The presentMRI results are in good agreement with previous findingsusing other imaging modalities, but MRI has a betterprecision and accuracy. Magnetic resonance imaging–derivedmeasures have been used for end point assessmentin several recent clinical trials of stem cell therapy for acuteand chronic ischemic heart disease. 14,15
Left ventricular remodeling and infarct healing havebeen studied extensively with echocardiography andnuclear imaging. More recently, MRI 4,16,17 and compu-terized tomography18 have offered a wide range of high-resolution imaging modalities. However, in using MRI-derived end points, it is important to acknowledge(especially in early trials without randomized controlgroups) the limited knowledge of the natural course ofmyocardial recovery after a reperfused acute myocardialinfarction. A striking example is the use of G-CSF after anacute myocardial infarction. Several early trials reportedvery positive results, 19,20 whereas 2 trials designed to testefficacy were neutral because the recovery in the placebogroup was substantial. 8,11
Most trials with stem cell therapy for ishemic heartdisease have used global or regional systolic function asend points. In our trial, myocardial perfusion wasadditionally assessed because poor microvascular perfu-sion is related to worse outcome21 and neoangiogenesis
is a proposed mechanism of stem cell therapy. We thushypothesized that baseline perfusion would predict theextent of systolic recovery. First-pass perfusion at rest byMRI was used to assess change in regional microvascularperfusion as previously described. 22 This method is notwidely validated (eg, it can be speculated if thereplacement of dead tissue with fibrous tissue in theinfarct area may lead to a change in paramagnetizationcharacteristics); however, we and others 1 found a strong
Figure 3
Change in infarct mass on double logarithmic scale. Regression line:(mass at 6 months) = 1.3 × (mass at baseline) 0.8.
Figure 4
Association between baseline perfusion in infarcted myocardium andchange in regional systolic function. P value is corrected for G-CSF orplacebo treatment. A, Regression line with 95% CI. B, Mean ± SE.
934 Ripa et alAmerican Heart Journal
November 2007

correlation between the baseline perfusion and subse-quent recovery of regional left ventricular function. At thesame time though, baseline perfusion did not predict therecovery of global systolic function (ejection fraction). Inaddition, we found postinfarction myocardial edemapresent for a prolonged period in most of the patients aspreviously shown by others. 23 The enhanced area on theSTIR images has in some trials been suggested as“myocardium at risk.” This is an interesting idea becausethis would allow for calculation of potential myocardialsalvage with MRI; however, the method needs validation.The present results could serve as preliminary data for
designing future drug-related interventional trials or evenas “controls” in the interpretation of future trials withouta control group. It is thus remarkable that left ventricularejection fraction increased with more that 8 percentagepoints, the SWT in the infarct area almost doubled, andthe perfusion of the infarcted myocardium increased withapproximately 50%. Thus, the effects of primary PCI,pharmacological therapy, and “nature” are substantial andimportant to recognize. In addition, we observed analmost 30% shrinkage of the infarct mass, a result verysimilar to the recent results of others. 2,24 Anotheressential observation is the fact that the changes almostexclusively occurred within the first month after theinfarction. Thus, baseline examinations should be per-formed as soon as possible after the STEMI to observethese changes.The inherent limitation of this study design is the
3 time points used for MRI imaging, which do notallow to draw firm conclusions about the precisetiming of the changes observed or if further changeoccurs after 6 months. The results were potentiallybiased by the missing data points especially theinfarct masses; however, the missing data pointsseemed to be randomly distributed between thepatients, and statistical analyses were based onrepeated measures where most of the patients had atleast 2 data points.These results are also of interest when assessing patients
in daily clinical practice. However, it is important to havein mind that these objective measures do not necessarilycorrelate with the subjective symptoms of the patients.
We appreciate the help from Professor C. Thomsen
and staff at the Section of Magnetic Resonance Imaging,
Rigshospitalet, Denmark.
References1. Baks T, van Geuns RJ, Biagini E, et al. Recovery of left ventricular
function after primary angioplasty for acute myocardial infarction.Eur Heart J 2005;26:1070-7.
2. Baks T, van Geuns RJ, Biagini E, et al. Effects of primary angioplastyfor acute myocardial infarction on early and late infarct size andleft ventricular wall characteristics. J Am Coll Cardiol 2006;47:40-4.
3. Petersen SE, Voigtlander T, Kreitner KF, et al. Late improvement ofregional wall motion after the subacute phase of myocardialinfarction treated by acute PTCA in a 6-month follow-up.J Cardiovasc Magn Reson 2003;5:487-95.
4. Schroeder AP, Houlind K, Pedersen EM, et al. Serial magneticresonance imaging of global and regional left ventricular remodelingduring 1 year after acute myocardial infarction. Cardiology2001;96:106-14.
5. Konermann M, Sanner BM, Horstmann E, et al. Changes of the leftventricle after myocardial infarction—estimation with cine magneticresonance imaging during the first six months. Clin Cardiol1997;20:201-12.
6. Bellenger NG, Swinburn JM, Rajappan K, et al. Cardiac remodellingin the era of aggressive medical therapy: does it still exist? Int JCardiol 2002;83:217-25.
7. Bellenger NG, Davies LC, Francis JM, et al. Reduction in samplesize for studies of remodeling in heart failure by the use ofcardiovascular magnetic resonance. J Cardiovasc Magn Reson2000;2:271-8.
8. Ripa RS, Jørgensen E, Wang Y, et al. Stem cell mobilization inducedby subcutaneous granulocyte–colony stimulating factor to improvecardiac regeneration after acute ST-elevation myocardial infarction:result of the double-blind, randomized, placebo-controlled StemCells in Myocardial Infarction (STEMMI) trial. Circulation 2006;113:1983-92.
9. Silber S, Albertsson P, Aviles FF, et al. Guidelines for percutaneouscoronary interventions. The Task Force for Percutaneous CoronaryInterventions of the European Society of Cardiology. Eur Heart J2005;26:804-47.
10. Zohlnhöfer D, Ott I, Mehilli J, et al. Stem cell mobilization bygranulocyte colony-stimulating factor in patients with acute myocar-dial infarction: a randomized controlled trial. JAMA 2006;295:1003-10.
11. Engelmann MG, Theiss HD, Hennig-Theiss C, et al. Autologous bonemarrow stem cell mobilization induced by granulocyte colony-stimulating factor after subacute ST-segment elevation myocardialinfarction undergoing late revascularization: final results from theG-CSF-STEMI (Granulocyte Colony-Stimulating Factor ST-SegmentElevation Myocardial Infarction) trial. J Am Coll Cardiol 2006;48:1712-21.
