Embed Size (px)
Citation preview

Journal ofNeurology, Neurosurgery, and Psychiatry 1991;54:345-350
The assessment of visuo-spatial neglect after acutestroke
S P Stone, B Wilson, A Wroot, PW Halligan, L S Lange, J C Marshall, R J Greenwood
AbstractForty four consecutive patients withacute hemispheric stroke and forty sevenelderly controls with no neurologicaldisease were assessed for visuo-spatialneglect, using a modified neglect test bat-tery. Neglect was found to be equallycommon in patients with right hemi-sphere and left hemisphere stroke threedays after stroke (72% versus 62%). Itwas more severe in those with a righthemisphere stroke and resolved morefrequently in those with a left hemis-phere stroke. The battery was validatedagainst an occupational therapist'sassessment of neglect on self-care tasks.The inter-observer reliability was goodand it was possible to monitor changesover time with the battery.
St Bartholomew'sHospital, LondonDepartment ofNeurosciencesS P StoneR J GreenwoodDepartment ofOccupational TherapyA WrootDepartment ofRehabilitationStudies, SouthamptonGeneral Hospital,University ofSouthampton,SouthamptonB WilsonRivermeadRehabilitation Centre,OxfordP W HalliganDepartment ofNeurosciences,Charing CrossHospital, LondonL S LangeNeuropsychologyUnit, The RadcliffeInfirmary, OxfordJ C MarshallCorrespondence to:Dr Stone, AcademicDepartment, GeriatricMedicine, Royal FreeHospital, Pond Street,London NW3 2QG, UKReceived 20 October 1989and in final revised form24 August 1990.Accepted 11 September 1990
Visuo-spatial neglect is an important predic-tor of poor outcome after stroke."' Thenatural history of neglect after stroke,however, remains unclear. Estimates of thefrequency of visuo-spatial neglect (33-85% inright and 0-25% in left hemisphere strokes)and of the frequency of recovery (0-50% inright and 60% in left hemisphere stroke) vary
widely.2'4 10The variation in these estimates is the
result, firstly, of the use of different tests todetect visuo-spatial neglect and, secondly, ofthe use of only one or two tests chosen oftenon the basis of their simplicity. This practiseis unsatisfactory, because clinical neglect isnot an all or none phenomenon." 12 Neglect isnot observed in all activities or all clinical testsat any one time.'3 It cannot therefore beassumed that all tests assess or measure thesame neuropsychological variable or mechan-ism.'4 15
Over 50 bedside tests of visuo-spatialneglect have been used in various combina-tions. The tests most commonly used are
probably line cancellation and drawingtasks.4616 Recently, Wilson et al developed theBehavioural Inattention Test (BIT),7 18 whichwas standardised on convalescent strokepatients. The BIT has been shortened andmodified for use with acute stroke patients.'9The aim of the current study was to evaluatethis modified battery as a clinical tool fordetecting and monitoring visuo-spatial neglectin patients with an acute stroke.
MethodForty four consecutive patients with a mean
345
(SD) age 71 2 (12 8) years, who had beenadmitted to hospital with an acute hemi-spheric stroke, were investigated. Eighteenhad a right hemispheric stroke, 26 had a lefthemispheric stroke. The diagnosis was confir-med by a physician (SPS) who administeredthe test battery at three days. Patients were re-examined at three months because after thisinterval most neurological deficits, includingvisuo-spatial neglect, made most of theirrecovery.9202' All patients received a non-con-trast CT brain scan at three to five days. Twopatients had a haemorrhage, the rest had aninfarct. In 21 patients (48%), the findings onexamination were validated against anoccupational therapist's assessment of neglectin activities of daily living (ADL). Inter-observer reliability was also established using12 of the stroke patients.Forty seven age-matched controls were also
examined once (see following paper).
The neglect test batteryAll tests were presented in front of thesubject's midline with the examiner seateddirectly opposite. No time limit was imposed.After patients had completed a test they wereasked to check that they had finished. Somepatients were unable to attempt tests due tothe level of consciousness, language difficultiesor fatigue. A fundamental feature of patientswith visuo-spatial neglect due to a righthemisphere lesion is that they begin tasks onthe right hand side.2223 In four of the eighttests, the presence of a "Right Hand Start"was assessed. The tests were administered inthe following order.
