Embed Size (px)
Citation preview

CM E Neurology ndash I
Pathological classification
Inflammation of peripheral nerves maybe due to autoimmune disease infec-tion or vasculitis The nerve fibres arenormally protected by a specialisedendothelium positive endoneurialpressure and perineurial barrier Mostcases of inflammatory neuropathy arecharacterised by endoneurial inflamma-tion and primary demyelination without
infection or vasculitis and are thoughtto have an autoimmune pathogenesisMacrophages penetrate the Schwanncell basement membrane ingest themyelin sheath and denude the axon(Fig 1(a)ndash(c)) If the inflammation issevere the axons may undergolsquobystanderrsquo degeneration In rare casesthe autoimmune response is directedagainst the axon and causes a primaryaxonal neuropathy (Fig 2) Some
organisms such as Mycobacterium lepraeand herpes zoster have a special abilityto grow within Schwann cells or sensoryneurons Vasculitis particularlyChurg-Strauss syndrome and poly-arteritis nodosa may affect peripheralnerves usually causing acute axonaldegeneration very occasiona llydemyelination and producing theclinical picture of multiple mono-neuropathy or symmetrical poly-neuropathy Rarely vasculitis is con-fined to peripheral nerves This reviewfocuses on autoimmune inflammatoryneuropathy
There is a temporal spectrum ofinflammatory demyelinating polyradicu-loneuropathies with similar pathologyfrom acute through subacute to chronic(Table 1) although there is an un-explained difference in response tosteroid treatment Guillain-Barreacutesyndrome (GBS) the commonest clinicalpresentation of an autoimmuneneuropathy is now agreed to be aheterogeneous condition incorporatingseveral pathological entities2
Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999 219
Autoimmune inflammatory
neuropathy
R D M Hadden MRCP Neurology Research Registrar
M P T Lunn MRCP Neurology Research Registrar
R A C Hughes MD FRCP Professor of Neurology
Guyrsquos Kingrsquos and St Thomasrsquo School of Medicine London
J R Coll Physicians Lond 199933219ndash24
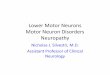
Fig 1 Electron micrograph of a sural nerve biopsy from apatient w ith Guillain- Barreacute syndrom e (acute inf lammatorydemyelinating polyradiculoneuropathy) (a) a macrophagesurrounds a normal myelinated axon (b) it penetrates anddigests the myelin and (c) strips the axon (Reproduced withpermission from Ref 1)
CM E Neurology ndash I
Guillain-Barreacute syndrome
Clinical features
The annual incidence of GBS is abouttwo per 100000 and increases withage3 Half the patients eventually makea complete recovery but many havepersistent fatigue 15 are still unableto walk unaided after a year and 8die A worse outcome is predicted byolder age preceding diarrhoea severeweakness and neurophysiologicallyinexcitable motor nerves Childrenusually recover faster and morecompletely
Two-thirds of patients have hadsymptoms of a respiratory or gastro-intestinal infection in the preceding twoweeks Campylobacter jejuni (Fig 3)cytomegalovirus Epstein-Barr virus andMycoplasma pneumoniae have all beenincriminated in case-control studies andmay be asymptomatic A popular butunproven hypothesis is that molecularmimicry between the infectingorganism and peripheral nerve antigenstriggers an autoimmune response2Treatment of the infection does notinfluence outcome
The major symptoms are weaknessandor sensory disturbance of upperandor lower limbs usually symmetri-cal often proximal and distal but notnecessarily lsquoascendingrsquo and progressing
for up to four weeks There may besevere neuropathic or radicular painReflexes are usually absent in affectedlimbs There is often involvement ofautonomic cranial and respiratorymuscle nerves
The diagnosis is made from thecharacteristic history with flaccid weak-ness raised cerebrospinal fluid (CSF)protein with normal white cell countand exclusion of other (eg toxic) causes(Table 2) Nerve conduction studies maysupport the diagnosis by showingfeatures of demyelination Difficulties indiagnosis may be caused by the fact
that reflexes CSF protein and neuro-physiology may all be normal particu-larly in the first few days of the diseaseMost cases of GBS have acute inflam-matory demyelinating polyradiculo-neuropathy but a small proportion hasacute motor (or motor and sensory)axonal neuropathy4 In either typeelectromyography four weeks later mayidentify axonal degeneration indicatinga poor outcome GBS is the mostcommon cause of acute neuromuscularparalysis but alternative diagnosesshould always be considered5 Anti-bodies to ganglioside GM1 are present
220 Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999
Fig 3 About 25 of cases of Guillain- Barreacute syndrom e followenteritis due to Campylobacter jejuni a flagellated Gram-negative bacterium Antibodies to the lipopolysaccharide in itscoat may cross-react with myelin antigens
Acute (lt 4 weeks progressive phase)ndash Guillain-Barreacute syndrome (GBS)
acute inflammatory demyelinating polyradiculoneuropathyacute motor axonal neuropathyacute motor and sensory axonal neuropathy
ndash Fisher syndromendash FisherGBS overlap syndromendash acute sensory neuronopathy
Subacute (4ndash8 weeks progressive phase)ndash subacute inflammatory demyelinating polyradiculoneuropathy
Chronic (gt 8 weeks progressive phase)ndash chronic inflammatory demyelinating polyradiculoneuropathy ndash multifocal motor neuropathy with conduction blockndash paraproteinaemic demyelinating neuropathy ndash chronic relapsing axonal neuropathy
Table 1 Classif ication of autoimmune inf lammatory neuropathy
Fig 2 Electron micrograph of a sural nerve biopsy from apatient w ith Guilla in-Barreacute syndrom e (acute motor andsensory axonal neuropathy) The axon degenerates while themyelin remains intact
CM E Neurology ndash I
in about a quarter of patients with GBSwhich is not sufficiently common tohelp with diagnosis (Fig 4) Antibodies toganglioside GQ1b are a sensitive andspecific diagnostic test for the un-common Fisher syndrome consisting ofophthalmoplegia ataxia and tendonareflexia without limb weakness whichoverlaps with and may develop intofull-blown GBS
Treatment
General management of GBS requiresalertness to the possibilities of cardiacarrhythmia (Fig 5) respiratory failure orthromboembolism as well as to theintensive care required by anyparalysed patient5 As with any complexrare condition there is a trend forpatients transferred to a specialistneurological centre to have a better out-come3 Resistant pain may requirenon-steroidal anti-inflammatory drugsamitriptyline carbamazepine or evenopiates
Several large randomised controlledtrials have shown that plasma exchangeimproves the rate and extent ofrecovery in GBS6 However intravenousimmunoglobulin (Ig) (04 gkgday forfive days) is currently preferred it is
equally beneficial safer and more con-venient7 Treatment should be started assoon as possible There is no evidenceto indicate whether treatment startedafter the first two weeks is helpful Our
practice is to treat patients who are stillworsening at that time but not thosewho are improving We also re-treat the10 of patients who suffer an earlyrelapse and are setting up arandomised controlled trial of a secondcourse of Ig for patients still bed-boundtwo weeks after the first course The lesscommon varieties of acute neuropathyare empirically treated in a similar wayAdverse effects of Ig include headachefever nausea eczema aseptic menin-gitis thrombosis and renal failure witha theoretical risk of blood-borne infec-tion Anaphylaxis is a rare but realhazard especially in patients with IgAdeficiency Corticosteroids are no betterthan placebo ndash a surprising observationpossibly explained by an adverse effecton denervated muscle8
Chronic inflammatoryneuropathies
Clinical features
Chronic inflammatory neuropathies aredistinguished from other chronic neuro-pathies by reduced or absent reflexes
Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999 221
Inflammatoryndash Guillain-Barreacute syndromendash vasculitis Churg-Strauss syndrome polyarteritis nodosa systemic lupus
erythematosus ndash infections diphtheria HIV Lyme borreliosis poliomyelitisndash sarcoidosis
Toxinsndash alcoholndash drugs gold isoniazid nitrofurantoin taxol vincristine ndash heavy metals (arsenic lead thallium) hexacarbons organophosphates
Metabolicndash diabetes mellitus porphyria tyrosinaemia
Critical illness polyneuropathy
Nutritional deficienciesndash thiamine
Lymphoma
Table 2 Causes of acute peripheral neuropathy
F ig 4 Schematic representat ion of gangliosides GM 1 and GQ1b Thesemembrane-bound glycolipids are widely distributed throughout the body Autoantibodiesto these and other gangliosides are found in many inflammatory neuropathies and canassist in diagnosis
Glucose
GM1
Ceramide Ceramide
GQ1b
Galactose
N-acetyl galactosamine
Sialic Acid (N-acetyl neuraminic acid)
CM E Neurology ndash I
raised CSF protein usually demyelinatingneurophysiology and the lack of a familyhistory (Table 3) Despite being treatablethey are underdiagnosed
Chronic inflammatory demyelinatingpolyradiculoneuropathy (CIDP) is hetero-geneous with a relapsing-remittingmonophasic or progressive course anda prevalence of at least oneper 100000 Symptoms commonlyinclude weakness andor numbnesspain and ataxia It is rarely severeenough to require ventilatory supportbut half of all patients suffer temporarysevere disability and 13 becomepermanently dependent9
