Embed Size (px)
Citation preview

Basic Coronary Artery Anatomy
Basic Coronary Artery Anatomy
Paul Fefer, MD.Interventional Cardiology Unit
Sheba Medical Center, Tel Hashomer
Courtesy of Frederick Feit, MD
Paul Fefer, MD.Interventional Cardiology Unit
Sheba Medical Center, Tel Hashomer
Courtesy of Frederick Feit, MD
The Cardiovascular Research FoundationThe Cardiovascular Research Foundation Transcatheter Cardiovascular TherapeuticsTranscatheter Cardiovascular Therapeutics
Medtronic Fellows PCI PrimerMedtronic Fellows PCI Primer

Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy
Sternocostal Aspect

Diaphragmatic Aspect
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Right Coronary ArteryRight Coronary Artery
• OriginRight aortic sinus (lower origin than LCA)
• CourseDown right AV groove toward crux of the heart, gives off PDA (85%) from which septals arise, continues in LAV groove giving off posterior LV branches (posterolaterals). PDA may originate more proximally, bifurcate early or be small with part of “its territory” supplied by an acute marginal branch.
• Supplies25% to 35% of Left Ventricle
• OriginRight aortic sinus (lower origin than LCA)
• CourseDown right AV groove toward crux of the heart, gives off PDA (85%) from which septals arise, continues in LAV groove giving off posterior LV branches (posterolaterals). PDA may originate more proximally, bifurcate early or be small with part of “its territory” supplied by an acute marginal branch.
• Supplies25% to 35% of Left Ventricle
Basic AnatomyBasic Anatomy

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Right Coronary ArteryRight Coronary Artery
• Conus Arteryusually very proximal; (~50% have a separate origin)-courses anteriorly and upward over the RV outflow tract toward the LAD. May be an important source of collaterals.
• SA Nodal Artery(~60%) usually 2nd branch of RCA-courses obliquely backward through upper portion of atrial septum and anteromedial wall of the RA-supplies SA node, usually RA and sometimes LA.
• Conus Arteryusually very proximal; (~50% have a separate origin)-courses anteriorly and upward over the RV outflow tract toward the LAD. May be an important source of collaterals.
• SA Nodal Artery(~60%) usually 2nd branch of RCA-courses obliquely backward through upper portion of atrial septum and anteromedial wall of the RA-supplies SA node, usually RA and sometimes LA.
Other BranchesOther Branches

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Right Coronary ArteryRight Coronary Artery
• Right Ventricular (Acute Marginal) Branches)Arise from mid RCA; supply anterior RV; may be a collateral source.• AV Nodal Artery
Arises at or near crux; supplies AV node.• PDA
Supplies inferior wall, ventricular septum, posteromedial papillary muscle.
• Right Ventricular (Acute Marginal) Branches)Arise from mid RCA; supply anterior RV; may be a collateral source.• AV Nodal Artery
Arises at or near crux; supplies AV node.• PDA
Supplies inferior wall, ventricular septum, posteromedial papillary muscle.
Other BranchesOther Branches

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Right Coronary ArteryRight Coronary Artery
• LAO (30) Cranial(30)particularly for distal bifurcation (AP Cranial may be better).
• RAOmain shaft; cranial enhances distal vessels and very proximal; caudal may help with Shepherd’s crook.
• Lateralbifurcations with RV branches-distal bifurcation, particularly with cranial.
• LAO (30) Cranial(30)particularly for distal bifurcation (AP Cranial may be better).
• RAOmain shaft; cranial enhances distal vessels and very proximal; caudal may help with Shepherd’s crook.
• Lateralbifurcations with RV branches-distal bifurcation, particularly with cranial.
Optimal View(s)Optimal View(s)

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
LAO Cranial Angiogram of RCALAO Cranial Angiogram of RCA
PDAPDAPDAPDA
Acute MarginalAcute MarginalAcute MarginalAcute Marginal

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
RAO Angiogram of RCARAO Angiogram of RCA

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Native RCA Lateral ViewNative RCA Lateral View
Acute Acute MarginalMarginalAcute Acute MarginalMarginal
Main RCAMain RCAMain RCAMain RCA
Demonstrating Origin of Acute MarginalDemonstrating Origin of Acute Marginal

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
AP Cranial View of Distal RCAAP Cranial View of Distal RCA
PDAPDAPDAPDA
AV
Gro
ove
AV
Gro
ove
AV
Gro
ove
AV
Gro
ove
RPL 1RPL 1RPL 1RPL 1
RPL 2RPL 2RPL 2RPL 2