1) POINTING TO OBJECTS LOCATED ABOUT THE
WARD24 (fig 1) The patient was asked to pointto and/or name all the objects that they couldsee on both sides scattered about their hospitalroom or ward. The examiner stood directly
Chart
Sink Gx X Gown
/ /~~~~x x
X X
|0?/x Sainsbury'sbag
Figure I Left visuo-spatial neglect on Pointing toobjects.
on Decem
ber 18, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.54.4.345 on 1 April 1991. D
ownloaded from

Stone, Wilson, Wroot, Halligan, Lange, Marshall, Greenwood
Figure 2 Left visuo-spatial neglect on Menu(of words underlined),with a right hand start(arrow).
BIT
X tTomato soup Grapefruit
Pork chop Ham & eggs
Shepherd's Pie Fried haddock
Jam tart Cheese
Ice cream Biscuits
Coffee Apple pie
Tea Roast chicken
hamburger Lamb chop / \
salad Turkey / >< >Xmilk Veal X X
appletart Boiled eggs X_
/ \
sandwiches Melon
- \~~~~~ K~--behind the patient. Using a photocopy of aclosed semicircle, with the position of thepatient's head marked at the centre of the baseand with marks on the circumference at 45, 90and 135 degrees, the examiner noted whichobjects were situated at 0, 45, 90, 135 and 180degrees and used these as landmarks. Whenthe patient pointed to or named objects in theroom the examiner marked their approximateposition relative to the landmarks andmeasured the approximate number of degreesomitted.
-X
Figure 4 Left visuo-spatial neglect on Line cancellationwith a Right Hand Start (arrow).
the article (117 words in small newsprint)were recorded separately. The presence orabsence of "Right Hand Start" was recorded.This test was not given to patients with a lefthemisphere stroke because the pilot study19that modified the BIT found that most of themhad reading difficulties.
2) FOOD ON A PLATE"7 Patients were asked topoint to each food item in a lifesize colourphotograph of a plate containing eight foods.Where necessary the examiner demonstratedwhat was required. The total number of itemsomitted was recorded. Correct verbal iden-tification of the food items was not required.
3) READING A MENU'7 (fig 2) The patient wasasked to open and read aloud from a menuthat listed 12 items of food on the left pageand 12 on the right. The number of wordsomitted on the left, right, and in total wasrecorded. Aphasic patients were allowed topoint to words. In a patient with a righthemisphere stroke "Right Hand Start" wasdefined as a failure to begin reading from thefirst left hand column2526 (see arrow on fig 2).
4) READING A NEWSPAPER ARTICLE (adaptedfrom 17) (fig 3) Patients were asked to readthe "newspaper" extract aloud. The examinermarked on a photocopy any words omitted.Some patients were unable to read small print,so the number of words omitted from theheadlines (10 words in bold print), theparagraph (five words in smaller capitals) and
Driver killed, 30 hurt aspacked train rams a loco
cab in a horror train smash last By CAROLE NEWTON the four-coach diesel when itnight. crashed near the vilage ofChinley
TRIP TEND Thiny others were hurt as a seriously - wererushedtohos- near Buxton.passenger train rammed two pital in a fleet of ambulances. The alarm was raised by acoupled locor ves on a track n young motor-cyclist who saw
- Last night emerency the crash and ran to a nearby
INJUREt rePennines. el e 0 school for help.the driver from the passengerThe injured- three of them train which was derailed. Two nurses on board the train
Figure 3 Left visuo-spatial neglect on the Newspaper(of words underlined).
5) LINE CANCELLATION (adapted from 1727) (fig4) The patient was presented with a sheet ofpaper on which 40 one inch lines had beenmarked in seven columns. The patient wasrequired to cross out all the lines on the pageafter the examiner had demonstrated what wasrequired by crossing out the four lines in thecentre column. A "Right Hand Start" wasconsidered present if the first lines to be can-celled were in the sixth or seventh columns onthe right of the page (see arrow in fig 4). Thenumber of lines omitted on the right, the leftand in total was recorded. If the patient'sdominant hand was too weak to cross out linesand they were unable to use the other hand,they were allowed to point to each line, whichthe examiner then crossed out.