Paraproteinaemic neuropathiesaccount for 10 of demyelinatingneuropathies and are more common inthe elderly10 The paraprotein is usuallya monoclonal gammopathy of un-determined significance of anyimmunoglobulin (Ig) subclass and theassociated clinical picture is heteroge-neous One relatively homogeneoussubgroup consists of the syndrome ofIgM (usually k) paraprotein antibodiesto myelin-associated glycoprotein avery slowly progressive predominantlysensory demyelinating neuropathy anda postural tremor Patients with IgGparaproteins commonly resemblepatients with CIDP though a few haveaxonal neurophysio logy Patients withIgG and IgA paraproteins may have aplasmacytoma or solitary myeloma thisshould always be considered especiallyin treatment resistant cases
Multifocal motor neuropathy withconduction block is an uncommondemyelinating motor neuropathypresenting with progressive patchyasymmetrical weakness beginning inthe upper limbs often with cramps andsometimes minor sensory symptoms11Clinical misdiagnosis as motor neurondisease is possib le because of thepredominant motor phenotype andoccurrence of fasciculations Antibodiesto ganglioside GM1 are present in mostcases but are neither sensitive norspecific
Neurophysiological examination isessentia l for the identification of ademyelinating neuropathy (Fig 6)
222 Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999
Inflammatoryndash autoimmune (D A) (see Table 1) ndash vasculitisconnective tissue disease (A)
Churg-Strauss syndrome polyarteritis nodosa rheumatoid arthritisWegenerrsquos granulomatosis
ndash infection (A D) leprosy herpes zoster HIV
Inheritedndash Charcot-Marie-Tooth disease (hereditary motor sensory neuropathy) (D A)ndash hereditary amyloid neuropathy (A)ndash metachromatic leucodystrophy (D)
Toxinsndash alcohol (A)ndash drugs amiodarone (D) dapsone disulfiram isoniazid metronidazole
nitrofurantoin phenytoin platinum vincristine (A)ndash chemicals (A) acrylamide carbon disulphide heavy metals
Metabolic (A)ndash diabetes mellitus acromegaly myxoedema uraemia
Nutritional deficiencies (A)ndash vitamin B12 pyridoxine thiamine niacin folic acid
Paraproteinaemic (D A)
Paraneoplastic (A D)ndash carcinoma polycythaemia rubra vera
Miscellaneous (A)ndash primary amyloidosis coeliac disease primary biliary cirrhosis
A axonal D demyelinating
Table 3 Causes of chronic peripheral neuropathy
Fig 5 Spontaneous transien t asystole in Guillain- Barreacute syndrom e Autonomicneuropathy may cause tachy- or bradyarrhythmias and a pacemaker may be required
CM E Neurology ndash I
In CIDP there is slowed nerve con-duction especially in motor nerves andthere may be multifocal conductionblock In chronic and severe cases thesuperimposition of axonal degenerationmay make the distinction from axonalneuropathy difficult In IgM para-proteinaemic demyelinating neuro-pathy with anti-myelin-associated glyco-protein antibodies the slowing of nerveconduction is more distal than proximaland there is no conduction block Inmultifocal motor neuropathy with con-duction block there are multiple persis-tent sites of motor conduction block butsensory conduction remains normal inthe same nerve segments In contrastinherited demyelinating neuropathieshave uniform slowing without conduc-tion block
Sural nerve biopsy is indicated only if thediagnosis remains uncertain It oftenshows only non-specific changes andmay cause unpleasant dysaesthesiaeIts greatest use is in the identification ofvasculitis
Treatment
Chronic inflammatory demyelinatingpolyradiculoneuropathy Immuno-modulatory therapy is usually meritedin CIDP except in very mild cases Oralprednisolone (120 mg on alternatedays reducing over 3 months)12 intra-venous Ig (04 mgkgday for 5 days)13
and plasma exchange (10 exchangesover 4 weeks)14 have all been shown tobe efficacious in short-term randomisedcontrolled trials (Ig and plasmaexchange have equiva lent efficacy)Sensory symptoms generally improveless than motor Azathioprine cyclo-phosphamide cyclosporin A and inter-feron a-2a have been reported to beeffective in some patients but have notbeen tested in randomised controlledtrials Our current recommendation forinitial therapy in CIDP is either Ig orpredniso lone (with conside ration ofosteoporosis prophylaxis) A trialcomparing these two is ongoingCombination therapy is often necessaryas the disease progresses If treatmentfails the diagnosis should be re-evaluated and a paraprotein re-sought
Paraproteinaemic demyelinating neuro-pathy has a slightly different treatmentresponse profile10 in that Ig benefitssome patients15 but steroids are gener-ally ineffective Plasma exchange some-times gives at least short-term benefitespecially in patients with an IgA or IgGparaprotein16 A bone marrow examina-tion or radiolog ical skeletal surveysometimes uncovers a primary plasma-cytoma or solitary myeloma treatmentof which may improve the neuropathy(Fig 7) Cyclophosphamide melphalanazathioprine chlorambucil fludarabineand interferon-a have been used butsound evidence is lacking17
Multifocal motor neuropathy with conduc-tion block Two-thirds of these casesrespond to intravenous Ig but treat-ment usually needs to be repeatedmonthly (which is expensive) Steroidshave no effect and may even worsenthe disease Oral or intravenouscyclophosphamide is often used to tryto sustain the response but evidence ofefficacy is lacking
Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999 223
Fig 7 Axial computed tomography of the pelvis of a 45-year old man referred w ithlsquot reatment resistant chronic inf lammatory demyelinating polyradiculo-neuropathyrsquo Serum protein electrophoresis revealed an immunoglobulin G paraproteinThe destructive lesion in the right sacrum was a solitary myeloma His neuropathyimproved after radiotherapy Serum electrophoresis should be done in the investigationof any chronic neuropathy
40
3
0
0
Time (ms)
1
4
21
3
21
10 20 30
Amplitude (mV)
Demyelinating
Axonal
Normal
2
0
6
0
5
Fig 6 Action potentials recorded fromthe thenar muscle after stimulation ofthe median nerve at the w r ist Neurophysiological examination is impor-tant in the diagnosis of a neuropathy Inaxonal neuropathy the major abnormalityis a reduced amplitude whereas indemyelinating neuropathy the response isdisproportionately delayed and dispersed
CM E Neurology ndash I
In all these chronic neuropathies asignificant but unknown proportion ofpatients eventually becomes lessresponsive to treatment as secondaryaxonal degeneration gradually accumu-lates A multidisciplina ry approach tofoot care orthoses physiotherapy andenvironmental aids then becomesparticularly important An excellentpatient support group is available18
Acknowledgments
We are grateful for financial supportfrom the BIOMED InflammatoryNeuropathy Cause and TreatmentProgramme (reference BMH4-CT96-0324) and from the Patrick BerthoudCharitable Trust for MPTL
References
1 Hughes RAC Guillain-Barreacute syndromeLondon SpringerndashVerlag 1990
2 Hahn AF Guilla in-Barreacute syndrome(review) Lancet 1998352635ndash41
3 Rees JH Thompson RD Smeeton NCHughes RAC Epidemiological study ofGuillain-Barreacute syndrome in south eastEngland J Neurol Neurosurg Psychiatry19986474ndash7
4 Hadden RDM Cornblath DR HughesRAC Zielasek J et al Electrophysiologicalclassification of Guillain-Barreacute syndromeclinical associations and outcome AnnNeurol 199844780ndash8
5 Hughes RAC Management of acuteneuromuscular paralysis J R CollPhysicians Lond 199832254ndash9
6 The Guillain-Barreacute Syndrome StudyGroup Plasmapheresis and acuteGuilla in-Barreacute syndrome Neurology1985351096ndash104
7 Plasma Exchange SandoglobulinGuillain-Barreacute Syndrome Trial GroupRandomised trial of plasma exchangeintravenous immunoglobulin andcombined treatments in Guillain-Barreacutesyndrome Lancet 1997349225ndash30
8 Hughes RAC Van der Mecheacute FGACorticosteroid treatment forGuilla in-Barreacute syndrome (CochraneReview) In The Cochrane Library Issue2 1999 Oxford Update Software
9 Lunn MPT Manti H Choudhary PPHughes RAC Thomas PK Chronic inflam-matory demyelinating polyradiculo-
neuropathy a prevalence study in southeast England J Neurol NeurosurgPsychiatry 199966677ndash80
10 Ropper AH Gorson KC Neuropathiesassociated with paraproteinemia(review) N Engl J Med 19983381601ndash7
11 Biessels GJ Franssen H Van den Berg LHGibson A et al Multifocal motorneuropathy (review) J Neurol 1997244143ndash52
12 Dyck PJ OrsquoBrien PC Oviatt KF DinapoliRP et al Prednisone improves chronicinflammatory demyelinating polyradicu-loneuropathy more than no treatmentAnn Neurol 198211136ndash41
13 Hahn AF Bolton CF Pillay N Chalk Cetal Plasma-exchange therapy in chronicinflammatory demyelinating poly-neuropathy ndash a double-blind sham-controlled cross-over study Brain 19961191055ndash66
14 Hahn AF Bolton CF Zochodne D FeasbyTE Intravenous immunoglobulin treat-ment in chronic inflammatory demyeli-nating polyneuropathy ndash a double-blind
placebo-controlled cross-over studyBrain 19961191067ndash77
15 Dalakas MC Quarles RH Farrer RGDambrosia J et al A controlled study ofintravenous immunoglobulin indemyelinating neuropathy with IgMgammopathy Ann Neurol 199640792ndash5
16 Dyck PJ Low PA Windebank AJ JaradehSS et al Plasma exchange in poly-neuropathy associated with monoclonalgammopathy of undetermined signifi-cance N Engl J Med 19913251482ndash6
17 Mariette X Chastang C Clavelou PLouboutin JP et al A randomised clinicaltrial comparing interferon-a and intra-venous immunoglobulin in poly-neuropathy associated with monoclonalIgM J Neurol Neurosurg Psychiatry19976328ndash34
