Embed Size (px)
Citation preview
Behandling av demens Friederike Fritze
overlege alderspsykiatrisk poliklinikk
SUS
03.10.12

Innhold
• Generelle tanker om temaet
• Nasjonale retningslinjer
• Internasjonale retningslinjer
• Cochrane
• Medisiner
• Klinisk erfaring
• Personsentrert omsorg
Skuffete Forventninger
• H. Lundbeck ilegges reklamegebyr for Ebixa
”Effekten kan måles allerede etter 4 uker": 07.05.2012:
Rådet (for legemiddelinformasjon) mener at slik
påstanden fremstår i reklamen gir den inntrykk av at
klinisk målbar effekt oppnås hos den enkelte pasient
etter 4 uker. Rådets konklusjon er at reklamen fremstår
som villedende. Klager gis medhold. H. Lundbeck
ilegges gebyr kr. 40.000,-
www.legemiddelverket.no
www.medscape.com
ww.nrk.no
Skuffende Forskningsresultater
• Juli 2012: Bapineuzumab (J and J og Pfizer) an
investigational monoclonal antibody that targets amyloid-ß
fails in Phase 3 Alzheimer's Trial (www.medscape.com)
• Status 03.10.2012: www.clinicaltrials.gov: 971 studies on
Alzheimer, 1896 studies on dementia
• Efficacy of psychosocial intervention in patients with mild Alzheimer's
disease: the multicentre, rater blinded, randomised Danish Alzheimer
Intervention Study (DAISY). Waldorff FB, Buss DV, Eckermann A,
Rasmussen ML, Keiding N, Rishøj S, Siersma V, Sørensen J, Sørensen LV,
Vogel A, Waldemar G. BMJ. 2012 Jul 17;345:e4693: did not have
significant effect
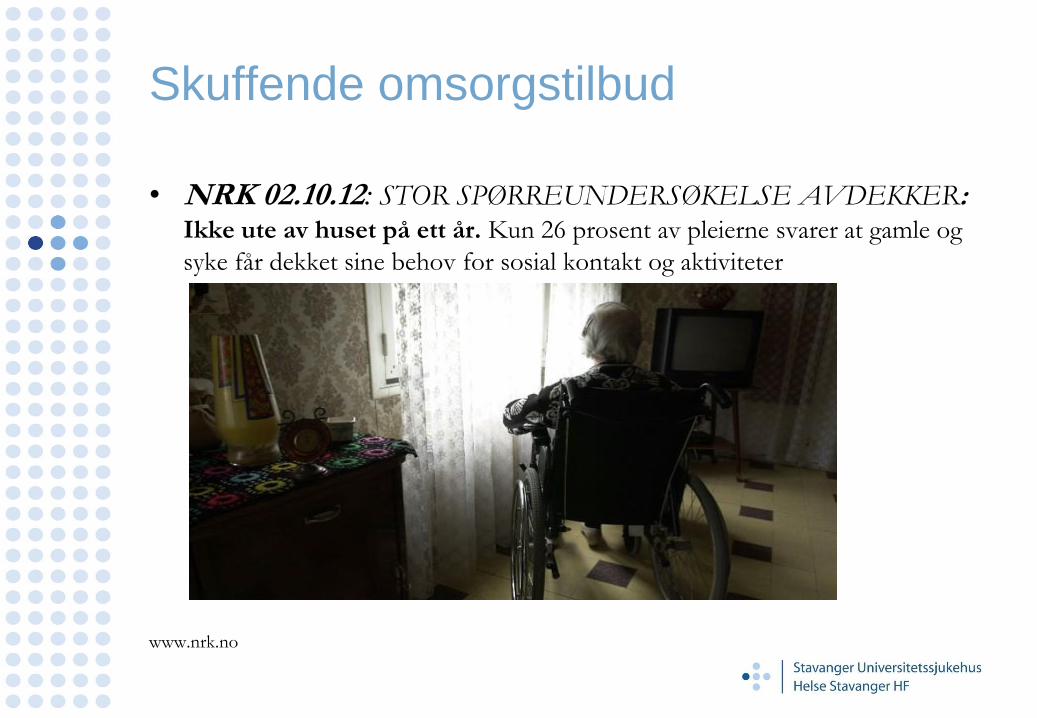
Skuffende omsorgstilbud
• NRK 02.10.12: STOR SPØRREUNDERSØKELSE AVDEKKER: Ikke ute av huset på ett år. Kun 26 prosent av pleierne svarer at gamle og
syke får dekket sine behov for sosial kontakt og aktiviteter
www.nrk.no
Noe generelt: Evidens
Evidence is knowledge produced by
research; it needs to be linked to the
knowledge produced form data analysis,
sometimes called statistics, and knowledge
from the experience of clinicians and
patients. Gray,M: Best current evidence strategy. NHS 2006
«Level of evidence» og «Grad of recommendation(good risk –
benefit ratio)»
Nasjonale retningslinjer
• Norge har som første land lansert en nasjonal demensplan (Demensplan 2015 -
”Den gode dagen”, en delplan til Omsorgsplan 2015) som skal vare fra 2007 til
2015 (revidert i 2011): Utbygging av dagaktivitetstilbud. «Smått er godt». «Større
bredde»
-Standardisert utredningsverktøy anbefalt av Helsedirektoratet og Nasjonalt
. kompetansesenter for aldring og helse (helsepersonell, leger og sykehjem)
-Veileder
- Håndbok for demensteam.
