-
8/7/2019 Asthma Clinical Guide
1/29
Building Healthy Lifestyles
Chronic Respiratory
AsthmaClinical Guide
Building
Lifestyles
Healthy1-866-506-6654
388-6654
-
8/7/2019 Asthma Clinical Guide
2/29
Asthma
Building Healthy LifestylesChinook Health Region 2
We would like to acknowledge the contribution of the following
groups:
Chronic Respiratory Interdisciplinary Working Group
Chronic Disease Physician Advisory Group
Chronic Disease Clinical Leadership Group
Specialist Consultants
Chronic Respiratory Clinical Champions
CHR Asthma Program Committee
Utilizing the Chronic Care model, these groups developed the
Asthma Clinical Guide as a decision-support tool for improved
functional and clinical outcomes. is Guide supports primary
care
interdisciplinary team-based practice with a strong focus on
self-management.
Please use and reproduce with acknowledgement to the Chinook
Health Region.
Chronic Disease Management and Prevention Network:An Alberta
Health Capacity Building Initiative
Chinook Health RegionLethbridge, Alberta
April 2006
-
8/7/2019 Asthma Clinical Guide
3/29
Asthma
Building Healthy LifestylesChinook Health Region 3
Table of Contents
1. Diagnosis
a. Definition
............................................................................................................5b.
Risk Factors
.........................................................................................................5c.
Screening
.............................................................................................................6d.
Signs and Symptoms
............................................................................................6e.
Testing and Evaluation
........................................................................................6f.
Further Testing
....................................................................................................7g.
Algorithm
............................................................................................................8
2. Classification/Type/Staginga. Stages/Types of Disease
........................................................................................11
3. Patient Care Flow Sheet for Health Teams
a. Patient Care Flow Sheet
......................................................................................13b.
Key Clinical Summary
.........................................................................................14
4. Management Strategies for Health Teamsa. Goals of Management
..........................................................................................15b.
Key Clinical Targets
.............................................................................................15c.
Non-Pharmacologic Strategies
.............................................................................15d.
Pharmacologic
Strategies......................................................................................16
5. Management Strategies for Patients/Clientsa. Self-Care
Support Information/Handouts/Tools
.................................................21b.
Patient/Client Checklist for Evidence-Based Care
................................................25
6. Referral to Specialists/Specialty Programa. Indications for
Referral to Medical Specialists
......................................................27b.
Indications for Referral to Specialty Programs
......................................................27c. Local
Contacts
.....................................................................................................27
7. Referencesa. Evidence
..............................................................................................................29b.
On-line Resources
...............................................................................................29c.
Supplementary Handouts Available
.....................................................................29
-
8/7/2019 Asthma Clinical Guide
4/29
Asthma
Building Healthy LifestylesChinook Health Region 4
-
8/7/2019 Asthma Clinical Guide
5/29
Asthma
Building Healthy LifestylesChinook Health Region 5
1. Diagnosis
BUILDING HEALTHY LIFESTYLESCHRONIC RESPIRATORY-ASTHMA
Unless clinical practice guidelines are followed, the danger of
bothunder- and over-diagnosis exists. e interpretation and
availabilityof tests to assess variable airway obstruction is
inconsistent. Becauseof the variable nature of the disease over
time, the tests for airwayobstruction and hyper-responsiveness may
not reveal a problem evenwhen asthma exists.
1. Diagnosis
a. Definitions:
Asthma: is characterized by paroxysmal or persistent
symptomssuch as dyspnea, wheezing, chest tightness, sputum
production andcough associated with variable airflow limitation and
airway hyper-responsiveness to endogenous or exogenous stimuli.
Exercise Induced Bronchospasm (EIB): is a reversible
airwayobstruction that occurs during or after strenuous physical
exertion.Solitary EIB is not asthma and it is important to
distinguish if exerciseinduced symptoms are the result of poorly
controlled asthma.
EIB versus Asthma
A therapeutic trial is a practical way to confirm EIB. e
clienttakes B-2 agonists, 15 minutes prior to exercise; the EIB
diagnosis isconfirmed if the medications prevent or diminish
symptoms. echallenge is to distinguish whether or not the patient
has asthma
with an exercise exacerbation or has solitary EIB. Because
treatmentis different for these two conditions, it is important to
evaluatethe patient for asthma using patient history, physical exam
andpulmonary function tests (spirometry).
Occupational Asthma (OA) is asthma induced by exposure to
aspecific agent in the workplace; is the most common
occupationallung disease in developed countries. OA has been
estimated to cause5 15 % of adult onset asthma.
An occupational cause should be suspected for all new cases
ofasthma in adults
Temporal associations are not sufficient to diagnose
work-related
asthma and objective tests are required to confirm the
diagnosis.Workers with asthma symptoms should not be told to leave
theirjob until diagnosis is proven because part of the diagnostic
work-up of OA may involve a return trial to work.
Referral to a medical specialist for evaluation of OA
Irritant-induced Asthma is caused by single or multiple
exposuresto high concentrations of an irritant vapour, fume or
smoke in peoplewho have no previous diagnosis or history of asthma
symptoms. Teterm Reactive airways dysfunction syndrome or RADS is
used
when the condition is caused by a single exposure.
Reactive Airways Disease (RADS) is poorly defined, confusing
andshould not be used in lieu of possible or probable Asthma.
b. Risk Factors
Major risk factors:i. Personal history of atopy, especially
atopic dermatitisii. Parental history of asthma or eczemaiii. ree
or more episodes of wheeze during the first three years
of life
Minor risk factors:i. Eosinophiliaii. Wheezing without colds
iii. Allergic rhinitisiv. Environmental tobacco smoke (ETS)
OCCUPATIONAL ASTHMA (OA)
Highest risk occupations and asthma-producing substances
OCCUPATION ASTHMA-PRODUCINGSUBSTANCES
Adhesive handlers Chemicals such as acrylate
Animal handlers, vets, researcher Animal proteins
Bakers, Millers Cereal Grains
Carpet makers Gums
Electronic workers Soldering resin
Forest workers, Carpenters,Cabinet makers
Wood dust
Hairdressers Chemicals such as persulfate
Healthcare professionals Latex and chemicals such
asglutaraldehyde
Janitors, Cleaning staff Chemicals such as chloramine-T
Pharmaceutical workers Drugs, enzymes
Seafood processors Seafood
Shellac handlers Chemicals such as amines
Solderers, Refiners Metals
Spray painters, Insulationinstallers, Plastic & Foamindustry
workers
Chemicals such as diisocyanates
Textile workers Dyes
Users of plastics, epoxy resins Chemicals such as anhydrides
-
8/7/2019 Asthma Clinical Guide
6/29
Asthma
Building Healthy LifestylesChinook Health Region 6
1. Diagnosis
c. Screening
ere is currently no organized approach to screening for asthma
inCanada.
d. Signs and Symptoms
Asthma
Coughing
Wheezing
Chest tightness
Shortness of breath
Trouble sleeping because of breathing difficulty
Reduced physical activity due to breathing difficulty
EIB:
Coughing, wheezing, shortness of breath and chest tightness
immediately following 6 to 8 minutes of strenuous exercise.ese
symptoms may occur during or after exercise.
e. Testing and Evaluation
Evaluation and diagnosis of asthma in clients able to
performlung function tests (Usually 6 years of age and older):
ere is no one definitive test that can be used to diagnose
asthma,requiring the bringing together of many sources of
information inorder to reach such a diagnosis. At the present time,
diagnosingasthma is based on the following:
the presence of typical symptoms of asthma and an
improvement
in these symptoms with asthma medication evidence of variable
airflow limitation and/or obstruction
in some circumstances, evidence of hyper-responsiveness of
theairways using a provocation challenge test
Steps in primary care setting to accurately diagnosis asthma,
suspectasthma based on symptoms, physical exam and patient
history.Next, confirm diagnosis through lung function tests
showingvariable airflow obstruction and/or response to trial of
asthmamedications.
orough history: covering symptoms and pattern of symptomsas well
as what triggers the symptoms. Personal history of atopy
(eczema, hay fever, hives, allergic rhinitis, allergies) and
familyhistory of atopy or asthma in close relatives.