18 The Guillain-Barreacute Syndrome SupportGroup of the UK Lincolnshire CountyCouncil Offices Eastgate SleafordLincolnshire NG34 7EB Tel fax01529 304 615 wwwgbsorguk
224 Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999
Autoimmune inflammatory neuropathy is a spectrum of disorders
copy acute and chronic
copy focal and generalised
copy demyelinating and axonal
Guillain-Barreacute syndrome
copy reflexes cerebrospinal fluid and neurophysiology may be normal in the early
stages
copy adverse prognostic factors older age preceding diarrhoea severe weakness
inexcitable nerves
copy treat w ith intravenous immunoglobulin
Chronic demyelinating neuropathy
copy check for a paraprotein
copy IgM k paraprotein with antibodies to myelin-associated glycoprotein is
associated with a benign predominantly sensory neuropathy
copy treat chronic inflammatory demyelinating polyradiculoneuropathy initially
w ith prednisolone or intravenous immunoglobulin
copy treat multifocal motor neuropathy with conduction block with intravenous
immunoglobulin
Key Points

CM E Neurology ndash I
Guillain-Barreacute syndrome
Clinical features
The annual incidence of GBS is abouttwo per 100000 and increases withage3 Half the patients eventually makea complete recovery but many havepersistent fatigue 15 are still unableto walk unaided after a year and 8die A worse outcome is predicted byolder age preceding diarrhoea severeweakness and neurophysiologicallyinexcitable motor nerves Childrenusually recover faster and morecompletely
Two-thirds of patients have hadsymptoms of a respiratory or gastro-intestinal infection in the preceding twoweeks Campylobacter jejuni (Fig 3)cytomegalovirus Epstein-Barr virus andMycoplasma pneumoniae have all beenincriminated in case-control studies andmay be asymptomatic A popular butunproven hypothesis is that molecularmimicry between the infectingorganism and peripheral nerve antigenstriggers an autoimmune response2Treatment of the infection does notinfluence outcome
The major symptoms are weaknessandor sensory disturbance of upperandor lower limbs usually symmetri-cal often proximal and distal but notnecessarily lsquoascendingrsquo and progressing
for up to four weeks There may besevere neuropathic or radicular painReflexes are usually absent in affectedlimbs There is often involvement ofautonomic cranial and respiratorymuscle nerves
The diagnosis is made from thecharacteristic history with flaccid weak-ness raised cerebrospinal fluid (CSF)protein with normal white cell countand exclusion of other (eg toxic) causes(Table 2) Nerve conduction studies maysupport the diagnosis by showingfeatures of demyelination Difficulties indiagnosis may be caused by the fact
that reflexes CSF protein and neuro-physiology may all be normal particu-larly in the first few days of the diseaseMost cases of GBS have acute inflam-matory demyelinating polyradiculo-neuropathy but a small proportion hasacute motor (or motor and sensory)axonal neuropathy4 In either typeelectromyography four weeks later mayidentify axonal degeneration indicatinga poor outcome GBS is the mostcommon cause of acute neuromuscularparalysis but alternative diagnosesshould always be considered5 Anti-bodies to ganglioside GM1 are present
220 Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999
Fig 3 About 25 of cases of Guillain- Barreacute syndrom e followenteritis due to Campylobacter jejuni a flagellated Gram-negative bacterium Antibodies to the lipopolysaccharide in itscoat may cross-react with myelin antigens
Acute (lt 4 weeks progressive phase)ndash Guillain-Barreacute syndrome (GBS)
acute inflammatory demyelinating polyradiculoneuropathyacute motor axonal neuropathyacute motor and sensory axonal neuropathy
ndash Fisher syndromendash FisherGBS overlap syndromendash acute sensory neuronopathy
Subacute (4ndash8 weeks progressive phase)ndash subacute inflammatory demyelinating polyradiculoneuropathy
Chronic (gt 8 weeks progressive phase)ndash chronic inflammatory demyelinating polyradiculoneuropathy ndash multifocal motor neuropathy with conduction blockndash paraproteinaemic demyelinating neuropathy ndash chronic relapsing axonal neuropathy
Table 1 Classif ication of autoimmune inf lammatory neuropathy
Fig 2 Electron micrograph of a sural nerve biopsy from apatient w ith Guilla in-Barreacute syndrom e (acute motor andsensory axonal neuropathy) The axon degenerates while themyelin remains intact
CM E Neurology ndash I
in about a quarter of patients with GBSwhich is not sufficiently common tohelp with diagnosis (Fig 4) Antibodies toganglioside GQ1b are a sensitive andspecific diagnostic test for the un-common Fisher syndrome consisting ofophthalmoplegia ataxia and tendonareflexia without limb weakness whichoverlaps with and may develop intofull-blown GBS
Treatment
General management of GBS requiresalertness to the possibilities of cardiacarrhythmia (Fig 5) respiratory failure orthromboembolism as well as to theintensive care required by anyparalysed patient5 As with any complexrare condition there is a trend forpatients transferred to a specialistneurological centre to have a better out-come3 Resistant pain may requirenon-steroidal anti-inflammatory drugsamitriptyline carbamazepine or evenopiates
Several large randomised controlledtrials have shown that plasma exchangeimproves the rate and extent ofrecovery in GBS6 However intravenousimmunoglobulin (Ig) (04 gkgday forfive days) is currently preferred it is
equally beneficial safer and more con-venient7 Treatment should be started assoon as possible There is no evidenceto indicate whether treatment startedafter the first two weeks is helpful Our
practice is to treat patients who are stillworsening at that time but not thosewho are improving We also re-treat the10 of patients who suffer an earlyrelapse and are setting up arandomised controlled trial of a secondcourse of Ig for patients still bed-boundtwo weeks after the first course The lesscommon varieties of acute neuropathyare empirically treated in a similar wayAdverse effects of Ig include headachefever nausea eczema aseptic menin-gitis thrombosis and renal failure witha theoretical risk of blood-borne infec-tion Anaphylaxis is a rare but realhazard especially in patients with IgAdeficiency Corticosteroids are no betterthan placebo ndash a surprising observationpossibly explained by an adverse effecton denervated muscle8
Chronic inflammatoryneuropathies
Clinical features
Chronic inflammatory neuropathies aredistinguished from other chronic neuro-pathies by reduced or absent reflexes
Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999 221
Inflammatoryndash Guillain-Barreacute syndromendash vasculitis Churg-Strauss syndrome polyarteritis nodosa systemic lupus
erythematosus ndash infections diphtheria HIV Lyme borreliosis poliomyelitisndash sarcoidosis
Toxinsndash alcoholndash drugs gold isoniazid nitrofurantoin taxol vincristine ndash heavy metals (arsenic lead thallium) hexacarbons organophosphates
Metabolicndash diabetes mellitus porphyria tyrosinaemia
Critical illness polyneuropathy
Nutritional deficienciesndash thiamine
Lymphoma
Table 2 Causes of acute peripheral neuropathy
F ig 4 Schematic representat ion of gangliosides GM 1 and GQ1b Thesemembrane-bound glycolipids are widely distributed throughout the body Autoantibodiesto these and other gangliosides are found in many inflammatory neuropathies and canassist in diagnosis
Glucose
GM1
Ceramide Ceramide
GQ1b
Galactose
N-acetyl galactosamine
Sialic Acid (N-acetyl neuraminic acid)
CM E Neurology ndash I
raised CSF protein usually demyelinatingneurophysiology and the lack of a familyhistory (Table 3) Despite being treatablethey are underdiagnosed
Chronic inflammatory demyelinatingpolyradiculoneuropathy (CIDP) is hetero-geneous with a relapsing-remittingmonophasic or progressive course anda prevalence of at least oneper 100000 Symptoms commonlyinclude weakness andor numbnesspain and ataxia It is rarely severeenough to require ventilatory supportbut half of all patients suffer temporarysevere disability and 13 becomepermanently dependent9
Paraproteinaemic neuropathiesaccount for 10 of demyelinatingneuropathies and are more common inthe elderly10 The paraprotein is usuallya monoclonal gammopathy of un-determined significance of anyimmunoglobulin (Ig) subclass and theassociated clinical picture is heteroge-neous One relatively homogeneoussubgroup consists of the syndrome ofIgM (usually k) paraprotein antibodiesto myelin-associated glycoprotein avery slowly progressive predominantlysensory demyelinating neuropathy anda postural tremor Patients with IgGparaproteins commonly resemblepatients with CIDP though a few haveaxonal neurophysio logy Patients withIgG and IgA paraproteins may have aplasmacytoma or solitary myeloma thisshould always be considered especiallyin treatment resistant cases
Multifocal motor neuropathy withconduction block is an uncommondemyelinating motor neuropathypresenting with progressive patchyasymmetrical weakness beginning inthe upper limbs often with cramps andsometimes minor sensory symptoms11Clinical misdiagnosis as motor neurondisease is possib le because of thepredominant motor phenotype andoccurrence of fasciculations Antibodiesto ganglioside GM1 are present in mostcases but are neither sensitive norspecific
Neurophysiological examination isessentia l for the identification of ademyelinating neuropathy (Fig 6)
