Embed Size (px)
Citation preview

Associate Professor Rohan
AmeratungaAdult and Paediatric Clinical Immunologist and
Allergist
Auckland
8:30 - 9:25 WS #87: Infections in Children - An Immunologist's View
9:35 - 10:30 WS #99: Infections in Children - An Immunologist's View
(Repeated)

The child with recurrent infections
Recurrent infections in children
• Too many
• Too severe
• Too long
• Not responding to treatment

Recurrent Infections in children
Globally

Malnutrition in the world

Childhood deaths in the world

Main categories
• Normal child 50%
• Child with atopy 30%
• Child with chronic disease and/or
anatomical problems 10%
• Immunodeficiency: primary or secondary
10%- detailed features when to suspect
Clinical investigation
• History detailed history incl pregnancy
• Examination
• Investigations- identifying PID
• Lab and imaging studies

Pregnancy history
• Infections
• Drug use legal or illegal
• HIV risk factors
• Tobacco

Birth history
• Length of gestation
• Neonatal complications
• Admission to PICU
• Any complications in hospital
Prematurity
• Increased risk of RSV in the first year
• Difficult to identify which subgroups are at
most risk
• Palivizumab
• Immunoglobulins transferred in the last
trimester
• Increased risk of other infections not as well
documented

Prematurity
• Bronchopulmonary dysplasia
• Still an issue with surfactant, reduced
oxygen, changes in ventilation strategy etc

Cost-effectiveness of palivizumab in New Zealand.Vogel A, McKinlay M, Ashton T, Lennon D, Harding J, Pinnock R,
Graham D, Grimwood K, Pattemore P, Schousboe M.
J Paediatr Child Health 2002 Aug;38(4):352-357

Growth and development
• Chronic disease- poor growth, some PIDS
• Heart and lung disease eg CF
• GI disease eg diarrhoea

Reactions to immunisation
• Adverse reactions to live vaccines eg
rotavirus, BCG
• Polio no longer live

Medications
• Steroids
• immunosuppressives

Family history
• Recurrent infections
• Early deaths
• Unexplained deaths in childhood
• Consanguinity
• Ethnicity
Normal child 50%
• 4-8 infections/yr
• Increased risk: sibling attending daycare
• Overcrowding
• no more than 1 pneumonia or 2 OM in the
first three years of life.
• Generally viral infections
• Complete recovery between infections

Socioeconomic factors and
recurrent infections in children
• The worried well
• Socio-economic status- Overcrowding
• Attendance at daycare
• Number of siblings
• Birth order
• Access to medical care

Socioeconomic factors and
recurrent infections in children
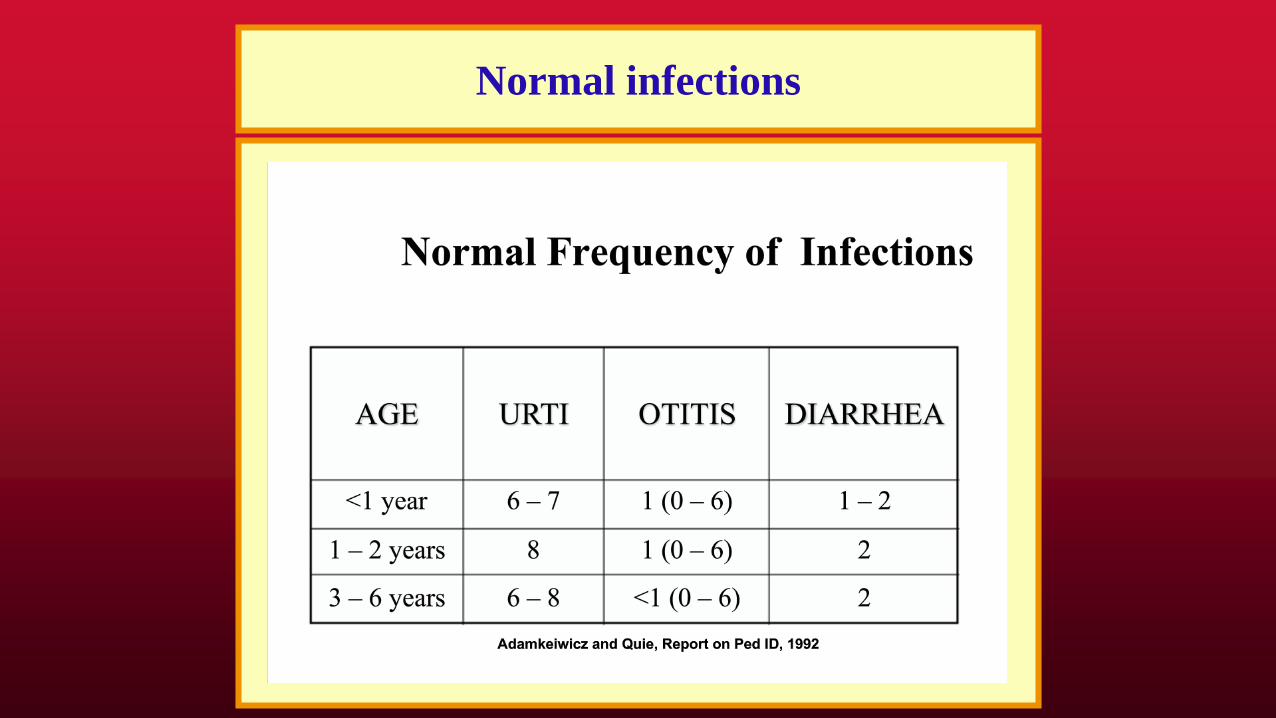
Normal infections

