Embed Size (px)
Citation preview

Zurich Open Repository andArchiveUniversity of ZurichMain LibraryStrickhofstrasse 39CH-8057 Zurichwww.zora.uzh.ch
Year: 2011
Asymmetrical translations of biomedicine in India: The cases ofcontemporary Ayurveda and psychiatry
Chopra, Ananda Samir ; Quack, Johannes
Posted at the Zurich Open Repository and Archive, University of ZurichZORA URL: https://doi.org/10.5167/uzh-122686Journal ArticlePublished Version
Originally published at:Chopra, Ananda Samir; Quack, Johannes (2011). Asymmetrical translations of biomedicine in India:The cases of contemporary Ayurveda and psychiatry. Viennese Ethnomedicine Newsletter, 13(2-3):13-24.

spring /summer 2011
viennese ethnomedicine newsletter
C E N T R E F O R P U B L I C H E A LT H , M E D I C A L U N I V E R S I T Y O F V I E N N Aq u o n d a m A C A D E M I A C A E S A R E O - R E G I A I O S E P H I N A 1 7 8 5
unit ethnomedicine and international health
volume XIII number 2-3
Ladakh, August 2010

ISSN 1681-553X
Submissions, announcements, reports or names to be added to the mailing list, should be sent to:Editors, Viennese Ethnomedicine Newsletter, Centre for Public Health, Unit Ethnomedicine andInternational Health, Währinger Strasse 25, A-1090 Vienna, AustriaFAX: (++)43-1-42779634, e-mail: [email protected]: http://www.univie.ac.at/ethnomedicine
Frontispiece In August 2010, Ladakh in North India was hit by a natural disaster: cloudbursts, floods and mud slidescaused the death of hundreds of people, and destruction all along the Indus river and in nearby areas.The picture shows the situation in the Tibetan refugee settlement Choglamsar the day following thedisaster.
(photograph: Nike-Ann Schröder, see article this issue)
Viennese Ethnomedicine Newsletteris published three times a year by the Unit Ethnomedicine and International Health,
Department of General Practice, Center for Public Health, Medical University of Vienna, Austria.
Editors in chief
Ruth Kutalek, Armin Prinz, Unit Ethnomedicine and International Health, Department of General Practice, Center for Public Health, Medical University of Vienna, Austria
Guest editor
William Sax, University of Heidelberg
Editorial board
John Janzen, University of Kansas; Wolfgang Jilek, University of British Columbia; Sjaak van der Geest, University of Amsterdam; Manfred Kremser, University of Vienna;
Wolfgang Kubelka, University of Vienna; Guy Mazars, University of Strasbourg; Rogasian Mahunnah, University of Dar es Salaam; Traude Pillai-Vetschera, University of Vienna;
Jun Takeda, University of Saga; Zohara Yaniv, Volcani Center, Israel
ContentMedical Anthropology at Heidelberg (William Sax) . . . . . . . . . . . . . . . . . . . . . . . 3Ritual Healing and Modernity in Western Kenya (Ferdinand Okwaro) . . . . . . . . . . . . . . 5Asymmetrical Translations of Biomedicine in India: The Cases of Contemporary Ayurveda andPsychiatry (Ananda Samir Chopra, Johannes Quack) . . . . . . . . . . . . . . . . . . . . . . 13Stress and Modern Work: Ethnographic Perspectives from Industries in Bangladesh (Christian Strümpell, Hasan Ashraf) . . . . . . . . . . . . . . . 24Experiencing a Natural Disaster in a Tibetan Refugee Camp. Who is Present When Life is in Danger? (Nike-Ann Schröder) . . . . . . . . . . . . . . . . . . 33Lifestyle Diseases in India – the Management of Type 2 Diabetes Mellitus (T2DM) in Kerala (Constanze Weigl) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
ISSN 1681-553X

13
that they had died after being ritually burnt byMB. Kirwa’s children stated that they heard ofa neighbor who had died after fighting with hisown father, but they were unaware that he wasinvolved in killing their father until he made theconfession at MB’s “X-ray” session. Howeverthe alleged masterminds of their father’s killing,who were well known to Kirwa’s children sincethey had an affinal relationship with them, hadnot succumbed. They appeared in subsequent“outcome” sessions and claimed that theyapproached other healers to protect them fromMB’s fire. The remedy for such a case for MBwas a new “hearing” and “judgment” sessionwhere the two would be set on fire together with their healers, followed by yet another“outcome” session. The case became protractedover several months in which MB set themasterminds on fire, and in subsequent out-come sessions, the enemies claimed to haveapproached new healers who protected them. Inthe last “outcome” sessions that I observed withKirwa’s children, the masterminds of theirfather’s murder reported that they were fatallyill. I did not encounter Kirwa’s children atMB’s rituals again, but in subsequent discus-sions at their home, they concluded that MBhad at least punished those who killed theirfather and it was just a matter of time beforethose who hired them also died. According tothem MB’s healing had addressed their con-cerns to their satisfaction.
Conclusion
Ritual healing is vibrant in Western Kenya and is neither a rejection of nor a resistance tomodernity. In its comprehensive etiology, ritualhealing accommodates and in some instancesattempts to domesticate “modernity”, as ritualhealers and their clients grapple with the issuesand problems occasioned by rapid societal
transformation. This societal transformation inthe name of modernization has solved manyproblems as well as creating new ones, and ithas also resulted in new avenues for dealingwith old problems. Ritual healing played animportant role in solving some of the problemsfaced by the people, since as one of my clientsreiterated regarding his consultations with MB,“We are dealing with African chemistry here”.
References
Comaroff, J., Comaroff, J. (1999) Occult economiesand the violence of abstraction: notes from theSouth African post colony. In: AmericanEthnologist 26, 2: 279-303.
Evans-Pritchard, E. E. (1937) Witchcraft oracles andmagic among the Azande. Oxford: Clarendon Press.
Fergusson, J. (1999) Expectations of modernity: Mythsand meanings of urban life on the Zambian copperbelt. Berkeley: University of California Press.
Good, M. C. (1987) Ethnomedical systems in Africa:Patterns of traditional medicine in rural and urbanKenya. New York: The Guildford Press.
Kirmayer, J. L. (2004) The cultural diversity of heal-ing: Meaning, metaphor and mechanism. In: BritishMedical Bulletin 69, 33-48.
Moore, H., Todd, S. (2001) Introduction. In: H.Moore, T. Sanders (ed.) Magical interpretations,material realities. Modernity, witchcraft and theoccult in postcolonial Africa. London: Routledge, 1-27.
Okoth-Owiro, A. (1994) Law and traditional medicine.In: A. Islam, R. Wiltshire (ed.) Traditional healthsystems and public policy. Ottawa: InternationalDevelopment and Research Center.
Sax, W. (2010) Ritual and the problem of efficacy. In J. Quack, W. Sax, I. Weinhold (ed.). The problemof ritual efficacy. Oxford: Oxford University Press,1-16.
Whyte, S. R. (1989) Anthropological approaches toAfrican misfortune. From religion to medicine. InA. Jackobsen-Widding, D. Westerlund (eds.)Culture experience and pluralism. Essays onAfrican ideas on illness and healing. Uppsala: ActaUniversitatis Upsaliensis, 289-301.
Introduction
The spread of modern Western biomedicine toall parts of the world in the past two centuries
Asymmetrical Translations of Biomedicine in India: The Cases of Contemporary Ayurveda and Psychiatry
Ananda Samir Chopra, Johannes Quack
represents one of the most conspicuous examp-les of transcultural flows. This flow of bio-medicine to different cultural and geographicalcontexts is informed by and again creates