• Å utarbeide retningslinjer vil kunne være en måte å sikre god standard på de
tjenestene som ytes, samt å sikre at ressursene som settes inn brukes på en best
mulig måte.
• Norge har så langt ikke utviklet retningslinjer, og i den grad det har vært
diskutert så har det først og fremst vært snakk om retningslinjer for demensutredning
www.aldringoghelse.no
www.kvalitetogprioritering.no
Nasjonale retningslinjer
• Medikamentell behandling av atferdsforstyrrelser og
psykologiske symptomer (BPSD) hos personer med
demens 2005. Statens legemiddelverk 24-12-23:
Finnes ikke lenger på nettsiden
• For oppdatering av aktuelle/fremtidige retningslinjer sjekk
www.helsebiblioteket.no
www.aldringoghelse.no
Internasjonale retningslinjer
• World Federation of Societies of Biological Psychiatry
(WFSBP)Guidelines for the Biological Treatment of
Alzheimer ’ s disease and other dementias 2011
• Storbritannia: NICE pathways dementia 2011
• Tyskland: S 3 Leitlinie Demenz 2009
• USA : American Psychiatric Association (APA) 2007.
American College of Physicians and the American Academy of
Family Physicians. American Academy of Neurology (AAN).
The American Geriatrics Society (AGS).
• Sverige, Kanada, Scotland, Taiwan
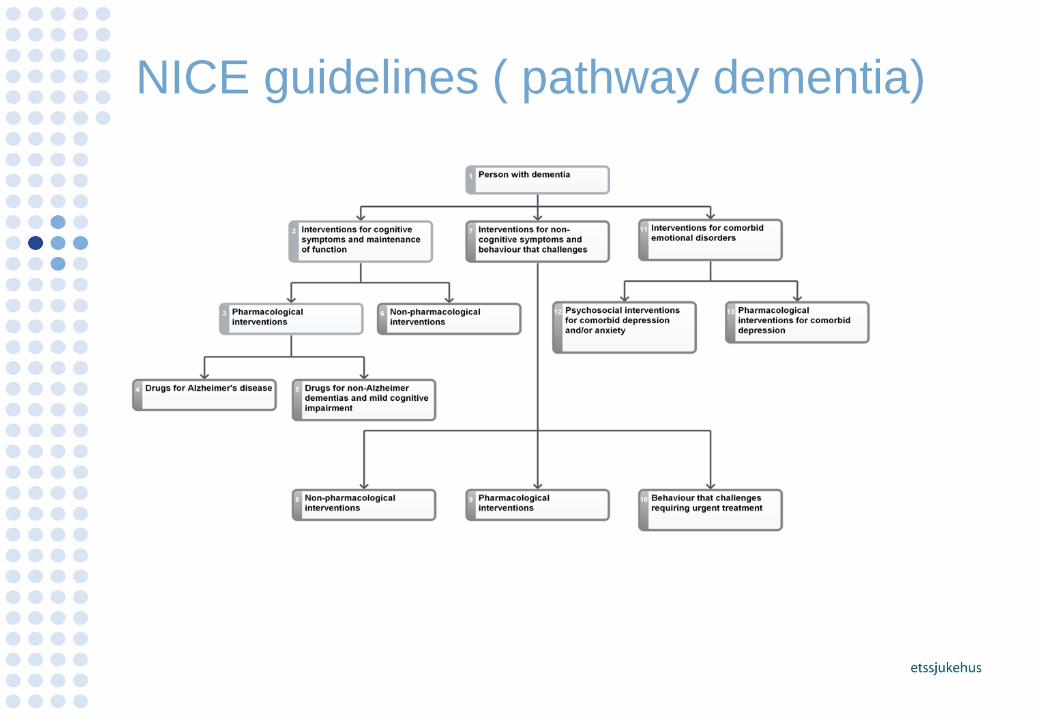
NICE guidelines ( pathway dementia)
NICE guidelines ( pathway dementia)
• Donepezil, galantamine, rivastigmine and
memantine
1. The three acetylcholinesterase (AChE) inhibitors…are recommended as
options for managing mild to moderate Alzheimer's disease under all of the
conditions specified in paragraphs 3 and 4 below.
2. Memantine is recommended …for people with moderate Alzheimer's
disease who are intolerant of or have a contraindication to AChE inhibitors or
severe Alzheimer's disease. Treatment should be under the conditions
specified in paragraph 3.
NICE guidelines ( pathway dementia)
3. Treatment should be under the following conditions:
• Only specialists in the care of patients with dementia (that is, psychiatrists,
neurologists, and physicians specialising in the care of older people) should
initiate treatment. Carers' views on the patient's condition at baseline should
be sought.
• Treatment should be continued only when it is considered to be having a
worthwhile effect on cognitive, global, functional or behavioural
symptoms.
• Patients who continue on treatment should be reviewed regularly using
cognitive, global, functional and behavioural assessment. Treatment should