12. Epstein FH, London JF, Peters DC, et al. Multislice first-pass cardiacperfusion MRI: validation in a model of myocardial infarction. MagnReson Med 2002;47:482-91.
13. Van de Werf F, Ardissino D, Betriu A, et al. Management of acutemyocardial infarction in patients presenting with ST-segment eleva-tion. The Task Force on the Management of Acute MyocardialInfarction of the European Society of Cardiology. Eur Heart J2003;24:28-66.
14. Wollert KC, Meyer GP, Lotz J, et al. Intracoronary autologous bone-marrow cell transfer after myocardial infarction: the BOOSTrandomised controlled clinical trial. Lancet 2004;364:141-8.
15. Ripa RS, Wang Y, Jørgensen E, et al. Intramyocardial injection ofvascular endothelial growth factor-A165 plasmid followed bygranulocyte–colony stimulating factor to induce angiogenesis inpatients with severe chronic ischaemic heart disease. Eur Heart J2006;27:1785-92.
16. Kramer CM, Rogers WJ, Theobald TM, et al. Dissociation betweenchanges in intramyocardial function and left ventricular volumes inthe eight weeks after first anterior myocardial infarction. J Am CollCardiol 1997;30:1625-32.
17. Nilsson JC, Groenning BA, Nielsen G, et al. Left ventricularremodeling in the first year after acute myocardial infarction and the
Ripa et al 935American Heart JournalVolume 154, Number 5

predictive value of N-terminal pro brain natriuretic peptide. Am HeartJ 2002;143:696-702.
18. Mahnken AH, Koos R, Katoh M, et al. Sixteen-slice spiral CT versusMR imaging for the assessment of left ventricular function in acutemyocardial infarction. Eur Radiol 2005;15:714-20.
19. Kuethe F, Figulla HR, Herzau M, et al. Treatment with granulocytecolony-stimulating factor for mobilization of bone marrowcells in patients with acute myocardial infarction. Am Heart J 2005;150:115.
20. Ince H, Petzsch M, Kleine HD, et al. Prevention of left ventricularremodeling with granulocyte colony-stimulating factor after acutemyocardial infarction: final 1-year results of the Front-IntegratedRevascularization and Stem Cell Liberation in Evolving AcuteMyocardial Infarction by Granulocyte Colony-Stimulating Factor(FIRSTLINE-AMI) trial. Circulation 2005;112:I73-80.
21. Wu KC, Zerhouni EA, Judd RM, et al. Prognostic significance ofmicrovascular obstruction by magnetic resonance imaging inpatients with acute myocardial infarction. Circulation1998;97:765-72.
22. Bodi V, Sanchis J, Lopez-Lereu MP, et al. Microvascular perfusion1 week and 6 months after myocardial infarction by first-passperfusion cardiovascular magnetic resonance imaging. Heart 2006;92:1801-7.
23. Nilsson JC, Nielsen G, Groenning BA, et al. Sustained postinfarctionmyocardial oedema in humans visualised by magnetic resonanceimaging. Heart 2001;85:639-42.
24. Hombach V, Grebe O, Merkle N, et al. Sequelae of acute myocardialinfarction regarding cardiac structure and function and theirprognostic significance as assessed by magnetic resonance imaging.Eur Heart J 2005;26:549-57.
936 Ripa et alAmerican Heart Journal
November 2007

ORIGINAL PAPER
Serial in vivo imaging of the porcine heart afterpercutaneous, intramyocardially injected 111In-labeledhuman mesenchymal stromal cells
Stig Lyngbæk • Rasmus S. Ripa • Mandana Haack-Sørensen •
Annette Cortsen • Linda Kragh • Claus B. Andersen • Erik Jørgensen •
Andreas Kjær • Jens Kastrup • Birger Hesse
Received: 23 July 2009 / Accepted: 29 October 2009 / Published online: 18 November 2009
� Springer Science+Business Media, B.V. 2009
Abstract This pilot trial aimed to investigate the
utilization of 111In-labeling of mesenchymal stromal
cells (MSC) for in vivo tracking after intramyocardial
transplantation in a xenotransplantation model with
gender mismatched cells. Human male MSC were
expanded ex vivo and labeled with 111In-tropolone.
Ten female pigs were included. The labeled cells
were transplanted intramyocardially using a percuta-
neous injection system. The 111In activity was
determined using gamma camera imaging. Excised
hearts were analyzed by fluorescence in situ hybrid-
ization (FISH) and microscopy. Gamma camera
imaging revealed focal cardiac 111In accumulations
up to 6 days after injection (N = 4). No MSC could
be identified with FISH, and microscopy identified
widespread acute inflammation. Focal 111In accumu-
lation, inflammation but no human MSC were
similarly seen in pigs (N = 2) after immunosuppres-
sion. A comparable retention of 111In activity was
observed after intramyocardial injection of 111In-
tropolone (without cells) (N = 2), but without sign of
myocardial inflammation. Injection of labeled non-
viable cells (N = 1) also led to high focal 111In
activity up to 6 days after intramyocardial injection.
As a positive control of the FISH method, we
identified labeled cells both in culture and immedi-
ately after cell injection in one pig. This pilot trial
suggests that after intramyocardial injection 111In
stays in the myocardium despite possible disappear-
ance of labeled cells. This questions the clinical use
of 111In-labeled cells for tracking. The results further
suggest that xenografting of human MSC into porcine
hearts leads to inflammation contradicting previous
studies implying a special immunoprivileged status
for MSC.
Stig Lyngbaek and Rasmus S. Ripa contributed equally to this
work.
S. Lyngbæk � R. S. Ripa � E. Jørgensen � J. KastrupDepartment of Cardiology, The Heart Centre,
Copenhagen University Hospital Rigshospitalet,
Copenhagen, Denmark
S. Lyngbæk � M. Haack-Sørensen � J. KastrupCardiac Stem Cell Laboratory, The Heart Centre,
Copenhagen University Hospital Rigshospitalet,
Copenhagen, Denmark
A. Cortsen � L. Kragh � A. Kjær � B. HesseDepartment of Clinical Physiology, Nuclear Medicine and
PET & Cluster for Molecular Imaging, Copenhagen
University Hospital Rigshospitalet, Copenhagen,
Denmark
C. B. Andersen
Department of Pathology, Copenhagen University
Hospital Rigshospitalet, Copenhagen, Denmark
R. S. Ripa (&)
Department of Clinical Physiology and Nuclear Medicine,
Frederiksberg Hospital, Nordre Fasanvej 57, 2000
Frederiksberg, Denmark
e-mail: [email protected]; [email protected]
123
Int J Cardiovasc Imaging (2010) 26:273–284
DOI 10.1007/s10554-009-9532-4

Keywords Imaging � Stem cell tracking �Ischemic heart disease � Indium labeling
Introduction
Utilization of stem cells has emerged as a potential
treatment modality for ischemic heart disease [1–3].
