Embed Size (px)
Citation preview
Atypical Right Atrial Flutter PatternsYanfei Yang, MD; Jie Cheng, MD, PhD; Andy Bochoeyer, MD; Mohamed H. Hamdan, MD;
Robert C. Kowal, MD, PhD; Richard Page, MD; Randall J. Lee, MD, PhD; Paul R. Steiner, MD;Leslie A. Saxon, MD; Michael D. Lesh, MD; Gunnard W. Modin, PhD; Melvin M. Scheinman, MD
Background—The purpose of our study was to define the incidence and mechanisms of atypical right atrial flutter.Methods and Results—A total of 28 (8%) of 372 consecutive patients with atrial flutter (AFL) had 36 episodes of sustained
atypical right AFL. Among 24 (67%) of 36 episodes of lower loop reentry (LLR), 13 (54%) of 24 episodes had earlybreakthrough at the lower lateral tricuspid annulus, whereas 11 (46%) of 24 episodes had early breakthrough at the highlateral tricuspid annulus, and 9 (38%) of 24 episodes showed multiple annular breaks. Bidirectional isthmus blockresulted in elimination of LLR. A pattern of posterior breakthrough from the eustachian ridge to the septum wasobserved in 4 (14%) of 28 patients. Upper loop reentry was observed in 8 (22%) of 36 episodes and was defined asshowing a clockwise orientation with early annular break and wave-front collision over the isthmus. Two patients hadatypical right AFL around low voltage areas (“scars”) in the posterolateral right atrium.
Conclusions—Atypical right AFL is most commonly associated with an isthmus-dependent mechanism (ie, LLR orsubeustachian isthmus breaks). Non–isthmus-dependent circuits include upper loop reentry or scar-related circuits.(Circulation. 2001;103:3092-3098.)
Key Words: electrophysiologyn atrial flutter n catheter ablationn mappingn tachycardia
Spontaneous clockwise (CW) and counterclockwise(CCW) isthmus-dependent atrial flutter (AFL) has been
well described. More recently, other types of isthmus-dependent and non–isthmus-dependent flutter patterns havebeen described.1–10 The purpose of the present study was todefine the incidence and mechanisms of right AFL in a largecohort of patients referred for catheter ablation of AFL.
MethodsA total of 372 consecutive patients with AFL were referred to ourinstitutions for ablation from January 1996 to August 2000. None ofthe patients in the present study had been previously reported.Patients with surgically corrected congenital heart disease wereexcluded from the study. We excluded 328 patients with sole typicalisthmus-dependent flutter and 16 with left AFL, leaving 28 (8%)patients (aged 59613 years) with atypical right AFL for study.Among the 28 patients, 16 (57%) had documented atrial fibrillationand AFL, whereas 12 had AFL alone. Six patients had structuralheart disease, but none had an atriotomy. Almost all antiarrhythmicdrugs had been withdrawn for at least 5 half-lives before the study;however, 6 patients were being treated with amiodarone at the timeof the study.
Informed written consent was obtained for all patients. Recordingswere obtained from a 20-pole electrode catheter along the tricuspidannulus (TA), the coronary sinus (CS), and the anteroseptal region(His bundle region), as previously described.7 Entrainment mapping
was attempted in all patients, and concealed entrainment wasdiagnosed when the difference between tachycardia cycle length(TCL) and postpacing interval was#30 ms, with identical intracar-diac and surface flutter wave morphology. Electroanatomic mappingusing the CARTO Biosense system (Biosense Webster Inc) wasavailable in 4 of the 28 patients.
DefinitionsSustained tachycardia was defined as that lasting$30 seconds.
Early breakthrough during AFL was described as a wave fronttraversing the subeustachian isthmus (SI) and activating the posteriorright atrium (RA) with early annular activation (break), producing 2wave fronts that result in collision along the TA.7
Statistical AnalysisThe difference between flutter TCL for each patient with both typicaland atypical flutter was analyzed by pairedt test. A value ofP,0.05was considered statistically significant.
ResultsWe identified 36 episodes of atypical right AFL in 28 (8%) of372 patients referred for ablation of AFL. Twenty patientshad both typical and atypical flutter, whereas 8 patients hadonly atypical flutter. A total of 32 episodes (89%) of atypicalflutter were sustained, and 26 (81%) of 32 were sufficientlyprolonged to allow for mapping, entrainment pacing, and/or
Received December 20, 2000; revision received April 5, 2001; accepted April 6, 2001.From the Cardiovascular Research Institute and Section of Cardiac Electrophysiology (Y.Y., J.C., A.B., R.J.L., P.R.S., L.A.S., M.D.L., G.W.M.,
M.M.S.), University of California, San Francisco, and the University of Texas Southwestern Medical Center and the Dallas Veterans Affairs MedicalCenter (M.H.H., R.C.K., R.P.), Dallas, Tex.
Presented in abstract form at the 21st Annual Scientific Sessions of North American Society of Pacing and Electrophysiology, Washington, DC, May19, 2000, and published in abstract form (Pacing Clin Electrophysiol.2000;23:579).
