Embed Size (px)
Citation preview

Autism Spectrum DisordersAutism Spectrum Disorders
Robin K. Rumsey, Ph.D., L.P.Robin K. Rumsey, Ph.D., L.P.
November 8, 2007November 8, 2007

Topics ReviewedTopics Reviewed
Diagnosis and Early IdentificationDiagnosis and Early Identification
Epidemiology/ Hypothesized CausesEpidemiology/ Hypothesized Causes
Treatment and InterventionTreatment and Intervention
Other ConsiderationsOther Considerations

DiagnosisDiagnosis
Qualitative impairments inQualitative impairments in
SOCIAL INTERACTION SOCIAL INTERACTION
CommunicationCommunication
Restricted, repetitive and stereotyped patterns Restricted, repetitive and stereotyped patterns of behavior, interests or activitiesof behavior, interests or activities
DiagnosisDiagnosis
QualifiersQualifiers
Onset in at least 1 domain before age 3Onset in at least 1 domain before age 3
Not better accounted for by other diagnosisNot better accounted for by other diagnosis

DiagnosisDiagnosis
Autistic DisorderAutistic Disorder
Asperger’s DisorderAsperger’s Disorder
Pervasive Developmental Disorder Not Pervasive Developmental Disorder Not Otherwise Specified (PDD NOS)Otherwise Specified (PDD NOS)
Diagnosis and DefinitionDiagnosis and Definition
Diagnosis in young childrenDiagnosis in young children Autism can be reliably diagnosed as young as Autism can be reliably diagnosed as young as
2 years2 years More variability with children with early More variability with children with early
diagnoses of PDD, NOSdiagnoses of PDD, NOS Repetitive behaviors are less common in both Repetitive behaviors are less common in both
very young children and high-functioning very young children and high-functioning adolescents and adultsadolescents and adults
DiagnosisDiagnosis
Medical Diagnosis versus Educational Medical Diagnosis versus Educational IdentificationIdentification

CHATCHATChecklist for Autism in ToddlersChecklist for Autism in Toddlers
18-month visit18-month visit
9 Parent Questions/5 physician Observations9 Parent Questions/5 physician Observations5 Key Items5 Key Items
1.1. Parent: “Enjoy playing peek-a-boo?” - Parent: “Enjoy playing peek-a-boo?” - joint attentionjoint attention2.2. Parent: “Use his/her index finger to point, to ASK for something?) Parent: “Use his/her index finger to point, to ASK for something?)
protoimperative pointingprotoimperative pointing3.3. Physician : “Oh look (point), there’s a (toy).” Physician : “Oh look (point), there’s a (toy).” - - following a pointfollowing a point4.4. Physician: “Can you pour a glass of water?”– Physician: “Can you pour a glass of water?”– pretendingpretending5.5. Physician: “Where’s the light?” - Physician: “Where’s the light?” - producing a pointproducing a point

