Embed Size (px)
Citation preview

Basics of Pacing Ruth Hickling, RN-BSN Tasha Conley, RN-BSN
The Cardiac Conduction
System

Cardiac Conduction System Review

Normal Conduction
P T
R
QS
PR Interval
QT Interval
ST segment
QRS Complex
PR segment
ST interval
Normal Conduction
P T
R
QS
PR Interval
QT Interval
ST segment
QRS Complex
PR segment
ST interval
Indications for Pacing Documented evidence of Arrhythmia and Symptoms
• Symptomatic Bradycardia • Sick Sinus Syndrome (AKA tachy/brady) • Sinus Arrest or Sinoatrial (SA) Exit Block • Atrial Fibrillation with slow V response or
s/p AVNA for AF with RVR • Atrioventricular Block
• First Degree (symptomatic) • Second Degree, Mobitz I and II • Third Degree or Complete Heart Block
• Carotid Sinus Hypersensitivity/Syncope

Possible Symptoms Syncope
Dizziness
Confusion
Fatigue
Shortness of Breath
Limited Exercise Tolerance

Keeping it Simple
If the Sinus Node Doesn’t Fire…
… then we need to pace the atrium

Keeping it Simple
If the AV node does not appropriately conduct…
...then we need to pace the ventricle

Pacemakers
1. Keep the heart from going too slow
2. Provide AV Synchrony
3. Aid in Chronotropic response
In a ‘Nut Shell’

Indications for ICD ImplantationSecondary Prevention • Prior Cardiac Arrest • Ventricular
Tachycardia • Ventricular
Fibrillation
Primary Prevention • Congenital Heart
Disease • Long QT Syndrome • Cardiomyopathy that
meets appropriate NYHE guidelines
Ischemic Non-Ischemic Idiopathic Hypertrophic

What makes up a Pacemaker / AICD
System?

• Pulse Generator• Battery• Circuitry • Case• Header
• Lead(s) • Systems can have up to
three leads depending on implant indication
Basic Components of Pacing/AICD System
Pacemaker

“Brain”
Components of a pacemaker pulse generator. Also called “the Can”

Single-Chamber System • The pacing lead is
implanted in the atrium
or ventricle, depending
on the chamber to be
paced and sensed

Dual Chamber Systems Have Two Leads
• One in the atrium
• One in the ventricle

Biventricular Pacing Systems Also called Cardiac Resynchronization Therapy (CRT) pacemakers have a Right ventricular lead and a left
ventricular lead. These leads force the ventricles
to contract at the same time for “resynchronization”
May not have atrial lead with
history of chronic atrial fibrillation
Implantable Cardiac Device Function and
Programming

Sensing What the device “sees” • Monitor the hearts intrinsic electrical activity
Think of a fence…
“Can’t see the hearts activity?!?”, (Undersensing)
“Sees too much!” (Oversensing)
“Ahhh, Just Right!” (Appropriate sensing)
EMI, Myopotential
Pacing The delivery of an electrical impulse to elicit contraction of the heart muscle. CAPTURE THRESHOLD – minimum amount of energy needed to elicit contraction of the heart. • Amplitude – How much energy (measured in Voltage) • Pulse Width – Over what time period (measured in ms)
Voltages are set to 2 times the amplitude of capture threshold to ensure safety

Pacing Parameters
Lower Rate Limit (LRL): Nominal - 60bpm Rest rate – 50bpm Pts with AF s/p AVNA 80bpm for 6 weeks PVCs Upper Rate Limit (URL): How fast device will pace Patient can have OWN intrinsic rates higher that programmed URL

Sensors – Rate Response (Not to be confused with “sensing”)
Provide appropriate increase in heart rate with activity for the those patients who have chronotropic incompetence “Accelerometer” • Spring board system • Measures heal strike
“Physiologic” • Only available in pacemakers • CLS (closed loop system) • Minute Ventilation – not
appropriate for patient’s on a ventilator

Magnet Response Pacemakers
• “Shuts the eyes of the
pacemaker” (Sensing) • Force A/V pacing at a
specific rate, which is dependent on the pacemaker manufacturer
(Ranging between 85-100bpm)
ICDs
• Temporarily deactivates ICD therapies

Basic Differences between Pacemakers and Defibrillators
Pacemakers Maintain HR, CO and
AV synchrony Pace at a specified rate
when magnet is applied Are not defibrillators
They do not stop fast
heart rates
Defibrillators All have pacemaker
component, but may not be utilized if no pacing indication
Treat sustained VT/VF with
pacing (ATP) and or shocks
Magnet application suspends detection for VT/VF and prevents treatment. It does not affect Pacing rates.