14
asymmetries on different levels. By presentingtwo cases from India we endeavor to analyzethe nature and effect of the transcultural flowof biomedicine and the asymmetries associatedwith it. Studying the practice of biomedicalpsychiatry in the context of a small Indian city,Johannes Quack examines the ways in whichpsychiatric concepts are made understandableto patients with a cultural background that isclearly different from the cultural backgroundof biomedicine. Cultural and economic factorsshape this process of translation as well as thepractice of biomedical psychiatry. The theme oftranslation also looms large in Ananda Chopra’sstudy of biomedicine’s impact on contemporaryAyurveda. A scholarly medical tradition with along literary history, Ayurveda reacts to bio-medicine and its overwhelming claim to scienti-fic truth in a complex way. On the institutionallevel the influence of biomedicine leads to aprocess of professionalization with the creationof ayurvedic institutions resembling biomedicalones. But on the conceptual level we find a com-plex process in the course of which Ayurvedaincorporates biomedical knowledge in a pecu-liar way that is shaped by classical Indiannotions of science.
The two projects presented here summarize thefirst findings of work in progress that is part ofa larger research project called “Asymmetricaltranslations: Mind and body in European andIndian medicine” (C3) which investigatesinstances of “asymmetrical translations” in atrans-cultural perspective with respect toIndian systems of medicine in the West andWestern systems of medicine in India. Thecentral hypothesis is that flows of ideas andpractices produced (and continue to produce)theoretical, practical, pedagogical, economic,aesthetic and other asymmetries within andamongst the European and South Asian healingsystems. These asymmetries are exemplified aswell as caused by practices of translation whichwe understand to include not only textual trans-lation, but also pedagogics and therapeutics. Inorder to test, substantiate, qualify or correctthis hypothesis the members of this project havebeen conducting research on transnationalflows within and between the quartet of biomed-icine, Ayurveda, psychology/psychiatry andvernacular healing, basing our investigation onlearned and popular texts as well as on theethnography of clinical and vernacular healing
practices. The central research question for allresearch projects is how texts and institutions(hospitals, medical schools, textbooks, doctors’reports, clinics, spas) of indigenous South Asianhealing systems adapt to the dominant bio-medical paradigm and vice versa. Furtherresearch questions address the different aspectsof translation, spanning from the “translationof systems” over the “translation of practices”to the “translation of concepts” and theirrespective interconnections with nosologies andtherapies.
One of the major strengths of the project is itsinter-cultural and inter-disciplinary nature,with inputs from medical anthropology, reli-gious studies, philology, history, and history ofmedicine. Besides the two authors, there aretwo doctoral students (Hari Kumar Nair andChristoph Cyrianski) and three other core teammembers working on the project “AsymmetricalTranslations”. The project is coordinated byWilliam S. Sax who is exploring the ways in which terms and ideas associated with“Western” psychology penetrate North Indianpopular culture. Bhargavi Davar is conductingan archival study of the ideational and institu-tional histories of psychology and psychiatry inIndia during the late colonial period. Finally,Harish Naraindas is working on the status ofAyurveda in the context of “complementary andalternative medicine” in Germany (seewww.asia-europe.uni-heidelberg.de).
Psychiatry in India
The massive worldwide export of “Western”psychiatry is a rather recent phenomenon. The health-related activities of internationaldevelopment agencies and especially nationalhealth ministries in developing countries have,for a long time, shown little interest in mentalhealth issues. This was partially due to the factthat international health professionals havetended to exclude mental illness from standardassessments of global health (Desjarlais et al.1996: 4). This situation, however, has begun tochange recently. Increasingly, the WHO stressesthat mental disorders make substantial contri-butions to the global burden of disease (GBD)while the proportion of those people withmental disorders who would need treatment butreceive no or inadequate mental health care – the so-called “treatment gap” – is estimated at

15
around 80% for low and middle-income coun-tries (www.who.int/mental_health). Global andnational institutions are therefore currentlyinvesting massively in the export of “Western”psychiatric techniques.
Such developments have been reflected uponcritically in historical (e. g. Bhugra 2001) andcontemporary perspectives (e. g. Watters 2010).Although ideas of the universality of psychiatricmodels and therapies are extremely powerful,many anthropological studies have shown thatbehavioral and psychological disturbances innon-Western settings cannot be easily equatedwith the categories of Western psychopathology,and that seemingly appropriate categories oftenhave a significantly different meaning in localcontexts (Kleinman’s classic “category fallacy”1977). While such studies focus primarily ondiagnostic categories, there are few comparablein-depth studies of how psychiatry is actuallypracticed in various local contexts outside theNorth-Atlantic world. Indeed, there are scien-tific, professional, institutional, economic andpeer pressures on psychiatrists to emphasize thetransculturally similar aspects of their practiceand to downplay local differences. Even ifpsychiatrists the world over have (more or less)similar teaching curricula, use the same dia-gnostic manuals, and prescribe the same drugs,they differ in their actual treatment and thetake-up of the treatment by patients variesgreatly; the health benefits of (and the harmcaused by) their various treatments are there-fore not the same.
Quack’s current research project engages withthe recent export of “Western” psychiatry, andaddresses problems related to the translation ofconcepts and practices from psychiatry intoNorth Indian realities. This work is part of theauthor’s long-term interest in issues of “mentalhealth” in India. During his doctoral fieldworkon rationalist organizations and their criticismof “traditional” healing practices (Quack 2011)he focused especially on the criticism of reli-gious healing sites. His work included shortethnographic field studies on “traditional” men-tal health-care at Balaji temple, Mehandipur,India and visits to “traditional” mental health-care sites such as the Vineyard Workers’Church (Pune), the “exorcist” Abid Kadiri(Ahmednagar), the Mirawali Durgah(Ahmednagar), the Mahanubhav Temple
(Phaltan), Farshiwale Baba (Nasik), and MiraDattar Durgah (Palanur). In addition, Quackconducted interviews with psychiatrists, mentalhealth activists, various NGO representatives,and self-help groups in Maharashtra and Delhi.
Against this background, Quack’s currentresearch aims can be divided into two parts.The first part is an ethnographic study of apsychiatric wing of an urban hospital in thestate of Uttarakhand in North India, based onlong-term fieldwork conducted there in 2010. Itcontributes to the small group of researchersworking on the actual practice of “Western”psychiatry in India (e. g. Addlakha 2008; Jainand Jadhav 2008, 2009) and other non-Westerncountries (e. g. Higginbotham 1984; Gaines1992).
The psychiatric system adopted from the Westis practiced in a specific way in India. The mostimportant difference is the lack of institutional-ized mental health care infrastructure, i. e.psychiatrists, psychologists, additional thera-peutic care and social workers. The two mostsignificant implications of this shortage ofhealth professionals are the very short consulta-tion times the therapists can dedicate to eachpatient, and the great distances that manypatients must travel to reach the doctor, whenand if one is available and affordable. Furtherproblems of infrastructure are that not onlymental health professionals but also some of themedicines are not available to or affordable forthe patients. The mental health care situation inUttarakhand was summarized by a WHOreport from 2006 in the following words:“Uttarkhand is a new state and it lacks in suffi-cient infrastructure, manpower, and facilities.The state has neither a mental hospital nor acommunity mental health facility. There is nospecific mental health related informationsystem in the state […]. Only 3.22 percent ofthe total planned budget for the year 2005-06has been earmarked for health of which only1.2 percent (INR 106.61 lakh [“lakh” is a unitin the Indian numbering system equal to onehundred thousand]) has been allocated forestablishment of a Mental Health Authority andthe construction of a mental hospital. The statedoes not have a mental health outpatient facilityin the public sector.” (WHO 2006: iv-v)
In general, this assessment still held true in