Can Autism be reliably diagnosed <36 Can Autism be reliably diagnosed <36 months?months?
Problems measurable by 18 mo and stable Problems measurable by 18 mo and stable through preschool age center around through preschool age center around development of development of joint attention and joint attention and communicationcommunication
Intense social interest in faces - 4 moIntense social interest in faces - 4 mo orienting to name - 12 moorienting to name - 12 mo Protoimperative pointing - 12-14 moProtoimperative pointing - 12-14 mo Protodeclarative pointing - 14-16 moProtodeclarative pointing - 14-16 mo Atypical or no language developmentAtypical or no language development Joint attention is substrate of cognition necessary Joint attention is substrate of cognition necessary
for language developmentfor language development
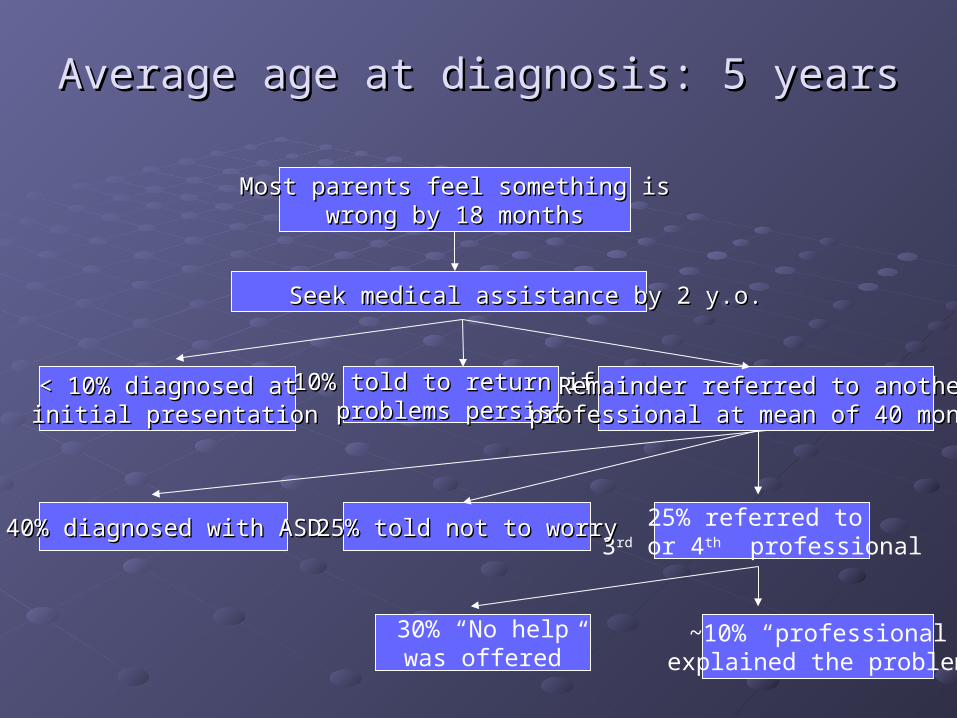
Average age at diagnosis: 5 yearsAverage age at diagnosis: 5 years
Most parents feel something isMost parents feel something iswrong by 18 monthswrong by 18 months
Seek medical assistance by 2 y.o.Seek medical assistance by 2 y.o.
< 10% diagnosed at< 10% diagnosed at initial presentationinitial presentation
10% told to return if 10% told to return if problems persistproblems persist
Remainder referred to anotherRemainder referred to anotherprofessional at mean of 40 monthsprofessional at mean of 40 months
25% referred to 3rd or 4th professional
40% diagnosed with ASD40% diagnosed with ASD 25% told not to worry25% told not to worry
30% “No help was offered”
~10% “professional explained the problem”

Early Developmental Early Developmental Trajectories in Typical Trajectories in Typical
DevelopmentDevelopment

