Embed Size (px)
Citation preview

Arch Orthop Trauma Surg ( 1984) 103:201-211Archives of Orthopaedicand Traumatic Surgery© Springer-Verlag 1984
On the Pathogenesis of Spondylosis Deformans and Arthrosis Uncovertebralis:Comparative Form-Analytical Radiological and Statistical Studieson Lumbar and Cervical Vertebral Bodies
H.-J Pesch, W Bischoff', Th Becker l, and H Seibold 2
1 Pathologisches Institut (Director: Prof Dr V Becker), Krankenhausstra Be 8-10, and2 Institut fir Medizinische Statistik und Dokumentation (Director: Prof Dr L Horbach) der Universitit Erlangen-Niirnberg,
Waldstra Be 6, D-8520 Erlangen, Federal Republic of Germany
Summary To investigate the etiopathogenesis of thecommon clinical symptoms of the lower lumbar spine(LS) and cervical spine (CS) (lower back pain andlocal cervical spine syndrome), the dimensions of thethird to fifth lumbar vertebral bodies (LVB) and thefifth to seventh cervical vertebral bodies (CVB) werestudied quantitatively and morphometrically in fron-tal and sagittal planes, as a function of sex and age, in105 human cadavers of both sexes aged between 16and 91 years The evaluation was done in X-ray pic-tures of 100-ptm-thick polished bone sections withthe aid of the Macro Facility of the Leitz TextureAnalysis System In each case, the maximum andminimum heights and widths and depths and thecomputed differences in heights, widths, and depthswere determined The results were evaluated statisti-cally and compared within and between the tworegions of the spine, using regression-correlationanalyses The heights, widths, and depths of the VBare all greater in men than in women; their behaviorduring ageing is, however, identical for both sexes.The heights of all the VB examined remain constantthroughout life after termination of growth Themaximun widths and the width differences reveal anincrease in both LVB and CVB in old age All depthparameters reveal constancy in the case of the LVBbut an increase in the case of the CVB in old age Thecorrelation coefficients of the maximum width of theVB within the spinal regions are very high in theLVB, but lower in the CVB Between the tworegions, in contrast, they are very low This behaviorsuggests a superordinate action principle within eachof the spinal regions which is based on characteristic
Offprint requests to: Prof H -J Pesch, Pathologisches Institutder Universitat Erlangen-Nurnberg, Krankenhausstra Be 8-10,D-8520 Erlangen, Federal Republic of Germany
anatomical construction and functional stressing Thestatic stressing of the LVB leads, laterally to disc pro-trusions As a result of this, traction forces acting onthe weak lateral elements of the anterior longitudinalligament, stimulate the accretion of spondyloticosteophytes at the point of insertion of the ligamenton the vertebral body Anteriorly, in contrast, theparticular strong anterior longitudinal ligament pre-vents such a remodelling process Posteriorly, thelongitudinal ligament is attached to the intervertebraldiscs, and can thus not stimulate the vertebral bodyto produce osteophytes The dynamic stressing of theCVB leads laterally to friction between the VB in theregion of the uncovertebral joints and to the forma-tion of arthrotic osteophytes Anteriorly, owing to theweak configuration of the anterior longitudinal liga-ment in this aspect, disc protrusion occur and, sub-sequently, spondylotic osteophytes accrete Poste-riorly, the (posterior) longitudinal ligament is alsoattached to the intervertebral discs, and can thus pro-vide no ossification stimulus Lateral arthrotic andanterior spondylotic osteophytes at the CVB are thusthe result of etiopathogenetically different processes,and can occur independently of each other The alsodiffering etiopathogenesis of lateral osteophytes inthe case of the LVB and CVB, presenting as spondy-losis or arthrosis, also finds statistical expression in avery small correlation of the maximum widths of theVB in both regions of the spine Spondylotic osteo-phytes occurring laterally at the LVB and anteriorlyat the CVB do not of themselves cause clinical symp-toms These are rather a sequela of motion segmentinstability, where overloading of the supportingstructures can give rise to a local chronic spinal syn-drome Arthrotic osteophytes occurring laterally onthe CVB, in contrast, can, as a result of the pressure

H.-J Pesch et al : Pathogenesis of Spondylosis Deformans and Arthrosis Uncovertebralis
they exert on nerves and blood vessels, themselvesgive rise to clinical symptoms with radiating pain andneurovegetative phenomena, known as chronic cervi-cal syndrome, in distant organs Contrasting withthese chronic, bone-associated spinal syndromes ofold age, are the acute soft-tissue-associated spinalsyndromes with radicular symptomatology, seen inyounger patients These arise through intervertebraldisc prolapse with root entrapment, by reason of theparticular anatomical and functional situation, pre-dominantly in the lower LS In addition to the newformation of bone seen in spondylosis and arthrosis,within the framework of osteoporosis with ageing, abreakdown of cancellous structure, which is said tobe due to osteoblast insufficiency, occurs simultane-ously This apparent contradiction of simultaneousnew formation and breakdown of bone resolves it-self, however, when one considers the reactive plas-ticity of bone tissue This implies that both processesare the result of the self-regulating adaptation of con-nective and supporting tissue to mechanical stresses.