16
2010. The major difference from 2006 is thatthe state has a new Mental Hospital, in Selaquinear Dehradun. It was not offering full servicewhen Quack last visited in October 2010, buthad begun to treat the first few inpatients.Beside this, the only mental health outpatientand day treatment facility is available at the
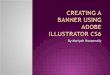
Himalayan Institute Trust Hospital nearDehradun. The dimension of the described lackof trained staff becomes most visible if com-pared to a Western country of the same size androughly the same amount of inhabitants such asSwitzerland.
per 10,000 population World S-E Asia India Uttarkhand SwitzerlandTotal Psychiatric Beds 1.69 0.33 0.25 Nil 13.2Psychiatric beds in mental hospitals 0.33 0.03 0.05 Nil 13.2per 100,000 population World S-E Asia India Uttarkhand SwitzerlandNumber of psychiatrists 1.2 0.2 0.2 0.08 23Number of neurosurgeons 0.2 0.03 0.06 Nil 0.8Number of psychiatric nurses 2.0 0.1 0.05 Nil 46Number of neurologists 0.3 0.05 0.05 Nil 3.4Number of psychologists 0.6 0.03 0.03 0.01 40.8Number of social workers 0.4 0.04 0.03 Nil 106
Table. 1: Psychiatric Beds and Professionals in Mental Health (Sources: for Uttarkhand WHO 2006: 6, for Switzerland WHO 2005: 449)
Thus, in the years 2005/06 there were 287.5times more psychiatrists in Switzerland than inUttarakhand, and 4080 times more psycholo-gists, not to speak of the trained social workersof which Switzerland has more than one per1000 inhabitants while Uttarakhand has nonefor more than 8,5 million inhabitants. Despitethe fact that Switzerland is a comparatively richWestern country, it does not take much imagi-nation to see that there is an enormous mis-match between the infrastructure within whichpsychiatric medicines and the respective thera-peutic interventions are planned, tested andimplemented in other parts of the world, suchas India, where they are transplanted into acompletely different infrastructure. The lack ofinfrastructure and time are two of the mostimportant reasons for the psychiatrists’ almostexclusive use of prescription drugs for thetreatment of the “mentally ill” in places likeUttarakhand. Other aspects of mental health-care such as psychotherapy, social work, or self-help groups were non-existent inUttarakhand in 2010. Studies on the quantitiesand ways in which psychotropic drugs are pre-scribed in India have been conducted, forexample, by Baby et al. (2009), Ecks and Basu(2009) and Jain and Jadhav (2009). The ques-tion as to why psychiatrists rely almost exclu-sively on pharmaceutical or somatic interven-tions in psychiatric settings has been addressedhead-on by Nunley (1996) and Jain and Jadhav(2009). In addition to the lack of infrastructure
they highlight the importance of mental healthplanning and policy-making.
A further important observation is that patientsin India do not take drugs as prescribed. Anextensive review of the literature on compliance(e. g. Cohen, Ross et al. 2004; Cramer et al.2008; Elliott et al. 2008) leads to several obser-vations. Firstly, a whole series of problems areoften lumped together under the rubric of“compliance”. These include issues such as thepatient “health literacy”, the available healthcare alternatives, the multilayered realm ofdoctor-patient relationship and the debatesaround drug side effects. Secondly, this set ofproblems results in forgone health benefits, newhealth problems and increasing productivitycosts. A number of patients, for example, dis-continue antipsychotics after some time becausethey do not feel relief from symptoms like hallu-cinations or delusions and, additionally, themedications can be quite expensive. The under-lying problem is that the antipsychotic medi-cines they got only show efficacy after two toeight weeks of continuous and correct intake.The Indian patients, some of whom have ageneralized perspective on biomedicine as being“fast” and “aggressive” (see also Halliburton2009: 14, 116, 190-195), are therefore unlikelyto spend a considerable amount of money onmedicines that appear ineffective to them.
Although the set of problems generally summa-

