Embed Size (px)
Citation preview

Archives ofDisease in Childhood 1995; 73: 413-417
Clinical value of monitoring eosinophil activity inasthma
D Y Koller, Y Herouy, M G6tz, E Hagel, R Urbanek, I Eichler
AbstractTo evaluate the use of eosinophil cationicprotein (ECP) in monitoring diseaseactivity in childhood asthma, serum ECPin 175 asthmatic children was assessed.Forty five patients with cystic fibrosis, 23with lower respiratory tract infections(LRTI), and 87 healthy children were usedas controls.Serum ECP concentrations (34.3 lug/l
v 9-8 ,ug/l) were significantly higher inchildren with bronchial asthma than inhealthy control subjects. In symptomaticpatients with asthma serum ECP concen-trations were increased compared withthose from asymptomatic patients (40-2,ug/l v 14*4 ,ug/l), irrespective of treatmentmodalities (that is steroids, 2 agonists, orsodium cromoglycate). Moreover, atopyand infection appeared to be factorsenhancing eosinophil activiti in bronchialasthma as measured by serum ECP (58.4,xg/l v 36-8 ,ugll and 68-8 pug/l v 42-2 ,ug/l,respectively). In a longitudinal trial, anti-asthmatic treatment modalities (that issteroids) reduced serum ECP within fourweeks (42.2 ,ugll v 19*0 ,ug/l).
In conclusion, the data indicate that (1)eosinophils also play a central part inchildhood asthma; (2) serum concentra-tions of ECP in children with bronchialasthma are related to the disease severityand may thus be used for monitoringinflammation in childhood asthma; (3)eosinophil activity appears to be enhancedby atopy and infection; and (4) longitudi-nal measurements of serum ECP concen-trations may be useful for optimisinganti-inflammatory treatment in childrenwith bronchial asthma.(Arch Dis Child 1995; 73: 413-417)
Keywords: asthma, eosinophils, eosinophil cationicprotein, infection.
Asthma is a chronic inflammatory disease,which is characterised by symptoms of airwayobstruction such as cough, wheezing, andbreathlessness. Bronchial inflammation inasthma can be assessed directly by patho-histological observations and indirectly byexamining cells and mediators present inperipheral blood. 1 2In adults the implication ofeosinophils in bronchial asthma is wellaccepted.3 A correlation between activatedeosinophils and pulmonary function ornon-specific bronchial hyperreactivity wasobserved.4 Moreover, activated eosinophilsrelease granule derived proteins, the most
accepted of which is eosinophil cationic protein(ECP) for estimation of eosinophil activation.5 6In vitro studies have shown the deleteriouseffect to bronchial mucosa of eosinophil derivedcytotoxic proteins5 7 and assessment of serumECP has been suggested for monitoring diseaseactivity and bronchial inflammation8 in adultbronchial asthma. In childhood asthma, how-ever, problems in diagnosing or monitoringdisease activity may occur because of non-specific symptoms as well as the inability toobtain reliable pulmonary function andprovocation tests in children less than 5 years ofage. Thus, monitoring by the assessment ofmediators, reflecting pulmonary inflammation,6could support an optimal management ofchildhood asthma.To evaluate the clinical value of activated
eosinophils in children with bronchial asthma,serum ECP and blood eosinophil counts weredetermined. Sensitisation to inhalant allergensas well as infections of both the upper and thelower respiratory tract are known to causeexacerbations in asthmatic children.9 To dif-ferentiate between various factors assumed toinfluence eosinophil activities, the patientstherefore were subdivided into groups due totreatment modalities, to atopy and infection.In addition, healthy non-atopic children andpatients with cystic fibrosis and lower respira-tory tract infections (LRTI) were used ascontrols.
