-
7/27/2019 Avian Malaria.docx
1/6
Avian Malaria
Introduction
Malaria is a protozoal disease caused by members of the
genus
Plasmodium. Infections may occur in both humans and
animals.Approximately 350-500 million people are infected
annually,with 1.3 million deaths. It is endemic to parts of Asia,
Africa,Central and South America, and certain Caribbean islands.
Thereare four species ofPlasmodium that cause disease in people:
P.falciparum, P. vivax, P. ovale, P. malariae. Plasmodium sp.
mayalso infect primates, rodents, reptiles, and birds. Many birds
canserve as a definitive host for these parasites. Plasmodium can
bepathogenic to penguins, domestic poultry, ducks,
canaries,falcons, and pigeons, but is most commonly carried
asymptomatically by passerine birds. Avian malaria has
aworldwide distribution and is of great economic significance is
tothe poultry industry. Organisms such as P. gallinaceum,
P.juxtanucleare and P. durae may cause up to 90% mortality
inpoultry. Incidentally, birds with avian malaria have been used
asmodel systems for studying the pathogenesis and treatment
ofmalaria in humans.
Clinical Signs
Infected birds are often weak, depressed, dyspneic andanorexic.
Birds may have abdominal protrusion (due tohepatosplenomegaly) and
ocular hemorrhage. Central nervoussystem ischemia may occur with P.
gallinaceum due to occlusionof capillaries by exoerythrocytic
schizonts in heavily parasitizedendothelial cells. Hemolytic
anemia, often accompanied byleukocytosis, lymphocytosis, and
hemoglobinuria, may also bepresent. Coma and death may occur
quickly when the parasiteburden is high. However, many birds,
especially passerines, donot become ill and play an important role
as asymptomatic
carriers of the parasite.
Life Cycle
Plasmodium may exploit several genera of mosquitoes
(Culex,Anopheles, Culiceta, Mansonia, and Aedes) as vectors
andintermediate hosts. The mosquito inoculates the bird
withsporozoites that enter the birds reticuloendothelial system.
Eachsporozoite develops into thousands of merozoites
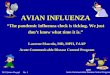
(pre-erythrocytic cycle) (Figure 1). These merozoites rupture
theirhost cell and invade endothelial cells or other cells of
the
reticuloendothelial system to complete another cycle
ofreplication. The merozoites then rupture that host cell and
enter
-
7/27/2019 Avian Malaria.docx
2/6
erythrocytes in the blood stream. This initiates
theintraerythrocytic cycle. Merozoites multiply in the RBC, forming
aschizont (shizogony). The schizont will rupture, killing the
RBCand releasing the merozoites to infect more RBCs.
Duringschizogony, the parasites feed on the RBC cytoplasm,
ingesting
hemoglobin which produces brown pigment granules. The
intra-erythrocytic cycles continue until the host dies or the
parasitesare suppressed by host immunity. After the initial cycles
inerythrocytes, a few merozoites develop into sexual
cells(microgametes and macrogametes) with each new cycle. Thesexual
cells are maintained in the RBC until they are consumedby a
mosquito with its blood meal.
Figure 1: Liver impression smear froma Penguin. Two
macrophagescontaining numerous Plasmodiummerozoites.
The sex cells are released in the mosquitos midgut.
Fertilizationand zygote formation occurs when a microgamete
encounters amacrogamete. The zygote matures into an elongated
mobile cellthat crosses the midgut wall. This cell is called an
ookinete. Theookinete forms an oocyst on the outer wall of the
midgut. Thenucleus of the oocyst divides into thousands of spindle
shapedsporozoites. The oocyst then bursts and releases
thesporozoites, some of which migrate to the salivary gland
wherethey are injected into a bird during the mosquitos blood
meal.