Zusammenfassung Zur Atiopathogenese des ge-hauften, jedoch unterschiedlich hiufigen Auftretensklinischer Beschwerden im Bereich der unteren LWSund HWS in Form akuter bzw chronischer WS-Syn-drome wurden bei 105 Verstorbenen beiderlei Ge-schlechts im Alter von 16 bis 91 Jahren nach Aus-schlu 13 klinisch manifester Knochenerkrankungendie Abmessungen des 3 -5 Lendenwirbelk 6 rpers(LWK) und des 5 -7 Halswirbelk 6 rpers (HWK) infrontaler bzw sagittaler Ebene in Abhaingigkeit vonGeschlecht und Lebensalter quantitativ-morpho-metrisch untersucht Die Auswertung erfolgte anRontgenbildern 100 ~t dicker Knochengro 13 flichen-schliffe mit Hilfe der Makroeinrichtung des Leitz-Textur-Analyse-Systems Dabei wurden die jeweilsgr 6 f 3 te und kleinste Hohe und Breite bzw Tiefesowie die daraus berechneten Differenzen derHohen, Breiten bzw Tiefen ermittelt Die Ergeb-nisse wurden statistisch ausgewertet und durchRegressions-Korrelations-Analysen innerhalb undzwischen den beiden Regionen der LWS und HWSuntersucht Hohe, Breite und Tiefe der WK sind beiden Mannern durchwegs gr 6 Ber als bei den Frauen;ihr Verhalten im Alter ist jedoch bei beiden Ge-schlechtern gleich Die Hohen aller untersuchtenWK sind nach Abschlu 1 des Wachstums lebenslangkonstant Die maximale Breite und die Differenz derBreiten weisen bei den Lenden und Halswirbelk 6 r-pern eine Zunahme im Alter auf Samtliche Para-meter der Tiefe zeigen beim Lendenwirbelk 6 rpereine Konstanz, beim Halswirbelk 6 rper dagegen eineZunahme im Alter Die Korrelationskoeffizientender maximalen Breite der WK sind innerhalb der
WS-Regionen in der LWS sehr hoch, in der HWSniedriger, zwischen beiden WS-Regionen dagegensehr niedrig Dieses Verhalten spricht fiir ein jeweilsiibergeordnetes Wirkungsprinzip innerhalb der WS-Regionen, das auf gleicher anatomischer Konstruk-tion und funktioneller Beanspruchung beruht Diestatistische Beanspruchung der LWS fihrt lateral zuBandscheibenprotrusionen Diese rufen fiber Zer-rung des dort schwicheren vorderen Lingsbandes andessen Insertionsstelle am Wirbelkorper den Anbauspondylotischer Knochenzacken hervor Ventraldagegen verhindert das besonders straffe vordereL Ungsband diesen Umbau Dorsal inseriert dasLingsband an den Bandscheiben und kann so keinenReiz zur Ossifikation auf den WK ausiiben Diedynamische Beanspruchung der HWS fhrt lateralzum Aufeinanderreiben der WK im Bereich der Un-covertebralgelenke und zum Anbau arthrotischerKnochenzacken Ventral kommt es wegen des hiernur schwach ausgebildeten vorderen Langsbandes zuBandscheibenprotrusionen und daraufhin ebenfallszum Anbau spondylotischer Randzacken Dorsalinseriert auch hier das Langsband an den Bandschei-ben und kann somit keinen Reiz zur Ossifikation aufden WK ausfiben Laterale und ventrale spondylo-tische Knochenzacken am HWK sind somit Ergebnisatiopathogenetisch verschiedener Prozesse und k 6 n-nen unabhaingig voneinander auftreten Die ebenfallsunterschiedliche Atiopathogenese lateraler Knochen-zacken an LWK und HWK als Spondylose bzw.Arthrose findet auch statistisch ihren Ausdruck ineiner sehr geringen Korrelation der maximalen Brei-ten der WK in beiden WS-Regionen SpondylotischeRandzacken lateral am LWK und ventral am HWKrufen selbst keine klinischen Beschwerden hervor.Diese sind vielmehr Folge der Insuffizienz im Be-wegungssegment, wobei durch die Oberbeanspru-chung der Haltestrukturen lokalisierte chronischeWS-Syndrome auftreten k 6 nnen Arthrotische Rand-zacken lateral am HWK k 6 nnen dagegen selbst durchNerven und Gefa Blkompression klinische Beschwer-den mit ausstrahlenden Schmerzen und neurovege-tativen Erscheinungen als chronische HWS-Syn-drome in entfernt liegenden Organen hervorrufen.Im Gegensatz zu diesen chronischen, knochenassozi-ierten, WS-Syndromen des hheren Alters stehendie akuten, weichteilassoziierten WS-Syndrome mitradikulirer Symptomatik des jfingeren Alters Sieentstehen durch Bandscheibenprolapse mit Wurzel-einklemmung aufgrund der besonderen anatomi-schen und funktionellen Situation vorwiegend in derunteren LWS Neben dem durch Spondylose undArthrose bedingten Knochenanbau kommt es gleich-zeitig im Rahmen der physiologischen Altersosteo-porose zum Abbau spongi 6 ser Strukturen, der auf
202

H.-J Pesch et al : Pathogenesis of Spondylosis Deformans and Arthrosis Uncovertebralis
der sogenannten Osteoblasteninsuffizienz beruhensoll Dieser scheinbare Widerspruch des gleichzeiti-gen An und Abbaus von Knochen 16st sich jedochunter Beriicksichtigung der reaktiven Plastizitit desKnochengewebes Danach sind beide VorgiingeErgebnis der selbstgesteuerten Anpassung vonBinde und Stiitzgewebe an mechanische Beanspru-chungen.
Intervertebral-disc-related symptoms affecting thelumbar spine (LS) and the cervical spine (CS) moreand more frequently induce patients of varying agesto seek the aid of an orthopedic specialist X-rayfilms obtained from such patients often reveal a nar-rowing of the disc space, sclerosis of the end platesand/or lipping at the edges of the vertebral bodies(VB) (marginal osteophytes) In the LS such changesare always referred to as spondylosis deformans, inthe CS sometimes as arthrosis uncovertebralis.
The clinical and radiological experience of suchconditions already indicate that these two entitiesmust represent two pathogenetically different bonelesions.
Thus, for example, LS symptoms occur earlierand more frequently, and are more uniform innature, while CS symptoms have a later onset, areless frequent, and are more multifarious (Kramer1978) Laterally in the lumbar vertebral body (LVB),and anteriorly in the cervical vertebral body (CVB),submarginal osteophytes are found, while laterally inthe CVB, osteophytes are uncovertebral in location(Idelberger 1975).
Today, it is possible to subject a large number ofhuman cadaver VB to structural and form analyses.The aim of such investigations is to draw conclusionsas to the origin of the radiological changes seen in theVB, and thus of the symptomatology they cause.
For this purpose, the three lowest LVB and thethree lowest CVB were analysed morphometricallyas a function of sex and age, and the results evaluatedstatistically.
Table 1 Age and sex distribution of the 105 cases investigated
Age lyearsl Sex (n)& Z
16-40 13 7 2041-50 10 9 1951-60 12 5 1761-70 11 8 1971-80 7 12 1981-91 6 5 11
YZ 59 46 105
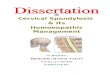
Fig la, b Schematic representation of the investigated frontaland sagittal vertebral body sections (magnification x 0 51) ofthe a LVB, b CVB
Fig 2 a,b Monitor picture of X-ray views of 100-lgm-thickpolished bone sections taken from the fifth CVB of a 49-year-old man (magnification approx x 1 93) with a smallest outerand b largest inner rectangular "mask"
Material and Methods
In 105 autopsy cases of both sexes, aged between 16 and91 years (Table 1) with no evidence of clinically manifest bonedisease, the dimensions of the third to fifth LVB, and of thefifth to seventh CVB were studied From the middle of thethird and fifth LVB and of the fifth and seventh CVB, 3-5-mm-thick slices were sawn out parallel to the frontal plane,and out of the middle of the fourth LVB and the sixth CVB,3-5-mm-thick slices were sawn out parallel to the sagittal plane(Fig i 1), and after fixation in Schaffer's solution, embedded inmethyl methacrylate From these blocks, 100-gm-thick polish-ed bone sections' were prepared on Plexiglas slides 2, and high-contrast X-ray pictures obtained 3 (further methodologicaldetails can be found in Pesch et al 1975, 1977 ; Henschke andPesch 1978) With the aid of the Leitz Texture AnalysisSystem 4 (Serra 1973), these polished sections were transmitted
1 Cutting machine Woco p 50, Conrad, Clausthal-Zellerfeldand precision polishing machine, Miller, Nuremberg, FRG
2 Plexiglas slides, Rohm, Darmstadt, FRGCyanoacrylate adhesive, Delo, Munich, FRG
3 Fully enclosed table X-ray unit, Faxitron, Priizisionstechnik,Cologne, now Hewlett and Packard, B 6 blingen, FRG
4 TAS, Leitz, Wetzlar, FRG
203

H.-J Pesch et al : Pathogenesis of Spondylosis Deformans and Arthrosis Uncovertebralis
to a monitor screen via a black-and-white television camera fora quantitative analysis of the form of the VB.