Correspondence to Melvin M. Scheinman, MD, Cardiac Electrophysiology, University of California, San Francisco, 500 Parnassus Ave, MU East 4S,Box 1354, San Francisco, CA 94143-1354. E-mail [email protected]
© 2001 American Heart Association, Inc.
Circulation is available at http://www.circulationaha.org
3092
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
ablation. During the studies, 22 (61%) of 36 episodes oc-curred spontaneously and were usually preceded by episodesof typical flutter, whereas 14 episodes were induced bypacing. Twenty (91%) of 22 spontaneous episodes and 12(86%) of 14 pacing-induced episodes were sustained.
Isthmus-Dependent AFL
Lower Loop Reentry TachycardiaA total of 24 of 36 episodes of atypical AFL fit the diagnosticcriteria of lower loop reentry tachycardia (LLR), suggestedby Cheng et al.7 Twenty of the 24 episodes were sustained,and 4 were nonsustained. Fifteen episodes occurred sponta-neously in patients with or without typical flutter, whereas 9occurred after atrial pacing.
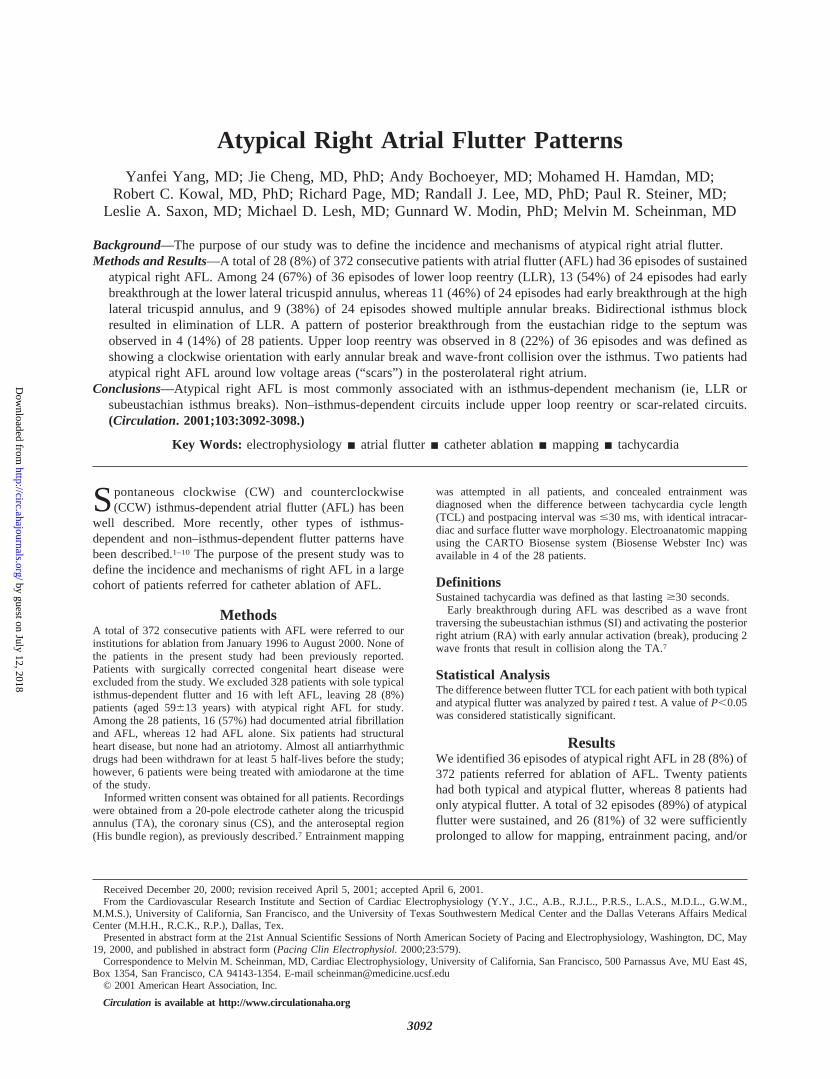
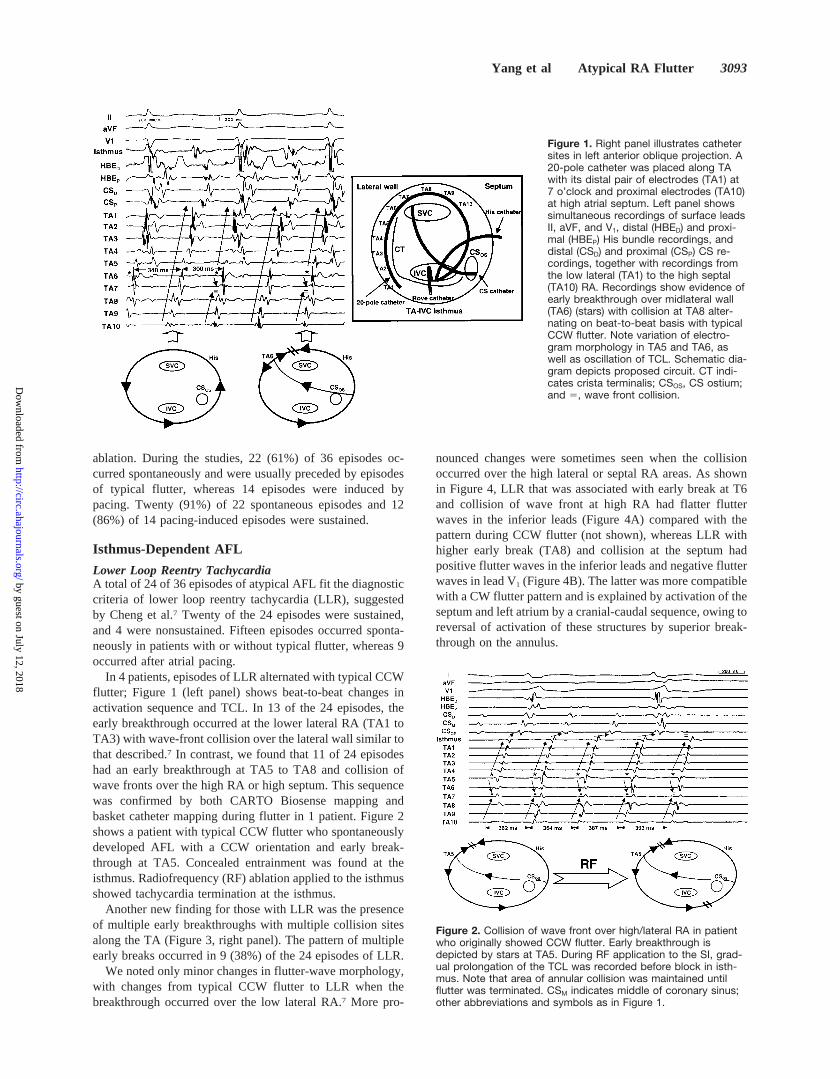
In 4 patients, episodes of LLR alternated with typical CCWflutter; Figure 1 (left panel) shows beat-to-beat changes inactivation sequence and TCL. In 13 of the 24 episodes, theearly breakthrough occurred at the lower lateral RA (TA1 toTA3) with wave-front collision over the lateral wall similar tothat described.7 In contrast, we found that 11 of 24 episodeshad an early breakthrough at TA5 to TA8 and collision ofwave fronts over the high RA or high septum. This sequencewas confirmed by both CARTO Biosense mapping andbasket catheter mapping during flutter in 1 patient. Figure 2shows a patient with typical CCW flutter who spontaneouslydeveloped AFL with a CCW orientation and early break-through at TA5. Concealed entrainment was found at theisthmus. Radiofrequency (RF) ablation applied to the isthmusshowed tachycardia termination at the isthmus.
Another new finding for those with LLR was the presenceof multiple early breakthroughs with multiple collision sitesalong the TA (Figure 3, right panel). The pattern of multipleearly breaks occurred in 9 (38%) of the 24 episodes of LLR.