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Left Coronary ArteryLeft Coronary Artery
• Originupper portion of left aortic sinus just below the sinotubular ridge. Typically 0-10 mm in length. Rarely no LM (separate origins).
• Catheterization Technique“The Judkins’ 4-Left coronary catheter will find the LCA orifice unless thwarted by the operator”. Just in case-other Judkins sizes for smaller or larger aortas; Amplatz, XB type curves. Watch for “damping”; For separate ostia-separate catheters, larger for Cx, or counterclockwise rotation for LAD.
• Optimal ViewsLAO caudal and cranial; AP-caudal, cranial or flat. Limit views. May need IVUS
• Originupper portion of left aortic sinus just below the sinotubular ridge. Typically 0-10 mm in length. Rarely no LM (separate origins).
• Catheterization Technique“The Judkins’ 4-Left coronary catheter will find the LCA orifice unless thwarted by the operator”. Just in case-other Judkins sizes for smaller or larger aortas; Amplatz, XB type curves. Watch for “damping”; For separate ostia-separate catheters, larger for Cx, or counterclockwise rotation for LAD.
• Optimal ViewsLAO caudal and cranial; AP-caudal, cranial or flat. Limit views. May need IVUS
Left Main Coronary ArteryLeft Main Coronary Artery

Sternocostal Aspect
77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.

Diaphragmatic Aspect
77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Left Anterior Descending ArteryLeft Anterior Descending Artery• Course
down the anterior interventricular groove-usually reaches apex. In 22% of cases does not reach apex.
• Branchesseptals and diagonals-supply lateral wall of LV, anterolateral papillary muscle; 37% have median ramus (courses like 1st diagonal).
• LADSupplies anterolateral, apex and septum; ~45%-55% of left ventricle.
• Coursedown the anterior interventricular groove-usually reaches apex. In 22% of cases does not reach apex.
• Branchesseptals and diagonals-supply lateral wall of LV, anterolateral papillary muscle; 37% have median ramus (courses like 1st diagonal).
• LADSupplies anterolateral, apex and septum; ~45%-55% of left ventricle.

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Left Circumflex ArteryLeft Circumflex Artery• Origin
from distal LMCA.• Course
down distal left AV groove.• Branches
obtuse marginal, posterolaterals-supply posterolateral LV, anterolateral papillary muscle. SA node artery-38%.
• Supplies15%-25% of LV, unless dominant (supplies 40-50% of LV).
• Originfrom distal LMCA.
• Coursedown distal left AV groove.
• Branchesobtuse marginal, posterolaterals-supply posterolateral LV, anterolateral papillary muscle. SA node artery-38%.
• Supplies15%-25% of LV, unless dominant (supplies 40-50% of LV).

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Left Coronary ArteryLeft Coronary Artery
• AP (30)CaudalLMCA, proximal LAD, Cx, distal LAD. Poor for mid LAD- RAO may be useful.
• AP (40)CranialLMCA, LAD, diagonals, septals, distal Cx-may need RAO to separate LAD and Cx.
• (45)LAO (35) CranialLMCA, LAD, diagonals, septals, and distal Cx.
• (45)LAO (30) CaudalLMCA, Cx,and prox LAD.
• Laterals (cranial, caudal)may be helpful.
• AP (30)CaudalLMCA, proximal LAD, Cx, distal LAD. Poor for mid LAD- RAO may be useful.
• AP (40)CranialLMCA, LAD, diagonals, septals, distal Cx-may need RAO to separate LAD and Cx.
• (45)LAO (35) CranialLMCA, LAD, diagonals, septals, and distal Cx.
• (45)LAO (30) CaudalLMCA, Cx,and prox LAD.
• Laterals (cranial, caudal)may be helpful.
Optimal ViewsOptimal Views

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
AP Caudal View of LCAAP Caudal View of LCA
LADLAD
CircCirc

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
SeptalSeptalSeptalSeptal
LADLADLADLAD
CxCxCxCx
DiagonalDiagonalDiagonalDiagonal
AP Cranial View of LCAAP Cranial View of LCA

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
AP Cranial LCA AngiogramAP Cranial LCA Angiogram
SeptalSeptalSeptalSeptal DiagonalsDiagonalsDiagonalsDiagonals
LADLADLADLAD
LMCALMCALMCALMCA CxCxCxCx

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
CircCircCircCirc
DiagonalDiagonalDiagonalDiagonalLADLADLADLAD
LAO Cranial View of LCALAO Cranial View of LCA

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
LAO Caudal View of LCALAO Caudal View of LCA
CircCircCircCirc
LADLADLADLAD Median RamusMedian RamusMedian RamusMedian Ramus