be reviewed by an appropriatespecialist team, unless there are locally agreed
protocols for shared care. Carers' views on the patient's condition at follow-
up should be sought.
NICE guidelines (pathway dementia)
If a person with dementia develops distressing non-cognitive
symptoms or behaviour that challenges, offer an early assessment to
identify factors that may influence the behaviour. Include:
• physical health
• depression
• possible undetected pain or discomfort
• side effects of medication
• individual biography
• psychosocial factors
• physical environmental factors
• behavioural and functional analysis in conjunction with carers and care
workers.
NICE guidelines (pathway dementia)
Address environmental, physical health and psychosocial
factors that may increase the likelihood of behaviour that challenges. These
include:
• overcrowding
• lack of privacy
• lack of activities
• inadequate staff attention
• poor communication between the person with dementia and staff
• conflicts between staff and carers
• weak clinical leadership
Principles of pharmacological control of
violence, aggression and extreme agitation • Use drugs to calm the person and reduce the risk of violence
and harm, rather than to treat any underlying psychiatric
condition. Aim to reduce agitation or aggression without
sedation.
• Use the lowest effective dose. Avoid high doses and drug
combinations, especially in elderly or frail people.
• Use drugs for control of behaviour with caution, particularly if
the person has been restrained, because of the following risks:
• loss of consciousness instead of sedation
• over-sedation with loss of alertness
• damage to the relationship between the person with dementia, their
carers and the care team
NICE guideline (pathway dementia) Use of antipsychotics • Risks and benefits have been fully discussed; assess cerebrovascular risk
factors and discuss possible increased risk of stroke/transient ischaemic
attack and possible adverse effects on cognition
• Changes in cognition are regularly assessed and recorded; consider
alternative medication if necessary
• Target symptoms have been identified, quantified and documented, and
changes are regularly assessed and recorded
• Comorbid conditions, such as depression, have been considered
• The drug is chosen after an individual risk–benefit analysis
• The dose is started low and titrated upwards
• Treatment is time limited and regularly reviewed (every 3 months or
according to clinical need).