Physical exam: should focus on upper respiratory
airway(nasopharynx) and lower respiratory airway (chest) as well
asthe skin. Physical exam may help confirm the diagnosis ofasthma,
but does not generally provide the diagnosis. Physicalexam alone
tends to underestimate the severity of an asthmaexacerbation.
Co-morbid conditions such as rhinitis, sinusitis,post nasal drip or
Gastroesphageal Reflux Disease (GERD) thatmimic or worsen asthma
symptoms should be evaluated andaddressed.
Findings with asthma that may be present are: use of accessory
muscles of respiration tracheal tug indrawing hyperinflation of the
chest decreased air entry
prolonged expiration wheezing wheeze with forced expiration
silent chest
Lung function tests (2 types): Objective measurements areneeded
to confirm the diagnosis of asthma and to assess itsseverity
accurately in all symptomatic patients.
i. Spirometry (preferred method)- A 12% (at least 180 mL in
adults) or greater improvement in
Forced Expiratory Volume (FEV)1.0 15 minutes (10 minutesis more
practical and used in the LRH PFT lab) after use ofan inhaled
short-acting beta-2 agonist will confirm diagnosis
of asthma*- A 20% (at least 250mL in adults) or greater
improvement in
FEV1.0 after 10-14 days of inhaled glucocorticosteriods
oringested prednisone, when symptoms are stable will
confirmdiagnosis of asthma
- A 20% (at least 250 mL in adults) or greater
spontaneousvariability in FEV1.0 over time is considered
significant and
will confirm the diagnosis of asthma
ii. Peak Expiratory Flow or PEF (used when spirometry
isunavailable or home monitoring is required to diagnose)
- Variable airflow obstruction can be documented by homemeasured
PEF that shows a 20% or greater diurnal variability
over a period of several weeks. is can confirm thediagnosis of
asthma.
- A 20% or greater improvement in PEF, 15 minutes (10minutes is
more practical) after the administration of a shortacting beta-2
agonist may be used to confirm asthma in aphysicians office when
spirometry is not available.
- Both these methods are not as reliable as spirometry.
erapeutic trial of asthma medications, which should
includeInhaled Corticosteroids (ICSs) daily and short-acting B-2
agonistas needed for a period of 2-4 weeks may be helpful in
confirmingthe diagnosis of asthma.
Evaluation and diagnosis of asthma in clients unable to
performlung function tests (Usually less than 6 years of age):
NOTE: ere are no age criteria for the diagnosis of asthmaas it
can be diagnosed at any age. However, caution should beused when
diagnosing asthma in clients less than one year ofage. Persistent
respiratory symptoms in infants and children may
warrant a referral to a specialist.
e diagnosis rests on careful and sometimes repeated
historytaking and physical examination as stated above
*Please note- in children age 6-17 only a 12% improvement in FEV
1.0 isrequired after bronchodilator.
-
8/7/2019 Asthma Clinical Guide
7/29
Asthma
Building Healthy LifestylesChinook Health Region 7
1. Diagnosis
Factors particularly useful in establishing a diagnosis in
youngpatients: severe episodes of wheezing wheezing after 1 year of
age more than 3 episodes of wheezing in a given year family history
of asthma/atopy
personal history of asthma/atopy maternal smoking clinical
benefits from acute bronchodilator therapy clinical evidence of
improvement after anti-inflammatory
treatment chronic cough (especially nocturnal or associated
with
exercise) wheezing when viral etiology is unlikely
e likelihood of a diagnosis of asthma increases with the
numberof these factors present.
Clinical Index for the Diagnosis of Asthma
Stringent Index: 3 or more episodes of wheeze during the first3
years of life with either one of the major riskfactors: parental
history of asthma or eczema, or2 of 3 minor risk factors;
eosinophilia, wheezing
without colds, allergic rhinitis
Loose Index: any wheezing during the first 3 years of life plus
1major or 2 minor risk factors
Clinical Clues to Alternate Diagnosis
Not asthma: poor response to therapy after ensuring
compliancewith trigger avoidance strategies, proper inhaler use and
compliance
with medical treatment. No history of atopy. Cystic fibrosis:
malabsorption, finger clubbing, nasal polyps
Pertussis: paroxysmal cough, ill contacts
Rhinitis/Sinusitis: no wheeze, throat clearing
Gastroesophageal Reflux (GER): previous regurgitation,
nighttime
Congenital malformation: age under one year
Foreign Body: sudden onset without Upper Respiratory
Infection(URI), focal findings
f. Further Testing
Referral to a medical specialist for bronchoprovocation testing
tohelp confirm or rule out asthma.
Appropriate allergy assessment is warranted in patients
withasthma and must be interpreted in light of patients
history.
Allergen exposure is a risk factor for severe, acute
asthma,especially if the patient is exposed to high concentrations
ofthe specific allergen. erefore, allergens to which a personis
sensitized should be identified through allergy testing.Once
identified, steps should be taken to eliminate or at
leastsubstantially reduce allergen exposure.
-
8/7/2019 Asthma Clinical Guide
8/29
Asthma
Building Healthy LifestylesChinook Health Region 8
1. Diagnosis
g. Algorithms
Approach to Asthma Diagnosis in Clients Able to Perform
Spirometry Tests
Reliably (usually 6 years of age or greater) in the Primary Care
Setting
Suspect asthma based on symptoms, patient history & physical
exam
Confirm diagnosis of asthma with Pre & Post Spirometry
Testing
Is there a >12% improvement in Forced ExpiratoryVolume FEV1.0
(of at least 180ml in adults 18+) 10 YES
minutes after short-acting bronchodilator*
Asthma diagnosis confirmedInitiate treatment & asthma
education(Referral to asthma educator)
Does pre & post spirometry test meet the following criteria
to be considered normal FEV1.0/FVC ratio > 0.7 FVC > 80% of
predicted value FEV1.0 > 80% of predicted value
NO
If FVC is < 80% predicted andFEV1.0/FVC ratio is > 0.7
Post bronchodilator FEV1.0/FVCratio is < 0.7bronchodilator
FEV1.0 is < 80%predicted
If post bronchodilatorFEV1.0/FVC ratio is < 0.7
Consider diagnosis of restrictivelung defect not consistent with
adiagnosis of asthma - referral to aspecialist may be warranted
Diagnosis of COPD can beconfirmed alone or co-existing
withasthma
Consider diagnosis of irreversibleobstructive lung defect
Is client currently symptomatic
YES NO
and post
Initiate proper COPD treatment
Initiate proper asthma therapy ofinhaled corticosteroids and
short-acting bronchodilators for one monththen follow up and
reassess
Repeat spirometry if and whensymptoms recur to confirmdiagnosis
of asthma or dismissdiagnosis of asthma
YES NO
Clinical benefits after proper asthmatherapy?
Asthma diagnosis may be confirmedConsider re-test with
spirometryInitiate treatment and asthmaeducation (referral to an
asthmaeducator)
Referral to a specialist for bronchoprovocation testing to help
confirm / rule out diagnosis of asthand investigate other
conditions that mimic asthma (i.e. Gastroesophageal Reflux Disease
(GEvocal cord dysfunction)
Notes:
FVC is forced vital capacity, FEV1.0 is forcedexpiratory volume
in 1 second.
Normal predicted values in spirometry are availablefor people 5
years of age and older. No normalpredicted values exist for
children younger than 5
years of age. Some children as young as 5 can givereliable
spirometry testing. Therefore, this may needto be decided by the
person performing the test.
*
NO YES
In children age 6 - 17 only a 12% improvement in
FEV1.0 10 minutes after a short-acting bronchodilator
is required to confirm a diagnosis of asthma.