We noted only minor changes in flutter-wave morphology,with changes from typical CCW flutter to LLR when thebreakthrough occurred over the low lateral RA.7 More pro-
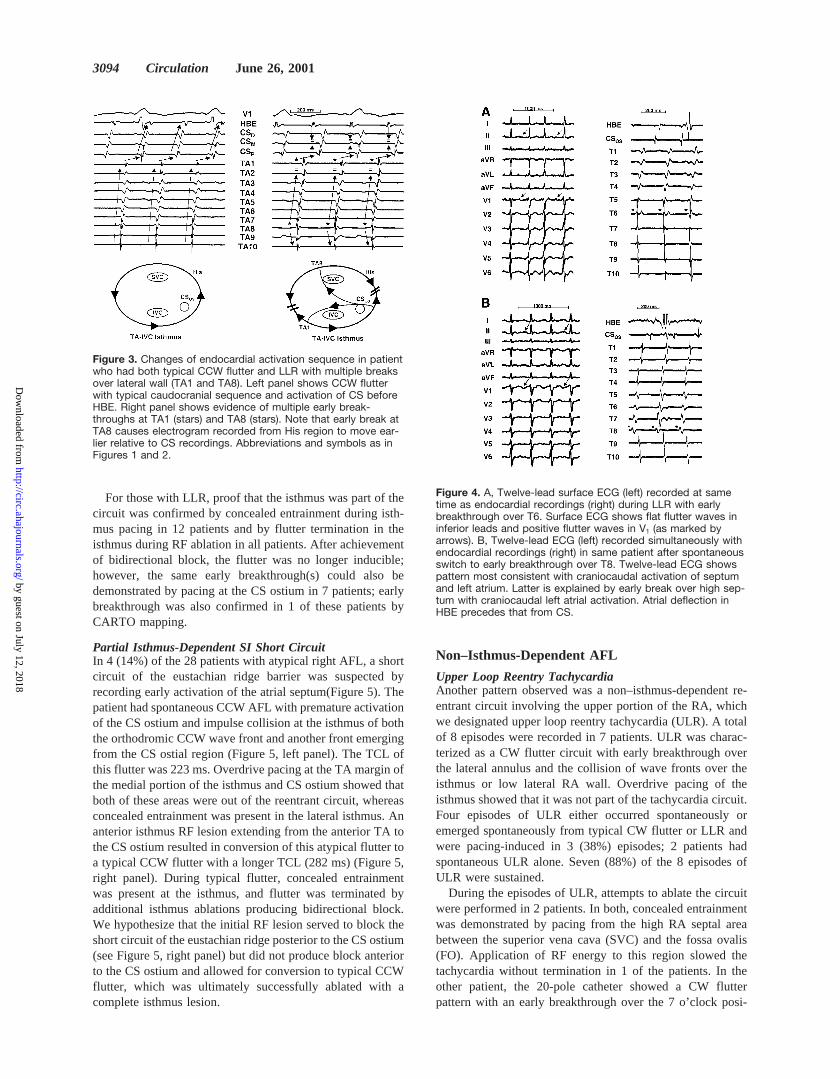
nounced changes were sometimes seen when the collisionoccurred over the high lateral or septal RA areas. As shownin Figure 4, LLR that was associated with early break at T6and collision of wave front at high RA had flatter flutterwaves in the inferior leads (Figure 4A) compared with thepattern during CCW flutter (not shown), whereas LLR withhigher early break (TA8) and collision at the septum hadpositive flutter waves in the inferior leads and negative flutterwaves in lead V1 (Figure 4B). The latter was more compatiblewith a CW flutter pattern and is explained by activation of theseptum and left atrium by a cranial-caudal sequence, owing toreversal of activation of these structures by superior break-through on the annulus.
Figure 1. Right panel illustrates cathetersites in left anterior oblique projection. A20-pole catheter was placed along TAwith its distal pair of electrodes (TA1) at7 o’clock and proximal electrodes (TA10)at high atrial septum. Left panel showssimultaneous recordings of surface leadsII, aVF, and V1, distal (HBED) and proxi-mal (HBEP) His bundle recordings, anddistal (CSD) and proximal (CSP) CS re-cordings, together with recordings fromthe low lateral (TA1) to the high septal(TA10) RA. Recordings show evidence ofearly breakthrough over midlateral wall(TA6) (stars) with collision at TA8 alter-nating on beat-to-beat basis with typicalCCW flutter. Note variation of electro-gram morphology in TA5 and TA6, aswell as oscillation of TCL. Schematic dia-gram depicts proposed circuit. CT indi-cates crista terminalis; CSOS, CS ostium;and 5, wave front collision.
Figure 2. Collision of wave front over high/lateral RA in patientwho originally showed CCW flutter. Early breakthrough isdepicted by stars at TA5. During RF application to the SI, grad-ual prolongation of the TCL was recorded before block in isth-mus. Note that area of annular collision was maintained untilflutter was terminated. CSM indicates middle of coronary sinus;other abbreviations and symbols as in Figure 1.