In the VB sectioned in the frontal plane, the maximum(outside) height Hmax and width Wma, and the minimum(inside) height Hmin and width Wjinwere determined with theaid of the smallest rectangular "mask" that could be placedoutside the VB to include the cortical bone, and the largestrectangular "mask" that could be placed inside the VB toexclude the cortical bone Likewise, in the VB section in thesagittal plane, the maximum (outside) height Hmax and depthDma,,, and the minimum (inside) height Hmin and depth Dmin,
were determined in the same way (Figs 6 and 7) Hereby, themaximum width of CVB 5 and 7 was selected to be the distancebetween the extreme tips of the uncinate processes, since thelateral transition of the VB into the costal process did not per-mit an accurate delimitation (Fig 2 a, b).
From the maximum and minimum heights, widths anddepths, the magnitudes AH = Hm Hmin, AW = Wmax -Wmi, and AD = Dma Din were computed as a measure ofthe deviation of the VB from the rectangular form To investi-gate possible sex or age-dependency, variance analyses werecarried out at a significance level of a = 5 % Taking into
Table 2 Mean values and standard deviations of the mean for maximum and minimum heights, and the differences in heights andmaximum and minimum widths, and the differences in widths of the (a) 3rd LVB, (b) 5th LVB, (d) 5th CVB, (e) 7th CVB, andmaximum and minimum depths, and the differences in depths of the (c) 4th LVB and (f) 6th CVB as a function of age
Age No of Heights Widths or depths
(years) cases Maximum Minimum Differences Maximum Minimum Differences(n) lmml S lmml S lmml S lmml S lmml S lmml s
20 29 8519 28 4617 30 0819 29 2119 28 8911 28 82
20 32 0319 29 3917 30 0619 30 3419 30 8411 30 70
20 30 9519 29 6217 31 2319 30 1619 30 4111 30 23
20 16 6619 16 8817 17 3719 17 3019 16 6011 17 07
20 18 6719 17 9217 18 8619 18 2619 17 5111 18 17
20 16 4219 14 1917 14 5719 14 2319 13 9011 14 15
0.310.390.420.410.520.45
1.170.310.670.450.640.73
0.420.360.320.390.390.31
0.400.350.510.410.420.61
0.420.500.450.390.520.56
0.290.300.280.260.280.35
23.71 0 3522.68 0 3423.11 0 5922.40 0 3921.72 0 6321.96 O 78
23.6422.7421.8422.4322.8322.71
23.1722.2924.0721.7021.7022.63
10.359.79
10.1310.049.609.98
11.0110.0910.5210.389.88
10.24
10.139.559.859.489.109.28
0.450.540.940.410.550.85
0.410.401.190.450.600.37
0.240.260.430.310.210.40
0.350.350.280.280.290.36
0.260.260.320.310.230.27
6.14 0 305.78 0 226.98 0 506.81 0 447.17 0 406.86 0 61
8.386.658.227.928.017.99
7.787.337.158.468.717.60
6.317.097.247.267.007.09
7.667.827.937.887.627.92
4.494.644.724.754.824.78
1.260.380.510.590.610.75
0.400.391.170.310.430.26
0.300.250.420.330.340.40
0.430.360.370.290.420.52
0.190.130.130.210.200.25
51.21 1 2350.36 0 8753.55 1 4454.5455.1353.88
53.5352.4757.7657.5658.4458.94
37.1836.1638.0837.4137.6637.62
21.6321.3923.0322.7821.9123.18
25.2924.0725.9724.7425.6828.28
17.1717.9019.5619.7119.5420.53
1.281.561.29
1.131.131.321.471.821.76
0.900.721.110.751.000.93
0.690.470.520.620.360.71
0.540.530.650.530.781.16
0.260.300.540.670.600.78
38.2536.8839.2037.7537.5337.70
41.5736.9343.2640.1938.8241.07
29.9428.0630.9528.8628.8629.62
16.9116.1416.8516.8815.8216.85
21.7420.5620.9419.9821.1823.61
12.1311.9013.1012.7613.2514.10
1.130.791.070.860.880.94
1.811.231.040.981.001.00
0.790.720.930.590.690.95
0.480.390.490.520.360.71
0.800.750.810.730.881.08
0.310.360.330.290.380.55
12.9513.4914.3516.7917.5916.19
11.9615.5414.5017.3719.6217.87
7.248.107.148.558.807.99
4.715.256.185.906.086.32
3.553.504.924.754.494.67
5.036.006.456.956.286.44
0.410.440.850.731.131.19
1.561.150.841.151.461.21
0.400.500.570.400.620.40
0.560.460.480.650.430.82
0.480.440.520.570.520.76
0.230.360.430.590.450.35
a) 16-4041-5051-6061-7071-8081-91
b) 16-4041-5051-6061-7071-8081-91
c) 16-4041-5051-6061-7071-8081-91
d) 16-4041-5051-6061-7071-8081-91
e) 16-4041-5051-6061-7071-8081-91
f) 16-4041-5051-6061-7071-8081-91
204

H.-J Pesch et al : Pathogenesis of Spondylosis Deformans and Arthrosis Uncovertebralis
account adequate group size and biological ageing, six age-groups were formed, and the mean values and standard devia-tions of these values computed for all the parameters Finally,with the aid of regression-correlation analyses, the relationshipof the measured parameters of the individual VB within andbetween the two regions of LS and CS were investigated.
All computations were carried out with the aid of the sta-tistic programme package SPSS (Beutel et al 1978) on theSiemens 7,541 computer system at the Computer Center of theMedical Department of the University Hospital, Erlangen.