Keeping it Simple
• ICDs are intended to treat potentially life threatening arrhythmias.
• ICDs can function as a Pacemaker when pacing is indicated.

NBG Code NASPE/BPEG Generic
I II III IV V
Chamber(s) Paced
Chamber(s) Sensed
Mode(s) of Response
Programmable Functions
Antitachycardia Functions
A = Atrium A = Atrium T = Triggered R = Rate Modulated
P = Paced
V = Ventricle V = Ventricle I = Inhibited C = Communicating
S = Shocks
D = Dual (A&V)
D = Dual (A&V)
D = Dual M = Multiprogrammable
D = Dual (P&S)
O= None O = None O = None P = Simple Programmable
O = None
O = None

Common Pacing Modes Single Chamber
• VVI • VVIR • AAI • AAIR
Dual Chamber • DDD • DDDR • DDI • DDIR

V V I
V: ventricle is paced V: ventricle is sensed I: pacing is inhibited in response to a sensed event R: rate responsive This is a ventricular demand mode with artificial rate response
R

D D D D: both chambers are paced D: both chambers are sensed D: pacemaker will either inhibit or trigger in response to a sensed event R: rate responsive This is a dual chamber “universal” mode with artificial rate response
R

Atrial pace - Ventricular pace Atrial pace - Ventricular sense Atrial sense - Ventricular sense Atrial sense - Ventricular pace
Four Faces of DDD Pacing