Yang et al Atypical RA Flutter 3093
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
For those with LLR, proof that the isthmus was part of thecircuit was confirmed by concealed entrainment during isth-mus pacing in 12 patients and by flutter termination in theisthmus during RF ablation in all patients. After achievementof bidirectional block, the flutter was no longer inducible;however, the same early breakthrough(s) could also bedemonstrated by pacing at the CS ostium in 7 patients; earlybreakthrough was also confirmed in 1 of these patients byCARTO mapping.
Partial Isthmus-Dependent SI Short CircuitIn 4 (14%) of the 28 patients with atypical right AFL, a shortcircuit of the eustachian ridge barrier was suspected byrecording early activation of the atrial septum(Figure 5). Thepatient had spontaneous CCW AFL with premature activationof the CS ostium and impulse collision at the isthmus of boththe orthodromic CCW wave front and another front emergingfrom the CS ostial region (Figure 5, left panel). The TCL ofthis flutter was 223 ms. Overdrive pacing at the TA margin ofthe medial portion of the isthmus and CS ostium showed thatboth of these areas were out of the reentrant circuit, whereasconcealed entrainment was present in the lateral isthmus. Ananterior isthmus RF lesion extending from the anterior TA tothe CS ostium resulted in conversion of this atypical flutter toa typical CCW flutter with a longer TCL (282 ms) (Figure 5,right panel). During typical flutter, concealed entrainmentwas present at the isthmus, and flutter was terminated byadditional isthmus ablations producing bidirectional block.We hypothesize that the initial RF lesion served to block theshort circuit of the eustachian ridge posterior to the CS ostium(see Figure 5, right panel) but did not produce block anteriorto the CS ostium and allowed for conversion to typical CCWflutter, which was ultimately successfully ablated with acomplete isthmus lesion.