Results
Firstly, the mean values of the parameters weredetermined, irrespective of age, for each sex sepa-rately.
The maximum and minimum heights of all VB,the maximum and minimum widths of the frontallysectioned LVB 3 and 5 and CVB 7, and the maxi-mum and minimum depths of the sagittally sectionedLVB 4 and CVB 6, differ between the sexes In con-trast, the differences in heights, widths, and depths ofall VB, and the maximum and minimum widths ofCVB 5, show no dependency on sex.
Height 3 LVBlmml
Hmax
20
10 H
Width 5 LVB
Depth 4 LVBlmml Dmx
50 i:i
160-40 4150 5 I-60 6 I-70 7 I-80 81 Age
Fig 3 Mean values and standard deviations of the means formaximum and minimum heights (Hma, and Hmin), widths (Wmaxand Wmin), and depths (Dma, and Dmi) and their differences
(A) of the three investigated LVB as a function of age
The maximum and minimum heights of the VBinvestigated are greater in men, both in the LS and inthe CS, than in women by an average of 1 2 mm,while the maximum and minimum widths and depthsare greater in men than in women by 3 mm in the LSand by 1 mm in the CS.
Finally, the mean values of the parameters as afunction of age were again determined separately foreach sex.
Corresponding parameters in the two sexes show-ed the same behavior with respect to the significanceof their age-related changes For this reason, for fur-ther evaluation, male and female data were pooledand investigated in six age-groups (Table 1).
The maximum heights (Table 2, Figs 3 and 4) ofall the VB show no significant changes in old age Inthe case of the LVB, the heights are, at 30 mm,approximately identical, whereas at 17 0 mm forCVB 5, 14 3 mm for CVB 6, and 18 2 mm for CVB 7they differ among the CVB.
The minimum heights of all VB also show no agedependency In the LVB they are equal at 22 6 mm,while in the CVB they differ appreciably, being 10 0
Height'lmml
15-
10-
5-
5.CVBH _.
Width 7 CVBlmml
25-
20-
15-
Fig 4 Mean values and standard deviations of the means forthe maximum and minimum heights (Hmax and Hin), widths(Wma, and Wmin), and depths (Dma and Dmin), and their differ-ences (A) of the three investigated CVB as a function of age
ra-i-_ li _ f e _ -
__ __ _ ~
205
I
'I �.�:·t
�I
s

H.-J Pesch et al : Pathogenesis of Spondylosis Deformans and Arthrosis Uncovertebralis
Table 3 Correlation coefficients of the maximum width (Wmax)of the frontally sectioned LVB and CVB
CVB 5 CVB 7 LVB 3
CVB 7 0 40LVB 3 0 33 0 21LVB 5 0 30 0 25 0 74
Wmaxlmml
60
55
50
45
a
wma,lmml
25
20
15
b
Wmaxlmml
30
25
c 20
3.LVB r= 074
5 LVB45 50 55 60 65 Wmax lmml
5.CV 1 ·r= O 4
//:
7 CVB20 25 3 Wmax lm ml
57.CVB r= 0, 27 CVB 'r,-021 ·
45 50 55 60 Wmax lmml
Fig 5 a-c Correlation diagrams for maximum width (Wmax) ofthe a LVB 3 and 5 (r = 0 74), b CVB 5 and 7 (r = 0 40), c CVB7 and LVB 3 (r = 0 21)
mm for CVB 5, 9 6 mm for CVB 6, and 10 4 mm forCVB 7.
In both regions of the spine, the height differencesalso reveal no dependency on age, and, at about7.4 mm, are similar in the LVB, whereas they differamong the CVB, being 7 0 mm for CVB 5, 4 7 mmfor CVB 6, and 7 8 mm for CVB 7.
The maximum width (Table 2, Figs 3 and 4) ofthe four frontally sectioned VB increases differentlywith age A significant increase of 5 % is found inLVB 3 from 51 5 mm, of 10 % in LVB 5 from 53 5mm, and of 12 % in CVB 7 from 23 3 mm Althoughno significant changes were demonstrable in CVB 5,the maximum width increased by 7 % from 21 6 mm.
The minimum widths of these four VB differ fromone another, and usually show no change with age.The figures are 37 9 mm for LVB 3, 40 2 mm forLVB 5, and 16 6 mm for CVB 5 An increase is alsoseen in CVB 7 of 8 % from 21 7 mm, but this is notsignificant.
The differences in the widths increase with age inboth regions of the spine This increase is significantfor LVB 3, namely 25 % from 13 0 mm, and forLVB 5, which increases by 50 % from 12 0 mm, buton account of marked variance of the measuredvalues, is not significant for CVB 5, which shows anincrease of 33 % from 4 7 mm, or in CVB 7, whichincreases by 32 % from 3 5 mm.
The maximum and minimum depths, and also thedifference between the depths in the two sagittallysectioned VB (Table 2, Figs 3 and 4) show a differentpattern of behavior with ageing No difference isfound for LVB 4 at 37 2 mm and 29 4 mm, for maxi-mum and minimum depth respectively, or for theirdifference.
In contrast, in CVB 6, there is a significant age-related increase in maximum depth by 20 % from 17 2mm, of 14 % in minimum depth from 12 2 mm, and of28 % in the difference in depths from 5 0 mm.
Correlation coefficients and regression lines de-scribe same-sense relationships between height,width, and depth among the three LVB and thethree CVB It appears that the relationship of theLVB to one another (Table 3, Fig 5 a) is markedlyclose than that of the CVB to one another (Table 3,Fig 5 b) In contrast, there is hardly any relationshipbetween the VB of these two regions of the spine(Table 3, Fig 5 c).