-
8/7/2019 Asthma Clinical Guide
9/29
Asthma
Building Healthy LifestylesChinook Health Region 9
1. Diagnosis
Approach to Asthma Diagnosis in Clients Able to Perform Peak
Expiratory Flow TestsReliably (usually 6 years of age or greater)
in the Primary Care Setting
Suspect asthma based on symptoms, patient history & physical
exam
Spirometry is not available
(Spirometry is the preferred method according to the CPGs)
Confirm Diagnosis of asthma with Peak Expiratory Flows (PEF)
YES NO YES
Is client currently symptomatic
YES
YES NO
Note: PEF is less reliable than spirometry for confirming the
diagnosis of asthmaTo calculate a 20% improvement in PEF following
administration of a short-acting B-2 agonist:
1. Obtain a peak flow reading prior to medication, e.g. 400
lpm2. Multiply that number by 1.2 to give value needed to confirm a
20% improvement in PEF (400 x 1.2 = 480).3. Give B-2agonist, wait
10 minutes then repeat PEF; this value must be > 480 lpm to show
a 20% improvement in
PEF and confirm diagnosis of asthmaTo calculate diurnal
variation of PEF:
1. Client is to measure peak flows in the am and pm of each day
for 2-4 weeks and record the best value of 3 triesin a diary
2. Once this data has been recorded, calculate the diurnal
variation of each day by using the following formula:Highest PEF
Lowest PEF (on the same day) x 100
Highest PEFFor example: Day 1 Day 2 Day 3
PEF am pm am pm am pm400 500 400 450 350 500
500 400 x 100 450 400 x 100 500 350 x 100500 450 500
= 20% diurnal variation = 11.1% diurnal variation = 30% diurnal
variation Children as young as 5 years of age may be able to
properly perform PEF. There are no predicted values for
childrenunder 5 years of age for peak flow.
>20% improvement in PEF 10 minutes afteradministration of
short-acting B-2 agonist
>20% or greater diurnal variability in PEFover a period of
several weeks
Asthma diagnosis confirmedInitiate treatment and asthma
education
(referral to an asthma educator)
Asthma diagnosis confirmedInitiate treatment and asthma
education
(referral to an asthma educator)
Initiate proper asthma therapy of inhaledcorticosteroids and
short-acting bronchodilatorsfor one month then follow up and
reassess
Repeat PEF if and when symptoms recur
Clinical benefits after proper asthma therapy
Asthma diagnosis may be confirmedConsider retesting with
spirometryInitiate treatment and asthmaeducationConsider a referral
to an asthmaeducator
Consider a referral to have pre & post spirometry done or
referral to aspecialist for bronchoprovocation test to help confirm
/ rule outasthma diagnosis and investigate other conditions that
mimic asthma(i.e. Gastroesophageal Reflux Disease (GERD), vocal
corddysfunction).
-
8/7/2019 Asthma Clinical Guide
10/29
Asthma
Building Healthy LifestylesChinook Health Region 10
1. Diagnosis
Approach to Asthma Diagnosis in Clients Unable to Perform
Reliable
Pulmonary Function Tests (less than 6 years of age) in the
Primary Care Setting
Suspect asthma based on symptoms, patient history & physical
exam
First, determine the presence of airway sensitivity by inquiring
about symptoms such as cough,wheeze, limited physical activity,
chest tightness and shortness of breath.
Second, look for evidence of inherited ability to react to
stimuli - is there a family history of atopyand a personal history
of eczema or atopy.
Third, establish that there is no underlying lung disease - look
for anything else that could becausing cough.
Therapeutic trial of asthma medications to confirm diagnosis of
asthma in preschool children
OR
Reassess response to asthma therapy in child Did Beta-2 agonist
provide relief from wheeze, chest tightness and SOB? Did cough
subside after one month of inhaled corticosteroids? Did cough
subside after 5 days of oral prednisone?
YES NO
NOTE- there is no age criteria for the diagnosis of asthma as it
can be diagnosed at any age. However,caution should be used when
diagnosing asthma in children less than one year of age.
Persistentrespiratory symptoms in infants and children may warrant
a referral to a specialist.
Asthma diagnosis may be confirmedespecially if symptoms recur
whenmedications are stoppedInitiate treatment and asthma
educationReferral to an asthma educator
Consider an alternate diagnosisConsider a referral to a
Pediatrician
Beta-2 agonists for relief of symptoms such as wheeze, chest
tightness and shortness of breath (SOB)
AND
Inhaled Corticosteroid for coughing for a period of one
month
Oral prednisone for therapeutic trial for coughing, 1mg/kg per
day up to a maximum of 50 mg x 5 days
CAUTION: ensure child is not incubating varicella virus. A
comprehensive varicella history should bedone
-
8/7/2019 Asthma Clinical Guide
11/29
Asthma
Building Healthy LifestylesChinook Health Region 11
2. Classification/Type/Staging
2. Classification/Type/Staging
Determining the Severity of Asthma
Assessment of asthma severity will help physician
determineappropriate level of therapy required, as well as when a
client
should be referred to a specialist.
e severity of asthma can be evaluated in two ways:
1. Before or without treatment which takes into accountsymptoms,
physiological indicators of airway disease (lungfunction tests) and
morbidity.
2. With treatment or when controlled asthma amount ofmedication
required to maintain control.
e primary measure of asthma severity in the treated
patientshould be the minimum therapy required to achieve
acceptablecontrol.
-
8/7/2019 Asthma Clinical Guide
12/29
Asthma
Building Healthy LifestylesChinook Health Region 12
2. Classification/Type/Staging
Asthma severity before or without proper treatment
Event or measurement Mild Moderate Severe
FEV1.0 or PEF, % of predicted >80% 60 79%
-
8/7/2019 Asthma Clinical Guide
13/29
Asthma
Building Healthy LifestylesChinook Health Region 13
Asthma Patient Care Flow Sheet Patient Name
Comorbid Conditions PHN
Year of Diagnosis
DATE: _________ _________ _________ ________ _________
_________
REVIEW ITEMSNeeds reliever medication 4 times/week(may use 1
dose/day for exercise)
Physical activity limited by symptoms (in past 3 months)(Sx:
coughing, wheezing or chest tightness)
Symptoms wake patient at night 1 times/week
Symptoms 4 days/week
Any urgent visits for asthma since last regular appointment
Absence from work/school because of asthma
(in last 3 months)
lortnoCamhtsA
*Client must answer all with NO to have Control , if Yes to one
or more questions asthma is not controlled reassess
Smoker or secondhand smoke in the home/vehicles. If yesaddress
smoking (ask, advise, assist, arrange 4As)
Identified asthma triggers:
Have steps been taken to reduce exposure to asthma triggers
ecnadiovAreggirT
A client that is not reducing exposure to allergens and asthma
triggers will be difficult to control. Referral to asthma
program
Does client have a written asthma action plan
* If not, provide a written CHR asthma action plan
Client understands how to use the asthma action plan
Is controller medication used regularly?Controller
medications:
Reliever Medications:
Economic Concerns (cost of meds):
ecnailpmoC
Have patient demonstrate how they use their inhaler
device(s)
*Ensure Proper Inhaler Technique
Sx of GERD, Rhinitis, Sinusitis
Asthma meds that may affect other diseases
(Prednisone use, test blood glucose)
Sx of depression, anxiety
ISIV
ECIFFO
RALUGER
AMHTSA
ROF
ST
seitidibromo
C * If any comorbidities exist with asthma, treat appropriately
as these may affect proper asthma control
Perform Pre & Post Spirometry testing yearly &
prnstseT
Height and weight (especially for pediatrics)BMD for
osteoporosis (If on ICSs and has risk factors)
Review asthma action plan, try to reduce medication required
while maintaining asthma control
Referrals: Asthma educatorfor education & evaluation
for initial education & follow up as needed
Medical Specialist as needed
YLLAUNNA
tnemeganaM
Vaccinations: Annual Influenza vaccine
Pneumoccocal vaccine if > 65 years
Immunizations up to date
Revised as of May 9, 2005 developed by the BHL/chronic
respiratory/ Chinook Health Region
3. Chronic Disease Patient Care Flow Sheet
3. Chronic Disease Patient Care Flowsheet