Non–Isthmus-Dependent AFL
Upper Loop Reentry TachycardiaAnother pattern observed was a non–isthmus-dependent re-entrant circuit involving the upper portion of the RA, whichwe designated upper loop reentry tachycardia (ULR). A totalof 8 episodes were recorded in 7 patients. ULR was charac-terized as a CW flutter circuit with early breakthrough overthe lateral annulus and the collision of wave fronts over theisthmus or low lateral RA wall. Overdrive pacing of theisthmus showed that it was not part of the tachycardia circuit.Four episodes of ULR either occurred spontaneously oremerged spontaneously from typical CW flutter or LLR andwere pacing-induced in 3 (38%) episodes; 2 patients hadspontaneous ULR alone. Seven (88%) of the 8 episodes ofULR were sustained.
During the episodes of ULR, attempts to ablate the circuitwere performed in 2 patients. In both, concealed entrainmentwas demonstrated by pacing from the high RA septal areabetween the superior vena cava (SVC) and the fossa ovalis(FO). Application of RF energy to this region slowed thetachycardia without termination in 1 of the patients. In theother patient, the 20-pole catheter showed a CW flutterpattern with an early breakthrough over the 7 o’clock posi-
Figure 3. Changes of endocardial activation sequence in patientwho had both typical CCW flutter and LLR with multiple breaksover lateral wall (TA1 and TA8). Left panel shows CCW flutterwith typical caudocranial sequence and activation of CS beforeHBE. Right panel shows evidence of multiple early break-throughs at TA1 (stars) and TA8 (stars). Note that early break atTA8 causes electrogram recorded from His region to move ear-lier relative to CS recordings. Abbreviations and symbols as inFigures 1 and 2.
Figure 4. A, Twelve-lead surface ECG (left) recorded at sametime as endocardial recordings (right) during LLR with earlybreakthrough over T6. Surface ECG shows flat flutter waves ininferior leads and positive flutter waves in V1 (as marked byarrows). B, Twelve-lead ECG (left) recorded simultaneously withendocardial recordings (right) in same patient after spontaneousswitch to early breakthrough over T8. Twelve-lead ECG showspattern most consistent with craniocaudal activation of septumand left atrium. Latter is explained by early break over high sep-tum with craniocaudal left atrial activation. Atrial deflection inHBE precedes that from CS.
3094 Circulation June 26, 2001
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

tion. Concealed entrainment was also documented in the areabetween the inferior vena cava (IVC) and FO (Figure 6A). Inthe same patient, double potentials were shown as the 20-polecatheter was moved to the septum (Figure 6B). Ablativelesions applied from the FO to the orifice of IVC resulted intachycardia slowing and then termination. We suspect that thetachycardia circuit for ULR, at least in some patients,involves a reentrant wave around the region of the FO (Figure6C). Electroanatomic mapping was not available for thesepatients.
In 3 of 20 patients with CCW-LLR, spontaneous isthmusblock occurred and resulted in a pattern of CW flutter withULR (Figure 7). This arrhythmia was associated with impulsecollision over the isthmus.
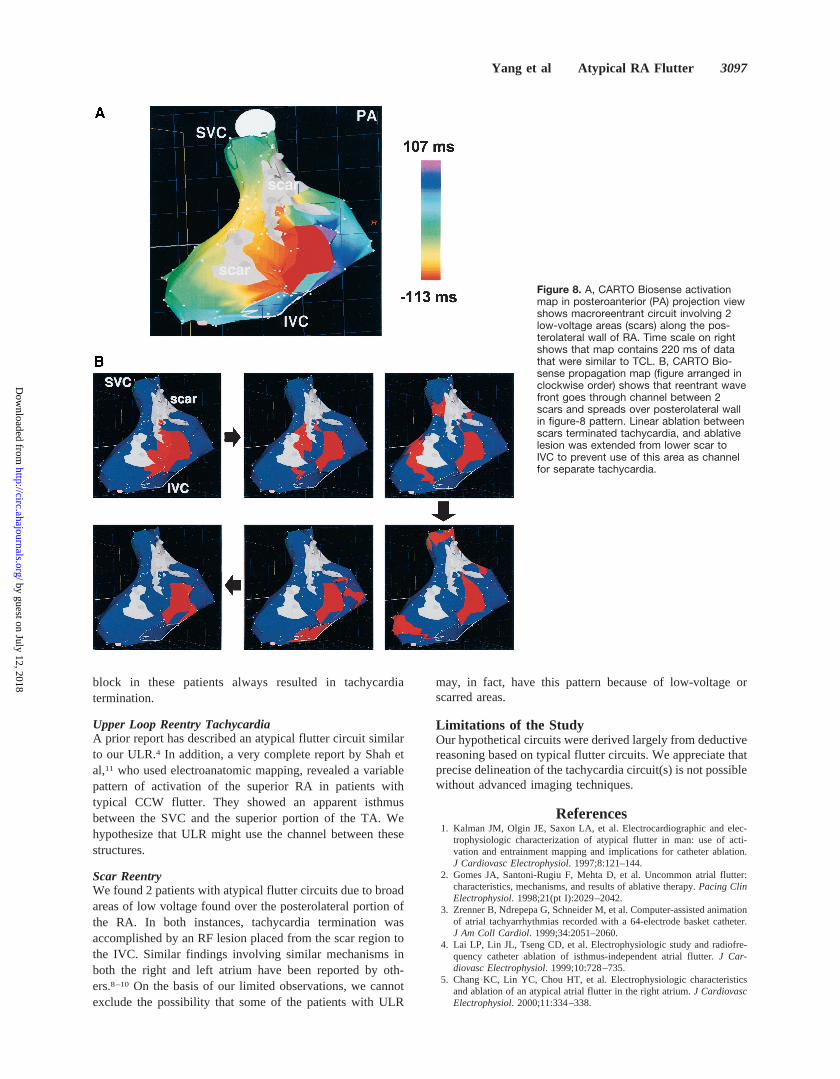
Right Atrial Scar ReentryTwo patients without prior atriotomy had evidence of reentryaround large low-voltage regions of the posterolateral RA, asdetermined by CARTO Biosense mapping. Both patients hadspontaneous episodes of typical CW or CCW as well asatypical flutter. Ablation at the isthmus abolished typicalflutter, but the atypical flutter persisted. Entrainment mappingat multiple sites showed evidence of manifest entrainment atthe midseptum, CS ostium, and SI. Concealed entrainmentwas present only over the superior-posterolateral and inferi-or-posterolateral sections of the RA. Voltage mapping con-firmed large areas of low voltage (,0.25 mV) over theposterolateral RA. Propagation and activation mappingshowed a macroreentrant circuit between the low-voltage