222 Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999
Inflammatoryndash autoimmune (D A) (see Table 1) ndash vasculitisconnective tissue disease (A)
Churg-Strauss syndrome polyarteritis nodosa rheumatoid arthritisWegenerrsquos granulomatosis
ndash infection (A D) leprosy herpes zoster HIV
Inheritedndash Charcot-Marie-Tooth disease (hereditary motor sensory neuropathy) (D A)ndash hereditary amyloid neuropathy (A)ndash metachromatic leucodystrophy (D)
Toxinsndash alcohol (A)ndash drugs amiodarone (D) dapsone disulfiram isoniazid metronidazole
nitrofurantoin phenytoin platinum vincristine (A)ndash chemicals (A) acrylamide carbon disulphide heavy metals
Metabolic (A)ndash diabetes mellitus acromegaly myxoedema uraemia
Nutritional deficiencies (A)ndash vitamin B12 pyridoxine thiamine niacin folic acid
Paraproteinaemic (D A)
Paraneoplastic (A D)ndash carcinoma polycythaemia rubra vera
Miscellaneous (A)ndash primary amyloidosis coeliac disease primary biliary cirrhosis
A axonal D demyelinating
Table 3 Causes of chronic peripheral neuropathy
Fig 5 Spontaneous transien t asystole in Guillain- Barreacute syndrom e Autonomicneuropathy may cause tachy- or bradyarrhythmias and a pacemaker may be required
CM E Neurology ndash I
In CIDP there is slowed nerve con-duction especially in motor nerves andthere may be multifocal conductionblock In chronic and severe cases thesuperimposition of axonal degenerationmay make the distinction from axonalneuropathy difficult In IgM para-proteinaemic demyelinating neuro-pathy with anti-myelin-associated glyco-protein antibodies the slowing of nerveconduction is more distal than proximaland there is no conduction block Inmultifocal motor neuropathy with con-duction block there are multiple persis-tent sites of motor conduction block butsensory conduction remains normal inthe same nerve segments In contrastinherited demyelinating neuropathieshave uniform slowing without conduc-tion block
Sural nerve biopsy is indicated only if thediagnosis remains uncertain It oftenshows only non-specific changes andmay cause unpleasant dysaesthesiaeIts greatest use is in the identification ofvasculitis
Treatment
Chronic inflammatory demyelinatingpolyradiculoneuropathy Immuno-modulatory therapy is usually meritedin CIDP except in very mild cases Oralprednisolone (120 mg on alternatedays reducing over 3 months)12 intra-venous Ig (04 mgkgday for 5 days)13
and plasma exchange (10 exchangesover 4 weeks)14 have all been shown tobe efficacious in short-term randomisedcontrolled trials (Ig and plasmaexchange have equiva lent efficacy)Sensory symptoms generally improveless than motor Azathioprine cyclo-phosphamide cyclosporin A and inter-feron a-2a have been reported to beeffective in some patients but have notbeen tested in randomised controlledtrials Our current recommendation forinitial therapy in CIDP is either Ig orpredniso lone (with conside ration ofosteoporosis prophylaxis) A trialcomparing these two is ongoingCombination therapy is often necessaryas the disease progresses If treatmentfails the diagnosis should be re-evaluated and a paraprotein re-sought
Paraproteinaemic demyelinating neuro-pathy has a slightly different treatmentresponse profile10 in that Ig benefitssome patients15 but steroids are gener-ally ineffective Plasma exchange some-times gives at least short-term benefitespecially in patients with an IgA or IgGparaprotein16 A bone marrow examina-tion or radiolog ical skeletal surveysometimes uncovers a primary plasma-cytoma or solitary myeloma treatmentof which may improve the neuropathy(Fig 7) Cyclophosphamide melphalanazathioprine chlorambucil fludarabineand interferon-a have been used butsound evidence is lacking17
Multifocal motor neuropathy with conduc-tion block Two-thirds of these casesrespond to intravenous Ig but treat-ment usually needs to be repeatedmonthly (which is expensive) Steroidshave no effect and may even worsenthe disease Oral or intravenouscyclophosphamide is often used to tryto sustain the response but evidence ofefficacy is lacking
Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999 223
Fig 7 Axial computed tomography of the pelvis of a 45-year old man referred w ithlsquot reatment resistant chronic inf lammatory demyelinating polyradiculo-neuropathyrsquo Serum protein electrophoresis revealed an immunoglobulin G paraproteinThe destructive lesion in the right sacrum was a solitary myeloma His neuropathyimproved after radiotherapy Serum electrophoresis should be done in the investigationof any chronic neuropathy
40
3
0
0
Time (ms)
1
4
21
3
21
10 20 30
Amplitude (mV)
Demyelinating
Axonal
Normal
2
0
6
0
5
Fig 6 Action potentials recorded fromthe thenar muscle after stimulation ofthe median nerve at the w r ist Neurophysiological examination is impor-tant in the diagnosis of a neuropathy Inaxonal neuropathy the major abnormalityis a reduced amplitude whereas indemyelinating neuropathy the response isdisproportionately delayed and dispersed
CM E Neurology ndash I
In all these chronic neuropathies asignificant but unknown proportion ofpatients eventually becomes lessresponsive to treatment as secondaryaxonal degeneration gradually accumu-lates A multidisciplina ry approach tofoot care orthoses physiotherapy andenvironmental aids then becomesparticularly important An excellentpatient support group is available18
Acknowledgments
We are grateful for financial supportfrom the BIOMED InflammatoryNeuropathy Cause and TreatmentProgramme (reference BMH4-CT96-0324) and from the Patrick BerthoudCharitable Trust for MPTL
References
1 Hughes RAC Guillain-Barreacute syndromeLondon SpringerndashVerlag 1990
2 Hahn AF Guilla in-Barreacute syndrome(review) Lancet 1998352635ndash41
3 Rees JH Thompson RD Smeeton NCHughes RAC Epidemiological study ofGuillain-Barreacute syndrome in south eastEngland J Neurol Neurosurg Psychiatry19986474ndash7
4 Hadden RDM Cornblath DR HughesRAC Zielasek J et al Electrophysiologicalclassification of Guillain-Barreacute syndromeclinical associations and outcome AnnNeurol 199844780ndash8
5 Hughes RAC Management of acuteneuromuscular paralysis J R CollPhysicians Lond 199832254ndash9
6 The Guillain-Barreacute Syndrome StudyGroup Plasmapheresis and acuteGuilla in-Barreacute syndrome Neurology1985351096ndash104
7 Plasma Exchange SandoglobulinGuillain-Barreacute Syndrome Trial GroupRandomised trial of plasma exchangeintravenous immunoglobulin andcombined treatments in Guillain-Barreacutesyndrome Lancet 1997349225ndash30
8 Hughes RAC Van der Mecheacute FGACorticosteroid treatment forGuilla in-Barreacute syndrome (CochraneReview) In The Cochrane Library Issue2 1999 Oxford Update Software
9 Lunn MPT Manti H Choudhary PPHughes RAC Thomas PK Chronic inflam-matory demyelinating polyradiculo-
neuropathy a prevalence study in southeast England J Neurol NeurosurgPsychiatry 199966677ndash80
10 Ropper AH Gorson KC Neuropathiesassociated with paraproteinemia(review) N Engl J Med 19983381601ndash7
11 Biessels GJ Franssen H Van den Berg LHGibson A et al Multifocal motorneuropathy (review) J Neurol 1997244143ndash52
12 Dyck PJ OrsquoBrien PC Oviatt KF DinapoliRP et al Prednisone improves chronicinflammatory demyelinating polyradicu-loneuropathy more than no treatmentAnn Neurol 198211136ndash41
13 Hahn AF Bolton CF Pillay N Chalk Cetal Plasma-exchange therapy in chronicinflammatory demyelinating poly-neuropathy ndash a double-blind sham-controlled cross-over study Brain 19961191055ndash66
14 Hahn AF Bolton CF Zochodne D FeasbyTE Intravenous immunoglobulin treat-ment in chronic inflammatory demyeli-nating polyneuropathy ndash a double-blind
placebo-controlled cross-over studyBrain 19961191067ndash77
15 Dalakas MC Quarles RH Farrer RGDambrosia J et al A controlled study ofintravenous immunoglobulin indemyelinating neuropathy with IgMgammopathy Ann Neurol 199640792ndash5
16 Dyck PJ Low PA Windebank AJ JaradehSS et al Plasma exchange in poly-neuropathy associated with monoclonalgammopathy of undetermined signifi-cance N Engl J Med 19913251482ndash6
17 Mariette X Chastang C Clavelou PLouboutin JP et al A randomised clinicaltrial comparing interferon-a and intra-venous immunoglobulin in poly-neuropathy associated with monoclonalIgM J Neurol Neurosurg Psychiatry19976328ndash34
18 The Guillain-Barreacute Syndrome SupportGroup of the UK Lincolnshire CountyCouncil Offices Eastgate SleafordLincolnshire NG34 7EB Tel fax01529 304 615 wwwgbsorguk
224 Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999
Autoimmune inflammatory neuropathy is a spectrum of disorders
copy acute and chronic
copy focal and generalised
copy demyelinating and axonal
Guillain-Barreacute syndrome
copy reflexes cerebrospinal fluid and neurophysiology may be normal in the early
stages
copy adverse prognostic factors older age preceding diarrhoea severe weakness
inexcitable nerves
copy treat w ith intravenous immunoglobulin
Chronic demyelinating neuropathy
copy check for a paraprotein
copy IgM k paraprotein with antibodies to myelin-associated glycoprotein is
associated with a benign predominantly sensory neuropathy
copy treat chronic inflammatory demyelinating polyradiculoneuropathy initially
w ith prednisolone or intravenous immunoglobulin
copy treat multifocal motor neuropathy with conduction block with intravenous
immunoglobulin
Key Points

CM E Neurology ndash I
