Embed Size (px)
Citation preview

Autopsies in outbreak
situations
Jeannette Guarner, MD
Department of Pathology and Laboratory Medicine
Emory University

Conflicts: none
Disclosures:
Paid by The Emory Clinic
Worked at CDC 1997-2007, now guest researcher
Brought up in Mexico, thus funny accent
Husband, at Emory University, Chair of Global Health
Images, own and from CDC:
http://phil.cdc.gov/phil/home.asp
http://dpd.cdc.gov/dpdx/HTML/Image_Library.htm
In the past 12 months, I have not had a significant financial interest or other
relationship with the manufacturer(s) of the product(s) or provider(s) of the
service(s) that will be discussed in my presentation.
This presentation will include discussion of diagnostic devices that have been
approved by the FDA.

Objectives
When is an autopsy important for
epidemiologic purposes?
What are the tissues that need to be
obtained?
Who does these autopsies?

Diseases that need to be reported
immediately
Animal or human
cases of:
Anthrax
Plague
Viral hemorrhagic
fevers: Ebola,
Marburg, Lassa,
Congo-Crimean

Diseases that need to be reported
immediately
Human cases of:
Botulism
Melioidosis
Smallpox
Tularemia
Novel influenza
viruses

Other reportable diseases STDs: (HIV, chancroid,
gonococcal infections, syphilis)
Encephalitis & meningitis (prions, viral, bacterial, fungal or parasitic)
Diarrheal bacterial diseases: Salmonella, E. coli 0157, Shigella, Vibrio, Campylobacter, Yersinia
Tuberculosis, leprosy
Invasive disease by: streptococci, meningococci, H. influenzae, S. aureus
Miscellaneous:
Rickettsia, Anaplasma, Ehrlichia, Coxiella, C. psittaci, C. trachomatis,
Listeria, Brucella, Leptospira, Bordetella, Borrelia, Legionella
Fungal: coccidioidomycosis
GI parasites: giardiasis, amebiasis, cryptosporidiosis, cyclosporiasis
Blood parasites: malaria, babesia
Viral diseases of childhood: mumps, measles, rubella, chickenpox—hospitalizations & deaths)
Hepatitis (A through E)
Miscellaneous: dengue, yellow fever, rabies, polio
Food poisoning related (ciguatera, scombroid, paralytic shellfish poisoning)

Other reportable diseases
Occurrence of any unusual disease
Outbreaks of any disease
Who usually
does the
reporting?

Recipient
17 years old male.
Use of allogenic tendon tissue
to repair of anterior cruciate ligament.
Admitted one week later for fever, chills, and pain and erythema around the knee incision.
Taken to surgery for debridement of necrotic tissue (muscle and allograft).
Streptococcus pyogenes was cultured from blood and surgical wound.

During the hospitalization the patient had persistent fever and fluid in the knee. The patient was treated with antibiotics.
The case is reported to CDC for investigation of transplant associated infection:
Was there contamination?
(donor, tissue collection, tissue bank, surgery...)

Retrospective review of donor
33 years old male with history of surgery to cervical vertebrae one month before death.
Seen by physician because of pain in back at the level of the chest, nausea, and vomiting.
Treated with tramadol and cyclobenzaprin.
Diagnosis: allergic reaction.
Sent to hospital for treatment but expires in transit.
Autopsy had been performed by the ME
He donates soft tissues and bone.

Autopsy of the donor:
Severe coronary atherosclerosis.
Focal bronchopneumonia.
Drug toxicity is considered the cause of death..
As part of the CDC investigation, autopsy material (paraffin blocks) are obtained from the donor for testing.

lung liver
Lee EH, et al. Invasive group-A streptococcal infection in an allograft
recipient. A case report. J Bone Joint Surg Am. 2007;89:2044-7.


In May 2004, 3
patients that had
received
transplants die of
encephalitis.
Autopsies
performed in
academic center.

Negative IHC tests for: enteroviruses,
arenaviruses, Chagas, toxoplasmosis,
herpes, flaviviruses…

Retrospective review of charts:
Common donor hospitalized for nausea,
vomiting, fever, and altered mental status.
Cocaine is found in urine. CT shows
subarachnoid hemorrhage.
All patients receiving organs (kidney and liver)
developed encephalitis that ended in coma and
death 3 weeks later.