-
8/7/2019 Asthma Clinical Guide
14/29
Asthma
Building Healthy LifestylesChinook Health Region 14
3. Patient Care Flow Sheet
Asthma Continuum of Care Reliever (Rescue) medications
Salbutamol (Ventolin) MDI 100 mcg per dose 1 or 2 inhalations as
needed Salbutamol (Ventolin) Diskus 200 mcg per dose
Adults & children 6 and older, 1 inhalation as needed
Terbutaline (Bricanyl) Turbuhaler 0.5 mg per dose
Adults & children 6 and older, 1 inhalation as needed
Salbutamol (Airomir) MDI 100 mcg per dose 1 to 2 inhalations as
needed
Inhaled Corticosteriods (Preventer/controller medications)ICSs
should be introduced as the initial maintenance treatment for
asthma,even in subjects who have very mild asthma and use their
relievermedication less than 3 times/week. Refer to chart on left
for proposeddoses for ICSs Fluticasone (Flovent) MDI 50, 125 &
250 mcg per dose
BID dosing most effective Fluticasone (Flovent) Diskus 50, 100,
250, 500 mcg per dose BID dosing most effective Budesonide
(Pulmicort) Turbuhaler 100, 200 & 400 mcg per dose BID dosing
most effective
Daily Long Term Inhaled Steroid Agents and Doses Beclomethasone
(Q-var) MDI 50 & 100 mcg per dose BID dosing most effective
Add on Therapy if requiredIf asthma is not controlled by low
doses of ICSs, additional therapyshould be considered:FIRST OPTION
Add long-acting beta2 agonist to existing therapy ofICSs and
short-acting beta 2 agonists, or replace ICSs with a
combinationmedication. Salmeterol (Serevent) MDI 25 mcg per dose
Adults 1 or 2 inhalations BID
Children 4 years of age and older 1 or 2 inhalations BID
Salmeterol (Serevent) Diskus 50 mcg per dose
Adults 1 inhalation BIDNote: children will auto scale their
inhaled medication dose, (take Children 6 years of age and older 1
inhalation BIDsmaller inspiratory volumes which results in less
dose reaching the Formoterol (Oxeze) Turbuhaler 6 or 12 mcg per
doselower airways) the same dose can be used for all asthma
medications Adults 1 inhalation of 6 or 12 mcg BID (max 48 mcg per
day)at all ages. Children 6-16 1 inhalation of 6 or 12 mcg BID (max
24 mcg day)FP= Fluticasone propionate (GSK Canada Inc)
ORBUD= Budesonide (AstraZeneca Canada Inc) Advair (Serevent 50
mcg/Flovent 100, 250 & 500 mcg per dose) DiskusBDP=
Beclomethosone dipropionate (3M Pharmaceuticals Canada) Adults and
children 12 and older, 1 inhalation BID
Children 6-11 years of age, 1 inhalation BID Advair (Serevent 25
mcg/Flovent 125 & 250 per dose) MDI
Adults and children 12 and older, 1 or 2 inhalations BID
Children 4 years of age and older, 1 or 2 inhalations BID
Symbicort (Oxeze 6 mcg/Pulmicort 100 & 200 mcg per dose)
Turbuhaler Adults and children 12 years of age and older, 1 or 2
inhalations BID
Children 6 to 11 years of age, 1 or 2 inhalations BIDSECOND
OPTION- Increase the inhaled corticosteriods (ICSs) to amoderate
dosage as per chart or add in a leukotriene receptor antagonist.
Montelukast (Singulair) 4, 5 & 10 mg chewable tablet Adults and
children 15 years of age and older one 10 mg tablet daily
at bedtime Children 6 to 14 years of age one 5 mg tablet daily
at bedtime Children 2 to 5 years of age one 4 mg tablet daily in
the evening
Zarfirlukast (Accolate) 20 mg tablet
Adults and children 12 years of age and older two 20 mg tablets
daily
THIRD OPTION consider theophylline, severe asthma may
requireadditional treatment with Prednisone. If required to
maintain control, referto the CPS for dosing requirements &
refer to medical specialist.
Prednisone for acute exacerbations of asthma, use the
followingdosages:
For ages 12 and over: 50 mg po daily for 3-10 days
For ages under 12: 1mg/kg po daily for 3-10 days (maximum dose:
2
mg/kg po daily)No Prednisone dose tapering required if less than
2 weeks
Treatment options from the Canadian Asthma Consensus Guidelines
update 2003, medications updated as of January 12, 2006
Mcg/day (all ages)
Low Medium HighProduct
BUD TurbuhalerPulmicort
FP pMDI and spacerFlovent
FP DiskusBDP pMDI (HFA)
Q-varBUD wet nebulization
< 400
< 250
< 250< 250
< 1000
401 800
251 500
251 500251 500
1001- 2000
> 800
> 500
> 500> 500
> 2000
Asthma Severity based on treatment needed to obtain control
Asthma Severity Symptoms Treatment required
Very mild Mild-infrequent None, or inhaled short-acting B-2
agonist rarely
Mild Well-controlled Short-acting B-2 agonist(occasionally) and
low doseinhaled steroids
Moderate Well-controlled Short-acting B-2 agonist andlow to
moderate doses ofinhaled steroids with orwithout add on therapy
Severe Well-controlled Short-acting B-2 agonist andhigh doses on
inhaledsteroids and add on therapy
Very severe May be Short-acting B-2 agonist andcontrolled or not
high doses of inhaledwell-controlled steroids and add on
therapy
and oral steroids
-
8/7/2019 Asthma Clinical Guide
15/29
Asthma
Building Healthy LifestylesChinook Health Region 15
4. Management Strategies for Health Teams
a. Goals of Management
To maintain acceptable asthma control use nonpharmacologic
andpharmacologic strategies. Asthma control is defined under
KeyClinical Targets.
b. Key Clinical Targets
Criteria for asthma control
Parameter Frequency or value
Daytime symptoms less than 4 days/week
Night-time symptoms less than 1 night/week
Physical activity Normal
Exacerbations Mild, infrequent
Absence from work/school None
Need for short-acting beta-2 agonist Less than 4 doses/week*
FEV1.0 or PEF > 85% of personal bestIdeally 90%
PEF diurnal variation < 15% of diurnal variation
*May use 1 dose/day for prevention of exercise-induced
symptoms
To be considered controlled asthma, all the above criteria
mustbe met. If they are not met, it is then considered
uncontrolledasthma.
Control can be achieved in uncontrolled asthma through
patient
education, trigger avoidance and medications.
c. Non-Pharmacologic Strategies for Asthma
Environmental Control:
Elimination of exposure to environmental tobacco smoke (ETS)
Identification of asthma triggers and implement triggeravoidance
strategies
Allergy testing to identify allergens to which a person
issensitized; once these allergens are identified, steps shouldbe
taken to eliminate or at least substantially reduce
allergenexposure
Current recommendations for protecting against developmentof
allergy and asthma in subsequent pregnancies and
subsequentchildren:1. Elimination of exposure to ETS (includes
during pregnancy)2. Promotion of exclusive breast feeding for at
least 4 months3. For families with biparental atopy, maternal
asthma or both,
it appears that there is substantive data to recommend againsthe
presence of a cat or dog in the home
IMPORTANT! Medication should not be substituted forenvironmental
control and trigger avoidance strategies.
Asthma Action Plan:
Devise a written action plan for the management ofexacerbations
that includes medication adjustment in responseto changes in
severity or frequency of symptoms, the need forsymptom relief
medication or changes in PEF. Provide the
written document or ask an asthma educator to do so. Pleaserefer
to Section 5, subsection a for a copy of the CHR Asthma
Action Plan.
Education and Follow-up:
Education is an essential component of asthma therapy and
shouldbe offered to all patients. Educational interventions may be
ofparticular benefit to patients with high asthma-related morbidity
or
severe asthma and at the time of emergency department visits
andadmissions to hospital.
All patients should self-monitor their asthma using symptoms
orPEF or both
Ensure regular follow-up (every 6 months). Asthma
controlcriteria should be assessed at each visit. Measurement
ofpulmonary function, preferably spirometry, should be
doneregularly in adults and children 6 years of age and older.
Review
written action plan and medication required with an aim toreduce
amount of medication while maintaining asthma control.
Smoking Cessation:
Smoking cessation interventions (4A model) should be offeredto
patients who smoke, or parents of children with asthma
whosmoke.
Influenza vaccination:
All patients with asthma should be encouraged to have an
annuainfluenza vaccination, as well as any family members living
withpatient (parents & siblings).
