Embed Size (px)
Citation preview

Automatic 3D segmentation of the breast in MRI
by
Cristina Gallego Ortiz
A thesis submitted in conformity with the requirementsfor the degree of Master of Science
Graduate Department of Medical BiophysicsUniversity of Toronto
Copyright © 2011 by Cristina Gallego Ortiz

Abstract
Automatic 3D segmentation of the breast in MRI
Cristina Gallego Ortiz
Master of Science
Graduate Department of Medical Biophysics
University of Toronto
2011
Breast cancer is currently the most common diagnosed cancer among women and
a significant cause of death. Breast density is considered a significant risk factor and
an important biomarker influencing the later risk of breast cancer. Therefore, ongoing
epidemiological studies using MRI are evaluating quantitatively breast density in young
women. One of the challenges is segmenting the breast in order to calculate total breast
volume and exclude non-breast surrounding tissues. This thesis describes an automatic
3D breast volume segmentation based on 3D local edge detection using phase congru-
ency and Poisson surface reconstruction to extract the total breast volume in 3D. The
boundary localization framework is integrated on a subsequent atlas-based segmentation
using a Laplacian framework. The 3D segmentation achieves breast-air and breast-chest
wall boundary localization errors with a median of 1.36 mm and 2.68 mm respectively
when tested on 409 MRI datasets.
ii

To my parents,
Cecilia Ortiz and
Conrado Gallego in memoriam
iii

Acknowledgements
I want to express my gratitude to my supervisor, Dr. Anne Martel who has offered in-
valuable guidance, advice, encouragement and mentorship throughout.
I have accumulated many debts to my supervisory committee members, Dr. Martin Yafee
and Dr. John Sled. I would like to thank them for their time and patience in helping me
plan and revise my work at every stage of my studies.
I owe special thanks to all Martel lab members, their friendship, constructive criticism
and professional collaboration meant a great deal to me.
To Dr. Norman Boyd and his research group, especially Anoma Gunasekara and Sofia
Chavez, for providing the high quality Breast MRI datasets and for their valuable col-
laboration.
Last but not least, I wish to express my gratitude to my beloved family. Specially to my
mother, for her unconditional love, understanding, and for supporting me on whatever I
have decided to pursue in life.
iv

Contents
1 Introduction 1
1.1 Breast anatomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
1.2 Breast development and cancer susceptibility . . . . . . . . . . . . . . . . 3
1.3 Mammographic density as a risk factor . . . . . . . . . . . . . . . . . . . 5
1.3.1 Assessment of breast density . . . . . . . . . . . . . . . . . . . . . 6
1.3.2 Measuring breast density with ultrasound . . . . . . . . . . . . . 9
1.3.3 Measuring breast density with MRI . . . . . . . . . . . . . . . . . 11
1.4 Segmentation of the breast in MRI . . . . . . . . . . . . . . . . . . . . . 14
1.5 Thesis Outline . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
2 Breast boundary localization and 3D extraction 18
2.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
2.2 Breast MRI datasets . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
2.3 Detecting the breast boundary . . . . . . . . . . . . . . . . . . . . . . . . 19
2.3.1 Features of edge strength . . . . . . . . . . . . . . . . . . . . . . . 19
2.3.2 Phase congruency edge detector . . . . . . . . . . . . . . . . . . . 22
2.3.3 Extracting local frequency via local energy . . . . . . . . . . . . . 23
2.4 Breast surface via Poisson reconstruction . . . . . . . . . . . . . . . . . . 26
2.4.1 Poisson surface reconstruction . . . . . . . . . . . . . . . . . . . . 26
2.4.2 Maximal phase congruency and edge point orientation . . . . . . 28
v

2.4.3 Implementation via Octree structures . . . . . . . . . . . . . . . . 29
2.4.4 Extracting the breast boundary as an isosurface . . . . . . . . . . 32
2.5 Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
3 Atlas-based segmentation of the breast in 3D 34
3.1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
3.2 Extracting a shape atlas of the breast in 3D . . . . . . . . . . . . . . . . 35
3.2.1 Groupwise registration and average volume extraction . . . . . . . 35
3.2.2 Population shape average and 3D shape representation . . . . . . 37
3.3 Mapping 3D atlas landmarks via a Laplacian framework . . . . . . . . . 38
3.4 Validation: Segmentation of population cases . . . . . . . . . . . . . . . . 40
3.4.1 Distance errors . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
3.4.2 Volume errors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
3.4.3 Evaluation of standard overlap metrics . . . . . . . . . . . . . . . 45
3.5 Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
4 Conclusions and future directions 50
4.1 Contribution of this work . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
4.1.1 Segmentation for breast density assessment . . . . . . . . . . . . . 50
4.1.2 Segmentation in the context of CAD systems . . . . . . . . . . . . 51
4.2 Future directions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
A Statistical shape model of the breast in 3D 56
Bibliography 57
vi

List of Tables
1.1 Factors that increase the relative risk for breast cancer in women. . . . . 7
3.1 Number of landmarks and triangles generated after surface mesh decimation 38
3.2 Distances from manually annotated surfaces discriminated by boundary
region after Poisson surface reconstruction. . . . . . . . . . . . . . . . . . 42
3.3 Distances from manually annotated surfaces discriminated by boundary
region after Laplacian correspondences. . . . . . . . . . . . . . . . . . . . 42
3.4 Agreement and error overlap results. . . . . . . . . . . . . . . . . . . . . 46
vii

List of Figures
1.1 Anatomy of the breast . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
1.2 Pike’s model of breast tissue exposure and age-incidence curve of breast
cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
1.3 Computer-assisted measurement of percent mammographic density. . . . 8
1.4 Breast density measurement by Ultrasound. . . . . . . . . . . . . . . . . 10
1.5 Breast density measurement using T1-weighted imaging. . . . . . . . . . 11
1.6 Breast density measurement using chemical shift imaging. . . . . . . . . 13
1.7 Breast segmentation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
1.8 Overall segmentation pipeline and thesis organization. . . . . . . . . . . . 16
2.1 Fourier series of a square waveform. . . . . . . . . . . . . . . . . . . . . . 20
2.2 Interpolation of a step feature to a line feature. . . . . . . . . . . . . . . 21
2.3 Polar plot of local energy model for phase congruency. . . . . . . . . . . 22
2.4 1D Log-Gabor transfer function and Quadrature pairs. . . . . . . . . . . 23
2.5 Phase congruency detection examples . . . . . . . . . . . . . . . . . . . . 25
2.6 Schematic of Poisson surface reconstruction in 2D. . . . . . . . . . . . . . 27
2.7 Extracting points of maximal phase congruency and estimating their ori-
entation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
2.8 Schematic drawing of an octree hierarchical subdivision. . . . . . . . . . 30
2.9 Initial breast boundary surface via Poisson surface reconstruction . . . . 32
viii

3.1 Population-based construction of the average volume . . . . . . . . . . . 36
3.2 Average shape representation with varying decimation factors . . . . . . 37
3.3 Initializing model points into optimal isosurface. . . . . . . . . . . . . . . 39
3.4 Experimental design to assess performance of segmentation. . . . . . . . 41
3.5 Box-and-Whisker plots: Comparison of target distance errors for the two
stages of segmentation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
3.6 Representative results of 2 breast boundary reconstructions. . . . . . . . 45
3.7 Bland-Altman plot showing the difference vs average of results . . . . . . 46
3.8 Overlap metric assessment for segmentation results . . . . . . . . . . . . 47
3.9 Distribution of overlap metrics, breast volumes and surface areas. . . . . 48
3.10 Percentage and Absolute percentage Volume and Surface errors. . . . . . 49
4.1 Model fitting compared to boundary localization distance error results . . 54
ix

List of Abbreviations
2D Two-dimensions. 14
3D Three-dimensions. 1
ABUS Automated whole breast ultrasound. 10
BIRADS Breast imaging reporting and data system. 8
BRCA1 Breast cancer gene 1. 5
BRCA2 Breast cancer gene 2. 5
CAD Computer-aided diagnosis. 17
CNNs Cellular neural networks. 50
DCE-MRI Dynamic contrast enhanced magnetic resonance imaging. 12
ETL Echo Train Length. 19
FCM Fuzzy C-Means algorithm. 11
FFD Free form deformation. 35
FOV Field-of-View. 15
FSE Fast spin-echo. 19
x

GUI graphical user interface. 51
GVF Gradient vector flow. 15
IQR interquartile range. 42
MLO Mediolateral oblique view. 13
MRI Magnetic Resonance Imaging. 1
PC Phase congruency. 22
SSM statistical shape model. 52
TDLU Terminal duct lobular unit. 3
TE Time to Echo. 19
TR Time of Repetition. 19
USPD Volumetric ultrasound percent density. 10
xi

Nomenclature
An(x) n-th Fourier term amplitude. 22
D octree depth. 30
E(x) local signal Energy. 22
FN false negative volume overlap. 45
FP false positive volume overlap. 45
Fo function space of sampled points. 30
Mo mean volume overlap or Dice coefficient. 45
NgbrD(p) eight depth-D nodes. 31
Siso isosurface binary representation. 39
Sm atlas binary representation. 39
T noise threshold. 25
To total volume overlap. 44
αo,p trilinear interpolation weights for point p. 31
φ(x) mean local phase of Fourier terms. 22
δ scaling factor on bank of filters. 25
xii

γ scalar parameter for surface reconstruction. 32
λmin smallest wavelength of the Log-Gabor filter. 25
C(s) parameterization of field line. 40
N normalized negative gradient of Laplace solution. 40
xi i-th atlas point. 42
xtargeti i-th closest point on target surface. 42
µ mean of the local Energy. 25
∇χM indicator function gradient. 26
∂M reconstructed isosurface. 32
φn(x) n-th Fourier term phase. 22
ψ Laplace solution. 39
σ standard deviation of the local Energy. 25
χM indicator function. 26
~V vector field of point normals. 27
b shape parameter of a SSM. 52
k/wo filter’s bandwidth. 24
wo filter’s center frequency. 24
xiii

Chapter 1
Introduction
While the incidence and mortality rates of breast cancer vary internationally, currently
it is the most commonly diagnosed cancer among women in most parts of the world
[1]. In Canada, breast cancer accounts for the second cause of cancer deaths despite the
significant improvement in survival rates since the mid-80s [2]. Currently the 5-year sur-
vival rate is 87% likely as a result of advances in treatment and breast cancer screening.
Breast cancer develops through multiple stages and the reason why some tumors even-
tually become invasive and metastatic and some of them remain non-invasive precancers
is still under investigation. Current research has looked at breast composition in an at-
tempt to determine significant risk factors that could be associated with the development
of cancer. Breast density, a representation of the amount of breast dense parenchyma
present in the breast, has been identified as a significant risk factor and an important
biomarker influencing the later risk of breast cancer. Ongoing epidemiological studies
conducted by Boyd et al. [3] are looking at quantitative assessment of breast density in
young women using MRI. However, it is known that quantitative evaluation of breast
density using MRI suffers from several limitations including inconsistent breast boundary
segmentation methods. This thesis presents a method to automatically segment the 3D
anatomy of the breast in MRI. Key contributions of this work are a proposed automatic
1

Chapter 1. Introduction 2
framework for extracting the boundaries of the breast region and for estimating the total
breast volume. The objective of the first chapter is to give an overview of the clinical
motivation and impact of this work. The following sections of this chapter review the
anatomy of the breast, introduce breast cancer risks and highlight breast density as an
important risk factor.
1.1 Breast anatomy
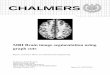
Figure 1.1: Anatomy of the breast: a) Gross anatomy of the breast. b) Terminal duct lobular
unit TDLU schematic. Adapted from: Schunke, et al. Thieme atlas of anatomy: general
anatomy and musculoskeletal system. Thieme 2006.
The breast is a modified skin gland that lies on top of the musculature that encases the
chest wall. The breast is not completely separated from these muscles, in fact only a layer
of adipose tissue and connective fascia separate the breast from the pectoral muscle. The
breast is composed of three major tissue types: glandular tissue (parenchyma), fibrous
stroma and fatty tissue. The stroma is composed of connective tissue, ligaments, blood
vessels, lymphatics, lymph nodes, and nerves [4] and its main function is to provide
support and to nurture the breast. The glandular tissue is organized in a ductal system

Chapter 1. Introduction 3
with a distribution that is essentially bilateral between the right and left breast. Current
literature agrees that the parenchyma of the breast consists of about 10 to 20 lobes,
each of which has a lactiferous major duct that opens on the nipple through a little
antechamber called the lactiferous sinus (see figure 1.1-a). Starting at the nipple, the
ductal system splits up in branches that reach the back of the breast. At the end of
each branch are the lobules that produce milk. Each lobule is composed of acini that
empty into the terminal ducts. The acini and terminal ducts form a complex also known
as the terminal duct lobular unit (TDLU) (see figure 1.1-b). The TDLU is the basic
secretory unit of the female breast and is of key importance in histopathology since there
is evidence to suggest that is the site where most malignant cancers originate [5].
1.2 Breast development and cancer susceptibility
Breast tissue unlike other tissues in the body is very sensitive to develop cancer. The
basis of this difference is the fact that cells in the breast mostly divide and differentiate
after birth and therefore are at a higher risk of acquiring mutations during development.
Cells in the breast of a newborn are very immature and remain this way until the onset of
puberty, when cells start to develop in response to sexual hormones. At this point, stem
cells in the breast begin to differentiate into duct cells or lobular cells. Research has found
that some stem cells remain undifferentiated perhaps to replenish injured cells. These
findings have motivated a new hypothesis focusing on these cells as origins of cancer [6].
On a different line of thought, some researchers have studied the factors that con-
tribute to breast cancer susceptibility. Pike [7] showed that breast tissue exposure to
carcinogens has the greatest susceptibility to cause abnormal mutations around the time
of puberty but decreases with the first pregnancy and continues to reduce further in pre-
menopausal and menopausal periods (see figure 1.2-a). Pike’s work also explained how
the area under the exposure-age curve could be used to describe the increasing incidence

Chapter 1. Introduction 4
of breast cancer with age (see figure 1.2-b). The incidence of breast cancer with age
has a distinctive curve. Below the age of 50 years, the incidence is about the same in
widely different geographical locations. However, around the age of menopause and after
menopause (> 50 years) the incidence is lower for non-western countries than for western
countries. The high incidence rates in white women in north America and in several
western European countries can be explained with the high prevalence of well known
reproductive factors associated with an increased risk, such as early menarche, late age
at first full-term pregnancy, fewer pregnancies and use of postmenopausal hormone ther-
apy (see table 1.1), but also non-reproductive factors such as increased detection with
mammography screening [1].
Rate(per 100,000)1000
100
10
1
0.1
5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 80+ Age
Figure 1.2: a) Pike’s model of breast tissue exposure. fo, f1, f2 are variables of the model,
FFTP=first full-term pregnancy, b is a variable to calculate age at menarche. Adapted from:
[8] and b) age-incidence of breast cancer in selected cancer registries. Adapted from: The
changing global patterns of female breast cancer incidence and mortality [9].
The pattern of premenopausal cancer have attracted the attention of several re-
searchers. While postmenopausal cancer is more likely to be explained by reproductive