Children with autismChildren with autism
Don’t have the basic presupposition that Don’t have the basic presupposition that they are like other people and others are they are like other people and others are like themlike them
Trouble imitating facial expressionsTrouble imitating facial expressions
Don’t point or follow objectsDon’t point or follow objects
Don’t understand false beliefsDon’t understand false beliefs
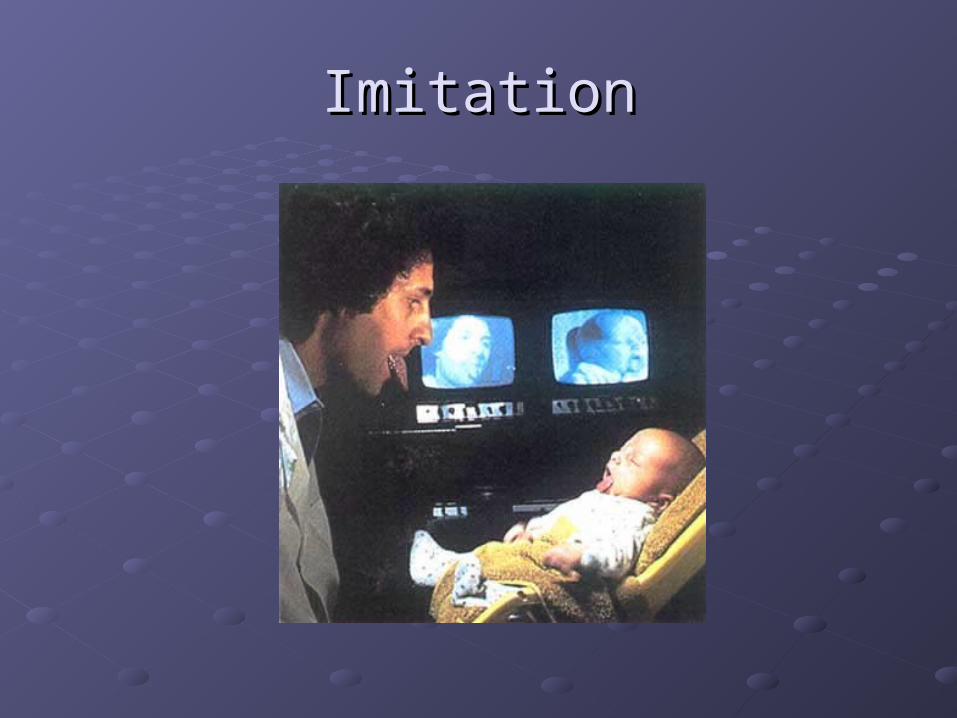
ImitationImitation
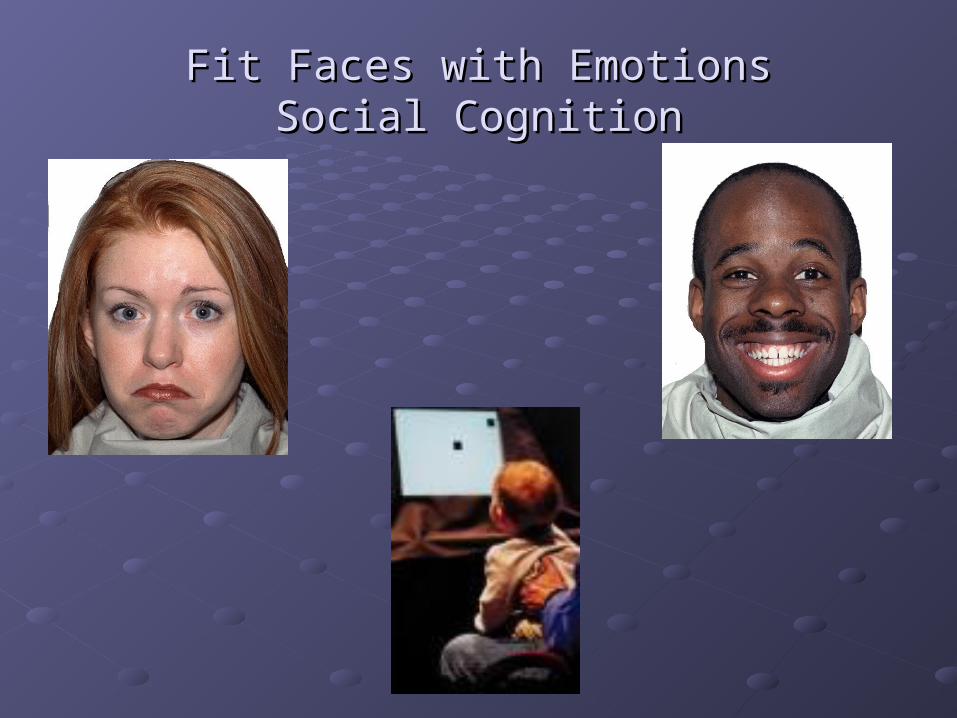
Fit Faces with EmotionsFit Faces with EmotionsSocial CognitionSocial Cognition