4. Management Strategies for Health Teams
-
8/7/2019 Asthma Clinical Guide
16/29
Asthma
Building Healthy LifestylesChinook Health Region 16
4. Management Strategies for Health Teams
Immunotherapy in Adults:
Immunotherapy is generally not recommended in the treatmentof
asthma
Immunotherapy should not be used in place of avoidance
ofenvironmental allergens
Immunotherapy with clinically relevant allergens may
beconsidered if disease activity is inadequately controlled
byavoidance of allergens and pharmacotherapy
Immunotherapy should be avoided while asthma is
poorlycontrolled
Well-controlled asthma is not a contraindication
forimmunotherapy for allergic rhinoconjunctivitis or insect
venomhypersensitivity
Immunotherapy must be administered only by trained personnelin
centres where there is medical supervision and
resuscitativeequipment (for both children & adults)
Immunotherapy in Children: Although debate about the value of
immunotherapy continues,
meta-analysis and review of immunotherapy support thepotential
value of immunotherapy in childhood; earlyimmunotherapy may prevent
development of asthma in childrensensitized to house dust mite
allergen
Physicians should consider injection immunotherapy
usingappropriate allergens for the treatment of allergic asthma
only
when allergic component is well documented
Physicians should not recommend the use of
injectionimmunotherapy in place of avoidance of environmental
allergens
Physicians may consider injection immunotherapy in addition
toappropriate environmental control and pharmacotherapy whenasthma
control remains inadequate
Immunotherapy is not recommended when asthma is unstable
d. Pharmacologic Strategies for Asthma
First Line erapy:
Reliever medications rescue
Salbutamol (Ventolin) MDI 100 mcg per dose 1 or 2 inhalations as
needed
Salbutamol (Ventolin) Diskus 200 mcg per dose Adults 1
inhalation as needed Children 6 years and older 1 inhalation as
needed
Terbutaline (Bricanyl) Turbuhaler 0.5 mg per dose Adults 1
inhalation as needed Children 6 years and older 1 inhalation as
needed
Salbutamol (Airomir) MDI 100 mcg per dose 1 to 2 inhalations as
needed
AND
Inhaled Corticosteroids (ICSs) low dose maintenance
Regular use of low dose ICSs is currently the
recommendedtreatment for persons with asthma of all ages, even for
thosewith intermittent asthma symptoms
Physicians should recommend that children with frequentsymptoms,
severe asthma exacerbations or both receive regular,not
intermittent, treatment with ICSs
e use of intermittent treatment as a strategy for managementof
intermittent asthma in childhood is not validated and
requiresfurther research especially in very young children
For patients who cannot or will not use ICSs,
leukotrienereceptor antagonists (LTRAs) should be the primary
treatmentchoice, although they are less effective than low dose
ICSs Fluticasone (Flovent) MDI 50, 125 & 250 mcg per dose
BID dosing most effective
Fluticasone (Flovent) Diskus 50, 100, 250, 500 mcg per dose BID
dosing most effective
Budesonide (Pulmicort) Turbuhaler 100, 200 & 400 mcg perdose
BID dosing most effective
Beclomethasone (Q-var) MDI 50 & 100 mcg per dose BID dosing
most effective
-
8/7/2019 Asthma Clinical Guide
17/29
Asthma
Building Healthy LifestylesChinook Health Region 17
4. Management Strategies for Health Teams
Dose equivalencies for inhaled corticosteroids - ICSs (All
ages)
Product
Low
Daily Dose (mcg/day)Moderate
High
BUD turbuhaler < 400 401 - 800 > 800
FP pMDI and spacer < 250 251 - 500 > 500FP Diskus < 250
251 - 500 > 500
BDP pMDI (HFA) < 250 251 - 500 > 500
BUD wet nebulization < 1000 1001 - 2000 > 2000
BDP= Beclomethasone dipropionate (Q-var)BUD= Budesonide
(Pulmicort)FP= Fluticasone propionate (Flovent)* Note: Children
will auto-scale their inhaled medication dose, (take
proportionately smaller inspiratory volumes compared to adults,
whichresults in less of the dispensed dose of inhaled medication
reaching the lungs). e same dose can be used for all medications at
all ages.
Add on erapy as Required:
If after reassessment of compliance with treatment,
triggeravoidance strategies, inhaler technique and
co-morbidities,asthma is not controlled by low dose ICSs,
additional therapyshould be considered:
FIRST OPTION Add long-acting beta-2 agonist to existingtherapy
of ICSs and short-acting beta-2 agonist, or replace ICSs
with a combination medication.
Salmeterol (Serevent) MDI 25 mcg per dose Adults 1 or 2
inhalations BID
Children 4 years of age and older 1 or 2 inhalations BID
Salmeterol (Serevent) Diskus 50 mcg per dose Adults 1 inhalation
BID Children 6 years of age and older 1 inhalation BID
Formoterol (Oxeze) Turbuhaler 6 or 12 mcg per dose Adults 1
inhalation of 6 or 12 mcg BID (max 48 mcg per
day) Children 6-16 1 inhalation of 6 or 12 mcg BID (max 24
mcg day)
OR
Advair (Serevent 50 mcg/Flovent 100, 250 & 500 mcg per
dose)
Diskus Adults and children 12 and older, 1 inhalation BID
Children 6-11 years of age, 1 inhalation BID
Advair (Serevent 25 mcg/Flovent 125 & 250 per dose) MDI
Adults and children 12 and older, 1 or 2 inhalations BID Children 4
years of age and older, 1 or 2 inhalations BID
Symbicort (Oxeze 6 mcg/Pulmicort 100 & 200 mcg per
dose)Turbuhaler Adults and children 12 years of age and older, 1 or
2
inhalations BID Children 6 to 11 years of age, 1 or 2
inhalations BID
SECOND OPTION- Increase the inhaled corticosteroids (ICSs)to a
moderate dosage as per chart or add in a leukotriene
receptorantagonist (LTRAs)
Montelukast (Singulair) 4, 5 & 10 mg chewable tablet Adults
and children 15 years of age and older one 10 mg
tablet daily at bedtime Children 6 to 14 years of age one 5 mg
tablet daily at
bedtime Children 2 to 5 years of age one 4 mg tablet daily in
the
evening
Zarfirlukast (Accolate) 20 mg tablet
Adults and children 12 years of age and older two 20 mgtablets
daily
THIRD OPTION Consider theophylline; severe asthma mayrequire
additional treatment with prednisone. If required tomaintain
control, refer to the CPS for dosing requirements andrefer to a
medical specialist.
Prednisone:
For acute exacerbations of asthma, use the following
dosages:
For ages 12 and over: 50 mg po daily for 3-10 days
For ages under 12: 1mg/kg po daily for 3-10 days (maximumdose: 2
mg/kg po daily)
No Prednisone dose tapering required if less than 2 weeks
-
8/7/2019 Asthma Clinical Guide
18/29
Asthma
Building Healthy LifestylesChinook Health Region 18
4. Management Strategies for Health Teams
Management of Acute Asthma Exacerbations (excluding ER andacute
care facilities)
Acute asthma exacerbation is defined as deterioration of
asthmacontrol that is not responding to B-2 agonist rescue
treatment inthe usual manner or a sustained worsening of asthma
symptomsleading to increased use of B-2 agonists as well as
increased use ofmaintenance medications and/or supplementation with
additionalmedicine. e following are loose criteria that can define
an acuteasthma exacerbation:
Bronchodilator use 4 times/week (excluding 1 dose/day
forexercise)
Nocturnal awakenings due to asthma 2 times/week
Daytime asthma symptoms 4 days/week
Recent absence from work or school due to asthma
Recent unscheduled physician visit due to asthma
Spirometry testing shows FEV1.0 < 80% of predicted normal
PEF tests fall below 80% of personal best value, or
predictedvalue if personal best is not known
Studies have shown that the major cause (80%) of
asthmaexacerbations is viral upper respiratory infections. With
viralupper respiratory infections the inflammatory response tends
tobe more neutrophilic than eosinophilic. Inhaled
corticosteroidsmay not be effective during neutrophilic
inflammatory responsesseen with viral upper respiratory
infections.