Chapter 1. Introduction 5
risk factors, premenopausal risk factors, prognosis of the disease and tumor biology have
been found to be somehow different in women below 40 years [10], suggesting that cancer
in this age subgroup is a different entity. The causes of some of these cancers seem re-
lated to hereditary mutations but their prevalence varies among different ethnic groups.
In Ashkenazi Jewish the prevalence of BRCA1 and BRCA2 mutations was 20% and 8%
respectively in women with breast cancer diagnosed before 42 years [11, 12]. In Iceland,
BRCA2 mutations were found in 24% of cancers diagnosed before 40 years [13]. However,
another study in the UK [14] reported a prevalence of only 3.1% and 3.0% on BRCA1
and BRCA2 mutation carriers respectively among patients from an out-bred population
with breast cancer who were younger than 50 years. This high prevalence of mutation
carriers among specific ethnic groups has been explained by genetic founder effects but
the fact that this prevalence is much lower on a more out-bred population reflects that
there are other underlying causes still to be understood.
1.3 Mammographic density as a risk factor
Mammographic density is defined as the proportion of breast that comprises epithelial
and stromal tissue on a mammogram. Dense tissue appears bright on a mammogram
while fat tissue, which is less dense, appears darker due to different x-ray attenuation
characteristics. The reason why some breasts are radiologically denser than others re-
lates to breast tissue composition. A systematic meta-analysis of 42 studies looked at the
strength of the association between breast density and breast cancer risk in the general
population. The study found an increasing relative risk of breast cancer with an in-
creasing percent density as measured on pre-diagnostic mammograms [15]. In addition,
the relative risk was found to be independent of age, ethnicity or menopausal status at
mammography. In women with > 75% mammographic density, the risk of breast cancer
was found to be 4.64 (95% CI 3.64 - 5.91) times the risk in women with little or no breast

Chapter 1. Introduction 6
density (< 5% mammographic density), a relative risk even stronger than the relative
risk variables considered on Gail’s model [16, 17], a model that has been validated for use
in women 35 years or older to provide 5-year and lifetime risk estimates for developing
breast cancer. Table 1.1 summarizes other known relative risks factors for comparison.
Epidemiological data have shown that there are parallel similarities between breast
density and breast tissue susceptibility with age [8]. Both breast tissue exposure based
on Pike’s model and average percent mammographic density decreases with age. Breast
density is also altered by pregnancy and menopause and decreases with age of stromal
and epithelial tissue. A study looked at the relationship between mammographic density
and histological features on randomly selected breast tissue samples taken from forensic
autopsies (Li et al.[19]). Using quantitative microscopy, the biopsy portion occupied
by cells (estimated by nuclear area), glandular structures, and collagen was correlated
with percent mammographic density. They found that percent mammographic density
was associated with greater total nuclear areas (p<0.001), greater proportion of collagen
(p<0.001), greater nuclear areas of both epithelial and non-epithelial cells as well as
greater area of glandular structures. The authors concluded that the age-related decline
of mammographic density could be explained by the reduction in epithelium and stroma,
a physiological process known as involution.
Some researches have thought of breast density as an intermediate phenotype for can-
cer [8], motivating new research on elucidating the genes that determine breast density.
A current hypothesis states that breast cancer originates on epithelial cells, and therefore
a greater content of fibroglandular tissue in the breast exposes a woman to a higher risk
due to carcinogenic influences.
1.3.1 Assessment of breast density
In 1976 the first classification system of the appearances of mammograms with their
association to breast cancer risk was proposed by Wolfe [20]. Wolfe’s classified the

Chapter 1. Introduction 7
Relative Risk Factor
> 4.0 • Age (65+ vs. <65 years, although risk increases across all ages until
age 80)
• BRCA1 and/or BRCA2
• ≥ 2 first-degree relatives with breast cancer diagnosed at an early age
• Personal history or breast cancer
2.1 - 4.0 • One first degree relative with breast cancer
• Biopsy confirmed atypical hyperplasia
• High dose radiation to chest
• High bone density (postmenopausal)
1.1 - 2.0 Reproductive factors
• Late age at first full-term pregnancy (>30 y)
• Early menarche (<12 y)
• Late menopause (>55 y)
• No full-term pregnancies
• Never breast fed a child
Factors that affect circulating hormones
• Recent oral contraceptive use
• Recent and long term use of hormone-replacement therapy
• Obesity (postmenopausal)
Table 1.1: Factors that increase the relative risk for breast cancer in women. Adapted from:
Dr. Susan Love’s Breast book. Fifth edition. [18]

Chapter 1. Introduction 8
breast parenchyma into four categories based solely on its appearance. The categories
were N1(essentially normal breast), P1(prominent ductal pattern to a minimal degree),
P2(prominent ductal pattern of a moderate to severe degree), and DY(extremely dense
parenchyma). Using this system on a sample screening population Wolfe determined that
by screening P2 and DY women, 76% of the total cancers were found, and by examining
P1 in addition to P2 and DY, 93.3% of the cancers could be found. Despite being a
preliminary study at the time it highlighted the potential benefits of routine repeated
screening examination for the P2 and DY group of patients. The breast imaging reporting
and data system (BIRADS) [21] have proposed a qualitative system to classify mammo-
graphic breast density. The BIRADS system includes 4 different categories: 1 (predom-
inately fat <25% glandular), 2 (scattered fibroglandular densities 25-50% glandular), 3
(heterogeneously dense 51-75% glandular), and 4 (extremely dense <75% glandular).
Figure 1.3: Computer-assisted measurement of percent mammographic density. a) Thresholded
digital mammogram: red contour defines edge of breast; green contour shows edge of dense
region [8]. b) Histogram with corresponding user-selected grey-level thresholds: breast edge
(iEdge) and density edge (iDY ) Adapted from: [22].
Computer-assisted measurement of percent mammographic density has also been pro-

Chapter 1. Introduction 9
posed. One approach uses interactive thresholding to separate tissue types based on their
radiographic appearances. With an interactive thresholding scheme, an observer selects
2 thresholds: first, a threshold at the boundary of the breast to exclude the background
and second, a threshold at the edge of a dense area to segment areas of high density in the
mammogram (see figure 1.3). The proportion of radiographic density is calculated as the
percentage of the total area of the breast that corresponds to dense tissue. Quantitative
approaches over qualitative methods for determining breast density have provided more
consistent results and larger gradients in risk. McCormack et al. [15] observed a linear
increasing trend in both incidence and prevalence in general population studies. The
area of the dense tissue has also been found to be a strong predictor of risk but debate
exists on whether or not percentage density is a stronger predictor.
Despite the current understanding of breast density as a strong predictor of breast
cancer risk, the incorporation of breast density assessment into a risk assessment model
have not made a big difference yet [23]. X-ray mammography for breast density assess-
ment has several limitations. It has been suggested that the measured mammographic
densities may vary with different projections, level and angle of compression, and scanner
calibration. X-ray mammography is a 2D imaging modality that offers only a projec-
tion image rather than a volumetric equivalent of the three-dimensional breast. More
importantly is perhaps the radiation dose limiting factor for measuring density in young
women. As a consequence, even though the majority of epidemiological evidence on
breast density as a risk factor is based on mammographic breast screening data, some
researchers have recognized the benefits of studying breast density with different imaging
modalities such as ultrasound and MRI.
1.3.2 Measuring breast density with ultrasound
Ultrasound imaging is relatively cheap, highly available and does not use ionizing radi-
ation. Ultrasound can measure breast density knowing that the speed at which sound

Chapter 1. Introduction 10
travels through a medium is related to tissue density and elasticity. One method for
measuring percent density by ultrasound tomography consists on segmenting areas of
fast sound speed from each speed tomogram, integrating these areas over the entire vol-
ume, and dividing by whole-breast volume to derive the volumetric ultrasound percent
density (USPD) (see figure 1.4-b) [24]. The authors reported a Spearman correlation
coefficient of 0.75 (P < .001) between USPD and percent mammographic density among
90 subjects (figure 1.4-c). Other methods for measuring density use automated whole
Figure 1.4: Breast density measurement by ultrasound. a) Automated whole breast ultrasound
(ABUS) images [25]. Structures labeled in letters are: (a) Skin, (b) nipple, (c) subcutaneous
fat, (d) glandular tissues, (e) retromammary fat, (f) pectoral muscles and (g) rib. b) Images
acquired using ultrasound tomography of the breast. c) Scatter plot of volumetric ultrasound
percent density (USPD) vs. percent mammographic density [24].
breast ultrasound (ABUS) to acquire the volume of the whole breast and then, by man-
ually excluding non-breast regions it is possible to derive the total fibroglandular area
(see figure 1.4-a). The percent density is calculated based on the ratio of the fibroglan-
dular area over the whole breast area for all of the acquired 2D slices [25]. However,
the authors did not report correlation with percent mammography density as measured
by mammography but found a high correlation with 3D breast MRI density measure-
ments using T1-weighted images and the fuzzy C-means (FCM) classifier to differentiate
fibroglandular tissue from fatty tissue [26] [27].

Chapter 1. Introduction 11
1.3.3 Measuring breast density with MRI
MRI is a very versatile imaging modality that provides a 3D view of the breast for
assessment of volumetric breast density without exposure to ionizing radiation. Based
solely on image analysis one can measure breast density using MRI. T1-weighted imaging
can be used to distinguish between fat tissue and dense tissue. The contrast mechanism in
MRI is dictated by tissue relaxation. Particularly, T1 relaxation describes the recovery of
the longitudinal magnetization due to the thermal interactions between hydrogen nuclei
(the spins) and large macromolecules within the tissue microenvironment (the lattice).
Due to differences in tissue composition, different tissues have different T1 values. In
the breast, T1 values are shorter for fat (about 250 ms at 1.5T) than for fibroglandular
tissues (about 700 ms at 1.5T) [28]. As a consequence, T1 effects tend to cause fat
tissue to have higher signal (appear brighter) than fibroglandular tissue. A number of
Figure 1.5: Breast density measurement using T1-weighted imaging. a) T1-weighted v-cut
segmented breast region, b) FCM clustering for 4 different tissue clusters. c) Cluster #1 (air
and lung tissue) is removed, c) Segmented breast after exclusion of chest wall muscle and skin,
d) Fibroglandular tissue segmentation via FCM-clustering, e) Breast outline and fibroglandular
region masks. Adapted from [27].

Chapter 1. Introduction 12
previous studies have used T1-weighted imaging to assess breast density. Lee et al.
[29] segmented fatty and fibroglandular volumes on 3D T1-weighted MRI estimating
pure-tissue averaged signal intensities via a two-compartmental model. Other authors
have proposed to measure breast density directly on standard clinical dynamic contrast
enhanced (DCE-MRI) data. Nie et al. [27] suggested the fuzzy C-means (FCM) algorithm
to determine the whole breast volume and fibroglandular volume on pre-contrast T1-
weighted images without fat saturation. Tissue cluster #1 on figure 1.5-d, corresponds
to fibroglandular tissue whereas clusters #2 and #3 both represent fatty tissues. Khazen
et al. in the UK [30] measured the proportion of fibroglandular tissue by interactive
thresholding of the signal intensities in pre-contrast T1-weighted images.
An alternative way in which MRI can evaluate breast density is by measuring breast
water as a surrogate for fibroglandular tissue and stroma. Research motivated on assess-
ing ex-vivo breast tissue properties using MRI revealed that the estimated water content
using MR spectroscopy was strongly correlated with the volumetric water content mea-
sured by enzymatic extraction. Water and fat are two spectrally different components
and therefore can be imaged separately using chemical shift imaging. Most fat in the
human body has a chemical shift with respect to water equal to 3.5 ppm (3.5 x 10−6),
which is equivalent to a frequency shift from the resonant frequency of water of 220 Hz at
1.5 T. The goal of fat/water imaging is to determine the relative signal contribution from
water and fat respectively in each voxel. Most fat and water separation MRI sequences
are based on the Dixon sequence published originally in 1984. Dixon’s sequence acquires
two separate images: the first is a conventional spin echo with water and fat signals in-
phase, and the second is acquired so that water and fat signals are 180°out-of-phase [31].
Dixon’s technique uses summation and subtraction of both complex signals to generate
fat-only and water-only images allowing direct fat and water quantification. Bright areas
on a water image correspond to water-containing tissues and represent a quantitative
surrogate for fibroglandular tissue (see figure 1.6-a, b). Further modifications have been

Chapter 1. Introduction 13
made to the original Dixon technique mainly to reduce the sensitivity of the method to
magnetic field inhomogeneities [32]. [33].
Figure 1.6: Breast density measurement using chemical shift imaging. Sagittal MRI slice of a)
breast fat and b) breast water, green contour shows the expert annotated outline of the breast.
c) Scatter plot of percent water by MRI vs percent density by X-ray mammography. [3].
Regardless of the quantification method of breast density using MRI, numerous stud-
ies have reported strong correlations between percent mammographic density as mea-
sured by X-ray mammography and MRI. Khazen et al. [30] found a correlation r=0.78
between MRI percent density and percent mammographic density estimated with Cumu-
lus software [34] for 138 high-risk women part of the UK MARIBS breast MRI screening
program. Wei et al. [35] found a correlation of r=0.89 between the volumetric fibrog-
landular tissue on MRI and the percent dense area on mediolateral oblique view (MLO)
mammograms for 65 patients. In a cross-sectional study by Boyd et al. [3], breast den-
sity was assessed in 100 woman using percent mammographic density as measured by
X-ray mammography and percent water as measured by MRI. The measurements had a
Spearman correlation coefficient r=0.85, p<0.0001 (see figure 1.6-c).