in about a quarter of patients with GBSwhich is not sufficiently common tohelp with diagnosis (Fig 4) Antibodies toganglioside GQ1b are a sensitive andspecific diagnostic test for the un-common Fisher syndrome consisting ofophthalmoplegia ataxia and tendonareflexia without limb weakness whichoverlaps with and may develop intofull-blown GBS
Treatment
General management of GBS requiresalertness to the possibilities of cardiacarrhythmia (Fig 5) respiratory failure orthromboembolism as well as to theintensive care required by anyparalysed patient5 As with any complexrare condition there is a trend forpatients transferred to a specialistneurological centre to have a better out-come3 Resistant pain may requirenon-steroidal anti-inflammatory drugsamitriptyline carbamazepine or evenopiates
Several large randomised controlledtrials have shown that plasma exchangeimproves the rate and extent ofrecovery in GBS6 However intravenousimmunoglobulin (Ig) (04 gkgday forfive days) is currently preferred it is
equally beneficial safer and more con-venient7 Treatment should be started assoon as possible There is no evidenceto indicate whether treatment startedafter the first two weeks is helpful Our
practice is to treat patients who are stillworsening at that time but not thosewho are improving We also re-treat the10 of patients who suffer an earlyrelapse and are setting up arandomised controlled trial of a secondcourse of Ig for patients still bed-boundtwo weeks after the first course The lesscommon varieties of acute neuropathyare empirically treated in a similar wayAdverse effects of Ig include headachefever nausea eczema aseptic menin-gitis thrombosis and renal failure witha theoretical risk of blood-borne infec-tion Anaphylaxis is a rare but realhazard especially in patients with IgAdeficiency Corticosteroids are no betterthan placebo ndash a surprising observationpossibly explained by an adverse effecton denervated muscle8
Chronic inflammatoryneuropathies
Clinical features
Chronic inflammatory neuropathies aredistinguished from other chronic neuro-pathies by reduced or absent reflexes
Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999 221
Inflammatoryndash Guillain-Barreacute syndromendash vasculitis Churg-Strauss syndrome polyarteritis nodosa systemic lupus
erythematosus ndash infections diphtheria HIV Lyme borreliosis poliomyelitisndash sarcoidosis
Toxinsndash alcoholndash drugs gold isoniazid nitrofurantoin taxol vincristine ndash heavy metals (arsenic lead thallium) hexacarbons organophosphates
Metabolicndash diabetes mellitus porphyria tyrosinaemia
Critical illness polyneuropathy
Nutritional deficienciesndash thiamine
Lymphoma
Table 2 Causes of acute peripheral neuropathy
F ig 4 Schematic representat ion of gangliosides GM 1 and GQ1b Thesemembrane-bound glycolipids are widely distributed throughout the body Autoantibodiesto these and other gangliosides are found in many inflammatory neuropathies and canassist in diagnosis
Glucose
GM1
Ceramide Ceramide
GQ1b
Galactose
N-acetyl galactosamine
Sialic Acid (N-acetyl neuraminic acid)
CM E Neurology ndash I
raised CSF protein usually demyelinatingneurophysiology and the lack of a familyhistory (Table 3) Despite being treatablethey are underdiagnosed
Chronic inflammatory demyelinatingpolyradiculoneuropathy (CIDP) is hetero-geneous with a relapsing-remittingmonophasic or progressive course anda prevalence of at least oneper 100000 Symptoms commonlyinclude weakness andor numbnesspain and ataxia It is rarely severeenough to require ventilatory supportbut half of all patients suffer temporarysevere disability and 13 becomepermanently dependent9
Paraproteinaemic neuropathiesaccount for 10 of demyelinatingneuropathies and are more common inthe elderly10 The paraprotein is usuallya monoclonal gammopathy of un-determined significance of anyimmunoglobulin (Ig) subclass and theassociated clinical picture is heteroge-neous One relatively homogeneoussubgroup consists of the syndrome ofIgM (usually k) paraprotein antibodiesto myelin-associated glycoprotein avery slowly progressive predominantlysensory demyelinating neuropathy anda postural tremor Patients with IgGparaproteins commonly resemblepatients with CIDP though a few haveaxonal neurophysio logy Patients withIgG and IgA paraproteins may have aplasmacytoma or solitary myeloma thisshould always be considered especiallyin treatment resistant cases
Multifocal motor neuropathy withconduction block is an uncommondemyelinating motor neuropathypresenting with progressive patchyasymmetrical weakness beginning inthe upper limbs often with cramps andsometimes minor sensory symptoms11Clinical misdiagnosis as motor neurondisease is possib le because of thepredominant motor phenotype andoccurrence of fasciculations Antibodiesto ganglioside GM1 are present in mostcases but are neither sensitive norspecific
Neurophysiological examination isessentia l for the identification of ademyelinating neuropathy (Fig 6)
222 Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999
Inflammatoryndash autoimmune (D A) (see Table 1) ndash vasculitisconnective tissue disease (A)
Churg-Strauss syndrome polyarteritis nodosa rheumatoid arthritisWegenerrsquos granulomatosis
ndash infection (A D) leprosy herpes zoster HIV
Inheritedndash Charcot-Marie-Tooth disease (hereditary motor sensory neuropathy) (D A)ndash hereditary amyloid neuropathy (A)ndash metachromatic leucodystrophy (D)
Toxinsndash alcohol (A)ndash drugs amiodarone (D) dapsone disulfiram isoniazid metronidazole
nitrofurantoin phenytoin platinum vincristine (A)ndash chemicals (A) acrylamide carbon disulphide heavy metals
Metabolic (A)ndash diabetes mellitus acromegaly myxoedema uraemia
Nutritional deficiencies (A)ndash vitamin B12 pyridoxine thiamine niacin folic acid
Paraproteinaemic (D A)
Paraneoplastic (A D)ndash carcinoma polycythaemia rubra vera
Miscellaneous (A)ndash primary amyloidosis coeliac disease primary biliary cirrhosis
A axonal D demyelinating
Table 3 Causes of chronic peripheral neuropathy
Fig 5 Spontaneous transien t asystole in Guillain- Barreacute syndrom e Autonomicneuropathy may cause tachy- or bradyarrhythmias and a pacemaker may be required
CM E Neurology ndash I
In CIDP there is slowed nerve con-duction especially in motor nerves andthere may be multifocal conductionblock In chronic and severe cases thesuperimposition of axonal degenerationmay make the distinction from axonalneuropathy difficult In IgM para-proteinaemic demyelinating neuro-pathy with anti-myelin-associated glyco-protein antibodies the slowing of nerveconduction is more distal than proximaland there is no conduction block Inmultifocal motor neuropathy with con-duction block there are multiple persis-tent sites of motor conduction block butsensory conduction remains normal inthe same nerve segments In contrastinherited demyelinating neuropathieshave uniform slowing without conduc-tion block
Sural nerve biopsy is indicated only if thediagnosis remains uncertain It oftenshows only non-specific changes andmay cause unpleasant dysaesthesiaeIts greatest use is in the identification ofvasculitis
Treatment
Chronic inflammatory demyelinatingpolyradiculoneuropathy Immuno-modulatory therapy is usually meritedin CIDP except in very mild cases Oralprednisolone (120 mg on alternatedays reducing over 3 months)12 intra-venous Ig (04 mgkgday for 5 days)13
and plasma exchange (10 exchangesover 4 weeks)14 have all been shown tobe efficacious in short-term randomisedcontrolled trials (Ig and plasmaexchange have equiva lent efficacy)Sensory symptoms generally improveless than motor Azathioprine cyclo-phosphamide cyclosporin A and inter-feron a-2a have been reported to beeffective in some patients but have notbeen tested in randomised controlledtrials Our current recommendation forinitial therapy in CIDP is either Ig orpredniso lone (with conside ration ofosteoporosis prophylaxis) A trialcomparing these two is ongoingCombination therapy is often necessaryas the disease progresses If treatmentfails the diagnosis should be re-evaluated and a paraprotein re-sought
Paraproteinaemic demyelinating neuro-pathy has a slightly different treatmentresponse profile10 in that Ig benefitssome patients15 but steroids are gener-ally ineffective Plasma exchange some-times gives at least short-term benefitespecially in patients with an IgA or IgGparaprotein16 A bone marrow examina-tion or radiolog ical skeletal surveysometimes uncovers a primary plasma-cytoma or solitary myeloma treatmentof which may improve the neuropathy(Fig 7) Cyclophosphamide melphalanazathioprine chlorambucil fludarabineand interferon-a have been used butsound evidence is lacking17
Multifocal motor neuropathy with conduc-tion block Two-thirds of these casesrespond to intravenous Ig but treat-ment usually needs to be repeatedmonthly (which is expensive) Steroidshave no effect and may even worsenthe disease Oral or intravenouscyclophosphamide is often used to tryto sustain the response but evidence ofefficacy is lacking
Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999 223
Fig 7 Axial computed tomography of the pelvis of a 45-year old man referred w ithlsquot reatment resistant chronic inf lammatory demyelinating polyradiculo-neuropathyrsquo Serum protein electrophoresis revealed an immunoglobulin G paraproteinThe destructive lesion in the right sacrum was a solitary myeloma His neuropathyimproved after radiotherapy Serum electrophoresis should be done in the investigationof any chronic neuropathy
40
3
0
0
Time (ms)
1
4
21
3
21