Social engagementSocial engagement
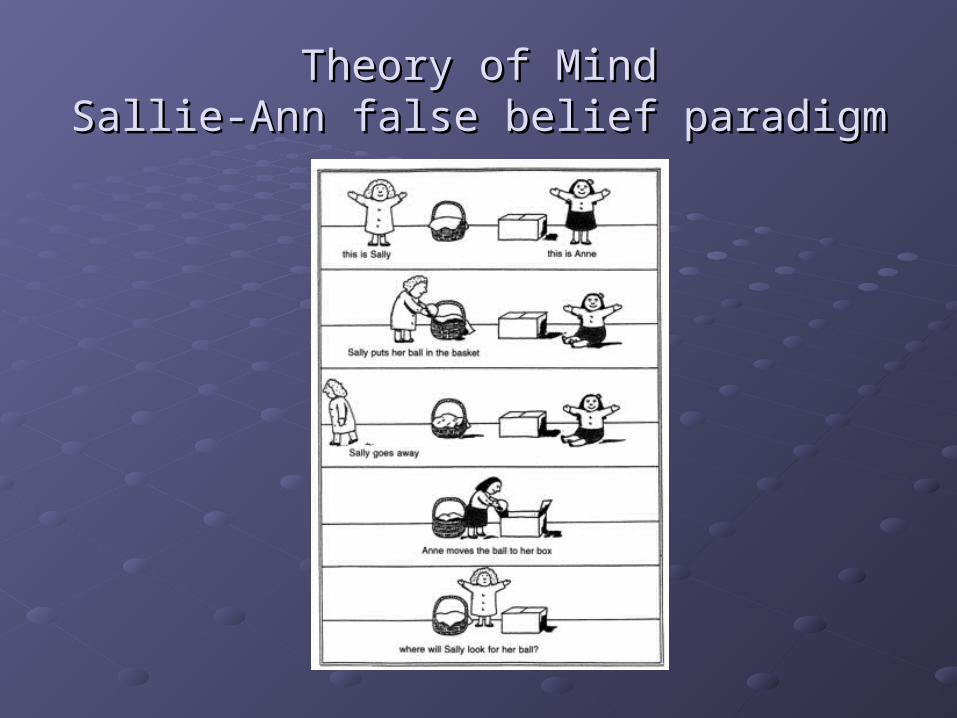
Theory of MindTheory of MindSallie-Ann false belief paradigmSallie-Ann false belief paradigm

Joint AttentionJoint Attention
Early IdentificationEarly IdentificationWhy?Why?
Self-imposed social deprivation Self-imposed social deprivation compromises behavioral and brain compromises behavioral and brain developmentdevelopment
Outcome evidence supports early Outcome evidence supports early interventionintervention Early identification Early identification intense structured intense structured
social input social input More typical development More typical development

Early IdentificationEarly Identification
First Signs videoFirst Signs video

Assessment for ASDAssessment for ASD
Should include direct assessment of Should include direct assessment of cognitive skills/ development, language, cognitive skills/ development, language, adaptive functioning, and behavior adaptive functioning, and behavior whenever possible.whenever possible.
Diagnosis should be based on parent Diagnosis should be based on parent interview, direct observation (Autism interview, direct observation (Autism Diagnostic Observation Schedule) and, if Diagnostic Observation Schedule) and, if possible, teacher observations.possible, teacher observations.

Hypothesized Causes/ EpidemiologyHypothesized Causes/ Epidemiology

Risk FactorsRisk Factors
MalesMalesMonozygotic twinsMonozygotic twins
60% for DSM-IV autistic disorder60% for DSM-IV autistic disorder 71% for ASD phenotype71% for ASD phenotype 92% broader phenotype of social and communication deficits 92% broader phenotype of social and communication deficits
SiblingsSiblings 3-20% (50-100x) 3-20% (50-100x)
Increasing maternal ageIncreasing maternal ageIntrauterine infections Intrauterine infections
rubella, CMV, herpes, HIV - probably additive brain trauma rubella, CMV, herpes, HIV - probably additive brain trauma rather than distinct ASD etiologyrather than distinct ASD etiology
Neurotoxin exposure during pregnancy including ETOH Neurotoxin exposure during pregnancy including ETOH (FAS/ARND)(FAS/ARND)
Risk Factors / Family HistoryRisk Factors / Family HistoryGenetic loading or genetic etiologiesGenetic loading or genetic etiologies
Dimensional DisorderDimensional Disorder
Within families – broader autistic phenotypeWithin families – broader autistic phenotype More social difficultiesMore social difficulties Higher cognitive, and executive function deficitsHigher cognitive, and executive function deficits Increased stereotypic behaviorIncreased stereotypic behavior Language and pragmatic disordersLanguage and pragmatic disorders Social problemsSocial problems Anxiety and OCDAnxiety and OCD Affect disordersAffect disorders Schizophrenia, anxiety, bipolar disorderSchizophrenia, anxiety, bipolar disorder LDLD Cognitive Adaptive DisorderCognitive Adaptive Disorder