Chapter 1. Introduction 14
1.4 Segmentation of the breast in MRI
It is known that quantitative evaluation of breast density using MRI suffers from sev-
eral limitations including inconsistent breast boundary segmentation, different pulse se-
quences, and lack of standardized computerized algorithms for accurate quantification.
During breast density assessment using MRI it is necessary to segment the breast in or-
der to calculate total breast volume and exclude non-breast surrounding tissues. Image
segmentation is commonly used to subdivide the image into its constituent regions. In
our case, we are interested on segmenting the gross anatomy of the breast represented on
2D as the breast-air boundary, breast-chest wall boundary and upper and lower limits of
breast for the entire extent of the breast, and on 3D as a convex surface delimiting the
entire volume of the breast (see figure 1.7).
Figure 1.7: Left: 2D segmentation consisting on the breast-air boundary (green contour) and
breast-chest wall boundary (purple contour). Right: 3D segmentation consisting on a convex
surface.
Breast segmentation can be performed using manual contouring which is assured by
expert annotation and even though this process is highly time consuming, tedious, and
inconsistent among different operators, it is commonly used as a gold standard. Semi-

Chapter 1. Introduction 15
automatic approaches have been proposed in order to facilitate the segmentation task
and improve reproducibility but they still require subjective operator initialization or
correction. Often times, simple grey-level intensity separation methods are used. In the
UK study [30], total breast volume segmentation was limited to a volume defined by
a thresholding operation excluding background air and a straight line anterior to the
pectoral muscles on each axial slice, an arbitrary constraint that clearly underestimates
the total breast volume. For the two-compartmental model approach by Lee et al. [29] the
total volume of the breast is determined on a slice-by-slice fashion using edge detection for
the breast-air interface and manual outlining of the breast-chest wall interface. Nie et al.
[27] used a V-shape cut to exclude the thoracic region based on anatomical landmarks on
each axial slice followed by tissue clustering and dynamic searching to exclude the chest
wall muscles and the skin. Such an approach however, lacks generalization to different
acquisition orientations and FOV.
Robust and reliable automatic segmentation is ideal although it is challenging. In
breast MRI, the image contrast is dependent on imaging protocols and acquisition param-
eters so that segmentation based on separation of grey-level intensities, such as threshold-
ing or region growing suffer from generalization ability. In addition, the contrast between
adjacent structures such as between breast tissue and the pectoral muscles is not distinc-
tively defined. In the computer vision literature, other researchers have proposed the use
of active contours also known as Snakes to perform low-level tasks such as edge detection
combined with high-level models for the purpose of segmentation [36]. Snakes are energy
minimizing splines that move within images to find object boundaries. In the original
formulation, the snake had an internal term which aims to impose smoothness on the
shape, and an external term which encourages movement towards the edges of the image.
Snakes however, have the disadvantage of distorting the anatomy of the structure to be
segmented since they lack global shape constraints. A more robust algorithm [37] uses
the Gradient vector flow (GVF) to model a physical object that has a tendency to both

Chapter 1. Introduction 16
stretch and bend to adapt better to regions of high curvature, has a higher capture range
which often solves the problem of stopping at local minima but since no force (other
than smoothness) is imposed, the model can still fold and deform to non-realistic shapes.
A model-based segmentation has the flexibility of the snakes to deform but the allowed
deformation is limited within a range of variability introduced using prior knowledge
about the structure of the object. This captured biological variability is then used to
add flexibility to the deformation so that the model can be fitted appropriately to the
object to be segmented by adjusting the model’s parameters in such a way that the fit
of the model to the image is maximized.
1.5 Thesis Outline
In the remaining of this thesis, the main steps proposed for the automatic segmentation
of the breast volume in MRI are described. The complete segmentation pipeline can be
briefly summarized as follows (see Figure 1.8). For each case to segment, image features
Localization of the
edges of the breast
1Extraction of the
breast boundary
2
For each case to segment:
3Refinement
via shape atlas
Chapter 2
Build population
3D atlas
For all cases on population:
Chapter 3
4Segmented
breast volume
Figure 1.8: Overall segmentation pipeline and thesis organization.

Chapter 1. Introduction 17
that highlight the edges of the breast are identified in order to extract the boundary of
the breast region, which in 3D corresponds to a surface. Then, the initial estimate of
the boundary of the breast is further refined by incorporating shape-prior information
in the form of a shape atlas representing the breast anatomy in 3D. A shape atlas can
be derived from all the cases in the population by building a consensus of the shape of
the breast in 3D. The final result of this pipeline is an automatically segmented breast
volume.
Chapter 2 describes the 500 breast MRI datasets from a breast density study in
young women [3], the localization of the edges of the breast region based on 3D local
edge detection, and the extraction of the boundary of the breast in 3D via a Poisson
surface reconstruction method.
Chapter 3 presents the construction of a breast atlas using 3D groupwise registration
to automatically generate subject correspondences in a population. Then follows the
description of the refinement of the breast surface by incorporating 3D shape information
from an atlas using a Laplacian framework.
Chapter 4 summarizes the contribution of this thesis and illustrates the relevance of
the proposed segmentation pipeline in the context of computer-aided diagnosis (CAD)
systems. In addition, this chapter elaborates on how the breast boundary localization
framework can be integrated as the starting point for a subsequent model-based segmen-
tation and presents preliminary results contained in Appendix A. Finally, this chapter
draws conclusions and presents ideas for future work.

Chapter 2
Breast boundary localization and 3D
extraction
2.1 Introduction
One of the challenges for volumetric breast segmentation is to provide optimal features
of edge strength so that the boundary of the whole breast is highlighted and accurately
localized to serve as a template during segmentation. This chapter focuses on the method-
ology applied to localize significant edges of the breast region and to extract the breast
boundary as a surface. The population of previously segmented breast cases as part of a
young women breast density study [3] is presented in section 2.2. Section 2.3 describes
phase congruency edge detectors, their advantages over gradient-based edge detectors
and addresses the implementation of such filters in this work. Section 2.4 presents a
surface reconstruction algorithm based on a Poisson system built from the extracted fea-
tures of edge strength. The bulk of this work has been submitted and accepted to the
Breast Image Analysis workshop, part of the MICAAI 2011 conference.
18

Chapter 2. Breast boundary localization and 3D extraction 19
2.2 Breast MRI datasets
A population of breast MRI datasets (n = 500) was used from a previous study by Boyd
et al. [3]. The population consisted on 400 young women aged 15 - 30 years and a random
sample (n=100) of their mothers, aged 40 - 60 years. Briefly, breast images were acquired
in the sagittal plane with a slightly modified version of the GE FSE Dixon sequence. A 28
cm field of view was used with a 256 x 128 acquisition matrix. The slice thickness was 7
mm interleaved with TE 14x8 ms, ETL 8 and TR 2500. The total imaging time for both
breasts was about 13 min to obtain 45 slices covering the entire volume of both breasts.
Each scan consists of three images of water and fat signals with phase shifts of 0, π and
2π, according to the three-point Dixon method [38]. The image corresponding to the zero
degree phase shift corresponds to an image were both the fat and water signals are in
phase. This in-phase image of the right breast was used for further segmentations. Each
breast was semi-automatically segmented by 3 observers (inter-reader and intra-reader
agreement was more than 0.94) using an active contour approach with manual correction
[3]. In this work, the 2D delineated contours for each breast were stacked together in
adjacent cross-sections and resampled to an isotropic voxel size of 2.56 mm. Surface
meshes representing the 3D volume of the breast were finally obtained and these surfaces
were used as the gold-standard to measure the accuracy of the automatic selection of
landmarks and the overall segmentation accuracy (see chapter 3).
2.3 Detecting the breast boundary
2.3.1 Features of edge strength
The edge detection literature provides several definitions of an edge feature. One defi-
nition refers to an edge as a place in the image where there is a jump in intensity or in
brightness also known as a step discontinuity. Gradient magnitude and Laplacian mag-

Chapter 2. Breast boundary localization and 3D extraction 20
nitude edge detectors such as Canny filters [39] attempt to detect edges based on local
extrema of the directional derivatives of the grey-level intensity function taken across
the edge [40] and therefore detect edges as points of maximal intensity gradient. Points
of maximal intensity gradient only occur at edges on cases of high image contrast and
homogeneous illumination, i.e when the structure of interest stands out clearly from the
background. Another alternative are phase congruency filters. Extensive work in this
area by Morrone and Owens [41] [42] and Kovesi [43] explained the relationship between
the phase and the perception of structures and showed that ”edges” are image features
perceived by the human brain as a wide variety of features besides points of maximal
gradient intensity. Perona and Malik [44] identified that most edge features in images are
composed of combinations of steps, roofs, ramps and mach bands feature types. Phase
congruency filters detect image features where the local Fourier components are max-
imally in phase. Phase congruency can be demonstrated in the 1D case by a square
waveform where the Fourier components are all in phase at the step of the square wave
(see figure 2.1).
Figure 2.1: Fourier series of a square waveform and sum of the first four terms. For a square
waveform p = 1 and φ = 0. Adapted from Kovesi [43].
The square waveform represents a pure step feature. The effect of different feature
orientations and illuminations on the perception of an ”edge” is exemplified on figure
2.2. The gradual interpolating from a step feature (top of image on figures 2.2-a,b) to a
line feature (bottom of image on figures 2.2-a,b) is generated by varying the phase offset

Chapter 2. Breast boundary localization and 3D extraction 21
φ from 0 to π/2 on the square waveform Fourier series with amplitude decay p = 1 (see
equation on figure 2.1). Despite the variation in the sharpness of the edge due to the
differences of illumination and orientations, our visual perception of the feature type as
an edge remains.
Figure 2.2: Interpolation of a step feature to a line feature. a) 2D grating pattern by varying
φ = [0, π/2] from top to bottom and using p = 1.0, b) Canny edge detector of (a), c) Phase
congruency edge detector of (a). Adapted from Kovesi [43].
If we attempt to detect the edges of the grating in image 2.2-a using both a Canny
edge detector [39] (shown in figure 2.2-b) and phase congruency (shown in figure 2.2-c)
for comparison, it is clear that phase congruency captures more accurately the location
of the edge. The Canny filter erroneously detects the location of the edge where the
feature corresponds to a line feature. At the bottom of the image, the response of the
Canny filter is doubled as it captures points of maximal change in gradient intensity at
each side of the line edge feature. This example clearly exhibits some of the limitations of
gradient based edge detectors. This work focuses on phase congruency filters for detecting
edge features on breast MRI since these filters provide a more uniform response and are
less affected by low contrast. Low contrast between tissue types on the chest wall and
potential variations in illumination that occur due to field inhomogeneities clearly affect
edge detection in breast MRI by maximal gradient intensity methods.

Chapter 2. Breast boundary localization and 3D extraction 22
2.3.2 Phase congruency edge detector
Points of phase congruency can be detected as points of maximal local energy. Morrone
and Owens [42] proposed a local energy model based on physiological evidence to ex-
plain the relationship between phase congruency, energy and Fourier components. The
schematic on figure 2.3 represents the Fourier components of a signal at a given location,
where the n-th Fourier term has an amplitude given by An(x) and a phase by φn(x). The
local energy of the signal E(x) is represented as the sum of the components added head
to tail, and the mean local phase of all Fourier terms is given by φ(x).
Figure 2.3: Polar plot of local energy model for phase congruency. The Fourier components of
the signal at a location x are plotted head to tail. Adapted from Kovesi [43].
The phase congruency function (PC) intends to measure the total phase deviation of
each Fourier component from the phase of the local energy of the signal E(x) [45] :
PC(x) = maxφ(x)∈[0,2π]
∑nAncos(φn(x)− φ(x))∑
nAn, n ≥ 0 (2.1)
A point of maximum phase congruency is defined as a point x where PC(x) reaches
a maximum. In this context, points of local phase congruency occur for all n where
φn(x)− φ(x) = 0 and thus PC(x) = 1. Furthermore, Venkatesh et al. [45] demonstrated

Chapter 2. Breast boundary localization and 3D extraction 23
that these points also correspond to maxima of E(x). Since E(x) is a sum of infinite
number of components, if they follow a distribution with a small standard deviation
about the phase of E(x), then the magnitude of E(x) will attain a local maximum. It is
shown that the energy of the signal is equal to the phase congruency scaled by the sum
of the Fourier component amplitudes:
E(x) = PC(x)∑n
An (2.2)
2.3.3 Extracting local frequency via local energy
The Gabor function can be used as band-pass filter to obtain frequency information at
a particular region of the image spectrum.
Figure 2.4: 1D Log-Gabor transfer functions in a) linear frequency scale and b) logarithmic
frequency scale. Quadrature pairs of log-Gabor wavelets in the spatial domain tuned to the
same center frequency wo = 0.05 and bandwidths of c) 1 octave, d) 2 octaves and e) 3 octaves.
The logarithmic Gabor function has additional advantages; It can be designed with
arbitrarily large bandwidths while maintaining zero DC component. In addition, Field

Chapter 2. Breast boundary localization and 3D extraction 24
[46] have shown that the log-Gabor function is more consistent with measurements on
mammalian visual systems indicating that cells in the visual cortex have responses that
are symmetric on the logarithmic frequency scale (see figure 2.4-a). The 1D log-Gabor
transfer function is defined as:
G(w) = exp
[− log (w/wo)
2
2 log (k/wo)2
](2.3)
where wo is the center frequency and k/wo is the bandwidth of the filter. k/wo should be
kept constant to achieve filters with equal bandwidths at different scales. Figure 2.4-a,b
shows examples of log-Gabor transfer functions with bandwidth of approximately 1, 2
and 3 octaves. Figure 2.4-c,d,e shows three log-Gabor filters in the spatial domain with
the same center frequency but different bandwidths. As expected, if the filter’s width in
the frequency domain increases the wavelet’s bandwidth in the spatial domain becomes
narrower. Filters should be designed to achieve a fairly even spectral coverage, avoiding
overlap between filters and minimizing aliasing artifacts.
Kovesi [47] described how phase congruency can be calculated in 2D images using
wavelets to obtain local frequency information via banks of filters. His approach consists
of building log-Gabor quadrature pairs, which are basically two linear operators with the
same amplitude response but phase responses shifted by 90°, to then apply them over
several scales and orientations via a bank of filters. Phase congruency information is
finally combined from each scale and orientation. A bank of filters is created by rescaling
a minimum wavelength to different scales so that an optimal overlap is obtained and the
sum of all transfer functions forms a relatively uniform coverage of the spectrum.
Computing phase congruency in 3D using a bank of filter imposes the complexity of
defining the number of appropriate orientations and the angular spread of the filters in
order to evenly cover the image spectrum. As an alternative, points of maximal phase
congruency can be detected as points of maximal local energy [42]. In this work, the
practical implementation of a phase congruency detector in 3D is simplified with the
computation of the local energy of the signal via a multidimensional generalization of

Chapter 2. Breast boundary localization and 3D extraction 25
quadrature filters [48]. In contrast to the bank of oriented filters approach, there is
no need for an additional summation along different orientations. The filter’s center
frequency at a given scale is determined by the following equation:
ws =1
λmin(δ)s−1 , s = 1, 2, ..., n (2.4)
here λmin is the smallest wavelength of the Log-Gabor filter and δ is a scaling factor
between successive scales. λmin is scaled up to the total number of scales n. A noise
threshold (T ) is applied to the computation of phase congruency in order to suppress the
noise response. T is calculated at the smallest scale assuming a Rayleigh distribution as
T = µ + kσ, where µ is the mean and σ is the standard deviation of the local energy
distribution, k is a positive constant set to 2 in this work. To investigate the effect
of different parameters on edge detection results one can scan the filter response over
different parameters. Values of λmin = 3, k/wo = 0.65, and δ = 2.1 over a total of 6
scales gave good edge localization results (see fig 2.5-b).
Figure 2.5: Phase congruency detection examples with different filter parameters. a) λmin = 1,
b) λmin = 3, c) λmin = 6.
The effect of decreasing λmin can be appreciated in fig 2.5-a, where the filter enhances
local features at relatively higher frequencies. In contrast, increasing λmin (fig 2.5-c)
appears to blur out some features and local structure is detected at lower frequencies.