10 20 30
Amplitude (mV)
Demyelinating
Axonal
Normal
2
0
6
0
5
Fig 6 Action potentials recorded fromthe thenar muscle after stimulation ofthe median nerve at the w r ist Neurophysiological examination is impor-tant in the diagnosis of a neuropathy Inaxonal neuropathy the major abnormalityis a reduced amplitude whereas indemyelinating neuropathy the response isdisproportionately delayed and dispersed
CM E Neurology ndash I
In all these chronic neuropathies asignificant but unknown proportion ofpatients eventually becomes lessresponsive to treatment as secondaryaxonal degeneration gradually accumu-lates A multidisciplina ry approach tofoot care orthoses physiotherapy andenvironmental aids then becomesparticularly important An excellentpatient support group is available18
Acknowledgments
We are grateful for financial supportfrom the BIOMED InflammatoryNeuropathy Cause and TreatmentProgramme (reference BMH4-CT96-0324) and from the Patrick BerthoudCharitable Trust for MPTL
References
1 Hughes RAC Guillain-Barreacute syndromeLondon SpringerndashVerlag 1990
2 Hahn AF Guilla in-Barreacute syndrome(review) Lancet 1998352635ndash41
3 Rees JH Thompson RD Smeeton NCHughes RAC Epidemiological study ofGuillain-Barreacute syndrome in south eastEngland J Neurol Neurosurg Psychiatry19986474ndash7
4 Hadden RDM Cornblath DR HughesRAC Zielasek J et al Electrophysiologicalclassification of Guillain-Barreacute syndromeclinical associations and outcome AnnNeurol 199844780ndash8
5 Hughes RAC Management of acuteneuromuscular paralysis J R CollPhysicians Lond 199832254ndash9
6 The Guillain-Barreacute Syndrome StudyGroup Plasmapheresis and acuteGuilla in-Barreacute syndrome Neurology1985351096ndash104
7 Plasma Exchange SandoglobulinGuillain-Barreacute Syndrome Trial GroupRandomised trial of plasma exchangeintravenous immunoglobulin andcombined treatments in Guillain-Barreacutesyndrome Lancet 1997349225ndash30
8 Hughes RAC Van der Mecheacute FGACorticosteroid treatment forGuilla in-Barreacute syndrome (CochraneReview) In The Cochrane Library Issue2 1999 Oxford Update Software
9 Lunn MPT Manti H Choudhary PPHughes RAC Thomas PK Chronic inflam-matory demyelinating polyradiculo-
neuropathy a prevalence study in southeast England J Neurol NeurosurgPsychiatry 199966677ndash80
10 Ropper AH Gorson KC Neuropathiesassociated with paraproteinemia(review) N Engl J Med 19983381601ndash7
11 Biessels GJ Franssen H Van den Berg LHGibson A et al Multifocal motorneuropathy (review) J Neurol 1997244143ndash52
12 Dyck PJ OrsquoBrien PC Oviatt KF DinapoliRP et al Prednisone improves chronicinflammatory demyelinating polyradicu-loneuropathy more than no treatmentAnn Neurol 198211136ndash41
13 Hahn AF Bolton CF Pillay N Chalk Cetal Plasma-exchange therapy in chronicinflammatory demyelinating poly-neuropathy ndash a double-blind sham-controlled cross-over study Brain 19961191055ndash66
14 Hahn AF Bolton CF Zochodne D FeasbyTE Intravenous immunoglobulin treat-ment in chronic inflammatory demyeli-nating polyneuropathy ndash a double-blind
placebo-controlled cross-over studyBrain 19961191067ndash77
15 Dalakas MC Quarles RH Farrer RGDambrosia J et al A controlled study ofintravenous immunoglobulin indemyelinating neuropathy with IgMgammopathy Ann Neurol 199640792ndash5
16 Dyck PJ Low PA Windebank AJ JaradehSS et al Plasma exchange in poly-neuropathy associated with monoclonalgammopathy of undetermined signifi-cance N Engl J Med 19913251482ndash6
17 Mariette X Chastang C Clavelou PLouboutin JP et al A randomised clinicaltrial comparing interferon-a and intra-venous immunoglobulin in poly-neuropathy associated with monoclonalIgM J Neurol Neurosurg Psychiatry19976328ndash34
18 The Guillain-Barreacute Syndrome SupportGroup of the UK Lincolnshire CountyCouncil Offices Eastgate SleafordLincolnshire NG34 7EB Tel fax01529 304 615 wwwgbsorguk
224 Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999
Autoimmune inflammatory neuropathy is a spectrum of disorders
copy acute and chronic
copy focal and generalised
copy demyelinating and axonal
Guillain-Barreacute syndrome
copy reflexes cerebrospinal fluid and neurophysiology may be normal in the early
stages
copy adverse prognostic factors older age preceding diarrhoea severe weakness
inexcitable nerves
copy treat w ith intravenous immunoglobulin
Chronic demyelinating neuropathy
copy check for a paraprotein
copy IgM k paraprotein with antibodies to myelin-associated glycoprotein is
associated with a benign predominantly sensory neuropathy
copy treat chronic inflammatory demyelinating polyradiculoneuropathy initially
w ith prednisolone or intravenous immunoglobulin
copy treat multifocal motor neuropathy with conduction block with intravenous
immunoglobulin
Key Points

CM E Neurology ndash I
raised CSF protein usually demyelinatingneurophysiology and the lack of a familyhistory (Table 3) Despite being treatablethey are underdiagnosed
Chronic inflammatory demyelinatingpolyradiculoneuropathy (CIDP) is hetero-geneous with a relapsing-remittingmonophasic or progressive course anda prevalence of at least oneper 100000 Symptoms commonlyinclude weakness andor numbnesspain and ataxia It is rarely severeenough to require ventilatory supportbut half of all patients suffer temporarysevere disability and 13 becomepermanently dependent9
Paraproteinaemic neuropathiesaccount for 10 of demyelinatingneuropathies and are more common inthe elderly10 The paraprotein is usuallya monoclonal gammopathy of un-determined significance of anyimmunoglobulin (Ig) subclass and theassociated clinical picture is heteroge-neous One relatively homogeneoussubgroup consists of the syndrome ofIgM (usually k) paraprotein antibodiesto myelin-associated glycoprotein avery slowly progressive predominantlysensory demyelinating neuropathy anda postural tremor Patients with IgGparaproteins commonly resemblepatients with CIDP though a few haveaxonal neurophysio logy Patients withIgG and IgA paraproteins may have aplasmacytoma or solitary myeloma thisshould always be considered especiallyin treatment resistant cases
Multifocal motor neuropathy withconduction block is an uncommondemyelinating motor neuropathypresenting with progressive patchyasymmetrical weakness beginning inthe upper limbs often with cramps andsometimes minor sensory symptoms11Clinical misdiagnosis as motor neurondisease is possib le because of thepredominant motor phenotype andoccurrence of fasciculations Antibodiesto ganglioside GM1 are present in mostcases but are neither sensitive norspecific
Neurophysiological examination isessentia l for the identification of ademyelinating neuropathy (Fig 6)
222 Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999
Inflammatoryndash autoimmune (D A) (see Table 1) ndash vasculitisconnective tissue disease (A)
Churg-Strauss syndrome polyarteritis nodosa rheumatoid arthritisWegenerrsquos granulomatosis
ndash infection (A D) leprosy herpes zoster HIV
Inheritedndash Charcot-Marie-Tooth disease (hereditary motor sensory neuropathy) (D A)ndash hereditary amyloid neuropathy (A)ndash metachromatic leucodystrophy (D)
Toxinsndash alcohol (A)ndash drugs amiodarone (D) dapsone disulfiram isoniazid metronidazole
nitrofurantoin phenytoin platinum vincristine (A)ndash chemicals (A) acrylamide carbon disulphide heavy metals
Metabolic (A)ndash diabetes mellitus acromegaly myxoedema uraemia
Nutritional deficiencies (A)ndash vitamin B12 pyridoxine thiamine niacin folic acid
Paraproteinaemic (D A)
Paraneoplastic (A D)ndash carcinoma polycythaemia rubra vera
Miscellaneous (A)ndash primary amyloidosis coeliac disease primary biliary cirrhosis
A axonal D demyelinating
Table 3 Causes of chronic peripheral neuropathy
Fig 5 Spontaneous transien t asystole in Guillain- Barreacute syndrom e Autonomicneuropathy may cause tachy- or bradyarrhythmias and a pacemaker may be required
CM E Neurology ndash I
In CIDP there is slowed nerve con-duction especially in motor nerves andthere may be multifocal conductionblock In chronic and severe cases thesuperimposition of axonal degenerationmay make the distinction from axonalneuropathy difficult In IgM para-proteinaemic demyelinating neuro-pathy with anti-myelin-associated glyco-protein antibodies the slowing of nerveconduction is more distal than proximaland there is no conduction block Inmultifocal motor neuropathy with con-duction block there are multiple persis-tent sites of motor conduction block butsensory conduction remains normal inthe same nerve segments In contrastinherited demyelinating neuropathieshave uniform slowing without conduc-tion block
Sural nerve biopsy is indicated only if thediagnosis remains uncertain It oftenshows only non-specific changes andmay cause unpleasant dysaesthesiaeIts greatest use is in the identification ofvasculitis
Treatment
Chronic inflammatory demyelinatingpolyradiculoneuropathy Immuno-modulatory therapy is usually meritedin CIDP except in very mild cases Oralprednisolone (120 mg on alternatedays reducing over 3 months)12 intra-venous Ig (04 mgkgday for 5 days)13
and plasma exchange (10 exchangesover 4 weeks)14 have all been shown tobe efficacious in short-term randomisedcontrolled trials (Ig and plasmaexchange have equiva lent efficacy)Sensory symptoms generally improveless than motor Azathioprine cyclo-phosphamide cyclosporin A and inter-feron a-2a have been reported to beeffective in some patients but have notbeen tested in randomised controlledtrials Our current recommendation forinitial therapy in CIDP is either Ig orpredniso lone (with conside ration ofosteoporosis prophylaxis) A trialcomparing these two is ongoingCombination therapy is often necessaryas the disease progresses If treatmentfails the diagnosis should be re-evaluated and a paraprotein re-sought
