Embed Size (px)
Citation preview

An Explanation of Asymmetric UpperExtremity Blood Pressures in Supravalvular
Aortic Stenosis
The Coanda Effect
By JAMES W. FRENCH, M.D., AND WARREN G. GUNTHEROTH, M.D.
SUMMARYThe Coanda effect, the tendency of a jet stream to adhere to a wall, was investigated
as an explanation of the unequal pressures in the upper extremities in patients withsupravalvular aortic stenosis (SVAS). Of 56 patients with SVAS reviewed, 48 had un-
equal blood pressures in the upper extremities. The average difference was 18 mm Hgsystolic. Although 11 of the 20 patients in the control group (valvular aortic stenosis)had some blood pressure asymmetry, the average difference was 3.5 mm Hg systolic.In valvular aortic stenosis, the velocity of the jet is quickly dissipated beyond thestenotic orifice, preventing any sustained high-velocity stream. However, the smooth,annular narrowing of SVAS creates a "step" between the orifice and the ascendingaortic wall which enhances the natural affinity of a jet for a boundary wall andconserves the kinetic energy of the jet stream. In most patients with SVAS, thehigh-velocity stream is along the right aortic wall, causing disproportionately high pres-
sure in the right arm.
Additional Indexing Words:Annular stenosis Jet stream
S UPRAVALVULAR aortic stenosis (SVAS)is one of several lesions which are
included in the congenital aortic stenosisgroup. Unequal systolic blood pressure in theupper extremities, which has been frequentlyreported with supravalvular stenosis,2-10 is animportant diagnostic sign because it has onlyrarely been reported in other congenitalcardiovascular lesions, except coarctation orinterruption of the transverse aortic arch.'1
From the Division of Pediatric Cardiology, Depart-ment of Pediatrics, University of Washington Schoolof Medicine, Seattle, Washington.
Supported by Training Grant TIHE-5281, andResearch Grant HE 07158 from the U. S. PublicHealth Service.
Presented in part at the 42nd Scientific Sessions,American Heart Association, Dallas, Texas, November1969. (Abstr.1)Received January 29, 1970; revision accepted for
publication April 22, 1970.
Circulation, Volume XLII, July 1970
Kinetic energy
We believe that aspects of fluid control theory,specifically the Coanda effect, offer a logicalexplanation of this phenomenon.The Coanda effect,'2-14 the tendency of a jet
stream to adhere to a boundary wall, was firstnoted in 1910 by Henri Coanda"5 andprobably represents a special case of the morefamiliar Bemoulli principle. As a jet exitsfrom a nozzle, it progressively broadens byentraining the surrounding fluid, the peakvelocity is proportionately diminished, and thekinetic energy of the jet is dissipated down-stream. An area of low pressure is produced atthe margins of the jet, and a counterflow iscreated to equalize the pressures (fig. LA). Ifa random disturbance causes the jet todeviate, inequalities will develop in thecounterflow, and the stream may "attach"' toone of the boundary walls. The course of thestream is then maintained by a combination of
31
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

FRENCH, GUNTHEROTH
a low pressure area adjacent to the boundarywall and the countercurrent flow from theopposite side of the jet. A similar deviation isproduced if the space or chamber around thenozzle is not symmetrical. The simplestexample of this is shown in figure lB. Onewall of the chamber has been moved closer tothe nozzle exit. It can be shown that the jetwill consistently attach to this near wall,12even following interruptions in the jet such asdiastole. This tendency of the jet stream toreestablish a specific pattern is termed "reset"or '"memory."'4 Other variations in the dimen-sions and the configuration of the chamberwill produce consistent changes in the courseof the jet stream. One important modificationis the introduction of a "shoulder" or "step" inthe wall close to the nozzle. Experimentalwork has shown that this particular configura-tion enhances the Coanda effect if the step isnot too abrupt.13 If the step is too abrupt, thejet will not follow the boundary wall, and thepeak energy of the jet will be dissipated in an
expanding volume downstream. The reasonfor the separation is the large angle ofreflection necessary to reach the boundarywall.'2, 14 This is termed an "anti-Coandaconfiguration."By introducing a splitter or bifurcation
downstream (figs. 1A and B), it is possible todemonstrate the kinetic energy of the jetstream as differential pressures or flows.12 14The bifurcation must be at least two nozzlewidths distant from the nozzle (2:1 ratio) toestablish the Coanda effect.To investigate the frequency and signifi-
cance of the unequal pressures, we havereviewed the data in six of our cases of SVAS,pressure and dimension data from 50 casespresented in the literature, and compared theresults with the data from 20 of our patientswith valvular aortic stenosis (VAS). The VASgroup was chosen as a control because of thesimilarities between the two lesions; thus, ifthere is a significantly greater pressure differ-ential in the supravalvular group, it should be
Splitter
k&I
Nozzle
A.Iw=-l
-.