Subjects and methodsPATIENTS AND CONTROLSA total of 175 children (78 girls and 97 boys)with bronchial asthma (diagnosis was based onepisodic cough, wheeze, and breathlessnessthat was responsive to 12 agonists, and afterother conditions have been excluded) wereenrolled for this study (mean (SD) age 9-8(3-8) years; 52 of the patients were less than 6years of age).At the time of examination the children were
divided into different treatment groups: (1)44 children on inhaled 12 agonists (33 withsalbutamol, 11 with fenoterol); (2) 37 oninhaled steroids (29 with budesonide, eightwith beclomethasone); (3) 47 on inhaledsteroids and 02 agonists; (4) 27 on inhaledsodium cromoglycate; and (5) 20 children withbronchial asthma who were newly diagnosedand thus without antiasthmatic medication.In 14 of these patients treatment wasinitiated with budesonide (600 ,ug daily) andsalbutamol (300 ,ug daily) for two weeks, andthereafter with budesonide alone. Every twoweeks follow up examinations, includingpulmonary function and blood sampling, were
Divisions ofAllergyand Pulmonology,University Children'sHospital, Vienna,AustriaD Y KollerY HerouyM GotzR UrbanekI Eichler
Department ofPaediatrics,Wilhelminen Hospital,Vienna, AustriaE Hagel
Correspondence and reprintrequests to: Dr Dieter Koller,University Children'sHospital, Wahringer Giirtel18-20, 1090 Vienna, Austria.Accepted 25 May 1995
413
on May 14, 2022 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.73.5.413 on 1 N
ovember 1995. D
ownloaded from

Koller, Herouy, Gotz, Hagel, Urbanek, Eichler
performed for a period of four weeks. Theremaining six patients were first treated withoral antibiotics - due to LRTI - and an inhaledIP2 agonist (salbutamol 300 ,ug daily) for 10days and thereafter with inhaled budesonide(600 pug daily).The controls comprised: (1) 23 non-
asthmatic children with LRTI (14 girls andnine boys; age 8-6 (2.5) years) before initiatingantibiotic treatment. (2) Forty five patientswith cystic fibrosis (22 girls and 23 boys; age
10-8 (6.5) years); 20 of these patients were
colonised with Pseudomonas aeruginosa and/orStaphylococcus aureus as proved by sputumcultures. Clinical condition was assessed by themethod of Shwachman-Kulczycki10 withoutreviewing the x ray resulting in a score between0-75. The median score in our patients investi-gated was 55 (range 24-73). Acute pulmonaryexacerbation in cystic fibrosis was defined as
marked increase of C reactive protein (medianconcentration 129 mg/l), by weight loss,anorexia, increased cough, increased sputumproduction, fever with and without new lunginfiltrates, deterioration of oxygen saturationand lung function. None of these patientsreceived systemic or inhaled steroids within themonth of blood drawing. (3) Eighty seven
healthy children (51 girls and 36 boys; age 10-2(4.5) years) with no history of atopy or asthmaand normal total serum IgE concentrations,who were free of infection for at least two weeksbefore the drawing of blood were recruited as
normal references.Parental agreement to blood sampling was
obtained in all cases and blood was obtained atroutine sampling for clinical evaluation.
DEFINITION OF ATOPIC STATUSPatients were defined as being atopic by havingincreased total serum IgE antibody concen-
trations and by the presence of specific IgEantibodies against at least two or more inhalantallergens tested (Dermatophagoides pteronyssinusand D farinae, cat, dog, alternaria, cladospo-rium, aspergillus, birch, alder, hazel, and grasspollens).
DEFINITION OF INFECTION IN CHILDREN WITH
BRONCHIAL ASTHMAInfection of the upper or lower respiratory tractwas diagnosed clinically, by leucocytosis,radiographic evidence of pulmonary infiltratesand - if possible - by sputum cultures andevidence of viral antigens in nasal fluids.
CLINICAL EVALUATION AND PULMONARY
FUNCTIONPhysical examination and a history of wheeze,cough (nocturnal), and dyspnoea within thelast two weeks before blood sampling allowedto divide the patients into symptomatic andasymptomatic children with bronchial asthma.Pulmonary function tests were performed -
as compliance of the patients and/or parentsallowed - in 52 children with bronchial asthmaand 38 patients with cystic fibrosis as follows.
Forced vital capacity (FVC), forced expiratoryvolume in the first second (FEV1) and maxi-mum expiratory flow at 50% (MEF50) and at25% (MEF25) of vital capacity were recordedin the form of a maximum flow volume curve(Masterlab, Jaeger, Germany) according to theAmerican Thoracic Society standard." Thebest of three efforts was used for calculations.Results were presented as percent predictedbased on accepted reference standards.12
BLOOD SAMPLESBlood eosinophil counts were determined byautomated counting (Sysmex NE-5500;Muller GesmbH, Austria) with a coefficient ofvariation about 7/0%. Serum was used for thedetermination of ECP. Assessments were doneby using a sensitive and specific doubleantibody radioimmunoassay (PharmaciaDiagnostics, Sweden) in which ECP in thesamples competes with a fixed amount of 1251.labelled ECP for the binding sites of specificantibodies.13 14 The interassay coefficient ofvariation for the assay was less than 10%.