Autism comorbidityAutism comorbidity
50-75% with Cognitive Adaptive Disorders50-75% with Cognitive Adaptive Disorders IQ best predicator of outcomeIQ best predicator of outcome
5-10% with Rare disorders5-10% with Rare disorders
10-30% with Epilepsy10-30% with Epilepsy
?% with ADHD and other DSM diagnoses?% with ADHD and other DSM diagnoses

Syndromic AutismSyndromic Autism

Causes of /Associations withCauses of /Associations withSyndromic AutismSyndromic Autism
Modified from Ozonoff et al 2003Modified from Ozonoff et al 2003
Chromosomal syndromesChromosomal syndromes Fragile X, Angelman syndrome, 15q duplications, Down Syndrome, del22q11, Fragile X, Angelman syndrome, 15q duplications, Down Syndrome, del22q11,
Ring 20, Rett disorderRing 20, Rett disorderSyndromes/associations without known chromosome anomaliesSyndromes/associations without known chromosome anomalies
Sotos, Smith-Lemli-Opitz, Moebius, CHARGE association, Joubert, Congenital Sotos, Smith-Lemli-Opitz, Moebius, CHARGE association, Joubert, Congenital Myotonic DystrophyMyotonic Dystrophy
Neurocutaneous syndromesNeurocutaneous syndromes Tuberous sclerosisTuberous sclerosis
Congenital and acquired infectionsCongenital and acquired infections RubellaRubella cytomegaloviruscytomegalovirus
In utero drug exposureIn utero drug exposure Thalidomide, valproic acidThalidomide, valproic acid
Inherited metabolic disordersInherited metabolic disorders PKUPKU Disorders of purine metabolismDisorders of purine metabolism
Miscellaneous, including hypoxic-ischemic encephalopathyMiscellaneous, including hypoxic-ischemic encephalopathy

EpidemiologyEpidemiology
Increase in prevalenceIncrease in prevalence 1966-1991: 4.4 cases per 10,0001966-1991: 4.4 cases per 10,000 1992-2001: 12.7 cases per 10,0001992-2001: 12.7 cases per 10,000
Factors that complicate interpretationFactors that complicate interpretation changes in diagnostic practicechanges in diagnostic practice Increased awareness of the disorderIncreased awareness of the disorder earlier diagnosisearlier diagnosis educational diagnoseseducational diagnoses

EpidemiologyEpidemiology
ImmunizationsImmunizations What are the concerns regarding Thimerosal What are the concerns regarding Thimerosal
exposure?exposure?

EpidemiologyEpidemiology
02 0
4 0
6 0
8 01 0 0
1 2 0
1 4 0
1 6 0
1 8 02 0 0
D T P H i b H e p B T o t a l E x p o s u r e
EpidemiologyEpidemiology
Theoretical and laboratory plausibilityTheoretical and laboratory plausibility Suggested similarities between Hg toxicity Suggested similarities between Hg toxicity
and autismand autism In-vitro biochemical effects of HgIn-vitro biochemical effects of Hg Studies in different strains of miceStudies in different strains of mice

Vaccine TheoryVaccine TheoryOnset of autismOnset of autism Early onset with progressionEarly onset with progression 30% have history o regression 12-24 months – No 30% have history o regression 12-24 months – No
established definition ~ MMR recommendation 12-established definition ~ MMR recommendation 12-15 months15 months
1998 Wakefield (Lancet, 1998) small 1998 Wakefield (Lancet, 1998) small circumstantial case series of MMR circumstantial case series of MMR association with GI symptoms, autistic association with GI symptoms, autistic regression – article later retracted by Lancetregression – article later retracted by LancetCalifornia Dept of Developmental services California Dept of Developmental services 273% increase in autism 1987-1998 273% increase in autism 1987-1998 Well after 1971 introduction of MMRWell after 1971 introduction of MMR Study also confirms also not 2o change in DSM Study also confirms also not 2o change in DSM
criteriacriteria