Paraproteinaemic demyelinating neuro-pathy has a slightly different treatmentresponse profile10 in that Ig benefitssome patients15 but steroids are gener-ally ineffective Plasma exchange some-times gives at least short-term benefitespecially in patients with an IgA or IgGparaprotein16 A bone marrow examina-tion or radiolog ical skeletal surveysometimes uncovers a primary plasma-cytoma or solitary myeloma treatmentof which may improve the neuropathy(Fig 7) Cyclophosphamide melphalanazathioprine chlorambucil fludarabineand interferon-a have been used butsound evidence is lacking17
Multifocal motor neuropathy with conduc-tion block Two-thirds of these casesrespond to intravenous Ig but treat-ment usually needs to be repeatedmonthly (which is expensive) Steroidshave no effect and may even worsenthe disease Oral or intravenouscyclophosphamide is often used to tryto sustain the response but evidence ofefficacy is lacking
Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999 223
Fig 7 Axial computed tomography of the pelvis of a 45-year old man referred w ithlsquot reatment resistant chronic inf lammatory demyelinating polyradiculo-neuropathyrsquo Serum protein electrophoresis revealed an immunoglobulin G paraproteinThe destructive lesion in the right sacrum was a solitary myeloma His neuropathyimproved after radiotherapy Serum electrophoresis should be done in the investigationof any chronic neuropathy
40
3
0
0
Time (ms)
1
4
21
3
21
10 20 30
Amplitude (mV)
Demyelinating
Axonal
Normal
2
0
6
0
5
Fig 6 Action potentials recorded fromthe thenar muscle after stimulation ofthe median nerve at the w r ist Neurophysiological examination is impor-tant in the diagnosis of a neuropathy Inaxonal neuropathy the major abnormalityis a reduced amplitude whereas indemyelinating neuropathy the response isdisproportionately delayed and dispersed
CM E Neurology ndash I
In all these chronic neuropathies asignificant but unknown proportion ofpatients eventually becomes lessresponsive to treatment as secondaryaxonal degeneration gradually accumu-lates A multidisciplina ry approach tofoot care orthoses physiotherapy andenvironmental aids then becomesparticularly important An excellentpatient support group is available18
Acknowledgments
We are grateful for financial supportfrom the BIOMED InflammatoryNeuropathy Cause and TreatmentProgramme (reference BMH4-CT96-0324) and from the Patrick BerthoudCharitable Trust for MPTL
References
1 Hughes RAC Guillain-Barreacute syndromeLondon SpringerndashVerlag 1990
2 Hahn AF Guilla in-Barreacute syndrome(review) Lancet 1998352635ndash41
3 Rees JH Thompson RD Smeeton NCHughes RAC Epidemiological study ofGuillain-Barreacute syndrome in south eastEngland J Neurol Neurosurg Psychiatry19986474ndash7
4 Hadden RDM Cornblath DR HughesRAC Zielasek J et al Electrophysiologicalclassification of Guillain-Barreacute syndromeclinical associations and outcome AnnNeurol 199844780ndash8
5 Hughes RAC Management of acuteneuromuscular paralysis J R CollPhysicians Lond 199832254ndash9
6 The Guillain-Barreacute Syndrome StudyGroup Plasmapheresis and acuteGuilla in-Barreacute syndrome Neurology1985351096ndash104
7 Plasma Exchange SandoglobulinGuillain-Barreacute Syndrome Trial GroupRandomised trial of plasma exchangeintravenous immunoglobulin andcombined treatments in Guillain-Barreacutesyndrome Lancet 1997349225ndash30
8 Hughes RAC Van der Mecheacute FGACorticosteroid treatment forGuilla in-Barreacute syndrome (CochraneReview) In The Cochrane Library Issue2 1999 Oxford Update Software
9 Lunn MPT Manti H Choudhary PPHughes RAC Thomas PK Chronic inflam-matory demyelinating polyradiculo-
neuropathy a prevalence study in southeast England J Neurol NeurosurgPsychiatry 199966677ndash80
10 Ropper AH Gorson KC Neuropathiesassociated with paraproteinemia(review) N Engl J Med 19983381601ndash7
11 Biessels GJ Franssen H Van den Berg LHGibson A et al Multifocal motorneuropathy (review) J Neurol 1997244143ndash52
12 Dyck PJ OrsquoBrien PC Oviatt KF DinapoliRP et al Prednisone improves chronicinflammatory demyelinating polyradicu-loneuropathy more than no treatmentAnn Neurol 198211136ndash41
13 Hahn AF Bolton CF Pillay N Chalk Cetal Plasma-exchange therapy in chronicinflammatory demyelinating poly-neuropathy ndash a double-blind sham-controlled cross-over study Brain 19961191055ndash66
14 Hahn AF Bolton CF Zochodne D FeasbyTE Intravenous immunoglobulin treat-ment in chronic inflammatory demyeli-nating polyneuropathy ndash a double-blind
placebo-controlled cross-over studyBrain 19961191067ndash77
15 Dalakas MC Quarles RH Farrer RGDambrosia J et al A controlled study ofintravenous immunoglobulin indemyelinating neuropathy with IgMgammopathy Ann Neurol 199640792ndash5
16 Dyck PJ Low PA Windebank AJ JaradehSS et al Plasma exchange in poly-neuropathy associated with monoclonalgammopathy of undetermined signifi-cance N Engl J Med 19913251482ndash6
17 Mariette X Chastang C Clavelou PLouboutin JP et al A randomised clinicaltrial comparing interferon-a and intra-venous immunoglobulin in poly-neuropathy associated with monoclonalIgM J Neurol Neurosurg Psychiatry19976328ndash34
18 The Guillain-Barreacute Syndrome SupportGroup of the UK Lincolnshire CountyCouncil Offices Eastgate SleafordLincolnshire NG34 7EB Tel fax01529 304 615 wwwgbsorguk
224 Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999
Autoimmune inflammatory neuropathy is a spectrum of disorders
copy acute and chronic
copy focal and generalised
copy demyelinating and axonal
Guillain-Barreacute syndrome
copy reflexes cerebrospinal fluid and neurophysiology may be normal in the early
stages
copy adverse prognostic factors older age preceding diarrhoea severe weakness
inexcitable nerves
copy treat w ith intravenous immunoglobulin
Chronic demyelinating neuropathy
copy check for a paraprotein
copy IgM k paraprotein with antibodies to myelin-associated glycoprotein is
associated with a benign predominantly sensory neuropathy
copy treat chronic inflammatory demyelinating polyradiculoneuropathy initially
w ith prednisolone or intravenous immunoglobulin
copy treat multifocal motor neuropathy with conduction block with intravenous
immunoglobulin
Key Points

CM E Neurology ndash I
In CIDP there is slowed nerve con-duction especially in motor nerves andthere may be multifocal conductionblock In chronic and severe cases thesuperimposition of axonal degenerationmay make the distinction from axonalneuropathy difficult In IgM para-proteinaemic demyelinating neuro-pathy with anti-myelin-associated glyco-protein antibodies the slowing of nerveconduction is more distal than proximaland there is no conduction block Inmultifocal motor neuropathy with con-duction block there are multiple persis-tent sites of motor conduction block butsensory conduction remains normal inthe same nerve segments In contrastinherited demyelinating neuropathieshave uniform slowing without conduc-tion block
Sural nerve biopsy is indicated only if thediagnosis remains uncertain It oftenshows only non-specific changes andmay cause unpleasant dysaesthesiaeIts greatest use is in the identification ofvasculitis
Treatment
Chronic inflammatory demyelinatingpolyradiculoneuropathy Immuno-modulatory therapy is usually meritedin CIDP except in very mild cases Oralprednisolone (120 mg on alternatedays reducing over 3 months)12 intra-venous Ig (04 mgkgday for 5 days)13
and plasma exchange (10 exchangesover 4 weeks)14 have all been shown tobe efficacious in short-term randomisedcontrolled trials (Ig and plasmaexchange have equiva lent efficacy)Sensory symptoms generally improveless than motor Azathioprine cyclo-phosphamide cyclosporin A and inter-feron a-2a have been reported to beeffective in some patients but have notbeen tested in randomised controlledtrials Our current recommendation forinitial therapy in CIDP is either Ig orpredniso lone (with conside ration ofosteoporosis prophylaxis) A trialcomparing these two is ongoingCombination therapy is often necessaryas the disease progresses If treatmentfails the diagnosis should be re-evaluated and a paraprotein re-sought
Paraproteinaemic demyelinating neuro-pathy has a slightly different treatmentresponse profile10 in that Ig benefitssome patients15 but steroids are gener-ally ineffective Plasma exchange some-times gives at least short-term benefitespecially in patients with an IgA or IgGparaprotein16 A bone marrow examina-tion or radiolog ical skeletal surveysometimes uncovers a primary plasma-cytoma or solitary myeloma treatmentof which may improve the neuropathy(Fig 7) Cyclophosphamide melphalanazathioprine chlorambucil fludarabineand interferon-a have been used butsound evidence is lacking17
Multifocal motor neuropathy with conduc-tion block Two-thirds of these casesrespond to intravenous Ig but treat-ment usually needs to be repeatedmonthly (which is expensive) Steroidshave no effect and may even worsenthe disease Oral or intravenouscyclophosphamide is often used to tryto sustain the response but evidence ofefficacy is lacking
Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999 223