DDD Pacing Example
Atrial Pace – Ventricular Pace
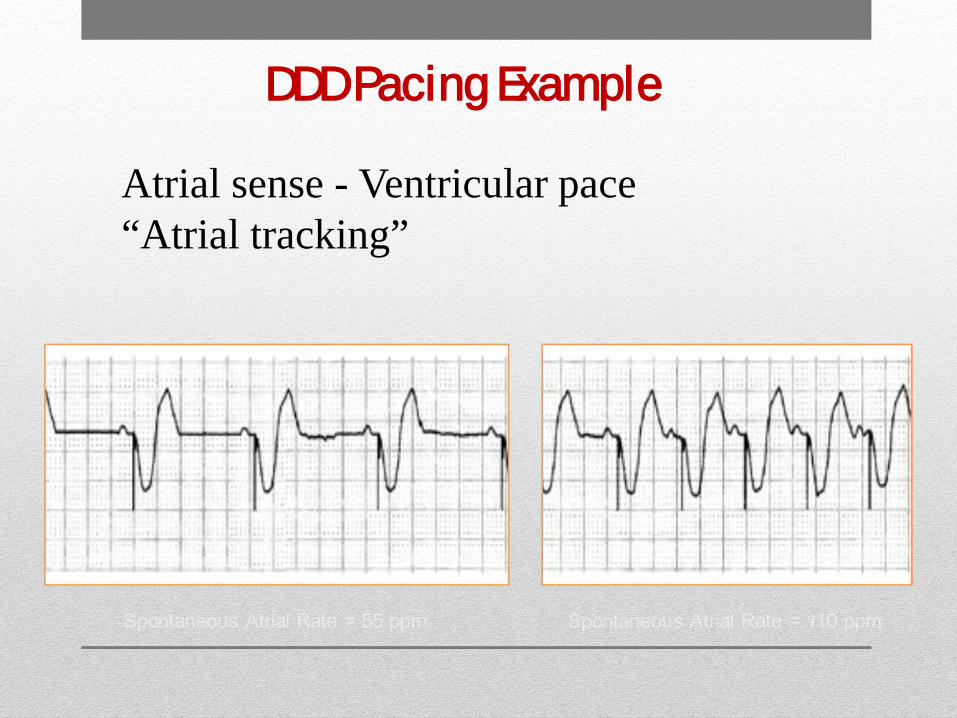
DDD Pacing Example
Atrial sense - Ventricular pace “Atrial tracking”
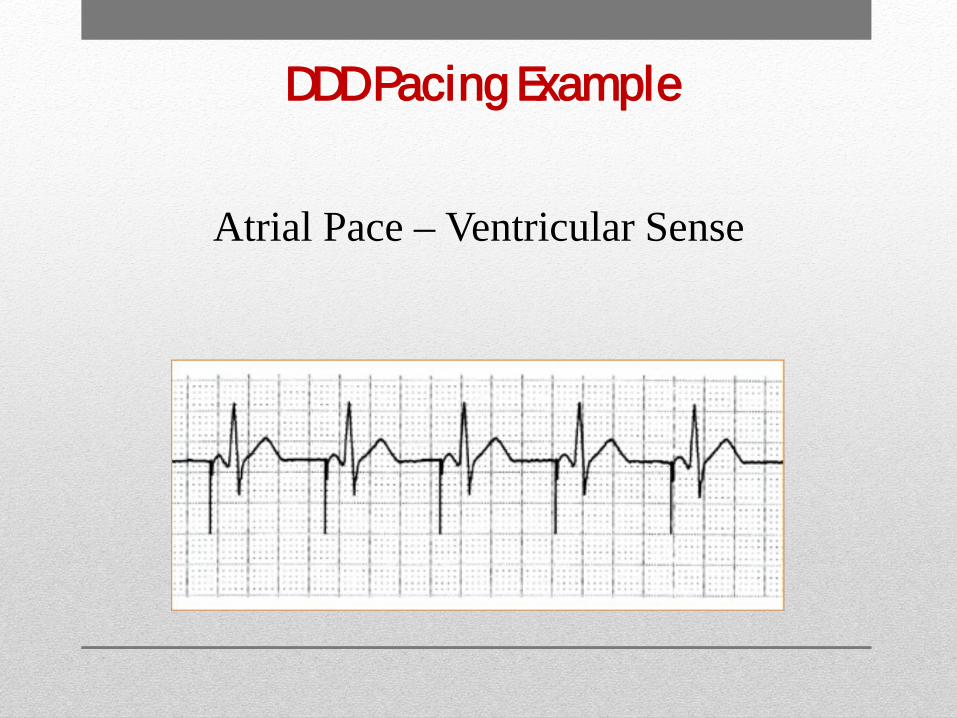
DDD Pacing Example
Atrial Pace – Ventricular Sense

Could this be normal DDD Pacemaker Function?
Normal sinus rhythm with no pacing
YES!

What About This?
Atrial Flutter with Variable V rate Absolutely!
Identifying Pacemaker/ICD Related Issues

Loss of Capture
What do you see?
Loss Of Capture Capture

Undersensing
What do you see?
Undersensed QRS
Loss Of Capture

More Undersensing
undersensing
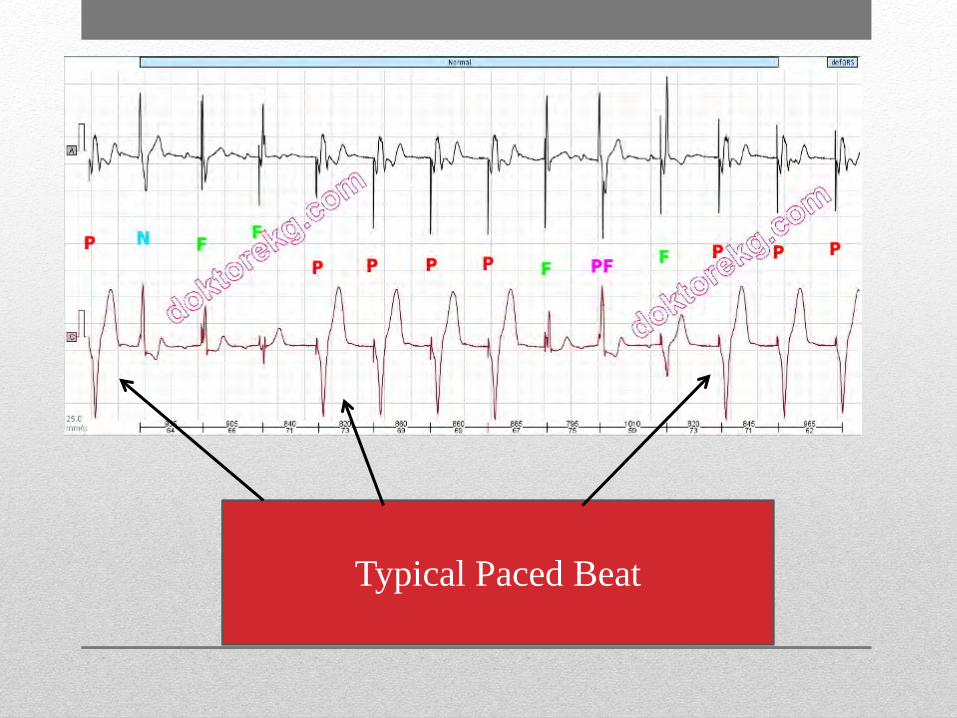
Typical Paced Beat