Thimerosal TheoriesThimerosal Theories
Thimerosal (ethylmercury) used since 1930s in Thimerosal (ethylmercury) used since 1930s in vaccinevaccine Prior to 2001 vaccines exposed children to >EPA Prior to 2001 vaccines exposed children to >EPA
recommended ethylmercury limitsrecommended ethylmercury limits Since 3/01 all vaccines available thimerosal freeSince 3/01 all vaccines available thimerosal free
Prenatal exposure to Prenatal exposure to methylmethylmercury associated mercury associated with neurodevelopmental abnormalitieswith neurodevelopmental abnormalitiesSimilarities but differences between signs of Similarities but differences between signs of mercury poisoning and autismmercury poisoning and autismRapid excretion and low blood levels of Rapid excretion and low blood levels of ethylmercuryethylmercuryNIH and CDC studies showed no relationship NIH and CDC studies showed no relationship with thimerosalwith thimerosal

EpidemiologyEpidemiology
EPA exposure guidelines are for methylmercuryEPA exposure guidelines are for methylmercury Low dose exposure primarily from fish or whale Low dose exposure primarily from fish or whale
consumptionconsumption
Thimerosal contains ethylmercuryThimerosal contains ethylmercury Few studies of exposure in humansFew studies of exposure in humans
Applicability of methylmercury guidelines to Applicability of methylmercury guidelines to ethylmercury exposure?ethylmercury exposure? Recent pharmacokinetic studies suggest that Recent pharmacokinetic studies suggest that
ethylmercury has a much shorter half-life than ethylmercury has a much shorter half-life than methylmercurymethylmercury

EpidemiologyEpidemiology
00 . 5
11 . 5
22 . 5
33 . 5
44 . 5
5
1 9 7 0 1 9 7 5 1 9 8 0 1 9 8 5 1 9 9 0 1 9 9 5 2 0 0 0
a g e s 2 - 4a g e s 5 - 6a g e s 7 - 9
Inci
denc
e pe
r 10
,000
per
sons
Removal of thimerosal-containing vaccines in 1992 in Denmark

IOM ReportIOM Report
2004 IOM2004 IOM ““Evidence favors rejection of causal Evidence favors rejection of causal
relationship”relationship”Consistent body of epidemiologic evidence Consistent body of epidemiologic evidence shows no associationshows no associationOriginal Wakefield case series uninformative Original Wakefield case series uninformative regarding causalityregarding causalityBiologic models linking MMR and ASD are Biologic models linking MMR and ASD are fragmentaryfragmentaryNo relevant animal models linking MMR and No relevant animal models linking MMR and ASDASD

IOM ReportIOM Report
“…“…conclusion does not exclude possibility conclusion does not exclude possibility that MMR could contribute to ASD in a that MMR could contribute to ASD in a small number of children, because small number of children, because epidemiologic evidence lacks the epidemiologic evidence lacks the precision to say this…”precision to say this…”

Is there an epidemic?Is there an epidemic?
More cases than in the past? YESMore cases than in the past? YES
Is the increase attributable to change in Is the increase attributable to change in real risk?real risk? Can’t Can’t rule outrule out changes in diagnosis or that we changes in diagnosis or that we
are diagnosing “better”are diagnosing “better” Can’t Can’t rule inrule in increases in real risk because increases in real risk because
etiology and all the risk factors are not knownetiology and all the risk factors are not known

Genetic Influences in AutismGenetic Influences in Autism
Epidemiological, twin and family data Epidemiological, twin and family data together suggest that the vast majority of together suggest that the vast majority of cases of ASD arise on the basis of a cases of ASD arise on the basis of a complex genetic predispositioncomplex genetic predisposition

Treatment and Treatment and InterventionIntervention

Treatment and InterventionTreatment and InterventionApplied Behavior Analysis (ABA) TherapyApplied Behavior Analysis (ABA) Therapy Most commonly studied treatmentMost commonly studied treatment What is it?What is it?
Uses principles of reinforcementUses principles of reinforcement
Variety of behavioral approaches (e.g., Discrete Variety of behavioral approaches (e.g., Discrete trial, pivotal response training, verbal behavior, trial, pivotal response training, verbal behavior, incidental teaching) to teach social interaction incidental teaching) to teach social interaction skills/ communication.skills/ communication.
25-40 hours a week25-40 hours a week
In-home versus center-basedIn-home versus center-based
Prerequisites for benefit (imitation, joint attention) Prerequisites for benefit (imitation, joint attention) and when see most benefitand when see most benefit

