Embed Size (px)
Citation preview

207V.W. Fazio et al. (eds.), Atlas of Intestinal Stomas, DOI 10.1007/978-0-387-78851-7_17, © Springer Science+Business Media, LLC 2012
Introduction
Retrograde rectal irrigation through various enema tech-niques is a well-accepted practice to empty the lower bowel and to relieve constipation and fecal soiling in patients with functional bowel disorders [ 1 ] . However, retrograde enemas can be technically challenging for elderly and disabled patients and may require caregiver assistance. For the patient with severe bowel dysfunction who is contemplating a per-manent colostomy, the antegrade colonic enema (ACE) pro-cedure may be a viable option. This procedure allows easy access to the colon through the abdominal wall with inter-mittent catheterization, irrigation of the colon, and rapid, controlled bowel purging (Fig. 17.1 ). The goal is to avoid wearing a stoma pouch while allowing the patient to inde-pendently manage his or her own bowel activities.
The ACE technique was fi rst described by Malone in 1990 using the appendix as the conduit but since them the cecum, ileum, and left colon have been utilized as the continence mechanism [ 2– 5 ] . Malone adapted this concept from the urology literature where a cutaneous appendicovesicostomy was introduced to maintain urinary continence [ 6 ] . These procedures have become increasingly popular for children with spinal dysraphism and anorectal malformations and are well reported in the pediatric literature [ 7 ] . The ACE proce-dure is gaining recognition in the adult population for patients with colonic neurologic dysfunction, colonic inertia, obstructed defecation, and fecal incontinence [ 8– 15 ] .
Variations to the traditional ACE procedure have also been reported with success. The results of laparoscopic ACE procedures using the technique of in situ appendix without cecoplication have promising results [ 16, 17 ] . Left-sided ACE procedures with irrigation of the descending colon for
Antegrade Colonic Enema (ACE)
Brooke Gurland, Crina V. Floruta, and Ian C. Lavery
17
B. Gurland (*) • C. V. Floruta • I. C. Lavery Department of Colorectal Surgery , Digestive Disease Institute, Cleveland Clinic Foundation , Cleveland , OH , USA e-mail: [email protected]
Fig. 17.1 The catheter is intermittently inserted into an orifi ce on the anterior abdominal wall and into the cecum for irrigation of the colon and rapid and controlled bowel purging. Illustration © CCF
208 B. Gurland et al.
patients with constipation have shown decreased irrigation times and require less fl uid compared to those patients with right colon access [ 18 ] . Percutaneous endoscopic placement of tubes into the left or right colon can provide minimally invasive access to the bowel for irrigation and decompres-sion [ 19 ] .
Indications/Patient Selection
Patients who have severe bowel dysfunction with fecal soil-ing or constipation who have failed medical or surgical treatments may be candidates for the ACE procedure. The ACE procedure does not preclude colectomy or stoma cre-ation. Successful outcomes depend on patient expectations and motivations. Colonic irrigation is a life-long commit-ment and a rigid, time-consuming regimen. Bowel irriga-tion and evacuation takes approximately 45–60 min every day or every other day to adequately purge the bowel. Determining the correct volume of fl uid irrigant and addi-tives for optimal colonic wash out is achieved through trial and error. Nursing support to work with patients to deter-mine the irrigation recipe is as important as the technical aspects of the procedure.