Tracking of these cells in vivo is pivotal for the future
implementation of stem cell therapy by determining
their fate in the patient. Imaging based cell-tracking
can potentially elucidate issues regarding homing,
engraftment and growth of cells following transplan-
tation. Furthermore, identification of cell redistribu-
tion to other organs where potential side effects may
take place is important. Several in vivo imaging
techniques are available and currently direct labeling
with radionuclides for gamma camera imaging or
positron emission tomography or labeling with iron
particles for magnetic resonance imaging appear
suitable [4]. Imaging of leukocyte distribution by
gamma camera imaging using 111In-tropolone or
-oxine is a safe clinical routine procedure. 111In is
commercially available with a half-life of 2.8 days
making in vivo tracking up to 2 weeks possible.
Several clinical studies regarding treatment of
ischemic heart disease with bonemarrowmononuclear
cell solutions have been conducted with conflicting
results. A potential disadvantage of utilizing mononu-
clear cell solutions is the low fraction of stem cells that
are believed to be therapeutically useful. This has
shifted the focus towards the use of more specific cells
lines. One candidate is multipotent mesenchymal
stromal cells (MSC), which can be isolated in low
numbers from the bone marrow. However, MSC can
be expanded in culture and stimulated to differentiate
into different cell types such as an endothelial or
cardiac phenotype before injection [5–7]. Labeling of
human MSC with 111In-tropolone does not appear to
affect viability or differentiation capacity [8].MSC are
currently used in several ongoing clinical trials of
ischemic heart disease.
The objective of this hypothesis-generating pilot
trial was to investigate whether the retention of ex-
vivo cultured MSC can be determined after direct
percutaneous intramyocardial transplantation in non-
ischemic tissue in a large animal model by 111In-
tropolone radiolabeling of human MSC and use of
gamma camera imaging.
Materials and methods
Experimental design
Human cells were transplanted into a xenogeneic
porcine model. Percutaneous intramyocardial injec-
tions were performed on day 0. Gamma camera
imaging was performed approximately �, 24 and
48 h after the cell injections.
The design is outlined in Fig. 1. In detail: pigs no.
1–2 were sacrificed following the 48 h scan whereas
the remaining pigs underwent an additional fourth
scintigraphy on day 4 or 6 just prior to euthanasia
(Fig. 1).The first 4 pigs were injected with sex-
mismatched 111In-labeled human MSC. Pigs no. 5
and 6 were immunosuppressed by treatment with
cyclosporine (5 mg/kg per day) from 3 days before
injection of 111In-labeled sex-mismatched human
MSC. Immunosuppression was sustained until the
pigs were sacrificed.
Four pigs were used as controls: Two (no. 7 and 8)
were injected with 111In-tropolone (without cells) to
test the clearance of 111In-tropolone from the myo-
cardium and to test the tissue response to the gamma
radiation from 111In. Pig no. 9 was injected with111In-labeled human MSC killed by heating in 60�Cjust prior to injection to test the clearance of 111In
from dead cells. The last pig was injected with 111In-
labeled human MSC immediately post-mortem to
serve as positive control of the histological identifi-
cation of the cells.
Fig. 1 Experimental protocol
274 Int J Cardiovasc Imaging (2010) 26:273–284
123

Animal protocol
Ten female domestic pigs weighing 35–40 kg were
included. Animal handling and care followed the
principles stated in the federal law on animal
experiments and the national animal research com-
mittee approved the protocol. The animals were
premedicated with midazolam. Anaesthesia was
induced and maintained with intramuscular tileta-
mine, zolazepam, xylazine, ketamine and methadone.
Cardiac catheterization was performed via an
arterial sheath in the right femoral artery. We did
not induce myocardial infarction since this would
potentially lead to migration of the cells and thus
difficulty in post-mortem cell identification. The pigs
were heparinised (100 IU bolus/kg and 50 IU/kg per
� h). Pigs no. 6 and 7 (immunosuppressed) were
treated with prophylactic antibiotic (dihydrostrepto-
mycin 25 mg/kg and benzylpenicillinprocaine
20.000 IU/kg) at the day of cell injection and the
following 2 days.
Bone marrow cell preparation
Bone marrow cells were obtained from the iliac crest
of 1 healthy male human volunteer by needle
aspiration under local anaesthesia. A total of 30 ml
of bone marrow aspirate was immediately combined
with 6 ml 1000 IE heparin/ml (Hospital pharmacy,
Copenhagen, Denmark). The marrow sample was
diluted 1:1 with phosphate-buffered saline (PBS)
minus Ca2? and Mg2? (Hospital pharmacy, Copen-
hagen, Denmark). The diluted marrow was processed
as previously described [8]. In short, the mononuclear
cells (MNC) were isolated with a density gradient
centrifugation method and collected using Lympho-
prep (Medinor, Denmark). The MNC were cultured
with GMP accepted EMEA-medium (Gibco, Invitro-
gen GmbH, Lofer, Austria) supplemented with 10%
EMEA-FBS (PAA Laboratories, by, Austria), and 1%
penicillin/streptomycin (GIBCO, Invitrogen GmbH,
Lofer, Austria). The cells were incubated and the
medium was changed every 3 or 4 days. When the
adherent MSC were confluent, the cells were har-
vested and frozen in 95% EMEA-FBS ? 5% dimeth-
ylsulfoxide (DMSO, Wak-Chemie Medical GmbH,
Steinbach, Germany) in liquid nitrogen until 5 days
prior to transplantation where the cells were thawed,
plated in 25 cm2 flasks in EMEA- medium and grown
to confluence.
111In-tropolone radiolabeling
Cells were labeled in 25 cm2 flasks (approximately
1 9 106 cells/flask), as previously described [8]. In
short, the adherent cells were washed with PBS and
incubated with 2.5 MBq 111In-tropolone per flask at
37�C for 15 min. Cells were washed twice with PBS
buffer and harvested by incubation with 3 ml Tryple
Select (animal origin free (GIBCO, Invitrogen,
Taastrup, Denmark) for 10 min at 37�C. To inacti-
vate the Tryple Select, 7 ml of the culture medium
was added and the cell-suspension was centrifuged.
Before injection, cells were resuspended in 2 ml of
PBS ? 1% HSA.
Labeling efficiency was measured with a dose
calibrator (CRC120 Capintec, Capintec Instruments
Inc, USA). Cell viability was determined by Nigrosin
staining after labeling.