A 4th patient that received a liver from another
donor also dies with rabies encephalitis.
Epidemiologic investigation showed that rabies
transmission to the 4th patient was through an
iliac artery fragment obtained from the donor
that had transmitted rabies to the other
recipients.

Kidney Home
Confusion
Agitation
Myoclonus
Donor
X
April - June, 2004
Liver Home
4-2
9
5-2
5-5
5-8
5-1
1
5-1
4
5-1
7
5-2
0
5-2
3
5-2
6
5-2
9
6-1
6-4
6-7
6-1
0
6-1
3
6-1
6
6-1
9
6-2
2
Kidney Home X
X
Home
X
X
Fever
Vent
Hemodynamic
instability
Transplant
nephrectomy
Mild
rejection Abdominal
- flank pain
Appendectomy
Agitation
seizures
Vent
Diffuse tremors
sleepiness
I&D of liver
abscess
Hepatic
artery
revision
Agitation
Seizures
Fever Delirium
Vent
Hemodynamic
instability
Fever
Fever
Vent
Hemodynamic
instability
Iliac Artery
Cyclosporin A
Sirolimus
Prednisone
Tacrolimus
Mycophenolate
mofetil Prednisone
Tacrolimus
Mycophenolate
mofetil Prednisone
Tacrolimus
Mycophenolate
mofetil Prednisone


Srinivasan A, et al. Transmission of Rabies Virus from an Organ Donor
to Four Transplant Recipients. N Engl J Med 2005;352:1103-1111.


October 2003
Report of deaths in children due to respiratory
disease in November and December.
Tested positive for H3N2 influenza A virus.
Surveillance is increased and included cases
from late September, 2003 to May, 2004.
153 deaths from 40 states of patients < 18
years old

Pathology of upper respiratory tract
Congestion 45/48 cases (94%)
Mononuclear inflammation in
submucosa 33 (69%)
Hemorrhage 25 (52%)
Epithelial necrosis 22 (46%)
Guarner J, et al Histopathologic
and immunohistochemical
features of influenza virus
infections in children during the
2003-04 season. Clin Infect Dis
2006;43:132-140

Interstitial inflammation 36/55 cases (65%)
Intraalveolar edema 36 (65%)
Intraalveolar hemorrhage 31 (56%)
Diffuse alveolar damage 38 (69%)

Location:
Bronchoepithelial cells
staining in 25 cases
Glandular cells staining in 8
Staining of cells in alveoli in
6
Amount:
15 (55%) significant
12 (44%) rare (2 to 3 cells)


San Diego, March 2009
10 year old presents with fever, cough and vomiting.
Mother and brother had had a similar respiratory disease.
A specimen is obtained since the clinic is testing a new diagnostic technique.
Patient is treated symptomatically.
9 year old presents with fever and cough.
Brother and cousin had has similar symptoms.
A specimen is obtained since they are performing an epidemiologic study.
Patient is treated symptomatically.

Initial tests in patient 1 demonstrate influenza A virus but could not be defined if the patient had H1N1, H3N2, or H5N1.
The San Diego Health Laboratory received the specimens of both patients and could not define the type of influenza virus.
Specimens are sent to CDC arriving April 13 and 17.

Mexico, April 2009 12th WHO is notified of an increase in the number of
cases with atypical pneumonia.
17th Increase surveillance and initiation of epidemiologic investigation.
23rd Canadian Reference Laboratory confirms that the virus in these cases is a novel H1N1. The PHO is notified.
24th Mexican Ministry of Health implements public measures in airports and vaccinates all healthcare professionals for seasonal influenza.
25th Presidential decree allowing sick people that do not require hospitalization to stay at home.
26th Mexico starts performing PCR for novel H1N1.
27th Schools are closed.

MMWR. May 8, 2009 / 58:453-458



Denison AM et al. Diagnosis of
influenza from respiratory autopsy
tissues: detection of virus by real-time
reverse transcription-PCR in 222
cases. J Mol Diagn 2011;13:123-8.

Munster VJ et al. Science 2009;325:481

Predictions were not fulfilled
Avian influenza,
Porcine
In Asia, in
America
In the winter, in
the summer

Index case
October 3, 2001: A local hospital calls the
Florida State Health Department as Bacillus
anthracis has been isolated from CSF of a
photographer that worked for a newspaper.
Presence of B. anthracis is confirmed and a BT
investigation was started by CDC and other local
and federal FBI authorities.
Patient had 2 days of fever, fatigue, sweats, and
altered mental status.