Non-Pharmacologic Strategies:
Avoid contact with environmental tobacco smoke
Continue to avoid personal asthma triggers
Refer to personalized written asthma action plan as to how
totemporarily modify asthma medications
Pharmacologic Strategies:
Prevention of asthma exacerbations needs to be the primarytarget
of asthma treatment and ICSs. is can be accomplishedthrough regular
use of ICSs as maintenance treatment forasthma.
Previous asthma guidelines have recommended the use of anaction
plan to manage asthma exacerbations. Many of theseplans advocate a
doubling of the dose of maintenance ICS as
one of the first steps in the management of worsening
asthma.However, there are no randomized controlled trials to
supportdoubling the dose of ICS on identification of exacerbations
ofasthma.
2 recent studies (adult & pediatric populations) have
providedevidence that early or impending asthma exacerbations
arenot always effectively treated by doubling the dose of
inhaledcorticosteroids at the first sign of an exacerbation. ese
resultsapply to those patients with asthma who regularly use
theirpreventer or controller medication as maintenance therapy
when
well.
ere is some evidence for the potential benefit of a
moresubstantial increase in the dose of ICS such as tripling
orquadrupling the regular maintenance dose at the first sign of
anasthma exacerbation.
e standard of care is that ICS dose should be increased duringan
asthma exacerbation, but there is not enough good evidence
to make a generic recommendation as what dose to increase theICS
from the maintenance dose during the exacerbation.
rough the COPD & Asthma Network of Alberta (CANA),as well as
consulting local CHR specialists we have summarizedcurrent clinical
practices utilized by both pediatric and adultrespiratory
specialists throughout Alberta in managing acuteasthma
exacerbations: If the client is on high doses of ICS for
maintenance
(or maximum daily dosage for that client as decided
byphysician), the clinical practice is to double the
maintenancedose of ICS or maintain the current dose of ICS and add
ina long-acting beta agonist (LABA) or leukotriene receptor
antagonist (LTRA) for a period of approximately 2 weeks. If
client is on low to moderate doses of ICS for maintenance,
the clinical practice is to increase to the full dose of
thespecific ICS for approximately 2 weeks, then return
tomaintenance dose.
Full dose:
Fluticasone (Flovent) 500 1000 mcg/dayBeclamethasone (Q-Var) 400
800 mcg/dayBudesonide (Pulmicort) 800 1600 mcg/day
e clinical practice of many respiratory specialists is
toincrease the dose of ICS at the first sign of an exacerbation
and whether the dose is doubled or quadrupled depends onthe
clients maintenance dose as well as personal history
ofexacerbations. ose who become ill quickly upon exposureto
triggers treat more aggressively than those who generallymanage
trigger exposure without significant incident.
If the asthma exacerbation is not responding to increaseddoses
of ICS and add on therapy, a short course of oralprednisone should
be considered. Recommended doses:
For ages 12 and over: 50 mg po daily for 3-10 days
For ages under 12: 1mg/kg po daily for 3-10 days(maximum dose: 2
mg/kg po daily)
No Prednisone dose tapering required if less than 2 weeks
Te above evidence is based on the opinions of those who have
writtenand reviewed the asthma guidelines, based on their
experience,knowledge of the relevant literature and discussion with
their peers.
-
8/7/2019 Asthma Clinical Guide
19/29
Asthma
Building Healthy LifestylesChinook Health Region 19
Special Considerations:
Asthma in the Elderly
Diagnosis
A diagnosis of asthma should be more widely considered inelderly
patients with dyspnea, wheezing or nocturnal cough.
Asthma may be difficult to diagnosis in the elderly because
ofmisconceptions about its prevalence and also because
olderpatients have diseases and disorders that mask the classic
featuresof asthma.
Treatment
In the elderly patient with asthma, it is particularly important
totake a careful medication history. Use of self-prescribed ASA
hasbecome common and may go unrecognized. ASA and NSAIDSare
commonly prescribed in the elderly and may cause late-on-set
asthma. Oral and topical B-adrenergic blocking agents andother
anti-arrhythmic agents, including verapamil and others
with acknowledged B-blocker potential, can exacerbate or
causeasthma in those who are predisposed to the disease.
Wheneverpossible, medications that might induce or aggravate
asthmashould be withdrawn.
Special care should be taken to allow elderly patients with
asthmato choose an inhaler device with which they are both
comfortableand competent.
Measures should be taken to prevent osteoporosis in
elderlypatients with asthma who require prolonged treatment with
oralcorticosteroids.
Elderly patients with asthma require careful follow-up
becausethey have an increased risk for exacerbations, which may
be
related to impaired perception of their disease severity.
Asthma in Pregnancy
Asthma is present in 4 7 % of pregnant women and is
therespiratory disorder that most frequently complicates
pregnancy.
e course of asthma during pregnancy is variable and
asthmacontrol may remain unchanged or become worse or improveand
return to the pre-pregnancy state within 3 months
afterparturition.
Overall, asthma control improves significantly in the last 4
weeksof pregnancy.
Asthmatic, pregnant women have been variably reported tohave an
increased risk of pregnancy-induced hypertension, pre-eclampsia,
caesarean section, placenta previa and antepartum orpostpartum
hemorrhage.
Recommendations
Do not stop asthma therapy during pregnancy. Poorly
controlledasthma may affect maternal comfort, safety and
pregnancyoutcome for both mother and child. Several well
designedstudies have shown fewer adverse infant and maternal
outcomesthan those without therapy.
Physicians should discuss medication choices and the
rationalefor treatment plan; they should emphasize that the
treatmentprogram is considered to entail less risk than the
uncontrolledillness that could result in its absence.
e use of systemic glucocorticosteriods for severe
asthma,especially for prolonged periods, may be associated with a
greater
risk of pre-eclampsia, antepartum or postpartum hemorrhage,low
birth weight, preterm birth and hyperbilirubinemia.
Patients requiring systemic glucocorticosteroid therapy should
beconsidered to be in a higher risk pregnancy.
Treatment
Avoidance of allergic and non-allergic triggering factors
shouldbe the first form of therapy for asthma during pregnancy.
Treatment should take the same approach as the
non-pregnantpatient and may include inhaled B-2 agonists,
inhaledcorticosteroids, ipratropium bromide, cromolyn and
systemicsteroids. eophylline may increase nausea and reflux and is
less
desirable. ere is significantly less information about the
effectsof long-acting B-2 agonists and leukotriene inhibitors and
thereis less clinical experience with these drugs than with other
classesof drugs. ese drugs should be used only for patients
whoseasthma cannot be controlled using the more studied
therapies.
For drugs with a longer history of usage, there tends to be
moredata to support a lack of adverse effects. Use of most
commonasthma medications (B-2 agonists, theophylline,
cromolyn,inhaled glucocorticosteroids) during pregnancy has not
beenshown to be associated with increased perinatal risks
includingcongenital malformations.
Although no asthma medications can be considered proven
safe for use during pregnancy, the ones listed above are usedto
prevent the potential direct and indirect consequences
ofuncontrolled asthma.
e patient must be aware of the risks and benefits ofappropriate
asthma control and must give her informed consentto the therapeutic
approach recommended during pregnancy.
4. Management Strategies for Health Teams
-
8/7/2019 Asthma Clinical Guide
20/29
Asthma
Building Healthy LifestylesChinook Health Region 20
Inhalation Devices for drug delivery In Asthma
Metered Dose Inhalers (MDIs)
Metered Dose Inhalers can be used with any age group. A spacer
orchamber should be used with children and elderly adults. A
spacershould also be used if patient is receiving inhaled
corticosteroids.
Under one year of age - a valved spacer and face mask should
beused with MDI. (orange infant aerochamber with face mask)
From 2 to 6 years of age - a valved spacer and face mask
shouldbe used with MDI. (yellow pediatric aerochamber with
facemask)
More than 6 years of age - a valved spacer with a
mouthpieceshould be used, rather than a face mask. (blue
aerochamber)
Try to use a valved spacer with mouthpiece in children at
theearliest age it becomes feasible. is will eliminate
breathingthrough the nose and maximize the chance of increased
airwaydeposition in the lungs. It has been clearly shown in
children
that breathing through a mask via the nose decreases
lungdeposition by up to 67% compared with breathing through
amouthpiece using a jet nebulizer.