From 1.5 to 3.3 9 106 cells were available for
injection in each pig with a mean activity of 1.4 ±
0.3 Bq/cell and with a mean viability of 96.7% (range
94–98). Pig no. 7 and 8 were injected with respec-
tively 4.6 and 4.4 MBq 111In-tropolone without cells.
NOGA-mapping and cell injection
Electromechanical evaluation of the left ventricle via
the groin was performed with the NOGA XP� system
(Biosense Webster A/S, Cordis, Johnson & Johnson)
[9]. The intramyocardial injections were done with
the 8-french-sized MYOSTAR� mapping-injection
catheter (Biosense Webster A/S, Cordis, Johnson &
Johnson) inserted into the left ventricle via the groin.
Ten 0.3 ml injections were given within a predefined
arbitrary chosen area. The injections were performed
slowly (30–40 s). Retained radioactivity in the cath-
eter and syringe was determined after delivery.
In pig no. 10 we injected cells in suspension into
small excised tissue-samples from the myocardium
(1–3 g) using a syringe and a needle immediately
prior to formaldehyde fixation since the objective of
pig no. 10 was to serve as a positive control of the
FISH method (and not as a control of the injection
method).
Int J Cardiovasc Imaging (2010) 26:273–284 275
123

Gamma camera image acquisition
All animals had a whole-body scanning performed
half an hour after injection of the 111In-labeled cells
(day 0). Scanning was repeated 1, 2, and in pigs no.
3–9 also 4 or 6 days after injection using the same
dual-headed gamma camera with identical settings
(GE Millenium, with two energy peaks 170 and
245 keV ± 10%, medium energy, general purpose
collimator). On day 1 or 2 99mTc-sestamibi (100–
150 MBq) was injected intravenously, and myocar-
dial SPECT was acquired 30 min later with the same
camera and collimator. The center of the lower
energy peak was changed from the usual 140 keV for
Tc-99 m to 155 keV, in order to reduce the high
count rate from the 99mTc-activity in the left
ventricular myocardium. With this dual isotope
image acquisition and window setting, the left
ventricle could be outlined as a ‘‘background image’’
for the much lower count rates derived from the focal,
myocardial 111In accumulations in the 245 keV
window representing the injected cells. With the
combined SPECT images (Fig. 2) the exact localiza-
tion of 111In activity in the left ventricular walls could
be well defined. Whole body scintigraphy of pig no. 1
after 24 h was performed after 99mTc-sestamibi
injection, making quantification of 111In retention at
this day impossible. As consequence, we injected99mTc-sestamibi after the whole body scintigraphy in
all subsequent pigs.
The myocardial retention of 111In at follow up was
determined by the decrease in count rates within
Fig. 2 a Endocardial NOGA mapping of a pig heart. The dotsindicate the injection sites. b Dual isotope SPECT images of
the left ventricle in the short axis showing a hot spot of 111In
activity in the anterior wall, corresponding to the injection sites
in the NOGA map
276 Int J Cardiovasc Imaging (2010) 26:273–284
123

regions of interest (ROI) as applied on the scintig-
raphy from day 0 (anterior view) after correction for
physical decay and background activity (a ROI
outside the pig). The size and shape of the ROI was
manually drawn to include the focal 111In accumu-
lation in the heart on the baseline image. This ROI
was copied onto the following examinations using the
imaging processing software. The position was
manually adjusted to cover the same part of the heart
potentially introducing a bias in the count-numbers.
However, this bias appeared minimal since the tissue
surrounding the focal 111In accumulation had very
low count-numbers compared to the focal accumula-
tion (as it is apparent from Fig. 3) and the size of the
ROI was set to include a minimum of surrounding
tissue.
Tissue harvesting
All animals were euthanized after the final imaging
session. Tissue-samples were collected from lungs,
liver, spleen and kidney (three samples per organ).
All samples were weighed (1–2 g), and the count
rates were measured together with an 111In standard
with known activity/ml in a lead-shielded well
counter (Packard COBRAII model 5003, Canberra
Packard Canada, Mississauga, Ontario, Canada) to
calculate the specific count rate per gram tissue
sample after correction for radioactive decay.
Sites of 111In-labeled cell injections in the left
ventricle were identified using a gamma detector
probe (Neo2000, Neoprobe, Dublin, OH, USA) and 3
transmural tissue-blocks (1–3 g) containing the
injection sites were fixed in formaldehyde for histol-
ogy and fluorescence in situ hybridization (FISH). In
addition, 3 tissue-blocks from injection sites and 3
blocks from remote myocardium were excised for
measurement of radioactivity in the well counter.
Histology and FISH
Formalin fixed transmural specimens from the heart
identified by the gamma detector probe were embed-
ded in paraffin from which serial sections were cut to
obtain full coverage of the tissue. Samples were
stained with haematoxylin-eosin.
FISH was applied using probes for the X- and Y-
chromosomes to distinguish transplanted human male
cells from female porcine cells. Bicolor FISH was
performed on 1–2 mm thick paraffin sections using
specific a-satellite DNA-probes for the X-chromo-
some (CEPHX (DXZ1, a-satellite) and Spectrum-
GreenTM (Vysis, Downers Grove, IL, USA)), and the
Y-chromosome (CEPHY (DYZ3, a-satellite) and
Spectrum-OrangeTM (Vysis)). The standard protocol
was recommended by DakoCytomation (Copenha-
gen, Denmark), using heating in pre-treatment-solu-
tion followed by proteolytic digestion by cold ready
to-use-pepsin at room temperature. Denaturation was
performed for 1 min at 82�C and hybridization took
place over night at 42�C. 111In-labeled human MSC
(identical to the ones injected in the pigs) in culture
were used as positive control of the Y-chromosome
probe. In addition, one pig was sacrificed immedi-
ately prior to cell injection and used as positive
control of the cell identification method (pig no. 10).
Fig. 3 Example of 111In retention with anterior gamma
camera at � h, 1, 2 and 6 days after intramyocardial injection
of 111In-labeled MSC with identical pig position. Left panelshows gamma camera image acquired 30 min after intravenous
99mTc-sestamibi infusion. From the 99mTc-sestamibi image it is
clearly demonstrated that the focal 111In activity is localized in
the myocardial region
Int J Cardiovasc Imaging (2010) 26:273–284 277
123

Statistics
Data are presented as mean ± SD. No statistical
significance testing was done in this exploratory trial
due to the few animals (1–2) in each regimen. All
count rates were corrected for both background
activity and for decay. Time-activity curves (Fig. 4)
were quantified by curve-fitting to assess clearance
half-lives using GraphPad Prism 5.02 (GraphPad
Software Inc, CA, USA). Retention following cell
injection (viable or dead) was best described using
two phase exponential fitting whereas one phase
exponential fitting described the clearance of 111In-
tropolone without cells (pig no. 7 and 8).