These differences between LVB and CVB areseen to be particularly marked in form-analytical X-ray images of the two regions of the spine in youngand advanced age (Figs 6 and 7) Owing to the age-dependent increase in maximum width, and the dif-ference in widths of the LVB (Fig 6), in this region,marginal osteophytes associated with the upper and
. H _
I/ 3 LVB
F / * ~~~ 3 LVB'
l I/
206

H.-J Pesch et al : Pathogenesis of Spondylosis Deformans and Arthrosis Uncovertebralis
< __ _-Wmax 11Wmin
Dmax | Dmin
Fig 6 a-d Form-analytical X-ray picturesof 100-gm-thick polished bone sections ofthe frontally sectioned fifth LVB (left)with maximum and minimum heights(Hmax and Hmin) and widths (Wax andWmin) and of the sagittally sectionedfourth LVB (right) showing maximumand minimum heights (Hmax and Hmi,)and depths (Dmax and Din) a and c of a39-year-old man, b and d of a 76-year-oldman (magnification approx x 0 94)
1 Wmax-1I I-Wmin I
H
,Dmax 1I Dmin f 1
max
HmirHmax
714
Hmax
Hmax
HmirL-
| m i in rmin
I a a , Dmax
Fig 7 a-d Form-analytical X-ray pictures of 100-jim-thickpolished bone sections of the frontally sectioned seventh CVB(left) showing maximum and minimum heights (H,ma and Hmin)and widths (Wmx and Wmin) and of the sagittally sectioned sixthCVB (right) showing maximum and minimum heights (Hm,,and Hmin) and depths (Dm, and Dmin) a and c of a 49-year-oldwoman, b and d of a 91-year-old man (magnification x 0 86)
lower plates are seen only laterally (Fig 6 a and b);anteriorly, owing to the age-constant depth, they arelacking (Fig 6 c and d) In contrast, in the case of theCVB (Fig 7), as a result of the slight increase inwidth and of the difference in widths in old age, onlyslight "lipping" of the uncinate process or slight for-mation of marginal osteophytes are seen laterally(Fig 7 a and b), while anteriorly, as a result of anincrease in the maximum and minimum depths and oftheir difference, a beak-like remodeling of the verte-bral body margin has occurred (Fig 7 c and d).
Discussion
The fact that the maximum and minimum heights ofall VB examined were greater by 1 2 mm in men than
in women is explainable by the fact that men are, onaverage, taller The resulting 3 cm greater length ofthe bony vertebral column (VC) in men is associatedwith a widening of the VB in the lower LS by about3 mm, but only of about 1 mm in the lower CS Atechnical equivalent of this situation would be a fac-tory chimney which is broader at the base.
Although the VC is described anatomically as aunit, there are considerable morphological and func-tional differences between the LS and the CS.
The LVB are largely constant in form With theexception of the maximum width and the differencebetween widths in old age, the other parameters,such as maximum and minimum height and their dif-ference, show no age-related changes This result isin agreement with the VC index described by Barnettand Nordin ( 1960), which also reveals no significantdependence on age, and is also in accordance withearlier investigations (Pesch et al 1980 b).
The equal-sense behavior of the form parametersof LVB 3 and 5 points to a mechanism of action inthis region of the spine that remains constant through-out life.
On the basis of the anatomical construction of theLS, the range of movement between the individualLVB is restricted in all directions by the strong liga-ments, the powerful supporting muscles, and thesagittally oriented vertebral joints In particular, norotational movements are possible between the LVB(Lippert 1966 ; Gregerson and Lucas 1967 ; Tittel1974 ; Wood 1979) This means that the LVB are sub-jected mainly to static forces, the force being trans-mitted through the elastic intervertebral disc in theform of pressure acting over the surface area of thetwo end plates (Pesch et al 1980 b).
-4-7
1mrHminHmax
_I
Hmin
Hmax
L -Dmin n
207
-~~"~ -rnu-I I I Ll UX

H.-J Pesch et al : Pathogenesis of Spondylosis Deformans and Arthrosis Uncovertebralis
The always greater maximum and minimumwidths of LVB 5 as compared with LVB 3 seen aftertermination of growth can be traced back to theincreasing loading of the VC in the craniocaudaldirection (Braus 1921 ; Benninghoff 1954 ; Schmorland Junghanns 1968) As a result of the simultaneousenlargement of the area of the upper end plate andincrease in the volume of the VB, an enlargement ofthe cross-section of the bearing cancellous boneoccurs, so that no increase in the loading of the indi-vidual bony trabeculae takes place (Kummer 1962 ;Pesch et al 1980 b).
As a result of the lateral waist-like concavities ofthe VB, differences in maximum and minimumwidths occur on termination of growth These conca-vities in the lateral aspects, are statically highly favor-able forms that can also be found in technical con-structions (e g , dams) Taking into account thecourse of the transverse force (Schliter 1965) and ofthe fracture behavior known from pressure experi-ments in material-testing laboratories (Sigwart 1974),the form of the LVB may be compared to apposedcones of pressure Accordingly, the material "remov-ed" by the central concavities corresponds to thatpart of the body which, subjected to critical compres-sive force, would be the first to rupture outward Theincrease in the difference in widths that can be seenwith advancing age is due to a continuous increase inmaximum width, associated with a constant mini-mum width (Pesch et al 1980 b) This "submarginal"(Idelberger 1975) accretion of bone in the form ofosteophytes or thickenings close to the upper andlower end plates is pathognomonic for spondylosisdeformans It occurs against the background ofunderlying insufficiency in the motion segment(Schmorl and Junghanns 1968), the localization ofthe osteophytes being determined by the anatomicalconstruction.
In the LS, the anterior longitudinal ligament isparticularly strong and thick in the anteromedialaspect, while laterally it comprises weaker and thin-ner fibers (Johnson et al 1975 ; Worsdorfer andMagerl 1980) Degenerative fissures in the annulusfibrosus of the intervertebral disc lead to protrusionof the disc at the "locus minoris resistentiae", whilethe "explosive potential" of the gelatinous nucleus ismaintained The point of least resistance is locatedlaterally where the components of the anterior longi-tudinal ligament are relatively weak As a result,instability of the motion segment occurs (Schmorland Junghanns 1968), and intermittent tractionforces act on the points of insertion of the lateralfibers of the longitudinal ligament As a result of this,owing to the increase in stretching stresses, ossifica-tion is initiated (Pauwels 1965) This bone formation
can lead to the production of spurs, marginal thicken-ings, and even bars that can develop to the extent ofproducing bone ankylosis between neighboring VB.Anteriorly, medially, the strong anterior longitudi-nal ligament prevents such a remodeling process.Posteriorly, the (posterior) longitudinal ligament isattached only to the intervertebral discs (Johnson etal 1975), and thus cannot act on the VB to provide astimulus for ossification This is the reason why, inagreement with earlier investigations (Nathan 1962),consistency of form is found in the sagittal sectionedLVB 4, even in advanced age.
The CVB have a characteristic appearance Theytherefore differ among themselves, and also frontallyand sagittally, more markedly than do the LVB.Owing to the median sectioning plane, the uncinateprocesses are not involved, so that compared with thefrontal section, sagittal measurements reveal a muchlower maximum height.
As in the case of the LVB, greater maximumand minimum widths and also heights are found inCVB 7 than in CVB 5, being the expression of theincreasing loading of the VC in the craniocaudaldirection The same-sense behavior of the form para-meters of these two VB in old age also points to auniform action mechanism in the lower CS through-out life Owing to the complicated anatomical con-struction of the CS, the transmission of forces be-tween the individual CVB is not in the vertical direc-tion, so characteristic of all LVB, but varies in thethree functionally different sections of the CS Thus,in the lower CS (CVB 5-7), in addition to anteriorand posterior flexion and lateral bending, torsionalmovements also occur In the upper CS (CVB 1 and2) at the atlanto-occipital joint, in contrast, mainlyrotational and anterior or posterior movementsoccur, while in the middle CS (CVB 3 and 4) mainlyposterior, to a lesser extent also anterior, flexion andlateral bending occur.