Preoperative Preparation
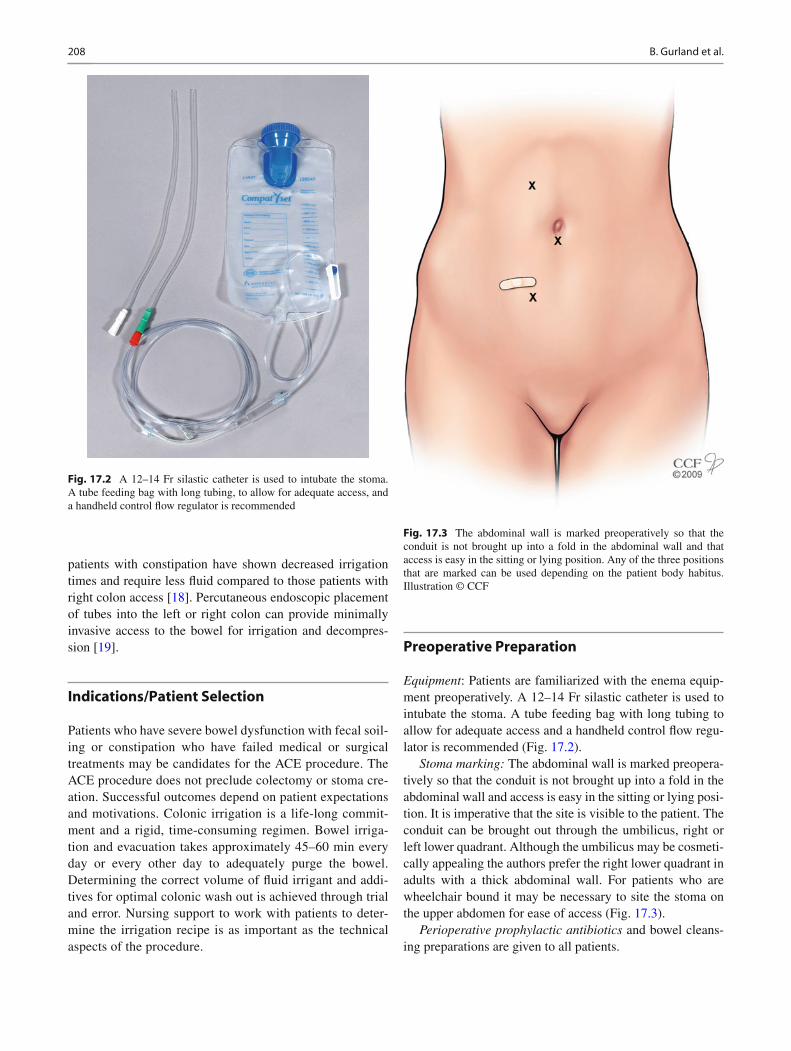
Equipment : Patients are familiarized with the enema equip-ment preoperatively. A 12–14 Fr silastic catheter is used to intubate the stoma. A tube feeding bag with long tubing to allow for adequate access and a handheld control fl ow regu-lator is recommended (Fig. 17.2 ).
Stoma marking: The abdominal wall is marked preopera-tively so that the conduit is not brought up into a fold in the abdominal wall and access is easy in the sitting or lying posi-tion. It is imperative that the site is visible to the patient. The conduit can be brought out through the umbilicus, right or left lower quadrant. Although the umbilicus may be cosmeti-cally appealing the authors prefer the right lower quadrant in adults with a thick abdominal wall. For patients who are wheelchair bound it may be necessary to site the stoma on the upper abdomen for ease of access (Fig. 17.3 ).
Perioperative prophylactic antibiotics and bowel cleans-ing preparations are given to all patients.
Fig. 17.2 A 12–14 Fr silastic catheter is used to intubate the stoma. A tube feeding bag with long tubing, to allow for adequate access, and a handheld control fl ow regulator is recommended
Fig. 17.3 The abdominal wall is marked preoperatively so that the conduit is not brought up into a fold in the abdominal wall and that access is easy in the sitting or lying position. Any of the three positions that are marked can be used depending on the patient body habitus. Illustration © CCF

20917 Antegrade Colonic Enema (ACE)
Operative Steps
1. The ACE can be performed via a laparoscopic or open technique with a midline, transverse, or right lower quad-rant abdominal incision. The cecum is mobilized so that it easily reaches the abdominal wall. Malone initially described using the reversed appendix as the conduit with the amputated tip tunneled in the cecum, but this is no longer recommended and the appendix is left in situ.
2. The tip of the appendix is removed and a stay suture is inserted to stretch out the appendix to reveal the mesen-tery. A 12 Fr catheter is passed through the appendix to the cecum (Fig. 17.4 ).
3. A valve mechanism is created to avoid backfl ow of fecal material through the conduit. The appendix is folded and the cecum is loosely wrapped around the appendix (Figs. 17.5 and 17.6 ). The suture picks up the seromuscu-lar layer on the cecum on each side of the appendix to anchor the tunnel. The cecum is anchored to the back of the anterior abdominal wall where the appendix emerges to prevent twisting and kinking of the conduit.
4. For patients without an appendix: A 5–10 cm segment of terminal ileum is isolated on its vascular pedicle (Fig. 17.7 ). A longer conduit is needed for a patient with a thicker abdominal wall. Bowel continuity is restored using a standard end-to-end anastomosis (Fig. 17.8 ). The isolated ileum is tubularized over a 12 Fr catheter by using a stapling device on the antimesenteric surface to narrow the lumen (Fig. 17.9 ). One end is then implanted into a submucosal tenial tunnel in the cecum and the other is brought to the skin as a stoma.