Results
111In labeling
Human MSC from a single male donor were cultured
and labeled with 111In-tropolene in vitro. From 1.5 to
3.3 9 106 cells were available for injection in each
pig with a mean activity of 1.4 ± 0.3 Bq/cell and
with a mean viability of 96.7% (range 94–98). We
have previously published results indicating that this
labeling does not affect cell viability or differentia-
tion using the same protocol [8]. The cells injected
were CD34 and CD45 negative, whereas the majority
of cells were positive for CD13 (99%), CD73 (98%),
CD90 (99%), and CD105 (97%). Approximately 27%
of the radioactivity was retained in the catheter
system and syringes after delivery.111In-labeled cells injected into pig no. 9 were
killed by heating (60�C) resulting in 33% viability
immediately following heating and 0% viability 12 h
later as determined by Nigrosin staining.
Gamma camera imaging of the pigs
The 111In activity in the heart was 35% (±11%) of
the total activity in the pig 1 h after injection of
viable 111In-labeled MSC and 30% in the pig injected
with dead cells. The corresponding initial activity in
the 2 pigs injected with 111In-tropolone alone was
only 11 and 16% respectively.
SPECT imaging qualitatively identified the 111In
within the myocardium corresponding to the loca-
tions of intramyocardial injections as identified on the
NOGA mapping system (Fig. 2). After 6 days a focal
accumulation in the cardiac region was still readily
identified on whole body scintigraphy (Fig. 3). The
relative retention of radioactivity in relation to the
initial, decay corrected, activity following intramyo-
cardial injection of 111In-labeled cells is shown in
Fig. 4 with an estimated half life of 0.6 days in the
initial rapid phase and 10 days in the slow phase.
Animals treated with immunosuppressive therapy
seemed to have higher retention after 6 days (rapid
half life 0.7 and slow phase 35 days). Less retention
was found following injection of dead cells (pig no.
9, rapid half life 0.3 and slow phase 7 days) or 111In
alone (pig no. 7–8, half life 0.9). This was most
pronounced initially, but retention after injection of
viable cells, dead cells and 111In followed a similar
pattern (Fig. 4).
Tissue distribution of 111In activity
The animals were sacrificed at various time points
following intramyocardial injection (Fig. 1) and the
count rates per gram tissue were measured in
different tissues (Table 1). Consistent with the in
vivo imaging, the injected myocardium had the
highest specific count rate in all animals. Injection
of living cells (pigs no. 1–6) lead to activities in the
lungs after both 2 and 6 days, whereas the kidneys
showed a high initial activity and then a decline. The
total radioactivity after 6 days was lower in all organs
(8% of delivered radioactivity) in the animal treated
Fig. 4 Relative retention of radioactivity after correction for
decay. Numbers on the graph corresponds to the pig number on
Fig. 1. Data from pig no. 1 were only available on days 0 and 2
and are indicated by black dots (see text)
278 Int J Cardiovasc Imaging (2010) 26:273–284
123

with dead cells (pig no. 9) compared to those
receiving living cells (13%). Injection of 111In alone
without cells (pigs no. 7–8) lead to a higher
accumulation of radioactivity in kidneys, liver, and
spleen, whereas the counts in non-injected (normal)
myocardium and lungs were lower when compared to
animals receiving labeled cells.
Detection of MSC by FISH and histology
Human male MSC were readily identified in cell
culture using FISH (Fig. 5a). The cells injected after
euthanization of pig no. 10 were identified by FISH
without unspecific labeling of the pig myocardium
(Fig. 5b).
Samples of myocardium with high count rates with
the gamma probe were analyzed by FISH and
microscopy to verify the presence of human MSC
2–6 days after injection (pig no. 1–4). However, we
were unable to identify any human MSC with Y-
chromosomes despite intensive search by an experi-
enced histopathologist and a technician skilled in
FISH. During section of the heart we observed
macroscopic changes on the endocardium at the site
of the injections (Fig. 6). The microscopy of haema-
toxylin-eosin stained sections from the first biopsies
(2 days) identified widespread necrosis bordered by
acute inflammatory cells in several cases clearly
outlining the needle shaped traces after the injection.
Later biopsies (6 days) showed increasing numbers
of mononuclear cells often with macrophages
forming multinuclear cells and early granulation
tissue formation. The lesions included the endocar-
dium and reached deep myocardium (Fig. 7a, b). In
the two animals (pigs no. 5–6) treated with immu-
nosuppression we could still not identify any human
cells by FISH despite high count rates in the tissue
samples. Inflammation as described above was still
evident with light microscopy. Two pigs (no. 7–8)
were injected with 111In-tropolone without cells. In
these two pigs radioactive tissue samples, identified
by a gamma detection probe, showed normal myo-
cardium without inflammation (Fig. 7c, d).
Discussion
This descriptive pilot study generates two important
hypotheses. First, as radioactivity from 111In-labeled
cells stays in the myocardium for a long time despite
the disappearance of transplanted cells, clinical use of111In-labeled cells for monitoring of MSC in the
human heart seems problematic. Second, our results
do not support the hypothesis that xenografting of
human MSC into a pig does not lead to an inflam-
matory response and fast degradation of the cells
even under pharmacologic immunosuppression.
Imaging techniques and labeling
The ideal imaging technique should allow for serial
tracking in humans for a prolonged period of time
Table 1 Postmortem
radioactivity count rate per
gram tissue
a Identified using a gamma
detector probe, except for pig
number 2
Injected
myocardiumaNormal
myocardium
Kidney Hepar Spleen Lungs
At day 2 after injection of 111In-labeled cells
Pig 1 63,155 385 1,234 929 209 6,827
Pig 2 357a 242 898 376 98 1,192
At day 6
Pig 3 13,578 22 N/A N/A N/A N/A
Pig 4 36,020 143 N/A N/A N/A 1,389
Pig 5 34,049 116 349 749 43 3,054
Pig 6 66,349 68 242 536 119 1,356
At day 4 after injection of 111In without cells
Pig 7 6,893 614 718 1,522 371 1,029
Pig 8 11,748 192 570 1,404 179 314
At day 6 after injection of dead cells
Pig 9 9,225 22 123 353 20 897
Int J Cardiovasc Imaging (2010) 26:273–284 279
123

with high spatial resolution and with the capability of
tracking a few cells without affecting the cells or the
organ. It is important that the marker remains in the
viable cell but is quickly cleared from the tissue upon
cell death.