Total serum IgE and specific IgE antibodieswere measured by using enzyme immuno-assays (Kallestad Diagnostics, USA).
STATISTICAL ANALYSISResults are expressed as medians (quartilel-quartile 3) unless mentioned otherwise.Correlation coefficients were obtained usingthe Kendall Tau B test. Non-parametric statis-tical tests were used in comparative analysis.The Kruskal-Wallis analysis was applied firstto the data in all groups. When this was signifi-cant, each pairing was examined by means ofthe Mann-Whitney U test. Changes related totreatment were tested for significance usingWilcoxon signed ranks test for paired samples.Probabilities of less than 5% were taken asstatistically significant.
ResultsCHARACTERISTICS OF PATIENTSAt the time of examination, 90 asthmaticchildren with bronchial asthma were asympto-matic whereas 85 patients had symptoms ofairway obstruction within the last two weeksbefore examination; 105 children presentedwith specific sensitisation against two ormore of tested allergens. Total serum IgE con-centrations were significantly increased in theatopic group (median: 457 kU/l) comparedwith the non-atopic asthmatics (median:
Table 1 Eosinophil counts as well as serum ECPconcentrations in children with bronchial asthma, cysticfibrosis, and LRTI compared with healthynon-atopic subjects
Eosinophils (cells/,d) ECP (pig/l)Bronchial asthma 443 (290-601) 34-3 (22-5-55-2)Cystic fibrosis 235 (105-350) 65-7 (39-8-82-5)LRTI 205 (125-230) 12-3 (8-7-16-3)Controls 209 (118-328) 9-8 (7-3-13-5)
Results are presented as median (quartile 1-quartile 3);p values in text (see results section).
414
on May 14, 2022 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.73.5.413 on 1 N
ovember 1995. D
ownloaded from

Clinical value of monitoring eosinophil activity in asthma
Table 2 Serum ECP and eosinophil counts in symptomatic and asymptomatic children with bronchial asthma subdividedinto treatment groups
ECP (p1g/) Eosinophils/u
Symptomatic Asymptomatic p Value Symptomatic Asymptomatic p Value
Untreated 43-4 (36-4-68 8) 388 (278-545)[n=20]
12 Agonists 39-9 (22-1-59-5) 13-4 (11-2-31-8) p<0005 404 (254-509) 398 (110-400) NS[n= 18] [n=26]
Steroids 48-5 (20 5-70 9) 14-3 (10-0-23-5) p<0 005 347 (210-580) 311 (188-411) NS[n= 17] [n=20]
Steroids and 12 agonists 33 0 (17-0-54-3) 15-0 (12-0-24-4) p<0-001 335 (289-481) 360 (320-450) NS[n=20] [n=27]
Sodium cromoglycate 41-4 (24 6-76 4) 14-7 (9 8-23 9) p<0-001 387 (254-467) 365 (298-485) NS[n= 10] [n= 17]
Results are presented as median (quartile l-quartile 3); p values=statistical differences between symptomatic and asymptomaticchildren with bronchial asthma. NS=not significant.
17 kU/l; p<00001). Infection of the lower orupper respiratory tract was present in 77children with bronchial asthma at the time ofexamination.
Assessment of pulmonary function in 52 ofthe asthmatics showed for symptomaticchildren (n=31) a median (range) FEV1 valueof 78A4% predicted (47-9-89-0%), MEF50value of 62-9% predicted (25-7-75-0%),and MEF25 value of 58 1% predicted(20.6-72.9%). Asymptomatic asthmatics(n=21) demonstrated a median (range) FEV1value of 95-6% predicted (88&6-120%),MEF50 value of 90 1% predicted(79-8-124-5%), and MEF25 value of 85-2%predicted (73 9-112 4%).