6) STAR CANCELLATION17 (fig 5) Patients werepresented with 56 small stars mixed up withmany large stars and capital letters. They wereinstructed to cross out the small stars after theexaminer had demonstrated this, crossing outtwo centrally positioned small stars. Thenumber of small stars omitted on the left, theright and in total was recorded. A "RightHand Start" was considered present if the
:.G *ARE
Figure 5 Left visuo-spatial neglect on Star cancellation,with a Right Hand Start.
346
/ --l
-- -7.
---_ --IC
on Decem
ber 18, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.54.4.345 on 1 April 1991. D
ownloaded from

The assessment of visuo-spatial neglect after acute stroke
'i
Figure 6 Left visuo-spatial neglect on Coin selection (unmarked coins).
patient began cancelling stars in the righthand third of the page. Patients with a weakdominant hand were allowed to point to eachstar.
7) COIN SELECTION17 (fig 6) A large card(32 x 21 cm) with three coins of each of thefollowing values (2p, 5p, 10p, 20p, 50p, £1)was presented to the patient with the three fivepence coins on the side opposite their cerebrallesion. The patient was asked to point to eachof the coins in turn. The examiner noted theresults on a photocopy of the test card. Thenumber of omissions on the left, right and intotal was recorded. Occasionally the examinerplaced a loose coin of the value required infront of aphasic patients or wrote the value ofthe coin on a piece of paper to help themunderstand which coin was required.
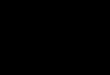
Figure 7 Right visuo-spatial neglect on Figurecopying with Crowding.
8) FIGURE COPYING FROM THE LEFT'7 (fig7) The patient was presented with a piece ofpaper divided into six squares. In the threesquares on the left were figures of a fourpointed star,7 a cube28 and a daisy.29 Thesewere to be copied into the empty three spaceson the right side. The number of major omis-sions (for example, half a cube) and the num-ber of minor omissions (for example, a leaf)was recorded for each figure. Each major omis-sion was given an arbitrary score of two andeach minor omission a score of one..' This testwas not given to those patients with a righthemisphere stroke as the pilot study thatmodified the BIT'9 indicated that this test wasless sensitive than many others. It proveduseful, however, for patients with left hemi-sphere stroke who often ignored the emptyright spaces and "crowded" their copies intothe left hand side of the page.
CRITERIA FOR VISUO-SPATIAL NEGLECTTo establish a normal range of performancefor each test the controls were examined; theseresults are given in an accompanying paper.Visuo-spatial neglect was considered presentin patients if they made more omissions onany one test than the age-matched controls.Thus two or more omissions on meal; one ormore on menu; five or more on lines; 16 ormore on stars; four or more on coins; two ormore on headlines; two or more on paragraph;seven or more on article; and 50 or moredegrees on pointing was regarded as evidenceof neglect. Major or minor omissions on leftfigure copying, Crowding and a Right HandStart on the reading tests never occurred incontrols and were thus considered clinicalindicators of neglect.
In addition, any stroke patient making threeunilateral omissions on coin sorting was con-sidered to have neglect on that test if neglectwas also present on another test. Similarly,neglect was considered present in star can-cellation when a stroke patient omitted be-tween six and 15 stars if there were at leasttwice as many omissions on one side of thepage as the other4 and if neglect was present inanother test. Also, a Right Hand Start on lineand star cancellation was taken as indication ofneglect if neglect was present on these orother tests. Combinations of these featureswere not observed in the controls.
SCORING THE TESTSThe total number of omissions made on lines,stars, meal, menu and coins was expressed as apercentage of the total number of items ineach test.4 The number of degrees omitted onpointing was expressed as a percentage of 180degrees. The number of words omitted inheadlines was expressed as a percentage out of10, the number omitted on Paragraph as apercentage of five, and the number in theArticle was expressed as a percentage of 117.The score for figure copying was convertedinto a percentage (of a maximum score of six).