17
rized under the rubric “compliance” is enor-mous the world over there are two reasons whythis issue has to be highlighted especially in thepresent case. Firstly, psychotropic medicationsrepresent the mainstay of treatment in India.Kumar and Sedgwick (2001: 280) argue thatthis is the case in countries with emerging anddeveloping economies in general. Secondly,there are many reasons why patients do notfollow the treatment regime as proposed by thedoctor, i. e. why “non-compliance” is particu-larly high in settings such as this one. Thereforeit is crucial to investigate the larger phenome-non of “compliance” (or “adherence”), particu-larly with a focus on the patients’ perspectives.The research in India by Quack further sug-gests that a significant factor is counseling byhealth professionals, including the adequacy oftheir communication and gained trust (see alsoChue 2004; Eley et al. 2006). Of central impor-tance is the fact that the patients’ perspectiveson the origins, central aspects and probableways of addressing their problems are more orless ignored by psychiatrists. These and relatedobservations are supported by Baby et al.(2009) who argue that the majority of noncom-pliant patients in India are less educated, andlive in rural areas. The follow-up counseling forthese patients is limited in scope as the psychia-trists are typically overburdened with heavypatient load. Family members and patients arereluctant to ask questions about their medica-tion and treatment and most of their doubtsremain unaddressed. The majority of the psy-chiatrists interviewed in Uttarakhand attri-buted non-compliance to the patients’ lack ofmental health “awareness”. They described howsome patients have generalized prejudices aboutpsychotropics such as the idea that bio-medi-cine is fast and aggressive and hence thepatients stop medication if there is no immedi-ate effect. The psychiatrists hardly reflected onthe question whether the differences in educa-tion and habitus were also a hindrance to theirtreatment approach. Such observations shouldnot be taken as criticism of the psychiatristsgiven the time pressure under which they haveto work and the fact that they are trained innatural and not social sciences. The challengesthey face every day are considerable. Forexample, the doctors do not only have to trans-late from medical terminology to everydayspeech, from English to Hindi and further – often via a third person – to Garhwali (the
language spoken by most of the people living in the northern Garhwal Division ofUttarakhand). But they generally also have totranslate from the logic of the Western text-books to the local realities of the patients. The“Western” psychiatric system only works if thepatients are able to understand and follow theunderlying therapeutic logic. This is often notthe case in Uttarakhand, not only becausepatients are at times not able to read and write,but, more importantly, because the approach of the Western-educated urban middle-classdoctor clashes with the “habitus” of thepatients. Addlakha, whose research producedsimilar findings as those presented here, con-cluded: “For Indian practitioners, medicaltraining is a double socialization, that is, intopsychiatric nosologies and treatment regimes,and into the culture of biomedicine. […] Thechallenge to indigenous professional practi-tioners, trained in a system that has developedin the context of an alien society and culture,but applying it to their own societies, is to nego-tiate their own commonsensical understandingwith the so-called objective and universalsdiscourse of the biomedical model.” (2006: 265-266)
This is much less true when one looks at thetraditional healing sector in India. In thisrespect the statement about the lack of mentalhealth infrastructure has to be qualified. Thefacts and figures about the number of psychia-trists, hospitals, beds, etc. in India take intoaccount only some aspects of mental healthcare. Mental health authorities and publichealth research nearly always ignore the signifi-cance of therapeutic alternatives for the main-stream medical system. The former head of the Psychiatry Department at the All-IndiaInstitute of Medical Sciences, New Delhi, andWHO consultant Jaswant Singh Neki estimatedin 1973 that around 80% of the Indian popula-tion approaches “folk” practitioners and“traditional” healing centers for treatment ofmental health problems (see Pakaslahti 1998:129). This figure has been subsequently con-firmed by various other studies (see Kapur1975, 2004; Campion and Bhugra 1997: 215;Shah 1984: 737; De Sousa and De Sousa 1984:6). India has a network of health practitionersoperating outside the institutionalized health-care system, often outside the purview of healthprofessionals (see Pakaslahti 1998: 129). This

18
“traditional” healing system provides the bulkof care and support for those who suffer frommental health and substance-dependenceproblems. On the question of the relationshipbetween the “traditional” alternatives favouredby psychiatric patients in India, there areseveral good anthropological studies (see forsimilar findings Basu 2009a,b, 2010a,b; Bibeauand Corin 2009, 2010). The first comparativeapproach addressing this question is providedby Incayawar et al. (2009).
Practically all Indian psychiatrists that Quackspoke to were partially aware of the observa-tions listed above. On the other hand, thispartial awareness had no bearing on their pro-fessional practice. Despite the fact that ininterviews and every-day conversations mostpsychiatrists questioned the exclusive prescrip-tion of drugs, complained that far too manypatients failed to take medicine as prescribed,and confirmed the importance of engaging withthe patients’ and healers’ explanatory models,religious beliefs and practices, these “insights”had few if any further consequences. Why doesthe everyday knowledge of psychiatrists notinfluence their professional practice? Ourhypothesis, to be developed in future publica-tions, is that they are faced with a dilemma: onthe one hand, psychiatrists want to stay true totheir professional training while on the otherhand this stance sometimes conflicts with thelocal realities. The cultural psychiatristFabrega summarizes his as well as the findingsof the anthropologist Nunley (1996) with thefollowing words: “To act like a doctor in Indiais to take an epidemic view, deal rapidly with aheavy patient load, quickly make provisionaldisease diagnoses, and prescribe drugs. To han-dle problems that are brought to them in anyother way would make psychiatrists less likeother doctors and more like gurus, spiritualcounselors, or faith healers, which are not whatpsychiatrists in India want to be.” (Fabrega2009: 614)
The fact that the therapists generally tend toprivilege abstract, professional knowledge overknowledge gathered in their every-day lives(lebensweltliches Wissen) is well recognized.This can reach such extent that the professio-nals become structurally blind to or “misrecog-nize” (in Bourdieuian terms) problems thatappear to be clearly visible from an outsider’s
perspective. It was observed, for example, thatpsychiatrists often prescribe medicines thatthey (should) know the patients cannot afford.They also often condemn religious beliefs andpractices they themselves adhere to in theirprivate lives. Furthermore, when asked aboutthe relevance of issues related to “culture” intheir practice, the “culture-bound syndromes”as listed in the international manuals come totheir mind, but not the many ways in whichthese manuals do not fit their therapeuticrealities. Grundmann et al. (2008) convincinglyargue that this discrepancy is the more pro-nounced the higher the perceived asymmetrybetween professional and every-day knowledge.With respect to India, it is important to notethat “Western” psychiatry is one of many colo-nial relics that unfolds with specific dynamics inthe post-colonial context (Ananth 1981; Bhugra2001; Bhugra and Littlewood 2001; Jadhav2004; Fabrega 2009). “Western medicine” or“English medicine” (as it is also called in India)continues to carry high prestige and is oftenopposed to “superstition” and “backwardness”.
Such factors help to explain why the psychia-trists studied in India do not engage with thoseexperiences and understandings of theirpatients which feature non-biomedical interpre-tations of their problems such as social circum-stances, relationship problems, broken taboos,or further religious explanations. Accordingly,many patients turn to the therapies of traditio-nal healers who engage with such issues.
The second part of Quack’s project attempts tocompare the ethnography of psychiatric prac-tices in North India with similar studies in dif-ferent cultural contexts. We lack comparativestudies of the many ways in which psychiatry is practiced in different local settings. Suchstudies would help us to identify commonalitiesand differences between local psychiatries,especially in non-Western countries, and thiscould represent the basis for improving mentalhealth services. Quack plans to research theways in which his observations on the practiceof psychiatry in India can be compared tosimilar studies in other countries in 2012 whenhe will become a research fellow at the Divisionof Social and Transcultural Psychiatry, McGillUniversity, Montreal. The aim of the project isto contribute to a more comprehensive under-standing of how different cultural contexts