5. The colonic submucosal tunnel is created by incising the seromuscular layer of the tenia with a scalpel down to the
Fig. 17.4 The tip of the appendix is removed and a stay suture is inserted to stretch out the appendix to reveal the mesentery. A 12 Fr catheter is passed through the appendix to the cecum. Illustration © CCF
Fig. 17.5 A valve mechanism is created to avoid backfl ow of fecal material through the conduit. Illustration © CCF
Fig. 17.6 The appendix is folded and the cecum is loosely wrapped around the appendix. Illustration © CCF

210 B. Gurland et al.
Fig. 17.7 For patients without an appendix, a 5–10 cm segment of ter-minal ileum is isolated on its vascular pedicle. Illustration © CCF
Fig. 17.8 Small bowel continuity is restored using a standard end-to-end anastomosis. Illustration © CCF
Fig. 17.9 The bowel is tubularized over a 12 Fr catheter by using a stapling device on the antimesenteric surface to narrow the lumen. Illustration © CCF
21117 Antegrade Colonic Enema (ACE)
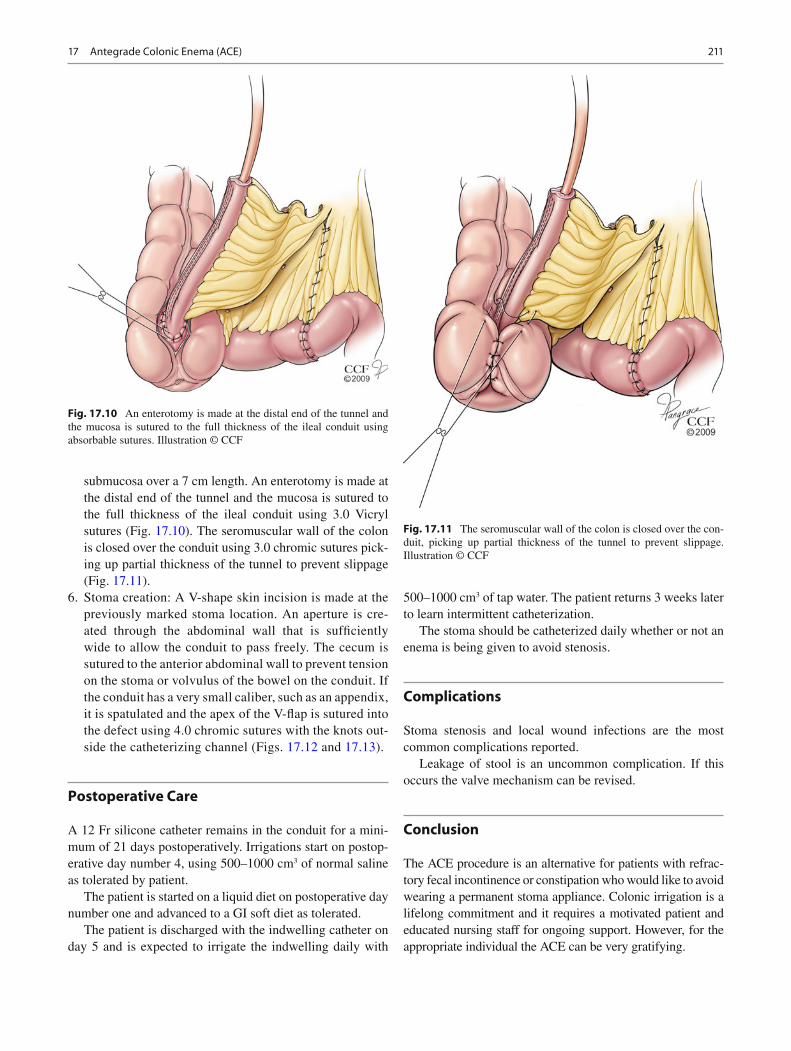
submucosa over a 7 cm length. An enterotomy is made at the distal end of the tunnel and the mucosa is sutured to the full thickness of the ileal conduit using 3.0 Vicryl sutures (Fig. 17.10 ). The seromuscular wall of the colon is closed over the conduit using 3.0 chromic sutures pick-ing up partial thickness of the tunnel to prevent slippage (Fig. 17.11 ).
6. Stoma creation: A V-shape skin incision is made at the previously marked stoma location. An aperture is cre-ated through the abdominal wall that is suffi ciently wide to allow the conduit to pass freely. The cecum is sutured to the anterior abdominal wall to prevent tension on the stoma or volvulus of the bowel on the conduit. If the conduit has a very small caliber, such as an appendix, it is spatulated and the apex of the V-fl ap is sutured into the defect using 4.0 chromic sutures with the knots out-side the catheterizing channel (Figs. 17.12 and 17.13 ).
Postoperative Care
A 12 Fr silicone catheter remains in the conduit for a mini-mum of 21 days postoperatively. Irrigations start on postop-erative day number 4, using 500–1000 cm 3 of normal saline as tolerated by patient.
The patient is started on a liquid diet on postoperative day number one and advanced to a GI soft diet as tolerated.
The patient is discharged with the indwelling catheter on day 5 and is expected to irrigate the indwelling daily with
500–1000 cm 3 of tap water. The patient returns 3 weeks later to learn intermittent catheterization.