areas and the vena cava (Figure 8). Linear ablation from the“scar” to the IVC terminated the flutter.
Changes of Flutter TCLIn the present study, 14 patients had both typical CCWflutter and LLR; 4 patients had both typical CW flutter andULR; 1 patient had typical CCW flutter and ULR; and 1
Figure 5. Left panel shows CCW pattern over lateral RA freewall. Of interest, however, is early breakthrough over CSOS (CSP)with impulse collision in isthmus from wave fronts generatedfrom CSP and wave front collision (5) between isthmus andTA1. Split potentials recorded at isthmus might indicate that thisregion acts as a pivot point for circulating wave front depictedin schematic diagram. Right panel shows that after single RFapplication over anterior isthmus region, flutter TCL increased(282 ms) and was associated with typical CCW pattern withmarked conduction delay in isthmus. We interpret this finding asdevelopment of block over posterior isthmus breakthrough site(see dark bar in schematic diagram) with development of CCWflutter circuit. Additional RF application over isthmus resulted intermination of tachycardia, and no tachycardia could be inducedin response to rapid atrial overdrive pacing. Abbreviations as inFigures 1 and 2.
Figure 6. A, In patient with ULR, clockwise flutter patternwith early breakthrough at TA4 (stars) was recorded from20-pole catheter placed along TA. Overdrive pacing (S1-S1200 ms) in region between FO and IVC shows postpacinginterval (PPI) equal to TCL (230 ms) and proves that thisregion is in circuit. B, In same patient, double potentials wererecorded from 20-pole catheter just posterior to FO, asshown on right (right anterior oblique projection view).Sequence of these potentials (shown on left) suggests clock-wise reentrant circuit around this area (functional line ofblock). C, In same patient, 20-pole catheter was repositionedacross SI so that distal electrodes were positioned at 5o’clock position of TA and proximal electrodes were posi-tioned at 7 o’clock position. Collision at isthmus (5) is appar-ently due to opposing wave fronts converging over isthmus(left). Proposed tachycardia circuit is displayed on right.Abbreviations as in Figure 1.
Yang et al Atypical RA Flutter 3095
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

patient had typical CCW and CW flutter, as well as LLRand ULR. For the patients with both CCW and LLR, therewas a statistically significant decrease in TCL comparingLLR (241646 ms) with CCW (253645 ms) (P50.005).Similarly, compared with those with CW flutter (259639ms), those with ULR had a shorter TCL (250636 ms)(P50.029). These results are best explained by the shortercircuits of the atypical flutter patterns compared with thetypical forms.
DiscussionMain FindingsIn an unselected group of patients referred for ablation ofAFL, we found that 8% had atypical right AFL patterns.These episodes generally (61%) occurred spontaneously frompreexisting typical flutter patterns and tended to be sustained(89%). Our results indicated that these atypical patterns werea reflection of independent stable circuits and not transientpatterns induced by rapid atrial pacing.
Patterns of LLRAn earlier study from our laboratory defined the characteris-tics of LLR.7 In that study, early breakthrough over the TAoccurred over the low lateral RA. Our present study confirmsand extends these observations. For example, we found that$1 annular break could occur at the lateral or anterolateralregions of the annulus. Proof that these circuits were isthmusdependent was shown by concealed entrainment and/or re-sponse to isthmus ablation. The observed patterns of atypicalright AFL could not be artifacts due to spontaneous changesin catheter position because the surface ECG frequently
showed changes in unison with changes in the endocardialrecordings(Figures 3, 4B, and 7).