F\
A
-High velocity jet stream
-Lowpressure Nozarea
Figure 1A jet stream flowing into a bounded chamber causes entrainment of fluid by the jet, genera-
tion of low pressures at the jet margins, and a counterflow (represented by arrows) of chamberfluid. (A) The jet kinetic energy is dissipated downstream, as the high-velocity stream broadens.(B) Unequal counterfiow as a result of asymmetry of the chamber causes deviation and "at-tachment" of the jet stream, with conservation of its kinetic energy and direction of thestream into the right branch.
Circulation, Volume XLII, July 1970
pressurearea
B
32
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

COANDA EFFECT
0 0
00
0000
0000
0
8
0
00
0 0
0 00
0
0 00000
0
0
0 000
oo
L>R R>L-o
SVAS
00 000 0
0
0 0
0 0
L>R R>LVAS
Figure 2
Differences in systolic blood pressures in upper ex-
tremities. Each dot represents one patient (total num-
ber of cases, 76). SVAS =supravalvular aortic ste-nosis group; VAS = control group with valvular aorticstenosis; R > L = systolic pressure in right arm ex-
ceeds that in left arm. L > R = systolic pressure inleft arm exceeds that in right arm.
due to the specific configuration of thesupravalvular lesion.
MethodsThe blood pressures in patients with supra-
valvular or valvular stenosis seen in the Universityof Washington Hospital were obtained with a
standard sphygmomanometer cuff by auscultation.The proper-sized cuff was judged to be 20% widerthan the diameter of the extremity where the cuffwas applied.16 All patients were examined eitherin the Pediatric Cardiology Clinic or as in-patients on the Pediatric Cardiology Service atUniversity Hospital. Cases were accepted fromliterature if blood pressures in both upperextremities were recorded in the report.3-10, 17-25Angiocardiographic films were reviewed forstep configuration (gradual transition betweenthe stenotic annulus and the poststenotic wall)and to determine the ratio of the chamber length(from the level of stenosis to the orifice of theinnominate artery) to the stenotic orifice.
Results (Table 1; Fig. 2)Of the 56 patients with SVAS under review,
48 or 86% had unequal systolic blood pressuresin the upper extremities. The average differ-ence in all cases of SVAS was 18 mm Hg(sE,+ 3.1). The range was 0 to 60 mm Hg.Higher pressures were obtained in the rightarm in 40 or 83% of the patients with adifference in pressures. In the control group of20 patients with valvular aortic stenosis, 11 or55% had a systolic pressure differential in theupper extremities, but the difference for allvalvular cases was only 3.5 mm Hg(SE, + 0.2). The range was 0 to 10 mm Hg.Higher pressures were obtained on the right infive or 45% of patients with differentialpressures. The average differences in systolicpressure between the two arms in SVAS, 18mm Hg, is significantly greater (P < 0.01) thanthe average difference in systolic pressures inVAS, 3.5 mm Hg. In all cases reviewed, theratio of chamber length to stenotic diameterexceeded the minimum 2:1 ratio necessaryfor the Coanda effect to be established.