Clinical features of concern
• More than two severe infections/ yr
• 3 respiratory infection incl sinusitis
• Abx > 2 months/yr
• Failure to respond to antibiotics
• Need for IV antibiotics
• Unusual complications eg empyema,
mastoiditis, abscesses
Parental smoking and other risk factors
for wheezing bronchitis in children.Rylander E, Pershagen G, Eriksson M, Nordvall L.
Eur J Epidemiol 1993 Sep;9(5):517-26
• 199 children with wheezing. 309 controls
• Parental smoking rr 1.8
• Strongest association with maternal
smoking and children,18/12

Parental smoking, bronchial reactivity
and peak flow variability in children
Cook, Derek G; Strachan, David P
Thorax 1998;53(4):295-301

Recurrent wheezy bronchitis
and viral respiratory infections.Mertsola J, Ziegler T, Ruuskanen O, Vanto T, Koivikko A, Halonen P.
Arch Dis Child 1991 Jan;66(1):124-9
• 54 pts 1-6 yrs recurrent wheezy bronchitis
• 115 episodes
Mycoplasma 52
Rhinovirus 34
• Associated with parental smoking
Atopic child
• AR mistaken for sinusitis
• Bronchitis vs pneumonia
• PID or anatomical problems can co-exist
with atopy
• Higher risk of atopy with some PIDS
• May have allergen specific IgE tests in PID

Allergy as a cause of
recurrent infections in children
• 5yr old boy with recurrent muco-purulent
nasal discharge.
• Requiring up to 12 Rx antibiotics per year
• Symptoms worse in winter
• Frequent sneezing and rhinorrhoea
• Other family members also atopic
• Strongly +ve spt tests to HDM, cats
Allergy as a cause of
recurrent infections in children
• Allergy treatment HDM prevention
measures
• Combination of Butacort and Loratadine
• Reduction in frequency of infections and
rhinitis symptoms
• Allergen-specific immunotherapy
The prevalence of atopic disorders in children
with chronic otitis media with effusion.Alles R, Parikh A, Hawk L, Darby Y, Romero JN, Scadding G
Pediatr Allergy Immunol 2001 Apr;12(2):102-6
• 209 chronic OME cases from an ENT clinic
• 89% had allergic rhinitis (hx, spts)
• cf 20% prevalence of allergic rhinitis
Child with chronic disease 10%
• Barrier failure
• Inadequate respiratory clearance
• Obstruction
• CV problems
• Foreign body
• Resistant organism
• Continuous reinfection eg contaminated
water

Host factors important in defense
• Skin
• Mucous membranes
• Lysozyme
• Digestive enzymes
• Respiratory mucous clearance mechanisms
Generalised anatomical factors predisposing
to recurrent infections in children
• Skin defects eg burns, eczema
• Multiple mechanisms: barrier loss,
nutritional compromise, secondary immune
defects, use of antibiotics, nosocomial
infections, immobility
• Infections in multiple anatomical areas

Cystic fibrosis
• Most patients identified by neonatal screening
• Can present later
• Children can look relatively well
• Nasal polyps in children
• Chronic cough, chronic sputum production,
clubbing
• Sweat testing +/- genetic testing
• Genetic testing

Localised anatomical factors predisposing to
recurrent infections in children
• Localised defects eg Bronchial obstruction
• Most infections in the same system and
same location
• Infections may be slow to respond to Rx
• There may be localised complications eg
bronchiectasis.
• Investigations and management focused on
correcting the anatomical defect.