Copyright © NICE 2011. Pathway last updated: 25 October 2011
The Cochrane Library 2008 og 2009
• Evidence suggests that risperidone and olanzapine are useful in reducing
aggression and risperidone reduces psychosis, but both are associated
with serious adverse cerebrovascular events and extrapyramidal
symptoms. Despite the modest efficacy, the significant increase in adverse
events confirms that neither risperidone nor olanzapine should be used
routinely to treat dementia patients with aggression or psychosis unless
there is severe distress or risk of physical harm to those living and working
with the patient.
• No evidence of the efficacy of vitamin B12 supplementation for
cognitive function
• Haloperidol (<3.5 mg/d), risperidone (1 mg), and olanzapine ( 2,5 mg)
were equally effective in treating delirium, with few adverse effects.
The Cochrane Library 2009
• Cholinesterase inhibitors (ChEIs), donepezil, galantamine and
rivastigmine are efficacious for mild to moderate Alzheimer's disease.
More patients leave ChEI treatment groups, 29%, on account of adverse
events than leave the placebo groups (18%)
• The analyses did not support the use of melatonin for treatment of
cognitive impairment associated with dementia. Meta-analysis of
psychopathologic behavior scale scores suggested that melatonin may be
effective in treating these dementia-related disturbances .
• There is insufficient evidence from randomised trials to allow any
conclusion about the efficacy of validation therapy for people with
dementia or cognitive impairment
• There is insufficient evidence to assess the value of light therapy for
people with dementia.
• Inconclusive evidence of the efficacy of reminiscence therapy for
dementia
The Cochrane Library 2010
• Evidence suggests that haloperidol was useful in reducing aggression, but was associated with adverse effects; there was no evidence to support the routine use of this drug for other manifestations of agitation in dementia. The present study confirmed that haloperidol should not be used routinely to treat patients with agitated dementia. Treatment of agitated dementia with haloperidol should be individualized and patients should be monitored for adverse effects of therapy.
• There is insufficient evidence to recommend statins for the treatment of dementia ( better effect: serum cholesterol was high at baseline, MMSE was higher at baseline or if they had an apolipoprotein E4 allele present)
• There is no substantial evidence to support nor discourage the use of
music therapy in the care of older people with dementia • No evidence of benefit of Ibuprofen for the treatment of Alzheimer's
disease • D-cycloserine has no place in the treatment of patients with Alzheimer's
disease.
The Cochrane Library 2011
• Currently there are relatively few studies of antidepressants for the
treatment of agitation and psychosis in dementia. The SSRIs sertraline
and citalopram were associated with a reduction in symptoms of
agitation when compared to placebo in two studies.
The Cochrane Library 2012
• The currently available evidence supports the use of cholinesterase inhibitors in patients with PDD, with a positive impact on global assessment, cognitive function, behavioural disturbance and activities of daily living rating scales. The effect in DLB remains unclear
• There was consistent evidence from multiple trials that cognitive stimulation programs benefit cognition in people with mild to moderate dementia over and above any medication effects.
• There is insufficient evidence to support HBOT as an effective treatment for patients with VaD
• The effectiveness of acupuncture for vascular dementia is uncertain.
• There is no evidence that MPACs (Metal protein attenuating compounds) are of benefit in Alzheimer's dementia
• Based on the studies carried out so far, the efficacy of aspirin, steroid and NSAIDs (traditional NSAIDs and COX-2 inhibitors) is not proven. Therefore, these drugs cannot be recommended for the treatment of AD.