Dry Powder Inhalers (DPIs)
Dry Powder Inhalers can be used by most patients by the time
theyreach 5 years of age. Spacer devices are not required with
thesedevices. e two devices in Canada are the Turbuhaler and
theDiskus inhaler.
MDIs vs Nebulizers:
Wet nebulizers for home use are rarely indicated in the
management of asthma at any age. e wet nebulizer device
iscumbersome and expensive and for the amount of
medicationdelivered the most costly of all methods.
ree meta-analyses of studies in children and adults
evaluatingMDI and wet nebulization indicate that the use of MDI
witha chamber or spacer is associated with a more rapid onset
ofbronchodilation, shorter duration of emergency
departmenttreatment, fewer side effects and greater patient
preference. Morerapid and profound bronchodilation is achieved when
sufficientdoses are given with an MDI plus spacer than when
conventionaldoses are administered with a wet nebulizer.
Note: Proper inhaler technique must be taught to client.
Referralto an asthma education program can ensure this is done. ere
aredevices available to measure inspiratory flow rate to ensure
patientcan adequately use a DPI.
4. Management Strategies for Health Teams
-
8/7/2019 Asthma Clinical Guide
21/29
Asthma
Building Healthy LifestylesChinook Health Region 21
5. Management Strategies for Patients / Clients
5. Management Strategies for Patients / Clients
ASTHMA ACTION PLANPatient Name:
(Last and First) _______________________________
Date of Birth: _________________________________
GREEN ZONE
YOUR ASTHMA IS IN GOOD CONTROL IF:
You do not wheeze, cough, feel tight or have
trouble breathing with your usual activities,
with exercise, or at night.
You require your reliever medicine less than
three times per week
Your peak flow is
between ________ and ________
(80% to 100% of personal best)
Action:
Avoid your personal asthma triggersAvoid tobacco smoke
exposureYearly flu immunization
Watch for asthma symptoms
If you have symptoms with exercise take
___________ 15 minutes beforehand and remember
to warm up and cool down with exercise
Check your peak flow _______ per day
Controller(s): ____________________________
____________________________
Reliever(s): ____________________________
____________________________
Other Actions: ____________________________
YELLOW ZONE
YOUR ASTHMA CONTROL IS DECREASING IF:
You wheeze, cough, feel tight or have
trouble breathing with your usual activities,
with exercise or at night
You develop cold symptoms
You require your reliever medicine more than
three times per week
Your peak flow is
between ________ and ________
(60% to 80% of personal best)
Action:
Avoid your personal asthma triggers
Avoid tobacco smoke exposure
Check your peak flow _______ per day
if not already doing so
Controller(s): ____________________________
____________________________
Reliever(s): ____________________________
____________________________
Other Actions: ____________________________
____________________________
Seek medical attention if your asthma control isnot improving
within 2 or 3 days
ORANGE ZONE
YOUR ASTHMA IS OUT OF CONTROL IF:
You wheeze, cough, feel tight or have
trouble breathing even at rest
Your symptoms are interrupting your sleep
You require your reliever medicine more than
four times in twenty four hours
Your peak flow is below _________
(60% of personal best)
Action:
Avoid your personal asthma triggers
Avoid tobacco smoke exposure
Check your peak flow _______ per day
if not already doing so
Controller(s): ____________________________
____________________________
Reliever(s): ____________________________
____________________________
Other Actions: ____________________________
____________________________
Seek medical attention if your asthma control isnot improving
within 12-24 hours
RED ZONE
YOU ARE IN THE DANGER ZONE IF:
You are getting little relief to no relief in 20
to 30 minutes after your reliever medicine
You are struggling to breathe or having
trouble walking or talking
Your lips or fingernails are turning blue
Action:
Call 911 or go to the nearest emergency department
immediately
You can repeat your reliever medicine every ____
minutes times ____ doses while assistance is being
arranged
Prepared by:
______________________________M.D./RT/CAE Date: ____________
Physician
Signature:____________________________________________
FC-532-01/06 adapted with permission: Alberta Lung Association
White: Chart Canary: Patient Pink: Physician
Appointments:
Personal best or predicted peak flow _______
Update yearly and as needed
-
8/7/2019 Asthma Clinical Guide
22/29
Asthma
Building Healthy LifestylesChinook Health Region 22
-
8/7/2019 Asthma Clinical Guide
23/29
Asthma
Building Healthy LifestylesChinook Health Region 23
5. Management Strategies for Patients / Clients
YOU HAVE JUST BEEN TOLD THAT YOU ORYOUR CHILD HAS ASTHMA, NOW
WHAT?
WHAT IS ASTHMA?
Asthma is an inflammatory disease of the small airways in
the
lungs that results in recurring episodes of difficult breathing
due tothe airways becoming more narrow (smaller) than normal.
eseepisodes may occur quite often or may come and go
intermittently.
Asthma ranges from very mild to severe.
WHAT ARE THE SYMPTOMS OF ASTHMA?
When the small airways in lungs begin to narrow, people
withasthma usually notice some or all of the following
problems:
Coughing
Wheezing
Chest tightness
Shortness of breath
Reduced ability to exercise
WHAT CAUSES AN ASTHMA EPISODE?(See diagram on back of this
page)
First, a trigger is inhaled into the lungs and irritates the
smallairways in the lungs.
Once the small airways are irritated, the insides of the
airwaysbecome red, swollen and narrower than normal. If nothing
isdone about the swelling it can get worse and people tend
todevelop more asthma symptoms.
Due to the swelling, the small airways in the lungs become
quitetwitchy. is causes the muscles on the outside of the airwayto
tighten and narrow the airways even more. Breathing becomesmuch
harder than normal at this point and could lead to aserious asthma
episode.
Asthma episodes, like asthma itself, can range from mild
tosevere. Severe asthma episodes can be life threatening and
canresult in a hospital stay or even death. erefore, prevention
ofepisodes is very important.
Common asthma triggers are smoke, colds, animal dander,
dust,pollen, cold air and exercise. Please note that exercise
shouldnot be avoided. If you or your child develops asthma
symptoms
with exercise, it may be a sign that your or your childs
asthmais poorly controlled. Contact a healthcare professional to
learnhow to improve asthma control. Triggers vary from person
toperson. Each person should learn about their own triggers andtry
to prepare for them and avoid them when possible.
IS ASTHMA A LIFELONG CONDITION?
As a general rule, asthma diagnosed in childhood is a
lifelong
condition. Asthma symptoms may diminish in adolescence, butcan
often return in adulthood. People with the following factorsare
most likely to have asthma that persists into adulthood:
A parent with asthma
A history of eczema (scaly red rashes on the skin)
Allergies or hay fever; allergic rhinitis (inflammation of the
liningin the nose)
THE GOOD NEWS FOR PEOPLE WITH ASTHMA:
Researchers are constantly seeking a cure. In the
meantime,asthma can be controlled. If asthma is well controlled,
there isa low risk for a serious asthma episode and a person can be
asactive as they like.
To control asthma you need to avoid contact with things
thattrigger your asthma and use your asthma medications regularly
asdirected by your doctor.
ere are people with well-controlled asthma who are
OLYMPICATHLETES!
WHO WILL HELP YOU TO MANAGE YOUR ASTHMA?
Your family doctor will diagnose and help manage your or
yourchilds asthma and should provide you with a written
asthmaaction plan.
Your pharmacist can also provide helpful information aboutasthma
and asthma medications.
Te Chinook Asthma Program is where you will meet withasthma
educators who can perform breathing tests to make sureyour lungs
are working at their best as well as provide you withinformation
about asthma and asthma medications. e asthmaeducators will work
with your doctor to develop a writtenasthma plan and ensure you
have the tools and confidence to feelat ease managing your or your
childs asthma.
To contact an asthma educator in your community, contact
theBuilding Healthy Lifestyles toll-free number at 1-866-506-6654or
388-6654.