347
on Decem
ber 18, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.54.4.345 on 1 April 1991. D
ownloaded from

Stone, Wilson, Wroot, Halligan, Lange, Marshall, Greenwood
Table I Number of stroke patients able to attempt each test at three days and numberwith neglect on each test
Right hemisphere stroke Left hemisphere stroke(n = 18) (n= 26)
Number patients Number Number patients Number withattempting with attempting with
Test test neglect test neglect
Point 16 11 20 9Meal 16 10 20 9Menu 16 8 20 10Newspaper 16 13 - -Lines 16 10 20 11Stars 15 11 14 8Coins 14 7 15 7Lfig - - 16 1
The percentage score on each test was thengraded: Grade 0: no neglect; Grade 1: up to20% of items omitted on the test; Grade 2: 21-40% items omitted; Grade 3: 41-60%; Grade4: 61-80%; Grade 5: 81-100%. Right HandStart and Crowding were both considered to bequalitative rather than quantitative measures ofneglect and were noted but not scored.
Results1 Stroke patients three days after stroke (table 1)At three days after stroke, two patients with aright hemisphere stroke could not be assessedon any test because of coma. All remaining 16patients could be tested on Pointing, Meal,Menu, Newspaper and Lines. One patient wastoo tired to do stars or coins, another could notrecognise coins.
Five patients with a left hemisphere strokecould not be assessed at three days because ofcoma or severe aphasia. Most of the remaining21 could be assessed on Pointing, Meal, Menuand Lines. Aphasia made it impossible forsome patients to attempt Stars, Coins andFigure copying because they were unable tounderstand the instructions.At three days 13/18 (72%) patients with a
right hemisphere stroke showed neglect on atleast one test. Neglect was present in 16/26(62%) patients with a left hemisphere stroke.The tests most likely to detect neglect in a
patient with a right hemisphere stroke wereNewspaper, Stars, Pointing, Meal and Lines(table 1). Eleven ofthese patients demonstrateda Right Hand Start.For patients with a left hemisphere stroke the
most likely tests to detect neglect were Meal,Menu, Lines and Pointing (table 1). Five of
Table 2 Number of stroke patients able to attempt each test at three months andnumber with neglect on each test
Right hemisphere stroke Left hemisphere stroke(n= 12) (n= 15)
Number patients Number Number patients Number withattempting with attempting with
Test test neglect test neglect
Pointing 1 1 3 15 2Meal 11 6 15 2Menu 11 3 15 3Newspaper 11 5 - -Lines 1 1 4 15 0Stars 11 7 12 3Coins 11 5 12 3Lfig - - 15 0
these patients showed Crowding. Althoughonly 10 patients could attempt Stars, eight ofthese exhibited neglect on that test.
2 Stroke patients three months after stroke(table 2)Twelve of the 13 patients with neglect due to aright hemisphere stroke survived until followup at three months. One patient was toodepressed to be tested. The 11 others were ableto attempt most tests. Both patients who hadoriginally been unable to do any test died.
Fourteen of the 16 patients with neglect dueto a left hemisphere stroke survived until followup at three months. One of the five who hadoriginally been unable to do any test survived.The 15 survivors were able to cooperate onnearly every test although language difficultystill prevented some patients understandingthe Coins and Stars test requirements.
Neglect was present in nine patients with aright hemisphere stroke (75%) and five lefthemisphere stroke patients (33%).
In those with a right hemisphere stroke thetests most likely to detect neglect were Stars,Meal, Coins and Newspaper. A Right HandStart was present in nine of these patients. Inpatients with a left hemisphere stroke the testsmost likely to detect neglect were Menu, Starsand Coins.
3 Validity of the test batteryTo ascertain the validity of the test battery anoccupational therapist blind to the results ofthe battery carried out an assessment on 21 ofthe patients, using the following checklist of"neglect behaviours".1) Did the patient fail to orientate to environ-mental stimuli on the side opposite the cerebrallesion?2) Did the patient fail to dress, wash or groomtheir contralateral side?3) Did the patient bump into doorways orobstacles on the contralateral side, when walk-ing or using a wheelchair? If using the latter,were they unable to turn contralaterally? Ifmobile, did the patient veer diagonally towardsthe contralateral side?4) Could any failure or reluctance to use thecontralateral limbs be attributed to neglectrather than weakness or apraxia?3'5) Did the patient show lack of awareness oflimbs with poor positioning?3'Four patients (two with a right, two with a
left hemisphere stroke) had no neglect on thebattery and none on the occupational thera-pist's checklist. The remaining 17, (12 with aright, five with a left hemisphere stroke), hadvisuo-spatial neglect on the test battery. Thir-teen of these had neglect on at least threechecklist items, two had neglect on two items(orientation, washing/dressing), and oneneglected on one item (orientation). Onepatient with marked left visuo-spatial neglecton the battery, a left homonymous hemianopiaand no hemiparesis, had no neglect on thechecklist.