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Dominance:Dominance:
• Definition 1:the coronary artery which reaches the crux of the heart and then gives off the PDA • Definition 2: (Allows for codominance)
the artery which gives off the PDA as well as a large posterolateral branch
• Definition 1:the coronary artery which reaches the crux of the heart and then gives off the PDA • Definition 2: (Allows for codominance)
the artery which gives off the PDA as well as a large posterolateral branch

LeftDominant
Circulation
LeftDominant
Circulation
77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
LCA AngiogramLCA Angiogram
Distal LADDistal LADDistal LADDistal LAD
Prox LADProx LADProx LADProx LADLMLMLMLM
OMOMOMOM
Distal CxDistal CxDistal CxDistal Cx
Occluded Median RamusOccluded Median RamusOccluded Median RamusOccluded Median Ramus
Dominant Cx AP CaudalDominant Cx AP Caudal

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
LCA Angiogram-Dominant Cx LAO-CaudalLCA Angiogram-Dominant Cx LAO-Caudal
Distal LADDistal LADDistal LADDistal LAD
LMLMLMLM
Prox CxProx CxProx CxProx Cx
LPDALPDALPDALPDA
OccludedOccludedMedianMedianRamusRamus
OccludedOccludedMedianMedianRamusRamus
Prox LADProx LADProx LADProx LAD

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
The Coronary Arteries Are ComplementaryThe Coronary Arteries Are Complementary
• Large PDA Small LAD• Huge Cx (posterolaterals) Small RCA continuation in AV Groove• Etc, etc, etc…..
• Large PDA Small LAD• Huge Cx (posterolaterals) Small RCA continuation in AV Groove• Etc, etc, etc…..

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Wrap Around LADWrap Around LAD

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Short LAD/Large RCA with Apical ExtensionShort LAD/Large RCA with Apical Extension

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
BYPASS GRAFTSBYPASS GRAFTS
• SVGLeft coronary grafts generally arise from left side of the aorta. Best cannulated with Judkins’ Right, IMA, LCB or MP.Right sided grafts-arise from right side of
the aorta-MP usually best.
• IMAdon’t forget to check subclavians.
• SVGLeft coronary grafts generally arise from left side of the aorta. Best cannulated with Judkins’ Right, IMA, LCB or MP.Right sided grafts-arise from right side of
the aorta-MP usually best.
• IMAdon’t forget to check subclavians.
All distal vessels must be accounted for; op notes and old films are extremely helpful.All distal vessels must be accounted for; op notes and old films are extremely helpful.

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
SVG-OM-LAO CaudalSVG-OM-LAO Caudal
Demonstrating Graft OstiumDemonstrating Graft Ostium
OstiumOstium

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
SVG-OM 1 AP CaudalSVG-OM 1 AP Caudal
Demonstrating AnastomosisDemonstrating Anastomosis
SVGSVGSVGSVG

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
LIMA to LADLIMA to LAD
Origin from left subclavian (AP Cranial)Origin from left subclavian (AP Cranial)

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
LIMA to LADLIMA to LAD
Distal Anastomosis-AP CranialDistal Anastomosis-AP Cranial
LIMALIMALIMALIMA
LADLADLADLAD

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Left Subclavian Artery StenosisLeft Subclavian Artery Stenosis
77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
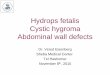
RIMA to RCARIMA to RCA

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
RIMA to RCARIMA to RCA

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Occluded Left-sided SVGOccluded Left-sided SVG

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Native LCA AP CaudalNative LCA AP Caudal
Stump of original Stump of original SVG to OM 1SVG to OM 1Stump of original Stump of original SVG to OM 1SVG to OM 1

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
SVG to OMSVG to OM
Lesion 1Lesion 1Lesion 1Lesion 1
Lesion 2Lesion 2Lesion 2Lesion 2

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
SVG to OMSVG to OMSlight change of view to demonstrate
unequivocal severity of lesionSlight change of view to demonstrate
unequivocal severity of lesion
Lesion 1Lesion 1Lesion 1Lesion 1
Lesion 2Lesion 2Lesion 2Lesion 2

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
SVG to RCASVG to RCA
Multipurpose Technique -LAOMultipurpose Technique -LAO
SVGSVGSVGSVG

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Ulcerated PlaqueUlcerated Plaque

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
LCA AP CaudalLCA AP Caudal
Severe stenosisSevere stenosisSevere stenosisSevere stenosis
Distal LADDistal LADwith slow flowwith slow flowDistal LADDistal LADwith slow flowwith slow flow