Treatment and InterventionTreatment and InterventionFirst randomized control trial of ABA First randomized control trial of ABA published in 2000 (Smith, Groen, & published in 2000 (Smith, Groen, & Wynn)Wynn) Children who received ABA made greater Children who received ABA made greater
gains than children in parent training gains than children in parent training control groupcontrol group
None changed diagnosisNone changed diagnosis Gains not dramaticGains not dramatic Children with PDD, NOS and higher IQ’s Children with PDD, NOS and higher IQ’s
made greater gainsmade greater gains

Treatment and InterventionTreatment and Intervention
Other studies of ABAOther studies of ABA Age at start of treatment may be a factor, but Age at start of treatment may be a factor, but
response to treatment is not limited to very response to treatment is not limited to very young preschool childrenyoung preschool children
Comparing newer ABA studies to Lovaas Comparing newer ABA studies to Lovaas studiesstudies fewer hours, therapists with less training, fewer hours, therapists with less training,
different IQ’s.different IQ’s.
Educational InterventionsEducational InterventionsDirect social skills instruction with opportunities Direct social skills instruction with opportunities to practice skills with typically developing peers to practice skills with typically developing peers (WITH SUPPORT)(WITH SUPPORT)
Social communication skillsSocial communication skills
Play skillsPlay skills
Affect trainingAffect training
Social storiesSocial stories
Peer tutoringPeer tutoring
**Should try and choose outcomes that are **Should try and choose outcomes that are MEASURABLE in order to monitor progress**MEASURABLE in order to monitor progress**

Educational InterventionsEducational Interventions
PredictabilityPredictability
Use of visuals to supplement Use of visuals to supplement communication as neededcommunication as needed
Functional Behavioral AssessmentFunctional Behavioral Assessment

Additional therapiesAdditional therapies
Speech/ Language therapySpeech/ Language therapy Should have experience working with children Should have experience working with children
with ASD. with ASD. Behavioral approach (e.g., verbal behavior) Behavioral approach (e.g., verbal behavior)
often most effective.often most effective. Social communicationSocial communication
Additional TherapiesAdditional Therapies
Occupational therapyOccupational therapy Sensory Integration – not supported by Sensory Integration – not supported by
research, but some anecdotal evidenceresearch, but some anecdotal evidence Motor coordinationMotor coordination
Relationship Development Relationship Development Intervention (RDI)Intervention (RDI)
Sounds promising, but not yet supported Sounds promising, but not yet supported by independent research.by independent research.

Supplements/ DietSupplements/ Diet
Some anecdotal evidence, but not Some anecdotal evidence, but not supported by research.supported by research. For families who want to try this, we try to help For families who want to try this, we try to help
them approach dietary changes/ supplements them approach dietary changes/ supplements in a scientific way.in a scientific way.
Treatment and InterventionTreatment and Intervention
No single approach is best for all No single approach is best for all individuals or even across time for the individuals or even across time for the same individual with ASDsame individual with ASD
Treatment and InterventionTreatment and Intervention
Greater recognition of the interplay Greater recognition of the interplay between different treatmentsbetween different treatments social storiessocial stories written cueswritten cues modifications of expansions of behavioral modifications of expansions of behavioral
treatmentstreatmentsincidental teachingincidental teaching
Pivotal Response InterventionPivotal Response Intervention
TEACCHTEACCH
Treatment and InterventionTreatment and Intervention
Studies on factors leading to successful Studies on factors leading to successful treatmenttreatment child’s engagement in taskschild’s engagement in tasks generalization has to be specifically generalization has to be specifically
addressedaddressed

Treatment and InterventionTreatment and Intervention
Communication interventionsCommunication interventions parent behavior parent behavior
Social skillsSocial skills limitations of full inclusion without limitations of full inclusion without
systematic or skills supportsystematic or skills support combined approaches (social stories, combined approaches (social stories,
problem solving, affect training, multi-site problem solving, affect training, multi-site support)support)

Treatment and InterventionTreatment and Intervention
Social skillsSocial skills Videotapes to help with complex play themes, Videotapes to help with complex play themes,
transitions, and play with siblingstransitions, and play with siblings Attempts to teach “theory of mind” improved Attempts to teach “theory of mind” improved
children’s ability to do tasks within teaching children’s ability to do tasks within teaching environment, but did not generalize.environment, but did not generalize.