While most avian infections occur through the bite of amosquito,
it is possible for a direct bird-to-bird transmission to
-
7/27/2019 Avian Malaria.docx
3/6
occur. Schizogony occurs in the RBC and, therefore,
blood-to-blood transfer without the intermediate host can result
ininfection. The life cycle of avian malaria is very similar to
thatseen in infected human beings. However, birds (unlikemammals)
suffer from repeated cycles of pre-erythrocytic
merogony with reinvasion of reticuloendothelial cells
byerythrocytic forms.
Clinicopathologic Features and Diagnosis
Experimental infection of domestic fowl resulted in
peakparasitemia six days post-infection in most birds. The birds
werefebrile and anemic (hematocrit
-
7/27/2019 Avian Malaria.docx
4/6
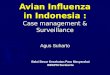
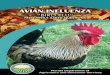
The intraerythrocytic gametocytes ofPlasmodium can easily
beconfused with those ofHaemoproteus because they both
containrefractive yellow to brown pigmented granules (Figures 3
and4).
Figure 3: Plasmodiumgametocytes in avianblood. Note the
smallersize when compared toHemoproteus organisms.
Figure 4:Hemoproteus inavian blood. Typicallylarger than
Plasmodiumgametocytes and oftenhave a characteristiccanoe shape
that wrapsaround the erythrocytenucleus.
Features that can help distinguish between the two
infectionsinclude:
Plasmodium gametocytes are smaller in size thanHaemoproteus
organisms, usually occupying less than one-halfof the host cell
cytoplasm
Some Plasmodium gamonts displace the RBC nucleus(Haemoproteus
does not)
Plasmodium may undergo schizogony in the peripheral
blood(Haemoproteus does not)
Plasmodium parasites can be found in cells other
thanerythrocytes (thrombocytes, leukocytes, and endothelial
cells).
-
7/27/2019 Avian Malaria.docx
5/6
In birds that die peracutely, organisms may be few to sparse
inthe blood. In these cases, schizonts can be found in
capillariesby examining impression smears of brain, lung, liver,
andspleen.
PCR has also been used to diagnose Plasmodium. However,
thisdiagnostic test is most often used in a research setting.
Treatment
Note: Treatment of animals should only be performed bya licensed
veterinarian. Veterinarians should consult thecurrent literature
and current pharmacologicalformularies before initiating any
treatment protocol.
Affected flocks can be treated with Chloroquine
(5-10mg/kg)potentiated with primaquine (0.3mg/kg). Chloroquine can
alsobe added to the drinking water at a dose of 250mg/120ml.Grape
or orange juice may be needed to override the bitter tasteof the
medication. Quinacrine at a dose of 1.6 mg/kg given IMfor 5 days is
another treatment possibility. Additional treatmentsinclude
sulfonamides combined with trimethoprim,pyrimethamine, and
chlorguanil. Due to strain differences insusceptablity, different
anti-malarial drugs can be tried. It is
important to remember that malaria can be prevented byscreening
chicken houses to prevent contact with the mosquitovectors.
References
Aiello SE (ed): The Merck Veterinary Manual, 8th ed.
NationalPublishing, Philadelphia, PA, 1998
Barriga O: Parasitology for Practitioners , 2nd ed.
InternationalGroup, Minnesota, 1997.
Campbell T: Avian Hematology and Cytology. Iowa StateUniversity
Press, Ames, 1998.
Kaufmann J: Parasitic Infections of Domestic Animals:
ADiagnostic Manual, Birkhauser Verlag, 1996.
Richie B, Harrison G, Harrison L: Avian Medicine: Principles
andApplications. Wingers Publishing, Lake Worth FL, 1997.
Slater LB. Malarial Birds: Modeling Infectious Human Disease
inAnimals. Bull. Hist. Med., 2005, 79: 261-294.
-
7/27/2019 Avian Malaria.docx
6/6
Williams RB: Avian Malaria: clinical and chemical pathology
ofPlasmodium gallinaceum in the domesticated fowl Gallus
gallus.Avian Pathology February 2005 34(1), 29-47.
Acknowledgement