SI Short CircuitAnother novel finding was demonstration of circuits withearly activation of the CS region. In this circuit, a typicalCCW wave front negotiated the lateral portion of the isthmusand skirted posterior to the CS ostium and the septum. Onepossible explanation is the presence of a pectinate muscleband from the crista effectively separating the isthmus intoanterior and posterior compartments. In all 4 patients, bidi-rectional isthmus block induced by RF lesion terminated thetachycardia.
Upper Loop Reentry TachycardiaULR is interpreted as the “converse” of LLR with a CWcircuit and break over the lateral or anterolateral annulus withimpulse collision in the isthmus. It should be emphasized thatelectroanatomic mapping studies were not available duringULR; hence, the precise confines of the circuit are not clear,although detailed entrainment mapping in 2 of these patientsshowed concealed entrainment at the posterior RA septalregion between the FO and either the SVC or the IVC. Also,supportive of our schema for ULR is the finding of sponta-neous conversion of either typical CW flutter or LLR to ULR(Figure 7). In 1 patient with LLR and multiple breakthroughs,conduction block over the isthmus was associated with thestart of an ULR loop.
Previous Studies
Lower Loop ReentryOur hypothesis explaining LLR has been verified by anumber of other authors.,3,5,11–15The finding of collision sitesalong the lateral or superior TA as well as LLR with multiplebreaks has actually been illustrated in a previous study(Figure 1 of Friedman et al15) Moreover, this important studyshowed that a posterior (intercaval) functional line of blockformed the posterior barrier for typical flutter circuits whiletransverse conduction over the crista terminalis was present.They hypothesized that the flutter circuit was a result ofcompeting wave fronts. Because the intercaval line was ofvariable length, activation of the posterior wall with penetra-tion of the crista allowed for expression of different collisionsites over the annulus. This formulation well explains ourobservations.
SI Short CircuitPrior studies by Olgin et al16 and Nakagawa et al17 showedthat breakthrough over the eustachian ridge posterior to theCS ostium may be observed in'25% to 50% of patients withtypical forms of flutter. In these reports, there was almostsimultaneous activation of the septum by wave fronts advanc-ing both anterior and posterior to the CS. In the patientsdescribed in the present study, the only way to explain theproposed circuit is to postulate that the wave front advancinganterior to the CS is delayed sufficiently, allowing forcollision with a return impulse from the CS that was previ-ously conducted via the posteriorly directed wave front(Figure 5). It should be emphasized that bidirectional isthmus
Figure 7. First 4 beats show evidence of LLR with breakthroughat TA1 and TA8. Evidence that LLR is “driver” is shown byincrease in TCL from isthmus, CS, and TA1 to TA8 as conduc-tion time through isthmus increases (dashed line from TA1 toCSOS). Septum is captured from TA8 breakthrough and is asso-ciated with less change in TCL compared with TA1 to TA8. Thelatter is interpreted as being due to early breakthrough overTA8, producing conduction slowing over upper septum. Notenear simultaneous activation of HBE and CSOS during those first4 beats. After spontaneous conduction block in isthmus (afterbeat 4), HBE electrogram clearly precedes that from CS, andpoint of collision moves to area of proximal isthmus. Schematicdiagram below beats 5 and 6 shows ULR pattern with same 2early breakthrough sites. Abbreviations and symbols as in Fig-ures 1 and 2.
3096 Circulation June 26, 2001
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
block in these patients always resulted in tachycardiatermination.
Upper Loop Reentry TachycardiaA prior report has described an atypical flutter circuit similarto our ULR.4 In addition, a very complete report by Shah etal,11 who used electroanatomic mapping, revealed a variablepattern of activation of the superior RA in patients withtypical CCW flutter. They showed an apparent isthmusbetween the SVC and the superior portion of the TA. Wehypothesize that ULR might use the channel between thesestructures.
Scar ReentryWe found 2 patients with atypical flutter circuits due to broadareas of low voltage found over the posterolateral portion ofthe RA. In both instances, tachycardia termination wasaccomplished by an RF lesion placed from the scar region tothe IVC. Similar findings involving similar mechanisms inboth the right and left atrium have been reported by oth-ers.8–10 On the basis of our limited observations, we cannotexclude the possibility that some of the patients with ULR
may, in fact, have this pattern because of low-voltage orscarred areas.
Limitations of the StudyOur hypothetical circuits were derived largely from deductivereasoning based on typical flutter circuits. We appreciate thatprecise delineation of the tachycardia circuit(s) is not possiblewithout advanced imaging techniques.
References1. Kalman JM, Olgin JE, Saxon LA, et al. Electrocardiographic and elec-
trophysiologic characterization of atypical flutter in man: use of acti-vation and entrainment mapping and implications for catheter ablation.J Cardiovasc Electrophysiol. 1997;8:121–144.
2. Gomes JA, Santoni-Rugiu F, Mehta D, et al. Uncommon atrial flutter:characteristics, mechanisms, and results of ablative therapy.Pacing ClinElectrophysiol. 1998;21(pt I):2029–2042.