Treatment and InterventionTreatment and Intervention
Pharmacological TreatmentsPharmacological Treatments Over past decade, shift from antipsychotic Over past decade, shift from antipsychotic
medications to the newer, atypical, medications to the newer, atypical, antipsychotics as well as to the use of the antipsychotics as well as to the use of the serotonin-blocking agentsserotonin-blocking agents

Treatment and InterventionTreatment and Intervention
Pharmacological treatmentsPharmacological treatments Atypical antipsychotics have more favorable Atypical antipsychotics have more favorable
side-effect profilesside-effect profiles Target symptomsTarget symptoms
self-injury, severe agitation or stereotyped self-injury, severe agitation or stereotyped movements, severe behavior problemsmovements, severe behavior problems
Decreased risk of extra pyramidal side effectsDecreased risk of extra pyramidal side effects
Treatment and InterventionTreatment and Intervention
Most extensive body of work has Most extensive body of work has development on risperidone development on risperidone significant benefitssignificant benefits
SSRI’sSSRI’s May be helpful with repetitive/ obsessive May be helpful with repetitive/ obsessive
behaviors, difficulties dealing with changebehaviors, difficulties dealing with change Not as well studiedNot as well studied Some support for fluoxetine (reduced levels Some support for fluoxetine (reduced levels
of compulsive behaviors and aggression)of compulsive behaviors and aggression)
Treatment and InterventionTreatment and Intervention
Stimulant medicationsStimulant medications Some suggestion that higher functioning Some suggestion that higher functioning
children may be more likely to respond children may be more likely to respond positivelypositively
Other ConsiderationsOther Considerations
InsuranceInsurance
PCA servicesPCA services
WaiverWaiver

Other ConsiderationsOther Considerations
Community resourcesCommunity resources Support groupsSupport groups WorkshopsWorkshops BooksBooks
Community ResourcesCommunity Resources
Support Groups/ Resources/ EducationSupport Groups/ Resources/ Education Autism Society of Minnesota (Autism Society of Minnesota (www.ausm.org)) Autism Speaks (Autism Speaks (www.autismspeaks.org) )
Multidisciplinary Team DiagnosisMultidisciplinary Team Diagnosis University of Minnesota Autism Spectrum University of Minnesota Autism Spectrum
Disorders Program (612-625-3617)Disorders Program (612-625-3617) Alexander Center (952-993-2498)Alexander Center (952-993-2498) Mayo Clinic (507-538-3270)Mayo Clinic (507-538-3270)
Community ResourcesCommunity Resources
Providers of in-home ABA Therapy (Twin Providers of in-home ABA Therapy (Twin Cities Area)Cities Area) Minnesota Early Autism Project (763-493-7935)Minnesota Early Autism Project (763-493-7935) Behavioral Dimensions (Behavioral Dimensions (
www.behavioraldimensions.com) ) Lovaas Institute (612-925-8365)Lovaas Institute (612-925-8365) Minnesota Autism Center (Minnesota Autism Center (www.mnautism.org) )
– also branches in St. Cloud, Rochester and – also branches in St. Cloud, Rochester and DuluthDuluth

Other ConsiderationsOther Considerations
Providers of Center-based ABA Therapy Providers of Center-based ABA Therapy (Twin Cities Area)(Twin Cities Area)
• Holland CenterHolland Center
• Partners In ExcellencePartners In Excellence
• Lazarus ProjectLazarus Project

Robin Rumsey, Ph.D., L.P.Robin Rumsey, Ph.D., L.P. [email protected]@umn.edu