A concern of radioactive labeling is the potential
radiation damage to the cell and determining the
effect of labeling on proliferation and differentiation
is imperative prior to clinical application to ensure
safety. We have previously shown that 111In labeling
of human MSC (with 30 Bq/cell) or freezing did not
affect viability or differentiation capacity in vitro [8,
10]. Similarly, Aicher et al. [11] found that 111In-
oxine labeling (15 MBq) of cultivated circulating
endothelial progenitor cells did not significantly
affect viability, proliferation, or migration. The same
group [12] found different results when labeling less
Fig. 5 Fluorescence in situ
hybridization. Y-chromosome
with green label (white arrow)and X-chromosome with
orange label (black arrow).a 111In-labeled human
mesenchymal stromal cells in
culture. b Paraffin embedded
myocardium from one pig (no.
10) sacrificed immediately
prior to cell injection (91,000)
Fig. 6 Macroscopic inflammation after cell injection
280 Int J Cardiovasc Imaging (2010) 26:273–284
123

differentiated circulating hematopoietic progenitor
cells with higher dose of radioactivity (30 MBq).
Experiments by Jin et al. [13] and Gholamrezanezhad
et al. [14] might suggest that the doses used in our
trial could be toxic to stromal cells and that the lethal
effect is not manifest until 48 h after labeling. We
previously tested viability and differentiation capac-
ity up to 1 week after labeling using the exact same
culture and labeling procedure as in the present study
with no indication of radiotoxic effects on viability
and/or function [8]. We can only speculate if
differences in culture or labeling procedures com-
pared to other trials could explain the differences in
results.
Cell labeling with 111In requires a chelator to
mediate the transport of 111In into the cell where 111In
binds firmly to macromolecules [15]. Both tropolone
and oxine can be used as chelator. We found no
difference in labeling efficiency or viability of MSC
with oxine compared to tropolone as chelator
(unpublished data).
An optimal route for cell delivery has not been
established. We used trans-endocardial injection
since evidence exists that intramyocardial injection
leads to higher retention 1 h after injection compared
to intracoronary infusion [16]. This was confirmed by
our findings that 1/3 of the total radioactivity in the
injected pigs � h after injection was still located in
the heart, compared to only 6.9 ± 4.7% after intra-
coronary infusion [17] and from 11.3 ± 3% [16] to
20.7 ± 2.3% [18] after trans-epicardiel injection.
Most of the initial loss after intramyocardial injection
might be caused by leakage trough the needle channel
and clearance through the capillary network of the
myocardium.
Xenografting of human MSC
When designing this study evidence existed that
MSC were immunoprivileged and both allografting
[19–21] and xenografting [22–25] of MSC would be
possible. In this context it was unexpected that we
found extensive inflammation in all cardiac biopsies
after injection of cells and were unable to detect any
transplanted cells by FISH even after only 2 days.
Two pigs were treated with immunosuppressive
therapy to diminish host-versus-graft reaction, but
injection of MSC still led to intense inflammation and
Fig. 7 Haematoxylin-eosin staining of paraffin embedded
myocardium. a, b, Pig injected with human 111In-labeled
MSC, show intense focal inflammation with central necrosis. c,
d, Pig injected with 111In-tropolone without cells show normal
myocardium. Magnification is 925 in a, c and 9100 in b, d
Int J Cardiovasc Imaging (2010) 26:273–284 281
123

cell degradation. Therefore, two experiments were
conducted that confirmed that 111In-tropolone label-
ing did not interfere with the FISH method: 111In-
tropolone labeled cells were identified by FISH in
culture, and immediately following intramyocardial
injection (Fig. 5). Obviously, we cannot exclude the
possibility that a few viable cells were present despite
the negative histological result; however, based on
the intense radioactivity in the tissue-sample excised
for FISH analysis, we would expect[105 human cells
per gram tissue (assessed using our mean activity of
1.4 Bq/cell). The myocardial tissue for the FISH
analysis was identified using a gamma detector probe
ensuring that cardiac tissue with 111In activity was
studied; in addition, the needle track was visible in
several samples. It seems unlikely that the cells
would have released the radioactivity after transplan-
tation and migrated into the myocardium especially
since no myocardial ischemia was induced. Two pigs
injected with 111In-tropolone without cells showed no
microscopic inflammation suggesting that neither the
gamma radiation from the 111In nor the transendo-
cardial injection causes inflammation. We speculate
that the clearance of transplanted cells is related to an
immunological reaction invoked. This hypothesis is
supported by the observation that immunosuppressed
pigs seem to have higher retention of the radioactivity
(Fig. 4). Our data supplement recent evidence sug-
gesting that MSC are not immunoprivileged and will
therefore lead to a cellular response after both
allogenic and xenogenic transplantation [26–28].
In vivo cell tracking
Previously, several studies have used 111In labeling of
both MSC and endothelial progenitor cells and
subsequent in vivo tracking of the radioactivity as a
surrogate measure of cell engraftment and migration
[17, 29–31]. However, we have consistently in 6 of 6
pigs found high retention of radioactivity despite cell
death. This is probably because 111In remains firmly
bound to macromolecules from within the cells.
In our opinion this makes 111In labeling problem-
atic for in vivo cell tracking in humans, since the
viability of the cells then must be determined in vivo
by another method, which is very difficult in humans.
It could be of future interest to repeat our labeling
studies with autologous MSC injections into the pig
and to compare the intramyocardial injection method
with intracoronary cell infusion.
Iron-oxide labeling for magnetic resonance imag-
ing tracking of injected cells has appeared as a
suitable alternative to 111In labeling, with the possi-
bility of even longer follow-up. However, recently
results very similar to ours using iron labeling were
found [32, 33]. After 3–4 weeks transplanted cells
could not be detected though a continued enhanced
magnetic resonance signal existed representing
engulfed labeling particles in cardiac macrophages
suggesting that iron-oxide labeling is also an unreli-
able marker for monitoring cell survival and migra-
tion [32, 33].
Another method for in vivo cell tracking has
emerged recently. Reporter gene imaging using
clinical positron emission tomography is a promising
modality [34], but the method still needs further
validation.
Limitations
We did not induce myocardial infarction in the pigs
since the objective was to evaluate the labeling
method and not engraftment, migration and func-
tional improvement. This probably led to impaired
engraftment and especially migration. We intended to
succeed with infarcted animals to address serial cell
tracking had the method proven efficient for human
use. We find it unlikely that a prior myocardial
infarction would have changed the conclusions of the
present trial, since the conclusions relates to efficacy
of the labeling method and not cell engraftment or
migration.
Our results indicate a fast immunological reaction
and degradation of human MSC following transplan-
tation into the pig heart. Results by other groups have
indicated that the radioactivity from the labeling
could have led to cell death [13, 14]. However, this
controversy does not in any way alter the primary
conclusion that cell death (caused by immunological
reaction or radioactivity) is not followed by fast
clearance of 111In. Thus labeling with 111In can
potentially lead to false conclusions in cell tracking
experiments.