19
shape, transform, or even corrupt psychiatricpractices by engaging with ethnographies ofpsychiatry that take into account the psychia-trists’, patients’ and care-givers’ experiencesand perspectives. A “radically empirical”(ethnographic) approach is crucial, since thedescriptive language prevalent in standard“Neo-Kraepelinian” (Gone and Kirmayer 2010)depictions of psychiatric practices tends to hidecultural differences while projecting apparentlyuniversal features.
Contemporary Ayurvedic Nosology and theInfluence of Biomedicine
The spread of biomedicine to India in the 19thand 20th century did not fail to have an impacton the indigenous scholarly medical tradition ofAyurveda. Chopra’s project on the nosology ofcontemporary Ayurveda aims to analyze thecomplex processes brought about by this tran-scultural flow. Nosology has been chosen as theobject of research because this is the part ofmedicine where practice is intimately related tothe theory of the relevant “medical system”.When the physicians assess signs and symptomsof the patient and classify them so as to nameone or more disease(s), they apply the cate-gories of their medical system to the realities ofdiseased patients and at the same time themedical system is confronted with the realitiesof disease. Therefore, one can assume thatchanging medical realities have an impact firstand most clearly on a medical system’s nosolo-gy. The study of nosology may thus also offerinsights into patterns of change within a partic-ular medical system. To research these process-es, Chopra combined field-work in Ayurvedicclinics in India with a study of contemporaryscientific literature of Ayurveda; in addition,results of historical-philological research, atleast on the major historical works of theAyurvedic tradition, had to be surveyed,because Ayurveda is typically defined as atraditional science and physicians as well aslearned authors constantly refer to traditionalliterature (Zimmermann 1978).
A most conspicuous effect of the influence ofbiomedicine on Ayurveda is the process termed“professionalization” (Leslie 1998 ?1976?),which in the course of the last century hasresulted in the institutionalization of Ayurvedaalong the lines of biomedicine. Thus, Ayurveda
is presently taught in colleges according to acentrally sanctioned curriculum and Ayurvedicphysicians obtain their own registration andform their own professional associations, toname just the most visible effects. These deve-lopments in the institutional representation ofAyurveda clearly reflect an asymmetry withbiomedicine as the dominant partner. However,when we go beyond these external representa-tions and ask if and how biomedical conceptshave influenced the practice and the scholarlyaspect of Ayurveda, the picture becomes morecomplex. As medical systems in general can beconsidered practical sciences, research shouldat best include practice as well as scholarlytheory in order to do justice to a learnedmedical system like Ayurveda.
Two short periods of field-study in two very dif-ferent Ayurvedic clinics in India reveal thatthere is noticeable diversity in the practice ofAyurveda in India. The first such study wasconducted over five months at a reputed mod-ern academic institution of Ayurveda in northIndia, which to a large extent is typical of con-temporary “professionalized” Ayurveda, whilethe second field-study took place for aboutthree months in the clinic of a highly respectedtraditional Ayurvedic physician in south-westIndia.
The presence of biomedicine is clearly felt inboth institutions, thus in both institutionsreports of biomedical (laboratory) tests areroutinely taken into consideration when dia-gnosing a patient and they are sometimes evenspecifically asked for. In the clinic of the acade-mic institution even external elements of theclinical encounter resemble those of biomedicalinstitutions, so that the physicians, for example,often wear white coats and carry a stethoscope.In the traditional clinic, on the other hand, theconsultation takes place in more family-likecircumstances and the physician, who happensto be a high-caste Brahmin, wears his tradition-al attire and his main diagnostic techniques arelooking at the patient and questioning him,while he rarely palpates e. g. the abdomen of apatient in the case of abdominal swellings orliver-enlargement.
Documentation in the professionalized institu-tion routinely takes place in English, eventhough the conversation with the patient is usu-

20
ally in Hindi. In many cases, though notalways, even the diagnostic category noteddown is drawn from the biomedical nomencla-ture. Although there is a dispensary ofAyurvedic medicines produced in the universityitself, where patients could procure medicines,the doctors show a clear predilection for pre-scribing the so-called “proprietary” Ayurvedicmedicines, pharmaceuticals produced by com-panies on the basis of traditional Ayurvedicrecipes, which are modified to a greater orlesser extent and thus become the “property” ofthe company. This process of prescription andsubsequent procurement of industrially pro-duced medicines from an (Ayurvedic) pharmacymight also be seen as an emulation of biomed-ical patterns. During the Chopra’s own field-research in this institution of professionalizedAyurveda, the prescription of biomedical drugsby physicians trained in the institutionalizedAyurveda, described as a frequent practice inthe literature, was witnessed only very rarely.
With respect to these practices the differencebetween the clinic of the professionalizedAyurvedic institution and the traditional physi-cian seems to be most pronounced. In the tradi-tional physician’s clinic the diagnosis is routine-ly noted down as an Ayurvedic disease-name(Sanskrit in Malayalam script), with the Englishbiomedical disease name sometimes noted inaddition. Interesting to note is that at times thispractice implies a translation which is tacitlyperformed. Thus, when asked about his prob-lem, a young male patient replies that he hasbeen diagnosed with ulcerative colitis, employ-ing the English disease name in the course of aconversation taking place in Malayalam. Thephysician’s assistant notes down the Ayurvedicdisease name grahan. ı without any discussion.However, such acceptance of a biomedical diag-nostic category, and its translation into anAyurvedic one, is not a common practice in thisclinic. In most cases the physician insists onmaking his own, Ayurvedic diagnosis on thebasis of his own diagnostic means, even if thepatient presents him with a biomedical diseasename. On the basis of this diagnosis the physi-cian then dictates his prescription, usually con-sisting of numerous herbal preparations of dif-ferent kinds (decoctions, powders, oils, pastesetc.) and their combination, all of which isnoted down by the assistant. While dictating theprescription the physician very often recites
Sanskrit verses from classical texts (most oftenfrom the As.t.an. gahr.dayasam. hita, but also fromthe As.t.an. gasam. graha, the Sahasrayogam, theCikitsamañjari and others), describing the for-mulation and the indications of the respectivepreparation. Almost all of the preparations thathe prescribes are found in the classical texts,the rest consisting of variations of classical for-mulations created by the physician himself.While prescribing these classical herbal reme-dies, the physician commonly combines ormixes the preparations so as to suit the needs ofthe individual patient. To make the clinicalencounter complete, a factory for these herbalpreparations also belongs to the estate of thistraditional physician. Therefore, the patientsusually take the prescription to the physician’sown dispensary where the remedies and theirspecific combinations are prepared for them.These freshly combined individual preparationsare then taken home by the patient, togetherwith a couple of typed pages containing infor-mation on how to take the medicines andincluding dietetic advice, too.
As these short sketches of two differentinstances of Ayurvedic consultations show,there is a marked diversity in the actual clinicalpractice of Ayurveda. However, when it comesto the question of the impact of biomedicine onAyurveda and specifically to the question ofhow biomedicine influences Ayurvedic nosology,one finds that the differences between differentcontemporary practitioners of Ayurveda are not as great as suggested by the observation ofpractice. Taking a close look at the way diseasesare presently named and conceptualized, wemay roughly distinguish three patterns.
The first pattern is represented by the rareinstance where a modern biomedical disease isaccepted as being a separate disease, not regu-larly found in the traditional Ayurvedic litera-ture. A case in point may be hypertension(“high blood-pressure”), which is mostly accept-ed as a separate disease and then even translat-ed into Ayurvedic parlance by being accorded a“new” Sanskrit name. (Although there is diver-sity here, too, see Chopra n.d.)
The second pattern is seen at the other extreme,that is, the Ayurvedic disease-entities continueto exist in their own identity. An example of thisfrom the practice of the traditional Ayurvedic