Chapter 2. Breast boundary localization and 3D extraction 26
2.4 Breast surface via Poisson reconstruction
2.4.1 Poisson surface reconstruction
In this section, the Poisson surface reconstruction method is tested to reconstruct the
breast surface from oriented points obtained from phase congruency filtering in order to
extract an initial estimation of the breast region boundary.
Seminal work on surface reconstruction methods [49, 50, 51, 52] have been motivated
on reconstructing surfaces from 3D range scanning data. Surface reconstruction from
point samples is a vast studied problem in computer graphics and has been previously
treated as an inverse problem. Hoppe et al. [49] proposed to infer automatically the
geometry and topology of a surface (or two dimensional manifold) S given as input par-
tial information about sampled points on or near the surface and information about the
sampling process. Furthermore, Kazhdan et al. [51] showed that the surface reconstruc-
tion problem from a set of oriented surface points could be treated as a spatial Poisson
problem. Solving a surface reconstruction problem as a Poisson system offers resilience
to noise and the fitting process is global to all data. The key insight to the Poisson for-
mulation is that there is a very close relationship between oriented set of points sampled
on a surface and the gradient of the surface’s indicator function χM , which is a labeling
function whose value is zero at points outside of the region enclosed by the surface and
is one at points inside, i.e:
χM(p) =
1 p ∈M
0 p /∈M(2.5)
This relationship is strengthen by the properties of the gradient function. First, the
gradient of the surface’s indicator function ∇χM is a vector field whose components are
the partial derivatives of χM . Second, the gradient function is zero almost everywhere
(since the indicator function is mostly constant) except at points near the surface, where
is equal to the inward surface normal. Thus, based on this geometric property of the

Chapter 2. Breast boundary localization and 3D extraction 27
gradient, a set of normal surface vectors can be viewed as samples of the gradient of the
indicator function.
Figure 2.6: Schematic of Poisson surface reconstruction in 2D. Adapted from [51].
In this context, Poisson surface reconstruction is an implicit function fitting method,
in which an implicit function in 3D is fitted to sampled points and then the surface is
extracted as an iso-surface of the implicit function (see figure 2.6). The idea behind this
approach is to infer the topology of an unknown surface by solving the 3D indicator
function χM ,
Khazhdan et al. [51] proposed to estimate the gradient of the indicator function χM ,
as the function that best approximates the vector field defined by point normals ~V , which
is equivalent to:
minχM‖∇χM − ~V ‖ (2.6)
This variational problem can be transformed into a Poisson problem: finding the best
solution involves computing a least-squared approximate solution of the scalar function
χM whose Laplacian (divergence of the gradient) equals the divergence of the vector field
~V :
∆χM ≡ ∇.∇χM = ∇.~V (2.7)

Chapter 2. Breast boundary localization and 3D extraction 28
The Poisson system on equation 2.7 is solved based on the fundamental theorem of
calculus which formalizes the relationship between a solid model and samples of oriented
points on its surface. The Divergence Theorem states that the integral of the divergence
of a vector field over a solid is equal to the surface integral of the vector field over the
boundary. So that, for example, integrating the divergence of ~V is equal to the value
obtained by walking over the boundary of the region M (see figure 2.6) and summing the
values of the dot-product between the vector field and the surface normals ~V (s).~n(s).
2.4.2 Maximal phase congruency and edge point orientation
Points of maximal phase congruency coincide with features of high edge strength and
therefore can be thought as points of maximal edge potential. To estimate the orientation
of points at the breast boundary that correspond to maximal phase congruency, points are
sampled with an orientation corresponding to the gradient of the image. The gradient of
an image is a vector field that encodes the directional changes of the grey-level intensities
in the image. Broadly speaking, at the air-breast boundary interface, the gradient vectors
are normal vectors in the direction of the maximum change in intensity (i.e point inward
the breast-air boundary). The change in intensity at the breast-chest wall for Dixon
sequences is in the expected direction as well. In the lower and upper portions of the
breast no real edge information is present and therefore points are not sampled on these
regions. Hole-filling is one of the appealing properties of implicit surface reconstruction
methods [50]. Even in the presence of holes or missing point samples, the reconstruction
algorithm is guaranteed to return the surface of a solid model under appropriate sample
density. Then, the reconstructed mesh will be a closed surface and all the holes will have
been filled in. One of the limitations of this approach is the necessity to invert the sign
of the gradient vectors if for a different MRI breast sequence, the breast region is hypo-
intense with respect to the chest wall tissue. Figure 2.7 shows maximal phase congruency
points and their corresponding orientations based on the gradient of the image at the

Chapter 2. Breast boundary localization and 3D extraction 29
Figure 2.7: Extracting points of maximal phase congruency and estimating their orientation.
a) mask of maximal phase congruency points, b) Image gradient for sampling orientation of
points.
same locations. In figure 2.7-a, a thresholded phase congruency image is shown where
bright areas correspond to regions of maximal phase congruency. Figure 2.7-b shows the
directional vectors of the corresponding locations. The color represents the magnitude
of the gradient at a given point. Also the inward direction of the vectors pointing to the
inside of the breast can be appreciated.
2.4.3 Implementation via Octree structures
The starting point for the Poisson problem is to obtain the vector field ~V from boundary
points. The Poisson inverse gradient method solves the inverse problem for approximating
a scalar field ( χM) when ~V is a non-conservative force field and therefore cannot be
expressed as the gradient of any scalar function. However, χM can be approximated over
a region such that the gradient of χM is the closest to ~V . Discretization of the problem
can be done in a natural manner using the pixel grid over which the image is defined, but

Chapter 2. Breast boundary localization and 3D extraction 30
such a uniform 3D regular grid becomes impractical for high resolution reconstructions
[50]. A more efficient discretization is possible using an adaptive octree. An adaptive
octree is a 3D hierarchical data structure, where the subdivision unit is a cube that can
recursively be subdivided into eight smaller cubes or octants, hence the name octree.
Octrees use a node structure to store volumetric elements. Figure 2.8 shows an octree
with 2 levels of subdivision or octree depths (D = 2). This sequential subdivision is
represented on a spanning tree, where each node has eight children nodes. In an octree,
the resolution in each dimension increases by two at each subdivision level. Therefore,
to reach a resolution grid of 256x256x256, an octree with depth equal to 8 is required
(28 = 256). Kazhdan et al. [51] approach uses the positions of the sample points to
Internal node
Leaf nodeRoot
Level 1
Level 2
Figure 2.8: Schematic drawing of an octree hierarchical subdivision. Left: Recursive subdivision
of a cube into octants. Right: The corresponding octree. Adapted from [?].
define an octree O and associate a function Fo to each node of the tree. The Octree
is defined over the dataset to be the minimal octree with the property that every point
sample falls into at a node that is no longer subdivided at depth D, also known as a
leaf node. The function space Fo is built in a multiresolution fashion for more efficient

Chapter 2. Breast boundary localization and 3D extraction 31
computation: high resolution near the samples and coarser resolution at farther distances.
The selection of space functions Fo has additional advantages since the vector field ~V
can then be represented as the linear sum of the Fo and the Poission equation can be
solved as a matrix multiplication in terms of Fo. For every node o ∈ O, Fo is set to be
the ”node function” centered about the node o and stretched by the size of o:
Fo(p) ≡ F
(p− cw
)1
w3(2.8)
where c and w are the center and the width of node o respectively. The function F is
defined as the n-th convolution of a box filter with itself:
Fo(x, y, z) = (B(x)B(y)B(z))n with B(t) =
1 |t| < 0.5
0 otherwise(2.9)
as n increases Fo approximates a unit-variance Gaussian, in this work n = 3. Trilinear
interpolation is used to sample the point sample position across the eight nearest neighbor
nodes NgbrD(p). Finally, the gradient of the indicator funcion can be approximated as:
~V (p) =∑p∈∂M
∑o∈NgbrD(p)
αo,pFo(p) ~N(p) (2.10)
where αo,p are the trilinear interpolation weights for point p closest to the eight depth-D
nodes NgbrD(p), and ~N(p) is the estimated orientation of point p. Having obtained the
vector field ~N(p), the next step is to solve the Poisson equation to find the function χ such
that its gradient ∇χM is the closest to ~V . In this work, the breast boundary indicator
function χ is represented in an adaptive octree and the Poisson equation is solved in
successive well conditioned sparse liner systems at multiple octree depths. The method
can be summarized in three main steps: 1) The relationship between the gradient of the
indicator function and an integral of the field of surface normals is established. 2) The
surface integral is solved by a summation over the given oriented point samples. 3) The
indicator function is reconstructed from the gradient field as a Poisson problem.

Chapter 2. Breast boundary localization and 3D extraction 32
2.4.4 Extracting the breast boundary as an isosurface
The indicator function for the breast boundary (χM) corresponds to a scalar field where
equal values define isolines in 2D or isosurfaces in 3D (see figure 2.9). In order to obtain
the breast boundary reconstructed surface ∂M , it is necessary to select an appropriate
isovalue and then extract the corresponding isosurface from the indicator function. An
optimal isovalue is one that extracts an isosurface that is closest to the edges of the
breast region (i.e the extracted surface should closely correspond to the position of the
input samples). A natural way to extract this isosurface is to evaluate χM at the sample
positions (s ∈ S) and used the average sampled value as the optimal isovalue:
∂M ≡ {q ∈ R3 | χM(q) = γ} with γ =1
|S|∑s∈S
χM(s) (2.11)
Figure 2.9: Initial breast boundary surface via Poisson surface reconstruction. a) Poisson
reconstruction of breast boundary indicator function with color-coded isolines in 2D at equal
isovalues. b) An example of a extracted breast boundary (∂M) obtained with equation 2.8. c)
A view on 2D of a slice of the closed surface.
Once an appropriate isovalue γ is found, the 3D mesh representing the surface is
extracted using a Marching Cubes isosurface generation algorithm [53] adapted to octree

Chapter 2. Breast boundary localization and 3D extraction 33
representations [54] [52]. Figure 2.9 shows a surface reconstruction example that was
solved using an octree depth of 8, which corresponds to an octree resolution of 2563. Some
spurious clusters of the surface are captured on the chest region where edge features are
also detected. These elements however, do not necessarily interfere with the estimation
of the complete breast surface and can be removed with an additional refinement step
described in the next chapter.
2.5 Conclusion
Phase congruency edge detectors were used to extract features of edge significance. The
computation of phase congruency in this work has the advantage of avoiding the use of an
oriented filter bank, which entails the selection of multiple appropriate filter orientations.
Surface reconstruction based on a Poisson formulation using edge features identified with
the edge detector robustly extracts the boundary of the breast as a surface. The results
obtained indicate that both methods are appropriate for building upon the next phase
of the segmentation pipeline, which attempts to redefine the surface of the breast region
to finalize the segmentation.

Chapter 3
Atlas-based segmentation of the
breast in 3D
3.1 Introduction
The extraction of an atlas of the breast in 3D using a population is described in this chap-
ter. Section 3.2 reports the feasibility of combining groupwise and pairwise registration
for establishing subject correspondences as well as the landmark-based representation of
the average volume. Generating a shape representation of the breast in 3D can be sum-
marized into two main sections: 1) Deriving the average breast volume in the population
using groupwise registration, and 2) generating an automatic shape representation based
on a 3D mesh.
The rationale for using an atlas for segmentation is to incorporate high-level or expert
knowledge about the shape of the breast in 3D. This approach is more robust to local
image artifacts and noise than low-level algorithms. In general, adapting an atlas or
model to an image suffers from a common problem to all local search algorithms, and
that is their vulnerability to stop at local minima and not necessarily find the global
optimum. However, if the search is properly initialized in proximity to the desired global
34

Chapter 3. Atlas-based segmentation of the breast in 3D 35
optimum often times the found local minimum will be close to the optimal solution and
the segmentation will be successful in matching the atlas to the desired image features.
For breast segmentation in MRI, thresholding operations to remove the background of
images have been proposed to obtain a scalar map of labels to guide the segmentation [27]
[55]. However, as explained on chapter 1, Breast MRI is often affected by low contrast,
field inhomogeneities and coil artifacts that render selective thresholding techniques weak
candidates to correctly separate tissues in the chest-wall. In this context, a more robust
approach is to use the edge map (phase-congruency, see section 2.3) and the estimation of
the breast region surface (Poisson reconstruction, see section 2.4) for proper initialization
of the atlas. The basic idea for proper initialization is to draw the atlas towards the edges
of the image so that its initial position is close to the desired boundaries.
This chapter describes the final step in the segmentation pipeline, which consist on
adapting the population atlas to the found target surface during initialization. Section
3.3 describes an approach to automatically map 3D landmarks from the atlas surface
to the initialization surface by treating landmark mapping as a correspondence problem
that can be solved using a Laplacian framework. Section 3.4 describes the validation
results of the segmentation and the evaluation of the algorithm performance.
3.2 Extracting a shape atlas of the breast in 3D
3.2.1 Groupwise registration and average volume extraction
An entropy-based groupwise registration using the stack entropy cost function (Balci et
al. [56]) and a multi-resolution B-spline free form deformation (FFD) introduced by
Rueckert et al. [57] was used to register the total set of available breast cases. Since
all breast datasets were acquired with the same acquisition protocol, they are similar in
terms of contrast, size, and orientation. Therefore, it is suitable to perform volumetric
grey-level registration. The choice of groupwise registration was motivated on finding a

Chapter 3. Atlas-based segmentation of the breast in 3D 36
population-based correspondence.
Figure 3.1: Population-based construction of the average volume. Selected sagittal slices of
mean volume and standard deviation volume in the population: a) before groupwise registration
and b) after groupwise registration. (Top row) mean and (Bottom row) standard deviation.
A common approach when registering a population of images is to register every sub-
ject in the population to a reference subject or template, using pairwise registration.
The problem with this approach is that some bias is introduced with the arbitrary se-
lection of the reference image. A strategy to overcome this bias is to avoid using an
arbitrary subject as an anatomical reference but rather construct a template from the
joint statistics of the population. Groupwise registration schemes have been developed
for this purpose. Balci and colleagues [56] used a multi-resolution registration approach
that considers the sum of univariate entropies along pixel stacks as a joint alignment
criterion. The registration starts with global affine transformation at a coarse scale and
proceeds with successive nonrigid deformations at finer scales in an attempt to capture
anatomical variability while minimizing the entropy in the population. The idea is that
if the images are aligned properly, intensity values at corresponding image locations will

Chapter 3. Atlas-based segmentation of the breast in 3D 37
form a low entropy distribution. The results of the registration were visually assessed
using the mean and the standard deviation volumes before (see Figure 3.1-a) and after
(see Figure 3.1-b) registration. The mean image appears to get sharper and the standard
deviation volume gets narrower, indicating that the alignment of the images increases
after performing groupwise registration.
3.2.2 Population shape average and 3D shape representation
The purpose of performing groupwise registration is to obtain the average breast volume
of the population. In this work, the average breast volume is further thresholded to
obtain a binary volume. The marching cubes algorithm [53] on the binary volume was
used to generate a dense surface representation of the shape of the breast in 3D. Following
surface generation, a series of local operations on geometry and topology on the surface
triangulation (Schroeder et al. [58]) were performed to reduce the number of surface
elements.
Figure 3.2: Average shape representation with varying decimation factors: a) 25% decimation,
b) 75% decimation and c) 95% decimation.
The decimation algorithm works by removing excess triangles where the curvature of