We have no results showing the 111In retention in
the myocardium with viable cells. However, results
by others [35] suggest that the retention we observe
282 Int J Cardiovasc Imaging (2010) 26:273–284
123

with dead cells is comparable to the one seen with
viable cells.
Conclusion
Our results suggest that 111In may remain in the
myocardial tissue for a prolonged period after cell
death. This makes 111In labeling of MSC unsuitable
for human use unless in vivo cell viability after
transplantation can be determined by another method.
The results further suggest that transplantation of
human MSC into porcine heart results in a fast
inflammatory response and cell degradation. There-
fore, this xenogenic model seems rather unsuitable
for pre-clinical trials. Due to the small number of
animals examined the results and hypotheses gener-
ated need confirmation, but call for caution in
interpretation of in vivo cell tracking studies.
Conflicts of interest The authors declare that they have no
conflict of interest.
References
1. Ripa RS, Jørgensen E, Wang Y, Thune JJ, Nilsson JC,
Søndergaard L, Johnsen HE, Køber L, Grande P, Kastrup J
(2006) Stem cell mobilization induced by subcutaneous
granulocyte-colony stimulating factor to improve cardiac
regeneration after acute ST-elevation myocardial infarc-
tion: result of the double-blind, randomized, placebo-con-
trolled stem cells in myocardial infarction (STEMMI) trial.
Circulation 113:1983–1992
2. Schachinger V, Erbs S, Elsasser A, Haberbosch W, Ham-
brecht R, Holschermann H, Yu J, Corti R, Mathey DG,
Hamm CW, Suselbeck T, Assmus B, Tonn T, Dimmeler S,
Zeiher AM (2006) Intracoronary bone marrow-derived
progenitor cells in acute myocardial infarction. N Engl J
Med 355:1210–1221
3. Lunde K, Solheim S, Aakhus S, Arnesen H, Abdelnoor M,
Egeland T, Endresen K, Ilebekk A, Mangschau A, Fjeld
JG, Smith HJ, Taraldsrud E, Grogaard HK, Bjornerheim R,
Brekke M, Muller C, Hopp E, Ragnarsson A, Brinchmann
JE, Forfang K (2006) Intracoronary injection of mononu-
clear bone marrow cells in acute myocardial infarction. N
Engl J Med 355:1199–1209
4. Beeres SL, Bengel FM, Bartunek J, Atsma DE, Hill JM,
Vanderheyden M, Penicka M, Schalij MJ, Wijns W, Bax JJ
(2007) Role of imaging in cardiac stem cell therapy. J Am
Coll Cardiol 49:1137–1148
5. Pittenger MF, Mackay AM, Beck SC, Jaiswal RK, Douglas
R, Mosca JD, Moorman MA, Simonetti DW, Craig S,
Marshak DR (1999) Multilineage potential of adult human
mesenchymal stem cells. Science 284:143–147
6. Haack-Sorensen M, Friis T, Bindslev L, Mortensen S,
Johnsen HE, Kastrup J (2008) Comparison of different
culture conditions for human mesenchymal stromal cells
for clinical stem cell therapy. Scand J Clin Lab Invest
68:192–203
7. Haack-Sorensen M, Friis T, Kastrup J (2008) Mesenchy-
mal stromal cell and mononuclear cell therapy in heart
disease. Future Cardiology 4:481–494
8. Bindslev L, Haack-Sørensen M, Bisgaard K, Kragh L,
Mortensen S, Hesse B, Kjaer A, Kastrup J (2006) Labelling
of human mesenchymal stem cells with indium-111 for
SPECT imaging: effect on cell proliferation and differen-
tiation. Eur J Nucl Med Mol Imaging 33:1171–1177
9. Kastrup J, Jørgensen E, Ruck A, Tagil K, Glogar D, Ru-
zyllo W, Bøtker HE, Dudek D, Drvota V, Hesse B,
Thuesen L, Blomberg P, Gyongyosi M, Sylven C (2005)
Direct intramyocardial plasmid vascular endothelial
growth factor-A165 gene therapy in patients with stable
severe angina pectoris a randomized double-blind placebo-
controlled study: the Euroinject One trial. J Am Coll
Cardiol 45:982–988
10. Haack-Sorensen M, Bindslev L, Mortensen S, Friis T,
Kastrup J (2007) The influence of freezing and storage on
the characteristics and functions of human mesenchymal
stromal cells isolated for clinical use. Cytotherapy 9:
328–337
11. Aicher A, Brenner W, Zuhayra M, Badorff C, Massoudi S,
Assmus B, Eckey T, Henze E, Zeiher AM, Dimmeler S
(2003) Assessment of the tissue distribution of transplanted
human endothelial progenitor cells by radioactive labeling.