Normal and Psuedofusion look the same

Pseudofusion

Fusion beats can have several different looks

Helpful steps to take when calling for trouble shooting assistance
• Make sure the telemetry monitor is not undersensing beats such as a PVC.
• Make sure the “pacing spikes” are not artifact
• Please save copies or telemetry strips for questionable rhythms. • Often we can determine if device functionality is
an issue just by looking at these.
• Whenever possible, make sure to save 2 ECG channels.

New Advancements in the World of Cardiac Devices

Implantable Loop Recorders

Implantable Loop Recorder A Smaller version
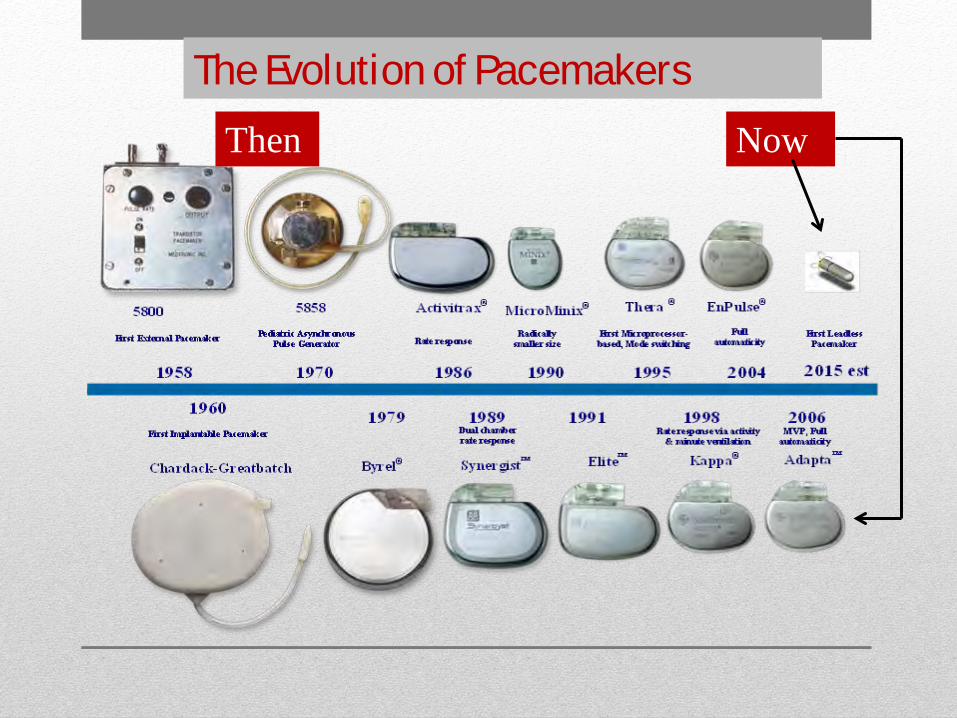
The Evolution of Pacemakers Then Now