Table 1
Data on Upper Extremity Systolic Blood Pressures in SVAS and VAS
SVAS VAS
Total no. of cases 56 20No. with unequal pressures 48 (86%7) 11 (55%o)
Right greater than left 40 5Left greater than right 8 6
Average difference (all cases) inblood pressures (mm Hg) 18 (=i=3.1)* 3.5 (-0.20)*
Range of difference (mm Hg) 0-60 0-10
*Standard error of mean.Circulation, Volume XLII, July 1970
70-
rz
$ 60-
^ 50-
C 40-
'AI)to
*. 20-
109
%,lo
33
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

FRENCH, GUNTHEROTH
DiscussionTwo principal explanations have been pro-
posed for the differential pressures in theupper extremities. A selective stenosis at theorigin of arch vessels has been suggested as acause of the unilaterally diminished pres-sure.4, 8, 20, 26, 27 However, recent reviews ofpathologic specimens by Peterson and associ-ates28 and radiologic material by Kupic andAbrams22 have suggested that the incidence ofsignificant selective aortic arch vessel stenosisis in the range of only 15 to 20%. Based on theradiologic report, selective stenoses of eitherthe left common carotid or left subelavianvessels are more common, although only 22 ofthe 121 cases reviewed had any significantstenosis of arch vessels. While it is probablethat selective arch vessel stenosis is significantin some cases, the frequency is too low toexplain the rather high incidence of differen-tial pressures in patients with SVAS.We support the alternate theory that the
cause of the differential pressures is a highvelocity jet streaming into the origin of aspecific arch vessel. In 1963, Lurie andMandelbaum,29 working with a canine model,and more recently Goldstein and Epstein,30with an aortic arch model, have confirmedthat the kinetic energy developed in a jetstream under simulated pathologic conditions(that is, with SVAS) is sufficient to cause theclinically observed difference in pressures. Ithas been suggested that the differential wasthe result of the alignment of the ascendingaorta and the orifice of the right innominateartery. However, this would not explainpatients with higher pressures on the left side.In addition, patients with VAS without SVAShave high velocity jets, but rarely unequalpressures. The high incidence of differentialpressures in SVAS logically suggests a uniquemechanism controlling the course of thestream between the stenotic area and the archvessel bifurcation.The major difference between the valvular
and supravalvular lesions occurs in the im-mediate poststenotic area. In valvular aorticstenosis, the initial step between the valveorifice and the ascending aortiic wall is large
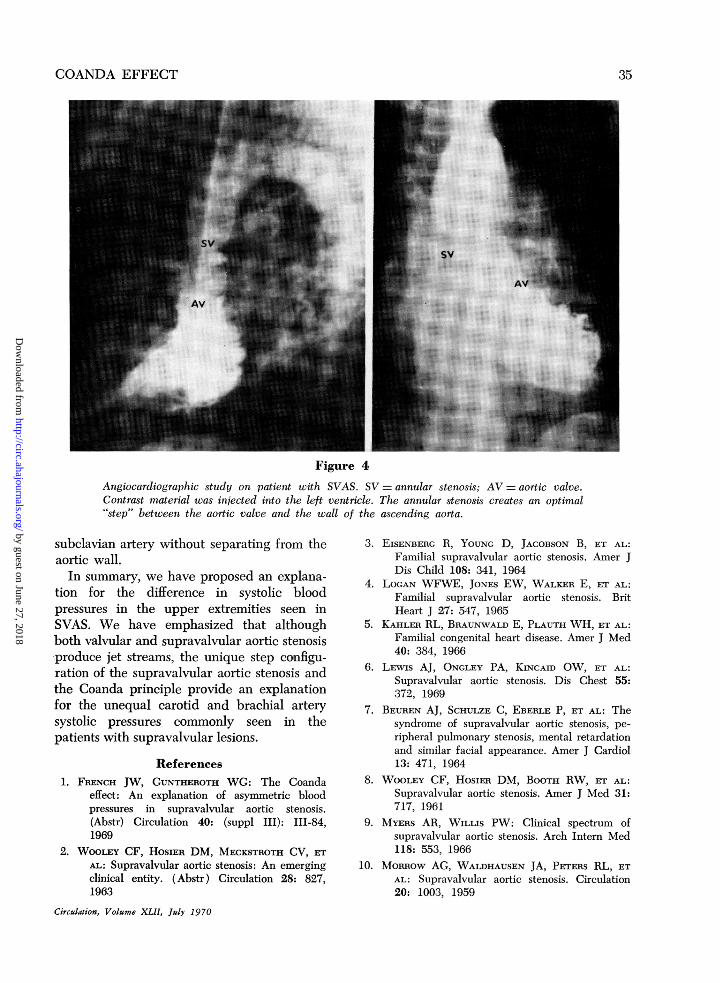
and abrupt (fig. 3A). This is made even moreextreme by the commonly associated postste-notic dilatation. Consequently, the jet streamdoes not attacb to the aortic wall. By contrast,the annular hourglass narrowing of thesupravalvular lesion creates an optimal step orshoulder transition between the stenotic areaand the wall of the ascending aorta (figs. 3Band 4). The limiting effect of the boundarywall on one surface and the confining effect ofthe counterflow on the opposite