Circulation 107:2134–2139
12. Brenner W, Aicher A, Eckey T, Massoudi S, Zuhayra M,
Koehl U, Heeschen C, Kampen WU, Zeiher AM, Dimm-
eler S, Henze E (2004) 111In-labeled CD34? hemato-
poietic progenitor cells in a rat myocardial infarction
model. J Nucl Med 45:512–518
13. Jin Y, Kong H, Stodilka RZ, Wells RG, Zabel P, Merrifield
PA, Sykes J, Prato FS (2005) Determining the minimum
number of detectable cardiac-transplanted 111In-tropolone-
labelled bone-marrow-derived mesenchymal stem cells by
SPECT. Phys Med Biol 50:4445–4455
14. Gholamrezanezhad A, Mirpour S, Ardekani JM, Bagheri
M, Alimoghadam K, Yarmand S, Malekzadeh R (2009)
Cytotoxicity of 111In-oxine on mesenchymal stem cells: a
time-dependent adverse effect. Nucl Med Commun 30:
210–216
15. Thakur ML, Segal AW, Louis L, Welch MJ, Hopkins J,
Peters TJ (1977) Indium-111-labeled cellular blood com-
ponents: mechanism of labeling and intracellular location
in human neutrophils. J Nucl Med 18:1022–1026
16. Hou D, Youssef EA, Brinton TJ, Zhang P, Rogers P, Price
ET, Yeung AC, Johnstone BH, Yock PG, March KL
(2005) Radiolabeled cell distribution after intramyocardial,
intracoronary, and interstitial retrograde coronary venous
delivery: implications for current clinical trials. Circulation
112:I150–I156
17. Schachinger V, Aicher A, Dobert N, Rover R, Diener J,
Fichtlscherer S, Assmus B, Seeger FH, Menzel C, Brenner
W, Dimmeler S, Zeiher AM (2008) Pilot trial on deter-
minants of progenitor cell recruitment to the infarcted
human myocardium. Circulation 118:1425–1432
Int J Cardiovasc Imaging (2010) 26:273–284 283
123

18. Tossios P, Krausgrill B, Schmidt M, Fischer T, Halbach M,
Fries JW, Fahnenstich S, Frommolt P, Heppelmann I,
Schmidt A, Schomacker K, Fischer JH, Bloch W, Mehl-
horn U, Schwinger RH, Muller-Ehmsen J (2008) Role of
balloon occlusion for mononuclear bone marrow cell
deposition after intracoronary injection in pigs with rep-
erfused myocardial infarction. Eur Heart J 29:1911–1921
19. Horwitz EM, Gordon PL, Koo WK, Marx JC, Neel MD,
McNall RY, Muul L, Hofmann T (2002) Isolated alloge-
neic bone marrow-derived mesenchymal cells engraft and
stimulate growth in children with osteogenesis imperfecta:
Implications for cell therapy of bone. Proc Natl Acad Sci
USA 99:8932–8937
20. Amado LC, Saliaris AP, Schuleri KH, St JM, Xie JS, Cat-
taneo S, Durand DJ, Fitton T, Kuang JQ, Stewart G, Lehrke
S, Baumgartner WW, Martin BJ, Heldman AW, Hare JM
(2005) Cardiac repair with intramyocardial injection of
allogeneic mesenchymal stem cells after myocardial
infarction. Proc Natl Acad Sci USA 102:11474–11479
21. Tse WT, Pendleton JD, Beyer WM, Egalka MC, Guinan
EC (2003) Suppression of allogeneic T-cell proliferation
by human marrow stromal cells: implications in trans-
plantation. Transplantation 75:389–397
22. Liechty KW, MacKenzie TC, Shaaban AF, Radu A,
Moseley AM, Deans R, Marshak DR, Flake AW (2000)
Human mesenchymal stem cells engraft and demonstrate
site-specific differentiation after in utero transplantation in
sheep. Nat Med 6:1282–1286
23. Allers C, Sierralta WD, Neubauer S, Rivera F, Minguell JJ,
Conget PA (2004) Dynamic of distribution of human bone
marrow-derived mesenchymal stem cells after transplan-
tation into adult unconditioned mice. Transplantation
78:503–508
24. Saito T, Kuang JQ, Bittira B, Al-Khaldi A, Chiu RC (2002)
Xenotransplant cardiac chimera: immune tolerance of adult
stem cells. Ann Thorac Surg 74:19–24
25. Plotnikov AN, Shlapakova I, Szabolcs MJ, Danilo P Jr,
Lorell BH, Potapova IA, Lu Z, Rosen AB, Mathias RT,
Brink PR, Robinson RB, Cohen IS, Rosen MR (2007)
Xenografted adult human mesenchymal stem cells provide
a platform for sustained biological pacemaker function in
canine heart. Circulation 116:706–713
26. Nauta AJ, Westerhuis G, Kruisselbrink AB, Lurvink EG,
Willemze R, Fibbe WE (2006) Donor-derived mesenchy-
mal stem cells are immunogenic in an allogeneic host and
stimulate donor graft rejection in a nonmyeloablative set-
ting. Blood 108:2114–2120
27. Poncelet AJ, Vercruysse J, Saliez A, Gianello P (2007)
Although pig allogeneic mesenchymal stem cells are not
immunogenic in vitro, intracardiac injection elicits an
immune response in vivo. Transplantation 83:783–790
28. Grinnemo KH, Mansson-Broberg A, Leblanc K, Corbascio
M, Wardell E, Siddiqui AJ, Hao X, Sylven C, Dellgren G
(2006) Human mesenchymal stem cells do not differentiate
into cardiomyocytes in a cardiac ischemic xenomodel. Ann
Med 38:144–153
29. Goussetis E, Manginas A, Koutelou M, Peristeri I, The-
odosaki M, Kollaros N, Leontiadis E, Theodorakos A,
Paterakis G, Karatasakis G, Cokkinos DV, Graphakos S
(2006) Intracoronary infusion of CD133? and CD133-
CD34? selected autologous bone marrow progenitor cells
in patients with chronic ischemic cardiomyopathy: cell
isolation, adherence to the infarcted area, and body dis-
tribution. Stem Cells 24:2279–2283
30. Caveliers V, De Keulenaer G, Everaert H, Van Riet I, Van
Camp G, Verheye S, Roland J, Schoors D, Franken PR,
Schots R (2007) In vivo visualization of 111In labeled
CD133? peripheral blood stem cells after intracoronary
administration in patients with chronic ischemic heart
disease. Q J Nucl Med Mol Imaging 51:61–66
31. Kurpisz M, Czepczynski R, Grygielska B, Majewski M,
Fiszer D, Jerzykowska O, Sowinski J, Siminiak T (2007)
Bone marrow stem cell imaging after intracoronary
administration. Int J Cardiol 121:194–195
32. Amsalem Y, Mardor Y, Feinberg MS, Landa N, Miller L,
Daniels D, Ocherashvilli A, Holbova R, Yosef O, Barbash
IM, Leor J (2007) Iron-oxide labeling and outcome of
transplanted mesenchymal stem cells in the infarcted
myocardium. Circulation 116:I38–I45
33. Terrovitis J, Stuber M, Youssef A, Preece S, Leppo M,
Kizana E, Schar M, Gerstenblith G, Weiss RG, Marban E,
Abraham MR (2008) Magnetic resonance imaging over-
estimates ferumoxide-labeled stem cell survival after
transplantation in the heart. Circulation 117:1555–1562
34. Gyongyosi M, Blanco J, Marian T, Tron L, Petnehazy O,
Petrasi Z, Hemetsberger R, Rodriguez J, Font G, Pavo IJ,
Kertesz I, Balkay L, Pavo N, Posa A, Emri M, Galuska L,
Kraitchman DL, Wojta J, Huber K, Glogar D (2008) Serial
Noninvasive In Vivo Positron Emission Tomographic
Tracking of Percutaneously Intramyocardially Injected
Autologous Porcine Mesenchymal Stem Cells Modified for
Transgene Reporter Gene Expression. Circ Cardiovasc
Imaging 1:94–103
35. Zhou R, Thomas DH, Qiao H, Bal HS, Choi SR, Alavi A,
Ferrari VA, Kung HF, Acton PD (2005) In vivo detection
of stem cells grafted in infarcted rat myocardium. J Nucl
Med 46:816–822
284 Int J Cardiovasc Imaging (2010) 26:273–284
123