The stoma should be catheterized daily whether or not an enema is being given to avoid stenosis.
Complications
Stoma stenosis and local wound infections are the most common complications reported.
Leakage of stool is an uncommon complication. If this occurs the valve mechanism can be revised.
Conclusion
The ACE procedure is an alternative for patients with refrac-tory fecal incontinence or constipation who would like to avoid wearing a permanent stoma appliance. Colonic irrigation is a lifelong commitment and it requires a motivated patient and educated nursing staff for ongoing support. However, for the appropriate individual the ACE can be very gratifying.
Fig. 17.10 An enterotomy is made at the distal end of the tunnel and the mucosa is sutured to the full thickness of the ileal conduit using absorbable sutures. Illustration © CCF
Fig. 17.11 The seromuscular wall of the colon is closed over the con-duit, picking up partial thickness of the tunnel to prevent slippage. Illustration © CCF

212 B. Gurland et al.
References
1. Briel JW, Schouten WR, Vlot EA, Smits S, van Kessel I. Clinical value of colonic irrigation in patients with continence disturbances. Dis Colon Rectum. 1997;40(7):802–5.
2. Malone PS, Ransey PG, Kiely EM. Preliminary report: the ante-grade continence mechanism. Lancet. 1990;336:1217–8.
3. Monti PR, Lara RC, Dutra MA, De Carvallo JR. New techniques for construction of efferent conduits based on the Mitranoff princi-ple. Urology. 1997;49:112–5.
4. Willams NS, Hughes SF, Stuchfi eld B. Continent colonic conduit for rectal evacuation in severe constipation. Lancet. 1994;343(8909):1321–4.
5. Kiely EM, Ade-Ajayi N, Wheeler RA. Caecal fl ap conduit for antegrade continence enemas. Br J Surg. 1994;81(8):1215.
6. Mitrofanoff P. Cystostomie continenente trans-appendiculare dans le traitment des vessies neurologiques. Chir Pediatr. 1980;21:297–305.
7. Sinha CK, Grewal A, Ward HC. Antegrade continence mechanism (ACE): current practice. Pediatr Surg Int. 2008;24(6):658–8.
8. Worsoe J, Christensen P, Krogh K, Buntzen S, Laurberg S. Long-term results of antegrade colonic enema in adult patients: assessment of functional results. Dis Colon Rectum. 2008;51(10):1523–8.
9. Poirier M, Abcarian H, Nelson R. Malone antegrade continent enema: an alternative to resection in severe defecation disorders. Dis Colon Rectum. 2007;50(1):22–8.
10. Dick AC, McCallion WA, Brown S, Boston VE. Antegrade colonic enemas. Br J Surg. 1996;83:642–4.
11. Gerharz EW, Vik W, Webb G, Leaver R, Shah PJ, Woodhouse CR. The value of the MACE procedure in adult patients. JAM Coll Surg. 1997;185:544–7.
12. Teichman JM, Harris JM, Currie DM, Barber DB. Malone ante-grade continence mechanism for adults with neurogenic bowel dis-ease. J Urol. 1998;160:1278–81.
13. Hirst GR, Arumugam PJ, Watkins AJ, Mackey P, Morgan AR, Carr ND, et al. Antegrade continence enema in the treatment in the treat-ment of obstructed defecation with or without fecal incontinence. Tech Coloproctol. 2005;9:217–21.
14. Lees NP, Hodson P, Hill J, Pearson RC, MacLennan I. Long term results of the antergrade continent enema procedure for adults with constipation. Colorectal Dis. 2004;6(5):362–8.
15. Rongen MJ, van der Hoop Gerritsen, Baeten CG. Cecal access for antegrade colon enemas in medically refractory slow transit consti-pation. Dis Colon Rectum. 2001;44:1644–9.
16. Nanigian DK, Kurzrock EA. Intermediate – Term outcome of the simplifi ed laparoscopic antegrade continence enema procedure: less is better. J Urol. 2008;179:299–303.
17. Webb HW, Barraza MA, Crump JM. Laparoscopic appendicostomy for management of fecal incontinence. J Pediatr Surg. 1997;32:457–8.
18. Sinha CK, Butler C, Haddad M. Left Antegrade Colonic Enema (LACE): review of the literature. Eur J Pediatr Surg. 2008;18(4):215–8.
19. Uno Y. Introducer method of percutaneous endoscopic cecostomy and antegrade continence enema by use of the Chait Trapdoor cecostomy catheter in patients with adult neurogenic bowel. Gastrointest Endosc. 2006;63:666–73.
Fig. 17.12 A V-shape skin incision is made at the previously marked location and the stoma is created. Illustration © CCF
Fig. 17.13 The ACE orifi ce





