Chapter 3. Atlas-based segmentation of the breast in 3D 38
the surface is low but preserves edges by keeping dense triangulations where the curvature
of the surface is high. After decimation, the spatial coordinates of the decimated mesh
vertices were selected as landmark points. Table 3.1 summarizes the number of landmarks
generated by using different decimation factors from an initial triangulation consisting on
Mesh decimation
Decimation factor 25% 50% 75% 95% 98%
# Landmarks 5743 3829 1915 384 348
# Triangles 11482 7654 3826 764 692
Table 3.1: Number of landmarks and triangles generated after surface mesh decimation.
7657 vertices and 15309 triangles. The density of triangle elements in the representation
of the average shape is reduced with an increasing decimation percentage (see figure 2.2).
The decimation percentage indicates the percent ratio between the triangle elements
that are eliminated with respect to the initial set of 7657 triangles. Different decimation
percentages (25%, 50%, 75%, 95% and 98%) were investigated. In addition, connectivity
data between landmark points was generated for further representation of structures.
3.3 Mapping 3D atlas landmarks via a Laplacian frame-
work
After obtaining the optimal isosurface to initialize the segmentation as explained on the
previous chapter, the next step in the segmentation pipeline is to incorporate shape
information contained on an atlas. For this purpose, the atlas is initially aligned to
the found isosurface by means of a rigid landmark transformation. The remaining step
before matching the atlas to the extracted surface is to map the atlas points to the
found optimal surface. This is in nature a correspondence problem and can be solved

Chapter 3. Atlas-based segmentation of the breast in 3D 39
using the mathematical properties of the Laplace equation. Figure 3.3 illustrates how
the correspondence can be solved and can be summarized as follows:
Figure 3.3: Initializing model points into optimal isosurface. a) binary versions of surfaces. b)
area enclosed between surfaces. c) Solution to Laplace equation. d) Normalized gradient.
Using the optimal isosurface on a binary image representation (Siso) and a binary
version of atlas (Sm), it is possible to find the region enclosed between the two aligned
surfaces (see figure 3.3-b) and solve a Laplacian equation with two boundary conditions,
each one corresponding to two fixed and different potentials as follows:
∇2ψ =δ2ψ
δx2+δ2ψ
δy2+δ2ψ
δz2= 0 (3.1)
with boundary conditions: ψ = ψ1 on Sm and ψ = ψ2 on Siso, where (ψ1, ψ2) are two
different fixed potentials. The solution to the Laplace equation is a scalar field ψ that
provides a transition from surface Sm to Siso as defined by set of nested surfaces [59] with
constant values between ψ1 and ψ2. Furthermore, given the geometric properties of the
Laplace equation, computing the normalized negative gradient of the Laplace solution,

Chapter 3. Atlas-based segmentation of the breast in 3D 40
N:
N =−∇ψ‖ −∇ψ ‖
(3.2)
returns a unit vector field that defines streamlines or field lines connecting both surfaces.
These streamlines are defined as being everywhere orthogonal to all equipotential surfaces
defined between the two surfaces. The resulting vector field can be used to map the path
between two corresponding points (i.e p1 on Sm to p2 on Siso). The path connecting p1
to p2 can be parameterized so the path is described by a vector function C(s) as follows:
∫ p2
p1
N(C(s))ds (3.3)
Initializing a given 3D landmarked point involves solving the above integral between the
atlas surface and the initialization iso-surface. This algorithm is implemented as follows:
Algorithm 3.1 Initializing model points into optimal isosurface Siso
Require: Binary representations of isosurface Siso and atlas Sm
Find region ∼ Sm ∩ Siso
Solve Laplace eq. 3.1 over ∼ Sm ∩ Siso
Find N = −∇ψ‖−∇ψ‖
Find∫ p2p1
N(C(s))ds
3.4 Validation: Segmentation of population cases
To quantitatively assess the performance of the 3D atlas-based segmentation approach,
segmentation errors with respect to target surfaces were determined for the total popu-
lation (n = 409) on a leave-one-out approach. The test can be summarized in 7 steps
which are illustrated on figure 3.4. First, a shape atlas is built using all but one case
of the training population. Second, the omitted case is treated as an unseen case, and

Chapter 3. Atlas-based segmentation of the breast in 3D 41
therefore a phase congruency edge map is extracted followed by the boundary surface via
Poisson surface reconstruction, and finally, the atlas is mapped to the breast boundaries
using a Laplacian approach explained on section 3.3.
Build population
atlas
1
Stage 2:
For omitted case on stage 1:
Phase congruency,
edge points selection
2
Sample point
orientations
3
Solve Poisson
system from V
4
Stage 1:
For all-but-one cases on population:
5Extract
isosurface
6map atlas points
to isosurface
Stage 3:
Final atlas-based segmentation
Figure 3.4: Experimental design to assess performance of segmentation using a leave-one-out
approach.
The test provided fully automatically segmented breast boundary surfaces. We com-
pared a total of 367 breast volumes, since 42 cases were excluded due to failures in the
initial surface alignment (steps b) and f) in fig. 3.6). The goal of our experiments was to
evaluate how accurate was the segmentation of the breast obtained with our algorithm
with respect to the expert segmentation. We therefore looked at distance errors from
surface to surface, volumetric errors in cm3 as well as standard overlap metrics such as
the the total volume overlap, the mean overlap and the Dice coefficient.

Chapter 3. Atlas-based segmentation of the breast in 3D 42
3.4.1 Distance errors
Distances were measured from the shape atlas to the breast boundary iso-surface after the
initial Poisson boundary reconstruction (see table 3.2) and after finding corresponding
points using the Laplacian equation (see table 3.3). Segmentation errors were computed
as the Euclidean distance (in mm) between each atlas point (xi) and the closest point
(xtargeti ), located on the surface of the original manually segmented shapes:
Serror = d(xi,xtargeti ) =
√√√√ N∑i=1
|xi − xtargeti |2 (3.4)
This distance reflects the proximity of the segmented surface to the target surface, since
a very accurate segmentation is attained when all atlas points lie on the target surface
and the segmentation error is zero.
After Poisson Quartiles of distances (mm)
Boundary region 0.25 0.50(median) 0.75 IQR
air-breast 0.63 1.41 3.61 2.97
breast-chest 0.63 1.40 3.93 3.30
Table 3.2: Distances from manually annotated surfaces discriminated by boundary region after
Poisson surface reconstruction. IQR=Interquantile range.
After Laplacian Quartiles of distances (mm)
Boundary region 0.25 0.50(median) 0.75 IQR
air-breast 0.79 1.36 2.93 2.15
breast-chest 1.12 2.68 4.82 3.70
Table 3.3: Distances from manually annotated surfaces discriminated by boundary region after
Laplacian correspondences. IQR=Interquantile range.
By labelling the relative position of each individual landmark in the shape atlas, one
can discriminate the mapping accuracy among specific regions of the breast boundary,

Chapter 3. Atlas-based segmentation of the breast in 3D 43
such as the chest-wall or the air-breast boundary regions. Table 3.2 and 3.3 summarizes
the mapping accuracy by the algorithm. Figure 3.5 shows a comparison between the
target distance errors for the two stages of segmentation, after Poisson surface recon-
struction and after Laplacian mapping of atlas points. The distance errors given by the
outliers in the distribution are larger for the Poisson surface reconstruction results. This
is likely the result from the spurious detection of edge features in the thoracic region,
which are mostly removed with the used of the 3D atlas Laplacian mapping stage. Due
to the fact that the Laplacian is a correspondence mapping procedure, the accuracy is
reduced in the chest wall as indicated by the median from 1.4 mm to 2.68 mm. This loss
in accuracy could be reversed by using the result of the Laplacian as a mask to remove
the spurious elements in the chest region.
Figure 3.6 shows representative results of the breast boundary reconstructions and
the atlas mapping segmentation. For illustrating the technique two cases are shown. The
first case (top row) is a large sized breast with a manually measured volume of 1229.21
cm3 and an atlas-based segmented volume of 1136.59 cm3. The second case (bottom
row) is a smaller sized breast with a manually measured volume of 572.8 cm3 and an
atlas-based segmented volume of 601.5 cm3. The color-coded surfaces on figure 3.6-d and
3.6-h illustrate the distance to target surfaces after mapping atlas points (figures 3.6-c
and 3.6-g) to the Poisson reconstructed surface (figures 3.6-a and 3.6-e).
3.4.2 Volume errors
In order to test the impact of the segmentation accuracy on the breast volume assessment,
in addition to distance errors, volume errors between manually annotated volumes and
the total volume enclosed by our segmentation boundaries were also computed according
to Alyassin et al. [60]. For the total breast volumes measured in cm3, the median of the
absolute percent measurement error was 6.75%. Figure 3.6 presents the Bland-Altman
plot that compares the volumes obtained automatically with the volumes measured from

Chapter 3. Atlas-based segmentation of the breast in 3D 44
0
10
20
30
40
50
60
70
80
90
100
Comparison of distance distributions after Poisson Reconstruction and Laplacian atlas mapping.
Breast-air region
after Poisson
Clo
sest dis
tance to s
urf
ace (
mm
)
Breast-air region
after Laplacian
Chest-wall region
after Poisson
Chest-wall region
after Laplacian
Figure 3.5: Box-and-Whisker plots: Comparison of target distance errors for the two stages
of segmentation, after Poisson surface reconstruction and after Laplacian mapping of atlas
points. Points are drawn as outliers if they are larger than q3 + 1.5(q3 − q1) or smaller than
q1− 1.5(q3− q1), where q1 and q3 are the 25th and 75th percentiles, respectively.
the manual segmentations. The magnitude of the disagreement (in terms of bias and
limits of agreement) was 29.8 cm3 (-141.5 to 201.1) cm3. The scatter of the values tends
to increase for larger volumes. The fact that some values are more scattered on the
negative side of the plot (with respect to zero difference line), indicates that in some
cases the automatic segmentation tends to underestimate the true volume of large breast
volumes (<900 cm3).

Chapter 3. Atlas-based segmentation of the breast in 3D 45
Figure 3.6: Representative results of 2 breast boundary reconstructions (top and bottom):
a) and e) Breast iso-surface (output of Poisson reconstruction). b) and f) Aligned mean of
population showing initial position of atlas points before Laplacian mapping. c) and g) Mapping
results to target surface via Laplace equation. d) and h) Color-coded closest distances to manual
annotated surfaces.
3.4.3 Evaluation of standard overlap metrics
The evaluation of standard overlap metrics [61] was performed to test the agreement of
our segmentation with the manual results. Overlapping metrics can be explained with a
Venn diagram (see figure 3.7). Basically, the idea is to quantify the overlapping fraction
of two partially overlapping objects: a source S (model-based) and target T (manual)
segmentation volumes. In this work, two agreement measures and two error measures
were explored. The two agreement measures consists of total volume overlap (To) and
mean overlap also known as the Dice coefficient (Mo), which are defined as follows:
To =|S ∩ T ||T |
(3.5)

Chapter 3. Atlas-based segmentation of the breast in 3D 46
Figure 3.7: Bland-Altman plot showing the difference between automatic and manual measure-
ments of total breast volume (in cm3) against the average of the two methods.
Standard overlap metrics results
Metric mean ± std
Total overlap 0.89 ± 0.05
Mean overlap (Dice) 0.88 ± 0.04
False-negatives 0.11 ± 0.05
False-positives 0.13 ± 0.07
Table 3.4: Agreement and error overlap results (n=367).
Mo = 2
(|S ∩ T ||S|+ |T |
)(3.6)
where the operator || indicates volume computed as number of voxels. The two error
measures were metrics indicating the false negative (FN) and false positive (FP ) frac-
tions. The false negative error for a given volume can be measured as the fraction of the
target that falls outside of the source volume. Similarly, the false positive error can be

Chapter 3. Atlas-based segmentation of the breast in 3D 47
Figure 3.8: Overlap metric assessment for segmentation results. Venn diagram illustrating the
relationship between partially overlapping objects.
measured by how much of the source volume falls outside of the target volume:
FN =|T \ S||T |
(3.7)
FP =|S \ T ||S|
(3.8)
The table 3.3 summarizes the results obtained with the aforementioned metrics. Re-
sults are expressed in fractions as mean ± std. Figure 3.8 shows the distribution of
target overlap, mean overlap (Dice), false-negative and false-positive values as well as
the volume and surface areas obtained for the population of segmented examples. Figure
3.9 shows the distribution of percentage and absolute percentage error for total breast
volume and total surface area.
3.5 Conclusion
In this chapter, a method for obtaining the average of the population and an automatic
breast volume segmentation were described. The boundary localization results demon-
strate error distances from manual surfaces with an IQR of 2.15 mm for the air-breast

Chapter 3. Atlas-based segmentation of the breast in 3D 48
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Distribution of Overlap metrics (n=367)
total mean union FN FP
(a) (b)
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
total mean FN FP
Distribution of overlap metric (n=367)
Figure 3.9: Boxplots: Distribution of overlap metrics, breast volumes and surface areas of
the manually segmented datasets compared with the atlas-based segmentation results. a) total:
total overlap, mean: Mean overlap (Dice), FN: false negative fraction, FP: false positive fraction.
b) Distribution of volumes and surface areas.
boundary and 3.7 mm for the breast-chest wall boundary. This indicates that the error
for localizing the breast-air boundary is within sub-resolution accuracy. Errors are rel-
atively higher for localizing the chest-wall boundary, probably due to the low contrast
between adjacent tissues to the breast in this region. However, the results obtained are
encouraging for using phase congruency edge detection and Poisson surface estimation to
segment the total volume of the breast. Furthermore, incorporating a manual override to
the automatic segmentation framework will be a feasible approach for computing total
breast volume during breast density assessment using MRI.

Chapter 3. Atlas-based segmentation of the breast in 3D 49
% Volume
error
70
60
50
40
30
20
10
0
-10
-20
-30
-40
% Absolute
Volume
error
% Surface
Area
error
% Absolute
Surface
Area error
Percentage and Absolute percentage Volume and Surface errors
Figure 3.10: % Error and Absolute % error for Volume and Surface areas when compared with
manual segmentations.