Thus, the three lower CVB are stressed largelydynamically The range of movement and the stress-ing of the intervertebral discs achieve their maximafor anterior and posterior flexion (Bowden 1966 ;White and Panjabi 1978 ; ten Have 1978 ; Isaacson1979 ; W 6 rsdorfer and Magerl 1980).
Torsional movements are readily possible owingto the upward inclination of the articular facets of theapophyseal joints In flexion-extension movements,the shovel-like uncinate processes are involved,which, in about the 9th year of life, develop upwardsfrom elements of the VB, as a result of which, in con-junction with a simultaneous curvature in the sagittaldirection, they give the upper end plate a saddle-likeshape.
208

H.-J Pesch et al : Pathogenesis of Spondylosis Deformans and Arthrosis Uncovertebralis
During the "erection" of the uncinate processes,horizontal fissures can develop in the intervertebraldiscs, in the lateral uncovertebral region (Ecklin1960 ; T 6ndury 1974); however, these must be consid-ered physiological Through synovial lining and in-sprouting of lateral menisci, these gaps secondarilydevelop an articular configuration (Ecklin 1960 ; T 6 n-dury 1974 ; Stahl and Huth 1980).
This anatomical structure of the CVB, which iscomplicated as compared with LVB, in conjunctionwith the functionally more multifarious dynamicstressing, leads to more complex changes of form inold age.
The increase in maximum width and the differ-ence in widths observed in CVB 5 and 7 correspondto a greater distance between the tips of the uncinateprocesses in the aged, which is caused by a lateral"bending" of the processes, or lateral accretion ofosteophytes These lateral uncovertebral osteophytesare pathognomonic for arthrosis uncovertebralis andin the CS are most frequently found in the threelower CVB (Krogdahl and Torgersen 1940 ; Epp1950 ; Exner 1954 ; Nathan 1962 ; Friedenberg andMiller 1963 ; Sager 1969) Since it is here that therange of movement is greatest, the most markedsigns of wear of the intervertebral discs also occurhere (Friedenberg et al 1959 ; Payne and Spillane1957 ; W 6 rsdorfer and Magerl 1980) These lead to anarrowing of the intervertebral space, to contact ofthe neighboring VB, with reactive sclerosis of theupper end plate, and to lateral "bending" of the un-cinate process (Giraudi 1931 ; Krogdahl and Torger-sen 1940 ; Lyon 1945 ; Frykholm 1951 ; Exner 1954 ;Friedenberg and Miller 1963 ; Hirsch et al 1967 ;Schmorl and Junghanns 1968), with the result that inthe extreme case, the CS presents a pot or plate-likeappearance in the a p X-ray film (Ecklin 1960) As aresult of these pathological anatomical changes in theregion of the uncovertebral joints, arthrotic osteo-phytes are then accreted laterally.
In the sagittally sectioned CVB 6, the maximumand minimum depths and their differences increasewith age At the anterior aspect, accretion of osteo-phytes occurs close to the end plates, to producebeak-like projections which must be consideredmorphological variants of spondylosis deformans.Since in the CS the anterior longitudinal ligamentis weakly developed (Johnson et al 1975), antero-medially, disc protrusion, and thus the developmentof osteophytes, can occur Posteriorly, as in the caseof the LS, the longitudinal ligament is attached onlyto the intervertebral discs, and thus cannot induceossification in the VB Therefore, lateral arthroticand anterior spondylotic osteophytes in the CVB can,in consequence of etiopathogenetically different pro-
cesses, occur independently of one another (Giraudi1931 ; Krogdahl and Torgersen 1940 ; Lyon 1945 ;Frykholm 1951 ; Schmorl and Junghanns 1968).
The likewise differing etiopathogenesis of lateralosteophytes at the LVB and CVB, in the form ofspondylosis deformans and arthrosis uncovertebralisrespectively, finds static expression, too, in the factthat the maximum width of the VB in the two regionsof the spine correlate only slightly with each other.The contrasting high correlation of the maximumwidths among the LVB suggests that lateral spondy-losis frequently occurs simultaneously at several VB,while the lower correlation of this parameter amongthe CVB indicates that lateral arthrosis uncoverte-bralis occurs isolated in individual VB.
Spondylosis deformans is the formation in the VBof end plate proximal osteophytes, due to an underly-ing degenerative disc injury with consecutive insuffi-ciency in the motion segment It occurs very com-monly with increasing age in all regions of the VC,but predominantly in the LS The extent and localiza-tion of the bone changes are determined individuallyby the anatomical situation presenting and by thefunctional stressing In the case of the LS, predomi-nantly static loading leads to lateral disc protrusions,which, anteriorly, are prevented by the in this aspectstrong anterior longitudinal ligament In the CS, incontrast, mainly dynamic stressing leads to anteriorprotrusions, since here the longitudinal ligament ismuch more weakly structured Any disc protrusionand insufficiency of the motion segment lead to trac-tion on the longitudinal ligament and thus induceossification in the form of spondylotic marginalosteophytes.
Clinically, during these remodeling processes, thespectrum of symptoms ranges from relative freedom,to severe localized chronic manifestations Thechronic spinal syndromes are not caused by the osteo-phytes themselves, but rather by the insufficiency ofthe motion segment and the associated overloadingof the ligamentous and muscular supporting struc-tures of the spine (Idelberger 1975 ; Rizzi 1976 ; Kra-mer 1978 ; Wood 1979) With further progress of thespondylosis to ankylosing bar formations and stiffen-ing of the motion segment, these symptoms candisappear spontaneously at the cost of limitation ofmobility.
Arthrosis uncovertebralis is the formation of later-al arthrotic osteophytes at the uncovertebral process,which develop as a late sequela of disc degenerationwith narrowing of the intervertebral spaces andwhich, on account of the high dynamic loading, occurpreferentially in the lower CS The condition occurswith increasing age, and is restricted to the CS Here,symptoms may be caused by the osteophytes them-
209

H.-J Pesch et al : Pathogenesis of Spondylosis Deformans and Arthrosis Uncovertebralis
selves Clinically, on account of the intimate anatom-ical relationship of the uncovertebral region to thespinal nerves, blood vessels, and the cervical sympa-thetic trunk, these symptoms comprise radiated pain,blood flow disturbances, and neurovegetative phe-nomena in distinct organs (Krogdahl and Torgersen1940 ; Friedenberg et al 1959 ; Bowden 1966 ; Pen-ning 1978 ; Stahl 1977 ; Kramer 1978 ; Wood 1979) Inconsequence of the bone changes, the chronic CSsyndromes only occur in middle to old age, with apeak in the 4th-6th decades (Krimer 1978).