21
physician in south-west India is the disease-entity usually called raktavata by him (in theliterature it is more often known as vatarakta);this comprises symptoms such as lower backpain and pain in the knee-joints. In these casesthe physician ostentatiously refused to look atbiomedical diagnostic reports (e. g. CT-scans,MRI-scans, X-ray-films) even if the patientsbrought them along. Instead, he examined theknees and the skin of the legs in accordancewith the description of this disease-entity in theclassical texts: needless to say, the therapy,too, followed the classical Ayurvedic lines. As is to be expected, this pattern of a classicalAyurvedic disease-entity retaining its own iden-tity is more frequently seen in the traditionalAyurvedic practice than in the practice of pro-fessionalized Ayurveda.
However, the third and by far the most commonpattern in both types of contemporaryAyurvedic practice is characterized by a com-plex process of translation on the basis ofcorrespondences between modern biomedicaldiseases and classical Ayurvedic disease-entities. Although this process has clearly per-ceptible bearings on everyday practice, onemight perhaps get a clearer idea of this kind ofprocess by taking a look at textbooks and other literature produced by contemporaryAyurvedic scholars. Studying the ways in whichdiseases are defined, classified and described intypical contemporary text-books of Ayurveda,one notices a translation-process on differentlevels: firstly, there is translation in the popularsense of the word, meaning linguistic transla-tion; secondly, and more importantly, there istranslation based on disease-symptoms; andthirdly, we find attempts at translating physio-logical concepts. As an example the diseasenamed prameha may be cited, a disease namewell known from the Ayurvedic tradition, start-ing with the earliest extant texts (for a criticalhistorical discussion of this disease-entity seeMüller 1932). A number of disease-conditionscharacterized by excessive discharge of urineand/or abnormalities of urine are subsumedunder this term (the classical theory mostlyknows of twenty different types of prameha)which can be translated literally as “excessiveurination”. Nowadays this term has becomealmost synonymous for the biomedical disease-entity of diabetes mellitus and is very oftendefined by the biomedical parameters that
define that disease. Thus the traditional physi-cian in south-west India routinely asks hispatients if they suffer from prameha, using thisSanskrit term in his (Malayalam) conversationand if the answer is affirmative, he asks for theresult of the latest blood sugar test (referring tothe result of a biomedical laboratory test).Clearly to him as well as his patients the termprameha is synonymous with the disease that isdefined by an abnormally elevated level ofblood sugar. This identification of pramehawith diabetes mellitus is partly enforced by thefact that the Greek term diabetes like theSanskrit term prameha means “excessive urina-tion”; in addition, at least one of the varieties ofprameha described in classical Ayurvedic textsis characterized by an excessive discharge ofsweet urine, usually referred to as madhumeha,the meaning of which corresponds to the bio-medical term diabetes mellitus, viz., “excessivedischarge of honey-sweet urine”. (One mightnote in passing that in this case the biomedicaldisease name reflects a historically older stagein the history of modern biomedicine.) Thus,this translation based on the similarity of symp-toms coincides with a semantic similarity ofdisease terms from different medical cultures.By narrowing down the meaning of prameha tosignify what in traditional scholarship is onlyone of its numerous varieties, namely the condi-tion of discharging sweet urine, the termbecomes synonymous with diabetes mellitus.This process of translation creates wider reper-cussions in the nosological system: prameha inthis new understanding is the Ayurvedic termfor diabetes mellitus, but this particular form ofprameha is not counted among the diseases ofthe urinary tract any more, where it would beplaced according to classical Ayurvedic ideas ofthe disease-process. Rather, it becomes a meta-bolic disease and is treated as such, albeit withAyurvedic means.
This example shows that biomedical conceptshave at times a formative influence on the for-mulation of contemporary Ayurvedic theoryand thus this seems like a clear instance ofasymmetrical translation demonstrating thedominance of biomedicine. However, if we takea closer look at the process of translation that iscarried out here and ask ourselves why suchgreat pains are taken to effect a translation inthe first place (would it not be easier to justtake over biomedicine wholesale as it is and not