Chapter 4
Conclusions and future directions
4.1 Contribution of this work
4.1.1 Segmentation for breast density assessment
As stated on chapter 1, breast segmentation is a prerequisite task for breast density as-
sessment using MRI. In general, prior to the quantification of the proportion of water
content in the breast it is necessary to determine the total breast volume. This thesis
presents an automatic segmentation framework that allows the computation of the total
volume of the breast while excluding non-breast tissues, which facilitates the quantifi-
cation of breast density. This work attempts to first identify features of local phase
information in the image and then adapt a shape atlas to the found features. The use of
invariant features to contrast and illumination for edge detection as well as the use of a
shape atlas are attractive characteristics of the method. This signifies that the segmenta-
tion framework is not dependent on image intensity and may be applicable to other MRI
sequences or imaging modalities such as 3D mammography with breast tomosynthesis.
Several breast segmentation methods and density assessment methods for breast MRI
have appeared in the literature. Khazen et. al [30] used non-uniformity correction based
on the proton density data before performing threshold-based segmentation to exclude
50

Chapter 4. Conclusions and future directions 51
the background. Nie et al. [27] separated fat and fibroglandular tissue by applying the
fuzzy C-means algorithm, which requires manual adjustments of the number of clusters
depending on the fat content in the breast, a reason why this method has been criticized.
The segmentation performance results agree well with other methods. Ertas et al. [62]
proposed extracting the breast region using two cellular neural networks (CNNs). The
first CNN performs grey-level thresholding, the second erases small objects by perform-
ing morphological operators. Although the authors compared two cases with manual
segmentations, no numerical error analysis were performed. A recently published work
by Wang et al. [63] uses Hessian-based filters to segment the Pectoralis muscle boundary
in breast DCE-MRI. The main idea is to differentiate the boundary based on sheet-like
local structure of neighbouring pixels. The authors reported a mean distance error of
1.43 mm with a standard deviation of 0.46 mm for 30 datasets.
4.1.2 Segmentation in the context of CAD systems
In recent years, magnetic resonance imaging (MRI) of the breast has received consider-
able attention as an emerging tool for the detection and diagnosis of breast tumors [64].
Dynamic contrast-enhanced MRI (DCE-MRI) provides information about increased vas-
cularity and capillary permeability in lesions which adds sensitivity for lesion differenti-
ation. Breast MRI has been shown to have higher sensitivity than mammography and
ultrasound [65] in high risk populations, particularly for detecting cancers in women with
genetic risk factors for breast cancer [65],[66] and with dense breasts [67]. Despite its
well known advantages, translation of MRI into clinical practice has encountered some
difficulties, especially the lack of standardization and interpretation guidelines. Some of
the main drawbacks of MR mammography are the high inter-observer variability [68], as
the interpretation of scans still relies on subjective visual assessment. Given the large
volume of data produced per exam, evaluation of these images by the radiologist is a
very time-consuming task and a experience dependent process. On the other hand, there

Chapter 4. Conclusions and future directions 52
is growing evidence to suggest that quantitative computerized interpretation in the con-
text of computer-aided diagnosis (CAD), may improve the accuracy [69], specificity [70],
objectivity and consistency [70],[71],[72] of breast MRI interpretation.
Current FDA approved breast MRI CAD workstations provide post-processing image
features (e.g color-maps of contrast kinetic parameters, time-intensity curves), which
facilitates the reviewing process, by making MRI data more comprehensible. However,
breast MRI CAD’s full potential has not been reach yet in providing a computer-aided
evaluation of the degree of suspicion in a lesion. The need for computer-aided diagnostic
(CAD) systems is relevant when it comes to improve diagnostic accuracy while retaining
high sensitivity and efficiency for breast cancer diagnosis. One of the fundamental ideas
for DCE-MRI automatic lesion detection is that surrounding non-breast regions such as
the chest wall muscles, thoracic cavity, lungs and heart must be previously segmented
out to prevent false-positive detections on these regions. Therefore, a prerequisite for
computer-aided lesion detection is the segmentation of the breast region. For this reason,
the 3D automatic breast segmentation presented in this work has important implications
in the context of CAD development and validation.
4.2 Future directions
Although no quantitative measurement of breast density was performed in order to com-
pare the automatically segmented results with the manually segmented ones, a feasible
extension of the stage of this work is the implementation of a graphical user interface
(GUI). With a GUI the automatic segmentation can be incorporated with a manual
override to the breast density assessment workflow.
The integration of the breast boundary localization described in this thesis as the
starting point for a subsequent model-based segmentation is a logical extension of this
work. The advantage of incorporating an additional step on the segmentation pipeline is

Chapter 4. Conclusions and future directions 53
to perform model-based segmentation, which offers potentially a more robust segmenta-
tion. Statistical shape models (SSM) incorporate prior knowledge about the structure of
the object to be segmented and are able to learn patterns of biological variability. This
variability is compactly represented with a model of variation and can be of shape or
appearance. Hence, a logical direction of this work is to build an statistical shape model
(SSM) from the groupwise registered shapes. Preliminary results towards this end were
obtained and are reported on Appendix A. The performance of the model-based seg-
mentation was tested on the total population of shapes that were initialized successfully
(n=367). It is expected that an additional model-based adjustment to the boundaries
will refine the 3D representation of the breast surface and reduce the distance errors.
In contrast, the comparison of results shown in figure 4.1 indicate that the chest-wall
distance errors increase with the SSM model fit to the boundary points as well as the
volume discrepancy, demonstrating that further improvement is necessary.
This increase on errors can be due to a number of pitfalls with the current model
fitting algorithm:
1) The least-square fit of the model to the points can be strongly affected by the pres-
ence of outliers during the search for landmark positions. Other optimization schemes
for matching the model to the found points during search could be optimal. Gradient
descent optimization could be implemented if the partial derivatives of an error function,
such as a weighting function that penalizes the fit to an outlier, is added to the min-
imization of the sum of squares. To this end Lekadir et al. [73] proposed a weighted
fitness measure using the ratio of interlandmark distances as a local shape dissimilarity
measure for each outlier based on a tolerance model.
2) Another problematic area is the use of PCA for dimensionality reduction, since
there is an explicit assumption that the data distribution forms a linear subspace. Fur-
thermore, by manipulating the shape parameter vector b on equation 9 (see appendix A),
different shapes can be generated. Now the allowed variation from the mean of the popu-

Chapter 4. Conclusions and future directions 54
(a) (b)
Volume
error %
Absolute
Volume error %
Volume
error %
Absolute
Volume error %
Figure 4.1: Model fitting compared to boundary localization distance error results. a) Distance
and Volume errors after Laplacian initialization of the atlas. b) Distance and Volume errors
after SSM model fitting.

Chapter 4. Conclusions and future directions 55
lation is limited by hard shape constraints imposed with the radial basis function matrix.
The quality of the radial basis functions or modes of variation used in the model is highly
relevant. It is clear that the captured variability should ideally only capture variation
due to shape differences among the training cases, an not due to correlated global differ-
ence (e.g changes in position). Therefore global linear transformation components such
as translations or rotations should be completely excluded from the deformations used
to aligned the cases (conventionally, Procrustes analysis [74]). If similarity deformations
are not removed, the first modes of variation will not necessarily capture the truly largest
variation in shape. In this work, it is possible that residual variation could be preventing
the modes of variations to broadly capture shape variability.
3) A third area of potential improvement is decreasing the shape constraints imposed
by the model. Relaxing the hard shape constraints and allowing additional flexibility
during model fitting has been previously proposed. One traditional approach on this
paradigm is to fit a normal SSM until convergence and then include an additional re-
finement stage that improves the fitness to edge-based features, usually using a free
deformation. Heimann et al. [75] combines a statistical shape model and a deformable
surface using posterior probabilities given by the data.

Appendix A
Statistical shape model of the breast
in 3D
56

Automatic model-based 3D segmentation of the breast in MRI
Cristina Gallegoa,b, Anne L. Martela,b aDepartment of Medical Biophysics, University of Toronto, Toronto, Canada
bDepartment of Imaging Research, Sunnybrook Health Sciences Centre, Toronto, Canada
ABSTRACT
A statistical shape model (SSM) is constructed and applied to automatically segment the breast in 3D MRI. We present an approach to automatically construct a SSM: first, a population of 415 semi-automatically segmented breast MRI volumes is groupwise registered to derive an average shape. Second, a surface mesh is extracted and further decimated to reduce the density of the shape representation. Third, landmarks are obtained from the averaged decimated mesh, which are non-rigidly deformed to each individual shape in the training set, using a set of pairwise deformations. Finally, the resulting landmarks are consistently obtained in all cases of the population for further statistical shape model (SSM) generation. A leave-one-out validation demonstrated that near sub-voxel resolution reconstruction (2.5mm) error is attainable when using a minimum of 15 modes of variation. The model is further applied to automatically segment the anatomy of the breast in 3D. We illustrate the results of our segmentation approach in which the model is adjusted to the image boundaries using an iterative segmentation scheme.
Keywords: Breast Segmentation, population-based statistical shape model, Breast MRI.
1. INTRODUCTION In recent years, Magnetic Resonance Imaging (MRI) has received considerable attention as an emerging diagnostic tool for detection and characterization of breast tumors as well as for breast cancer risk assessment. As a consequence, the number of MRI breast examinations carried out is expanding rapidly and computational tools to analyze these studies are becoming widely demanded. In particular, excluding any non-breast regions is a prerequisite for many image analysis tasks such as in the case of computing image metrics for breast density assessment or for computer-aided diagnosis. In the development of computer-aided diagnosis (CAD) systems for breast MRI, automatically excluding non-breast regions particularly in the chest wall has become an important initial step to leave out all the potential false positive detections that occur in the chest wall during training and validation of the CAD.
Model-based segmentation based on statistical shape models (SSM) has been proposed as a suitable technique for locating objects with known structure. One of the most attractive aspects of SSM is their ability to incorporate prior knowledge about the anatomy to be segmented that accounts for biological variability and is introduced with the annotation of training cases. Coots et al.1 demonstrated the applicability of Active Shape Models (ASM) for segmenting structures in 2D images. However, constructing a 3D statistical shape model requires dense representation of surfaces in a training population as well as establishing correspondences among all surfaces. We have focused on automatically generating landmark correspondences using a population-based approach based on 3D deformable groupwise registration.
This work aims to develop a 3D SSM of the breast for fully automatic 3D breast segmentation. Our approach can be broken down into four main sections: 1) automatic landmark-based representation of the average shape in a training population, 2) automatic identification of landmark correspondences between the average shape and each individual shape in the population, 3) construction of a SSM and 4) adaptation of the SSM for 3D breast MRI segmentation.
In sections 2.2 and 2.3, we report the feasibility of combining groupwise and pairwise registration for establishing landmark correspondences, and test the ability of the SSM to reconstruct all shapes in the population in section 3.2. In sections 2.4 and 2.5, we present our approach to derive a SSM and match it to the anatomical boundaries of the breast for segmentation. Section 3 describes the experimental setup and validation of our methodology using a population of 415 training cases. Sections 4 and 5 present discussion of the significance of this work and conclusions.
Medical Imaging 2011: Image Processing, edited by Benoit M. Dawant, David R. Haynor, Proc. of SPIE Vol. 7962, 796215 · © 2011 SPIE · CCC code: 0277-786X/11/$18 · doi: 10.1117/12.877712
Proc. of SPIE Vol. 7962 796215-1
Downloaded from SPIE Digital Library on 06 Apr 2011 to 142.76.1.62. Terms of Use: http://spiedl.org/terms

2. MATERIALS AND METHODS 2.1 Segmented Breast Cases
A population of breast segmentations (n = 415) was used from a previous study by Boyd et al.2. Breast images were acquired in the sagital plane with a slightly modified version of the GE FSE Dixon sequence. A 28 cm field of view was used with a 256 x 128 acquisition matrix. The slice thickness was 7 mm interleaved with TE 14x8 ms, ETL 8 and TR 2500.
Each segmented breast consists of semi-automatically 2D delineated contours using an active contour approach with manual correction2. The delineated contours were stacked together in adjacent cross-sections. The resulting stacked volume was resampled to isotropic voxel size of 2.56 mm. Surface meshes representing the 3D breast anatomy were finally obtained from the isotropic volumes and these surfaces were used as the “gold-standard” for testing the accuracy of our automatic selection of landmarks (section 3.2) and the performance of our model-based segmentation approach (section 3.4).
2.2 Groupwise registration and 3D shape representation
An entropy-based groupwise registration using the stack entropy cost function (Balci et al.3) and a multi-resolution B-spline free form deformation (FFD) introduced by Rueckert et al.4 was used to register the total set of available breast cases. Grey-level isotropic volumes were used to derive the average breast volume of the population which was thresholded to obtain the final binary volume. The marching cubes algorithm on the final binary volume was used to generate a dense surface representation of the average shape in the population. Following surface generation, a series of local operations on geometry and topology (Schroeder et al.5) were performed to reduce the number of triangles. The decimation works by removing excess triangles where the curvature of the surface is low but preserves edges by keeping dense triangulations where the curvature of the surface is high. After decimation, the spatial coordinates of the decimated mesh vertices were selected as landmark points. Different decimation percentages (25%, 50%, 75%, 95% and 98%) were investigated. In addition, connectivity data between landmark points was generated for further representation of structures. Table 1 summarizes the number of landmarks generated by using different decimation factors from an initial set of 7657 landmarks. Results of the decimation are illustrated in Figure 1.
Figure 1. Decimation results with varying decimation factor of a) 25% decimation, b) 75% decimation, c) 95% decimation.
Proc. of SPIE Vol. 7962 796215-2
Downloaded from SPIE Digital Library on 06 Apr 2011 to 142.76.1.62. Terms of Use: http://spiedl.org/terms

Table 1. Number of landmarks generated after triangle mesh decimation with different decimation factors.
Triangle mesh decimations Decimation factor 25% 50% 75% 95% 98%
Total Landmarks 5743 3829 1915 384 348
2.3 Automatic selection of landmarks
Having obtained a set of landmarks on the average shape of the population, corresponding landmarks on each individual shape were generated using volumetric grey-level registration between individual cases and the average volume data. The result of this registration is a deformation field that can be use to map landmarks on the average shape in the registered space, to corresponding landmarks on each individual case back into the unregistered space, a method that is called “landmark propagation”. We assessed the accuracy of landmark propagations using both pairwise transformations between individual cases and the average volume data as well as inverted groupwise transformations already employed during the average volume extraction. A comparison between the groupwise and the pairwise generated deformation fields and their ability to produce suitable landmarks was performed. The landmark propagation error (equation 1) was computed as the Euclidean distance (in mm) between the ith
propagated landmark pix and the closest point surface
ix located on the surface of the original meshes described in
section 2.1. The closest point surfaceix to a landmark point p
ix is found using a spatial search structure 6.
( ) ∑=
−==N
i
surfaceiisurfacep xxXXdgElandmarkin
1
2p, (1)
2.4 Statistical shape model construction
After obtaining a set of corresponding landmarks among N shapes, a statistical shape model (SSM) is generated as introduced by Cootes et al.1. A single vector of concatenated 3D landmark coordinates represents each shape (equation 2) and principal component analysis (PCA) of the covariance matrix (equation 4) describes the principal modes of variation φk that can be captured in the population. Here φk is referred as the “kth eigenvector” and λk is the corresponding “kth eigenvalue” with the kth largest variance (equation 5). After sorting the eigenvectors φk and eigenvalues λk in descending order (i.e 1+≥ kk λλ ), the number of modes of variation is chosen so that the total variance of the model (equation 6) is at least 98%. As a result, the eigenvector matrix Φ is obtained by concatenating the first t eigenvectors (equation 7). { }111111000 ,,,...,,,,...,,,,,, −−−= imimimikikikiiiiiii zyxzyxzyxzyxX (2)
X =1N
Xii=1
n∑ (3)
Proc. of SPIE Vol. 7962 796215-3
Downloaded from SPIE Digital Library on 06 Apr 2011 to 142.76.1.62. Terms of Use: http://spiedl.org/terms