In contrast to the bone-associated chronic symp-toms caused by spondylosis or arthrosis, the acutevertebral syndromes with radicular character andrelatively uniform symptomatology, are based onsoft-tissue changes that take the form of disc pro-lapse They occur, on average, 10 years earlier thanthe chronic CS syndromes (Kramer 1978), and morethan 90 % are located in the two lowermost motionsegments, L 4/L 5 and L 5/51 (Idelberger 1975) Here,the high and constant stressing by compressive forcesin the region of transition between the lumbar lordo-sis and the fixed sacral kyphosis, in conjunction withmaximum loading through anteroposterior flexion,may cause disc diseases at a young age.
Prolapse of the two lower intervertebral discsmost frequently lead to clinically manifested sciati-form symptoms Both in monoradicular and biradicu-lar entrapment, owing to the anatomical situation,these symptoms are relatively uniform, since, on theone hand, the discs and intervertebral foramina arelocated at the same level, while on the other, the dia-meter of the intervertebral foramen vis-a-vis that ofthe nerve root becomes relatively smaller in the cau-dal direction On the basis of their anatomical con-struction and their high static and dynamic stressingrespectively, the lower LS and the lower CS are "pre-destined" to develop acute and chronic diseases.
In the thoracic spine, in contrast, clinically rele-vant acute or chronic symptoms are virtually neverseen, since on the one hand, owing to the position ofthe intervertebral foramen on the level of the VB,the intimate spatial relationship of disc and nerveroots is lacking, while on the other, on the basis ofthe functional-anatomical integration, extreme staticand dynamic stresses usually do not occur in the tho-rax.
The changes in external form of the VB due tospondylosis and arthrosis are brought about by boneaccretion At the same time, however, changes in theinternal structure also occur, in the sense of physio-logical age-related osteoporosis This breakdown ofbone is commonly (Albright et al 1940 ; Bartelhei-mer and Schmitt-Rohde 1956 ; Frost 1963 ; Eger et al.1967 ; Schenk et al 1969 ; Schenk and Merz 1969 ;Delling 1973, 1974 ; Tanaka 1974 ; Jesserer 1975,
1978) ascribed to an age-related diminishment inosteoblast activity-so-called osteoblast insufficiency.The apparent contradiction between simultaneousnew formation and breakdown of bone resolves,however, when one considers the reactive plasticityof bone tissue (Pliess 1969), which adapts itself to theage-related mechanical situation presenting Thus,bone accretion, in the form of spondylotic or arthrot-ic osteophytes, must be considered a local reaction tomechanical stimuli, which act on the bone tissue sub-sequent to chronic disc degeneration with instabilityof the motion segment.
Bone breakdown in old age varies locally (Lauer1980) Thus, the LVB loses more than 1/3, the CVBonly just lo O of its original bony mass (Pesch et al.1980 b,1985) Owing to the age-related reduction inthe range of movements, and in physical activity,there is but a weak "preservation stimulus" for thecancellous bone in the LS, which is stressed largelystatically by axial compressive forces In contrast,the dynamic loading of the CS, which remains largelyconstant even in old age (Buytendijk 1956), whichsubserves orientation in space, and which consists oftraction and torsional forces acting from variousdirections, provides a powerful stimulus that securesthe preservation of the cancellous trabeculae Forthis reason, a considerably smaller breakdown ofspongy bone occurs in the CVB than in the LVB inold age.
The new formation and breakdown of bone thusrepresent reactive-adaptive processes that are theresult of the self-regulating adaptation of connectiveand supporting tissue to mechanical stressing (Peschet al 1980 a, von Glass and Pesch 1983).
References
Albright F, Blommberg E, Smith RH ( 1940) Postmenopausalosteoporosis Trans Ass Am Phys 55:298
Barnett E, Nordin B ( 1960) The radiological diagnosis ofosteoporosis A new approach Clin Radiol 11:166
Bartelheimer H, Schmitt-Rohde JM ( 1956) Osteoporose alsKrankheitsgeschehen Ergeb Med Kinderheilkd NF 7:454
Benninghoff A ( 1954) Lehrbuch der Anatomie des Menschen,Bd I Urban und Schwarzenberg, Berlin Miinchen
Beutel P, Kiiffner H, R 6 ck W, Schub 6 W ( 1978) Statisticalpackage for the social sciences Fischer, Stuttgart NewYork
Bowden R ( 1966) The applied anatomy of the cervical spineand brachial plexus Proc R Soc Med 59:1147
Braus H ( 1921) Anatomie des Menschen, Bd 1 Springer, Ber-lin
Buytendijk FJJ ( 1956) Allgemeine Theorie der menschlichenHaltung und Bewegung Springer, Berlin G 6 ttingen Hei-delberg
Delling G ( 1973) Age-related bone changes Histomorpho-metric investigation of structure of human cancellousbone Curr Top Pathol 58:117
Delling G ( 1974) Altersabhangige Skeletveranderungen KlinWochenschr 52:318
210

H.-J Pesch et al : Pathogenesis of Spondylosis Deformans and Arthrosis Uncovertebralis
Ecklin U ( 1960) Die Halswirbelsiule Springer, Berlin G 6 ttin-gen Heidelberg
Eger W, Gerner HJ, Ktimmerer H ( 1967) Bau und Dichte dermenschlichen Spongiosa in Rippe, Wirbel und Becken alsAusdruck der statischen Funktion Arch Orthop UnfallChir 62:97
Epp W ( 1950) Die Spondylosis deformans der Halswirbel-saule Diss, Ziirich
Exner G ( 1954) Die Halswirbelsiule Thieme, StuttgartFrancis C ( 1956) Certain changes in the aged white cervical
spine Anat Rec 125:783Friedenberg Z, Miller ( 1963) Degenerative disc disease of the