Leadless Pacemakers

Progression of ICDs
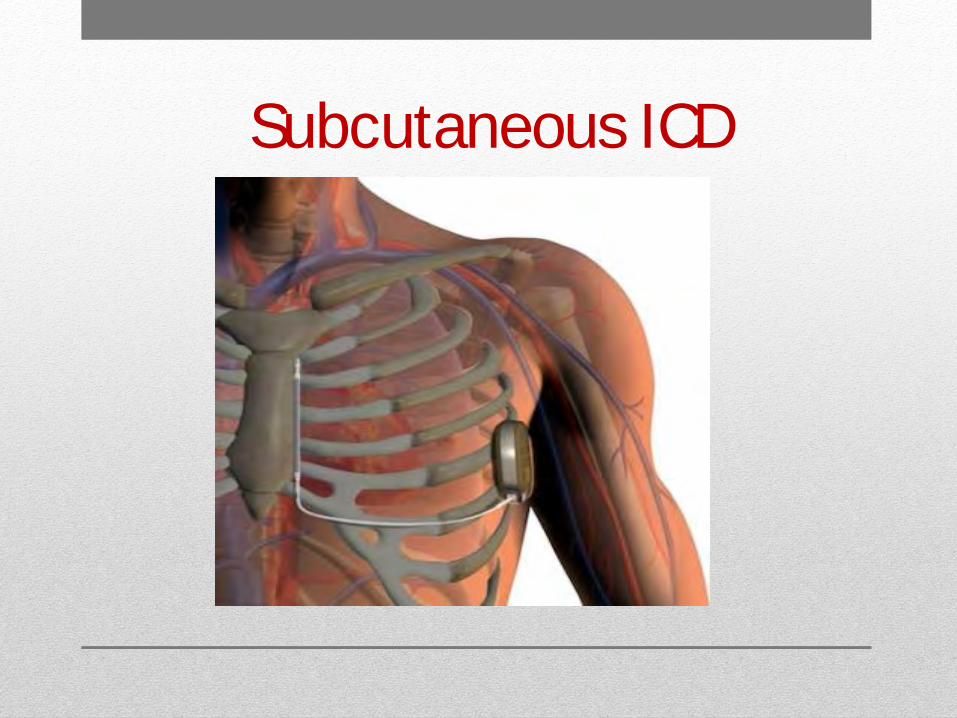
Subcutaneous ICD

It is always a good idea to have device settings posted above the head of the bed.
• Device settings can be obtained from the cardiac rounding
nurse • Signs for posting should be located at central stations on
your unit • Essential information lower and upper rate limits for pacing Intervention rates for VT and VF

Need Help? Questions or Concerns?
Page the Pacemaker Nurse (734) 670-1825 Available M-F 8am to 5pm After hours page appropriate company representative P

Questions?!?

References Biotronik (n.d.). Closed Loop Stimulation (CLS). Retrieved February 16, 2015 from http://www.biotronik.com/wps/wcm/connect/en_us_web/biotronik/sub_top/ healthcareprofessionals/products/bradycardiatherapy?p=http://www.biotr onik.com/wps/wcm/connect/en_us_web/biotronik/sub_top/healthcareprofes sionals/products/bradycardiatherapy/closed_loop_stimulation/page_closed _loop_stimulation&pw=974&pt= Boston Scientific. (2011). Restoring Appropriate Rate for Chronotropic Incompetence. Retrieved February 16, 2015 from http://www.chronotropic- incompetence.eu/en/treatment-of-chronotropic-incompetence Kutalek, S., Sharma, A., McWilliams, M., Wilkoff, B., Leonen, A., Hallstrom, A., & Kudenchuk, P. (2008). Effect of pacing for soft indications on mortality and heart failure in the dual chamber and VVI implantable defibrillator (DAVID) trial. Pacing & Clinical Electrophysiology, 31(7), 828-837 Medtronic, (2013). Clinical gudelines and inidcations. Retrieved February 16, 2015 from http://www.medtronic.com/for-healthcare-professionals/products-therapies/cardiac- rhythm/therapies/tachyarrhythmia-management/clincial-guidelines-indications/ The NBG Code, (n.d.). The NBG Code: NASPE?BEPG generic. Retrieved February 16, 2015 from http://www.pacemaker.vuurwerk.nl/info/nbg_code__naspe.htm





