-
8/7/2019 Asthma Clinical Guide
24/29
Asthma
Building Healthy LifestylesChinook Health Region 24
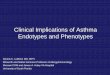
What is asthma?
As the swelling in the airway increases,
the lining of the airway becomes very
sensitive and small muscles around it
start to twitch and tighten.
3 Inflammation ofairway and mucous
6 Emergency room visit
2 Something startsinflammation
5 Muscles aroundairway tighten
1 Normal airway =normal function
houu
wheeze
5. Management Strategies for Patients / Clients
Reprinted with permission from theAsthma Society of Canada
www.asthma.cawww.asthma-kids.ca
-
8/7/2019 Asthma Clinical Guide
25/29
Asthma
Building Healthy LifestylesChinook Health Region 25
5. Management Strategies for Patients / Clients
Client Checklist for Asthma
What to expect at each office visit with your family
physician:
Assess asthma control:
Discuss frequency of asthma symptoms
Amount of rescue medication required (blue inhaler usage)
Review triggers and trigger avoidance strategies
Demonstrate use of inhaler device
Make or review a written asthma action plan
Discuss roles and use of asthma medications
Aim to reduce asthma medication dosage while maintaining proper
control of asthma
Discuss any other concerns about asthma with your doctor
Tests & Measurements that should be done or discussed on a
yearly basis,or as recommended by your family physician:
Lung function testing (spirometry)
Height and weight measurements
Screening for osteoporosis if on inhaled corticosteroids for
asthma and you have the following risk factors:
Age > 60 years Postmenopausal state without hormone
replacement therapy
Male impotence or infertility
Previous fractures with minor trauma
Family history of fractures (parental)
Past or current chronic glucocorticoid therapy
Smoking or alcoholism
Physical inactivity
Referral to an Asthma educator for education &
evaluation
Vaccinations
Annual influenza vaccine
Ensure immunizations are up to date
-
8/7/2019 Asthma Clinical Guide
26/29
Asthma
Building Healthy LifestylesChinook Health Region 26
-
8/7/2019 Asthma Clinical Guide
27/29
Asthma
Building Healthy LifestylesChinook Health Region 27
6. Indications for a Referral to Medical Specialist or Specialty
Program
6. Indications for a Referral to Medical Specialist or Specialty
Program
a. and b. Indications for Referral to MedicalSpecialists and
Specialty Programs
e following circumstances warrant a referral to an
appropriate
specialist:
ere is doubt about the diagnosis of asthma
Factors, including aeroallergens and occupational
exposures,could be involved and have not been properly evaluated;
orsuspected occupational asthma
Asthma is severe according to severity rating criteria
ere is an apparent discrepancy between the severity ofsymptoms
and success of treatment
ere has been a need for emergency treatment or
hospitaladmission
Any persistent respiratory symptoms in infants (under 1 year
ofage) and young children (age 1-6)
Normal spirometry tests and/or peak flows, but client
requiresexcessive medication for symptom control or fails to
respondto therapy after the clinician has confirmed compliance
withtreatment and proper inhaler device technique
c. Local Contacts
In the CHR the primary care physicians would refer their
adultpatients to see Dr. Wilde. Once the specialist has seen the
client,they will book additional tests as they see fit.
Dr. E. Wilde, Specialist Internal & Respiratory
Medicinephone 320-0633
In the CHR the primary care physicians would refer their
pediatricpatients to see the following pediatricians:
Dr. K. Chan, Telephone 328-8101Dr. M. Harilal, Telephone
320-2236Dr. J. Holland, Telephone 320-7825
Or
e primary care physician could refer pediatric clients to
theLethbridge Pediatric Asthma Clinic. A pediatrician will assess
and
make recommendations for each child who attends the clinic.
eprimary care physician would complete a referral form and fax it
tothe Building Healthy Lifestyles Program.
Telephone: 388-6654 or 1-866-506-6654Fax: 317-0435
Key contacts in the CHR for Asthma:
Adult Specialists
Dr. Eric Wilde, Telephone 320-0633Pediatric Specialists
Dr. K. Chan, Telephone 328-8101Dr. M. Harilal, Telephone
320-2236Dr. J. Holland, Telephone 320-7825
Lethbridge Educators
Pediatric Asthma clinic, Telephone 388-6180 Adult Asthma Clinic,
Telephone 388-6180
Rural Educators
Taber Asthma program, Telephone 223-3525Cardston Telephone
653-4411Magrath Telephone 758-4411Pincher Creek, Telephone
627-1234Crowsnest Pass, Telephone 562-2831Fort Macleod, Telephone
553-5311Raymond, Telephone 752-4561Milk River, Telephone
647-3500Picture Butte, Telephone 732-4762
By contacting Building Healthy Lifestyles 388-6654
or1-866-506-6654 an appointment can be booked for the patientand
BHL will notify the appropriate asthma educator.
Clinical Guides are available on-line at:
www.chinookprimarycarenetwork.ab.ca/extranet/resources/guides.php
-
8/7/2019 Asthma Clinical Guide
28/29
Asthma
Building Healthy LifestylesChinook Health Region 28
-
8/7/2019 Asthma Clinical Guide
29/29
Asthma7. References
7. References
a. Evidence1. Becker, Allan, MD; Berube, Denis, MD; Montgomery,
Mark, MD; Sears, Malcolm, MD; Spier, Sheldon, MD; on behalf of
the Canadian Pediatric Asthma Consensus Guidelines 2003 (updated
to December 2004) Supplement to CMAJ 2005; 173(6 suppl): S1-S56
2. Boulet,Louis-Philippe, MD; Becker, Allan, MD; Berube, Denis,
MD; Beveridge,Robert, MD; Ernst, Pierre MD; on behalfof the
Canadian Asthma Consensus group. Canadian Asthma Consensus Report
1999. Supplement to CMAJ 1999; 161(11 suppl)
3. British Columbia Guidelines & Protocols Advisory
Committee, Diagnosis and Management of Asthma July 1, 2003
4. FitzGerald JM, Becker A, Sears MR, et al. Doubling the dose
of budesonide versus maintenance treatment in asthmaexacerbations.
orax 2004;59:550-6
5. Green RH, Brightling CE, McKenna S, et al. Asthma
exacerbations and sputum eosinophil counts: a randomised
controlledtrial. Lancet 2002; 360:1715-21
6. Harrison TW, Oborne J, Newton S, et al. Doubling the dose of
inhaled corticosteroid to prevent asthma exacerbations:randomised
controlled trial. Lancet 2004;363:271-5
7. Jarjour NN, Gern JE, Kelly EA, et al. e effect of an
experimental rhinovirus 16 infection on bronchial lavage
neutrophils.J Allergy Clin Immunol 2000;105:1169-77
8. Johnston SL, Pattemore PK, Sanderson G, et al. Community
study of role of viral infections in exacerbations of asthma in9-11
year old children. BMJ 1995;310:1225-9
9. Lemiere,C; Bai,T; Balter, M, et al, on behalf of the Canadian
Adult Consensus group of the Canadian oracic Society.Adult Asthma
Consensus guidelines update 2003. Can Respir J 2004; 11 (Suppl A);
9A 18A
10. Respiratory Division, Cardio-Respiratory diseases and
diabetes bureau, laboratory centre for disease control, Health
Canada.e national asthma control task force. e prevention and
management of asthma in Canada 2000
b. On-line Resources1. Canadian Lung Association www.lung.ca
2. Canadian oracic Society www.lung.ca/cts/3. COPD & Asthma
Network of Alberta (CANA) www.canahome.org
4. Family Physicians Airways Group of Canada www.fpagc.com
5. Canadian Network for Asthma Care (CNAC) www.cnac.net
6. Child Asthma Network iCan
www.calgaryhealthregion.ca/ican/
7. National Institute of Health www.nhlbi.nih.gov
8. Canadian Society of Allergy & Clinical Immunology
www.csaci.medical.org
9. Global Initiative for Asthma www.ginaasthma.com
10. Calgary Allergy Network www.calgaryallergy.ca
11. American Academy of Allergy, Asthma & Immunology
www.aaaai.org
12. Asthma Society of Canada www.asthma.ca
Available CHR Resources Winning with Asthma www.chr.ab.ca