348
on Decem
ber 18, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.54.4.345 on 1 April 1991. D
ownloaded from

The assessment of visuo-spatial neglect after acute stroke
Table 3 Severity of neglect in 11 patients with a right hemisphere and in 14 patientswith a left hemisphere stroke at three days and at three months after stroke
Right hemisphere stroke Left hemisphere strokeMedian score Median score
Test 3 days 3 months 3 days 3 months
Pointing 3-0 0.0 1-0 0 0Meal 3-0 1-0 0.0 0-0Menu 30 0-0 2-0 0-0Lines 4-0 0-0 2-0 0-0Stars 3-0 2-0 3-0 0-0Coins 3-0 2-0 2-0 0-0Headlines 1.0 0-0 - -Paragraph 4-0 0-0Article 2-0 0-0 - -
Lfig - - 0-0 0-0
4 Reliability of the test batteryInter-observer reliability was established bythe simultaneous scoring of 12 patients (eightwith a right and four with a left hemispherestroke) with neglect by two examiners trainedin the administration of the battery.Each patient was assessed on nearly every
test, although only 11 were able to do Pointing,Meal, Menu and Stars. There was agreement as
to the presence or absence of neglect in everytest except in Coins in one patient to whom thenewer coins may have been unfamiliar. Bothobservers agreed on the graded score on eachtest except in Newspaper in one patient whomumbled inaudibly.
5 Sensitivity to changes in neglectTable 3 shows the median test scores of thosepatients presenting with neglect at three daysafter stroke who survived and were able to beexamined at three months. There were 11 witha right and 14 with a left hemisphere stroke.At three days neglect was greater in patients
with a right than in patients with a left hemi-sphere stroke, but the difference only reachedsignificance for Lines (p = 0 04; Mann-Whit-ney tests). At three months neglect haddeclined on all tests in right hemispherepatients. This was significant at the 0 02 levelfor Lines, Stars, and Pointing; and at the 0 05level for Paragraph. Neglect also declined inleft hemisphere strokes. This was significant atthe 0-01 level for Lines, and at the 0 05 level forPointing, Meal, Menu, and Stars (Wilcoxontests).
DiscussionThe study describes the use of a test battery todetect, measure and monitor visuo-spatialneglect. It is relevant, valid, reliable, simple to
administer, sensitive and gives a result that canbe communicated to fellow professionals.32The battery includes tests from the BIT
which simulate performance in everydayactivities, for example, reading, looking aroundthe room, selecting coins, and eating. Thesetests would seem more relevant to real life andmay indicate to therapists appropriate areas fortreatment.'7 18 The validity study showed that16 out of 17 patients with neglect on thebattery, had neglect on the OT checklist. Thismethod ofvalidating clinical tests ofneglect hasbeen used by Battersby et al who found that
neglect on clinical testing did not always gen-eralise to daily activities.2333 We observed onesuch patient, but cannot say whether such adiscrepancy is an example of a dissociationbetween neglect in different tasks.'5
In 12 patients assessed by two observers, thereliability of the battery was good with respectto the presence and severity of neglect in eachtest. The tests were easy to administer. Thepresence of aphasia was not as great an obstacleto assessment as had been anticipated forsufficient gestural comprehension was oftenretained. Seven consecutive patients whoseperformance was timed completed the batteryin a mean (SD) time of 11 minutes 10 seconds (3minutes 1 1 seconds).The battery was sensitive to the presence of