( )( )∑=
−−−
=N
i
Tii XXXX
ND
111
(4)
Dφk = λkφk (5)
∑=
=t
kkTV
1λ (6)
Φ = φ1, | ... |φk | ... |φt( ) (7)
With a statistical shape model (SSM), all shapes in the training population can be approximated using the mean shape (equation 3) and a linear combination of modes that account for the majority of the variation Φ weighted by appropriate shape parametersb (equation 8). Given the assumption that eigenvector matrix Φ is orthogonal, parameter b is a t-dimensional vector given by equation 9. bXX Φ+≈model (8)
( )XXb T −Φ= (9)
The ability of the model to accurately reconstruct each of the training cases was evaluated on a leave-one-out test. Before obtaining a reconstructed shape with the model a set of b parameters is computed using equation 9, where X are
the propagated landmarks (obtained in section 2.3), X is the mean shape and, TΦ is the transposed eigenvector matrix. The average reconstruction error (equation 10) was computed as the Euclidean distance (in mm) between the ith
predicted landmark ( modelix ) by the model of the omitted case and the ith propagated landmark ( p
ix ) of the same case.
( ) ( )∑=
−==N
iiip xxXXdtionEreconstruc
1
2pmodelmodel, (10)
2.5 Model-based segmentation of the breast
In this framework, a model-based segmentation is based on adapting the shape model to the boundaries of the breast. Points located in the air-breast boundary airy , are obtained in the normal direction of each model point as they intersect a boundary mesh product of a thresholding operation excluding the background and the chest wall region. Points located in the chest wall boundary chesty , are obtained in the normal direction of current model points as well but using the magnitude of the grey-level gradient of the image to locate the strongest edge. The edge strength is quantified as the image intensity in the magnitude gradient image. It is assumed that the strongest edge corresponds to the boundary of the breast. For locating the breast-air boundary this assumption is highly correct, since the maximum gradient magnitude corresponds to the step edge between the skin and the background. However, for locating the chest-wall boundary this assumption can be wrong since in clinical breast MRI the contrast between the chest muscles and the breast might be not sufficient and the strongest edge does not necessarily correspond to the chest-wall boundary. This could lead to a local minima and the model would be fitted to an inaccurate boundary in the chest wall. To overcome this limitation, a close initialization to the boundaries of interest is performed prior to the model-based segmentation. To tackle the initialization of the model in the image we proposed to use a rigid landmark registration that finds a rigid transformation (translation, rotation, scaling) needed to minimize the distance between model points and points obtained at the image boundary by simple thresholding operations and surface reconstructions.
Proc. of SPIE Vol. 7962 796215-4
Downloaded from SPIE Digital Library on 06 Apr 2011 to 142.76.1.62. Terms of Use: http://spiedl.org/terms

Starting with an optimal initialization in the image, our model-based segmentation approach continues to look for locations of maximum edge strength along a normal direction and within a 50 to 10 mm radius. The found points during search form an incomplete vector of candidate model points chestairsparse yyy += . The robustness of the statistical
shape model approach allows us to obtain a non-sparse update of the shape parameters b , using a sparse matrix of coefficients that correspond to the sparse candidate model points (equation 11).
( )Xyb Tsparse −=Φ sparse (11)
Finally, a new shape instance is computed with the found shape parameters using equation 8. This iterative process is repeated until there is no relevant change (less than 5%) on the shape parameters.
3. RESULTS 3.1 Groupwise registration and 3D shape representation
We successfully applied a population-based atlas construction to obtain the average shape of the population. The results of the registration were visually assessed using the mean and the standard deviation volumes before (Figure 2-a) and after (Figure 2-b) registration. The mean image appears to get sharper and the standard deviation volume gets narrower, indicating that the alignment of the images increases after performing groupwise registration.
Figure 2. Population-based atlas construction of the average shape. Mean volume selected sagital slices a) before groupwise registration and b) after groupwise registration.
3.2 Automatic selection of landmarks
We successfully applied a population-based atlas construction to obtain the average shape of the population. The results of the registration were visually assessed using the mean and the standard deviation volumes. Furthermore, 3D shape representation based on the marching cubes reconstruction resulted on a set of 7657 landmarks that were subsequently decimated to only 384 landmark points, using 95% decimation factor. The comparison between the groupwise and the pairwise generated deformation fields and their ability to produce suitable landmarks, (i.e. landmarks in close proximity to the target surface) yielded smaller registration errors for pairwise generated deformation fields. Over 80% of the
Proc. of SPIE Vol. 7962 796215-5
Downloaded from SPIE Digital Library on 06 Apr 2011 to 142.76.1.62. Terms of Use: http://spiedl.org/terms

generated landmarks using the pairwise generated deformation fields were located below 5 mm distance from the surface, as shown in figure 3-a) and b). Figure 3-c) shows the mean, median and standard deviation of distances to target surface when propagating landmarks using groupwise and pairwise corresponding deformation fields according to equation 1. Given this advantage of the pairwise over the groupwise deformations, we generated corresponding landmarks using the pairwise deformation fields.
Figure 3. Propagation of landmark points: a) Cumulative distribution of distances to target surface for generated landmarks. b) Frequency of distances to target surface for total generated landmarks using pairwise registration. c) Summary statistics of landmark generation errors. c) Mean, median and standard deviation of distances to target surface for generated landmarks using registration (groupwise and pairwise).
3.3 Shape variability and ability of the model the reconstruct training cases
The first 10 principal modes of variation account for over 90% of the variation explained by the model as shown in figure 4-a). The ability of the model to represent the shapes in the training population was investigated using a leave-one-out test. The average reconstruction error was computed. The error (in mm) between the predicted landmarks using optimal model parameters and the original landmarks was calculated according to equation 10. The average reconstruction error as a function of the number of principal modes is plotted in figure 4-b). Near sub-voxel resolution reconstruction (2.5mm) error is attainable when using a minimum of 15 main modes of variation.
Figure 4. Model construction results: a) Cumulative variance explained by the model as a function of modes of variation. b) Average reconstruction error for the leave-one-out validation as a function of modes of variation.
Proc. of SPIE Vol. 7962 796215-6
Downloaded from SPIE Digital Library on 06 Apr 2011 to 142.76.1.62. Terms of Use: http://spiedl.org/terms

3.4 Iterative segmentation: Matching the shape model to the anatomical boundaries of the breast.
Optimal adjustments of the model are those that relocate the model surface points to the edges of the breast. This adaptation is performed in an iterative fashion. Figure 5 illustrates cross-sections of the segmented image in two segmentation cases. In figure 5-a) the breast-air boundaries as well as the chest-wall boundary have been correctly found and therefore the segmentation of the breast is correct. In figure 5-b) the chest-wall boundary localization fails to identify the true chest-wall boundary so the iterative search falls in local minima.
Figure 5. 2D slices over the 3D segmentation result: a) Correct segmentation example. b) Segmentation fails to locate exact boundary corresponding to the breast tissue boundary in the chest wall.
4. DISCUSSION The results indicate that our approach of average shape construction using groupwise registration followed by pairwise propagation of landmarks from the average shape to each individual shape in the population is suitable for automatic identification of landmark correspondences. One of the advantages of using groupwise registration for this purpose is the reduction of the bias introduced with the selection of the reference image and therefore the landmarked average shape is not biased towards any specific shape representation in the population. Testing the ability of the model to reconstruct training cases using a leave-one-out validation demonstrated that near sub-voxel resolution reconstruction (2.5mm) error is attainable when using a minimum of 15 main modes of variation, higher accuracy in the reconstruction of 1mm is attainable when using up to 200 modes of variation. In this aspect, our work
Proc. of SPIE Vol. 7962 796215-7
Downloaded from SPIE Digital Library on 06 Apr 2011 to 142.76.1.62. Terms of Use: http://spiedl.org/terms

relates well with previous research done in this area. Frangi et al.7 reported an average placement error of 2.2 mm between landmarks manually placed and those propagated from a mean atlas. Further work is needed to improve the localization of the chest wall given that the model matching is prone to fail in local minima.
5. CONCLUSIONS Our approach is a population-based automatic construction of statistical models of shape for 3D breast that can be applied to 3D automatic breast segmentation in MRI. Our approach is not grey-level dependent so it can potentially be applied to different MRI acquisitions. Results of the generation of landmarks using groupwise and pairwise registration have been presented. A leave-one-out validation test demonstrated that on average the reconstruction error is of sub-voxel accuracy is attainable. Full validation of the segmentation performance with improved chest wall localization will be a matter of further work.
6. ACKNOWLEDGMENTS This research was supported by the Canadian Breast Cancer Research Alliance. The authors would like to thank Dr. Norman Boyd at the Campbell Family Institute for Breast Cancer Research, Ontario, Canada, for facilitating the breast MRI data for this study and also thanks to Anoma Gunasekara and Sofia Chavez for their valuable contributions.
REFERENCES
[1] Cootes, Tf., Hill, A., Taylor, Cj., Haslam, J., "Use of active shape models for locating structures in medical images." Image and Vision Computing 12, 355-365 (1994).
[2] Boyd, N., Martin, L., Chavez, S., Gunasekara, A., Salleh, A., Melnichouk, O., Yaffe, M., Friedenreich, C., Minkin S., Bronskill, M., "Breast-tissue composition and other risk factors for breast cancer in young women: a cross-sectional study," Lancet Oncology 10(6), 569-580 (2009).
[3] Balci, SK., Golland, P., Shenton, M., Wells, WM., "Free-Form B-spline Deformation Model for Groupwise Registration", Statistical Registration Workshop: MICCAI 2007, 23-30 (2007).
[4] Rueckert, D., Sonoda, L., Hayes, C., Hill, D., Leach, M., Hawkes, DJ., "Nonrigid registration using free-form deformations: application to breast MR images" IEEE Trans. Med. Imag. 18(8), 712-721 (1999).
[5] Schroeder, W. J., "Decimation of Triangle Meshes," Computer Graphics 26, 65 - 70 (1992). [6] Meagher, D. J., "Efficient synthetic image generation of arbitrary 3D objects." Pattern Recognition and Image
Processing Conference IEEE, 473-478 (1982). [7] Frangi, A. F., Rueckert, D., Schnabel, J. A., and Niessen, W. J., "Automatic construction of multiple-object three-
dimensional statistical shape models: Application to cardiac modeling," IEEE Trans. Med. Imag. 21, 1151-1166 (2002).
Proc. of SPIE Vol. 7962 796215-8
Downloaded from SPIE Digital Library on 06 Apr 2011 to 142.76.1.62. Terms of Use: http://spiedl.org/terms

Bibliography
[1] A. Jemal, M. M. Center, C. DeSantis, and E. M. Ward, “Global patterns of can-
cer incidence and mortality rates and trends.,” Cancer epidemiology, biomarkers &
prevention : a publication of the American Association for Cancer Research, cospon-
sored by the American Society of Preventive Oncology, vol. 19, pp. 1893–907, Aug.
2010.
[2] . Canadian Cancer Societys Steering Committee: Canadian Cancer Statistics 2010.
Toronto: Canadian Cancer Society, “Canadian Cancer Statistics 2010,” 2010.
[3] N. Boyd, L. Martin, S. Chavez, A. Gunasekara, A. Salleh, O. Melnichouk, M. Yaffe,
C. Friedenreich, S. Minkin, and M. Bronskill, “Breast-tissue composition and other
risk factors for breast cancer in young women: a cross-sectional study,” The Lancet
Oncology, vol. 10, no. 6, pp. 569–580, 2009.
[4] E. A. Morris, “The Normal Breast,” in Breast MRI Diagnosis and Intervention,,
vol. 1, pp. pp. 329–333., New York: Springer New York, 2005.
[5] E. R. Fisher, S. R. Land, B. Fisher, E. Mamounas, L. Gilarski, and N. Wolmark,
“Pathologic findings from the National Surgical Adjuvant Breast and Bowel Project:
twelve-year observations concerning lobular carcinoma in situ.,” Cancer, vol. 100,
no. 2, pp. 238–44, 2004.
[6] M. Al-Hajj, M. S. Wicha, A. Benito-Hernandez, S. J. Morrison, and M. F. Clarke,
“Prospective identification of tumorigenic breast cancer cells.,” Proceedings of the
57

Bibliography 58
National Academy of Sciences of the United States of America, vol. 100, pp. 3983–8,
Apr. 2003.
[7] M. Pike, M. Krailo, B. Henderson, J. Casagrande, and D. Hoel, “”Hormonal’ risk
factors, ’breast tissue age’ and the age-incidence of breast cancer,” Nature Publishing,
no. 303, pp. 767–770, 1983.
[8] N. F. Boyd, J. M. Rommens, K. Vogt, V. Lee, J. L. Hopper, M. J. Yaffe, and A. D.
Paterson, “Mammographic breast density as an intermediate phenotype for breast
cancer.,” The Lancet oncology, vol. 6, pp. 798–808, Oct. 2005.
[9] F. Bray, P. McCarron, and D. M. Parkin, “The changing global patterns of fe-
male breast cancer incidence and mortality.,” Breast cancer research : BCR, vol. 6,
pp. 229–39, Jan. 2004.
[10] C. a. Gabriel and S. M. Domchek, “Breast cancer in young women.,” Breast cancer
research : BCR, vol. 12, p. 212, Oct. 2010.
[11] S. Neuhausen, T. Gilewski, L. Norton, T. Tran, P. McGuire, J. Swensen, H. Ham-
pel, P. Borgen, K. Brown, M. Skolnick, and Others, “Recurrent BRCA2 6174delT
mutations in Ashkenazi Jewish women affected by breast cancer,” Nature genetics,
vol. 13, no. 1, pp. 126–128, 1996.
[12] K. Offit, T. Gilewski, P. McGuire, a. Schluger, H. Hampel, K. Brown, J. Swensen,
S. Neuhausen, M. Skolnick, L. Norton, and D. Goldgar, “Germline BRCA1 185delAG
mutations in Jewish women with breast cancer.,” Lancet, vol. 347, pp. 1643–5, June
1996.
[13] G. Johannesdottir, J. Gudmundsson, J. T. Bergthorsson, A. Arason, B. A. Agnars-
son, R. Bja, A. Borg, S. Ingvarsson, D. F. Easton, and V. Egilsson, “High Prevalence
of the 999del5 Mutation in Icelandic Breast and Ovarian Cancer Patients Advances
in Brief Cancer Patients1,” Cancer Research, pp. 3663–3665, 1996.

Bibliography 59
[14] J. Peto, N. Collins, R. Barfoot, S. Seal, W. Warren, N. Rahman, D. F. Easton,
C. Evans, J. Deacon, and M. R. Stratton, “Prevalence of BRCA1 and BRCA2
gene mutations in patients with early-onset breast cancer.,” Journal of the National
Cancer Institute, vol. 91, pp. 943–9, June 1999.
[15] V. A. McCormack and I. dos Santos Silva, “Breast density and parenchymal patterns
as markers of breast cancer risk: a meta-analysis.,” Cancer epidemiology, biomarkers
& prevention : a publication of the American Association for Cancer Research,
cosponsored by the American Society of Preventive Oncology, vol. 15, pp. 1159–69,
June 2006.
[16] M. H. Gail, L. a. Brinton, D. P. Byar, D. K. Corle, S. B. Green, C. Schairer, and
J. J. Mulvihill, “Projecting individualized probabilities of developing breast cancer
for white females who are being examined annually.,” Journal of the National Cancer
Institute, vol. 81, pp. 1879–86, Dec. 1989.
[17] B. Rockhill, D. Spiegelman, C. Byrne, D. J. Hunter, and G. a. Colditz, “Validation
of the Gail et al. model of breast cancer risk prediction and implications for chemo-
prevention.,” Journal of the National Cancer Institute, vol. 93, pp. 358–66, Mar.
2001.
[18] S. A. Love and K. Lindsey, Dr. Susan Love’s Breast Book (A Merloyd Lawrence
Book). No. 202, New York: Da Capo Lifelong Books, 5th ed., 2010.
[19] T. Li, L. Sun, N. Miller, T. Nicklee, J. Woo, L. Hulse-Smith, M.-S. Tsao, R. Khokha,
L. Martin, and N. Boyd, “The association of measured breast tissue characteristics
with mammographic density and other risk factors for breast cancer.,” Cancer epi-
demiology, biomarkers & prevention : a publication of the American Association
for Cancer Research, cosponsored by the American Society of Preventive Oncology,
vol. 14, pp. 343–9, Feb. 2005.