Lobar pneumonia

Localised anatomical factors predisposing to
recurrent infections in children
• Localised defects eg enlarged adenoids
• Frequent URTIS and OME
• ENT referral if suspected.
• Surgery +/- tympanostomy tubes

Localised anatomical factors predisposing to
recurrent infections in children
• Localised defects eg chronic tonsillitis
• ENT referral
• Removal if indicated
• Frequent cause of ill health, URTIS,
abdominal symptoms etc
• Foreign bodies- unilateral nasal symptoms

The immune response to cancer
Infections in cancer
• Destruction of the immune system esp Leukemia
• Drugs- chemotherapy
• Radiotherapy- multiple mechanisms
• Localised obstruction eg Ca bronchus
• Malnutrition
• Probably worse with hematological malignancy

Suspected immunodeficiency 10%
• Family history of immunodeficiency or unexplained early
death (eg, before age 30 years)
• Failure to gain weight or grow normally (failure to thrive)
• Need for intravenous antibiotics and/or hospitalization to
clear infections
• Six or more ear or respiratory tract infections/ year
• Two or more serious sinus infections or pneumonias within
one year
• Four or more new ear infections within one year
• Two or more episodes of sepsis or meningitis in a lifetime
• Two or more months of antibiotics with little effect

• Recurrent or resistant oral or cutaneous candidiasis
• Recurrent deep skin or organ abscesses
• Infection caused by an unusual microbe and/or in an unusual location
• Complications from a live vaccine (eg, rotavirus, varicella, and BCG vaccines)
• Chronic diarrhea
• Nonhealing wounds
• Extensive skin lesions
• Persistent lymphopenia (age dependent)
• Unexplained autoimmunity or fevers
• Granulomas
• Hemophagocytic lymphohistiocytosis (HLH)
• Lymphoma in infancy
• Features typical of syndromic PIDs
Suspected immunodeficiency

Primary immune deficiency
Stem
cell
Hematopoeisis
BM
Thymus
CD4
CD8
IgG
IgA
IgM
antigenX
XXX
XX
XTh1
Th2
X

• B cell defects- Bruton’s, CVID, XLA
• T cell defects- di George
• Combined defects- SCID, XHIM
• Other well-defined disorders- WAS
• Complement defects
• Phagocytic defects- CGD
• Disorders of innate immunity- TLRs
• Autoinflammatory disorders- FMF, TRAPS
• Disorders of Apoptosis- ALPS
• Phenocopy
WHO classification of
primary immune deficiency

Patients with PID by Reported Diagnosis
Source: IDF Patient Survey N=2815
12%
1%
1%
34%
24%
17%
8%
4%
4%
2%
2%
0% 10% 20% 30% 40%
Common Variable
IgG Subclass
IgA Subclass
X-Linked Agamma
Severe Combined
CGD
Hyper IgM
DiGeorge
Wiskott-Aldrich
Ataxia
Other