22
bother about translations?) this clear-cut judg-ment becomes fuzzy. In general, the process oftranslation presupposes that the target languageis, at least broadly, as capable of expressingfacts as the source language is. Or, to apply thiscommonplace notion to the case at hand, thepresupposition here is that the science ofAyurveda and its idiom are as capable of con-ceptualizing diseases as modern biomedicine is.Taking this idea further, we cannot avoid askinghow the contemporary proponents of Ayurvedaview the status of their own science vis-à-visbiomedicine. Considering the fact that biomedi-cine with its close relationship to the modernnatural sciences has a strong if not exclusiveclaim to being based on and representing scien-tific truth, the question arises what the ontolog-ical status of Ayurveda and its own epistemolog-ical foundation would be in relation to biomedi-cine. Surveying the writings of contemporaryproponents of Ayurveda (mainly text-bookswritten by learned authors in modern Indianlanguages like Simha 1994-2001, Shukla 1997)and discussing this question with Ayurvedicdoctors personally, one comes to notice a ratherunexpected kind of asymmetry, according towhich it is the science of Ayurveda as embodiedin the tradition which is actually representingtrue and complete knowledge. Or, as a highlyrespected retired professor of Ayurveda point-edly formulated it, “Ayurveda is a developedscience while modern medicine is a developingscience” (Ram Harsh Singh, Varanasi, personalcommunication, March 2010). This idea isbased on a classical notion of science, which isdeeply rooted in Indian culture (and has beendescribed by Pollock [1985] in a seminalarticle). According to this classical notion, asastra, a “traditional science” is true and com-plete; it is “primordial” as it is typically said tohave been revealed by the creator himself. Thisconcept is often combined with a narrative ofparts of the science having become lost in thecourse of history; any kind of scientific progressis in this context understood to be only a redis-covery of lost parts of the sastra. This narra-tive is not limited to the traditional sciences ofthe Indian culture but is also reflected in ageneral historical discourse which forms part ofthe so called renaissance of Indian culture inthe 19th and 20th century (cf. Leslie 1992 and1998). A recurring motif in this discourse is thenotion of an ancient golden era of the Indianculture, the achievements of which were lost or
even suppressed during the intervening era offoreign dominance (first by Muslims, thenEuropeans, to put it simply). So if contempo-rary proponents of Ayurveda identify themodern biomedical disease-entities with classi-cal Ayurvedic diseases, they are re-constitutinglost knowledge and at the same time taking partin the larger cultural project of reclaiming analleged golden era of Indian culture.
Thus, we see that in addition to the apparentdominance of biomedicine there is a differentkind of asymmetry, one that is perhaps not aseasily perceptible as the first one, in whichAyurveda happens to be the dominant partner.Ayurveda thus incorporates biomedical ideas bytranslating them into its own system withoutgiving up fundamental Ayurvedic notions. Seenfrom a more traditional perspective the pro-cesses sketched above would be described as an incorporation of biomedical ideas into the – true and complete – science of Ayurveda andnot as an example of biomedical influences onit. For the status of Ayurveda and its contempo-rary proponents this means that they stronglyassert the validity of their own medical tradi-tion in this age when biomedicine is dominant.The fact that the arguments for this propositioncoincide with and are enforced by a larger dis-course in contemporary Indian society remindsus that even developments in the seeminglyautonomous field of medicine cannot be viewedin isolation from the social and political con-text. In this context one should not forget thatbiomedicine and Ayurveda in contemporaryIndia not only compete for scientific validity,but also for political influence and finances.Presently, it is biomedical institutions thatreceive by far the largest share of publicfinances.
Conclusion
In the two projects presented here the com-plexity of the translation processes involved inthe transcultural flow of biomedicine is clearlyevident. These processes of translation areinformed by the scientific concepts of biomedi-cine as much as by concepts of the respectiveother medical system, be it lay-concepts of psy-chic disease as in the case of psychiatry in ruralnorth India or scholarly concepts of Ayurveda.Cultural and social circumstances might enforcecertain aspects of these translations as well as

23
economic factors, such as the allocation ofpublic spending on health. In the long termthese translation processes might even changethe face of biomedicine and result in very localmanifestations of an allegedly global scientificmedical system.
References
Addlakha, R. (2008) Deconstructing mental illness: Anethnography of psychiatry, women and the family.New Delhi: Zubaan.
Ananth, J. M. D. (1981) Is western training relevant toIndian psychiatry? In: Indian Journal of Psychiatry23, 2: 120-127.
Baby, R. S., Gupta, S., Sagar, R. (2009) Attitudes andsubjective reasons of medication compliance andnoncompliance among outpatients with schizophre-nia in India. In: Internet Journal of Epidemiology7, 1.
Basu, H. (2009a) Contested practices of control:Psychiatric and religious mental health care inIndia. In: Curare 32, 1+2: 28-39.
Basu, H. (2009b) Schmutzige Methoden: Geisteskrankdurch Besessenheit und schwarze Magie inGujarat/Indien. In: A. Malinar, M. Voehler (eds.)Un/Reinheit: Konzepte und Erfahrungsmodi imKulturvergleich. München: Fink Verlag, 47-66.
Basu, H. (2010a) Besessenheitskrankheit undPsychiatriereform in der indischen Moderne. In: D. Schulz, J. Seebode (eds.) Spiegel und Prisma.Ethnologie zwischen postkolonialer Kritik undDeutung der eigenen Gesellschaft. Hamburg:Argument Verlag, 195-209.
Basu, H. (2010b) Healing madness through ritualtrials. In: K. Leonard, G. Reddy, A. G. Gold (eds.)Histories of intimacy and situated ethnography.Delhi: Manohar, 215-38.
Bhugra, D. (2001) The colonized psyche: Britishinfluence on Indian psychiatry. In: D. Bhugra, R. Littlewood (eds.) Colonialism and psychiatry.New Delhi: Oxford University Press, 46-76.
Bhugra, D., Littlewood, R. (eds.) (2001) Colonialismand psychiatry. New Delhi: Oxford UniversityPress.
Bibeau, G., Corin, E. (2009) Turning many into one:Mental health at the junction of classic Hindu texts, religious practice, and modern psychiatricknowledge. In: B. Sébastian (ed.). Restoring mentalhealth in India: Pluralistic therapies and concepts.New Delhi: Oxford University Press, 285-310.
Bibeau, G., Corin, E. (2010) Dr Ravi L. Kapur (1938-2006): A psychiatrist at the crossroads ofmultiple worlds. In: Transcultural Psychiatry 47, 1:159-180.
Campion, J., Bhugra, D. (1997) Experiences of reli-gious healing in psychiatric patients in South India.In: Social Psychiatry and Psychiatric Epidemiology32, 4: 215-221.
Chopra, A.S. (n.d.) Disorder of blood, disorder ofmind: Conceptualizing essential hypertension incontemporary Ayurveda. In: H. Naraindas, J. Quack, W. Sax (ed.) Ideologies of health (forth-coming).
Chue, P. (2004) Compliance and convenience: Dophysicians and patients see depot medication differ-ently? In: Acta Neuropsychiatrica 16: 314-318.
Cohen, N. L., Ross, E.C., Bagby, M., Farvolden, P.,Kennedy, S.H. (2004) The 5-factor model of person-ality and antidepressant medication compliance. In:Canadian Journal of Psychiatry 49, 2: 106-113.
Cramer, J. A., Roy, A., Burrell, A., Fairchild, C.J.,Fuldeore, M.J., Ollendorf, D.A., Wong, P.K. (2008)Medication compliance and persistence:Terminology and definitions. In: Value in Health11, 1: 44-47.
De Sousa, A., De Sousa, D. A. (1984) Psychiatry inIndia. Bombay: Bhalani.
Desjarlais, R., Eisenberg, L., Good, B., Kleinman, A.(1996) World mental health: Problems and priori-ties in low-income countries. New York, Oxford:Oxford University Press.
Ecks, S., Basu, S. (2009) The unlicensed lives of anti-depressants in India. Generic drugs, unqualifiedpractitioners, and floating prescriptions. In:Transcultural Psychiatry 46, 1: 86-106.
Eley, D., Hunter, K., Young, L., Baker, P., Hunter, E.,Hannah, D. (2006) Tools and methodologies forinvestigating the mental health needs of indigenouspatients: It’s about communication. In:Australasian Psychiatry 14, 1: 33-37.
Elliott, R. A., Shinogle, J. A., Peele, P., Bhosle, M.,Hughes, D. A. (2008) Understanding medicationcompliance and persistence from an economics per-spective. In: Value in Health: International Societyfor Pharmacoeconomics and Outcomes Research11, 4: 600-610.
Fabrega Jr., H. (2009) History of mental illness inIndia: A cultural psychiatry retrospective. Delhi:Motilal Banarsidass Publishers.
Gaines, A. D. (ed.) (1992) Ethnopsychiatry: The cul-tural construction of professional and folk psychia-tries. Albany: State University of New York Press.
Gone, J. P., Kirmayer, L. (2010) On the wisdom of con-sidering culture and context in psychopathology. In:T. Millon, R. F. Kruger, E. Simonsen (eds.)Contemporary directions in psychopathology:Scientific foundations of the DSM-V and ICD-11.New York: Guilford Press, 72-96.
Grundmann, M., Bittlingmayer U.H., Dravenau, D.,Groh-Samberg, O. (2008) Bildung als Privileg undFluch: zum Zusammenhang zwischenlebensweltlichen und institutionalisiertenBildungsprozessen. In: R. Becker, W. Lauterbacher(eds.) Bildung als Privileg: Erklärungen undBefunde zu den Ursachen der Bildungsungleichheit.Wiesbaden: VS Verlag, 47-74.
Halliburton, M. (2009) Mudpacks and Prozac:Experiencing ayurvedic, biomedical and religioushealing. Walnut Creek: Left Coast Press.