In patients with cystic fibrosis (n=38)median (range) FEV1 was 74-2% predicted(22-8-135-8%), a median MEF50 50 0% pre-dicted (5.7-92.4%), and MEF25 30-8% pre-dicted (3-9-91-5%). In addition, atopy wasobserved in 24 children with cystic fibrosis asproved by specific sensitisation againstinhalant allergens and increased total serumIgE concentrations (median 480 kU/l) com-pared with 21 non-atopic patients with cysticfibrosis (median 26 kU/l; p<0 0001).
BRONCHIAL ASTHMA, CYSTIC FIBROSIS, ANDLRTIEosinophil counts in peripheral blood were
significantly increased in children with bron-chial asthma compared with control subjects(p<0 005), to patients with cystic fibrosis(p<0 005), and to children with LRTI(p<0 005; table 1). Eosinophil numbers in
asthmatic children were weakly correlated withserum concentrations of ECP (r=0-316;p<0 0001). In asthmatic children, serumECP was raised in comparison with LRTI(p<0 001) and with healthy controls(p<0 0001), but were not different to ECPconcentrations in samples obtained frompatients with cystic fibrosis (table 1).
Subdivision into symptomatic and asympto-matic asthmatic children demonstrated signifi-cant differences for serum ECP concentrations(table 2) whereas eosinophil counts were notdifferent (table 2). In addition, symptomaticpatients with bronchial asthma had serumconcentrations of ECP within the same patho-logical range, irrespective if treated withsteroids, 12 agonists, or sodium cromoglycate(table 2). Serum ECP and eosinophil countsdid not differ significantly between the younger(less than 6 years) and the older (more than 6years) patients.ECP concentrations in sera of patients with
bronchial asthma were not correlated withvariables of pulmonary function. In patientswith cystic fibrosis, however, a relationshipwith pulmonary function as measured by FEV1predicted (r=-0-634; p<0 001) and theShwachman-Kulczycki score (r= -0-678;p<0-001) was given.
EOSINOPHIL COUNTS AND SERUM ECP INATOPIC BRONCHIAL ASTHMAIn children with atopic bronchial asthma bothserum ECP concentrations as well as eosinophilcounts were increased (table 3) compared withasthmatic patients without atopy. Atopic
Table 3 Atopy: influence on serum ECP and eosinophil counts in children with bronchial asthma on different medicationand in cystic fibrosis
ECP (pug/l) Eosinophils (ceWllp)Non-atopic Atopic p Value Non-atopic Atopic p Value
Bronchial asthmaUntreated 36-8 (15-7-48-5) 58-4 (42-1-80-7) p<0 05 367 (250-478) 485 (390-660) p<0 05
[n=9] [n=112 Agonists 12-7 (8-1-21-9) 32-4 (13-8-43-0) p<0-01 222 (100-310) 386 (230-484) p<0 05
[n= 12] [n=32]Steroids 20-0 (8-0-28-0) 23-5 (12-0-51-6) NS 320 (240-423) 480 (300-640) p<0 05
[n= 15] [n=22]Steroids and 2 agonists 19-5 (12-0-39-0) 19-0 (12-0-36-0) NS 343 (312-450) 453 (320-612) p<0 05
[n=22] [n=25]Sodium cromoglycate 18-8 (9-8-29 4) 29-9 (10-8-44-7) p<0 05 334 (298-417) 465 (312-608) p<0 05
[n= 12] [n= 15]Cystic fibrosis 61-3 (98-71-4) 55-0 (13-265-8) NS 180 (120-220) 160 (90-280) NS
[n=26] [n= 19]
Results are presented as median (quartile 1-quartile 3); p values indicate significant differences between atopics and non-atopics.NS=not significant.
415
on May 14, 2022 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.73.5.413 on 1 N
ovember 1995. D
ownloaded from

Koller, Herouy, Gotz, Hagel, Urbanek, Eichler
Table 4 Infection: influence on serum ECP in children with bronchial asthma (subdividedinto different treatment groups), cystic fibrosis, and with LRTI
ECP (,g/l)Infection No infection p Value
Bronchial asthmaUntreated 68-8 (500-85 5) 42-2 (36-3-48 5) p<0 05
[n=6] [n= 14]12 Agonists 35-3 (32 5-58 3) 20-1 (12-1-37-7) p<0 05
[n=23] [n=21]Steroids 63-2 (26 3-76 6) 15-4 (11-8-26-7) p<0O005
[n= 17] [n=20]Steroids and 12 agonists 54-0 (390-114-0) 17-0 (120-32-0) p<0O001
[n= 18] [n=29]Sodium cromoglycate 57-4 (38-2-76 4) 18-9 (8-9-29 8) p<0O005
[n= 13] [n= 14]Cystic fibrosis 30 4 (13-2-57-3) 48-8 (9 8-658) NS
[n= 17] [n=28]LRTI 12-3 (8-7-16-3)
[n=23]
Results are expressed as median (quartile I-quartile 3); p values indicate significant differencesbetween infected and non-infected patients. NS=not significant.