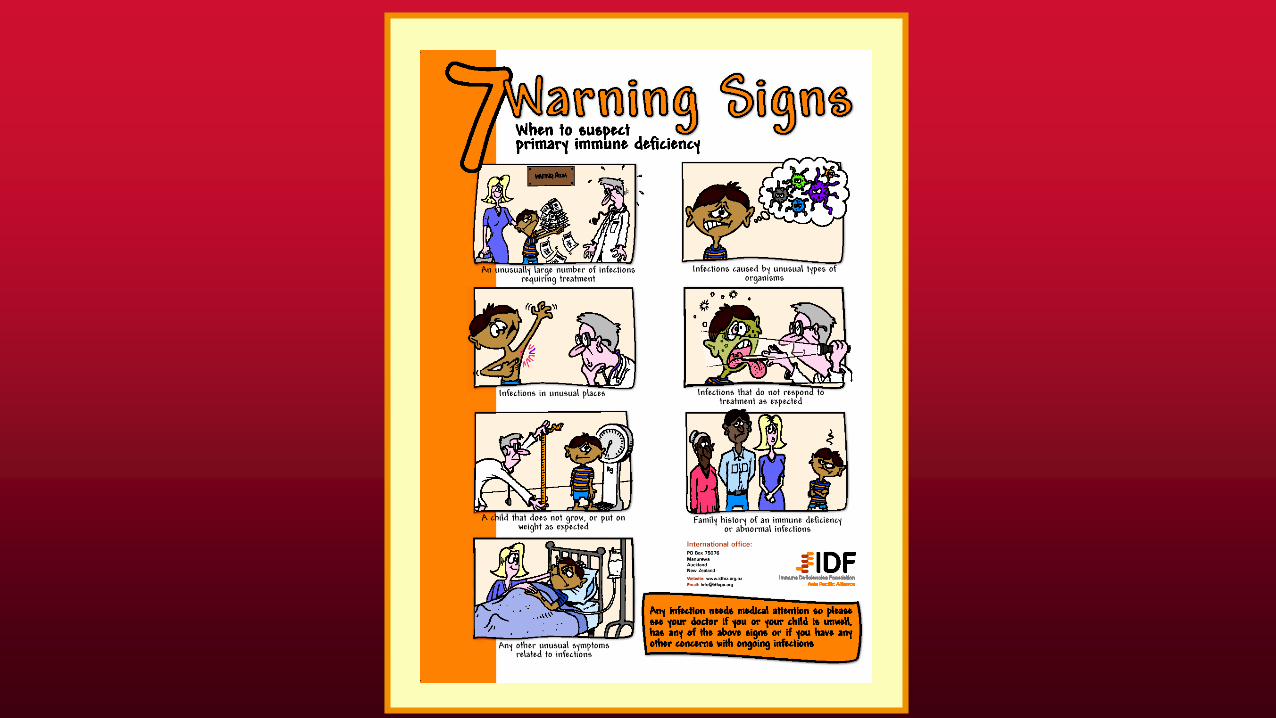
When to suspect primary immune deficiency
• Increased # of infections
• Unusual organisms
• Unusual site of infections
• Failure to respond as predicted
• Failure to thrive/ growth retardation
• Other clinical features
• Family history


Times Hospitalized before Diagnosis
None
30%
One
17% 2-5
32%
6-10
10%
11-20
6%
21+
5%
Source: IDF Patient Survey N=2,708

Possible presentations of PID
• ID: Rec bacterial, fungal, viral infections
• GI: Chronic diarrhea with Giardia, Crypto
• Chest: Bronchiectasis, bronchitis
• Rheum: SLE (comp), Oligoarthritis
• ENT: Sinusitis, otitis media
• Endo: Mucocutaneous Candidiasis
• Haem: AIHA, tcp, lymphoma
• Onc: Lymphoma, SCC


Recognition of PIDs
• Institution of correct therapy
• Prevention of complications
• Addressing issues related to chronic disease
(marriage, work, school, support IDFNZ)
• Genetic implications for family members

Health Status: Before and
After Treatment
28%
29%
16%4%
4%
11%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Year Before Diagnosis Last Year on IVIG
Good
Very Good
Excellent

Why Patient was Initially Tested for PID
7%
1%
66%
6%
11%
8%
0% 20% 40% 60% 80%
Family History
Routine Checkup
Repeated Infections
Unusual Infection
Overwhelming Infection
Other
PID: Typical history
• 2yr old boy
• Recurrent chest infections since 6 mo
• Frequent OM
• Family history: 2 uncles died at 1 yr of age
• OE/ Absent tonsils
• Inx IgG 1.2 g/l
• No response to specific vaccines

Some examples of primary immune deficiencies
• T cell (HIV), diGeorge
• B cell Bruton’s, CVID
• Combined SCID, XHIM,
• Complement C1inh
• Neutrophil CGD, LAD