visuo-spatial neglect, and to changes in itsseverity over time. At three days the incidenceof visuo-spatial neglect was 72% (right hemi-sphere) and 62% (left hemisphere). At threemonths the incidence in survivors was 75%(right hemisphere) and 33% (left hemisphere).Other studies which have used a simple linecancellation and figure copying battery4 6 havereported a lower incidence of visuo-spatialneglect in acute stroke. Had Line cancellationbeen used as the sole test of neglect theincidence of neglect would have been 55%(right hemisphere) and 42% (left hemisphere)at three days after stroke. At three months theincidence ofneglect would have been only 33%(right hemisphere) and 0% (left hemisphere).The likely reason for our higher incidence ofneglect is that we used a larger battery andconsidered neglect to be present when itappeared in a single test.30 Neglect may be task-specific.'1115 Assessment of patients by a largerbattery is therefore more likely to result in thedetection of visuo-spatial neglect than assess-ment by a one or two test battery.0 The use of alarger battery has a particular bearing on thedetection of neglect in left hemisphere stroke.Although some patients were unable to under-stand what was required in some tests, theyoften understood and attempted others. Thismay be why neglect was nearly as common afterleft hemisphere stroke as after right. Otherworkers have found this273034 but the classicview is that neglect is associated almost solelywith right brain damage.35There is no one standard method of measur-
ing neglect.417 1 13036 Some sensitive indicatorsin our battery are not scorable on an ordinalscale, for example Right Hand Start and Crow-ding but they remain useful clinical signs ofneglect, possibly reflecting abnormalities in eyemovements reported in patients with unilateralbrain damage who begin visual search tasks byexploring ipsilesional space.2234 Expressing thepercentage of items omitted from each test as agrade on a 0-5 scale is simple and each grade iseasily understood. It avoids giving too muchweight to small changes over time in the rawscore, expresses the result of each test in thesame arbitrary units and enables change to bemonitored. Our observation that neglect ismore severe in those with a right than in thosewith a left hemisphere stroke is consistent withother reports.' '
349
on Decem
ber 18, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.54.4.345 on 1 April 1991. D
ownloaded from

Stone, Wilson, Wroot, Halligan, Lange, Marshall, Greenwood
In conclusion, the battery takes into accountthe behavioural inconsistency of neglect and issuitable for use with patients after an acutestroke.
SPS was supported by a grant from the Chest Heart and StrokeAssociation. We are grateful to Dr J R Jenner, Consultant inRehabilitation, and in particular to Dr CM C Allen, ConsultantNeurologist, Addenbrookes, Cambridge for early discussions;and also the library staff of the Royal Society of Medicine.
Figures 2, 4-7 are produced with kind permission of theThames Valley Test Company.
I Feigenson JS, Mccarthy ML, Greenberg SD, FeigensonWD. Factors influencing outcome and length of stay in astroke rehabilitation unit. Part 2. Comparison of 318screened and 248 unscreened patients. Stroke 1977;8:657-62.
2 Kinsella G, Ford B. Acute recovery patterns in strokepatients. Neuropsychological factors. Med J Australia1980;2:663-6.
3 Denes G, Semenza C, Stoppa E, Lis A. Unilateral spatialneglect and recovery from hemiplegia. A follow up study.Brain 1982;105:543-52.
4 Fullerton KJ, Mackenzie G, Stout RW. Prognostic indicesin stroke. Q JMed 1988;66:147-62.
5 Adams GF, Hurwitz LJ. Mental barriers to recovery fromstrokes. Lancet 1963;2:532-7.
6 Cutting J. The study of anosognosia. J Neurol NeurosurgPsychiatry 1978;41:548-55.
7 Oxbury JM, Campbell DC, Oxbury SM. Unilateral spatialneglect and impairment of spatial analysis and visualperception. Brain 1974;97:551-64.
8 Hier DB, Mondlock J, Caplan LR. Behavioural abnor-malities after right hemisphere stroke. Neurology1983;33:337-44.
9 Hier DB, Mondlock J, Caplan LR. Recovery of behaviouralabnormalities after right hemisphere stroke. Neurology1983;33:345-50.
10 Campbell DC, Oxbury SM. Recovery from unilateral spatialneglect? Cortex 1976;12:303-12.
11 Mesulam M-M. A cortical network for directed attentionand unilateral neglect. Ann Neurol 1981;10:309-25.
12 Friedland RP, Weinstein EA. Hemi-inattention and hemi-sphere specialization: introduction and historical review.Advances in Neurology 1977;18:1-31.