cervical spine J Bone Joint Surg lAml 45:1171Friedenberg Z, Eideken, Spencer, Tolentino ( 1959) Degene-
rative changes in the cervical spine J Bone Joint SurglAml 41:61
Frost HM ( 1963) Bone remodelling dynamics Thomas,Springfield (I 11)
Frykholm R ( 1951) Lower cervical vertebrae and interverte-bral discs Surgical anatomy and pathology Acta ChirScand 101:345
Giraudi G ( 1931) L'artrosi deformante uncovertebrale RadiolMed, Torino
von Glass W, Pesch H-J ( 1983) Zum Ossifikationsprinzip desKehlkopfskelets von Mensch und Siugetieren Acta Anat116:153
Gregerson GG, Lucas DB ( 1967) An in-vivo study of the axialrotation of the human thoracolumbar spine J Bone JointSurg lAml 49:247
ten Have H ( 1978) Voor-achterwaartse Beweeglijkheid enAfwijkingen van de Halswervelkolom Diss, Leiden
Henschke F, Pesch H-J ( 1978) Kunststoffeinbettung im Kno-chenlabor Priparative Voraussetzungen zur Schnitt undSchlifftechnik MTA 5:211
Hirsch C, Schajowicz, Galante ( 1967) Structural changes in thecervical spine Acta Orthop Scand lSuppll 109
Idelberger K ( 1975) Lehrbuch der Orthopidie Springer, Ber-lin Heidelberg New York
Isaacson PR ( 1979) Living anatomy: an anatomic basis for theosteopathic concept JAOA 79:745
Jesserer H ( 1975) Osteoporose: Pathologie, Klinik und Thera-pie Therapiewoche 29:2970
Jesserer H ( 1978) Osteoporose Rhein Arztebl 16 a: 619Johnson R, Crellin, White, Panjabi, Soutwick ( 1975) Some
new observations on the functional anatomy of the lowercervical spine Clin Orthop 111:192
Krimer J ( 1978) Bandscheibenbedingte Erkrankungen.Thieme, Stuttgart
Krogdahl T, Torgersen ( 1940) Uncovertebralgelenk undArthrosis deformans uncovertebralis Acta Radiol(Stockh) 21:23
Kummer B ( 1962) Funktioneller Bau und funktionelle Anpas-sung des Knochens Anat Anz 110:261
Lauer G ( 1980) Zur mechanisch orientierten Elastizitit spon-gi 6 ser Knochen Eine vergleichende Strukturanalyse.Diss, Erlangen
Lippert H ( 1966) Anatomie der Wirbelsiule unter Aspektenvon Entwicklung und Funktion Med Klin 61:41
Lyon E ( 1945) Uncovertebral osteophytes and osteochondro-sis of the cervical spine J Bone Joint Surg 27, Nr 2
Nathan H ( 1962) Osteophytes of the vertebral column J BoneJoint Surg lAml 44:243
Pauwels F ( 1965) Gesammelte Abhandlungen zur funktionel-len Anatomie des Bewegungsapparates Springer, BerlinHeidelberg New York
Payne E, Spillane ( 1957) The cervical spine: an anatomicopa-thological study of 70 specimens with particular referenceto the problem of cervical spondylosis Brain 80:571
Penning L ( 1978) Normal movements of the cervical spine.Am J Roentgenol 130:317
Pesch H-J, Henschke F, Seibold H ( 1977) Einflu B von Mecha-nik und Alter auf den Spongiosaumbau in Lendenwirbel-kdrpern und im Schenkelhals Virchows Arch A PatholHistol 377:27
Pesch H-J, Gunther CC, Strau B HJ ( 1980 a) Die diaphyslreVerlingerungsosteotomie an Katzenfemora Z Orthop118:768
Pesch H-J, Scharf HP, Lauer G, Seibold H ( 1980 b) Der alter-sabhingige Verbundbau der Lendenwirbelkorper Vir-chows Arch A Pathol Anat Histol 386:21
Pesch H-J, Becker Th, Bischoff W, Seibold H ( 1985) ZurRelevanz der physiologischen Osteoporose und der soge-nannten Osteoblasteninsuffizienz im Alter Vergleichenderadiologisch-morphometrische und statistische Unter-suchungen der Spongiosa von Lenden und Halswirbel-k 6 rpern Orthopide (im Druck)
Pliess G ( 1969) Die reaktive Plastizitt des Knochens DtschZahnirztl Z 24:99
Rizzi M ( 1976) Biomechanics of the spine Manuelle Medizin.Fischer, Heidelberg
Sager P ( 1969) Spondylosis cervicalis Diss, KopenhagenSchenk R, Merz W ( 1969) Histologisch-morphometrische
Untersuchungen fiber Altersatrophie und senile Osteo-porose in der Spongiosa des Beckenkammes Dtsch MedWochenschr 94:206
Schenk RK, Merz WA, Miiller J ( 1969) A quantitative histo-logical study on bone resorption in human cancellousbone Acta Anat 74:44
Schlfiter K ( 1965) Form und Struktur des normalen und patho-logisch verlinderten Wirbels Die Wirbelsaule in For-schung und Praxis, Bd 30 Hippokrates, Stuttgart
Schmorl G, Junghanns ( 1968) Die gesunde und kranke Wirbel-siule in R 6 ntgenbild und Klinik Thieme, Stuttgart
Serra I ( 1973) Theoretische Grundlagen des Leitz-Textur-Analyse-Systems Leitz-Mitt Wiss Tech lSuppl Il 4:125
Sigwart H ( 1974) Werkstoffkunde Dubbel In: Sass F, BoucheC, Leitner A (eds) Taschenbuch fr den Maschinenbau.Springer, Berlin Heidelberg New York
Stahl C ( 1977) Untersuchungen zur Mobilitat der cervikalenBandscheiben sowie Studien fiber die Anatomie des cervi-kalen und lumbalen Bewegungssegmentes Diss, Dussel-dorf
Stahl C, Huth ( 1980) Morphologischer Nachweis synovialerSpaltriume in der Uncovertebralregion cervicaler Band-scheiben Z Orthop 118:721
Tanaka Y ( 1974) A radiographic analysis on human lumbarvertebrae in the aged Virchows Arch A Pathol AnatHistol 366:351
Tittel K ( 1974) Beschreibende und funktionelle Anatomie desMenschen Fischer, Stuttgart
T 6ndury G ( 1974) Morphology of the cervical spine In: JungA, Kehr P, Magerl F, Weber BG (eds) The cervical spine.Huber, Bern
White A, Panjabi ( 1978) Clinical biomechanics of the spine.Lippincott, Philadelphia
Worsdorfer O, Magerl F ( 1980) Funktionelle Anatomie derWirbelsiule Hefte Unfallheilkd 149: 1
Wood PM ( 1979) Applied anatomy and physiology of the ver-tebral column Physiotherapy 65:248
Received August 7, 1984
211

























![Spondiloza Cdl Studenţi Mg 2010presentation1 [Autosaved]](https://img.dokumen.tips/doc/110x75/55cf972a550346d033900956/spondiloza-cdl-studenti-mg-2010presentation1-autosaved.jpg)