patients with bronchial asthma treated with 12
agonists and sodium cromoglycate had signifi-cantly higher concentrations ofECP than non-
atopic subjects treated with these agentswhereas atopic patients treated with inhaledsteroids had similar concentrations of ECP tonon-atopic children treated with inhaledsteroids (table 3). Total eosinophil counts, how-ever, were unaffected by inhaled steroids, thusno differences for eosinophil counts in eachtreatment group between atopic and non-atopicasthmatic children could be observed (table 3).
EOSINOPHIL COUNTS AND SERUM ECP ININFECTIONInfection caused an increase of ECP in child-hood asthma but not in patients with cysticfibrosis and with LRTI (table 4). Eosinophilcounts, however, were not altered (median 378cells/ptl v 328 cells/pld).
EFFECT OF INHALED BUDESONIDE ON SERUMECPTreatment with budesonide (600 ,ug/daily) forfour weeks and salbutamol (300 ,ug/daily) fortwo weeks in 14 children with newly diagnosed
120 r
100 F-
p<<-0
L- p<0-005-I
80
CD
0L0L
60
40 F-
20
Before Week 2 Week 4 Before Week 2 Week 4
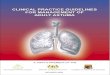
Figure 1 The change in serum concentrations ofECP and FEV, in 14 newly diagnosedasthmatic children. Examinations were performed before starting treatment, after two weeksof treatment with budesonide and salbutamol and after the following two weeks of treatmentwith budesonide alone. Median serum ECP concentration before treatment: 42-2 ,ugil; after2 weeks: 23-9 ,jg/l; after 4 weeks: 19 - ,ug/l. Median FEy1 % predicted before treatment:82-9%; after 2 weeks: 94-1%°o; after 4 weeks: 97A4%. No significant changes of eosinophilcounts were observed.
bronchial asthma resulted in a significantdecrease of serum ECP and improvement ofpulmonary function (fig 1). Eosinophil counts(median eosinophil count before treatment:388 cells/pdl; after two weeks treatment withbudesonide and salbutamol: 400 cells/pul; afteradditional two weeks with budesonide alone:364 cells/pul) did not change significantly.
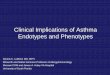
In children (n=6) with bronchial asthmapresenting with LRTI oral antibiotic andinhaled 12 agonist treatment resulted in nosignificant change of ECP concentrationswithin 10 days (fig 2). Only inhalation ofbudesonide (600 ,ug/l) caused a significantreduction of serum ECP concentrations(p<0 03) in these patients (fig 2).