surface tendto stabilize the jet and retard its naturaltendency to broaden and disperse. With theaortic wall as a boundary, a positivelydirected, sustained jet stream is produced.Although the higher pressures are usuallyrecorded in the right arm, the Coanda effectwould apply equally well to patients who havehigher pressures in the left arm. This is logicalif the aorta is considered in its threedimensions (fig. 4). The jet stream couldeasily flow up the posterior wall of the aorta,bypassing the right innominate artery and en-tering the left common carotid or the left
A B
Figure 3Diagrammatic representations. (A) Valvular aorticstenosis with mild poststenotic dilatation. Note abrupttransition between stenotic valve and ascending aorticwall. (B) Supravalvular aortic stenosis. Note gradualtransition (step) between annular stenosis and ascend-ing aortic wall.
Circulation. Volume XLII, July 1970
34
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from
COANDA EFFECT
Figure 4
Angiocardiographic study on patient with SVAS. SV =annular stenosis: AV=aortic valve.Contrast material was injected into the left ventricle. The annular stenosis creates an optimal"'step" between the aortic valve and the wall of the ascending aorta.
subclavian artery without separating from theaortic wall.
In summary, we have proposed an explana-tion for the difference in systolic bloodpressures in the upper extremities seen inSVAS. We have emphasized that althoughboth valvular and supravalvular aortic stenosisproduce jet streams, the unique step configu-ration of the supravalvular aortic stenosis andthe Coanda principle provide an explanationfor the unequal carotid and brachial arterysystolic pressures commonly seen in thepatients with supravalvular lesions.
References1. FRENCH JW, GUNTHEROTH WG: The Coanda
effect: An explanation of asymmetric bloodpressures in supravalvular aortic stenosis.(Abstr) Circulation 40: (suppl III): 111-84,1969
2. WoouEY CF, HOsIER DM, MECKSTROTH CV, ETAL: Supravalvular aortic stenosis: An emergingclinical entity. (Abstr) Circulation 28: 827,1963
Circulaion, Volume XLII, July 1970
3. EISENBERG R, YOUNG D, JACOBSON B, ET AL:Familial supravalvular aortic stenosis. Amer JDis Child 108: 341, 1964
4. LOC;AN WFWE, JONES EW, WALKER E, ET AL:Familial supravalvular aortic stenosis. BritHeart J 27: 547, 1965
5. KAHLER RL, BRAUNWALD E, PLAUTH WH, ET AL:Familial congenital heart disease. Amer J Med40: 384, 1966
6. LEwIS AJ, ONGLEY PA, KINCAID OW, FT AL:Supravalvular aortic stenosis. Dis Chest 55:372, 1969
7. BEUREN AJ, SCHULZE C, EBERLE P, ET AL: Thesyndrome of supravalvular aortic stenosis, pe-ripheral pulmonary stenosis, mental retardationand similar facial appearance. Amer J Cardiol13: 471, 1964
8. WoouxY CF, HosiER DM, BOOTH RW, ET AL:Supravalvular aortic stenosis. Amer J Med 31:717, 1961
9. MYERS AR, WILLIS PW: Clinical spectrum ofsupravalvular aortic stenosis. Arch Intern Med118: 553, 1966
10. MoRRow AG, WALDHAUSEN JA, PETERS RL, ETAL: Supravalvular aortic stenosis. Circulation20: 1003, 1959
35
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

FRENCH, GUNTHEROTH