13 Leicester J, Sidman M, Stoddard LT, Mohr JP. Somedeterminants of visual neglect. J Neurol Neurosurg Psy-chiatry 1969;32:580-7.
14 De Lacy Costello A, Warrington EK. The dissociation ofvisuo-spatial neglect and neglect dyslexia. J NeurolNeurosurg Psychiatry 1987;50:1110-6.
15 Bisiach E, Perani D, Vallar G, Berti A. Unilateral neglect:personal and extra-personal. Neuropsychologia1986;24:759-67.
16 Andrews K, Brocklehurst JC, Richards B, Laycock PJ. Theprognostic value of picture drawings by stroke patients.Rheum Rehabil 1980;19:180-8.
17 Wilson B, Cockburn J, Halligan P. Development of abehavioural test of visuo-spatial neglect. Arch Phys Med1987;68:98-102.
18 Wilson B, Cockburn J, Halligan P. The Behavioural Inatten-tion Test. Fareham, Hampshire: Thames Valley TestCompany.
19 Stone SP, Wilson B, Rose FC. The development of astandard test battery to detect, measure and monitorvisuo-spatial neglect in acute stroke. Int J Rehab Res1987;10: 110.
20 Skilbeck CE, Wade DT, Hewer RL, Wood VA. Recoveryafter stroke. J Neurol Neurosurg Psychiatry 1983;46:5-8.
21 Allen CMC. Predicting the outcome of acute stroke: aprognostic score. J Neurol Neurosurg Psychiatry1984;47:475-80.
22 Chedru F, Leblanc M, L'Hermitte F. Visual searching innormal and brain-damaged subjects (a contribution to thestudy of uni-lateral attention). Cortex 1973;9:94-1 11.
23 Weinburg J, Diller L, Gordon WA, Gerstmann LJ, Lieber-mann A, Lakin P, et al. Visual scanning training effect onreading related tasks in acquired right brain damage. ArchPhys Med Rehabil 1977-58:479-86.
24 Patterson A, Zangwill 0. Disorders of visual space percep-tion associated with lesions of the right cerebral hemis-phere. Brain 1944;67:331-58.
25 Mesulam MM. The functional anatomy and hemisphericspecialization for directed attention. The role of theparietal lobe and its connectivity. Trends Neurosci1983;6:384-7.
26 Holmes G. Disturbances ofvisual orientation. Br J Ophthal-mol 1918;2:449-68.
27 Albert ML. A simple test of neglect. Neurology 1973;23:658-64.
28 Gainotti G, Messerli P, Tissot R. Qualitative analysis ofunilateral spatial neglect in relation to laterality ofcerebrallesions. J Neurol Neurosurg Psychiatry 1972;35:545-50.
29 Gregory ME, Aitken JA. Assessment of parietal lobe func-tion in hemiplegia. Occupational Therapy 1971;34:9-17.
30 Ogden JA. Anterior-posterior interhemispheric differencesin the loci of lesions producing visual hemi-neglect. Brainand Cognition 1985;4:59-75.
31 Heilman KM, Watson RT, Valenstein E. Neglect andrelated disorders. In: Heilman KM, Valenstein E, eds.Clinical Neuropsychology OUP 1985;243-50.
32 Wade DT, Hewer RL, Skilbeck CE, David RM, eds. Stroke.A critical approach to diagnosis, treatment and man-agement, London: Chapman and Hall, 1985.
33 Battersby WS, BenderMR, Pollack M, Kahn RL. Unilateral"spatial agnosia" ("inattention") in patients with cerebrallesions. Brain 1956;79:68-93.
34 Chain F, Leblanc M, Chedru F, L'Hermitte F. Negligencevisuelle dans les lesions posterieures de l'hemispheregauche. Rev Neurol 1979;135:105-26.
35 Haecen H. Clinical symptomatology of right and left hemi-sphere lesions. In: Mountcastle VB, ed. Interhemisphericrelations and cerebral dominance. Baltimore: John HopkinsPress, 1962.
36 Wade DT, Wood VA, Hewer RL. Recovery of cognitivefunction soon after stroke; a study of visual neglect,attention span and verbal recall. J Neurol NeurosurgPsychiatry 1988;51:10-13.
350
on Decem
ber 18, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.54.4.345 on 1 April 1991. D
ownloaded from