DiscussionInflammation is being increasingly recognisedas a major factor in childhood asthma. One ofthe predominant inflammatory cells in theasthmatic lung is the eosinophil granulocyte,which has been suggested to contribute tobronchial hyperreactivity and tissue injury.' 3The activity of eosinophils could be deter-mined by the measurement of eosinophilgranule proteins, such as ECP. In addition,assessment ofserum ECP has been assumed toreflect pulmonary inflammation in bronchialasthma.5 6 8We have found increased blood eosinophil
counts and more significantly increased serumconcentrations of ECP in children with bron-chial asthma compared with a group of age andsex matched normal healthy control subjects.ECP concentrations were not different betweenchildren less or more than 6 years of age, as pre-viously reported.15 The median serum ECPconcentrations were raised, however, with manypatients having normal values. This could beexplained partly by the fact that inhaled steroidsreduce the concentrations of ECP due to thedirect inhibitory effect on eosinophil activa-tion.'5 However, many children on 12 agonistsalone, also demonstrated low ECP despitepublished data, showing no in vitro effect Of (2agonists on eosinophil activation.'6 By dividingchildren with bronchial asthma into sympto-matic and into asymptomatic patients we wereable to demonstrate that symptomatic childrenhad higher ECP concentrations than asympto-matic asthmatics, independent of treatmentmodalities (that is inhaled steroids, 12 agonists,combination of both, or sodium cromoglycate).These results suggest that determination ofserum ECP may be useful for assessing asthmaseverity. In addition, measurement of raisedserum ECP concentrations may reflect theongoing inflammation in the asthmatic lung andmay therefore be used to predict the needfor intensified anti-inflammatory treatmentmodalities. Similar findings were reported onlyrecently.'5 To emphasise this hypothesis, wewere able to demonstrate the effectiveness ofinhaled steroids in suppressing eosinophilactivity in a four week prospective trial.Improvement of pulmonary function wasstrongly associated with a fall of serum ECP,in all subjects investigated, suggesting that
416
- P<0.001p<0.002
on May 14, 2022 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.73.5.413 on 1 N
ovember 1995. D
ownloaded from

Clinical value of monitoring eosinophil activity in asthma 417
120 100
100 90
80 --80 (
0 4~~~~~~~~~~~~~0
Bfr60 70
0~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~-1
40 w 60lLL
20 -50
0 40Before 10 days 28 days Before 10 days 28 days
Figure 2 The change in serum concentrations ofECP and ofFEV1 in six newlydiagnosed asthmatic children with infection of the lower respiratory tract infection.Examinations were done before starting treatment, after 10 days of treatment by oralantibiotics and inhaled salbutamol, and after 18 days of treatment by budesonide andsalbutamol. Median serum ECP concentrations before treatment: 68-8 gfi/ after 10 days:38-2 Ag/ (p=NS compared values on day 0); after 28 days: 13-5 pLg/l (p<0-03 comparedto values on day 0). Median FEV1 % predicted before treatment: 73 9%; after 10 days:85-4% (p<0-05 compared with values on day 0); after 28 days: 96&0% (p<0-03compared with values on day 0).
longitudinal measurements of serum ECPmight be used to predict the outcome of treat-ment. The eosinophil counts did not fall, sug-gesting that serum ECP is not dependent on thetotal eosinophil count8 and, in addition, ECPappears to correlate better with the severity ofasthma than does the eosinophil count.17The main factors causing exacerbation of
asthma in childhood are allergens and infec-tions of either the upper or lower respiratorytract. To investigate whether atopy and infec-tion influence the activity of eosinophil granu-locytes, children with bronchial asthma weredivided into different groups (atopic v non-atopic; infection v asthmatic children withoutinfection). Children with atopic bronchialasthma (without anti-inflammatory treatment)had significantly higher ECP concentrationsthan non-atopic asthmatic patients. Thus, itcould be speculated that atopy is a factor'boosting' inflammatory processes in childhoodasthma, consecutively increasing bronchialhyperreactivity.4 18 Our data also clearlydemonstrated that inhaled steroids appeared tosuppress significantly inflammation in atopicasthma, as ECP concentrations in steroidtreated atopic asthmatics were no different tothose in non-atopic asthmatic children.
Infections of the respiratory tract raisedserum ECP concentrations in patients withbronchial asthma. As infection caused anincrease of ECP in children with asthma only,and not in patients with LRTI and cysticfibrosis, it might thus be suggested specific forbronchial asthma.
In a previous study we reported increasedserum ECP concentrations in children withcystic fibrosis.19 In this study, our previousfindings were confirmed, but - in contrast tobronchial asthma - no influence of atopy oracute infection on serum EGP concentrationscould be detected. Normal eosinophil countsin patients with cystic fibrosis in the presenceof increased serum ECP thus suggest different
mechanisms of eosinophil activation than inpatients with bronchial asthma.14 Anotherexplanation might be that in cases with normalor moderately high eosinophil numbers, thereduced availability may be compensated forby the increased activity of cells, which isenough to achieve sufficient concentrations ofthe inducers of the inflammatory process.
In conclusion, our findings demonstratedincreased serum ECP concentrations inchildren with bronchial asthma. By theseresults, it has become likely that the eosinophilplays a central part in the asthmatic inflam-mation in children, as it does in adults. Inaddition, our data suggest that the determina-tion of serum ECP may be used for monitoringthe disease activity. As both atopy and infectioncaused increased ECP concentrations - that isenhanced eosinophil activation - we hypo-thesise that both may act as 'boosting factors'for inflammatory processes in bronchial asthma.Finally, our results suggest that serum ECPmeasurements may be useful to predict the needfor intensified anti-inflammatory treatment.