24
Higginbotham, H. N. (1984) Third world challenge topsychiatry. Honolulu: University of Hawaii Press.
Incayawar, M., Wintrob, R. et al. (eds.) (2009)Psychiatrists and traditional healers: Unwittingpartners in global mental health. London: WileyBlackwell.
Jadhav, S. (2004) How culture bound is “cultural”psychiatry? http://www.indianpsychiatry.com/CulturalPsych.htm [May 7, 2008].
Jain, S., Jadhav, S. (2008) Cultural critique of commu-nity psychiatry in India. In: International Journalof Health Services 38, 3: 561-584.
Jain, S., Jadhav, S. (2009) Pills that swallow policy:Clinical ethnography of a community mental healthprogram in Northern India.
Kapur, R. L. (1975) Mental health care in rural India:A study of existing patterns and their implicationsfor future policy. In: British Journal of Psychiatry127: 286-293.
Kapur, R. L. (2004) The story of community mentalhealth in India. In: S. P. Agrawal (ed.) Mentalhealth: An Indian perspective 1946-2003. NewDelhi: Ministry of Health and Family Welfare, 92-100.
Kleinman, A. (1977) Depression, somatization and thenew cross-cultural psychiatry. Social Science andMedicine 11, 1: 3-10.
Kumar, S., Sedgwick P. (2001) Can the factorsinfluencing medication compliance reported fromwestern populations be applied to an EasternIndian context? Part I. Journal of Mental Health10, 3: 267-277.
Leslie, C. (1992) Interpretations of illness: Syncretismin modern Ayurveda. In: C. Leslie, A. Young (eds.)Paths to Asian medical knowledge. Berkeley, LosAngeles, Oxford: University of California Press,177-208.
Leslie, C. [1998] (1976) The Ambiguities of medicalrevivalism in modern India. In: C. Leslie (ed.)Asian medical systems: A comparative study. 1stIndian edition. Delhi: Motilal Banarsidass, 356-367.(Indian Medical Tradition Vol. III).
Müller, Reinhold F. G. [2008] (1932) Die Harnruhr derAlt-Inder, Prameha (unter besonderer
Berücksichtigung der Carakasamhita). SudhoffsArchiv für Geschichte der Medizin 25: 1-42.(Reprinted in Müller, R. F. G. (2008) KleineSchriften zur traditionellen Medizin Südasiens,hrsg. von Rahul Peter Das. Wiesbaden:Harrassowitz Verlag: 116-157).
Nunley, M. (1996) Why psychiatrists in India prescribeso many drugs. In: Culture, Medicine andPsychiatry 20, 2: 165-197.
Pakaslahti, A. (1998) Family-centered treatment ofmental health problems at the Balaji tempel inRajasthan. In: A. Parpola, S. Tenhunen (eds.)Changing patterns of family and kinship in SouthAsia. Helsinki: Studia Orientalia, 129-166.
Pollock, S. (1985) The theory of practice and the prac-tice of theory in Indian intellectual history. In:Journal of the American Oriental Society 105, 3:499-519.
Quack, J. (2011, forthcoming) Disenchanting India:Organized rationalism and criticism of religion inIndia. New York: Oxford University Press.
Shah, V. D. (1984) Mental health service in India. In:A. De Sousa, D. A. De Sousa (eds.) Psychiatry inIndia. Bombay: Bhalani, 733-756.
Shukla, V. (1997) Ayurvedıya Vikçti Vijñana.(According to the syllabus of Central Council ofIndian Medicine, New Delhi). 4th edition. Delhi:Chaukhamba Sanskrit Pratishthan (VrajajıvanaAyurvijñana Granthamala 5).
Simha, R. (1994-2001) Kayacikitsa. 2 Vols. Dillı:Caukhamba Sanskrit Pratishthan (VrajajıvanaAyurijñana Granthamala 21).
Watters, E. (2010) Crazy like us: The globalization ofthe American psyche. New York: Free Press.
WHO (2005) Mental health atlas. http://www.who.int/globalatlas/default.asp. [May 8, 2008].WHO (2006) Who-Aims report on mental health system
in Uttarkhand, India. Dehradun: World HealthOrganization and Ministry of Health Dehradun,Uttarkhand, India.
Zimmermann, F. (1978) From classic texts to learnedpractice: Methodological remarks on the study ofIndian medicine. In: Social Science and Medicine12: 97-103.
Introduction
Less than a century ago Western medicalscience developed the concept “stress” which,after the Second World War, was rapidly takenup and disseminated by the mass media andsince then permeates everyday discourse (Young1980: 133). In Western Europe and NorthAmerica, stress is the dominant trope on the
predicament of modern fast-paced and success-oriented societies, especially in the context ofmodern work. About one out of four Europeanworkers reports having to work at very highspeed all or almost all the time, and in the USAone out of four workers complains about beingfrequently burned out or stressed by his or herjob (European Foundation for the Improvementof Living and Working Conditions 2006).
Stress and Modern Work: Ethnographic Perspectivesfrom Industries in Bangladesh
Christian Strümpell, Hasan Ashraf