3. Zrenner B, Ndrepepa G, Schneider M, et al. Computer-assisted animationof atrial tachyarrhythmias recorded with a 64-electrode basket catheter.J Am Coll Cardiol. 1999;34:2051–2060.
4. Lai LP, Lin JL, Tseng CD, et al. Electrophysiologic study and radiofre-quency catheter ablation of isthmus-independent atrial flutter.J Car-diovasc Electrophysiol. 1999;10:728–735.
5. Chang KC, Lin YC, Chou HT, et al. Electrophysiologic characteristicsand ablation of an atypical atrial flutter in the right atrium.J CardiovascElectrophysiol. 2000;11:334–338.
Figure 8. A, CARTO Biosense activationmap in posteroanterior (PA) projection viewshows macroreentrant circuit involving 2low-voltage areas (scars) along the pos-terolateral wall of RA. Time scale on rightshows that map contains 220 ms of datathat were similar to TCL. B, CARTO Bio-sense propagation map (figure arranged inclockwise order) shows that reentrant wavefront goes through channel between 2scars and spreads over posterolateral wallin figure-8 pattern. Linear ablation betweenscars terminated tachycardia, and ablativelesion was extended from lower scar toIVC to prevent use of this area as channelfor separate tachycardia.
Yang et al Atypical RA Flutter 3097
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

6. Cheng J, Scheinman MM. Acceleration of typical atrial flutter due todouble-wave reentry induced by programmed electrical stimulation.Cir-culation. 1998;97:1589–1596.
7. Cheng J, Cabeen WR, Scheinman MM. Right atrial flutter due to lowerloop reentry: mechanism and anatomic substrates.Circulation. 1999;99:1700–1705.
8. Kall JG, Rubenstein DS, Kopp DE, et al. Atypical atrial flutter originatingin the right atrial free wall.Circulation. 2000;101:270–279.
9. Nakagawa H, Shah N, Matsudaira K, et al. Characterization of reentrantcircuit in macroreentrant right atrial tachycardia after surgical repair ofcongenital heart disease: isolated channels between scars allow “focal”ablation.Circulation. 2001;103:699–709.
10. Bogun F, Bender B, Li YG, et al. Ablation of atypical atrial flutter guidedby the use of concealed entrainment in patients without prior cardiacsurgery.J Cardiovasc Electrophysiol. 2000;11:136–145.
11. Shah DC, Jais P, Haissaguerre M, et al. Three-dimensional mapping ofthe common atrial flutter circuit in the right atrium.Circulation. 1997;96:3904–3912.
12. Tai CT, Chen SA, Chen YJ, et al. Conduction properties of the cristaterminalis in patients with typical atrial flutter: basis for a line ofblock in the reentrant circuit.J Cardiovasc Electrophysiol. 1998;9:811–819.
13. Arenal A, Almendral J, Alday JM, et al. Rate-dependent conduction blockof the crista terminalis in patients with typical atrial flutter: influence onevaluation of cavotricuspid isthmus conduction block.Circulation. 1999;99:2771–2778.
14. Schumacher B, Jung W, Schmidt H, et al. Transverse conduction capa-bilities of the crista terminalis in patients with atrial flutter and atrialfibrillation. J Am Coll Cardiol. 1999;34:363–373.
15. Friedman PA, Luria D, Fenton AM, et al. Global right atrial mappingof human atrial flutter: the presence of posteromedial (sinus venosaregion) functional block and double potentials: a study in biplanefluoroscopy and intracardiac echocardiography.Circulation. 2000;101:1568 –1577.
16. Olgin JE, Kalman JM, Fitzpatrick AP, et al. Role of right atrial endo-cardial structures as barriers to conduction during human type I atrialflutter: activation and entrainment mapping guided by intracardiac echo-cardiography.Circulation. 1995;92:1839–1848.
17. Nakagawa H, Lazzara R, Khastgir T, et al. Role of the tricuspid annulusand the eustachian valve/ridge on atrial flutter: relevance to catheterablation of the septal isthmus and a new technique for rapid identificationof ablation success.Circulation. 1996;94:407–424.
3098 Circulation June 26, 2001
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

ScheinmanRandall J. Lee, Paul R. Steiner, Leslie A. Saxon, Michael D. Lesh, Gunnard W. Modin and Melvin M.
Yanfei Yang, Jie Cheng, Andy Bochoeyer, Mohamed H. Hamdan, Robert C. Kowal, Richard Page,Atypical Right Atrial Flutter Patterns
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2001 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.103.25.3092
2001;103:3092-3098Circulation.
http://circ.ahajournals.org/content/103/25/3092Wide Web at:
The online version of this article, along with updated information and services, is located on the World
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe middle column of the Web page under Services. Further information about this process is available in thethe online version of the published article for which permission is being requested is located, click Request Permissions in
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. OnceCirculation Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from





