It may be that assessment of mediators willallow further investigation of important anduntil now unanswered questions in childhoodasthma, namely: When is the onset ofeosinophilic inflammation in the asthmaticchild? and What is first: bronchial hyperreac-tivity or inflammation?
1 Gleich GJ. The eosinophil and bronchial asthma: currentunderstanding. Allergy Clin Immunol 1990; 85: 422-36.
2 Ayars GH, Altman LC, Gleich GJ, Loegering DA, BakerCB. Eosinophil- and eosinophil granule-mediated pneu-mocyte injury. JAllergy Clin Immunol 1985; 76: 595-604.
3 Bousquet J, Chanez P, Lacoste JY, et al. Eosinophilic inflam-mation in asthma. NEnglJMed 1990; 323: 1033-9.
4 Ferguson AC, Wong FWM. Bronchial hyperresponsivenessin asthmatic children. Correlation with macrophages andeosinophils in broncholavage fluid. Chest 1989; %: 988-91.
5 Spry CFJ. Eosinophils: a comprehensive review, and a guide tothe scientific and medical literature. Oxford: OxfordUniversity Press, 1988.
6 Venge P, Dahl D, Fredens K, Hallgren R, Peterson C.Eosinophil cationic proteins (ECP and EPX) in healthand disease. In: Yoshida T, Torisu M, eds. Immunobiologyof the eosinophiL New York: Elsevier, 1983: 163-79.
7 Flavahan NA, Shifman NR, Gleich GJ, Vanhutte PM.Human eosinophil major basic protein causes hyperreac-tivity of respiratory smooth muscle: role of the epithelium.Am Rev Respir Dis 1988; 138: 685-8.
8 H5llgren R, Venge P. The eosinophil in inflammation. In:Matsson P, Ahlstedt S, Venge P, Thorell J, eds. Clinicalimpact of monitonng of allergic inflammation. London:Academic Press, 1991: 119-40.
9 Warner JO, G6tz M, Landau LI, et al. Management ofasthma. A consensus statement. Arch Dis Child 1989; 64:1065-79.
10 Shwachman H, Kulzcycki L. Long-term study of 105patients with cystic fibrosis. AmJDis Child 1958; 96: 6-15.
11 American Thoracic Society. Standardization of spirometry- 1987 update. Am Rev Respir Dis 1987; 2: 1285-98.
12 Zapletal A, Samanek M, Paul T. Lung-function in childrenand adolescents. Methods, reference values. Progress inRespiratory Research 1987; 22: 113-218.
13 Venge P, Roxin LE, Olsson I. Radioimmunoassay of humaneosinophil cationic protein. BrJHaematol 1977; 37: 331-6.
14 Koller DY, Urbanek R, G6tz M. Increased degranulation ofeosinophil and neutrophil granulocytes in cystic fibrosis.Am J Respir Crit Care Med 1995 (in press).
15 Zimmerman B. Enander I, Zimmerman R, Ahlstedt S.Asthma in children less than 5 years of age: eosinophilsand serum levels of the eosinophil proteins ECP and EPXin relation to atopy and symptoms. Clin Exp Allergy 1994;24: 149-55.
16 Yukawa T, Chanez P, Dent G, et al. Bronchodilator agentsdo not inhibit oxygen free radical release from guinea pigeosinophils. Am Rev Respir Dis 1988; 137 (suppl 4): A27(abstract).
17 Horn BR, Robin ED, Theodore J, Van Kessel A. Totaleosinophil counts in the management of bronchialasthma. NEnglJ3tMed 1975, 292: 1152-5.
18 Frick WE, Sedgwick JB, Busse WW. The appearance ofhypodense eosinophils in antigen-dependent late phaseasthma.AmRevRespirDis 1989; 139: 1401-6.
19 Koller DY, Gotz M, Eichler I, Urbanek R. Eosinophilicactivation in cystic fibrosis. Thorax 1994; 49: 496-9.
on May 14, 2022 by guest. P
rotected by copyright.http://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.73.5.413 on 1 N
ovember 1995. D
ownloaded from