Retningslinjer generelt
• Utredning før behandling
• Utredning og behandling må inkludere
familie/pleiepersonalet
1. Behandling av kognitive symptomer
2. Behandling av atferdssymptomer
3. Behandling av psykiske symptomer/lidelser
• Vurder alltid ikke medikamentelle tiltak
• Gi tydelig informasjon
• Sett behandlingsmål , kontroller resultater
Medisiner. OBS: Off label bruk
• Psykose: KHE mot hallusinasjoner. Risperdal not mor
than 1 mg. Olanzapine max 5 mg x2. Quetiapin max 75
mg x2
• Depression: Antidepressiva ? Obs falltendens. GIT
blødninger. Hjerte-kar – bivirkninger. Mixed results. Lite
evidens: citalopram 20 mg ? TZA?
• Agitasjon: Ebixa 20 mg. Citlaopram 20 mg. Carbamazepin
etter speil OBS interasksjoner
• Frontotemporallappsdemens: SSRI
• Angst og søvn: foredrag 4.10.12
www.uptodate.com
Fremtidige intervensjonsmål
• Nutritional precursors and cofactors for synapse
formation: Souvenaid (omega-3 fatty acids, choline,
uridine monophosphate, and a mixture of antioxidants
and B vitamins ) RCT : significant improvement in NTB
memory scores over 24/48 weeks
• Marques-Aleixo I, Oliveira PJ, Moreira PI, Magalhães J,
Ascensão A. Physical exercise as a possible strategy for
brain protection: Evidence from mitochondrial-mediated
mechanisms. Prog Neurobiol. 2012 Aug 23.
Forebygging er målet
• Methodological challenges in designing dementia
prevention trials - The European Dementia
Prevention Initiative (EDPI). Richard, E. et al. J Neurol Sci. 2012
Jul 18
• Alzheimer's research. Stopping Alzheimer's before it
starts .Miller, G. Science. 2012 Aug 17;337(6096):790-2
• Alzheimer's Prevention Initiative: a plan to accelerate
the evaluation of presymptomatic treatments.Reiman EM,
Langbaum JB, Fleisher AS, Caselli RJ, Chen K, Ayutyanont N, Quiroz YT, Kosik KS, Lopera
F, Tariot PN. J Alzheimers Dis. 2011;26 Suppl 3:321-
Momenter fra egen praksis
• Somatisk utredning !
• Pasientens plager: Hva er det verste for deg? Hva bør bli
bedre? Ta plagene på alvor.
• Pårørende: Samspill med pasienten. Informasjon om
sykdommen. Behov for gruppetilbud, støttesamtaler.
Involver barna. Komparentinformasjon om bivirkninger,
medisininntak, hjelpebehov.
• Tilbud i kommunen : Dagssenter!! Miljøtjeneste.
• Opptrapping av KHE til maks dose pas. tåler.
Somatisk Utredning ved APSD
• Kroppslig undersøkelse inkludert BT (ortostatisk), puls, EKG,
vekt, hud, hørsel, syn, nevrologisk status, gangbildet
• Anamnese: vannlating, avføring
• CCT/CMRT: Metastaser? Angiom? Strategiske infarkter?
WML særlig frontal?
• Blodprøver: Anæmi, hypothyreose, hypovitaminose, Natrium ,
Kalsium , nyreinsuffisiens, inflammasjon (leuko , CRP),
tumormarker?
• Søvnforstyrrelser: Apnoe, RLS, REMsøvnatferdsforstyrrelse
• Kartlegging av smerter (MOBID 2 scale)
• Evaluering av aktuell medikasjon: interaksjoner, bivirkninger
Personsentrert omsorg
• Anne Marie Mork Rokstad. Nasjonalt kompetansesenter
for aldring og helse:
1.Anerkjennelse av menneskets absolutte verdi uavhengig
av alder eller kognitiv funksjon
2.En individuell tilnærming som vektlegger det unike hos det
enkelte menneske
3. Evnen til å forstå verden sett fra beboerens perspektiv
4. Støttende tilrettelegging av det psykososiale miljø på en
slik måte at den enkelte beboer kan oppleve trivsel og
velvære.

Personsentrert omsorg
Trøst Kjærlighet Identitet
Inklusjon Beskeftigelse Tilknytning





