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Thrombus In LADThrombus In LAD
Post-NTG-Thrombus has migrated distally but still adherentPost-NTG-Thrombus has migrated distally but still adherent
ThrombusThrombusThrombusThrombus

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
AP Cranial Thrombus In LADAP Cranial Thrombus In LAD
ThrombusThrombusThrombusThrombus

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Embolization of Thrombus During AngiographyEmbolization of Thrombus During Angiography
ThrombusThrombusThrombusThrombus

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Calcified Native RCACalcified Native RCA(LAO Cranial)
“Bone Island” Simulating Thrombus(LAO Cranial)
“Bone Island” Simulating Thrombus

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Myocardial BridgingMyocardial Bridging
• Almost always LAD
• Occurs in 5-12% of patients
• Usually not hemodynamically significant
• Almost always LAD
• Occurs in 5-12% of patients
• Usually not hemodynamically significant
Intramyocardial SegmentIntramyocardial Segment

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Myocardial BridgingMyocardial Bridging
LCA-RAO ProjectionLCA-RAO Projection
LAD DiastoleLAD DiastoleLAD DiastoleLAD Diastole LAD SystoleLAD SystoleLAD SystoleLAD Systole

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Coronary Artery FistulaCoronary Artery Fistula
• Origin50% RCA.• Clinical Syndromes: CHF, endocarditis,
ischemia, and rupture of aneurysmal fistula. 50% are asymptomatic.
• Drainage: RV-41%; RA-26%; PA-17%; LV-3%, and SVC-1%.
• Origin50% RCA.• Clinical Syndromes: CHF, endocarditis,
ischemia, and rupture of aneurysmal fistula. 50% are asymptomatic.
• Drainage: RV-41%; RA-26%; PA-17%; LV-3%, and SVC-1%.

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Coronary Artery FistulaCoronary Artery FistulaLCA-RAO Projection
LAD to PA FistulaLCA-RAO Projection
LAD to PA Fistula
LADLADLADLAD
PAPAPAPA
FistulaFistulaFistulaFistula

Anomalous Origin of LCA from theRight Sinus of Valsalva
Anomalous Origin of LCA from theRight Sinus of Valsalva
• Rare• Course relative to great vessels is variable
and must be defined. If interarterial, surgical therapy is warranted.
• Rare• Course relative to great vessels is variable
and must be defined. If interarterial, surgical therapy is warranted.
77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.

Anomalous Origin of RCA from Left Coronary Sinus
Anomalous Origin of RCA from Left Coronary Sinus
• Rare• Arises anterior to the origin of the LCA• Engage with Left Amplatz, or Left Judkins’• RCA runs an interarterial course• Usually benign
• Rare• Arises anterior to the origin of the LCA• Engage with Left Amplatz, or Left Judkins’• RCA runs an interarterial course• Usually benign
77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.

Normal and Anomalous Origins of the Coronary Arteries
Normal and Anomalous Origins of the Coronary Arteries
77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Benign Anomalies (0.5-1%)Benign Anomalies (0.5-1%)
• Left Circumflex from right Sinus of ValsalvaMost common “benign” anomalyCircumflex courses behind aorta
• High Anterior Origin of RCAAbove sinotubular ridge
• Left Circumflex from right Sinus of ValsalvaMost common “benign” anomalyCircumflex courses behind aorta
• High Anterior Origin of RCAAbove sinotubular ridge

77thth Annual Interventional Cardiology Self-Assessment Course at TCT2004 Annual Interventional Cardiology Self-Assessment Course at TCT2004
Basic Coronary Artery AnatomyBasic Coronary Artery Anatomy: Frederick Feit, M.D. : Frederick Feit, M.D.
Anomalous Circumflex ArteryAnomalous Circumflex Artery



![Aportes para conmemorar el Levantamiento del Gueto de ......Liderado por el polaco Mordejai Anielewicz, miembro del movimiento juvenil judío Hashomer Hatzair [La Guardia de la juventud],](https://img.dokumen.tips/doc/110x75/60c11374ee3108307571e2d0/aportes-para-conmemorar-el-levantamiento-del-gueto-de-liderado-por-el-polaco.jpg)
![arXiv:1707.06053v2 [cs.CV] 20 Jul 2017 · 2 Sheba Medical Center, Diagnostic Imaging Department, Tel Hashomer, Israel 3 Engineering Faculty, Bar-Ilan University, Israel Abstract](https://img.dokumen.tips/doc/110x75/5f4b78873807d920b93030e7/arxiv170706053v2-cscv-20-jul-2017-2-sheba-medical-center-diagnostic-imaging.jpg)