Fig 7 Axial computed tomography of the pelvis of a 45-year old man referred w ithlsquot reatment resistant chronic inf lammatory demyelinating polyradiculo-neuropathyrsquo Serum protein electrophoresis revealed an immunoglobulin G paraproteinThe destructive lesion in the right sacrum was a solitary myeloma His neuropathyimproved after radiotherapy Serum electrophoresis should be done in the investigationof any chronic neuropathy
40
3
0
0
Time (ms)
1
4
21
3
21
10 20 30
Amplitude (mV)
Demyelinating
Axonal
Normal
2
0
6
0
5
Fig 6 Action potentials recorded fromthe thenar muscle after stimulation ofthe median nerve at the w r ist Neurophysiological examination is impor-tant in the diagnosis of a neuropathy Inaxonal neuropathy the major abnormalityis a reduced amplitude whereas indemyelinating neuropathy the response isdisproportionately delayed and dispersed
CM E Neurology ndash I
In all these chronic neuropathies asignificant but unknown proportion ofpatients eventually becomes lessresponsive to treatment as secondaryaxonal degeneration gradually accumu-lates A multidisciplina ry approach tofoot care orthoses physiotherapy andenvironmental aids then becomesparticularly important An excellentpatient support group is available18
Acknowledgments
We are grateful for financial supportfrom the BIOMED InflammatoryNeuropathy Cause and TreatmentProgramme (reference BMH4-CT96-0324) and from the Patrick BerthoudCharitable Trust for MPTL
References
1 Hughes RAC Guillain-Barreacute syndromeLondon SpringerndashVerlag 1990
2 Hahn AF Guilla in-Barreacute syndrome(review) Lancet 1998352635ndash41
3 Rees JH Thompson RD Smeeton NCHughes RAC Epidemiological study ofGuillain-Barreacute syndrome in south eastEngland J Neurol Neurosurg Psychiatry19986474ndash7
4 Hadden RDM Cornblath DR HughesRAC Zielasek J et al Electrophysiologicalclassification of Guillain-Barreacute syndromeclinical associations and outcome AnnNeurol 199844780ndash8
5 Hughes RAC Management of acuteneuromuscular paralysis J R CollPhysicians Lond 199832254ndash9
6 The Guillain-Barreacute Syndrome StudyGroup Plasmapheresis and acuteGuilla in-Barreacute syndrome Neurology1985351096ndash104
7 Plasma Exchange SandoglobulinGuillain-Barreacute Syndrome Trial GroupRandomised trial of plasma exchangeintravenous immunoglobulin andcombined treatments in Guillain-Barreacutesyndrome Lancet 1997349225ndash30
8 Hughes RAC Van der Mecheacute FGACorticosteroid treatment forGuilla in-Barreacute syndrome (CochraneReview) In The Cochrane Library Issue2 1999 Oxford Update Software
9 Lunn MPT Manti H Choudhary PPHughes RAC Thomas PK Chronic inflam-matory demyelinating polyradiculo-
neuropathy a prevalence study in southeast England J Neurol NeurosurgPsychiatry 199966677ndash80
10 Ropper AH Gorson KC Neuropathiesassociated with paraproteinemia(review) N Engl J Med 19983381601ndash7
11 Biessels GJ Franssen H Van den Berg LHGibson A et al Multifocal motorneuropathy (review) J Neurol 1997244143ndash52
12 Dyck PJ OrsquoBrien PC Oviatt KF DinapoliRP et al Prednisone improves chronicinflammatory demyelinating polyradicu-loneuropathy more than no treatmentAnn Neurol 198211136ndash41
13 Hahn AF Bolton CF Pillay N Chalk Cetal Plasma-exchange therapy in chronicinflammatory demyelinating poly-neuropathy ndash a double-blind sham-controlled cross-over study Brain 19961191055ndash66
14 Hahn AF Bolton CF Zochodne D FeasbyTE Intravenous immunoglobulin treat-ment in chronic inflammatory demyeli-nating polyneuropathy ndash a double-blind
placebo-controlled cross-over studyBrain 19961191067ndash77
15 Dalakas MC Quarles RH Farrer RGDambrosia J et al A controlled study ofintravenous immunoglobulin indemyelinating neuropathy with IgMgammopathy Ann Neurol 199640792ndash5
16 Dyck PJ Low PA Windebank AJ JaradehSS et al Plasma exchange in poly-neuropathy associated with monoclonalgammopathy of undetermined signifi-cance N Engl J Med 19913251482ndash6
17 Mariette X Chastang C Clavelou PLouboutin JP et al A randomised clinicaltrial comparing interferon-a and intra-venous immunoglobulin in poly-neuropathy associated with monoclonalIgM J Neurol Neurosurg Psychiatry19976328ndash34
18 The Guillain-Barreacute Syndrome SupportGroup of the UK Lincolnshire CountyCouncil Offices Eastgate SleafordLincolnshire NG34 7EB Tel fax01529 304 615 wwwgbsorguk
224 Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999
Autoimmune inflammatory neuropathy is a spectrum of disorders
copy acute and chronic
copy focal and generalised
copy demyelinating and axonal
Guillain-Barreacute syndrome
copy reflexes cerebrospinal fluid and neurophysiology may be normal in the early
stages
copy adverse prognostic factors older age preceding diarrhoea severe weakness
inexcitable nerves
copy treat w ith intravenous immunoglobulin
Chronic demyelinating neuropathy
copy check for a paraprotein
copy IgM k paraprotein with antibodies to myelin-associated glycoprotein is
associated with a benign predominantly sensory neuropathy
copy treat chronic inflammatory demyelinating polyradiculoneuropathy initially
w ith prednisolone or intravenous immunoglobulin
copy treat multifocal motor neuropathy with conduction block with intravenous
immunoglobulin
Key Points

CM E Neurology ndash I
In all these chronic neuropathies asignificant but unknown proportion ofpatients eventually becomes lessresponsive to treatment as secondaryaxonal degeneration gradually accumu-lates A multidisciplina ry approach tofoot care orthoses physiotherapy andenvironmental aids then becomesparticularly important An excellentpatient support group is available18
Acknowledgments
We are grateful for financial supportfrom the BIOMED InflammatoryNeuropathy Cause and TreatmentProgramme (reference BMH4-CT96-0324) and from the Patrick BerthoudCharitable Trust for MPTL
References
1 Hughes RAC Guillain-Barreacute syndromeLondon SpringerndashVerlag 1990
2 Hahn AF Guilla in-Barreacute syndrome(review) Lancet 1998352635ndash41
3 Rees JH Thompson RD Smeeton NCHughes RAC Epidemiological study ofGuillain-Barreacute syndrome in south eastEngland J Neurol Neurosurg Psychiatry19986474ndash7
4 Hadden RDM Cornblath DR HughesRAC Zielasek J et al Electrophysiologicalclassification of Guillain-Barreacute syndromeclinical associations and outcome AnnNeurol 199844780ndash8
5 Hughes RAC Management of acuteneuromuscular paralysis J R CollPhysicians Lond 199832254ndash9
6 The Guillain-Barreacute Syndrome StudyGroup Plasmapheresis and acuteGuilla in-Barreacute syndrome Neurology1985351096ndash104
7 Plasma Exchange SandoglobulinGuillain-Barreacute Syndrome Trial GroupRandomised trial of plasma exchangeintravenous immunoglobulin andcombined treatments in Guillain-Barreacutesyndrome Lancet 1997349225ndash30
8 Hughes RAC Van der Mecheacute FGACorticosteroid treatment forGuilla in-Barreacute syndrome (CochraneReview) In The Cochrane Library Issue2 1999 Oxford Update Software
9 Lunn MPT Manti H Choudhary PPHughes RAC Thomas PK Chronic inflam-matory demyelinating polyradiculo-
neuropathy a prevalence study in southeast England J Neurol NeurosurgPsychiatry 199966677ndash80
10 Ropper AH Gorson KC Neuropathiesassociated with paraproteinemia(review) N Engl J Med 19983381601ndash7
11 Biessels GJ Franssen H Van den Berg LHGibson A et al Multifocal motorneuropathy (review) J Neurol 1997244143ndash52
12 Dyck PJ OrsquoBrien PC Oviatt KF DinapoliRP et al Prednisone improves chronicinflammatory demyelinating polyradicu-loneuropathy more than no treatmentAnn Neurol 198211136ndash41
13 Hahn AF Bolton CF Pillay N Chalk Cetal Plasma-exchange therapy in chronicinflammatory demyelinating poly-neuropathy ndash a double-blind sham-controlled cross-over study Brain 19961191055ndash66
14 Hahn AF Bolton CF Zochodne D FeasbyTE Intravenous immunoglobulin treat-ment in chronic inflammatory demyeli-nating polyneuropathy ndash a double-blind
placebo-controlled cross-over studyBrain 19961191067ndash77
15 Dalakas MC Quarles RH Farrer RGDambrosia J et al A controlled study ofintravenous immunoglobulin indemyelinating neuropathy with IgMgammopathy Ann Neurol 199640792ndash5
16 Dyck PJ Low PA Windebank AJ JaradehSS et al Plasma exchange in poly-neuropathy associated with monoclonalgammopathy of undetermined signifi-cance N Engl J Med 19913251482ndash6
17 Mariette X Chastang C Clavelou PLouboutin JP et al A randomised clinicaltrial comparing interferon-a and intra-venous immunoglobulin in poly-neuropathy associated with monoclonalIgM J Neurol Neurosurg Psychiatry19976328ndash34
18 The Guillain-Barreacute Syndrome SupportGroup of the UK Lincolnshire CountyCouncil Offices Eastgate SleafordLincolnshire NG34 7EB Tel fax01529 304 615 wwwgbsorguk
224 Journal of the Royal College of Physicians of London Vol 33 No 3 MayJune 1999
Autoimmune inflammatory neuropathy is a spectrum of disorders
copy acute and chronic
copy focal and generalised
copy demyelinating and axonal
Guillain-Barreacute syndrome
copy reflexes cerebrospinal fluid and neurophysiology may be normal in the early
stages
copy adverse prognostic factors older age preceding diarrhoea severe weakness
inexcitable nerves
copy treat w ith intravenous immunoglobulin
Chronic demyelinating neuropathy
copy check for a paraprotein
copy IgM k paraprotein with antibodies to myelin-associated glycoprotein is
associated with a benign predominantly sensory neuropathy
copy treat chronic inflammatory demyelinating polyradiculoneuropathy initially
w ith prednisolone or intravenous immunoglobulin
copy treat multifocal motor neuropathy with conduction block with intravenous
immunoglobulin
Key Points