T cell immune defects
• T cell immune defects eg diGeorge
syndrome
• Infections: viral, fungal, parasitic, protozoal
• Impaired growth in children
B cell immune defects
• B cell immune defects eg XLA (Brutons)
• Infections: bacterial, protozoal, (viral)
• Normal growth in children
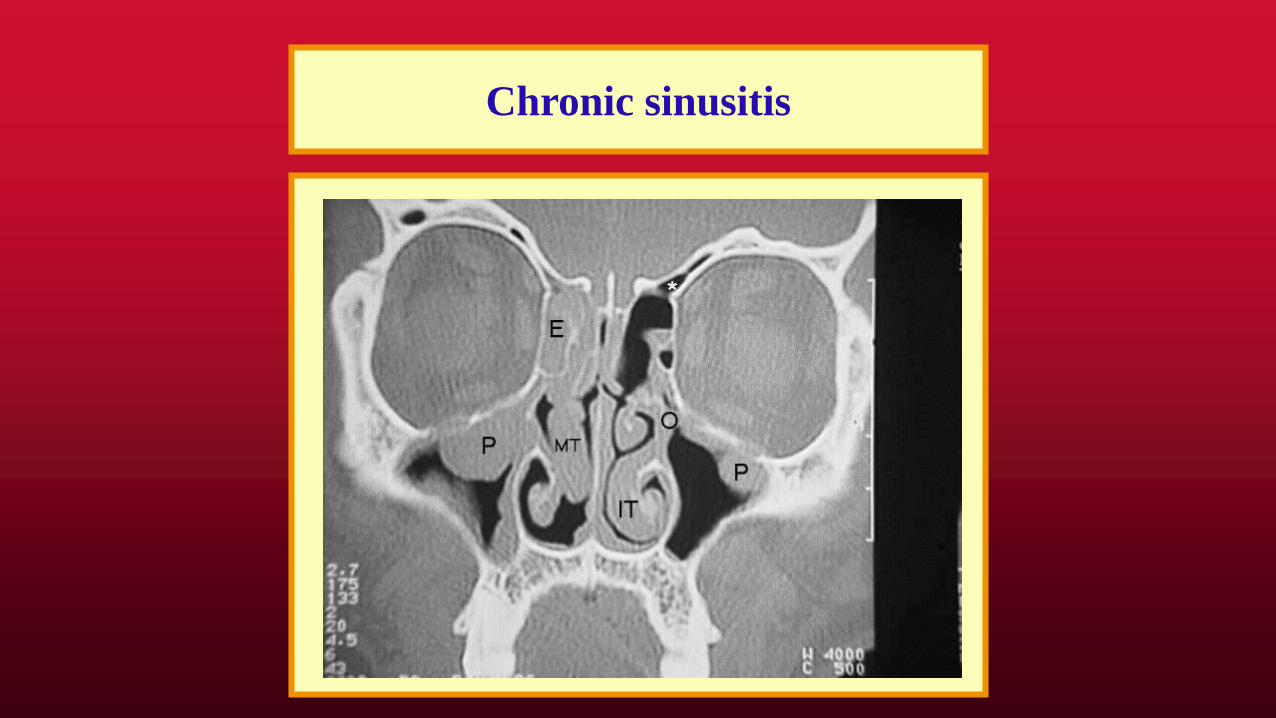
Chronic sinusitis

Chronic sinusitis

Bronchiectasis



Giardia

IVIG

Screening tests for immune deficiency
• FBC ESR
• Blood film
• Immunoglobulins
• Specific antibodies: proteins eg tetanus toxoid
• Specific antibodies: carbohydrates blood group
• HIV test
Interpretation of immunoglobulin levels
• Age of the child
• Prematurity
• Concurrent infections
• Medication
• Lab-lab variations

Interpretation of immunoglobulin levels

Advanced tests for PID
• Vaccine responses
• Flow cytometry
• Electron microscopy
• Molecular diagnosis

Summary: An approach to the child
with recurrent infections
• Accurately document the numbers of infections
• Are the infections localised to 1 organ system?
• Are they localised to one anatomical location?
• Are there obvious predisposing factors? Incl smk
• Failure to thrive/ growth retardation?
• Unusual features of the infections
• Relevant Family history

Main categories
• Normal child 50%
• Child with atopy 30%
• Child with anatomical problems 10%
• Immunodeficiency: primary or secondary
10%