Case definition
Patient with clinical disease compatible
with cutaneous, gastrointestinal or
inhalational anthrax with
B. anthracis isolated from the affected site, or
2 other tests positive for B. anthracis
PCR, serology, or immunohistochemistry.

Patient died October 5
Reasons to do the
autopsy:
Route of infection
Potential homicide
People involved in
process

Autopsy measures
Measures needed to perform the autopsy:
Universal precautions (sharps)
DO NOT use electrical saw to open skull
Clean the autopsy room with 0.5% HCl and
autoclave instruments used.
DO NOT embalm, recommend incineration
Once tissues are formalin fixed they are
non-infectious



Concomitant second case, also in
Florida
A mailroom worker from the same newspaper
was being treated with antibiotics because of a
pneumonia.
This patient had persistent bilateral pleural
effusions.
Cultures in clinic were negative.
Later, evidence of anthrax by IHC and PCR on
pleural fluid cell block and pleural fluid.

Third case, in New York City
Secretary working at TV station
developed cutaneous lesion, onset
September 25.
Received antibiotics without obtaining
culture lesion samples.
October 12, 2001: biopsy obtained
Culture and PCR: negative for B.
anthracis.
Evidence anthrax by IHC on biopsy
and positive serology.


Summary of cases related with the
2001 bioterrorism attack
Inhalational anthrax: 11 cases all confirmed, 5
deaths.
Cutaneous anthrax: 10 cases 8 confirmed, no
deaths.
Jernigan JA, et al. Bioterrorism-related inhalational anthrax: the first 10
cases reported in the United States. Emerg Infect Dis 7: 933-944, 2001.
Jernigan DB, et al. Investigation of bioterrorism-related anthrax, United States, epidemiologic findings. Emerg Infect Dis 2002;8: 1019-28.
Guarner J, et al. Pathology and pathogenesis of bioterrorism-related inhalational anthrax . Am J Pathol 2003;163:701-709.
Shieh WJ, et al. The critical role of pathology in the investigation of bioterrorism-related cutaneous anthrax. Am J Pathol 2003;163(5): 1901-10.
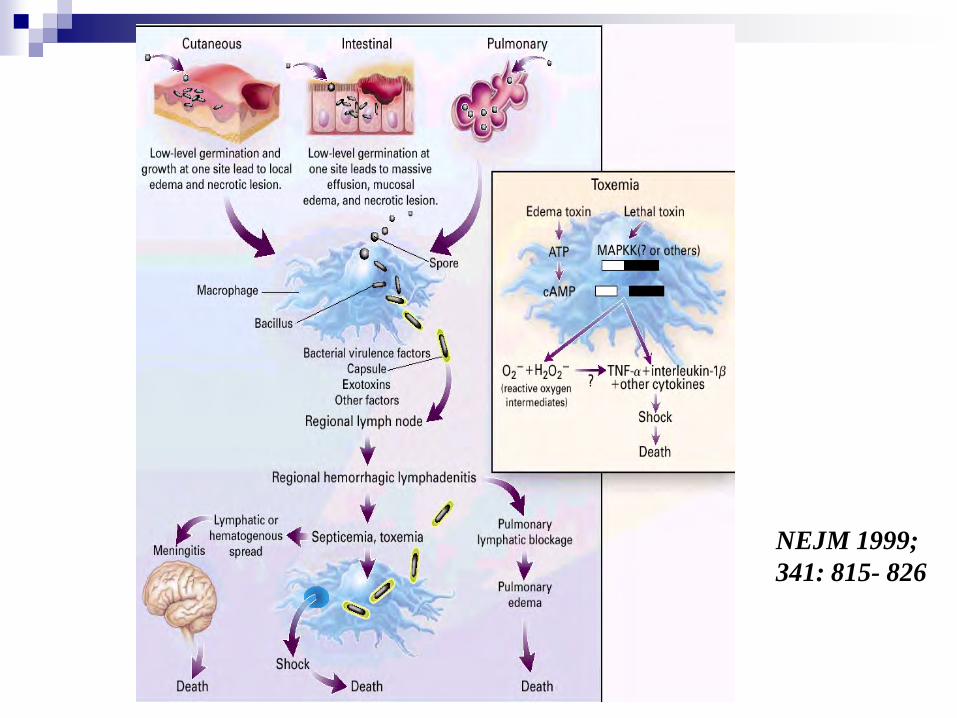
NEJM 1999;
341: 815- 826

Pathogenesis of
inhalational anthrax With IHC, large amounts of bacilli and
antigens are found in mediastinal lymph nodes and pleura. Hypothesis: Pleural effusions could be attributed to
direct bacterial damage.
It is possible that some macrophages with spores go directly to the pleura where bacilli germinate and cause damage.
The persistent effusions could be due to persistence of antigens in the pleura.