11. SISSM;sAN NJ: Anomalies of the aortic archcomplex. In Heart Disease in Infants, Childrenand Adolescents, edited by AJ Moss, FHAdams. Baltimore, Williams & Wilkins Co.,1968, p 418
12. AUGRIST SW: Fluid control devices. Sci Amer211: 81, 1964
13. REBA I: Applications of the Coanda effect. SciAmer 214: 84, 1966
14. CUTLER SS, BURBANK B: Fluid control devices,'"rheostasis,' and the huiman circulation. JThorac Cardiovasc Surg 56: 558, 1968
15. COANDA H: Procede de propulsion dans unfluide. Brevet Invent Gr Cl 2 no 762688 Re-publique Francaise, 1932, cited in reference 13and in Willie R, Fernholz H: Report of thefirst European mechanics colloquium on theCoanda effect. J Fluid Mech 23: 801, 1965
16. PARK MK, GUNTHEROTH WG: Direct bloodpressure measurements in arms and legs. Cir-culation 41: 231, 1970
17. GARCIA RE, FRIEDMAN WF, KABACK MM, ETAL: Idiopathic hypercalcemia and supravalvu-lar aortic stenosis: Documentation of a newsyndrome. New Eng J Med 271: 117, 1964
18. JUE KL, NOREN GR, ANDERSON RC: Thesyndrome of idiopathic hypercalcemia of in-fancy with associated congenital heart disease.J Pediat 67: 1130, 1965
19. ANITA AU, WILTSE HE, ROWE RD, ET AL:Pathogenesis of the supravalvular aortic stenosissyndrome. J Pediat 71: 431, 1967
20. FRANCH RH, ERDOGEN 0: Asymmetric arm and
neck pulses: A clue to supravalvular aorticstenosis. (Abstr) Circulation 28: 722, 1963
21. BOURASSA MG, CAMPEAu L: Combined supra-valvular aortic and pulmonic stenosis. Circu-lation 28: 572, 1963
22. KUPIC FA, ABRAMS HL: Supravalvular aorticstenosis. Amer J Roentgen 98: 822, 1966
23. FARREII C, DOTTER CT, GRISWOLD HE:Supravalvular aortic stenosis. Amer J Dis Child108: 335, 1964
24. CHAUTLER C, DAvIs DH, JOSEPH MC: Cardio-vascular and other associations of infantile hy-percalcemia. Guys Hosp Rep 115: 221, 1966
25. NAJAF H, DYE WS, JULIAN OC: Successful onestage correction of both supravalvular aorticstenosis and typical coarctation of aorta in onepatient. J Thorac Cardiovasc Surg 48: 644,1964
26. FRIEDMAN WF: Letter to editor: Supravalvularaortic stenosis. Amer J Dis Child 109: 261,1965
27. EISENBERG R: Letter to the editor. Amer J DisChild 109: 262, 1965
28. PETERSON TA, TODD DB, EDWARDS JE: Supra-valvular aortic stenosis. J Thorac CardiovascSurg 50: 734, 1965
29. LURIE PR, MANDELBAUM I: Mechanism ofbrachial pulse asymmetry in congenital aorticstenotic lesions (Abstr) Circulation 28: 760,1963
30. GOLDSTEIN RE, EPSTEIN SE: Mechanism ofelevated innominate artery pressure in supra-valvular aortic stenosis. (Abstr) Circulation 40(suippl III): III-92, 1969
Circulaton, Volume XII, July 1970
36
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from

JAMES W. FRENCH and WARREN G. GUNTHEROTHSupravalvular Aortic Stenosis: The Coanda Effect
An Explanation of Asymmetric Upper Extremity Blood Pressures in
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1970 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.42.1.31
1970;42:31-36Circulation.
http://circ.ahajournals.org/content/42/1/31located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on June 27, 2018http://circ.ahajournals.org/
Dow
nloaded from





