Bibliography 60
[20] J. N. Wolfe, “Risk for breast cancer development determined by mammographic
parenchymal pattern,” Cancer, vol. 37, no. 5, pp. 2486–2492, 1976.
[21] American College of Radiology, “The American College of Radiology Breast imaging
reporting and data system atlas (BIRADS).,” pp. 1–14, 2003.
[22] J. W. Byng, N. F. Boyd, E. Fishell, R. a. Jong, and M. J. Yaffe, “The quantitative
analysis of mammographic densities.,” Physics in medicine and biology, vol. 39,
pp. 1629–38, Oct. 1994.
[23] J. Chen, D. Pee, R. Ayyagari, B. Graubard, C. Schairer, C. Byrne, J. Benichou, and
M. H. Gail, “Projecting absolute invasive breast cancer risk in white women with
a model that includes mammographic density.,” Journal of the National Cancer
Institute, vol. 98, pp. 1215–26, Sept. 2006.
[24] N. F. Boyd, L. J. Martin, M. Bronskill, M. J. Yaffe, N. Duric, and S. Minkin, “Breast
tissue composition and susceptibility to breast cancer.,” Journal of the National
Cancer Institute, vol. 102, pp. 1224–37, Aug. 2010.
[25] W. K. Moon, Y.-W. Shen, C.-S. Huang, S.-C. Luo, A. Kuzucan, J.-H. Chen, and
R.-F. Chang, “Comparative study of density analysis using automated whole breast
ultrasound and MRI,” Medical Physics, vol. 38, no. 1, p. 382, 2011.
[26] K. Nie, D. Chang, J.-H. Chen, C.-C. Hsu, O. Nalcioglu, and M.-Y. Su, “Quantitative
analysis of breast parenchymal patterns using 3D fibroglandular tissues segmented
based on MRI,” Medical Physics, vol. 37, no. 1, p. 217, 2010.
[27] K. Nie, J.-H. Chen, S. Chan, M.-K. I. Chau, H. J. Yu, S. Bahri, T. Tseng, O. Nal-
cioglu, and M.-Y. Su, “Development of a quantitative method for analysis of breast
density based on three-dimensional breast MRI,” Medical Physics, vol. 35, no. 12,
p. 5253, 2008.

Bibliography 61
[28] R. Hendrick, “Tissue Relaxation,” in Breast MRI: Fundamentals and Technical As-
pects, pp. 19–29, Springer New York, 2008.
[29] N. Lee, H. Rusinek, J. Weinreb, R. Chandra, H. Toth, C. Singer, and G. Newstead,
“Fatty and fibroglandular tissue volumes in the breasts of women 20-83 years old:
comparison of X-ray mammography and computer-assisted MR imaging,” American
Journal of Roentgenology, vol. 168, no. 2, p. 501, 1997.
[30] M. Khazen, R. M. L. Warren, C. R. M. Boggis, E. C. Bryant, S. Reed, I. Warsi, L. J.
Pointon, G. E. Kwan-Lim, D. Thompson, R. Eeles, D. Easton, D. G. Evans, and
M. O. Leach, “A pilot study of compositional analysis of the breast and estimation
of breast mammographic density using three-dimensional T1-weighted magnetic res-
onance imaging.,” Cancer epidemiology, biomarkers & prevention : a publication of
the American Association for Cancer Research, cosponsored by the American Society
of Preventive Oncology, vol. 17, pp. 2268–74, Sept. 2008.
[31] W. T. Dixon, “Simple proton spectroscopic imaging.,” Radiology, vol. 153, pp. 189–
194, Oct. 1984.
[32] J. Ma, “Dixon techniques for water and fat imaging.,” Journal of magnetic resonance
imaging : JMRI, vol. 28, pp. 543–58, Sept. 2008.
[33] S. J. Graham, S. Ness, B. S. Hamilton, and M. J. Bronskill, “Magnetic resonance
properties of ex vivo breast tissue at 1.5 T.,” Magnetic resonance in medicine : offi-
cial journal of the Society of Magnetic Resonance in Medicine / Society of Magnetic
Resonance in Medicine, vol. 38, pp. 669–77, Oct. 1997.
[34] J. Byng, M. Yaffe, R. Jong, R. Shumak, G. Lockwood, D. Tritchler, and N. Boyd,
“Analysis of mammographic density and breast cancer risk from digitized mammo-
grams.,” Radiographics, vol. 18, no. 6, p. 1587, 1998.

Bibliography 62
[35] J. Wei, H.-P. Chan, M. a. Helvie, M. a. Roubidoux, B. Sahiner, L. M. Hadjiiski,
C. Zhou, S. Paquerault, T. Chenevert, and M. M. Goodsitt, “Correlation between
mammographic density and volumetric fibroglandular tissue estimated on breast MR
images,” Medical Physics, vol. 31, no. 4, p. 933, 2004.
[36] M. Kass, A. Witkin, and D. Terzopoulos, “Snakes: Active contour models,” Inter-
national Journal of Computer Vision, vol. 1, pp. 321–331, Jan. 1988.
[37] C. Xu and J. L. Prince, “Snakes, shapes, and gradient vector flow.,” IEEE trans-
actions on image processing : a publication of the IEEE Signal Processing Society,
vol. 7, pp. 359–69, Jan. 1998.
[38] G. H. Glover, “Multipoint Dixon technique for water and fat proton and suscep-
tibility imaging.,” Journal of magnetic resonance imaging : JMRI, vol. 1, no. 5,
pp. 521–30, 1991.
[39] J. Canny, “A Computational Approach to Edge Detection,” IEEE Transactions on
Pattern Analysis and Machine Intelligence, vol. PAMI-8, pp. 679–698, Nov. 1986.
[40] R. M. Haralick, “Digital Step Edges from Zero Crossing of Second Directional Deriva-
tives,” IEEE Transactions on Pattern Analysis and Machine Intelligence, vol. PAMI-
6, pp. 58–68, Jan. 1984.
[41] M. Morrone, J. Ross, D. Burr, and R. Owens, “Mach bands are phase dependent,”
Nature, vol. 324, no. 6094, pp. 250–253, 1986.
[42] M. Morrone and R. Owens, “Feature detection from local energy,” Pattern Recogni-
tion Letters, vol. 6, pp. 303–313, Dec. 1987.
[43] P. Kovesi and Others, “Edges are not just steps,” in ACCV2002: The 5th Asian
Conference on Computer Vision, vol. 8, pp. 23–25, Citeseer, 2002.

Bibliography 63
[44] P. Perona and J. Malik, “Detecting and localizing edges composed of steps, peaks
and roofs,” in Computer Vision, 1990. Proceedings, Third International Conference
on, pp. 52–57, IEEE, 2002.
[45] S. Venkatesh and R. Owens, “On the classification of image features,” Pattern Recog-
nition Letters, vol. 11, pp. 339–349, May 1990.
[46] D. J. Field, “Relations between the statistics of natural images and the response
properties of cortical cells.,” Journal of the Optical Society of America. A, Optics
and image science, vol. 4, pp. 2379–94, Dec. 1987.
[47] P. Kovesi, “Image features from phase congruency,” Videre: Journal of Computer
Vision Research, vol. 1, no. 3, pp. 1–27, 1999.
[48] M. Felsberg and G. Sommer, “The multidimensional isotropic generalization of
quadrature filters in geometric algebra,” Algebraic Frames for the Perception-Action
Cycle, vol. 357, no. 357, pp. 175–185, 2000.
[49] H. Hoppe, T. DeRose, T. Duchamp, J. McDonald, and W. Stuetzle, “Surface recon-
struction from unorganized points,” ACM SIGGRAPH Computer Graphics, vol. 26,
pp. 71–78, July 1992.
[50] M. Kazhdan, “Reconstruction of Solid Models from Oriented Point Sets,” Compu-
tational Geometry, 2005.
[51] M. Kazhdan, M. Bolitho, and H. Hoppe, “Poisson surface reconstruction,” in Euro-
graphics Symposium on Geometry Processing (2006), (New York, New York, USA),
p. 10, ACM Press, 2006.
[52] M. Kazhdan, A. Klein, K. Dalal, and H. Hoppe, “Unconstrained isosurface extrac-
tion on arbitrary octrees,” in Proceedings of the fifth Eurographics symposium on
Geometry processing, pp. 125–133, Eurographics Association, 2007.

Bibliography 64
[53] W. Lorensen and H. Cline, “Marching cubes: A high resolution 3D surface construc-
tion algorithm,” ACM Siggraph Computer Graphics, vol. 21, no. 4, pp. 163–169,
1987.
[54] J. Wilhelms and A. Van Gelder, “Octrees for faster isosurface generation,” ACM
Transactions on Graphics, vol. 11, pp. 201–227, July 1992.
[55] T. Twellmann, O. Lichte, T. W. Nattkemper, and An, “Adaptive tissue characteri-
zation network for model-free visualization of dynamic contrast-enhanced magnetic
resonance image data,” IEEE Trans. Med. Imaging, vol. 24, no. 10, p. 1256, 2005.
[56] S. K. Balci, P. Golland, M. Shenton, and W. M. Wells, “Free-Form B-spline De-
formation Model for Groupwise Registration,” Statistical Registration Workshop:
MICCAI 2007, pp. 23–30, 2007.
[57] D. Rueckert, L. Sonoda, C. Hayes, D. Hill, M. Leach, and D. J. Hawkes, “Nonrigid
registration using free-form deformations: application to breast MR images,” IEEE
Trans. Med. Imag, vol. 18, no. 8, pp. 712–721, 1999.
[58] W. J. Schroeder, J. a. Zarge, and W. E. Lorensen, “Decimation of triangle meshes,”
ACM SIGGRAPH Computer Graphics, vol. 26, pp. 65–70, July 1992.
[59] S. E. Jones, B. R. Buchbinder, and I. Aharon, “Three-Dimensional Mapping of
Cortical Thickness Using Laplace s Equation,” Human brain mapping. Vol 11,
vol. 32, pp. 12–32, 2000.
[60] A. Alyassin, J. Lancaster, J. Downs III, and P. Fox, “Evaluation of new algorithms
for the interactive measurement of surface area and volume,” Medical physics, vol. 21,
pp. 741–752, 1994.
[61] A. Klein, J. Andersson, B. a. Ardekani, J. Ashburner, B. Avants, M.-C. Chiang,
G. E. Christensen, D. L. Collins, J. Gee, P. Hellier, J. H. Song, M. Jenkinson,

Bibliography 65
C. Lepage, D. Rueckert, P. Thompson, T. Vercauteren, R. P. Woods, J. J. Mann,
and R. V. Parsey, “Evaluation of 14 nonlinear deformation algorithms applied to
human brain MRI registration.,” NeuroImage, vol. 46, pp. 786–802, July 2009.
[62] G. Ertas, H. Gulcur, O. Osman, O. Ucan, M. Tunaci, and M. Dursun, “Breast MR
segmentation and lesion detection with cellular neural networks and 3D template
matching,” Computers in biology and medicine, vol. 38, no. 1, pp. 116–126, 2008.
[63] L. Wang, K. Filippatos, O. Friman, and H. K. Hahn, “Fully automated segmenta-
tion of the pectoralis muscle boundary in breast MR images,” Proceedings of SPIE,
vol. 7963, pp. 796309–796309–8, 2011.
[64] C. Kuhl, “The Current Status of Breast MR Imaging Part I. Choice of Technique,
Image Interpretation, Diagnostic Accuracy, and Transfer to Clinical Practice,” Ra-
diology, vol. 244, no. 2, 2007.
[65] R. M. L. Warren, L. Pointon, D. Thompson, R. Hoff, F. J. Gilbert, A. Padhani,
D. Easton, S. R. Lakhani, and M. O. Leach, “Radiology Reading Protocol for Dy-
namic Contrast-enhanced MR Images of the Breast : Sensitivity and Specificity
Analysis,” Radiology, vol. 236, no. 3, pp. 779–788, 2005.
[66] M. O. Leach, “MRI for breast cancer screening,” Annals of Oncology, vol. 17,
no. Supplement 10, pp. 325–331, 2006.
[67] F. Pediconi, C. Catalano, A. Roselli, V. Dominelli, S. Cagioli, A. Karatasiou,
A. Pronio, M. Kirchin, and R. Passariello, “The Challenge of Imaging Dense Breast
Parenchyma Is Magnetic Resonance Mammography the Technique of Choice? A
Comparative Study With X-Ray Mammography and Whole-Breast Ultrasound,”
Investigative Radiology, vol. 44, no. 7, pp. 412–421, 2009.
[68] D. M. Ikeda, N. M. Hylton, K. Kinkel, M. G. Hochman, C. K. Kuhl, W. A. Kaiser,
J. C. Weinreb, S. F. Smazal, H. Degani, P. Viehweg, J. Barclay, and M. D. Schnall,

Bibliography 66
“Development , Standardization , and Testing of a Lexicon for Reporting Contrast-
Enhanced Breast Magnetic Resonance Imaging Studies,” Journal of Magnetic Res-
onance Imaging, vol. 895, pp. 889 – 895, 2001.
[69] P. Andreas, T. Baltzer, C. Freiberg, S. Beger, T. Vag, M. Dietzel, P. A. T. Baltzer,
A. B. Herzog, M. Gajda, O. Camara, and W. a. Kaiser, “Clinical MR-mammography:
are computer-assisted methods superior to visual or manual measurements for curve
type analysis? A systematic approach.,” Academic radiology, vol. 16, no. 9, pp. 1070–
6, 2009.
[70] E. Deurloo, S. S. H. Muller, J. L. J. Peterse, A. P. E. A. Besnard, and K. G. A.
Gilhuijs, “Clinically and Mammographically Occult Breast Lesions on MR Images:
Potential Effect of Computerized Assessment on Clinical Reading1,” Radiology,
pp. 693–701, 2005.
[71] K. Gilhuijs, M. Giger, and U. Bick, “Computerized analysis of breast lesions in three
dimensions using dynamic magnetic-resonance imaging,” Medical physics, pp. 1647–
1654, 1998.
[72] L. A. Meinel, A. H. Stolpen, K. S. Berbaum, L. L. Fajardo, and J. M. Reinhardt,
“Breast MRI lesion classification: improved performance of human readers with a
backpropagation neural network computer-aided diagnosis (CAD) system.,” Journal
of magnetic resonance imaging, vol. 25, no. 1, pp. 89–95, 2007.
[73] K. Lekadir, R. Merrifield, and G.-Z. Yang, “Outlier detection and handling for robust
3-D active shape models search.,” IEEE transactions on medical imaging, vol. 26,
pp. 212–22, Feb. 2007.
[74] T. Heimann and H.-P. Meinzer, “Statistical shape models for 3D medical image
segmentation: a review.,” Medical image analysis, vol. 13, no. 4, pp. 543–63, 2009.

Bibliography 67
[75] T. Heimann, S. Munzing, H.-P. Meinzer, and I. Wolf, “A shape-guided deformable
model with evolutionary algorithm initialization for 3D soft tissue segmentation.,”
Information processing in medical imaging : proceedings of the ... conference, vol. 20,
pp. 1–12, Jan. 2007.