Pathogenesis of inhalational
anthrax Presence of vasculitis:
Previous reports describe vasculitis and capillaritis.
The cases related with the bioterrorism attack appear to have less vasculitis. Hypothesis:
Early diagnosis and treatment with new antibiotic and better medical support care.
Differences may be due to the dose or the type of aerosol.



Case
A 22-year-old man presented with fever and
hemoptysis.
His chest X ray showed no effusions or
infiltrates.
He had attended the funeral of his sister the
previous week in a rural community in Ecuador.
Several family members were also sick,
including his father who had died suddenly also
of a febrile disease and hemoptysis.

Blood culture was obtained and grew:
Gabastou JM et al. An outbreak of plague including cases with
probable pneumonic infection, Ecuador 1998.
Trans R Soc Trop Med Hyg 2000;94:387-91.
Non motile, catalase positive, but
negative for oxidase, urease, and indole
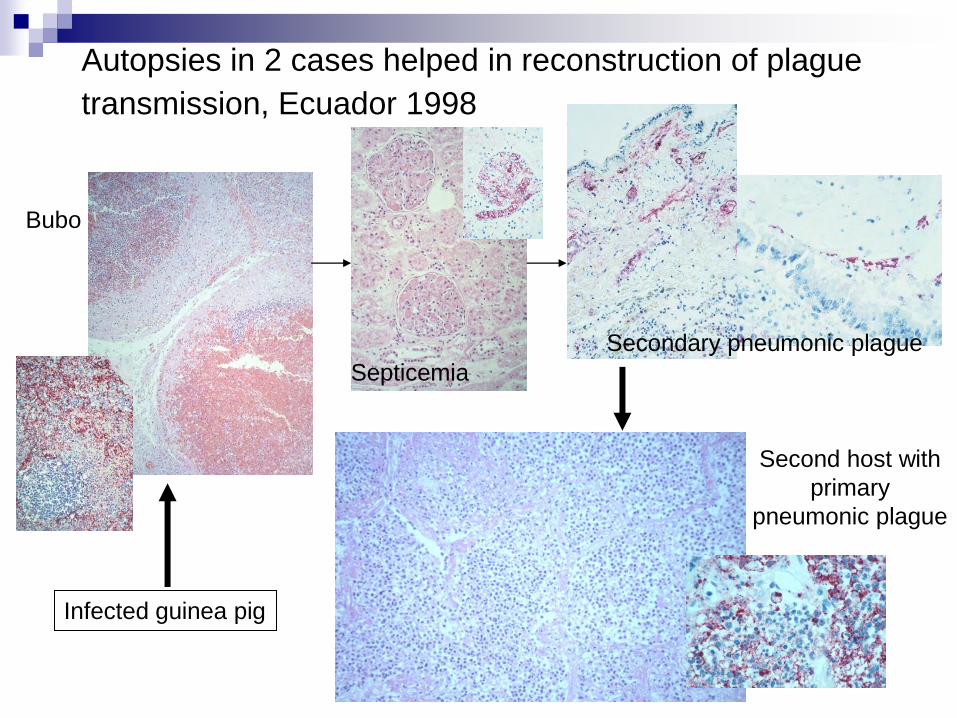
Autopsies in 2 cases helped in reconstruction of plague
transmission, Ecuador 1998
Infected guinea pig
Bubo
Septicemia
Secondary pneumonic plague
Second host with
primary
pneumonic plague

Objectives
When is an autopsy important for epidemiologic purposes? All the time as you never know which ones will and which will not be useful for epidemiologic purposes. There are only a handful that you know in advance.
What are the tissues that need to be obtained? Depends on the pathogenesis of the possible infectious disease. If you suspect an infectious diseases but no agent has been implicated you will need to take an array of tissues and keep some frozen for PCR and culture.
Who does these autopsies? Every pathologists that performs autopsies.






























